Pediatric TB Basics and Evaluation and Management of Exposed Neonates
Ann M. Loeffler, MDRandall Children’s Hospital, Portland OR &Curry International TB Center, Oakland CA
September, 2017
No Disclosures
Objectives:• Describe the basic differences between pediatric and
adult TB in order to optimize patient outcomes• Assess the risk of transmission to a neonate following
an exposure in a nursery / NICU and identify those who will need evaluation
• Evaluate a neonate for evidence of TB disease following a known exposure

Pediatric Tuberculosis Basics
When it comes to tuberculosis -
Children are really and truly not just small adults!

1) Young children are more likely to get disease
TB infected adults have a 5 – 10% lifetime risk of developing TB disease (aka active TB ) Increased risk with HIV, cancer, immunosuppression, diabetes, renal failure
Babies less than one year of age have a 40% chance of developing disease! The risk gradually declines until age 5 yrs
Adolescents have a higher risk again
The same immunocompromising
conditions increase risk of TB in
children as adults
9/12/2017 RANDALL CHILDREN'S HOSPITAL 4

2) Children have different radiographic abnormalities
Adults commonly have apical and cavitary disease > Streaky fibrotic changes might indicate scarring
Children can have disease in any lobe of the lung> 25% have more than one lobe affected
Children VERY commonly have intrathoracic lymph node swelling> Perihilar, mediastinal, paratracheal, subcarinal nodes> Often seen best or confirmed on the lateral view> Can cause airway compression with post obstructive infiltrate, collapse or
hyperinflation> Can erode through the airway and cause endotracheal disease /
bronchogenic spread Young children are more likely to have miliary disease Children rarely have cavitary disease or pleural disease
9/12/2017 RANDALL CHILDREN'S HOSPITAL 5

9/12/2017 RANDALL CHILDREN'S HOSPITAL 6

9/12/2017 RANDALL CHILDREN'S HOSPITAL 7

9/12/2017 RANDALL CHILDREN'S HOSPITAL 8
ME
3) Children with TB often have subtle or no symptoms
Most US children with TB are asymptomatic Often identified during a “contact investigation”
The chest x-ray findings have NO correlation with signs and symptoms If a child has no symptoms and an impressive
radiograph, it’s more likely that they have TB disease
Infants and adolescents with TB are most likely to have signs and symptoms – fever and cough
9/12/2017 RANDALL CHILDREN'S HOSPITAL 9

9/12/2017 RANDALL CHILDREN'S HOSPITAL 10

9/12/2017 RANDALL CHILDREN'S HOSPITAL 11
4) Most young children are not contagious
In general, young children are not contagious with their TB disease
This is because they have few organisms in their lung lesions
Most of what you see on X-ray is the immune response – not lots of germs like in adult cavities
There have been a few newborns with TB who have been contagious
Adolescents and teenagers can be contagious
9/12/2017 RANDALL CHILDREN'S HOSPITAL 12

5) It’s hard to collect sputum from children
25 – 50% of children have culture proven tuberculosis Older children can undergo sputum induction with 7%
hypertonic saline and are taught to cough into a cup In some places, younger children inhale the
aerosolized hypertonic saline and as they cough, folks thread a tube into the back of their throat and collect sputum
I generally prefer gastric aspiration for young children and get about 40% yield
http://www.currytbcenter.ucsf.edu/products/pediatric-tuberculosis-guide-gastric-aspirate-procedure/video
9/12/2017 RANDALL CHILDREN'S HOSPITAL 13

9/12/2017 RANDALL CHILDREN'S HOSPITAL 14
Nicholas Loeffler in his first acting role
Neutralize the specimen with bicarbonate promptly
6) Kids have more extrapulmonary TB
• Lymphatic – mediastinal and scrofula• 13% meningeal• 6% pleural• 5% miliary• 4% bone and joint• 5% others
intra-abdominal ears and mastoids skin, laryngeal, kidneys, etc.
9/12/2017 RANDALL CHILDREN'S HOSPITAL 15
7) It’s really hard to get the meds in In the US, TB drugs don’t come in kid-friendly formulations
The liquid INH which is commercially made causes belly ache and diarrhea is > 50% of kids (better tolerated in babies)
INH crushed into sugary liquid breaks down and is not effective
9/12/2017 RANDALL CHILDREN'S HOSPITAL 16

7) It’s really hard to get the meds in Try crushed or fragmented pills / capsules layered into soft foods
For babies, can put it into some breastmilk, formula or water –preferably just before dosing.
Put it in a small volume so they don’t have to drink a whole bottle to get the dose down
It doesn’t dissolve well, so use a medicine dropper or med syringe with a bigger opening
Try puffing in their face to elicit a swallow. http://www.currytbcenter.ucsf.edu/products/pediatric-tuberculosis-
online-presentation/resources (and here on the webinar!)
9/12/2017 RANDALL CHILDREN'S HOSPITAL 17

All doses are once daily / close to the same time
9/12/2017 RANDALL CHILDREN'S HOSPITAL 18
Child’s weight INH daily dose (10-15mg/kg/d)
Kilograms Pounds Milligrams 100mg tabs
300 mg tabs
3-5 kg 6.6-11 # 50 mg ½5-7.5 11-16.4 75 ¾
7.5-10 16.5-22 100 110-15 22-33 150 ½ 15-20 33-44 200 2
Over 20 Over 44 300 1Maximum dose 300 mg !!
Vitamin B 6 (pyridoxine) supplementation Not needed for most children
Exceptions> Exclusively breastfed babies> HIV Infected> Milk & meat deficient diets > Symptoms of peripheral neuropathy / CNS side effects
Doses (all once daily; can give with INH):> Babies ¼ of a 25 mg tablet = 6.25 mg> Toddlers ½ of a 25 mg tablet = 12.5 mg> Older kids 25 mg tablet
9/12/2017 RANDALL CHILDREN'S HOSPITAL 19
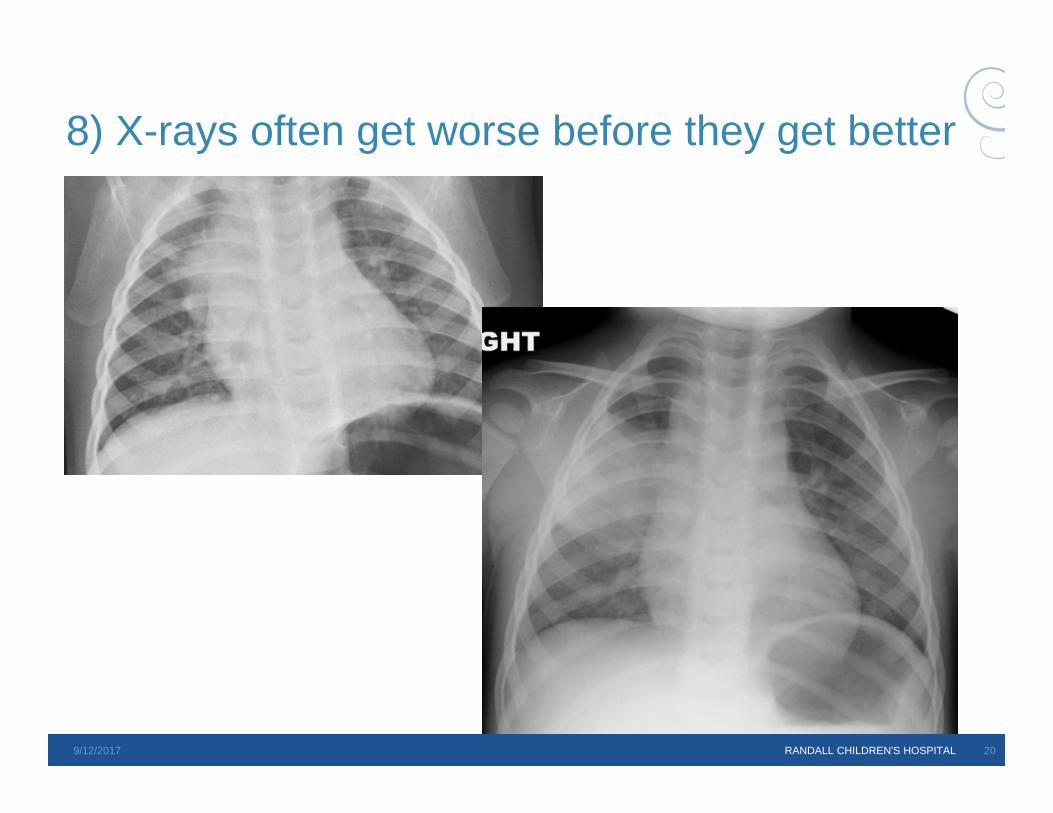
8) X-rays often get worse before they get better
9/12/2017 RANDALL CHILDREN'S HOSPITAL 20

9/12/2017 RANDALL CHILDREN'S HOSPITAL 21
Is she clinically improving?Is she getting the right drugs?Is she getting the right doses?Is she missing doses?Do we have the right diagnosis?
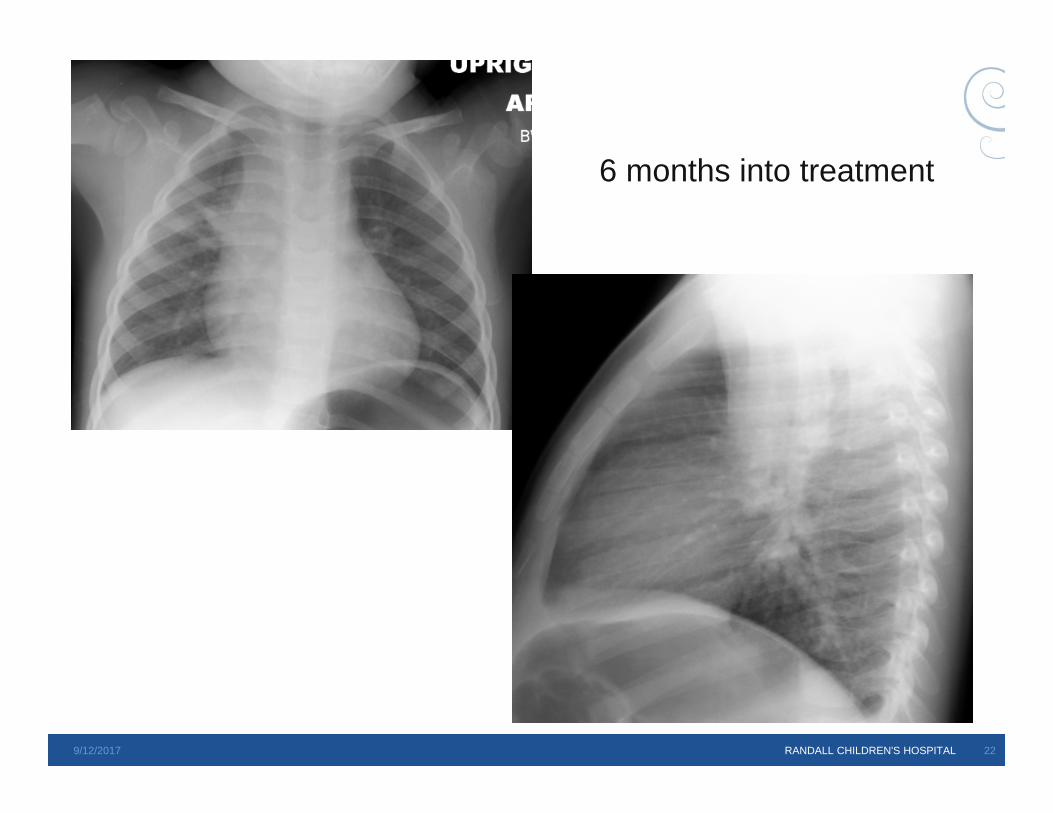
9/12/2017 RANDALL CHILDREN'S HOSPITAL 22
6 months into treatment

Perinatal Tuberculosis Like other infections of the newly born, TB can be
> Congenital – acquired in utero Hematogenous acquisition, often during maternal bacillemia
– Primary or disseminated TB in mom most common Tubercule can rupture into amniotic fluid and baby can swallow
or “inhale” infected fluid into the lung
> Natal – acquired during the birth process Late swallowing or inhaling of amniotic fluid or urogenital
secretions
> Postnatal Inhalation of tubercle bacilli when mom or another caregiver has
contagious pulmonary / laryngeal TB
Perinatal TB infection
Much more common than congenital TB More pulmonary, miliary and disseminated
disease Source case
> Mother> Father> Other household> Nursery contacts
High risk / rapid progression with HIV co-infection
TB Exposures Like all TB exposures, variables predict transmission
> Smear / cavitary status of source case> Duration of exposure > Volume of shared air / air exchange rate / pattern> Virulence of the individual strain> Cough hygiene of the source case or aerosolizing procedures
Nursery / NICU exposures> Infants with TB disease> Mother / visitor with TB disease> Health care worker with TB disease
“Young children with TB are not contagious”> Except when they are
13 cases of < 10 yr old transmitters reported before 2006;5 were < 1 yr of age and 3 were congenitally infected
9/12/2017 RANDALL CHILDREN'S HOSPITAL 25
Nursery Exposures - HCW
1974 Light Am Rev Resp Dis 109:415-419> Nurse’s aid with pulmonary TB
259 low risk infants skin tested / followed. None converted their TST 139 higher risk infants skin tested / treated with INH. None converted their TST
1976 Steiner Am Rev Resp Dis 113:267-72> Nurse’s aid with pulmonary TB
2 infants who had been in the nursery developed miliary TB 1647 infants skin tested / evaluated – all neg TST / no evidence of disease
1978 Burk South Med J 71:7-10> Nurse with pulmonary TB
514 infants evaluated – none converted their TST or developed TB disease
9/12/2017 RANDALL CHILDREN'S HOSPITAL 26
Nursery Exposures - HCW
1998 Kim Pediatric Rad 28:836-40> 5 Korean babies 2 – 3 months of age were diagnosed with culture proven TB
disease> Source was likely nursery exposure
1998 Nivin Clin Infect Dis 26:303-7> 3 of 184 “exposed” infants developed MDR-TB > Median hospital stay 5 days> Dx TB 4 - 15 months after birth> One mother also diagnosed with MDR 12 months later> ? Source - HCW or non-compliant adult patient
9/12/2017 RANDALL CHILDREN'S HOSPITAL 27

Nursery Exposures - HCW 2003 CDC MMWR 12/23/2005 1280-3
> Nurse diagnosed with TB disease 78% of coworkers had prior positive TST and none tx for LTBI
– Remaining co workers all TST negative Extensive outreach found only 36% of 600 infants and 24 % of 900 women 5 of 227 infants were TST positive (one had received BCG) 9 of 216 women converted TST (assoc with foreign birth; not contact with RN)
2008 Ohno J Infect Chemother 14:66-71> Nurse developed 3+ smear pos TB> 1 mother and 2 co-workers could have been infected > Babies received window prophylaxis and all TST neg
2011 Borgia Euro Surveill 16:pii=19984> Italian nurse diagnosed with pulmonary TB> 1 infant diagnosed with TB disease > 9% of infants had positive QFT-TB; none positive TST and no TB disease
9/12/2017 RANDALL CHILDREN'S HOSPITAL 28
Nursery Exposures – mother
2006 Berkowitz Infect Contr Hosp Epi 27:604-11> HIV infected, smear negative mom diagnosed with TB disease> Decision model developed to compare use of INH prophylaxis for
exposed infants with no prophylaxis> Risk of infection estimated at 1 in 1000 based on Light, Steiner, Burk,
Myers and Spark reports> Prophylaxis indicated if risk of infection > 2/10,000> $930,000 / death prevented for SAT> $21,000,000 / death prevented for DOPT
9/12/2017 RANDALL CHILDREN'S HOSPITAL 30
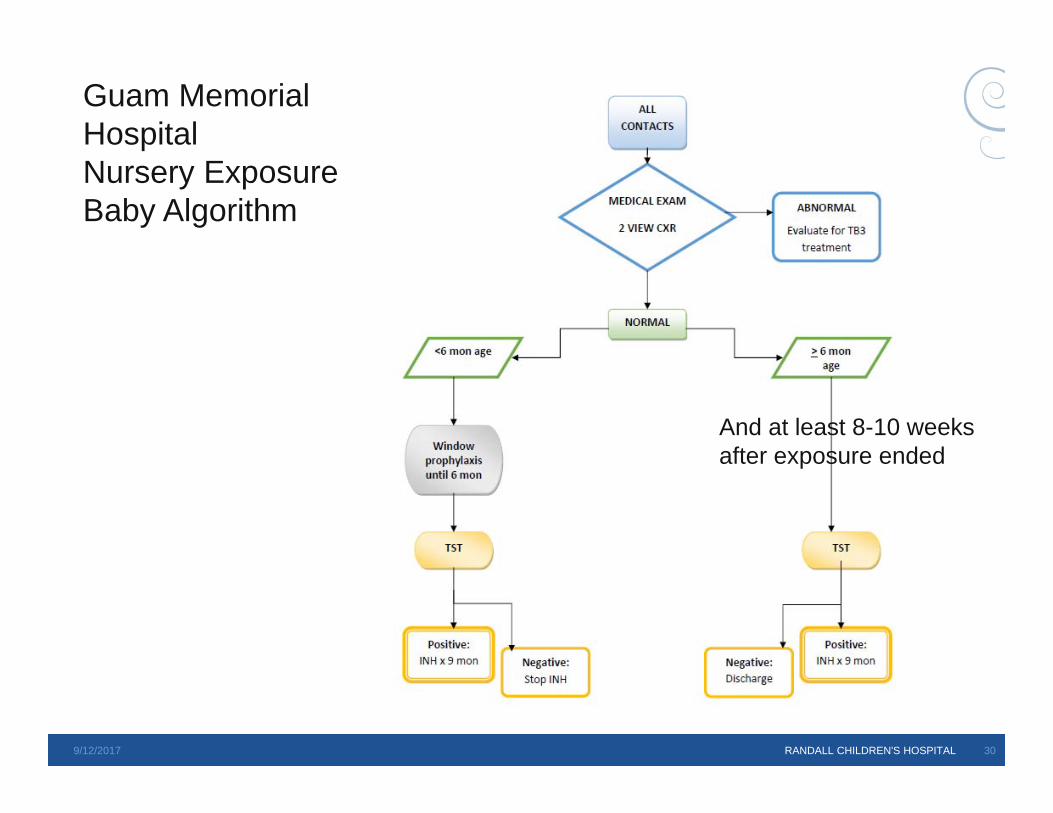
Guam Memorial HospitalNursery ExposureBaby Algorithm
And at least 8-10 weeks after exposure ended

Teaching Points Young children are more likely to develop TB disease if
infected Young children may have no symptoms or subtle symptoms Chest radiographic changes might include airspace disease
in any lobe / lymph node disease / miliary disease Young children are rarely contagious with TB It’s hard to dose children with TB medicines It’s hard to collect sputum from young children Children more often have extrapulmonary TB Their chest radiographs often worsen on therapy due to the
immune reconstitution phenomenon
Teaching Points Gastric aspirates have great yield in babies
> Gastric aspirate video and instructions – Nicholas Loefflerhttp://www.currytbcenter.ucsf.edu/pediatric_tb/resources.cfm
Consider INH prophylaxis once active disease has been ruled out (probably not necessary most of the time)
Use B6 if breastfed baby INFECTION CONTROL

Teaching Points TB has been transmitted in nurseries and NICUs from:
> Babies with congenital tuberculosis> Health care workers> Moms> Unknown source (? Other adult patients or visitors)
Contact investigation should be customized > Multidisciplinary team convened> Closest contacts and highest risk contacts prioritized> Risk of transmission assessed based on smear positivity, cavitation,
duration of symptoms, ventilation, duration of exposure, etc.> Window prophylaxis should be considered if significant risk discerned> Window prophylaxis should be continued until at least 8 – 10 weeks of age
and the child is at least 6 months of age. THEN repeat a TST, and if negative, stop the therapy.
> Watch the child monthly for signs / symptoms of TB disease or toxicity> Reinforce adherence
9/12/2017 RANDALL CHILDREN'S HOSPITAL 33

Thank you!













![Pediatric TB radiographsnid]/05a...1 Pediatric TB radiographs Ann M. Loeffler, MD Curry International Tuberculosis Center Radiology Best quality frontal and lateral views of the chest](https://static.cupdf.com/doc/110x72/609633be3922801af21c02d2/pediatric-tb-radiographs-nid05a-1-pediatric-tb-radiographs-ann-m-loeffler.jpg)
![TB Activist Toolkit - TB Basics [Facilitators Notes]](https://static.cupdf.com/doc/110x72/568c366e1a28ab02359801e7/tb-activist-toolkit-tb-basics-facilitators-notes.jpg)