Nutrition in AdolescenceJ U N E 2 0 1 8 // B R I E F
Why Focus on Adolescents?
Malnutrition during adolescence can have lifelong consequences. Adolescents undergo rapid biological and socioemotional changes and set lifelong dietary and related habits. Gender norms can leave girls disproportionately impacted by food insecurity, but many adolescent boys are malnourished as well. Adolescent girls are at risk of dropping out of school, marrying, and becoming pregnant—all of which can harm their nutrition and health as well as that of their offspring. Moreover, adolescence marks the last window of opportunity to reverse stunting.
Adolescent Nutrition in Bangladesh
� A nutrition transition is occurring, but undernutrition is still common among adolescents: Stunting has declined but remains high, thin-ness has remained steady, and overweight is increasing. Anemia and deficiencies in iodine, zinc, and vitamin A are common.
� Adolescents—especially girls in poorer households—consume inadequately diverse diets.
� Other determinants of poor nutrition include early marriage, which is declining but still common, and low secondary school enrollment, which is widespread.
� Within Bangladesh, there is large regional variation in different forms of malnutrition and their determinants.
� While there is less nutritional data on adolescent boys, they also experience a high burden of malnutrition, especially thinness.
B A N G L A D E S H
Full technical report available from GAIN upon request: Adolescent nutrition in Bangladesh. 2017. Global Alliance for Improved Nutrition.

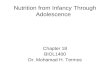
Nutritional Status and Trends
n Nonpregnant, nonlactating women15–49 yearsn Children 6–14 yearsn Iron deficiency anemia
21%
6%
Vitamin A
57%
Zinc Anemia
26%
40% 42%
Iodine
Severe vitamin A deficiency (as shown in the graph) is relatively low, but marginal deficiency is much higher—74% in children 6–14 years and 40% in nonpregnant, nonlactating women.
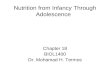
Overweight and obesity, which are risk factors for diet-related noncommunicable diseases such as diabetes and cardiovascular disease, are rising in Bangladesh, as they are worldwide.
Anthropometry in adolescent girls 10-18 years
Thinness—indicating acute deficiency in macronutrients, chronic undernutrition, or both—appears relatively low. This is because the standard measure of this indicator for ado-lescents uses a cutoff reflecting a severe level of thinness. If a cutoff that better corresponded with the severity of adult thinness were used, the prevalence of thinness would probably be closer to that of stunting.
Prevalence of thinness in adolescent girls 10–18 years by division in 2014
7%
8%
9%
10%
11%
12%
13%
14%
15%
16%
17%
Rangpur
Rajshahi
Dhaka
Sylhet
Chittagong
Barisal
Khulna
23%
24%
25%
26%
27%
28%
29%
30%
31%
32%
Rangpur
Rajshahi
Dhaka
Sylhet
Chittagong
Barisal
Khulna
Stunting, which reflects past and recent chronic undernutrition, is declining among adolescent girls but remains high.
Prevalence of stunting in adolescent girls 10–18 years by division in 2014
Prevalence of micronutrient deficiencies and anemia in 2011–2012
2011 2012 2013 2014
32%30%
29%
26%
12%11%
12%11%
3%4%
5%7%
Overweight or obesity
Thinness
Stunting

41%
44%
47%
50%
53%
56%
59%
62%
65%
68%
Rangpur
Rajshahi
Dhaka
Sylhet
Chittagong
Barisal
Khulna
Diets of school-going adolescent boys and girls 13–17 years
Key Determinants of Adolescent Malnutrition
Dietary intake
More than half of adolescent girls and women consumed inadequately diverse diets nationally in 2014.
About 80% of kilocalories per capita per day in Bangladesh are from very micronutrient-poor foods, and 70% are from rice alone (75% for rural adolescents).
Only 58% of households have adequately iodized salt.
Dietary diversity varies by season: it is lowest during the post-aus season and highest during the monsoon.
Wealth quintile
5
(richest)
Wealth quintile
4
Wealth quintile
3
Wealth quintile
2
Wealth quintile
1
(poorest)
77%
65%
54%
44%
32%
¢ 1 or 2 food groups ¢ 3 food groups ¢ 4 food groups
Note: Inadequate dietary diversity is defined here as consumption of fewer than 5 out of the 9 food groups in the previous 24 hours.
By wealth quintile By division
Prevalence of inadequate dietary diversity in women and adolescent girls 10–49 years in 2014
n Boys n Girls
Experienced hunger
sometimes,often,or always
in the past month
Consumed fruit less than onceper day
Consumedvegetables less than
onceper day
Drank carbonated soft drinks
at least once per day
Consumed fast food at least once per week
52%
57%
50% 50%
26%24%
47% 47%
56%
47%

Adolescents11–15 years
Adolescents16–20 years
78%85%
46%35%
n Male n Female
34%
37%
40%
43%
46%
49%
52%
Rangpur
Rajshahi
Dhaka
Sylhet
Chittagong
Barisal
Khulna
15.0 yr
15.5 yr
16.0 yr
16.5 yr
17.0 yr
17.5 yr
18.0 yr
Rangpur
Rajshahi
Dhaka
Sylhet
Chittagong
Barisal
Khulna
Key Determinants of Adolescent Malnutrition
Child marriage and school attendance
Delaying marriage by 1 year in Bangladesh has been associated with nearly a quarter-of-a-year increase in schooling as well as increased literacy for adolescent girls. Educational attain-ment is associated with a host of nutritional outcomes.
Percentage of adolescents attending school by age and sex in 2014
Median age at first marriage among women 20–49 years by division in 2014
Percentage of adolescents 11–17 years attending secondary school by division in 2014
What Can Be Done? � Carry out interventions to promote safe and healthy diets rich in micronutrients and fiber,
including fruits and vegetables, legumes, fish, eggs, meats, and dairy, and that aim to reduce consumption of energy-dense, nutrient-poor foods, such as sugar, refined flours, and oils.
� Expand programs that incentivize school enrollment, delay marriage, and increase educational attainment, especially for adolescents in the poorest households.
� Increase coverage of fortified rice, salt, oil, and wheat flour.
Join us in the fight against malnutrition!www.gainhealth.org
@GAINalliance
www.facebook.com/GAINalliance
Global Alliance for Improved Nutrition