Pediatric Basics The Journal of Pediatric Nutrition and Development Number 100 | Fall 2002 ® Learning from the Best: Will Wonders Never Cease? Kath Ferguson Gerber Products Company page 1 Feeding Strategies for Older Infants and Toddlers Kay Toomey, PhD Colorado Pediatric Therapy and Feeding Specialists, Inc page 2 Feeding Problems During Weaning and Beyond Erika G. Gisel, PhD, OTR, erg Montreal Children’s Hospital page 14 ®

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

PediatricBasicsThe Journal of Pediatric Nutrition and Development Number 100 | Fall 2002
®
Learning from the Best:
Will Wonders Never Cease?
Kath FergusonGerber Products Company
page 1
Feeding Strategies
for Older Infants
and Toddlers
Kay Toomey, PhDColorado Pediatric Therapyand Feeding Specialists, Inc
page 2
Feeding Problems
During Weaning and Beyond
Erika G. Gisel, PhD, OTR, ergMontreal Children’s Hospital
page 14
®

The Journal of Pediatric Nutrition and Development Number 100 | Fall 2002
1 Learning from the Best: Will Wonders Never Cease?
Your clinical experience likely confirms that there are twoperiods of great stress for parents and their children duringthe transition to table foods. Our recent experience withexperts who specialize in infants and young children withphysical and sensory disabilities broadened our perspectiveon infant feeding by offering bits of wisdom that parents of all children could benefit from.
2 Feeding Strategies for Older Infants and Toddlers Putting Research into Practice / 7
It’s important for parents to establish a feeding plan earlyon that will help their older infant and toddler master theincremental skills needed to transition from pureed babyfoods to textured table foods. Educating parents about thecomplexity of the learning to eat process empowers themand helps them realize that there are things they can do tomake the feeding experience go better for both their childand themselves.
14 Feeding Problems During Weaning and Beyond Putting Research into Practice / 19
Children with eating impairments that involve oral-motorskills (dysphagia) are at risk of life-long feeding problems.They are typically children born prematurely, with failure-to-thrive, genetic syndromes, oral apraxias, encephalopathies,traumatic brain injury or developmental delay. Recognitionof the symptoms and classification of the nature of theproblem will allow the pediatrician to take the necessarysteps to ensure that the family receives the care and follow-up needed.
Kath Ferguson
Vice President of Product Development and Nutritional SciencesGerber Products Company
Erika G. Gisel, PhD, OTR, erg
Professor, School of Physical & OccupationalTherapy, McGill UniversityDirector, Swallowing and Dysphagia Clinic,Montreal Children’s HospitalMontreal, Quebec
Gerber Products CompanyRegional Medical Marketing Representatives
East: Patti Branch 703-222-3827Central: Pat Sheehan 913-829-8774West: Noreen Wintergalen 602-224-9194
Professional Information Line: 1-800-595-0324Professional E-mail Address: [email protected] Address: http://www.gerber.com
Pediatric Basics® (ISSN #1096-1038) is publishedfour times a year as a service to pediatric profes-sionals by the Medical Marketing Department,Gerber Products Company, 200 Kimball Drive,Parsippany, NJ 07054-0622
Editorial Offices: Folio One Communications, 820 Monroe NW, Grand Rapids, MI 49503
© 2002 Gerber Products Company. All rightsreserved. Reproductions without special permissionare prohibited. Pediatric Basics® is a registered trademark of the Gerber Products Company.
Kay Toomey, PhD
DirectorColorado Pediatric Therapy and FeedingSpecialists, IncDenver, Colorado
PediatricBasics®

Learn
ing fro
m th
e B
est: W
ill Wonders N
eve
r Cease
?Kath FergusonVice President of Product Development and Nutritional SciencesGerber Products Company
Learning from the BestWill Wonders Never Cease?
For 75 years, Gerber has been the industry leader in infantfood and feeding, relying on scientific research, theexpertise of our own nutrition and food science teams, aswell as national and international experts in infant nutritionand feeding. Continuous feedback from moms “in thefield” through consumer testing, focus groups and our800 number has allowed us to develop a wide variety ofproducts that are “baby tested, mom approved.” Our aimhas always been to make the feeding experience enjoyablefor both baby and caregiver by matching our productsto the developmental capabilities and needs of thenormally developing child, who moves through the tradi-tional developmental milestones in an orderly progression.
Another Set of EyesRecently, we had an opportunity to tap into the wisdom offeeding experts who specialize in infants and young chil-dren with physical and sensory disabilities. This enlight-ening experience seemed to open a window and broadenour perspective on infant feeding by offering bits ofwisdom that parents of all children could benefit from.
For example, we learned that eating is not instinctual afterthe early months of infancy, as many people often believe.Children must learn feeding skills during an educationprocess that occurs over many months of practice, trialand error. While parents do play a key role in helping theirchildren learn those skills, the learning and teaching isreciprocal between parent and child. Together they navi-gate the transition from an all-milk diet to one that includesa variety of healthy foods.
We also confirmed some core beliefs, like how babies havean amazing way of finding solutions to solve their ownproblems. They suck their thumbs to calm themselves.They will place their finger or fist in their mouth to promotesucking. They know when they have had enough to eat.We all need to pay attention to the lessons that these tinyteachers have to offer.
Our conversations also confirmed that sensory stimulationis critical to an infant’s normal growth and development.Sensory stimulation covers a lot of areas, from texturedtoys, to the colors in the playpen, to the foods offered at
mealtimes — their flavor notes (bitter, sour, sweet), color,temperature, and texture. Free exploration during feedingfacilitates sensory learning.
Through our years ofexperience we havelearned that if parents canoffer the right foods at theright time, i.e., when theirbabies are ready to learnnew feeding skills, theprocess is much easier,less stressful, and morefun and enjoyable for allconcerned. The food is atool that the infant can useto learn and practice newskills on, if the food’s size,shape and texture meetthe infant’s developmentalabilities.
A Message for All ParentsAs pediatric professionals, your clinical experience likelyconfirms that the two periods of greatest stress for parentsand their children during the transition to table foods areinitially, when a child first learns to eat cereal from a spoon,and later, when a child makes the transition from purees tofoods with particulates. While it is true most normallydeveloping children eventually master their feeding difficul-ties, the wait-and-see approach provides little comfort tofrustrated parents in the throes of daily mealtime battles.This issue of Pediatric Basics features articles by infantfeeding specialists Kay Toomey, Ph.D. and Erika Gisel,Ph.D., who offer an in-depth look at how older infants and toddlers learn to eat and practical suggestions forparents struggling with difficult and problem feeders.
At Gerber, we believe that learning to eat should be anatural, stress-free progression for families with youngchildren. With the right foods, at the right time, it can be a pleasant and fun experience too. �
Number 100 | Fall 2002 1PediatricBasics®
®

One of the common myths about eating is that it is easy andinstinctive. Eating is actually the most complex physicaltask humans engage in. It is the only physical task that
utilizes all of the body’s organ systems: the brain and cranial nerves;the heart and vascular system; the respiratory, endocrine and meta-bolic systems; all the muscles of the body and the entire gastroin-testinal tract. Just swallowing, for example, requires the coordinationof 26 muscles and six cranial nerves.1 Eating is also the only taskwhich children do that requires the simultaneous coordination of allof the sensory systems. The ability to manage this physical coordi-nation begins instinctively, but only for the first month of life. Fromthe end of the first month to the end of the fifth or sixth month oflife, the primitive motor reflexes (rooting, sucking, swallowing) takeover as the older infant lays down pathways in the brain for the volun-tary motor and sensory control over eating. After the fifth or sixthmonth of life, eating is actually a learned behavior.
Because eating involves the interplay of so many body systems andactivities, it is important for parents to establish a feeding plan earlyon that will help their older infant and toddler master the incre-mental skills needed to transition from pureed baby foods to texturedtable foods. The skills that need to be achieved for successful eatinginclude: 1) postural stability, which is affected by the type of chairsupporting the growing infant; 2) oral-motor skills, which need toprogress from a sucking movement for purees to the side-to-sidetongue movements needed for eating table foods; 3) jaw skills, whichprogress from a suck, to a munch, to a rotary chewing motion so that
Kay Toomey, PhDDirectorColorado Pediatric Therapy and Feeding Specialists, IncDenver, Colorado
Feeding Strategies for Older Infants and Toddlers
2
Synopsis — Eating is the most complex physical task humans engage in. It is the only physical taskthat utilizes all of the body’s organ systems, which is why it is important for parents to establish afeeding plan early on that will help their older infant and toddler master the incremental skillsneeded to transition from pureed baby foods to textured table foods. The skills needed forsuccessful feeding include: postural stability, oral-motor skills, jaw skills, sensory skills, hand-to-mouth skills, and parenting skills.
Parental stress around feeding can be greatly alleviated through guidance by a pediatric practitionerwho can educate them about the complexity of the learning to eat process. This education empowersparents and helps them realize that there are things they can do to make the feeding experience gobetter for both their child and themselves.

foods with textures can be prop-erly broken apart; 4) sensory skills,which allow the older infant andtoddler to tolerate the “feel” offoods in their mouth, to learn tolike the taste of table foods, andto track where the food is in themouth at any given time; 5) hand-to-mouth skills, which allow thechild to learn to self feed; and 6) parenting skills,which encourage the infant to enjoy a variety offoods and the feeding experience throughout theformative years.
Postural StabilityAs with the younger infant just learning to eat babycereal, the ability to sit upright independently is crit-ical for transitioning on to more difficult-to-managefoods. Once a child is able to sit independentlywithout falling over for approximately 10 minutes, it’s time to make the transition from an infant feedingseat to a standard high chair. This usually takes placesomewhere between 8-9 months of age for mostchildren. Today’s new high chairs frequently havegood side and front supports, often with a saddle barin the center to prevent the older infant from slidingforward out of the chair. If the family does not havethis type of high chair, a non-skid mat under the rearend and a foam insert called a “High Chair Helper”can provide the same level of support and securesitting.
As the older infant grows into a toddler, parents willnotice their child’s increased interest in sitting at thetable with the rest of the family, usually around 18months of age. Since this is also an age when childrenbecome very interested in imitating others, it is impor-tant to have meals at a family table where the childcan closely watch the family eating.2 While keepingtoddlers in high chairs may keep them contained(somewhat), it also perpetuates physical separationfrom the family and doesn’t allow them to see well
enough to learn by imitation.Ideally, the family will use aheight-adjustable high-chairwhich can be pushed up to the family table with the trayremoved. This will allow theinquisitive and active toddler to remain in a stable seat, whilestill joining the family.
If the high chair is not adjustable, a booster seat, withvery high side arms and a stable back, should be used.The booster seat will need to be securely attached tothe front edge of the adult chair so that the toddler’slegs are in a 90 degree position with the feet supportedby a foot rest. Sliding a booster seat to the back of anadult’s chair will cause the child’s legs to stick outunder the table at an odd angle, and does not permitstable seating. The lack of a stable seating arrangementis the most common clinical reason for toddlers torepeatedly get in and out of their chairs during meals.Running away from the table during meals does notsupport good eating habits.
Oral-motor SkillsThe oral-motor skills needed for transitioning to fingerfoods and table foods are different from those used forbreast/bottle feeding and spoon-feeding. Breast/bottlefeeding predominantly involves forward/backwardtongue movements. Spoon-feeding skills develop overtime from a normal tongue thrust to tongue “waves”that transfer foods from front to back of the mouth,after about a month of practicing with the spoon.Between 7-9 months, the infant learns to cup thetongue for the spoon, and close their lips around thespoon to help draw the food into the mouth.1
In order to eventually manage the transition to tablefoods, the older infant/toddler needs to learn how tomove the tongue to the sides of the mouth and placea bite of food onto the molar area of the gums. Thismovement pattern, known as a lateral tongue move-
Feedin
g S
trate
gie
s for O
lder In
fants a
nd To
ddle
rsAs with the younger infant just learning to eat baby cereal, theability to sit upright independently is critical for transitioningon to more difficult-to-manage foods.
®
PediatricBasics® Number 100 | Fall 2002 3
continued on page 5

Even the typically developing childcan become a picky eater whenallowed to food jag. This is becauseif children are only exposed to thesame few foods every day, they do not learn how to manage thecomplex sensory informationneeded to eat difficult foods, suchas raw vegetables, hard-to-chewmeats, or wet/slippery fruits. Theinfant who once ate all types offruits and vegetables as a pureedbaby food doesn’t learn how toeat the table food versions. Or, the toddler who has becomeneophobic of every green food isno longer given the sensory prac-tice of eating peas because thechild is tantruming.
The key here is to back down thesensory progression of learningabout foods on the “Steps to EatingHierarchy” to a level the toddlercan tolerate. This means that atoddler may need to back downfrom actually eating peas to justsquishing them for a while tobecome reacquainted with theirsensory qualities. Gradually, theparent can move their child backup the sensory steps towards eating.
To move a child up the sensoryhierarchy, the parent needs tocreate “play with a purpose”, withthe purpose being to move thechild up to the next sensory step inthe progression. For example, foran older infant or toddler who doesnot want to even look at the food,making it wiggle in front of themcan often times attract their atten-tion. Pretending the food is ananimal coming to talk to them isalso engaging. Stirring, pouring anddumping from a spoon are all good(and fun) ways to encourage a childto interact with food. Having anolder child help with food prepara-tion is also an excellent way tomove up to interacting with thefoods while achieving the smell
step of the hierarchy. Breaking,pulling, waving and crushing thefoods are all excellent strategies forteaching a child about how thefood will move once it is in theirmouth, as well as moving them upto the touch step of the hierarchy.Blowing “rockets” into a cup – orbetter yet into the trash – is theeasiest way to get children to taste a food they otherwise would not gonear. Remember, playing with thefood is not the end goal of thisprocess. These are merely moremanageable steps along the way to actually eating the food.
Parents can prevent food jags inthe first place by changing somephysical property about thepreferred food EVERY time it ispresented. This means that thesize, shape, color, texture,temperature or taste will need to be different each time the childis given their food jag food. Forexample, for the child who will onlyeat macaroni and cheese from ablue box, begin by putting the rawingredients in a plain, sealed plasticbag or bowl first. Next, offer thechild the preferred noodle shapewith the pieces cut in half, thenchange to a different shapednoodle for several exposures.
By this time the child should be ableto tolerate the different flavor of themacaroni and cheese created byadding Parmasean cheese to themix. Finally, parents can change thecolor of the macaroni and cheesemixture by adding a small amountof food coloring.
Many parents and professionalstreat food jags as a normal toddlerbehavior that can be tolerated.While the appearance of the patternmay be normal, maintaining it is notand will only serve to limit a child’sexposure to a variety of other foods,reinforcing the child’s preferencefor a very limited number of foods.
Preventing and Treating “Food Jags”
4
If children are only exposedto the same few foods everyday, they do not learn how tomanage the complex sensoryinformation needed to eatdifficult foods, such as rawvegetables, hard-to-chewmeats, or wet/slippery fruits.
Steps to Eating Hierarchy*
1. Visually tolerating the food
2. Interacting with the foodwithout actually touching it(vestibular; kinesthetic andproprioceptive systems)
3. Smelling
4. Touching
5. Tasting and then, finally
6. Eating
* In order of most basic to most difficult.

ment, is critical for successfullytransitioning from baby foodpurees to table foods. Acontrolled “lateral tongue move-ment pattern” is learned in devel-opmental stages that begin withlearning to tolerate the feel of along hard object in the mouth.The mouthing of teething toysand other developmentally appro-priate objects of different textureshelps infants and toddlers learnto manage the feeling of objectsin their mouth and teaches themhow to move their tongue fromside to side. Initially, the handshelp move the foods around in the mouth. Over timeand with practice, the “lateral tongue reflex” comesunder voluntary control and food is moved aroundwithout as much assistance from the hands.3 Typically,this skill develops around 8-9 months of age. Olderinfants who have mastered lateral tongue movementsare ready to try age-appropriate finger foods.
It is important to recognize that, in order to correctlymanage textured table food from an oral-motor stand-point, lateral tongue movements must be learned first.When older infants are given pureed baby foods thathave chunks of other foods in them before they learnhow to lateralize their tongue, the chunk of food maybecome stuck on the top of the tongue and cause thechild to gag. (You can find out just how uncomfort-able this feels, as well as come to a better under-standing of the oral mechanics of eating texturedfoods, by conducting the experiment on page 6.)Infants and toddlers who frequently gag on food learnthat eating is not a pleasant experience and, conse-quently, may avoid textured foods or avoid foodaltogether.
The oral-motor skills necessary for cup drinking arealso quite different from those used with breast andbottle feeding. Most importantly, the older infantneeds to learn how to hold a small amount of fluid inthe mouth, and to pull it into a ball (or bolus) forswallowing.3 Cups with no-spill valves perpetuate abottle/breast drinking oral pattern in which the fluidis sucked back using negative pressure with the tongueflat held underneath a spout (or nipple) and do not
support the development of themore mature drinking skills. Anopen cup or sipper cup withouta no-spill valve is a more appro-priate first cup choice. Ideally,the cup would have two handlesand a recessed lid so the olderinfant can easily hold andmanipulate the cup, as well as avoid compressing the noseagainst the lid.
Jaw SkillsAs previously noted, breast/bottle-fed infants primarily usetheir tongue for feeding. While
there is some jaw movement involved in both earlyfluid feeding (compression movements) and spoonfeeding (open and close), the role of the jaw andchewing is small compared to that of the tongue.1
Between 9 and 10 months of age, the jaw becomesvery active in eating as the child learns to break foodapart by moving the jaw up and down with pressureon the food. An up and down jaw movement isreferred to as a “munch.”3
Rotary chewing emerges between 12 and 14 monthsof age as the toddler encounters more chewy texturedfoods.1 Appropriately sized and shaped, soft tablefoods can be introduced once a child adds a smallgrind with the teeth on the food, along with a smallside-to-side motion of the jaw (rotary chew).
Sensory SkillsEating requires the simultaneous integration of alleight of our sensory systems. These senses include thefive which are well known: seeing, hearing, tasting,touching and smelling, as well as the lesser-knownsenses of balance, awareness of body in space andinformation received from one’s joints. The latterthree sensory systems are known as the vestibular,kinesthetic and proprioceptive systems respectively.Once an infant is sitting independently, these threesensory systems start to play a very large role infeeding.
Another one of the myths about feeding is that eatingis our body’s first priority, when actually it is only thethird. Breathing is the body’s number one priority and
Feedin
g S
trate
gie
s for O
lder In
fants a
nd To
ddle
rsBetween 9 and 10 months of age, the jaw becomes veryactive in eating as the child learns to break food apart bymoving the jaw up and down with pressure on the food.
®
PediatricBasics® Number 100 | Fall 2002 5
Older infants who have mastered lateraltongue movements are ready to try age-appropriate finger foods.
continued from page 3

balance is the second. As such, the vestibular/balancesystem becomes very important when the infant is nolonger held by an adult who is providing balance. Inaddition, every time humans move their heads, thefluid in our inner ear shifts and the vestibular systemmust readjust our sense of balance. In order to spoonfeed, the older infant needs to come to midline andopen their mouth; a task which shifts the head in spaceand requires an adjustment in balance. Chewing tablefoods is an even more difficult task as humans do notnaturally chew with their heads perfectly still. Youngtoddlers especially move their head with every chewingmotion, and therefore have to readjust their sense ofbalance with each munch or chew that they make.
With regard to kinesthesia, drinking from a nippledoes not require much body awareness since thenipple fills up much of the mouth. A puree coats theinside of the mouth and is not difficult to locate froma body awareness standpoint either. However, a smallpiece of table food can be easily lost in the mouth ifthere is not good body awareness. Older infants andtoddlers need to be able to track each piece of food in their mouth so they do not accidentally bite theirtongue or cheek instead of the food. In addition, thefood must be followed inside the mouth to know that
it has been placed correctlyonto the molars, and where it is located when it is time to swallow. You have experi-enced a kinesthetic awarenessproblem if you have evereaten popcorn and ended upwith a popcorn shell stuck inthe back of your throat. Yoursensory system lost track ofthe location of that shell andit ended up in a place it didnot belong.
During feeding, informationreceived from the jaw joint viathe proprioceptive system isalso different depending onwhether the infant is drinkinga fluid, sucking back a puree,or chewing table foods.Remember, drinking is
actually more of a tongue than a jaw movement, andspoon-feeding requires primarily an open/closemotion of the mouth. Chewing, however, is quitecomplex and gives a large amount of shifting infor-mation as a food is broken apart for a swallow.(Think about how different the cracker you chewedin the above experiment felt from the first chew tothe last and what kind of jaw pressure differencesyou registered).
Another very important developmental sensory eventthat occurs during this time is the change in functionof a toddler’s taste buds.4,5 Prior to this age, the tastebuds on the back of the tongue, soft palate, uvula andback of the throat were primarily used. Shortly after achild’s first birthday, the taste buds on the front of thetongue become predominant and the others decreasein function and/or disappear. As such, the toddlerbegins to reject baby foods because the taste is nolonger preferred. The toddler also becomes resistantto being spoon fed at this age because changes incognitive and emotional development inspire them totest their independence.6,7
In order to eat textured table foods then, the toddlerneeds to be able to simultaneously integrate informa-tion from all 8 of his sensory systems with every singlechewing motion; the sight of the food changes as it ischewed, how it feels changes, what it sounds like inthe mouth changes, the taste and the smell actuallychange, and adjustments need to be made in balance,location of the food, and pressure being exerted. Diffi-culties with the sensory system is the most commonclinical reason for children not being able to transi-tion from baby food purees to textured table foods.
continued on page 8
Another one of the myths about feeding is that eating is ourbody’s first priority, when actually it is only the third. Breathing is the body’s number one priority and balance is the second.
6
Do Try This at Home
Take a large bite of a soda-type cracker. Chew thecracker 4-5 times, then place the pieces onto the centerof your tongue. Now, attempt to swallow the chewedcracker from here — without lifting your tongue intoyour palate. This should be difficult and uncomfortable.
Next, close your eyes and take another bite of thecracker. As you chew and swallow normally, visualizehow and where you move the cracker in your mouth,where you chew it, and from where you swallow it. All ofthese skills must be in place for eating table foods well.
Eating requires the simultaneousintegration of all eight of oursensory systems.

Feedin
g S
trate
gie
s for O
lder In
fants a
nd To
ddle
rs
®
Number 100 | Fall 2002 7PediatricBasics®
“Nobody knows the trouble I’m in…”might be the perfect lament of chil-dren with feeding disorders. Theyoften struggle along on minimalchoices from each food group. Theyaggravate their parents at every bite;while equally frustrated pediatricianstry to reassure parents that “at leastyour child is growing along a normalcurve.” No one may suspect thechild is in the early stages of abonafide feeding disorder, andfewer people know how to identifyand correct them.
This occurs because our basictraining is excellent in the areas ofgeneral nutrition, gross and finemotor development, electrolytebalance, and the recognition ofvarious deficiency states, but isoften inadequate in understandingthe natural process of learning toeat. Eating is first and foremostexperiential, ultimately requiring theintegration of a child’s sensory,gross, fine and oral-motor capaci-ties. The accompanying article byDr. Kay Toomey, details this elegantjourney of learned behavior. Sheprovides the “rest of the story” theydidn’t tell us in medical school.
It’s easy to appreciate the interde-pendency of these processes whenfaced with a disorganized preemie ora child who, for whatever reason,has been fed by a G-tube from anearly age. They have to learn orrelearn the process, and it is no easytask. At a more subtle level, thesame impediments to learning aretaking place with our problem eaters.
All of us can recognize a child withpoor weight gain, ongoing choking,gasping, coughing and vomiting, andthe child that arches and cries ateach meal. These symptoms promptearly and intense work ups, andusually demonstrate a suspectedmetabolic disorder, mechanical swal-lowing difficulty, or GE reflux.
But what about the otherwise normalchild who, due to a combination ofphysical and/or behavioral issues,won’t eat, or will only eat a fewfoods? To the right are some redflags suggesting early signs of anemerging feeding disorder. The usualcause of each problem follows inparenthesis.
Simple and Effective Office InterventionsMany feeding difficulties can beprevented or treated with a littleguidance from you early on. Forexample:
Rethink your feeding recommenda-tions along developmental ratherthan nutritional lines. Success withthe early feeding of solids is bestattained when a child has learned tosit alone. Early on, an infant or swingseat works well. Later, a high chairwith a t-strap fastener (or a non-skidpad) and adequate back support isbest.
Suggest to parents that initially foodshould be explored by the sensesrather than eaten.
Encourage parents to demonstratehow to eat and explore new foodsbecause babies learn best throughimitation. Along those lines, encourageparents to smile when their babygrimaces at a new taste — notimitate their baby’s frown.
Remind parents that it may take 10-20 exposures before a child acquiresa taste for a new food. Don’t give uptoo early.
Instruct parents that the spoonshould just touch their child’s lips.The child should be allowed toexplore and taste the food, ulti-mately taking the spoon into themouth by his own initiative.
Look carefully for signs of sensoryproblems, such as finger splaying,grimacing, extending legs, andclosing their eyes during feeding.
Aversion to loud noises, motion sick-ness, avoiding climbing stairs, orlack of interest in exploring anythingwith the mouth can also be signs ofsensory problems.
Refer a picky eater — sooner ratherthan later — to a feeding specialistwith OT/ST support, so that the oral-motor sensory dynamics can be fullyevaluated and effectively treated.
In summary, don’t be content withthe picky eater who consumes a few items from each food group, yet continues to grow at a normalvelocity on the curve. There isusually an underlying correctablereason that is worth pursuing.Persistence in your investigationand/or referral can make a world ofdifference early on in the lives ofyour patients and their families. �
Putting Research Into Practice with Michael Frank, MD, FAAP
Dr. Michael Frank is a pediatrician inprivate practice in Denver specializing in feeding disorders and ADHD; clinicalinstructor for The University ofColorado HealthScience Center, andMedical Director ofthe Colorado Pedi-atric Therapy andFeeding Specialists,Inc.
Early Signs of a Feeding Disorder
1. Inability to transition to baby foodpurees by 10 months (oral-motor/sensory)
2. Inability to accept table foods by 12 months. (oral-motor/sensory)
3. Inability to transition from breast/bottleby 16 months. (lack of proper exposure/oral motor)
4. Inability to wean off baby foods by 16 months. (oral-motor/sensory)
5. Avoidance of foods of specific texturesor food groups. (sensory)
6. Parents report that the child is difficultfor anyone to feed and meals are abattle zone. (any combination of theabove)

Hand-to-Mouth SkillsFinger feeding builds on the earlier skills of reachingfor and transferring of objects hand-to-hand acquiredbetween four and six months of age. By six months,children have developed a palmar grasp which allowsthem to rake an object into their palm and hold it upto their mouths. Oral exploration of larger toys andobjects really accelerates at this point. Oral and touchexploration of many different types of textures is crit-ical during this time for developing finger feedingskills and interest. Around eight to nine months ofage, children gain the ability to pick up small objectsusing their thumb opposed to their second and thirdfingers (radial-digital grasp). This allows them tobegin to hold on and more efficiently get a hard
munchable texture to their mouth for the oral explo-ration of food tastes. One end of a stick-shaped, hardfood can be held in one hand while exploring theother end with the mouth. This teaches the tonguehow to begin to lateralize by moving the food aroundthe mouth with the hand, since the hand is morecoordinated than the tongue at this point. When thepincer grasp develops between 10-12 months, the childis able to pick up a small cube of food and place it inthe mouth.
While finger feeding should become noticeably effi-cient around 14-16 months, utensil use does notbecome efficient until after 24 months and should notbe the primary way of self-feeding until after the ageof 3 years. The best toddler utensil is one that is shortin length (not the long infant feeding spoon), with an enlarged handle covered in a textured surface.This type of utensil is ideally suited to allow for thetoddler’s wider and less proficient grasp pattern. Ametal spoon bowl and metal blunted fork tines arepreferred by the toddler to assist with poking thefoods and because the rubber tipped infant feedingspoon has usually become a non-preferred item.The metal makes the toddler utensils differentfrom the infant spoons and allows them to be morelike the others in their family using “grown up”utensils. A heavy or weighted spoon is ideal as theslightly increased weight helps the toddler with theirfine motor control.
The Parents’ RoleThe most important tasks for parents teaching theirolder infants and children how to eat are: focusing onthe mechanics of the task; choosing developmentallyappropriate foods; and making the experience enjoy-able. Pleasant, fun mealtimes help establish a life-long,healthy relationship with food.
In order for parents to teach their children to be goodeaters, they need to become aware of the messagesthat they may be sending their child about food and/or about their own food preferences. If a parent isconcerned that their older infant or toddler may notbe able to handle a particular food and then looksworried about it, the child will get the message thatthe food is not safe and should be rejected.
Difficulties with the sensory system is the most commonclinical reason for children not being able to transition frombaby food purees to textured table foods.
continued from page 6
8
continued on page 10

Feedin
g S
trate
gie
s for O
lder In
fants a
nd To
ddle
rsThe overall goal of all treatment with children whowon’t eat is to create a situation that positivelyreinforces normal, healthy eating patterns.
®
When children won’t eat, parents and professionals areoften tempted to classify them in one of two categories:those who have “organic” or “physical” problems andthose who have “behavioral” problems. These kinds oflabels are not particularly helpful. First, because there isan implication of blame in this system, which is neithervery accurate nor useful when trying to help childrenwith feeding problems. Second, children with physicaldifficulties often develop behavioral problems after theirattempts to eat don’t go well, and children with behav-ioral eating difficulties develop physical disorders afterhaving poor nutrition for a period of time. So, there isn’ta clear-cut distinction between the two.
Rather than force children into categories where theydon’t belong, we need to think about children who won’teat as having had poor learning experiences with food. In other words, just as children learn to eat, they can alsobe taught not to eat by the circumstances in their lives.
Research shows that learning about food occurs in twomain ways. The first is when a connection is madebetween one stimulus (a natural event, behavior, orobject) and a second neutral stimulus. For example, we know that feeling sick to your stomach causes thephysical reaction of appetite suppression. If feelingnauseous (a natural event) is consistently paired with aspecific food (previously a neutral thing), eventually thefood itself will cause nausea. Another example would bewhen pain is paired over time with food, as occurs withGastroesophageal reflux (GER). When that happens aperson learns to avoid or escape from situations thatinvolve eating.
The second way that we learn is through reinforcementand punishment. Eating followed by praise or imitation(positive reinforcement) leads to more eating. Similarly,refusing food followed by lots of attention/interaction
(also positive reinforcement)leads to more food refusal.So, in addition to increasingdesired behaviors, positivereinforcement can causemore of an undesired
behavior as well.
Punishmentaround food
is also verypowerful. Boothshowed that ifthe learning
about food is unpleasant, our bodies turn off ourappetites. Weingarten and Martin showed that if nega-tive connections are made to the cues of eating (e.g.,sitting down at the table, the utensils used, the peoplepresent, the room where meals are eaten), a child learnsto avoid the feeding situation completely.
The overall goal of all treatment with children who won’teat is to create a situation that positively reinforcesnormal, healthy eating patterns through:
Structure — Have a routine to mealtimes, eating inthe same room, at the same table, with the sameutensils, which capitalizes on the need for repetitionin learning.
Social modeling — Allow children to learn throughthe observation of good mealtime role models.Parents who are poor or picky eaters will have adifficult time helping their children.
Positive reinforcement — Meals need to bepleasant and enjoyable, and any interaction withfood should be rewarded. Verbal praise, a smile, a touch, a cheer, and hand clapping are all greatoptions.
Manageable foods — Foods need to be preparedin small, easily chewable bites, or in long, thin stripsthat a child can easily hold.
Learning about “the physics” of food — The mouthand teeth will need to use hard pressure to breakapart a carrot stick. Wiggly, squishy string cheese ischewy in the mouth. Yogurt, which is cold, wet andsmooth, can just be sucked down.
When parents understand that eating is a learnedbehavior, in which there is an interplay between theirchild’s physical capabilities and his experiences withfood, they can take on a positive teaching role with their children rather than a negative/forcing or no-limitsapproach to feeding. It clarifies for parents that there are things they can do to make the feeding situationbetter, and gives them hope. The approach also teachesparents, and reminds us professionals, that there arethings we can do that may make the situation worseand reminds us how to avoid the pitfalls of working with children who won’t eat.
Booth D: Learned role of tastes in eating motivation. In: Taste, Experienceand Feeding, E Capaldi and T Powley (eds), pgs 179-95. American Psycho-logical Association, Washington DC, 1990.
Weingarten HP, Martin GM: Mechanisms of conditioned meal initiation.Physiol Behav 45:735-40, 1989.
Understanding Why Children Won’t Eat and How to HelpKay Toomey, Ph.D.
Number 100 | Fall 2002 9

If the parent is concerned at all about their child’sphysical capability of managing a food, they shouldinstead “show and tell” the child how to eat the food.This means literally talking their older infant andtoddler through the process of biting and chewing, as well as showing the child in an over-exaggeratedfashion exactly how to move the food around in themouth. For example, a parent would want to explainin very simple language how they manage a bite of acracker by saying, “I’m going to bite with my frontteeth and move it back to my strong back teeth withmy tongue. Then I am going to chew, chew, chew.”The language needs to be paired with a large bitingmotion, with an open mouth to show how the tonguemoves and then with an up and down head movementto emphasize the chewing motion. Recall that chil-dren in this age range learn best by watching othersengage in an action. As such, parents need to be goodrole models for their infants and toddlers. This appliesnot only to role modeling the mechanics of eating,but also our food choices. If a parent makes a faceand complains that they don’t like broccoli, it isdoubtful that their child will eat this food either.Recent research suggests that the likes and dislikes ofparents play a large role in whether or not their chil-dren learn to eat fruits and vegetables throughouttheir lives.8
Parents also need to remember that it may take anaverage of ten exposures to a new food, paired withpositive reinforcement, before a child will consistently
accept the food.9-11 If a child appears to dislike a food,the parent should maintain their cheerful face, reas-sure the child that they are “okay” using a positivevoice and then model taking another bite themselves.If the reaction is very large again, the parent cancontinue to reassure and praise the child for takingthe bite, but move on to a different food. The ques-tionable food then needs to be tried again on adifferent day.
The flip side of needing to try new foods several timesbefore prior to acceptance is not permitting a child tochoose to eat the same food over and over again tothe exclusion of any other foods. Known as a “foodjag”, this behavior is especially prevalent in oldertoddlers and thought to be related to their discomfortwith new foods, or neophobia.2,7 Food jagging is alsobelieved to be a typical toddler feeding pattern and,therefore, is not viewed as a problem. However, achild allowed his food jags, eventually “burns out” ona particular food and refuse to eat it again, even aftera month or more hiatus in children with feeding diffi-culties. As a result, the child loses more and morefoods out of their food repertoire as they jag and burnout on each successive food, until there may be only 5-10 foods that he will eat. This child then needsprofessional help in order to assure a nutritionallyadequate diet. For the typically developing child, abreak from the food for about two weeks seems to besufficient to allow the child to become willing to eatthe food again.
Parents need to be good role models for their infantsand toddlers. This applies not only to role modelingthe mechanics of eating, but also our food choices.
Picky Eaters Versus Problem Feeders
Picky Eaters Problem Feeders
Decreased range or variety of foods. Restricted range or variety of foods, Will eat 30 different foods or more. usually less than 20 different foods.
Foods lost due to “burn out” because of a food Foods lost due to food jags are NOT jag are usually re-gained after a 2 week break. re-acquired.
Able to tolerate new foods on plate and usually Cries and “falls apart” when can touch or taste a new food (even if reluctantly). presented with new foods.
Eats at least one food from most all food Refuses entire categories of texture groups. food textures.
Will add new foods to repetoire in 15-25 steps Adds new foods in more than on Steps to Eating Hierarchy. 25 steps.
continued from page 8
10

Lastly, parents should not forget that their olderinfant, and especially toddler, is becoming more inter-ested in exploring the world than in eating. If mealsand foods are not made fun and an extension ofthe child’s exploration of the world, there will belittle incentive to come to the table to eat. Parentsshould feel free to get creative with the food — usingcookie cutters to make different shapes in the foodand natural food colorings to create foods that lookinteresting to eat. Describing the physical propertiesof the foods (texture, temperature, consistency,pliability) facilitates exploration by teaching chil-dren the “physics of food” and helps them under-stand how the food will feel, break apart and move intheir mouths. Allowing the older infant and toddler toget messy and “play” with their food, will be especiallyhelpful for gaining and maintaining interest in food.
Play centered on food needs to be “play-with-a-purpose”; play which teaches the child something newabout the food. This type of play is different than playthat happens when a child is done eating. Play-with-a-purpose allows the older infant and toddler to explorefood as one more exciting and fun part of their world,as well as teach them how to manage food once itgets into their mouths. Hopefully while using thesestrategies, parents will re-discover an enjoyment ineating for themselves, which they can then impart totheir children.
ConclusionWhen parents of typically developing children in pedi-atric practices are polled, up to 33% of them indicatethat they have problems getting their infant or toddlerto eat.12,13 Parental stress around feeding can be greatlyalleviated through guidance by a pediatric practitionerwho can educate parents about the complexity of theprocess of learning to eat. This education empowersparents and helps them realize that there are thingsthey can do which will make the feeding experiencego better for their child and themselves. This guidancecan also give them hope that their child will have afuture healthy relationship with food. �
Dr. Kay Toomey is a Pediatric Psychologist specializing in theassessment and treatment of children with feeding difficulties.She has been working with children who won’t eat for overten years. Dr. Toomey co-founded the Oral Feeding Clinicat The Children’s Hospital in Denver in 1990, and acted asDirector of the Rose Medical Center’s Pediatric FeedingCenter from 1995 to 2001. Currently, Dr. Toomey is in privatepractice as the Director of the Colorado Pediatric Therapy &Feeding Specialists, Inc. She lectures nation-wide regardingher feeding treatment program, the SOS Approach ToFeeding.
References1 Glass R, Wolf L: Feeding and Swallowing Disorders In Infancy. Therapy
Skill Builders, Tuscon, AZ, 1992.
2 Rozin P: Sociocultural influences on human food selection. In: Why we eatwhat we eat: The psychology of eating. E Capaldi (ed.), (pp. 233-63).American Psychological Association, Washington DC, 1996.
3 Morris SE, Klein MD: Pre-Feeding Skills. Therapy Skill Builders, Tucson,AZ, 1987.
4 Mennella JA, Beauchamp GK: The early development of human flavorpreferences. In: Why we eat what we eat: The psychology of eating. ECapaldi (ed.), (pp. 83-112). American Psychological Association, Wash-ington DC, 1996.
5 Duffy VB, Bartoshuk LM: Sensory factors in feeding. In: Why we eat whatwe eat: The psychology of eating. E Capaldi (ed.), (pp. 145-71). Amer-ican Psychological Association, Washington DC, 1996.
6 Liberman A, Birch LL: Interactional developmental approach. In: Failure toThrive. D Drotar (ed), pgs 259-77. Plenum Press, New York, 1985.
7 Satter E: Child of Mine: Feeding With Love and Good Sense. Palo Alto,CA: Bull Publishing Company, 2000.
8 Birch L, Fisher J: Development of eating behaviors among children andadolescents. Pediatrics 101:539-49, 1998.
9 Birch L: Development of food acceptance patterns. DevelopmentalPsychology 26:515-19, 1990.
10 Birch L, Fisher J: Appetite and eating behavior in children. In: The PediatricClinics of North America: Pediatric Nutrition. GE Gaull (ed.) (pp. 931-53).Saunders, Philadelphia, Pennsylvania, 1995.
11 Birch, L. & Fisher, J. The role of experience in the development of chil-dren’s eating Behavior. In: Why we eat what we eat: The psychology ofeating. E Capaldi (ed.) (pp. 113-41). American Psychological Association,Washington DC, 1996.
12 O’Brien M: Child-rearing difficulties reported by parents of infants andtoddlers. J Pediatr Psychol 21: 433-46, 1996.
13 Crist W, Napier-Phillips A. Mealtime behaviors of young children: Acomparison of normative and clinical data. Developmental and BehavioralPediatrics, 22:279-86, 2001.
Feedin
g S
trate
gie
s for O
lder In
fants a
nd To
ddle
rsPlay centered on food needs to be “play-with-a-purpose,”which allows the older infant and toddler to explore food asone more exciting and fun part of their world, as well as teachthem how to manage food once it gets it into their mouths.
Number 100 | Fall 2002 11PediatricBasics®
®

Number 100 | Fall 2002
®
PediatricBasics®
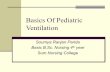
• Babies first learn to“munch” soft foods with their jaws up anddown (9-10 months)
• “Chewing,” comes secondby adding a small grindwith the teeth and a side-to-side motion with thejaw (between 12-14 month)
Babies need to learn to:• First, move food around in their
mouths without gagging• Then, move their tongues from
side to side• Finally, place food on the molar
area of the gums for chewing
• Begin cup drinking witha spillable, two-handledsipper cup. Let babyexplore stick-shaped toysand foods (8 months)
• Add small, very meltable pieces of food (9 months)
• Introduce utensilsaround 1st birthday, but encourage fingerfeeding until after 2nd
For a complimentary supply of this wall poster, call 1-800-595-0324
ORAL SKILLS
SENSORY SKILLS
Coordination of the eight senses:• Seeing• Hearing• Tasting• Touching• Smelling• Balance• Body Awareness• Joint Information
POSTURNALSTABILITY
• Start feeding your baby inan infant seat
• Move her to a high chairaround 8 months
• Bring your toddler in closeto the family table
PARENT SKILLS
Babiesneed to
explore toysand food with
their hands and mouths.
Addsoft table
foods whenyour baby
starts“chewing.”
Do allowyour baby toget messy!
• Choose appropriate foods• Show and tell your baby how to eat
and enjoy new foods• Don’t give in to “food jags”• “Dress up” the flavor of foods to make
them more interesting – cheese sauce on peas, lemon sprinkled on cooked carrots
Repeatedexposure isthe key to
learning to like agood variety
of foods.
Ratherthan spooningfood in, gently
touch the spoon toyour baby’s lips
and let her comefor it.
JAW SKILLS
HAND-TO-MOUTH SKILLS
Goodback and
side support is essential for goodeating.
when you’re still learning…there’s more to food than just eating

Forty-percent of mothers of normally developingchildren will report difficult behaviors duringmealtimes in the first 2 years of life.1 These
feeding problems, which include picky eating, foodjags, refusal to eat textured foods, refusal to eat at all,and stalling, are typically outgrown. Another groupof children—those with eating impairments thatinvolve oral-motor skills (dysphagia)—are atrisk of life-long feeding problems. Theseare children born very prematurely,with failure-to-thrive,2 geneticsyndromes, oral apraxias,
encephalopathies, traumatic brain injury or develop-mental delay.3 Whether the eating impairment ismild, moderate or severe, these children will notoutgrow their feeding difficulties. Therapy willimprove their overall feeding skills, but it will notcompletely eliminate the problem.
This article will discuss the pathologies and severity of the clinical manifestations of eating impair-
ments and help the pediatrician determineif a feeding problem can be dealt with in
the office, or if a referral or furtherevaluation/treatment are indicated.
Erika G. Gisel PhD, OTR, ergProfessor, School of Physical & Occupational Therapy, McGill UniversityDirector, Swallowing and Dysphagia Clinic, Montreal Children’s HospitalMontreal, Quebec
Feeding Problems During Weaning and Beyond
Synopsis — Children with eating impairments that involve oral-motor skills (dysphagia) are at risk oflife-long feeding problems. They are typically children born prematurely, with failure-to-thrive, geneticsyndromes, oral apraxias, encephalopathies, traumatic brain injury or developmental delay. Thosewith moderate to severe feeding problems are best referred for evaluation by a dysphagia specialist,who relies on observational as well as instrumental assessments of anthropometric growth, feedingefficiency, and oral-motor skills for diagnosis and treatment.
The pediatrician is often the first medical professional to examine and diagnose children with feedingproblems. Recognition of the symptoms and classification of the nature of the problem will allow thepediatrician to take the necessary steps to ensure that the child and family receive the care andfollow-up needed.
14

Neither the cause nor theeffect of feeding problems is isolated to the ingestivesystem; thus, problems thatcan arise from and affectother systems of the bodywill also be discussed.
Behavioral Characteristics ofIngestive ProblemsFeeding difficulties duringinfancy most frequentlymanifest as problems with: 1) eating efficiency, (i.e., the feeding effort of the childand indirectly the caregiver), 2) controlling the inges-tion of liquids, and 3) poor oral-motor skills. Difficultywith the ingestion of liquids and poor oral-motor skillsare not independent of poor eating efficiency. Both ofthese skills need to be well-developed to ingest a mealwith ease and in a reasonable amount of time (20-30minutes).4 Mealtimes exceeding this range may pointtoward greater feeding effort. When feeding effortexceeds the required energy intake, a child may not beable to keep up with growth demands and marginalnutrition or frank energy malnutrition may result.5,6
Interestingly, children with mild feeding problems take longer to eat solid foods, whereas children withmoderate and severe problems take significantlylonger to eat both solids and purees. While this obser-vation may appear counter-intuitive at first glance, itpoints to the fact that manipulating and controlling“runny” food substances in the mouth is more difficultthan the more solid, firm food textures.7
Triage in the Pediatrician’s OfficeA thorough medical history will help the cliniciandetermine to what extent underlying medical prob-lems may contribute to an infant or child’s feedingproblem(s). Anthropometric measurements providean indication of whether feeding problems are acute,manifested by wasting, or long standing as indicated
by stunting.5,8,9 A feedingobservation would help theclinician determine if feedingdifficulties are complicated byinteraction problems betweenthe child and feeder. Becauseliquids are the most difficultto ingest, children with oral-motor problems are oftenconstipated.10 The caregivermay believe adequate amountsof liquids are being offered,but much (up to 50%) of the
volume may be lost due to spilling.5 A child who isconstipated is not interested in eating.
Examination of the oral phase begins with an observa-tion of the general oral health, the shape of the palateand the dentition. Children with carious lesions oftenexperience sensitivities to hot or cold, or to sweetfoods and may refuse foods that cause pain. Promptdental care usually resolves the problem.3 A determi-nation of feeding efficiency follows, by getting an esti-mate of meal duration and if the child is able to eatdifferent food textures, enjoys or at least toleratesdifferent flavors, and how difficult drinking is. Thefrequency of coughing during or after meals, regurgi-tation, choking or vomiting needs to be established.Food refusals may be texture or taste related or, whennutrient related, may point toward food allergies.There may be oral sensory deficits but, unless veryobvious, these are difficult to examine reliably.
Examination of the pharyngeal phase may begin with anobservation of how often children swallow on a bite of food. One or two swallows are considered normal.11
Repeated effortful swallowing points toward ineffi-ciency in feeding and possible associated pharyngealproblems. If the child sounds congested and the care-giver indicates that this is the child’s normal function,or if there is a history of recent repeated pneumonias,then aspiration may be suspected. Referral for a video-fluoroscopy would be justified.
Feedin
g P
roble
ms D
urin
g W
eanin
g a
nd B
eyo
nd
Number 100 | Fall 2002 15
Feeding difficulties during infancy most frequently manifest as problems with: 1) eating efficiency, (i.e., the feeding effort of the child and indirectly the caregiver),2) controlling the ingestion of liquids, and 3) poor oral-motor skills.
PediatricBasics®
®
A thorough medical history and physical examinationwill help determine to what extent underlying medicalproblems may be contributing to a child’s feedingproblem.

Examination of the esophageal phase. Persistent gastro-esophageal reflux with regurgitation may indicate achronic condition that can be very painful and leadto food refusal. Pharmacologic treatment of thecondition has been described.12 In-coordination ofthe peristaltic wave initiated by swallowing has beendescribed in children with encephalopathies,13 butcan also be present in myopathies. Liquids may stillbe ingested adequately, but the transport of a solidbolus will be much more difficult and may causediscomfort. These children may be reluctant toaccept the tacky and more solid food textures. Peri-staltic in-coordination is not isolated to the esoph-agus and delayed gastric emptying oftenaccompanies coordination disorders.14,15
Some private, as well as hospital-based clinics exist thatspecialize in ingestive problems, hence patients maybe referred for evaluation and treatment in this highlyspecialized field. If these resources are not readilyavailable due to geographic distance, consultation byphone, fax or e-mail can usually be arranged. Chil-dren who require specialized care and long-termfollow-up due to the complexity of their medical andrehabilitation needs are best referred for evaluationand services by a multidisciplinary team.
Assessment by a Feeding SpecialistTo evaluate the nature andextent of a feeding problem, thedysphagia specialist relies onobservational as well as instru-mental assessments of anthro-pometry, feeding efficiency, andoral-motor skills.
Anthropometric measurements ofheight and weight measurementscontribute to the classification ofthe problem as mild, moderate orsevere.16 If a reliable measurementof height is difficult to obtain, dueto contractures or other growthdeformities, body segments of arm-and leg length may be substi-tuted.17 Measurements of skinfolds(triceps, subscapular)18,19 are excel-lent indicators of energy reserves.20
Measurement of feeding efficiency helps identify thefeeding effort of the child and indirectly the caregiver.Standards of feeding efficiency for young children, 6 months to 2 years21 and 2 to 8 years,22 have beendeveloped. Examination of eating efficiency requiresthe eating of three textures of food: puree (unsweet-ened apple sauce), viscous (raisins) and solid (wheatbiscuits). The examination is videotaped so that theduration (in seconds) for each texture can be calcu-lated. This examination has proven very useful forthe diagnostic characterization of mild, moderateand severe problems.4
Standardized reliable and valid assessments also maybe used. The Schedule for Oral Motor Assessment [SOMA]is intended for children, 8 months to 2 years of age,who have mild eating impairments23,24 and The Multi-disciplinary Feeding Profile was developed for childrenwith neurologically based eating impairments.25,26 Giseland collaborators have used the Functional FeedingAssessment (FFA) extensively for the assessment of chil-dren with cerebral palsy and feeding impairments.27-34
The FFA consists of a meal observation covering bothnormal and abnormal feeding responses in sixdomains: spoon feeding, biting, chewing, cup- andstraw-drinking and the externally visible signs ofswallowing. The FFA is sensitive to change so that theeffectiveness of treatment can be determined.34
Anthropometric measurements,feeding efficiency and oral-motorskills constitute the basic compo-nents of our initial assessment,but other domains may needfurther evaluation, such assensory and taste perceptions. Forchildren with oral-motor deficits,reliable sensory responses are verydifficult to obtain. Assessmentsoften require verbal responsesthat children may not be able togive reliably, or tests require themanipulation of an object in themouth. The motor deficit mayhinder the manipulation of theobject and affect accurate sensoryperception of the stimulus.35
Some children have oral
To evaluate the nature and extent of a feeding problem, the dysphagiaspecialist relies on observational as well as instrumental assessmentsof anthropometry, feeding efficiency, and oral-motor skills.
16
Children who are born very prematurely areat risk of life-long eating impairments thatinvolve oral-motor skills.

Oral-Motor Milestones During Infancy
During early infancy, the oralmovements of suckling occurin rhythmic unison with thejaw.1 The lips form a sealaround the nipple, and thelowering of the jaw creates avacuum in the oral cavity thatpermits the extraction ofliquid.2 There is also a compo-nent of compression, throughthe closing of the jaw thatsqueezes milk from the nipple.3
Together, suction and expres-sion contribute to a highly effi-cient system of feeding.
Later, during weaning the olderinfant begins to munch (verticalmovements of the jaw) and chew (vertical and rotary move-ments of the jaw) modified solid food textures of an adultdiet.4 In this process the jaw assumes a stabilizing function,permitting the tongue greater freedom of movement to placefood between the teeth for chewing (lateral movements) andto direct food in preparation for swallowing. Drinking from acup or straw requires that the jaw be held in a semi-open,stable position and that the lips engage the drinking utensilso that the liquid content can be taken in a sequence of sips.4
These movements emerge spontaneously in the typicallydeveloping child. However, infants experiencing difficultywith the oral-motor components of weaning, particularlystabilization of the jaw, often confirm earlier suspicions thatthere may be developmental delay or disability. A childwhose development does not progress to a stable jaw willhave great difficulty or may not be able to make the transi-tion to the feeding of solids. While delay vs. disability duringweaning may be difficult to distinguish, recent work hasshown that many children do not “grow out” of these difficul-ties.5 Hence, prompt attention to mothers’ concerns, evalua-tion and therapy are essential to ameliorate these problems.
1 Bosma JF: Development of feeding. Clin Nutr 5:210-8, 1986.
2 Bosma J, Hepburn J, Josell SD, Baker K: Ultrasound demonstration of tonguemotions during suckle feeding. Dev Med Child Neurol 32:223-9, 1990.
3 Sameroff AJ: The components of sucking in the human newborn. J Exp Psychol6:607-23, 1968.
4 Morris SE, Klein MD: Pre-feeding Skills: A Comprehensive Resource for FeedingDevelopment. Therapy Skill Builders, Tucson, AZ, 1987.
5 Gisel EG, Tessier MJ, Lapierre G, Seidman E, Drouin E, Filion G: Feeding manage-ment of children with severe cerebralpalsy and eating impairment: An exploratorystudy. Phys Occup Ther Pediatr, 2002 (in press).
Feedin
g P
roble
ms D
urin
g W
eanin
g a
nd B
eyo
nd
dys/apraxias,36 which make viscous and fibrous foodtextures particularly difficult to eat. Dental occlusionsno doubt contribute to the efficiency of chewing inchildren with neurological eating impairments.37 Morework is necessary to unequivocally establish such anassociation.
Treatment OptionsGisel and Alphonce have proposed a classificationsystem of mild, moderate and severe problemsbased on anthropometric measurements, feedingefficiency and oral-motor skills.4 This approach hasproven very helpful for diagnosis and treatmentplanning because children in each category havedifferent treatment needs.
Mild Feeding Problems Children with mild feeding problems may benefitfrom special feeding utensils. These may be designedto make the grasp of the utensil easier, provide ascooping edge on the plate to facilitate food pick-up,or prevent the spill of liquids by providing a lid with adrinking spout on cups. Children’s weight should bemonitored at least twice a year to ensure they followtheir established growth trajectory. In general, children may require more time to eat than theirpeers and where possible, this extra time should beprovided.3 Children with mild feeding problems tendto eat foods with softer textures (muffins, yogurts, softfruits etc.), which can reduce feeding effort and somaximize intake.38 One component of oral-motorproblems may be a deficit in motor planning, i.e. adyspraxia or apraxia.36 A study is currently in progressto determine if praxis training may improve oral-motor, hence, feeding skills.39
Moderate Feeding ProblemsIn terms of oral-motor competence, two treatmentapproaches have been systematically studied in chil-dren with moderate feeding problems: a) sensori-motor treatment and b) treatment with intra-oraldevices.
Sensorimotor treatment. Five to 7 minutes of sensori-motor exercises once a day for 5 days a week, over a period of 10 weeks, has resulted in significantimprovements in biting, chewing, the handling ofpurees and swallowing.29,31 The maintenance of theseskills over the longer term has not yet been studied.
Children with mild feeding problems tend to eat foodswith softer textures (muffins, yogurts, soft fruits etc.),which can reduce feeding effort and maximize intake.
PediatricBasics®
®
Number 100 | Fall 2002 17

While improved oral-motor skills may facilitate theday-to-day feeding, as children enter their adolescentgrowth spurt, when growth demands double, oral-motor therapy alone cannot meet their growth needs.Oral supplementation with high calorie foods anddrinks will be necessary. This group of children is alsoprone to upper respiratory infections; they tend tolose weight during bouts of illness and catching up ingrowth after recovery is difficult if not impossible.29
Oral appliance therapy. Appliance therapy with theInnbruck Sensorimotor Activator and Regulator(ISMAR) has been studied extensively in children withmoderate feeding impairments.32-34,37,40 The appliancefacilitates the permanent stabilization of the jaw,thereby permitting the tongue to begin moving morefreely.34 In general, children wear the appliance for atleast a year in order to benefit maximally from itsimpact on the oral-pharyngeal apparatus.33 Follow-upduring a second year showed that children maintainedthe skills gained during the first year of ISMARtherapy.32
Children with moderate feeding problems may haveambulatory problems and depend on wheelchairs,walkers or tricycles for transportation. They may beincontinent, lack trunk and head control to variousdegrees, and be dependent on others in many activi-ties of daily living. It has been our working hypothesisover a number of years that a reciprocal relationshipexists between body posture and oral structures andvice versa. Examination of this relationship withISMAR therapy has demonstrated that there weresignificant improvements in head-trunk-foot controland that the ambulatory status of children improvedsignificantly above the level of maturation.33 Childrenon ISMAR therapy (mean age 8.3+0.9 years) alsogained sufficient weight to sustain their growth trajec-tory over the study period of 2 years. While there wereno significant changes in terms of weight catch-up, theskills gained nevertheless allowed them to eat more, sothat they could sustain the increased growth needs oftheir larger bodies.
Severe Feeding Problems Children with severe feeding problems come to theattention of the clinician during the first months oflife. Suckling is disorganized and inefficient, and the
infant quickly fails togain weight. There maybe gastro-esophgealreflux and the infantmay be irritable anddifficult to calm.Current managementapproaches are basedon the fact that infantstriple their body weightin the first year of lifeand gain another 30%during the secondyear.3 To meet thisextraordinary growthneed, nutritionalsupport via tubefeeding41,42 must beinstituted promptly.Children needingsupplemental tubefeeds for longer than 4 weeks will be consideredfor gastrostomy feeding43 to free the nasal passages, as well as the pharyngeal-esophageal structures of thetube which occasionally can be irritating to the child.
Tube feeding may persist throughout childhood andoften results in children who will no longer want toeat orally. Therefore, the benefits of adequate nutri-tion and typical use of the oral ingestive system mustbe weighed carefully when such decisions have to bemade. Since there is a risk of aspirating saliva if thechild no longer takes anything by mouth, our philos-ophy is to encourage limited food intake with texturesthat are safe to ingest (determined by clinical historyand videofluoroscopy). Importantly, parents have indi-cated to us that feeding their child is one of the fewremaining meaningful activities for them. Thus, froma social point of view providing “sustenance” is essen-tial for the caregiver. As severely affected childrenhave many medical and rehabilitation needs, theyare usually managed by a multidisciplinary teamconsisting of, but not limited to, a developmentalpediatrician, physical-, occupational- and speechtherapist, and other health professionals as specifichealth needs arise.
continued on page 20
Children with moderate feeding problems may haveambulatory problems, be incontinent, lack trunk andhead control to various degrees, and be dependenton others in many activities of daily living.
18
Whether a child’s feeding problems are mild, moderate orsevere, the timing of feedingsshould be dictated by thefamily’s individual preferencesand available resources.

With the “Back to Sleep” movementand convenience of baby carriers,many parents and care providershave lost sight of the fact thatbabies need to experience manydifferent positions and movementsto develop normally. Clinically, weare now seeing babies with flattenedskulls, poor head control, an inabilityto lift or support their head, extremeresistance to being placed prone,delayed motor milestones, poor finemotor skills, and an increased inci-dence of tortocollis.
A 50% reduction in SIDS deathsconfirms that “Back to Sleep” saveslives. In addition, infants need tospend daily waking time on theirtummy to promote the normal devel-opmental sequence. Tummy timedevelops neck extensors and recip-rocal innervation with the flexors,which provides head control andallows the child to lift the head toclear the nose and airway if acciden-tally moved into this position. Headcontrol also plays an important role inthe suck/swallow/breathe synchrony,speech, chewing, swallowing, sittingand standing. Head turning estab-lished during tummy time supportsairway drainage and throat clearing.Working in the tummy down positionalso promotes strengthening of allback extensors, shoulder girdle,arms, hands and eyes.
Experiencing tummy time from dayone will prevent the vestibularsystem from losing comfort of beingin all positions, expressed as ababy’s discomfort in or dislike fortrying new positions. The vestibularsystem of a two or three month olddoes not accommodate changeeasily. Instead, the body will experi-ence a negative often nauseatingresponse, leading to a negativelimbic response that yields an aver-sion to the activity expressed as anegative physical and emotionalresponse to the position. The effectis similar to an adult experiencing anamusement park ride for the firsttime at the age of 30.
What to Tell ParentsIn utero babies move around andexperience every conceivable posi-tion, all of which are comfortable forthem. Continued experience with avariety of positions and movementsfollowing birth helps babies remaincomfortable with these positionswhile promoting normal development.
Initially, when young babies are ontheir tummy they work on strength-ening muscles in their neck, upperback, arms, hands, and eyes. Thiswill lead to the ability to lift theirchest off the floor and eventually tothe ability to push onto hands andknees and begin rocking and thencrawling. The same muscles strength-ened for crawling also provide thefoundation for fine motor skill such asself-feeding, dressing and eventuallybuilding with blocks and writing.
Babies need to move and experi-ence movement to develop. So for at least fifteen minutes each day —while they are awake, alert andsupervised — babies need practicemoving on their backs, sides, andtummies. While infant seats andcarriers are wonderful conveniences,babies also need to be carried inupright and horizontal positions intheir parent’s arms, on their hip, or in a baby sling or front pack. Thisallows the child to experience move-ment in all planes of motion and tosee the world from many perspec-tives and positions. Viewing theirparents from up, down, front andback also helps babies developvisual perception skills.
Parents who share running commen-taries with their babies, such as “Iam going to pick you up, lay you onyour back, and change your diaper,”help their infants learn what toexpect as they are moved throughspace and give their baby an oppor-tunity to prepare the body for themovement while promoting languagedevelopment. Experiencing move-ment sensations also develops thevestibular or balance center in thebrain. Parents who wear, dance, andtalk with their baby promote theirbaby’s normal development.
If you have any question aboutdelays in development or potentialdevelopmental issues, please referto a pediatric physical or occupa-tional therapist early. It is mucheasier and less expensive to treatissues before incorrect motor path-ways have been established. Parentsof infants and toddlers readily learntherapeutic handling, positioning,and other techniques. Many states in the US have federal funding toprovide early intervention service toyoung children. Frequently the serv-ices are provided at home. If servicesare provided through the federalprogram they are free to the family.Public schools or hospitals withNICU facilities typically channelaccess to these services. Free serv-ices are frequently educationallyrelated. A child may see a clinicianto provide medical and rehabilitativeservices simultaneously. Refer earlyto a pediatric therapist at a school,private clinic, or hospital for anydevelopmental issues. �
Feedin
g P
roble
ms D
urin
g W
eanin
g a
nd B
eyo
nd
Putting Research Into Practice Jacquelin Kilburn, MA, OTR
Jackie Kilburn has been a pediatric occupational therapist for thirty-one years.Before opening herprivate pediatricclinic in LivingstonCounty, Michigan,she supervised the occupationaltherapy depart-ment at Mott Children’s Hospitalin Ann Arbor, MI.
®
PediatricBasics® Number 100 | Fall 2002 19

Whether a child’s feeding problems are mild,moderate or severe, the timing of feedings should bedictated by the family’s individual preferences andavailable resources. For example, some families mayprefer to feed their child before the regular familymeal so their attention can be focused on the childwith special needs. When only a limited number offamily members are able to feed the child, the burdentypically falls on the same person at each meal. Someof our families hire helpers who feed the affectedchild, which provides considerable relief to the care-giver. Children need to be fed at least three times aday so unique strategies that minimize the feedingeffort are usually worked out. The clinician needs tobecome familiar with these unique strategies. Simi-larly, many of the treatment approaches require adaily commitment of the family to do exercises. Alimited number of treatments by a therapist will nothave the same effect as sustained daily treatment overa specified period of time. Therapy will only occur ifthe time commitment fits into the family’s routine, or they are willing to make time available for it.
Feeding Problems Can Arise From andAffect Different Body FunctionsThe oral phase of ingestion constitutes only the begin-ning of the ingestive process, when food is chewedand mixed with saliva in preparation for swallowing.The second, the pharyngeal phase of ingestion, startswith the voluntary swallow and is followed by theesophageal phase, which begins with the entry of foodinto the esophagus and ends with the passage of foodinto the stomach through the relaxation of the loweresophageal sphincter.44 While the three phases areuseful for describing ingestion conceptually, they arecontinuous and there is functional and temporalcontinuity between them.45 Feeding problems, whichcan manifest anywhere along this continuum, are notlimited to the ingestive system and can affect otherbody systems as well.
Pulmonary ProblemsChildren whose rhythmic coordination of suckling orchewing and swallowing is impaired due to underlyingmedical problems are at risk for aspirating liquids or
Children with severe feeding problems come to theattention of the clinician during the first months oflife. Suckling is disorganized and inefficient, andinfants quickly fail to gain weight.
continued from page 18
Mothers are excellent judges of their children’s feeding abilities.1 Theyrecognize and report when they are feeding their child more frequently thanthey had an older sibling, or compared to children of other mothers. Oftenthe duration of the feeds will also be longer than that of comparison children.Mothers may change from breast to bottle-feeding, as it requires lesseffort.1 Nipple holes may be enlarged to facilitate flow,2 or different nippleshapes may be tried to find the most suitable for the child. If the infant isdistractible, extraneous distractions such as blaring radios and TVs willbe turned off, and sibling noise kept to a minimum. As children begin towean, mothers may add extra calories to the food such as butter in pablums,and use milk products with high fat contents, such as full milk, yogurts andpuddings.
All these strategies reflect a greater feeding effort on the part of the motheras well as the child. Careful judgment needs to be exercised to determinewhen such efforts may be exhausting to the mother and alternative strate-gies must be considered to relieve her, as well as to permit the child tocontinue to grow along a desirable growth trajectory.3
1 Ramsay M, Gisel EG, McCusker J, Bellavance F, Platt R: Infant sucking ability, non-organic failureto thrive, maternal characteristics, and feeding practices: a prospective cohort study. Dev MedChild Neurol 44:405-14, 2002.
2 Mathew OP: Determinants of milk flow through nipple units: role of hole size and nipple thickness.Am J Dis Child 144:222-4, 1990.
3 Gisel EG: Oral-motor skills following sensorimotor intervention in the moderately eating-impairedchild with cerebral palsy. Dysphagia, 9:180-92, 1994b.
Coping Strategies
Mothers are excellent judges oftheir children’s feeding abilities.
20
continued on page 22

Feedin
g P
roble
ms D
urin
g W
eanin
g a
nd B
eyo
nd
Number 100 | Fall 2002 21PediatricBasics®
®
Medical History
Height _____________________ Weight _____________________ BMI* _____________________
Skin folds: (Triceps) __________________________ (Subscapular) __________________________
Underlying medical problems, such as premature birth, genetic syndromes, oral apraxias, encephalopathies, failure to thrive, traumatic brain injury, or developmental delay? . . . . . . . . . . . . . . . . .Yes. . . . . . . . . . No
Oral Evaluation
General oral health?. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Good . . . Fair . . .Poor
Shape of palate . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Well Rounded . . High Rounded
Dental condition?. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Good . . . Fair . . .Poor
Estimated time of feeding/meal duration? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30 mins . . . . >30 mins
Any food textures that your child…refuses to eat? If yes, which ones? __________________________________________________ . . . . . . .Yes. . . . . . . . . . Noprefers to eat? If yes, which ones? __________________________________________________ . . . . . . .Yes. . . . . . . . . . No
Any food flavors that your child…refuses to eat? If yes, which ones? __________________________________________________ . . . . . . .Yes. . . . . . . . . . Noprefers to eat? If yes, which ones? __________________________________________________ . . . . . . .Yes. . . . . . . . . . No
Pharyngeal Evaluation
How many times does your child swallow on a bite of food? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1-2 . . . . 3 or more
Does your child frequently have colds or congestion? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Yes. . . . . . . . . . No
Does your child have a history of pneumonia? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Yes. . . . . . . . . . No
Esophageal Evaluation
Does your child cough/spit up/vomit/choke during feedings/meals? . . . . . . . . . . . . . . . . . . . . . . . . . . . .Yes. . . . . . . . . . No
Any discomfort (fussing, crying, arching the body) during or after feeding/meals? . . . . . . . . . . . . . . . . . .Yes. . . . . . . . . . No
Is your child reluctant to accept liquids? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Yes. . . . . . . . . . No
Is your child reluctant to accept solid foods? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Yes. . . . . . . . . . No
Does your child spit up during the night (wet pillow)? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Yes. . . . . . . . . . No
Feeding Evaluation
If previously breast-fed, why was child changed to bottle feeding? _________________________________________________________________________________________________________________________________________________________________
Have you altered the artificial nipple to facilitate feeding? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Yes. . . . . . . . . . NoIf yes, in what manner? _________________________________________________________________________________________
How would you describe mealtimes with your child? _____________________________________________________________________________________________________________________________________________________________________________
* The newly revised pediatric growth charts – which include the new Body Mass Index (BMI) sets – are available on the Centers for Disease Control website(http://www.cdc.gov/growthcharts/.)
Pediatric Feeding Evaluation

more textured food substances into the lungs duringswallowing. A healthy reaction to mis-swallowing is avigorous cough to expectorate the aspirated material.Children who chronically aspirate minute amounts,however, learn to suppress the cough reflex. These arethe “silent” aspirators. Videofluoroscopy (modifiedbarium swallow) is the method of choice to determinethe nature and extent of the problem.46
Some children tire from the “work” of eating and maybe at greater risk for aspiration at the end of the meal,which is usually not examined in videofluoroscopy.
However, recent work indi-cates that careful positioningof the child can minimize oreven eliminate aspiration.43,47
In general, liquids are aspi-rated more frequently thansolids.27,43,47-51 It is not known as yet, however, whether aspiration of small amountsof solids is as detrimental asthe more frequent aspirationof liquids.43
Children who aspirate chroni-cally sound congested, havefrequent colds or even pneu-monia.43 A causal relationshipbetween aspiration andpulmonary disease is difficultto establish,52 partly becausepulmonary disease is treated
symptomatically. If children respond well to a course ofantibiotic therapy, the diagnosis is often made a poste-riori. Hence, the causative factors may not be identi-fied. Preliminary work by Gisel and collaborators hasshown that when children are well-positioned and aspi-ration is controlled, oral feeding may proceed withfood textures that are safe to ingest.43 Pulmonary func-tion improves significantly over the course of one year.
Gastrointestinal ProblemsA discussion of digestive and absorptive problems isbeyond the scope of this review. However, a majorproblem in children who have oral-motor disabilitiesis gastro-esophageal reflux (GER).53 It may manifest
itself as repeated vomiting during or after meals orthere may be a suspicion of reflux when childrenexpress signs of hunger and eagerness to start eating,but then refuse to continue a meal because eating isassociated with discomfort or pain from the passage offood into the stomach. Reflux of acidic material intothe esophagus can cause inflammation,54 hence thepain. Material from GER may also enter the respi-ratory tree and cause irritation and disease of thelungs.52,55-57 The method of choice for identifying refluxis 24hr pH monitoring which can be done on anambulatory basis. Standards exist to determine theseverity of the problem.58 Reflux is usually treatedmedically, but if the reflux cannot be controlled, amore invasive procedure such as fundoplication, asurgical tightening of the LES, may be considered.59,60
These procedures are not without risks and 15-50%complications have been reported.59,60 Food regurgita-tion, vomiting during or after meals, or spitting up atnight (wet pillow) may cue the clinician to explorefurther the association between meals, regurgitationand pulmonary complications.
Oral ingestive problems touch upon an anatomy,physiology and patho-physiology that encompassmany medical specialties: oto-rhinology, radiology,gastro-enterology, respirology, psychology and rehabili-tation. While each specialty has its area of expertise,the collaboration of each may be needed to addressthe unique problems of children with oral ingestivedysfunctions. Children with encephalopathies,muscular disorders, prematurity and specific geneticdisorders are still in need of further study to describethe diagnosis-specific needs of evaluation and treatment.
A particular challenge are children with metabolicdisorders who frequently have associated oral-ingestiveproblems i.e. fucosidosis. The interaction of the twoproblems often limits aggressive oral-motor treatment.Our approach so far has been to focus first on nutri-tion, in order to meet caloric and nutrient needs,before addressing the oral-motor problems. Whilevideofluoroscopy is a helpful adjunct to evaluate thenature and safety of the swallow, there is an urgentneed for a non-invasive methodology that will permitextended and repeated visualization of the swallow.
A healthy reaction to mis-swallowing is a vigorous cough toexpectorate the aspirated material. Children who chronicallyaspirate minute amounts, however, learn to suppress thecough reflex. These are the “silent” aspirators.
continued from page 20
22
Children who aspirate chronicallysound congested, have frequentcolds or even pneumonia.

Conclusion Research in pediatric dysphagia has progressed rapidlyover the past 20 years, with the accurate diagnosis andefficacy of specific interventions better understoodthan ever before.4,27,31,32,34,35,61,62 The pediatrician is oftenthe first medical professional to examine and diag-nose children with feeding problems. Recognition ofthe symptoms and classification of the nature of theproblem will allow the pediatrician to take the neces-sary steps to ensure that the family receives the careand follow-up needed. �
Dr. Erika Gisel’s research on the oral-motor development ofchildren and the efficacy of interventions for children withfeeding disabilities is known internationally. She is a memberof the Academy of Research of the American OccupationalTherapy Foundation, and a member of the Research AdvisoryBoard, Feeding Disorders Center at Baylor College ofMedicine, Department of Pediatrics, Houston, TX. Dr. Gisel is on the editorial boards of Physical & Occupational Therapy in Pediatrics and Occupational Therapy in Health Care.
References1 Ramsay M, Gisel EG: Neonatal sucking and maternal feeding practices.
Dev Med Child Neurol 38:34-47, 1996.
2 Ramsay M, Gisel EG, Boutry M: Non-organic failure to thrive: growth failuresecondary to feeding skills disorder. Dev Med Child Neurol 35:285-97,1993.
3 Gisel EG, Birnbaum R, Schwartz S: Helping the feeding impaired child.Recent Advances in Paediatrics16:59-71, 1998.
4 Gisel EG, Alphonce E: Classification of eating impairments based on eatingefficiency in children with cerebral palsy. Dysphagia 10:268-74, 1995.
5 Patrick J, Gisel EG: Nutrition for the feeding impaired child. J Neurol Rehab4:115-9, 1990.
6 Sullivan PB, Juszczak E, Lambert BR, Rose M, Ford-Adams ME, JohnsonA: Impact of feeding problems on nutritional intake and growth: OxfordFeeding Study II. Dev Med Child Neurol 44:461-7, 2002.
7 Gisel EG, Patrick J: Identification of children with cerebral palsy unable tomaintain a normal nutritional state. Lancet 1:283-6, 1988.
8 Martorell R, Khan LK, Schroeder DG: Reversibility of stunting: epidemiolog-ical findings in children from developing countries. Eur J Clin Nutr 48 Suppl1: S45-57, 1994.
9 Stallings VA, Charney EB, Davies JC, Cronk CE: Nutrition related growthfailure of children with quadriplegic cerebral palsy. Dev Med Child Neurol35:126-38, 1993.
10 Staiano A, Simeone D, Giudice ED, Miele E, Tozzi A, Toraldo C: Effect ofthe dietary fibre glucomannan on chronic constipation in neurologicallyimpaired children. J Pediatr 136:41-5, 2000.
11 Sochaniwskyj AE, Koheil RM, Bablich K, Milner M, Kenney DJ: Oral-motorfunctioning, frequency of swallowing and drooling in normal children and inchildren with cerebral palsy. Arch Phys Med Rehabil 67:866-74, 1986.
12 Andersson T, Lundborg P, Radke M, Dalvag A, Behrens R, Becker M,Goethberg C, Hassall E, Shepherd R, Marcon M, Martin S, Koletzo S,Drouin E: Pharmacokinetics of orally administered omeprazole in children.Am J Gastroenterol 95:3101-6, 2000.
13 Gustafsson P, Tibbling L: Gastro-oesophageal reflux and oesophagealdysfunction in children and adolescents with brain damage. Acta Paedi-atrica 83:1081-5, 1994
14 Hillemeier AC, Lange R, McCallum R, Seashore J, Gryboski, J: Delayedgastric emptying in infants with gastroesophageal reflux. J Pediatr 98:190-3, 1981.
15 Lin CH, Tolia V, Kuhns LR, Dubois RS: Role of gastric emptying in infantswith complicated gastroesophageal reflux. Pediatr Res 25:18A, 1989.
16 Kuczmarski RJ, Ogden CL, Grummer-Strawn LM, Flegal KM, Guo SS, WeiR, Mei Z, Curtin LR, Roche AF, Johnson CL: CDC Growth Charts: UnitedStates. Advanced Data 314:1-28, 2000.
17 Spender QW, Cronk CE, Charney EB, Stallings VA: Assessment of lineargrowth of children with cerebral palsy: use of alternative measures to heightor length. Dev Med Child Neurol 31:206-14, 1989.
18 Frisancho AR: Triceps skin fold and upper arm muscle size norms forassessment of nutritional status. Am J Clin Nutr 27:1052-8, 1974.
19 Tanner JM, Whitehouse RH: Revised standards for triceps andsubscapular skinfolds in British children. Arch Dis Child 50:142-5, 1975.
20 Patrick, J, Boland M, Stoski D, Murray GE: Rapid correction of wasting inchildren with cerebral palsy. Dev Med Child Neurol 28:734-9, 1986.
21 Gisel EG: Effect of food texture on the development of chewing of childrenbetween 6 months and 2 years of age. Dev Med Child Neurol 33, 69-79,1991.
22 Gisel EG: Chewing cycles in 2- to 8-year-old normal children: a develop-mental profile. Am J Occup Ther 42:40-6, 1988.
23 Reilly S, Skuse D, Mathisen B, Wolke D: The objective rating of oral-motorfunctions during feeding. Dysphagia 10:177-91, 1995.
24 Skuse D, Stevenson J, Reilly S: Schedule for oral-motor assessment(SOMA): methods of validation. Dysphagia, 10:192-202, 1995.
25 Judd PL, Kenny DJ, Koheil R., Milner M, Moran R: The multidisciplinaryfeeding profile: a statistically based protocol for assessment of dependentfeeders. Dysphagia 4:29-34, 1989.
Feedin
g P
roble
ms D
urin
g W
eanin
g a
nd B
eyo
nd
Food regurgitation, vomiting during or after meals, or spitting up atnight (wet pillow) may cue the clinician to explore further the associationbetween meals, regurgitation and pulmonary complications.
Number 100 | Fall 2002 23PediatricBasics®
®

26 Kenny DJ, Koheil RM, Greenberg J, Reid D, Milner M, Moran R, Judd PL:Development of a multidisciplinary feeding profile for children who aredependent feeders. Dysphagia 4:16-28, 1989.
27 Gisel EG, Applegate-Ferrante T, Benson J, Bosma J: Effect of sensori-motor treatment on measures of growth, eating efficiency and aspiration inthe dysphagic child with cerebral palsy. Dev Med Child Neurol 37:528-43,1995.
28 Gisel EG: Oral sensorimotor therapy: assessment, efficacy and futuredirections. Occup Ther Int 1:209-32, 1994a.
29 Gisel EG: Oral-motor skills following sensorimotor intervention in the moder-ately eating-impaired child with cerebral palsy. Dysphagia 9:180-92,1994b.
30 Gisel EG: Effect of oral sensorimotor treatment on measures of growth andefficiency of eating in the moderately eating-impaired child with cerebralpalsy. Dysphagia 11:48-58, 1996.
31 Gisel EG, Applegate-Ferrante T, Benson JE, Bosma JF: Oral-motor skillsfollowing sensorimotor therapy in two groups of moderately dysphagic chil-dren with cerebral palsy: aspiration vs non-aspiration. Dysphagia 11:59-71,1996.
32 Gisel EG, Schwartz S, Haberfellner H: Impact of oral appliance therapy: areoral skills and growth maintained 1 year after termination of therapy?Dysphagia 16:296-307, 2001.
33 Gisel EG, Schwartz S, Petryk A, Clarke DD, Haberfellner H: "Whole body"mobility after one year of intra-oral appliance therapy in children with cere-bral palsy and moderate eating impairment. Dysphagia 15:226-35, 2000.
34 Haberfellner H, Schwartz S, Gisel EG: Feeding skills and growth after oneyear of intra-oral appliance therapy in moderately dysphagic children withcerebral palsy. Dysphagia 16:83-96, 2001.
35 Solomon B: The Relation of Oral Sensation and Perception to Chewing,Drinking and Articulation in Athetoid Children and Adults. UnpublishedDoctoral dissertation, Pennsylvania State University, University Park, 1965.
36 Gisel EG, Alphonce E, Ramsay M: Assessment of ingestive and oral praxisskills: children with mild cerebral palsy vs controls. Dysphagia 15:236-44,2000.
37 Schwartz S, Gisel EG, Clark D: Association of occlusion with eating effi-ciency in children with cerebral palsy and moderate eating impairment. JDent Child 2002 (accepted for publication).
38 Gisel EG, Alphonce E, Ramsay H, Patrick J: Growth characteristics andeating skills of children with cerebral palsy and mild eating impairment,2000 (in preparation).
39 Gisel EG: Oral praxis training to facilitate ingestion in children with cerebralpalsy: A novel treatment approach, 2002 (research in progress)
40 Gisel EG, Schwartz S, Haberfellner H: The Innsbruck Sensorimotor Acti-vator and Regulator (ISMAR): construction of an intra-oral appliance tofacilitate ingestive functions. J Dent Child 66:180-7, 1999.
41 Rempel GR, Colwell SO, Nelson RP: Growth in children with cerebral palsyfed via gastrostomy. Pediatrics 82:857-62, 1988.
42 Sanders KD, Cox K, Cannon R, Blanchard D, Pitcher J, Papatakis P,Varella L, Maughan R: Growth response to enteral feeding by children withcerebral palsy. J Parenter Enteral Nutr 14:23-6, 1990.
43 Gisel EG, Tessier MJ, Lapierre G, Seidman E, Drouin E, Filion G: Feedingmanagement of children with severe cerebral palsy and eating impairment:An exploratory study. Phys Occup Ther Pediatr, 2002 (in press).
44 Bosma JF: Development of feeding. Clin Nutr 5:210-8, 1986.
45 Hiiemae KM, Palmer JB: Food transport and bolus formation duringcomplete feeding sequences on foods of different initial consistency.Dysphagia 14:31-42, 1999.
46 Logemann JA: Manual for the Videoflurographic Study of Swallowing.College Hill Press, Inc, San Diego, CA,1986.
47 Larnert G, Ekberg O: Positioning improves the oral and pharyngeal swal-lowing function in children with cerebral palsy. Acta Paediatr 84:689-92,1995.
48 Griggs CA, Jones PM, Lee RE: Videofluoroscopic investigation of feedingdisorders of children with multiple handicap. Dev Med Child Neurol31:303-8, 1989.
49 Morton RE, Bonas R, Fourie B, Minford J: Videofluoroscopy in the assess-ment of feeding disorders of children with neurological problems. Dev MedChild Neurol 35:388-95, 1993.
50 Rogers BT, Arvedson J, Buck G, Smart P, Msall, M: Characteristics ofdysphagia in children with cerebral palsy. Dysphagia, 9:69-73, 1994.
51 Rogers BT, Arvedson J, Msall M, Demerath RR: Hypoxemia during oralfeeding of children with severe cerebral palsy. Dev Med Child Neurol 35:3-10, 1993.
52 Euler AR, Byrne WJ, Ament ME, Fonkalsrud EW, Strobel CT, Siegel SC,Katz RM, Rachelefsky GS: Recurrent pulmonary disease in children: acomplication of gastroesophageal reflux. Pediatrics 63:47-51, 1979.
53 Orenstein SR: Gastroesophageal reflux. Curr Probl Pediatr 21:193-241,1991.
54 Heine RG, Reddihough DS, Catto-Smith AG: Gastro-oesophageal refluxand feeding problems after gastrostomy in children with severe neurologicalimpairment. Dev Med Child Neurol 37:320-9, 1995.
55 Christie DL, O'Grady LR, Mack DV: Incompetent lower esophagealsphincter and gastroesophageal reflux in recurrent acute pulmonarydisease of infancy and childhood. J Pediatr 93:23-7, 1978.
56 Darling DB, McCauley RGK, Leonidas JC, Schwartz AM: Gastroe-sophageal reflux in infants and children: correlation of radiological severityand pulmonary pathology. Radiology 127:735-40, 1978.
57 Hoyoux C, Forget P, Lambrechts L, Geubelle F: Chronic bronchopul-monary disease and gastroesophageal reflux in children. Pediatr Pulmonol1:149-53, 1985.
58 Boix-Ochoa J, Lafuenta JM, Gil-Vernet JM: Twenty-four hour esophagealpH monitoring in gastroesophageal reflux. J Pediatr Surg 96:74-8, 1978.
59 Byrne WJ, Euler AR, Ashcraft E, Nash DG, Seibert JJ, Golloday ES:Gastroesophageal reflux in the severely retarded who vomit: criteria for andresults of surgical intervention in twenty-two patients. Surgery 91:95-8,1982.
60 Turnage RH, Oldham KT, Coran AG, Blane CE: Late results of fundoplica-tion for gastroesophageal reflux in infants and children. Surgery, 105:457-64, 1989.
61 Reilly S, Skuse D: Characteristics and management of feeding problems ofyoung children with cerebral palsy. Dev Med Child Neurol 34:379-88,1992.
62 Reilly S, Skuse D, Poblete X: Prevalence of feeding problems and oralmotor dysfunction in children with cerebral palsy: a community survey. JPediatr 129:877-82, 1996.
Recognition of the symptoms and classification of thenature of a feeding problem will allow the pediatricianto take the necessary steps to ensure that the familyreceives the care and follow-up needed.
24

There’s more to foodthan just eating.Feeding specialists know that children
learn best during mealtimes filled with
delicious, pint-sized fun, where practice
makes perfect. Gerber® 3rd FOODS and
Graduates were designed with toddlers
in mind. They provide both the valuable
nutrients and great tastes that growing
children need to explore their new-found
independence.
A good source of fun, learning and
independence.
©2002 Gerber Products Company
Professional Information Line:1-800-595-0324

Learn
ing fro
m th
e B
est: W
ill Wonders N
eve
r Cease
? | Feedin
g S
trate
gie
s for O
lder In
fants a
nd To
ddle
rs | Feedin
g P
roble
ms D
urin
g W
eanin
g a
nd B
eyo
nd
Num
ber 100 | Fall 2002
Medical Marketing DepartmentGerber Products Company200 Kimball DriveParsippany, NJ 07054-0622
PRSRT STDUS POSTAGE
PAIDMIDLAND MI
PERMIT NO 16
Each quarter “Pediatrics On-Line” features new, unusual or topical Internetwebsites of interest to pediatric professionals. Below is the quarter’sfeatured list.
If you wish to recommend a website to your colleagues, please call theGerber Professional Information Line at 1-800-595-0324, contact us via e-mail [email protected], or write Gerber Products Company, 200 Kimball Drive, Parsippany, NJ 07054-0622.PediatricsOn-Line
®
Dysphagia Resource Centerhttp://www.dysphagia.com
The Disphagia Resource Center featuresvery good information for those interestedin swallowing and swallowing disorders.Links are provided to sites featuring theanatomy and physiology of swallowing, casestudies, conferences, organizations, andresources. If you’re new to the site, youmight want to begin with their impressivelist of tutorials and articles.
National Center for Research Resourceshttp://www.ncrr.nih.gov
The National Center for Research Resources(NCRR) “serves as a ‘catalyst for discovery’by creating and providing critical researchtechnologies and shared resources” foraddressing pressing trans-NIH researchissues. Program directions emphasize“smart,” network-connected technologies,computer-aided drug design, developmentand testing of gene and molecular therapies,bioengineering approaches to decreasehealth care costs, and enhanced trainingand career development for patient-orientedresearch.
Jump-In Therapy Productshttp://www.jump-in-products.com
JUMP-IN™ Therapy Products, founded byoccupational therapist and product devel-oper Jacquelin Kilburn, features 450 therapyproducts for professionals, families andcare providers that encourage sensoryprocessing, physical restoration and fun. You will find a generous offering of books,videos, and therapy music, as well as handfunction squeeze toys, and self-care products.
American Academy of Family Physicianshttp://familydoctor.org
The American Academy of Family Physi-cians (AAFP) is a national, non-profitmedical association serving family physi-cians, family practice residents and medicalstudents. Their website features terrificinformation for parents, young childrenand teens, including Q&As about stayinghealthy and common health concerns,Health Topics Plus (detailed info on themost common health issues), facts oncommon medicines, herbal remedies and dietary supplements, and advice for what parents can treat at home andwhen they need to call the doctor.
Economic Research Servicehttp://www.ers.usda.gov
The Economic Research Service (ERS) isthe main source of economic informationand research from the U.S. Department ofAgriculture. The ERS examines dietaryquality, nutrient intake, and the roles ofeconomic factors and nutrition educationand information. In addition to recom-mended reading, such as America's EatingHabits: Changes and Consequences, theERS site offers a body of research andanalysis on key topics, including food andnutrition. The site also features: The U.S.Food Marketing System, 2002, The FoodAssistance Landscape, and Examining theWell-Being of Children.
Wide Smileshttp://www.widesmiles.org
One child in 700 is born cleft-affected. It isthe fourth most common birth defect, andthe first most common facial birth defect.Wide Smiles offers support, inspiration,information and networking for familiesdealing with the challenges associated withcleft lip and cleft palate. In addition to an extensive array of short articles on allaspects of feeding an infant with a cleft lipor palate, the site also features articles on:terms and definitions, surgery, causes,insurance issues, dentistry/orthodontia,audiology, speech, school and self-esteem,and much more.
Dysphagia Resource CenterResources for swallowing and swallowing disorders
WIDE SMILESCleft Lip and Palate Resource
Related Documents