1
Case ReportEnchephalopathy
Presentators: Dewi Putri Rejekinta Berutu
Azmeilia Syafitri Lubis
Supervisor:Prof. dr. H. Munar Lubis, Sp.A (K)
DEPARTMENT OF PEDIATRIC HAJI ADAM MALIK GENERAL HOSPITAL
FACULTY OF MEDICINEUNIVERSITY OF NORTH SUMATERA
2012

2
Chapter 1
• Introduction• Objective

3
. Introductionis a general term for a disease that alters a person’s brain function and mental state.
Enchephalopathy

4
Introduction
• There are many possible precipitants of encephalopathy.• Symptomps of enchephalopathy can generalized causing
decreased level of conciousness from minimal lethargy to coma.

5
Objective
• The aim of this study is to explore more about the theoritical aspects on metabolic enchephalopathy, and to integrate the theory and application of hepatic enchephalopathy case in daily life.

6
Chapter 2
• Literature Review: Enchepalophathy

7
Defenition
•Encephalopathy is an acute confusional state that is accompanied by an alterations in cortical function and disturbances of consciousness may range from mild confusional states to coma

8
Some types of enchephalopathy :
• Glycine enchephalopathy : caused by a metabolic disorder• Hepatic enchephalopathy : caused by disorders that affect the liver• Hypoxic enchephalopathy : caused by reduce oxygen to brain• Static enchephalopathy : permanent brain damage• Uremic enchephalopathy : caused by toxins remaining in the body• Wernicke’s enchephalopathy : caused by a thiamine deficiency, usually due to alcoholism.• Hashimoto’s enchephalopathy : an autoimmune disorder • Hypertensive enchehalophaty : caused by very high blood pressure• Toxic-metabolic enchephalopathy : general term to describe enchephalopathies caused by
infections, toxins or organ failure.

9
Etiology
• Infections• Trauma, Tumor/Paraneoplastic• Seizures, Stroke, (P)Sychiatric• Drugs (intoxication withdrawal), dementia
(Decompensated Dementia)• Electrolytes• Low glucose, Leukoencephalopathy• Inflammatory• Rheumatologic• Intracranial Pressure• Uremia• Metabolic, Malnutrition, Mitochondrial
Epidemiology
•Over 5.5 million people in the United States have been diagnosed with cirrhosis. One of this population, 30–45 % of patients develop overt encephalopathy during the course of their disease. This debilitating condition can negatively impact quality of life for patients and their families.•The frequency of hospitalization for enchephalopathy has nearly doubled over the last decade, with lengths of stay between 5 and 7 days.

10
RISK FACTOR
DehydrationHyponatremiaHypokalemia
Excessive dietary protein
Hepatocellular carcinoma
Terminal liver disease
Superimposed liver injuryTransjugular intrahepatic
portal-systemic
shunt
SurgeryCentral nervous
system acting drugs
Infections
Renal FailureUrinary
ObstructionGastrointerstinal bleedingConstipation

11
Some types of enchephalopathy :
• Glycine enchephalopathy : caused by a metabolic disorder• Hepatic enchephalopathy : caused by disorders that affect the liver• Hypoxic enchephalopathy : caused by reduce oxygen to brain• Static enchephalopathy : permanent brain damage• Uremic enchephalopathy : caused by toxins remaining in the body• Wernicke’s enchephalopathy : caused by a thiamine deficiency, usually due to alcoholism.• Hashimoto’s enchephalopathy : an autoimmune disorder • Hypertensive enchehalophaty : caused by very high blood pressure• Toxic-metabolic enchephalopathy : general term to describe enchephalopathies caused by
infections, toxins or organ failure.• Metabolic enchephalopathy : broad category that describes abnormalities of the water, electrolytes,
vitamins and other chemicals that adversely affect brain function

12
Pathophysiology
The pathogenesis of encephalopathy is incompletely understood, and the discussion that follows represents a collection of ideas and concepts that have emerged from recent research.
There is probably no single pathophysiology. Rather, many different perturbations of brain function may produce the same clinical syndrome. Potential mechanisms include a deficiency of substrates for oxidative metabolism, impaired synaptic transmission, and gross alterations in the water and electrolyte composition of the internal milieu. These mechanisms may be interrelated.
For example, Hyponatraemia is defined as a serum sodium <135 mEq/l. Under normal circumstances, the human body is able to maintain the plasma sodium within the normal range (135–145 mEq/l) despite wide fluctuations in fluid intake. The body’s primary defence against developing hyponatraemia is the kidney’s ability to generate a dilute urine and excrete free water. Hyponatraemia usually develops when there are underlying conditions that impair the kidney’s ability to excrete free water. There are a few clinical settings where patients most often develop hyponatraemic encephalopathy.

13
DIAGNOSIS
Mild•Change in sleep patterns•Changes in thinking•Confusion that is mild•Forgetfulness•Mental fogginess•Personality or mood changes•Poor concentration•Poor judgment•Worsening of handwriting or loss of other small hand movements
Severe•Abnormal movements or shaking of hands or arms•Agitation, excitement, or seizures (occur rarely)•Disorientation•Drowsiness or confusion•Inappropriate behavior or severe personality changes•Slurred speech•Slowed or sluggish movement
Symptoms many begin slowly and gradually worsen, or they may begin suddenly and be severe from the start. Patients with hepatic encephalopathy can become unconscious, unresponsive,
and possibly enter a coma.

14
•Jaundice, petechial hemorrhages, gastrointestinal bleeding, ascites, or hypothermia may indicate hepatic dysfunction.• A coarse facies, dry hair, or bradycardia suggests hypothyroidism.• Acne, obesity, and hypertension are common in Cushing syndrome.• Needle tracks in the skin raise the possibility of a toxic encephalopathy.• Hypertension suggests that the encephalopathy is caused by a metabolic disorder (e.g., a renal or endocrinologic disorder) or an ischemic disorder (e.g., a cerebrovascularor cardiovascular condition), and•Hepar enlargement, lead to cirrhosis hepatic.• Hypothermia suggests a metabolic or toxic cause.•Neurologic examination
PHYSICAL EXAMINATION

15
Blood testCT Scan of the head or MRIEEGLumbar PunctureArterial blood gasesElectrolyteChest radiograph
Tests may include:

16

17
Management & Treatment
•Dehydration : diuretics, intravenous infusion of physiologic saline, and therapy for the underlying cause of increased fluid and electrolyte losses. • Gastrointestinal bleeding is identified and treated appropriately. •Hypokalemia : vigorously corrected with parenteral potassium in enchephalopathy. •Severe hyponatremia : Limited infusions of hypertonic saline (3% NaCl, 150 mL intravenous) may be needed for very severe hyponatremia.
Correction
Precipating Factor
s

18
Management & Treatment
•Dietary protein : Restriction of dietary protein to 40 g/day or less used to be advocated for patients with enchephalopathy because of excessive dietary protein. The current recommended protein diet for patients is 0.8 to 1.5 g/kg/d.•Tranplantation•Adjuvant (antibiotics & dissacharides)•Symptomatic
Correction
Precipating Factor
s

19
Brain herniationBrain swellingIncreased risk of: Cardiovascular collapseKidney failureRespiratory failureSepsisPermanent nervous system damage (to movement, sensation, or mental state)Progressive, irreversible comaSide effects of medications
Complication

20
Acute encephalopathy may be treatable. Chronic forms of the disorder often keep getting worse or continue to come back.
Prognosis

21
Chapter 3
• Case Report

22
Case Report
Name : AIPAge : 4 monthsSex : Female Date of Admission:
May, 7th 2012

23
Main Complain
Seizure
3 days ago
Tonic clonic
Frek 10 times/day;
5’
Precipated by fever

24
Diarrhoea (+)◦ 3 days before fever◦ Frequency >10 times /day especially after having milk◦ Volume = 10-20 cc/ diarrhoea◦ Watery
Impairment of consciousness (+)◦ weak cry with moan impression (+) 2 days ago after
seizure.
Urine output(+) ◦ Colour : yellow (+)◦ Volume : less◦ Vomit (-)◦ history of melena (+) since 2 days ago◦ dyspnoe (-).

25
• Spontaneous and cried immediately• Help by midwives in clinic.• BW =3 Kg and BBL =48 cm• Injection of vitamin K (+)
History of Birth
• hypertension , DM, using herbal medicine (-).
• Early fetal membrane broken (+)
Historyof Pregnancy
• From birth to 3 months : Breast milk• From 3 months to now : Breast milk
+ formula milk
Feeding History
• Patient has been able to face downward
History of Growth and
Development
• Hep B, BCG, Polio, DPTHistory of Immunisation

26

27
Sensorium
Consciousness: ◦Alert (GCS 12: E:4, C=3, M=5)◦Temperature: 38oC.◦Body length: 63 cm. Head circumferences: 38 cm.
Upper Arm Circumferences: 9,5 cm.Anemic (-). Icteric (-). Cyanosis (-).
Oedema (-). Dyspnoe (+). BB/U = 5,3/6,2 x 100 % = 85,48 %TB/U = 63/62 x 100 % = 101,6 BB/TB = 5,3/6,6 x 100 % = 80,3 %Impression: Mild malnutrition

28
Localized Status
Head Neck Thorax•Fontanella : Large open flat, concave (+)•Hair: black, rarely, easily removed (-)•Head circumference: 38 cm•Eye: light reflex (+/+), isochoric pupillary, palpebra inferior conjunctival pallor (-/-), icteric sclera (-)•Nose: nostrils in breathing (+). •Ear and mouth: within normal limit
• Lymph node enlargement (-)
• Stiff neck (-)
•Simetris fusiformis. Retraction (+) epigastrial, intercostal, and suprasternal.• HR: 158 bpm, regular, murmur (-)• RR: 30 bpm, reguler, rales (-), wheezing (-).

29
Localized Status
Abdomen Urogenital Exremities
•Soepel•Peristaltik (+) normal•Hepar/Lien within normal limit
•Female,•Diapper rash (+)
•Ptechiae (-)•Pulse 158 bpm, regular, adequate pressure and volume•Warm acral•Capillary refill time < 3”.

30
Parameters Value Normal Value
Complete Blood Count
Hemoglobin 10,5 gr% 11,5 – 16,5 gr%
Erithrocyte 4,05 x 106 /mm3 4,2 – 5,4 x 106 /mm3
Leucocyte 13,7 x 103 /mm3 4- 11 x 103 /mm3
Hematocrite 31,6% 37 – 47%
Platelet 80.000 /mm3 150000 – 440000 /mm3
MCV 77,8 fL 80 – 95 fL
MCH 25,9 pg 27 – 32 pg
MCHC 33,3 gr% 32 – 36 gr%
RDW 12,7 % 11,6 – 15,5 %
MPV 9,90 fL 6,5 – 12.0 fL
PCT 0,079% 0,100- 0,500
LED 8 mm/hours < 15 mm/hours
Laboratory Findings (7th May 2012):

31
Diftel
Neutrophil 78,0 % 55 – 70 %
Limfosit 16 % 20 – 40 %
Monosit 4 % 2 – 8 %
Eosinophil 2 % 1 – 6 %
Basophil 0.100 % 0 – 1 %
ELECTROLYTE
Natrium 148 mEq/l 135- 155 mEq
Kalium 5,8 mEq/l 3,6- 5,5 mEq/l
Chloride 10/l2 mEq 96-106 mEq/l

32

33
Management• Head elevation 30 °• O2 ½ - 1 L/i nasal canule• IVFD RL 99 gtt/i micro
(rehydration from 19.30 to 23.30)• Inj. Ampicilin 250 mg/6 hours/iv• Inj. Cefotaxim 350 mg/8 hours/iv• Inj. Dexamethasone 1 mg/8
hours/ iv• Paracetamol 3x 100 mg (if need)• Diet based milk or complement-
based milk 60 cc/ 2 hours/ NGT
Diagnostic Planning• Consult to neurology• Consult to respirology• Mantoux test• Lumbal Punction• EEG• Head CT-Scan• Check electrolyte (Ca, Mg),
LFT, RFT, blood culture, urine culture, AGDA, CRP,
• Blood Glucose Level• Chest X-Ray

34
Follow Up

35
May 7th 2012
S Seizure (-), fever (-)
O Sens: GCS:12 (E=4, V=3, M=5), Temp: 36,1°C. Anemic (-). Icteric (-). Oedema (-). Cyanosis (-). Dyspnoe (+),
Body weight: 5,3 kg.
Head Eye: Light reflex (+)/(+).
Conjunctiva palpebra inferior anemic (-/-).
Isochoric pupil.
Sunken eye (+).
Prominent fontanella (- )
Ear-mouth: within normal limit. Nose: nostrils in breathing (+)
Neck Lymph node enlargement (-). Stiff neck (-).
Thorax Symmetrical fusiformis. Retraction (+) epigastrial and suprasternal.
HR: 160 bpm, reguler, murmur (-).
RR: 65 bpm, regular, rales (-/-). Snoring (-).
Abdomen Soepel, skin pinch fastly, peristaltic (+) N, Hepar/Lien: Palpable ± 1 cm under arcus costae, blunt.
Extremities Pulse 160 bpm, regular, adequate p/v, warm, CRT < 3”. Physiology reflex (APR + Normal, KPR +Normal).
Patologic reflex (Babinsky +, Meningeal -)
Genital Female. Eritematous lesion in anal area.
AEnchephalitis + bronchopneumony + mild – moderate dehydrationMeningoenchephalitis + bronchopneumony + mild – moderate dehydrationMeningoenchephalitis + bronchopneumony + Mild - moderate dehydration

36
P Management:•Head elevation 30°•O2 ½ - l L/i nasal canule•Rehydration RL 99 gtt/I since 19.30 pm - 23.30 pm•Injection of Ampicillin 250 mg/6 hr/iv (Skin Test)•Injection of Cefotaxim 350 mg/8 hr/iv (Skin Test)•Injection of dexamethasone 1mg/8 hr/iv•Paracetamol 3 x 100 mg (if needed)•Diet breast milk/ PASI 60 cc/2 hr/NGT•10.00 pm Injection Phenytoin 100 mg in 20 cc NaCl 0,9 % out in 20 minutes, after 12 hours 25 mg/12 hr in 20 cc NaCl 0.9 %.

37
Complete Blood Count
Hemoglobin 10,5 gr% 11,5 – 16,5 gr%
Erithrocyte 4,05 x 106 /mm3 4,2 – 5,4 x 106 /mm3
Leucocyte 13,7 x 103 /mm3 4- 11 x 103 /mm3
Hematocrite 31,6% 37 – 47%
Platelet 80.000 /mm3 150000 – 440000 /mm3
MCV 77,8 fL 80 – 95 fL
MCH 25,9 pg 27 – 32 pg
MCHC 33,3 gr% 32 – 36 gr%
RDW 12,7 % 11,6 – 15,5 %
MPV 9,90 fL 6,5 – 12.0 fL
PCT 0,079% 0,100- 0,500
LED 8 mm/hours < 15 mm/hours
Diftel:
Neutrophil 78,0 % 55 – 70 %
Limfosit 16 % 20 – 40 %
Monosit 4 % 2 – 8 %
Eosinophil 2 % 1 – 6 %
Basophil 0.100 % 0 – 1 %
ELECTROLYTE
Natrium 148 mEq/l 135- 155 mEq
Kalium 5,8 mEq/l 3,6- 5,5 mEq/l
Chloride 10/l2 mEq 96-106 mEq/l
Laboratory Findings on 7th May 2012

38
May 8 th 2012
S Seizure (-), fever (-).
O Sens: GCS:12 (E=4, V=3, M=5), Temp: 36,1°C. Anemic (-). Icteric (-). Oedema (-). Cyanosis (-).
Dyspnoe (+), Body weight: 5,3 kg.
Head Eye: Light reflex (+)/(+).
Conjunctiva palpebra inferior anemic (-/-).
Isochoric pupil.
Sunken eye (+).
Prominent fontanella (-)
Ear-mouth: within normal limit.. Nose: nostrils in breathing (+)
Neck Lymph node enlargement (-). Stiff neck (-).
Thorax Simetrical fusiformis. Retraction (+) epigastrial and suprasternal.
HR: 140 bpm, reguler, murmur (-).
RR: 52 bpm, regular, rales (-/-). Snoring (-).
Abdomen Soepel, skin pinch fastly, peristaltic (+) N, Hepar/Lien: Palpable ± 1 cm under arcus costae, blunt.
Extremities Pulse 140 bpm, regular, adequate p/v, warm, CRT < 3”. Physiology reflex (APR + Normal, KPR
+Normal). Patologic reflex (Babinsky +, Meningeal -)
Genital Female. Eritematous lesion in anal area.
A - Enchephalitis
- Meningoenchephalitis + Bronkhopneumonia
- Meningoenchephalitis + Mild to moderate dehydration

39
P Management:•Head elevation 30°•O2 ½ - l L/i nasal canule•IVFD D5 restriction 25 % 16 gtt/i•Phenytoin 25 mg/12 hr/iv in 20 cc NaCl 0,9 % out in 20 minutes•Injection of Ampicillin 250 mg/6 hr/iv (H1)•Injection of Cefotaxim 350 mg/8 hr/iv (H1)•Injection of dexamethasone 1mg/8 hr/iv (H1)•Paracetamol 3 x 100 mg (if needed)•Diet breast milk/ PASI 70 cc/3 hr/NGT.•(10.30 am) : Phenytoin 10 mg/kgBW in 6cc NaCl 0,9% out in 20 minutes•(05.00 pm): Correction of hipocalsemy (Ca= 6,6 mg/dl) 0,5 mg/kg BB= 0,5 x 5,3= 2,65 mg in 3 cc out in 20 minutes
R •Consult to neurology•Consult to respirology•Mantoux test•Lumbal punction•Electroenchepalograph•Head CT-Scan•Electrolyte test: LFT, RFT, blood culture, urine culture, AGDA, CRP, procalcitonin, lactate acid, LED

40
Dipstic Results:Leu/Nit/Uro/Pro/pH/Blo/SG/Ket/Bil/Glu:± /- /- /++ /6 /1,030 /- /- /- /-
Blood Glucose Test: 46 mg/dl
Blood Culture: Bacteria was not found

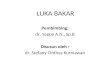
41Chest Radiograph
Result of Consult to Radiology: - The heart, sinus & diaphragma are normal. - The lung: consolidation upper right lung field. There is triangle opaque shadow at lower right lung field.-Impression: a. Pneumoniab. Atelectasis segmental at posterior right lung

42
Laboratory finding on 8th May 2012
Parameters Value Normal Value
Complete Blood Count
Hemoglobin 10,3 gr% 10,7 – 17,1 gr%
Erithrocyte 3,72 x 106 /mm3 3,75 – 4,95 x 106 /mm3
Leucocyte 11,12 x 103 /mm3 6,0- 17,5 x 103 /mm3
Hematocrite 30,80 % 38 – 52%
Platelet 103.00 /mm3 217000 – 497000 /mm3
MCV 82,80 fL 93 -115 fL
MCH 27,70 pg 29 – 35 pg
MCHC 33,4 gr% 28 – 34 gr%
RDW 13,5 % 14,9 – 18,7 %
MPV 10,40 fL 7,2 – 10,00 fL
PCT 0,011 %
Diftel:
Neutrophil 94,10 % 37 – 80 %
Limfosit 4,20 % 20 – 40 %
Monosit 1,70 % 2 – 8 %
Eosinophil 0.00 % 1 – 6 %
Basophil 0,000 % 0 – 1 %
Kesan: normocrom normositter anemia+ trombositopenia

43
BLOOD GASES ANALYSIS
pH 7,40 7,35- 7,45
pCO223,0 38- 42 mmHg
pO2173,3 85- 100 mmHg
HCO314,20 22- 26 mmol/l
CO2 total 14,90 19- 25 mmol/l
BE -9,3 -2 2
O2 saturation 99,3 % 95- 100
ELECTROLYTE
Calsium 6,6 8,4- 10,8 mg/dl
Natrium 134 135- 155 mEq
Kalium 3,7 3,6- 5,5 mEq
Phospor 3,2 5,0- 10,8 mEq
Cloride 110 96- 106 mEq
Magnesium 1,61 1,4- 1,8 mEq
Procalcitonin 79,03 <0.05 ng/ mL

44
9th May 2012
S Seizure (-), fever (-), Conciousness: increase (this patient crying more loudly).
O Sens: GCS:14 (E=4, V=4, M=5), Temp: 37,5°C. Anemic (-). Icteric (-). Oedema (-). Cyanosis (-).
Dyspnoe (+), Body weight: 5,5 kg.
Head Eye: Light reflex (+)/(+)
Conjunctiva palpebra inferior anemic (-/-)
Isochoric pupil
Sunken eye (-)
Prominent fontanella (-)
Ear-mouth: within normal limit. Nose: nostrils in breathing (-)
Neck Lymph node enlargement (-). Stiff neck (-).
Thorax Symmetrical fusiformis. Retraction (-)
HR: 140 bpm, reguler, murmur (-).
RR: 48 bpm, regular, rales (-/-). Snoring (-).
Abdomen Soepel, skin pinch fastly, peristaltic (+) N, Hepar/Lien: Not palpable
Extremities Pulse 140 bpm, regular, adequate p/v, warm, CRT < 3”.
Genital Female. Within normal linit
A Enchephalopathy

45
P Management:
Head elevation 30°
O2 ½ - l L/i nasal canule
IVFD D5 Na Cl 0,9 % 16 gtt/i micro
Injection of Phenytoin 25 mg/12 hr/iv in 20 cc NaCl 0,9 % out in 20 minutes
Injection of Ampicillin 250 mg/6 hr/iv (H2)
Injection of Cefotaxim 350 mg/8 hr/iv (H2)
Injection of dexamethasone 1mg/8 hr/iv (H2)
Paracetamol 3 x 100 mg (if needed)
Nebule Na Cl 2,5 cc +1 amp Ventoline/ 8 jam
Diet breast milk/ PASI 70 cc/3 hr/NGT.
R Waiting for the answer neurology consult
Consult to respirology
Mantoux test
Check electrolyte
The Result of Consult Respirology:Clinically, symptom of respirology was not found.

46
Parameters Value Normal Value
Function of hemostatic
PT +INR
Protombine Time
Control
Patient
12,50 sec
18,0 sec
INR 1,36
APTT
Control
Patient
29,50
29,70
Electrolyte
Calcium 6,9 8,4- 10,8 mg/dl
Natrium 136 135-155 mEq
Kalium 3,3 3,6- 5,5 mEq
Chloride 103 95- 106 mEq
Magnesium 1,77 1,4- 1,8 meq

47
10th May 2012
S Seizure (-), fever (-), diarrhoea (+)
O Sens: GCS:15 (E=5, V=4, M=5), Temp: 37,1°C. Anemic (-). Icteric (-). Oedema (-). Cyanosis (-).
Dyspnoe (+), Body weight: 5,5 kg.
Head Eye: Light reflex (+)/(+).
Conjunctiva palpebra inferior anemic (-/-).
Isochoric pupil.
Sunken eye (-).
Prominent fontanella (-).
Ear-mouth: within normal limit. Nose: nostrils in breathing (-)
Neck Lymph node enlargement (-). Stiff neck (-).
Thorax Symmetrical fusiformis. Retraction (-)
HR: 135 bpm, reguler, murmur (-).
RR: 42 bpm, regular, rales (-/-). Snoring (-).
Abdomen Soepel, skin pinch fastly, peristaltic (+) N, Hepar/Lien: not palpable
Extremities Pulse 135 bpm, regular, adequate p/v, warm, CRT < 3”.
Genital Female. Within normal limit.
A Enchephalopathy ec electrolyte imbalance + GE without dehydration

48
P Management:
IVFD D5 Na Cl 0,25 % 16 gtt/i2
Injection of Phenytoin 25 mg/12 hr/iv in 20 cc NaCl 0,9 % out in 20
minutes
Injection of Cefotaxim 350 mg/8 hr/iv (H3)
Injection of dexamethasone 1mg/8 hr/iv (H3)
Paracetamol 3 x 100 mg (if needed)
Nebule Na Cl 2,5 cc +1 amp Ventoline/ 8 jam
Diet breast milk/ PASI 70 cc/3 hr/NGT.
Zink 1 x 10 mg
R Consult to gastroenterohepatology

49
11th May 2012 S Seizure (-), fever (+), diarrhoea (+)
O Sens: GCS:13 (E=4, V=4, M=5), Temp: 37,8°C. Anemic (-). Icteric (-). Oedema (-). Cyanosis (-).
Dyspnoe (+), Body weight: 5,5 kg.
Head Eye: Light reflex (+)/(+).
Conjunctiva palpebra inferior anemic (-/-).
Isochoric pupil.
Sunken eye (-).
Prominent fontanella (-).
Ear-mouth: within normal limit. Nose: nostrils in breathing (-)
Neck Lymph node enlargement (-). Stiff neck (-).
Thorax Symmetrical fusiformis. Retraction (-)
HR: 132 bpm, reguler, murmur (-).
RR: 40 bpm, regular, rales (-/-). Snoring (-).
Abdomen Soepel, skin pinch fastly, peristaltic (+) N, Hepar/Lien: not palpable
Extremities Pulse 132 bpm, regular, adequate p/v, warm, CRT < 3”.
Genital Female. Within normal limit.
A Enchephalopathy + Gastroenteritis without dehydration

50
P
R
Management:
IVFD D5 Na Cl 0,25 % 16 gtt/i
Injection of Phenytoin 25 mg/12 hr/iv in 20 cc NaCl 0,9 % out in 20 minutes
Injection of Cefotaxim 350 mg/8 hr/iv (H4)
Injection of dexamethasone 1mg/8 hr/iv (H4)
Paracetamol 3 x 100 mg (if needed)
Nebule Na Cl 2,5 cc +1 amp Ventoline/ 8 jam
Diet breast milk/ PASI 70 cc/3 hr/NGT.
Zink 1 x 10 mg
Give low lactose milk
Check routine feces
Feces culture
Parameters Value Normal Value
ELECTROLYTE
Calcium (Ca) 7,2 8,4 – 10,8 mg/dL
Natrium (N) 158 135 – 155 mEq/L
Kalium (K) 3,3 3,6 – 5,5 mEq/L
Phospor 2,9 5,0 – 10,8 mEq/ L
Chloride (Cl) 108 96 – 106 mEq/L
Magnesium (Mg) 1,71 1,4 – 1,8 mEq/L

51
12th May 2012
S Seizure (-), fever (-), diarrhoea (+)
O Sens: Compos mentis Temp: 36,8°C. Anemic (-). Icteric (-). Oedema (-). Cyanosis (-).
Dyspnoe (-), Body weight: 5,6 kg.
Head Eye: Light reflex (+)/(+).
Conjunctiva palpebra inferior anemic (-/-).
Isochoric pupil.
Sunken eye (-).
Prominent fontanella (-).
Ear-mouth: within normal limit. Nose: nostrils in breathing (-)
Neck Lymph node enlargement (-). Stiff neck (-).
Thorax Symmetrical fusiformis. Retraction (-)
HR: 104 bpm, reguler, murmur (-).
RR: 42 bpm, regular, rales (-/-). Snoring (-).
Abdomen Soepel, skin pinch fastly, peristaltic (+) N, Hepar/Lien: not palpable
Extremities Pulse 104 bpm, regular, adequate p/v, warm, CRT < 3”.
Genital Female.
A Enchephalopathy + Gastroenteritis without dehydration + suspect cows milk allergy

52
P
R
Management:
IVFD D5 Na Cl 0,25 % 16 gtt/i
Injection of Phenytoin 2x 25 mg
Injection of Cefotaxim 350 mg/8 hr/iv (H5)
Zink 1 x 10 mg
Lacto B Sach 2 x 1
Paracetamol 3 x 100 mg (if needed)
Nebule Na Cl 2,5 cc +1 amp Ventoline/ 8 jam
Diet breast milk/ PASI low lactose 70 cc/3 hr/NGT.
Check routine feces
Feces culture

53
13th May 2012
S Seizure (-), fever (-), diarrhoea (+)
O Sens: Compos mentis Temp: 36,8°. Anemic (-). Icteric (-). Oedema (-). Cyanosis
(-). Dyspnoe (-), Body weight: 5,6 kg.
Head Eye: Light reflex (+)/(+).
Conjunctiva palpebra inferior anemic (-/-).
Isochoric pupil.
Sunken eye (-).
Prominent fontanella (-).
Ear-mouth: within normal limit. Nose: nostrils in breathing (-)
Neck Lymph node enlargement (-). Stiff neck (-).
Thorax Symmetrical fusiformis. Retraction (-)
HR: 100 bpm, reguler, murmur (-).
RR: 40 bpm, regular, rales (-/-). Snoring (-).
Abdomen Soepel, skin pinch fastly, peristaltic (+) N, Hepar/Lien: not palpable
Extremities Pulse 100 bpm, regular, adequate p/v, warm, CRT < 3”.
Genital Female.
A Enchephalopathy ec electrolyte imbalance+ Gastroenteritis without
dehydration + suspect cows milk allergy

54
P
R
Management:
IVFD D5 Na Cl 0,25 % 16 gtt/i
Injection of Phenytoin 2x 25 mg
Injection of Cefotaxim 350 mg/8 hr/iv (H6)
Zink 1 x 10 mg
Lacto B Sach 2 x 1
Paracetamol 3 x 100 mg (if needed)
Nebule Na Cl 2,5 cc +1 amp Ventoline/ 8 jam
Diet breast milk/ PASI low lactose 70 cc/3 hr/NGT.
Check routine feces
Feces culture
Blood culture

55
14th May 2012
S Seizure (-), fever (-), diarrhoea (+)
O Sens: Compos mentis Temp: 36,8°. Anemic (-). Icteric (-). Oedema (-). Cyanosis
(-). Dyspnoe (-), Body weight: 5,6 kg.
Head Eye: Light reflex (+)/(+).
Conjunctiva palpebra inferior anemic (-/-).
Isochoric pupil.
Sunken eye (-).
Prominent fontanella (-).
Ear-mouth: within normal limit. Nose: nostrils in breathing (-)
Neck Lymph node enlargement (-). Stiff neck (-).
Thorax Symmetrical fusiformis. Retraction (-)
HR: 104 bpm, reguler, murmur (-).
RR: 38 bpm, regular, rales (-/-). Snoring (-).
Abdomen Soepel, skin pinch fastly, peristaltic (+) N, Hepar/Lien: not palpable
Extremities Pulse 104 bpm, regular, adequate p/v, warm, CRT < 3”.
Genital Female.
A Enchephalopathy ec electrolyte imbalance+ Gastroenteritis without
dehydration + suspect cows milk allergy

56
P
R
Management:
IVFD D5 Na Cl 0,25 % 16 gtt/i
Injection of Phenytoin 2x 25 mg
Injection of Cefotaxim 350 mg/8 hr/iv (H7)
Zink 1 x 10 mg
Lacto B Sach 2 x 1
Paracetamol 3 x 100 mg (if needed)
Nebule Na Cl 2,5 cc +1 amp Ventoline/ 8 jam
Diet breast milk/ PASI low lactose 75 cc/3 hr/NGT.
Check electrolyte (Ca, Mg)

57
15th May 2012
S Seizure (-), fever (-), diarrhoea (-)
O Sens: Compos mentis Temp: 37°. Anemic (-). Icteric (-). Oedema (-). Cyanosis
(-). Dyspnoe (-), Body weight: 5,6 kg.
Head Eye: Light reflex (+)/(+).
Conjunctiva palpebra inferior anemic (-/-).
Isochoric pupil.
Sunken eye (-).
Prominent fontanella (-).
Ear-mouth: within normal limit. Nose: nostrils in breathing (-)
Neck Lymph node enlargement (-). Stiff neck (-).
Thorax Symmetrical fusiformis. Retraction (-)
HR: 116 bpm, reguler, murmur (-).
RR: 42 bpm, regular, rales (-/-). Snoring (-).
Abdomen Soepel, skin pinch fastly, peristaltic (+) N, Hepar/Lien: not palpable
Extremities Pulse 116 bpm, regular, adequate p/v, warm, CRT < 3”.
Genital Female.
A Enchephalopathy ec electrolyte imbalance + Gastroenteritis without
dehydration + suspect cows milk allergy

58
P
R
Management:
IVFD D5 Na Cl 0,25 % 16 gtt/i
Injection of Phenytoin 2x 25 mg
Injection of Cefotaxim 350 mg/8 hr/iv (H8)
Zink 1 x 10 mg
Lacto B Sach 2 x 1
Paracetamol 3 x 100 mg (if needed)
Nebule Na Cl 2,5 cc +1 amp Ventoline/ 8 jam
Diet breast milk/ PASI low lactose 75 cc/3 hr/NGT.
Waiting for blood electrolyte result
Result of bactery culture: negative
Laboratory Finding on 15th May 2012Parameters Value Normal Value
ELECTROLYTE
Calcium (Ca) 8,4 8,4 – 10,8 mg/dL
Natrium (N) 136 135 – 155 mEq/L
Kalium (K) 3,7 3,6 – 5,5 mEq/L
Phospor - 5,0 – 10,8 mEq/ L
Chloride (Cl) 109 96 – 106 mEq/L
Magnesium (Mg) 1,62 1,4 – 1,8 mEq/L

59
16th May 2012
S Seizure (-), fever (-), diarrhoea (-)
O Sens: Compos mentis Temp: 37° C. Anemic (-). Icteric (-). Oedema (-). Cyanosis
(-). Dyspnoe (-), Body weight: 5,6 kg.
Head Eye: Light reflex (+)/(+).
Conjunctiva palpebra inferior anemic (-/-).
Isochoric pupil.
Sunken eye (-).
Prominent fontanella (-).
Ear-mouth: within normal limit. Nose: nostrils in breathing (-)
Neck Lymph node enlargement (-). Stiff neck (-).
Thorax Symmetrical fusiformis. Retraction (-)
HR: 106 bpm, reguler, murmur (-).
RR: 36 bpm, regular, rales (-/-). Snoring (-).
Abdomen Soepel, skin pinch fastly, peristaltic (+) N, Hepar/Lien: not palpable
Extremities Pulse 106 bpm, regular, adequate p/v, warm, CRT < 3”.
Genital Female.
A Enchephalopathy ec electrolyte imbalance

60
P Management:
IVFD D5 Na Cl 0,25 % 16 gtt/i
Injection of Phenytoin 2x 25 mg
Injection of Cefotaxim 350 mg/8 hr/iv (H9)
Zink 1 x 10 mg
Lacto B Sach 2 x 1
Paracetamol 3 x 100 mg (if needed)
Nebule Na Cl 2,5 cc +1 amp Ventoline/ 8 jam
Diet breast milk/ PASI low lactose 75 cc/3 hr/NGT.
Waitng for blood electrolyte result
This patient may go home

61
HOME VISIT 25th May 2012
S Seizure (-), fever (-), diarrhoea (-)
O Sens: Compos mentis Temp: 36,2°C. Anemic (-). Icteric (-). Oedema (-).
Cyanosis (-). Dyspnoe (-), Body weight: 5,6 kg. Head circumference= 38 cm,
Upper arm circumference= 9,5 cm.
Head Eye: Light reflex (+)/(+).
Conjunctiva palpebra inferior anemic (-/-).
Isochoric pupil.
Sunken eye (-).
Prominent fontanella (-).
Ear-mouth: within normal limit. Nose: nostrils in breathing (-)
Neck Lymph node enlargement (-). Stiff neck (-).
Thorax Symmetrical fusiformis. Retraction (-)
HR: 158 bpm, reguler, murmur (-).
RR: 26 bpm, regular, rales (-/-). Snoring (-).
Abdomen Soepel, skin pinch fastly, peristaltic (+) N, Hepar/Lien: not palpable
Extremities Pulse 158 bpm, regular, adequate p/v, warm, CRT < 3”.
Genital Female.
A

62
P
R
Management: Amoxycillin syrup 3 x 1 cthAmbroxol pulv 3 x 1
Control to General Hospital Of Haji Adam Malik Medan

63
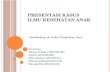
Size of house 4 x 5 meter
Bathroom, Toilet & Location to wash Kitchen
Guest room+Family room+Making cake room Bed room
PintuJendela
Jendela
Impression: Bad ventilasion, small house but crowded people, bad sanitation.
SKETCH OF HOUSE

64
Home Visit (25th May 2012)
Address:Pasar 11, Gg.Rejeki, Kec. Percut, Sei Tuan
Impression :Bad Sanitation

65
Discussion
THEORY PATIENT
Definition Encephalopathy is an acute confusional state that is accompanied by an alterations in cortical function and disturbances
In this patient, mental status changes and conciousness impairment was found
Causes DehydrationElectrolyte imbalanceExcessive dietary proteinRenal FailureUrinary ObstructionGastrointerstinal bleedingSurgeryInfectionsDrugsHypoxia, intravascular diseaseetc
In this patient, the precipitating factor is dehydration (electrolyte imbalance)
Types Glycine. Hepatic, Hypoxic, Static, Uremic, Wernicke. Hashimoto’s. Hypertensive, Toxic & Metabolic
This patient is metabolic enchephalopathy

66
THEORY PATIENT
Clinical Manifestation
• Change in sleep patterns• Changes in thinking• Confussion impairment• Mental fogginess• Personality or mood changes• Poor concentration• Abnormal movements or shaking of hands or arms• Agitation, excitement, or seizures (occur rarely)• Disorientation• Drowsiness or confusion• Inappropriate behavior or severe personality changes• Slurred speech• Slowed or sluggish movement
In this patient, seizure and conciousness impairment was found
Supporting Examination
Blood testCT Scan of the head or MRIEEGLumbar PunctureArterial blood gasesElectrolyteChest radiograph
In this patient, supporting examinations are:-Complete blood count-Chest radiograph-Arterial blood gases-Electrolyte

67
THEORY PATIENT
Management
Correction by Precipating Factors, adjuvant therapy (antibiotics and dissacharides), transplantation and symptomatic.
Treatment of this patients are:- RL 99 gtt/i micro (rehydration from 19.30 to 23.30)•Head elevation 30°•O2 ½ - l L/i nasal canule•IVFD D5 Nacl 25 % 16 gtt/i•Phenytoin 25 mg/12 hr/iv in 20 cc NaCl 0,9 % out in 20 minutes•Injection of Ampicillin 250 mg/6 hr/iv (H1)•Injection of Cefotaxim 350 mg/8 hr/iv (H1)•Injection of dexamethasone 1mg/8 hr/iv (H1)•Paracetamol 3 x 100 mg (if needed)•Diet breast milk/ PASI 70 cc/3 hr/NGT.•(10.30 am) : Phenytoin 10 mg/kgBW in 6cc NaCl 0,9% out in 20 minutes•(05.00 pm): Correction of hipocalsemy (Ca= 6,6 mg/dl) 0,5 mg/kg BB= 0,5 x 5,3= 2,65 mg in 3 cc out in 20 minutes
Prognosis Acute encephalopathy may be treatable. Chronic forms of the disorder often keep getting worse or continue to come back.
In this patient, enchephalopathy was treatable.,

68
THANK YOU

69
References
Camara-Chua, Pia Teresa A, MD., Enchephalopathies. 2010. Available from: NEJM.org\
Garcia-Tsao G. Cirrhosis and its sequelae. In: Goldman L, Ausiello D, eds. Cecil Medicine. 24th ed. Philadelphia, Pa: Saunders Elsevier; 2011:chap 156.
K. Lin , Chou-Ching. EEG Manifestations in Metabolic Encephalopathy.2005. Acta Neurologica Taiwanica Vol 14 No 3 September 2005
Kaplan PW, Fisher RS, Pathophysiology of Encephalopathy. 2005. New York: Demos Medical Publishing.
Munos, J.S., Hepatic Enchephalopathy. Available from: http://www.med.upenn.edu/gastro/documents/MedClinNAencephalopathy2008.pdf
Myer, Edwin, MD., Acute toxic-metabolic encephalopathy in children.2010. Available from: file:///E:/Print/acute-toxic-metabolic-encephalopathy-in-children.htm
Riordhan, M.S., Treatment of hepatic enchepalophaty. 2012. Available from: http://www.nejm.org/action/showImage?doi=10.1056%2FNEJM199708143370707&iid=t01
Spundorfer, Phillip., Electrolyte and Fluids. Comprehensive Pediatric Hospital Medicine. 2007. Philadhelpia: Mosby Elsevier.
Swaiman, K.F., Pediatric Neurology Principles & Practise. 1999. Missouri: A Hartcourt Health Sciences Company.
Wright, W.L., Current Clinical Neurology: Handbook of Neurocritical Care. 2004. Totowa NJ: Humana Press Inc.