REFRAT RSOP
FRAKTUR TERBUKA
Oleh:
Intannuari Paringga G0006
Rizqinia Sheila Mar’ah G0007147
Yoni Frista Vendarani G0008039
Pembimbing:
Iwan Budiwan Anwar, dr., Sp.OT
KEPANITERAAN KLINIK SMF ORTHOPAEDI DAN TRAUMATOLOGI
FAKULTAS KEDOKTERAN UNS / RSOP PROF. DR. R. SOEHARSO
SURAKARTA
2012

HALAMAN PENGESAHAN
Refrat ini disusun untuk memenuhi persyaratan kepaniteraan klinik Ilmu Bedah
Fakultas Kedokteran Universitas Sebelas Maret Surakarta.
Refrat dengan judul:
FRAKTUR TERBUKA
Oleh :
Intannuari Paringga G0006
Rizqinia Sheila Mar’ah G0007147
Yoni Frista Vendarani G0008039
Pembimbing
Iwan Budiwan Anwar, dr., Sp.OT
2

BAB I.
PENDAHULUAN
Salah satu trauma muskuloskeletal yang menyebabkan morbiditas yang
tinggi adalah patah tulang panjang terbuka (Bedah UGM, 2009). Epidemiologi
dari patah tulang terbuka masih belum banyak diketahui. Kejadiannya bervariasi
di tempat dan institusi yang berbeda, tergantung pada kejadian kecelakaan lalu
lintas dan luka tembak. Level satu trauma center biasanya mendapatkan lebih
banyak kasus patah tulang terbuka dari pada rumah sakit kecil di daerah terpencil
(Court-Brown, McQueen, & Tornetta, 2006). Insidens patah tulang terbuka 4%
dari semua kasus patah tulang. Pada penelitian Grecco et al tahun 2002 yang
berjudul “Epidemiology of Tibial Shaft Fractures” di Brazil, mendapatkan dari
179 patah tulang pada tibia, 120-nya merupakan patah tulang terbuka. Sedangkan
penelitian yang dilakukan oleh Ibeanusi dan Ekere (2007) tentang patah tulang
tibia terbuka di rumah sakit pendidikan Universitas Port Hartcourt, di Nigeria
menemukan dari 72 pasien, 70 merupakan patah tulang terbuka.
BAB II
ISI
A. DEFINISI
Fraktur terbuka adalah putusnya kontinuitas jaringan tulang dimana terjadi
kerusakan kulit dan jaringan dibawahnya berhubungan langsung dengan
dunia luar. Compound fracture merupakan nama lain dari fraktur terbuka
namun istilah tersebut sudah tidak digunakan lagi (Koval & Zuckerman,
2006).
Cedera jaringan lunak dalam fraktur terbuka mungkin memiliki tiga
konsekuensi penting:
- Kontaminasi dari luka dan patah tulang oleh paparan lingkungan.
3

- Peremukan, pengelupasan, dan devaskularisasi menyebabkan jaringan
lunak rentan terhadap infeksi.
- Kerusakan atau kehilangan jaringan lunak dapat mempengaruhi
metode imobilisasi fraktur, membahayakan kontribusi dari jaringan
lunak di atasnya untuk penyembuhan (misalnya, kontribusi sel
osteoprogenitor), dan mengakibatkan hilangnya fungsi dari otot, saraf
tendon, pembuluh darah , ligamen, atau kerusakan kulit.
B. MEKANISME
Fraktur terbuka terjadi karena suatu kekuatan yang keras. Energi kinetik
(.5 mv2) didisipasikan oleh jaringan lunak dan struktur tulang (Tabel 3.1)
Jumlah tulang yang berpindah dan kominusi dapat menandakan tingkat
cedera dan gaya yang diterapkan.
Table 3.1. Energy transmitted by injury mechanism
Injury
Energy (Foot-
Pounds)
Fall from curb 100
Skiing injury 300–500
High-velocity gunshot wound (single missile) 2,000
20-mph bumper injury (assumes bumper strikes fixed
target)
100,000
Sumber: Bucholz et al, 2006.
C. DERAJAT
Tujuan dari sistem klasifikasi patah tulang terbuka manapun adalah
untuk mengira keadaan fraktur dan parameter penatalaksanaan (Cross and
Swiontkowski, 2008). Walau banyak sistem klasifikasi untuk patah tulang
terbuka, sistem klasifikasi Gustillo-Anderson-lah yang paling sering
digunakan di seluruh dunia. Sistem ini menilai patah tulang terbuka
berdasarkan ukuran luka, derajat kerusakan jaringan lunak dan
kontaminasi, dan derajat fraktur (Gustillo et al, 1990). Hal-hal lain yang
4

juga diperhatikan antara lain adalah ada atau tidaknya kerusakan pada
saraf, energy transfer (derajat comminution dan periosteal stripping ), dan
wound dimension . Terdapat tiga macam patah tulang terbuka pada sistem
klasifikasi Gustillo-Anderson, dengan derajat yang ke tiga dibagi ke
dalam tiga subtype lagi berdasarkan kerusakan periosteal, Ada
tidaknya kontaminasi dan derajat kerusakan pembuluh darah (Gustillo et
al, 1990). Pengklasifikasian patah tulang terbuka menurut Gustillo-
Anderson adalah sebagai berikut:
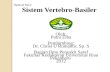
1. Derajat I: Luka biasanya berupa tusukan kecil dan
bersih berukuran kurang dari 1 cm. Terdapat tulang yang
muncul dari luka tersebut. Sedikit kerusakan jaringan
lunak tanpa adanya crushing dan patah tulang tidak
kominutif. Patah tulang biasanya berupa sederhana,
melintang, atau oblik pendek. Biasanya berupa patah
tulang energi rendah.
Gambar 1: Fraktur Terbuka Gustilo-Anderson derajat 1(http://eorif.com/General/Open%20Fx%20Class.html)
2. Derajat II: Luka lebih besar dari 1 cm, tanpa adanya skin flap
ataupun avulsion. Kerusakan pada jaringan lunak tidak begitu
banyak. Kominusi dan crushing injury terjadi hanya
sedang. Juga terdapat kontaminasi sedang. Bisanya juga
berupa patah tulang energi rendah.
5

Gambar 2: Fraktur Terbuka Gustilo-Anderson derajat 2(http://eorif.com/General/Open%20Fx%20Class.html)
3. Derajat III: Terdapat kerusakan yang luas pada kulit, jaringan
lunak, struktur neurovaskuler, dengan adanya kontaminasi
pada luka. Dapat juga terjadi kehilangan jaringan lunak. Luka
yang berat dengan adanya high-energy transfer ke
tulang dan jaringan lunak. Biasanya disebabkan oleh
trauma kecepatan tinggi sehingga fraktur tidak stabil
dan banyak komunisi. Amputasi traumatik, patah
tulang segemental terbuka, luka tembak kecepatan tinggi,
patah tulang terbuka lebih dari 8 jam, patah tulang terbuka
yang memerlukan perbaikan vaskuler juga termasuk dalam
derajat ini. derajat III ini dibagi lagi menjadi tiga
subtype:
a. Derajat IIIA : Tulang yang patah dapat
ditutupi oleh jaringan lunak, atau terdapat penutup
periosteal yang cukup pada tulang yang patah.
Gambar 3: Fraktur Terbuka Gustilo-Anderson derajat 3a(http://eorif.com/General/Open%20Fx%20Class.html)
6

b. Derajat IIIB : Kerusakan atau kehilangan
jaringan lunak yang luas disertai dengan
pengelupasan periosteum dan komunisi yang
berat dari patahan tulang tersebut. Tulang
terekspos dengan kontaminasi yang massif.
Gambar 4: Fraktur Terbuka Gustilo-Anderson derajat 3b(http://eorif.com/General/Open%20Fx%20Class.html)
c. Derajat IIIC : Semua patah tulang terbuka
dengan kerusakan vaskuler yang perlu diberbaiki,
tanpa meilhat kerusakan jaringan lunak yang terjadi
(Apley dan Solomon, 2001 dan Gustillo et al, 1990).
Gambar 5: Fraktur Terbuka Gustilo-Anderson derajat 3c(http://eorif.com/General/Open%20Fx%20Class.html)
Klasifikasi ini menjadi sangat penting untuk menentukan
terapi. Klasifikasi ini juga menunjukkan resiko terjadinya
infeksi, dilihat dari derajat kontaminasi, derajat kerusakan 7

jaringan lunak, dan tindakan operatif pada patah tulang. Resiko
infeksi semakin meningkat seiring dengan derajat yang terjadi.
Resiko terjadinya infeksi pada derajat I adalah 0-12%, pada derajat II 2-
12%, dan pada derajat III 9-55%. Derajat patah tulang terbuka ini juga
sangat erat kaitannya dengan kejadian amputasi, delayed union
dan non-union, dan kecacatan atau penurunan fungsi
ekstermitas. Penentuan derajat patah tulang terbuka secara
definitive dilakukan setelah debridement yang adekuat telah
dilakukan (Gustillo et al, 1990).
D. TATALAKSANA
1. Evaluasi Klinis
Nilai ABCDE:airway, breathing, circulation, disability, and
exposure.
Lakukan resusitasi dan penanganan cedera yang mengancam jiwa.
Evaluasi cedera dari kepala, thorak, abdomen, pelvis dan vertebra.
Identifikasi semua cedera hingga ekstremitas.
Nilai status neurovascular di sepanjang cedera.
Nilai kerusakan kulit dan jaringan lunak: eksplorasi luka dalam
keadaan darurat tidak diindikasikan jika intervensi operatif
direncanakan karena risiko kontaminasi lebih lanjut dandapat
menimbulkan perdarahan lebih lanjut.
Benda asing yang jelas mudah dibersihkan di ruang gawat
darurat dalam kondisi steril.
Irigasi luka dengan salin normal steril dapat dilakukan
dalamruang gawat darurat jika tindakan bedah ditunda.
Injeksi steril sendi dengan salin dapat dilakukan untuk
menentukan jalan keluar dari sisi luka untuk mengevaluasi
kemungkinan kontinuitas.
8

Identifikasi cedera tulang; memerlukan pemeriksaan radiografi.
2. Emergency Room Management
Table 3.3. Factors that modify open fracture classification regardless of initial skin defect
Contamination
A. Exposure to soil
B. Exposure to water (pools, lakes/streams)
C. Exposure to fecal matter (barnyard)
D. Exposure to oral flora (bite)
E. Gross contamination on inspection
F. Delay in treatment >12 hours
Signs of high-energy mechanism
A. Segmental fracture
B. Bone loss
C. Compartment syndrome
D. Crush mechanism
E. Extensive degloving of subcutaneous fat and skin
F. Requires flap coverage (any size defect)
From Bucholz RW, Heckman JD, Court-Brown C, et al., eds. Rockwood and
Green’s Fractures in Adults, 6th ed. Philadelphia: Lippincott Williams &
Wilkins, 2006.
After initial trauma survey and resuscitation for life-threatening injuries (see
Chapter 2):
Perform a careful clinical and radiographic evaluation as outlined earlier.
Wound hemorrhage should be addressed with direct pressure rather than
limb tourniquets or blind clamping.
9

Initiate parenteral antibiosis (see later).
Assess skin and soft tissue damage; place a saline-soaked sterile dressing
on the wound.
Perform provisional reduction of fracture and place a splint.
Operative intervention: open fractures constitute orthopaedic emergencies,
because intervention less than 8 hours after injury has been reported to
result in a lower incidence of wound infection and osteomyelitis. In certain
centers, there has been a move to delay operating on lower-energy open
fractures in the middle of the night and to treat the injury as the first case
of the morning. The patient should undergo formal wound exploration,
irrigation, and debridement before definitive fracture fixation, with the
understanding that the wound may require multiple debridements.
Important
Do not irrigate, debride, or probe the wound in the emergency room if
immediate operative intervention is planned: this may further contaminate
the tissues and force debris deeper into the wound. If a surgical delay is
anticipated, gentle irrigation with normal saline may be performed. Only
obvious foreign bodies that are easily accessible should be removed.
Bone fragments should not be removed in the emergency room, no matter
how seemingly nonviable they may be.
Antibiotic Coverage for Open Fractures (Table 3.4)
Table 3.4. Intravenous antibiotic therapy for open fracturesa
Type
I
Type
II
Type
III
Organic
Contamination
Cefazolin, 1 g every 8 hours X X X
Aminoglycoside, 3–5 mg/kg/dayb X
Penicillin, 2,000,000 units every 4 hours
(or metronidazole, 500 mg every 6
X
10

hours)aAntibiotic doses for adult patients.bVaries with renal function of patient.
From Bucholz RW, Heckman JD, Court-Brown C, et al., eds. Rockwood and
Green’s Fractures in Adults, 6th ed. Philadelphia: Lippincott Williams &
Wilkins, 2006.
Grade I, II: First-generation cephalosporin
Grade III: Add an aminoglycoside
Farm injuries: Add penicillin and an aminoglycoside
Tetanus prophylaxis should also be given in the emergency room (see later). The
current dose of toxoid is 0.5 mL regardless of age; for immune globulin, the dose
is 75 U for patients <5 years of age, 125 U for those 5 to 10 years old, and 250 U
for those >10 years old. Both shots are administered intramuscularly, each from a
different syringe and into a different site.
Requirements for Tetanus Prophylaxis
Immunization history dT TIG dT TIG
Incomplete (<3 doses) or not known + – + +
Complete/>10 years since last dose + – + –
Complete/<10 years since last dose – – –a –
Key: +, prophylaxis required; -, prophylaxis not required; dT, diphtheria and
tetanus toxoids; TIG, tetanus immune globulin; a, required if >5 years since last
dose.
3. Operative Treatment
- Irrigation and Debridement
Adequate irrigation and debridement are the most important steps in open fracture
treatment:
The wound should be extended proximally and distally to examine the
zone of injury.
11

The clinical utility of intraoperative cultures has been highly debated and
remains controversial.
Meticulous debridement should be performed, starting with the skin and
subcutaneous fat (Table 3.5).
Table 3.5. Factors of muscle viability
Color Normally beefy red; rarely, carbon monoxide exposure
can be deceiving
Consistency Normally firm, not easily disrupted
Capacity to bleed Can be deceiving because arterioles in necrotic muscle
can bleed
Typically reliable
Contractility Responsive to forceps pinch or low cautery setting
Typically reliable
From Bucholz RW, Heckman JD, Court-Brown C, et al., eds. Rockwood
and Green’s Fractures in Adults, 6th ed. Philadelphia: Lippincott
Williams & Wilkins, 2006.
o Large skin flaps should not be developed because this further
devitalizes tissues that receive vascular contributions from vessels
arising vertically from fascial attachments.
o A traumatic skin flap with a base-to-length ratio of 1:2 will
frequently have a devitalized tip, particularly if it is distally based.
o Tendons, unless severely damaged or contaminated, should be
preserved.
o Osseous fragments devoid of soft tissue may be discarded.
o Extension into adjacent joints mandates exploration, irrigation, and
debridement.
12

The fracture surfaces should be exposed, with recreation of the injury
mechanism.
Pulsatile lavage irrigation, with or without antibiotic solution, should be
performed. Some authors have demonstrated decreased infection rates
with >10 L of irrigation under pulsatile lavage.
Meticulous hemostasis should be maintained, because blood loss may
already be significant and the generation of clot may contribute to dead
space and nonviable tissue.
Fasciotomy should be considered, especially in the forearm or leg.
Historically, it has been advocated that traumatic wounds should not be
closed. One should close the surgically extended part of the wound only.
More recently, certain centers have been closing the open wound after
debridement with close observation for signs or symptoms of sepsis.
The wound, if left open, should be dressed with saline-soaked gauze,
synthetic dressing, a vacuum assisted closure (VAC) sponge, or an
antibiotic bead pouch.
Serial debridement(s) should be performed every 24 to 48 hours as
necessary until there is no evidence of necrotic soft tissue or bone.
Foreign Bodies
Foreign bodies, especially organic ones, must be sought and removed because
they can lead to significant morbidity if they are left in the wound. (Note: Gunshot
injuries are discussed separately.)
Wood may become blood soaked and difficult to differentiate from
muscle.
Cloth and leather are usually found between tissue planes and may be
remote from the site of injury.
13

The foreign material itself usually incites an inflammatory response,
whereas intrinsic crevices may harbor pathogenic organisms or spores.
Fracture Stabilization
In open fractures with extensive soft tissue injury, fracture stabilization (internal or
external fixation) provides protection from additional soft tissue injury, maximum access
for wound management, and maximum limb and patient mobilization. (See individual
chapters for specific fracture management) (Table 3.6).
Table 3.6. Relative indications for type of skeletal fixation in open fractures
External fixation
1. Severe contamination: any site
2. Periarticular fractures
A. Definitive
Distal radius
Elbow dislocation
Selected other sites
B. Temporizing
Knee
Ankle
Elbow
Wrist
Pelvis
3. Distraction osteogenesis
4. In combination with screw fixation for severe soft tissue injury
Internal fixation
14

1. Periarticular fractures
A. Distal/proximal tibia
B. Distal/proximal femur
C. Distal/proximal humerus
D. Proximal ulnar radius
E. Selected distal radius/ulna
F. Acetabulum/pelvis
2. Diaphyseal fractures
A. Femur
B. Tibia
C. Humerus
D. Radius/ulna
From Bucholz RW, Heckman JD, Court-Brown C, et al., eds. Rockwood and
Green’s Fractures in Adults, 6th ed. Philadelphia: Lippincott Williams &
Wilkins, 2006.
Soft Tissue Coverage and Bone Grafting
Wound coverage is performed once there is no further evidence of
necrosis.
The type of coverage—delayed primary closure, split-thickness skin
graft, rotational or free muscle flaps—is dependent on the severity and
location of the soft tissue injury.
Bone grafting can be performed when the wound is clean, closed, and dry.
The timing of bone grafting after free flap coverage is controversial. Some
15

advocate bone grafting at the time of coverage; others wait until the flap
has healed (normally 6 weeks).
Limb Salvage
Choice of limb salvage versus amputation in Gustilo Grade III injuries is
controversial. Immediate or early amputation may be indicated if:
The limb is nonviable: irreparable vascular injury, warm ischemia time >8
hours, or severe crush with minimal remaining viable tissue.
Even after revascularization the limb remains so severely damaged that
function will be less satisfactory than that afforded by a prosthesis.
The severely damaged limb may constitute a threat to the patient’s life,
especially in patients with severe, debilitating, chronic disease.
The severity of the injury would demand multiple operative procedures
and prolonged reconstruction time that is incompatible with the personal,
sociologic, and economic consequences the patient is willing to withstand.
The patient presents with an injury severity score (ISS; see Chapter 2) of
>20 in whom salvage of a marginal extremity may result in a high
metabolic cost or large necrotic/ inflammatory load that could precipitate
pulmonary or multiple organ failure.
The expected postsalvage function does not justify limb salvage.
The Mangled Extremity Severity Score (MESS) was designed to predict the
likelihood of amputation based on four criteria. A
score of >7 has been reported to predict amputation accurately in both retrospective
and prospective studies (Table 3.7).
Table 3.7. Mangled extremity severity score (MESS) for prediction of amputation
A.Skeletal/soft tissue injury Pointsa
1.Low energy (stab, simple fracture, low-velocity gunshot wound) 1
2.Medium energy (open/multiple fractures or dislocations) 2
3.High energy (close-range shotgun, high-velocity gunshot, crush) 316

4.Very high energy (above plus gross contamination, soft tissue
avulsion)
4
B.Limb ischemia
1.Pulse reduced or absent but perfusion normal 1b
2.Pulseless, paresthesias, diminished capillary refill 2b
3.Cool, paralyzed, insensate, numb 3b
C.Shock
1.Systolic blood pressure always >90 mm Hg 0
2.Hypotensive transiently 1
3.Persistent hypotension 2
D.Age (Years)
1.<30 0
2.30–50 1
3.>50 2aMESS = total points.bScore doubles for ischemia >6 hours.
COMPLICATIONS
Infection: Open fractures may result in cellulitis or osteomyelitis, despite
aggressive, serial debridements, copious lavage, appropriate antibiosis,
and meticulous wound care. Gross contamination at the time of injury is
causative, although retained foreign bodies, soft tissue compromise, and
multisystem injury are risk factors for infection.
Compartment syndrome: This devastating complication results in severe
loss of function, especially in tight fascial compartments including the
forearm and leg. It may be avoided by a high index of suspicion with serial
neurovascular examinations accompanied by compartment pressure
monitoring, prompt recognition of impending compartment syndrome, and
fascial release at the time of surgery.
17

18

BAB III.
KESIMPULAN
19

DAFTAR PUSTAKA
Apley, A.G., Nagayam S., Solomon, L., Warwick, D. (2001). Apley’s System of Orthopaedics and Fractures. :Arnold
Bedah UGM.(2009). Fraktur Terbuka. Retrieved from http://www.bedahugm.net/tag/fraktur-terbuka/ ( 3 April 2012).
Bucholz RW, Heckman JD, Court-Brown C, et al., eds. Rockwood and Green’s Fractures in Adults, 6th ed. Philadelphia: Lippincott Williams & Wilkins, 2006.
Court-Brown, C. M., McQueen, M.M., Tornetta, P.(2006).Open Fractures in P. Tornetta (Eds) Trauma. Baltimore: Lipincott Williams & Wilkins.
Cross & Swiontkowski. (2008). Treatment Principles in the Management of Open Fractures. Indian Journal of Orthopaedics. 42(4). 377-386.
Gustillo, R. B., Merkow, R. L., Templeman, D.(1990).The Management of Open Fractures. The Journal of Bone and Joints Surgery.72-A(2).299-304
http://eorif.com/General/Open%20Fx%20Class.html
Ibeanusi, S.E.B. & Ekere, A.U.(2007).Epidemiology of Open Tibial fractures in a Teaching Hospital. Port Harcourt Medical Journal.1.156-160.
Koval, K.J. & Zuckerman, J. D. 2006. Handbook of Fractures, 3rd Edition. Lippincott Williams & Wilkins. Pp: 20-29.
20