8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 1/134
dNP
Multiple SclerosisFor Non Neurologists
Naraporn Prayoonwiwat, M.D.Neurology Division, Department of Medicine
Siriraj Hospital
[email protected] 02 419 7101-2
September 24, 2009; Khonkaen
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 2/134
Multiple Sclerosis
MS is a rare disease, it is unlikely tobe seen in my general practice.
d NP
Do you think so?
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 3/134
Diagnosis: optic neuritis
Rx: high dose steroids
Case Presentation
A young woman had dimmed
vision of the left eye for 2 days. Eyedrop tried without improvement.
d NP
Eye:
Vision got worse. Pain on eye
movement was noted.
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 4/134
Case Presentation
A young woman felt spinning for
a few days, getting worse withmotion. There was no hearing lossor visual blurring.
d NP
Diagnosis: vertigo
Rx: antivertigo drug
ENT:
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 5/134
Case Presentation
A young woman difficulty in
voiding for 3 days.Urinalysis: WBC 3-5, RBC 5-10, fewbacteria
d NP
Diagnosis: acute urinary retention
Rx: Foley’s catherization, quinolone
Urology:
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 6/134
Case Presentation
A middle age woman had
nausea and vomiting for 5 days. Shehad very frequent hiccoughs for 1day.
EGD: showed mild gastritis
d NP
Diagnosis: acute gastritis
Rx: intravenous PPI
GI:
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 7/134
Case Presentation
A middle age woman had gait
difficulty 2-3 weeks. She could notproperly lift her feet above theground. There was some numbness
at the lower legs.
d NP
Diagnosis: lumbar spondylosis
Inx: CT myelogram
Orthopedics:
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 8/134
Case Presentation
A middle age man experienced
itching at the anterior chest left sidefor 1 week. No rash was noted.
d NP
Diagnosis: dermatitis
Rx: topical steriods
Skin:

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 9/134
Case Presentation
A middle age woman had
headache for 1-2 months. She couldnot do her routine work, was slow inresponse. Mild weakness was noted.
d NP
Inx: CT brain with contrast -mass
Diagnosis: brain tumor
Surgery:

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 10/134
Multiple Sclerosis
The neurological deficits inthese patients were caused by
demyelinating disease of the CNS. All of had MS.
d NP
Do you agree?
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 11/134
Demyelinating Disease
• What is a demyelinating
disease of the CNS?
• What is the significance of
myelin?
d NP
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 12/134
Demyelinating Disease
• Myelin wraps around thenerve axon and contributes to
the conduction velocity of thenerve.
d NP

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 13/134
Demyelinating Disease
• Oligodendrocytes areresponsible for myelin
production in the CNS; whileSchwann cells are responsiblein the PNS.
d NP
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 14/134
Demyelinating Disease
• Diseases affecting the CNSmyelin cause white matter
lesions in the CNS, whereasdiseases affecting the PNScause demyelinating type of
peripheral neuropathy.
d NP
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 15/134
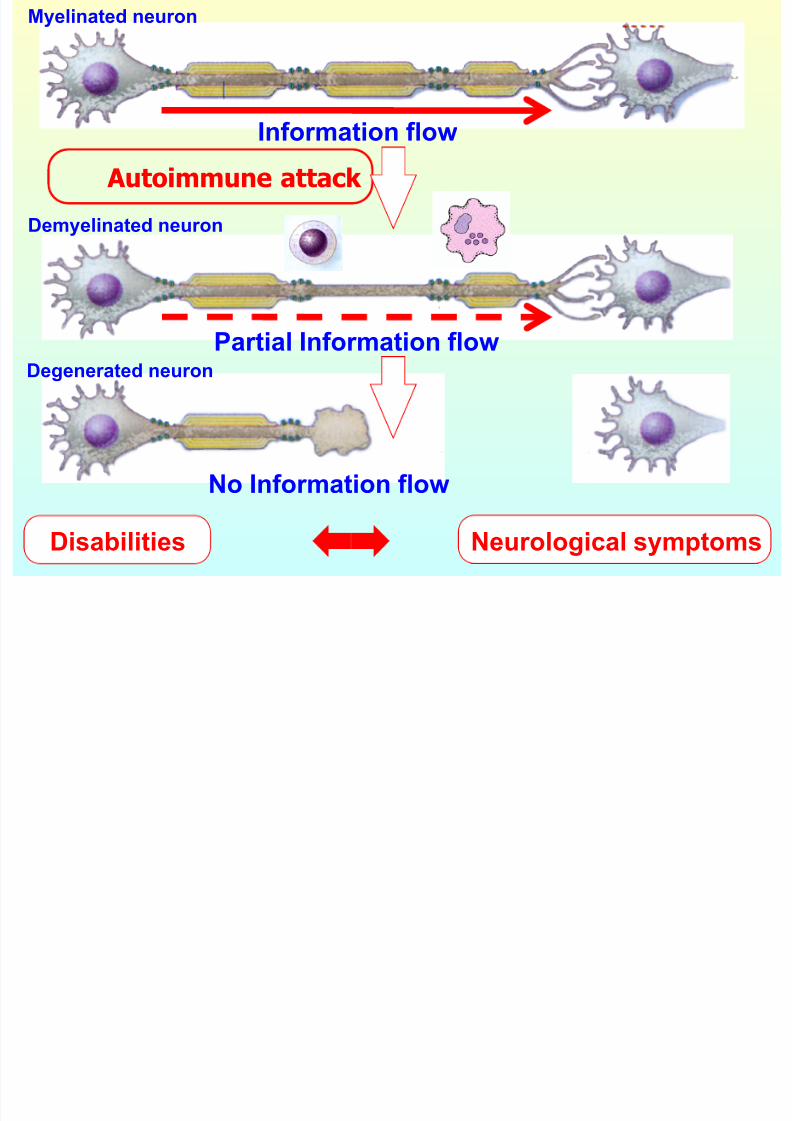
Immunopathogenesis
Myelinated neuron
Demyelinated neuron
Autoimmune attack
Degenerated neuron
Information flow
Partial Information flow
No Information flow
Disabilities Neurological symptoms

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 16/134
Demyelinated fiber
Node of Ranvier
axon
Myelinated fiber
Nerve Conductions
d NP
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 17/134
Demyelinating Disease
• What is MS?
d NP
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 18/134
Multiple Sclerosis
An immune-mediated disorderinvolving mainly the white matter
(myelin) of the CNS which affectssusceptible individuals of both sexesafter exposure to certain
environmental factors.
d NP

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 19/134
Multiple Sclerosis
- Immune-mediated disorderof the CNS
- White matter (myelin)involvement
- Response to environmentalfactors in susceptible persons
- Affect both sexes
d NP
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 20/134
Multiple Sclerosis
Scope:
Clinical manifestations
Pathology
Pathogenesis
DiagnosisTreatment in MS
d NP

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 21/134
dNP
Clinical Presentation
Multiple Sclerosis
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 22/134
Multiple SclerosisClinical Presentation
Cerebrum
Optic nerve
Cerebellum/cerebellar pathway
Brainstem
Spinal cordBladder & Bowel function
Other
d NP
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 23/134
Multiple SclerosisClinical Presentation
Cerebrum
Cognitive impairment
: deficits in attention, reasoning,
executive function (early)
dementia (late)Hemiparesis: UMN
Hemisensory loss
NP

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 24/134
Multiple SclerosisClinical Presentation
Cerebrum (2)
Affects (mainly depression)
Epilespy (rare)
Focal cortical deficits (rare)
Psychiatric symptoms (rare)
NP

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 25/134
Multiple SclerosisClinical Presentation
Optic nerve
Unilateral painful loss of vision
: scotoma
: reduced visual acuity
: impaired color vision: relative afferent pupillary
defect (RAPD)
NP
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 26/134
Multiple SclerosisClinical Presentation
Cerebellum/cerebellar pathway
Tremor
: postural tremor
: intention tremor
Clumsiness and poor balance: limb in-coordination
: gait ataxia
NP

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 27/134
Multiple SclerosisClinical Presentation
Brainstem
Diplopia (double vision)
Internuclear ophthalmoplegia: INO
Nystagmus
Vertigo
d NP

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 28/134
Multiple SclerosisClinical Presentation
Brainstem (2)
Dysarthria (slurred speech)
Dysphagia (swallowing difficulty)
Pseudobulbar palsy
d NP

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 29/134
Multiple SclerosisClinical Presentation
Spinal cord
Weakness
: upper motor neuron signs
Stiffness
: spasticityPainful spasms
d NP
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 30/134
Multiple SclerosisClinical Presentation
Spinal cord (2)
Bladder dysfunction
Erectile dysfunction (impotence)
Constipation
d NP
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 31/134
Multiple SclerosisClinical Presentation
Other
Pain
Fatigue
Paroxysmal symptoms
Temperature sensitivityExercise intolerance
d NP
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 32/134
Multiple SclerosisCommon Presentations
Optic neuritis acute visual loss,
intraorbital pain on eye movement
Acute myelitis limb weakness,
numbness, urinary retention
Brainstem diplopia, INO, facialnumbness, hemiparesis,
hemisensory loss, ataxia
d NP

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 33/134
Multiple SclerosisFunctional Status System
Cerebrum
Optic nerve
Cerebellum/cerebellar pathway
Brainstem
Spinal cordBladder & Bowel function
Other
d NP
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 34/134
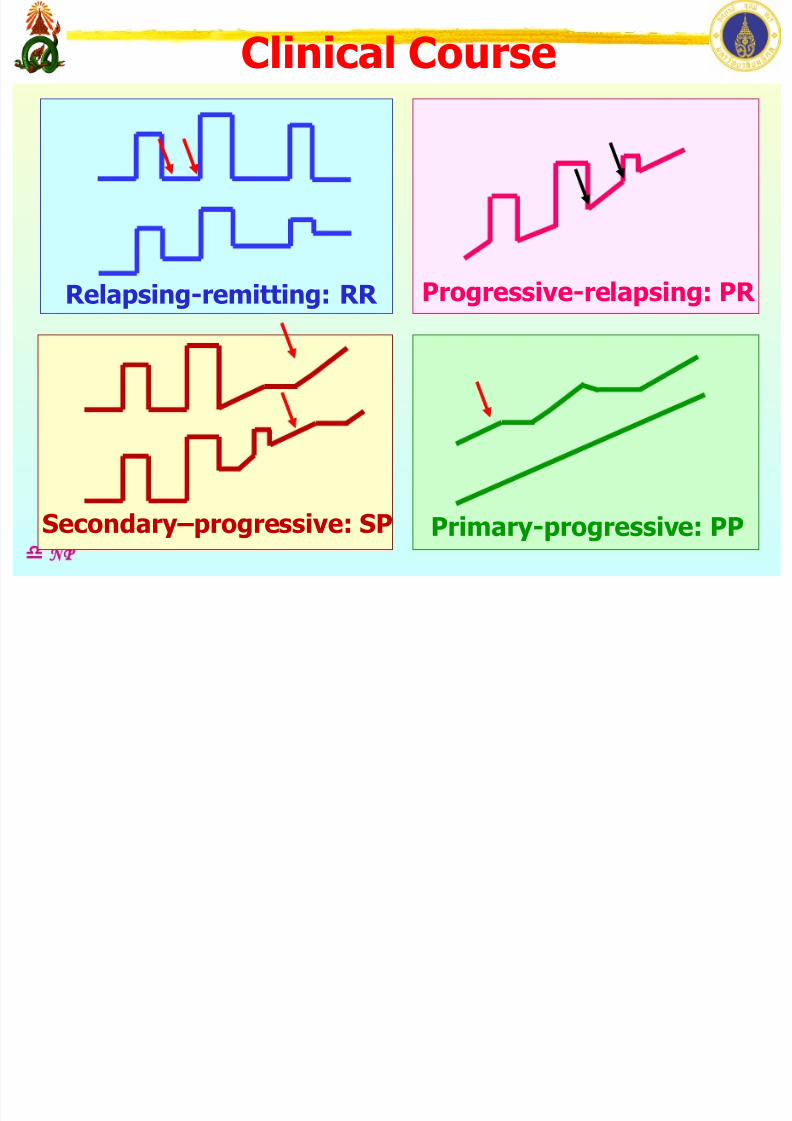
Clinical Course
d NP
Primary-progressive: PPSecondary–progressive: SP
Progressive-relapsing: PR Relapsing-remitting: RR

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 35/134
Clinical Course
d NP
Clinical threshold
Inflammation
Axonal loss
Brain
volume
Relapses
PR RR
PPSP
PR
RR
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 36/134
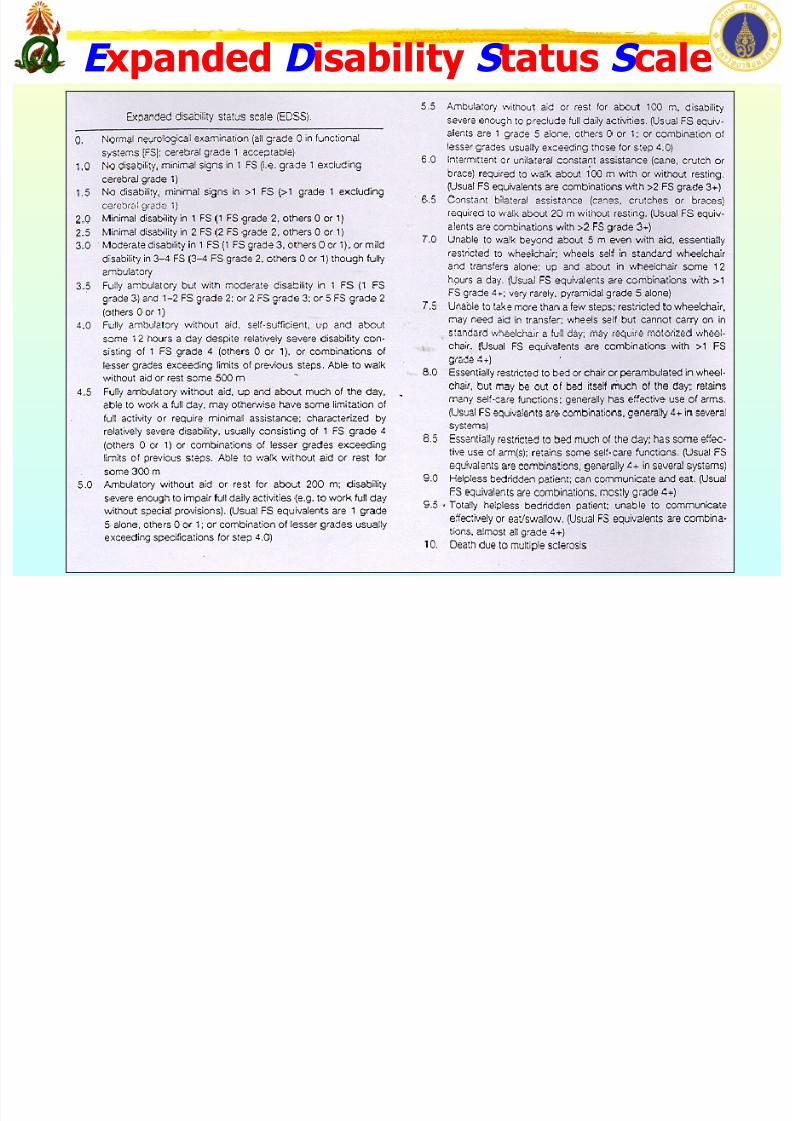
E xpanded D isability S tatus S cale

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 37/134
Multiple Sclerosis
Scope:
Clinical manifestations
Pathology
Pathogenesis
DiagnosisTreatment in MS
d NP
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 38/134
dNP
Pathology
Multiple Sclerosis
MS: Pathology
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 39/134
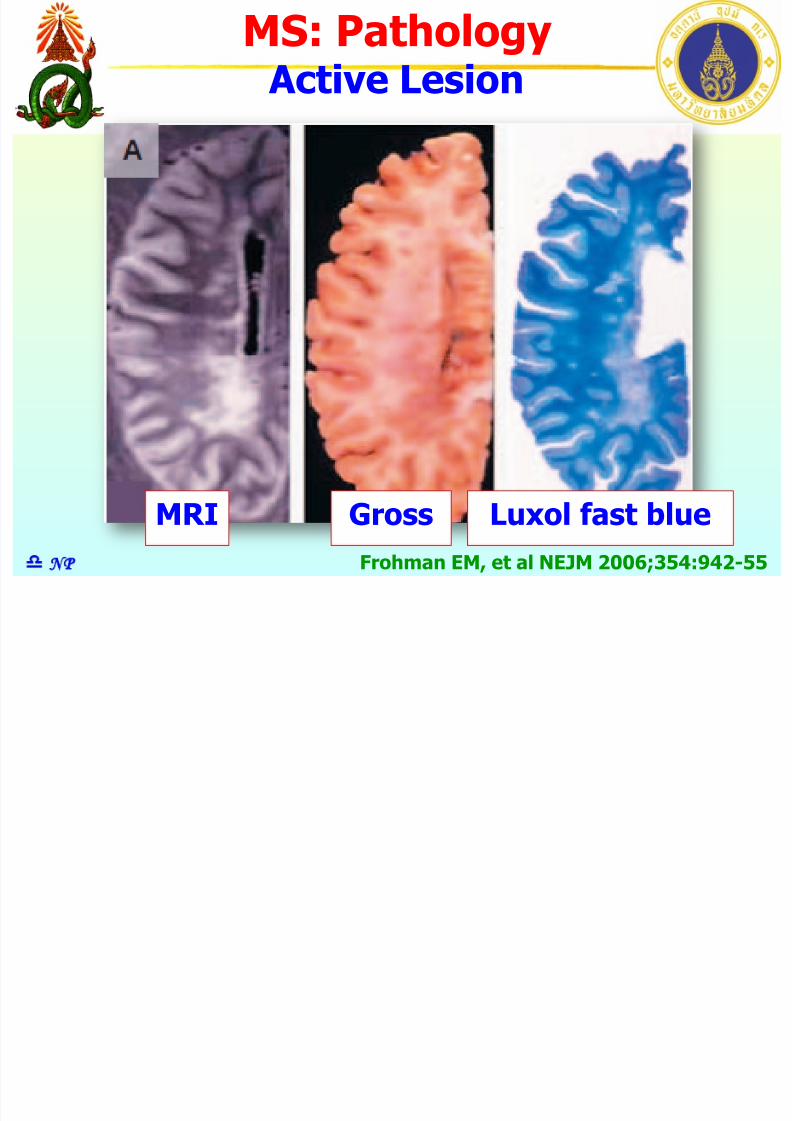
MS: Pathology Active Lesion
d NP
Gross Luxol fast blue
Frohman EM, et al NEJM 2006;354:942-55
MRI
MS: Pathology

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 40/134
d NP Frohman EM, et al NEJM 2006;354:942-55
LFB stain
Perivascular infiltratesMRP14
(Macrophage)
Numerousmacrophage
PLP mRNA in situ hybridization
Toluidine
blue
Electron
Micrograph
Loss of myelin
Demyelination
MS: Pathology
MS Plaque: Acute
MS Patholog

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 41/134
MS: Pathology
MS Plaque: Chronic
d NP Frohman EM, et al NEJM 2006;354:942-55
LFB stainNumerousmacrophage
Demyelinated area Chronic gliotic lesion
Toluidine blue
Astrocyte
No Oligodendrocyte
EM
Astrocyte
Demyelinated axon
Macrophage
Remyelinated axon
Microglia nuclei
MS: Pathology

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 42/134
MS: Pathology
Demyelination-Remyelination
d NP Frohman EM, et al NEJM 2006;354:942-55
EM
Demyelinated axon
Remyelinated axon
RemyelinationDemyelination
MS: Pathology

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 43/134
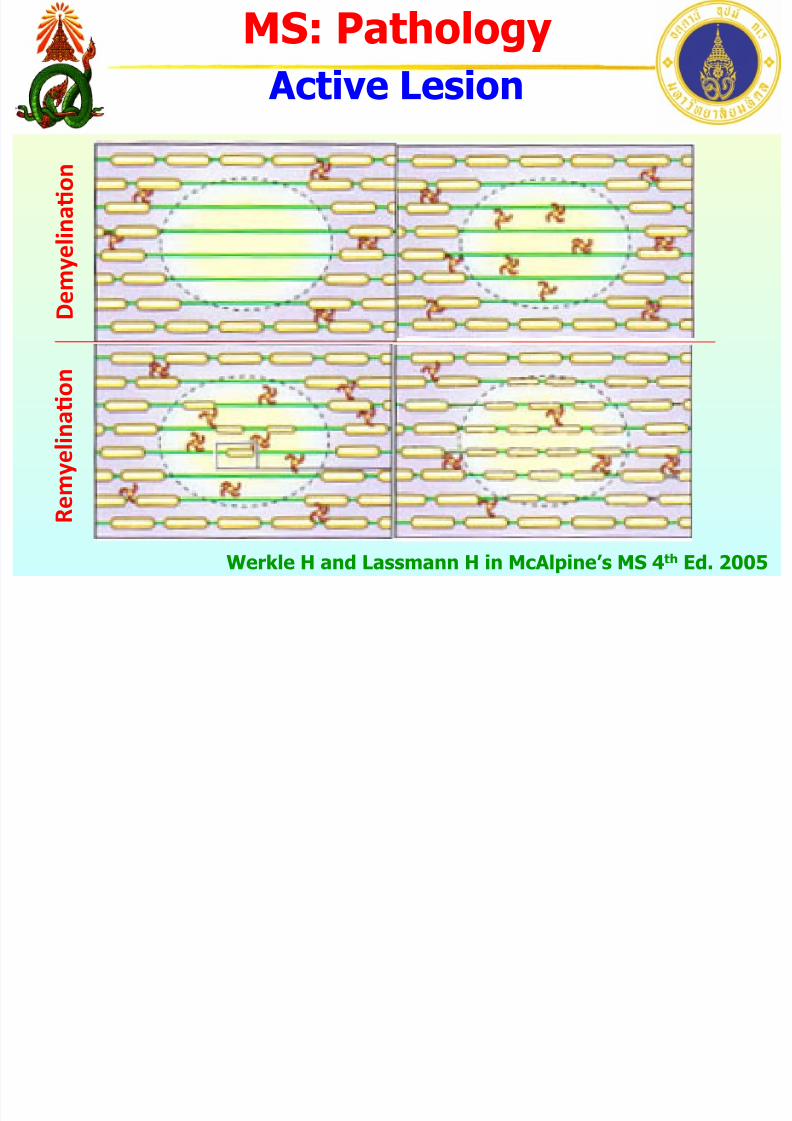
MS: Pathology
Active Lesion
Werkle H and Lassmann H in McAlpine’s MS 4th Ed. 2005
LossofOPC OPCpreserved
Demyelina5on
OPC: oligodendrocyte progenitor cell
MS: Pathology

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 44/134
MS: Pathology
Active Lesion
Werkle H and Lassmann H in McAlpine’s MS 4th Ed. 2005
Early Completed
Remyelina5on
OPC: oligodendrocyte progenitor cell
MS: Pathology
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 45/134
MS: Pathology
Active Lesion
Werkle H and Lassmann H in McAlpine’s MS 4th Ed. 2005
R e m y e l i n a 5 o n
D e m
y e l i n a 5 o n
MS: Pathology

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 46/134
MS: Pathology
Chronic Lesion
Werkle H and Lassmann H in McAlpine’s MS 4th Ed. 2005
R e m y e l i n a 5 o n
D e m
y e l i n a 5 o n
Arrestofremyelina5ngprocess
l
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 47/134
Template SR
[email protected] March 26, 2009 02 419 7101-2d NP

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 48/134
Multiple Sclerosis
Scope:
Clinical manifestations
PathologyPathogenesis
DiagnosisTreatment in MS
d NP
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 49/134
dNP
Pathogenesis
Multiple Sclerosis
Pathogenesis
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 50/134
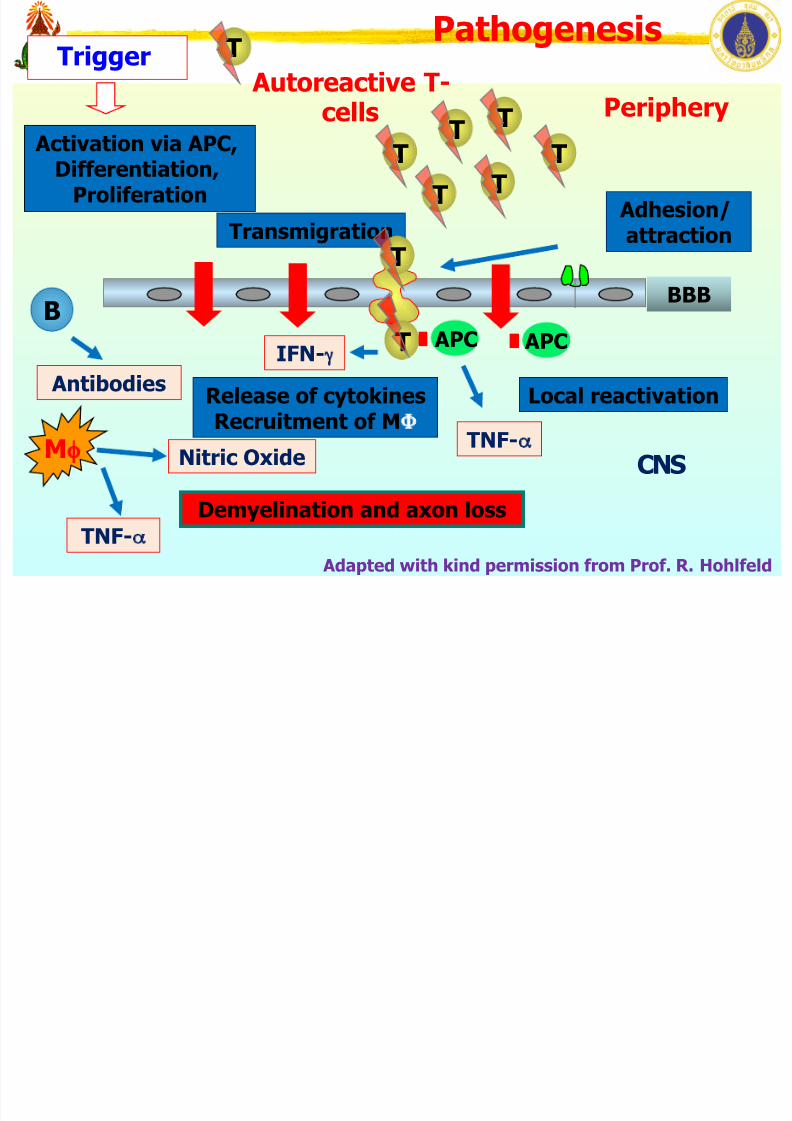
T
Periphery
Demyelination and axon loss
BBB
Transmigration
Activation via APC,Differentiation,
Proliferation
Trigger
Local reactivation
APC
Adhesion/attraction
Release of cytokinesRecruitment of MΦ
Antibodies
B
Mφ Nitric Oxide
IFN-γ
TNF-α
TNF-α Adapted with kind permission from Prof. R. Hohlfeld
Pathogenesis
Autoreactive T-cells
TT
T
T
T
T
T
CNS
T APC
T
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 51/134
Multiple Sclerosis
Scope:
Pathology
PathogenesisClinical manifestations
Diagnosis Treatment in MS
d NP
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 52/134
dNP
Diagnosis
Multiple Sclerosis
Multiple Sclerosis

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 53/134
Multiple SclerosisDiagnosis
Schumacher 1965Poser 1983
McDonald 2001Revised 2005*
d NP
Recommended Diagnostic Criteria for MS:Guidelines from International Panel.McDonald et al. Ann Neurol 2001;50:121-7*Diagnostic Criteria for Multiple Sclerosis:
2005 Revisions to the “McDonald Criteria”.
Polman, et al. Ann Neurol 2005;58:840-6.
Multiple Sclerosis
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 54/134
Multiple SclerosisDiagnosis
Schumacher 1965Poser 1983
McDonald 2001Revised 2005*
d NP
Recommended Diagnostic Criteria for MS:Guidelines from International Panel.McDonald et al. Ann Neurol 2001;50:121-7*Diagnostic Criteria for Multiple Sclerosis:
2005 Revisions to the “McDonald Criteria”.
Polman, et al. Ann Neurol 2005;58:840-6.
Multiple Sclerosis
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 55/134
Multiple SclerosisDiagnostic Consideration
• Objective evidence of
dissemination in time and space
d NP
• Clinical evidence:
presence of clinical signs
history of symptoms:
Ann Neurol 2001;50:121-7
insufficient
Multiple Sclerosis

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 56/134
Multiple SclerosisInvestigations
• Magnetic resonance imaging
• Evoked potentials:
visual auditorysomatosensory motor
• CSF analysis
cell count IgG index
oligoclonal band
d NP
Multiple Sclerosis
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 57/134
Multiple SclerosisMRI Criteria
MRI criteria:• Dissemination in space
brain MRIspinal cord MRI
• Dissemination in time
Barkhof F. Brain 1997;120:2059-69Tintore M. Am J Neuroradiol 2000;21:702-6 NP
Multiple Sclerosis

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 58/134
Multiple SclerosisMRI Criteria
MRI criteria:• Dissemination in space
brain MRI spinal cord MRI
• Dissemination in time
Barkhof F. Brain 1997;120:2059-69Tintore M. Am J Neuroradiol 2000;21:702-6 NP
Multiple Sclerosis

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 59/134
Multiple SclerosisDissemination in Space
Brain MRI criteria:• 9 T2 hyperintense lesions or
1 Gd-enhancing lesion• > 1 infratentorial lesion
• > 1 juxtacortical lesion
(subcortical U-fiber)• > 3 periventricular lesions
Barkhof F. Brain 1997;120:2059-69Tintore M. Am J Neuroradiol 2000;21:702-6
Lesion > 3 mm in cross section
3 i n 4
Spinal cord
d NP
MRI Criteria for

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 60/134
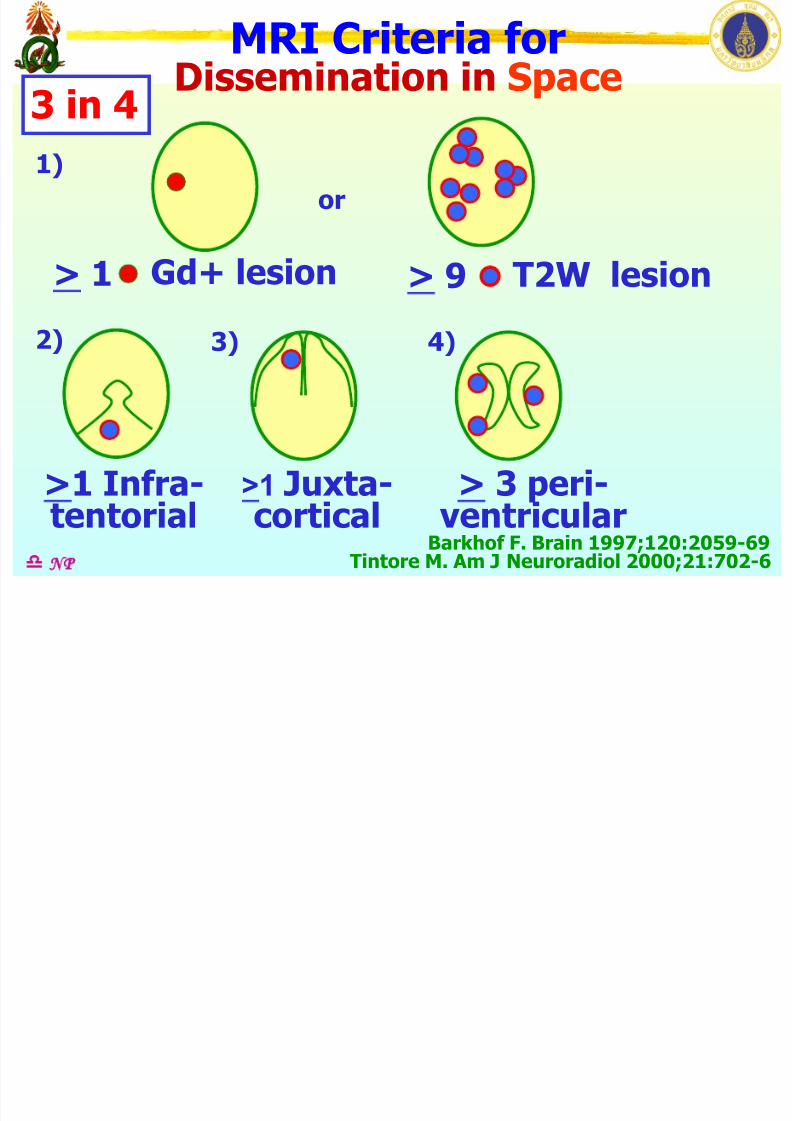
T2W lesions > 9
MRI Criteria for Dissemination in Space
or
Gd+ lesion
3 in 4 1)
2) 3) 4)
>1 Infra-tentorial
>1 Juxta-cortical
> 3 peri-ventricular
> 1
Barkhof F. Brain 1997;120:2059-69Tintore M. Am J Neuroradiol 2000;21:702-6 NP
MRI Criteria for
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 61/134
MRI Criteria forDissemination in Space
or
Gd+ lesion
3 in 4
T2W lesion
1)
2) 3) 4)
>1 Infra-tentorial
>1 Juxta-cortical
> 3 peri-ventricular
> 1 > 9
Barkhof F. Brain 1997;120:2059-69Tintore M. Am J Neuroradiol 2000;21:702-6 NP
Nine or more hyperintense

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 62/134
Nine or more hyperintense
lesions in T2 (or FLAIR)
FLAIR T2Wd NP Ann Neurol 2001;50:121-7
One Gd enhancing lesion

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 63/134
One Gd enhancing lesionin T1
T1W T1W c Gdd NP Ann Neurol 2001;50:121-7
At least one

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 64/134
At least one infratentorial lesion
d NP Ann Neurol 2001;50:121-7
At least one
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 65/134
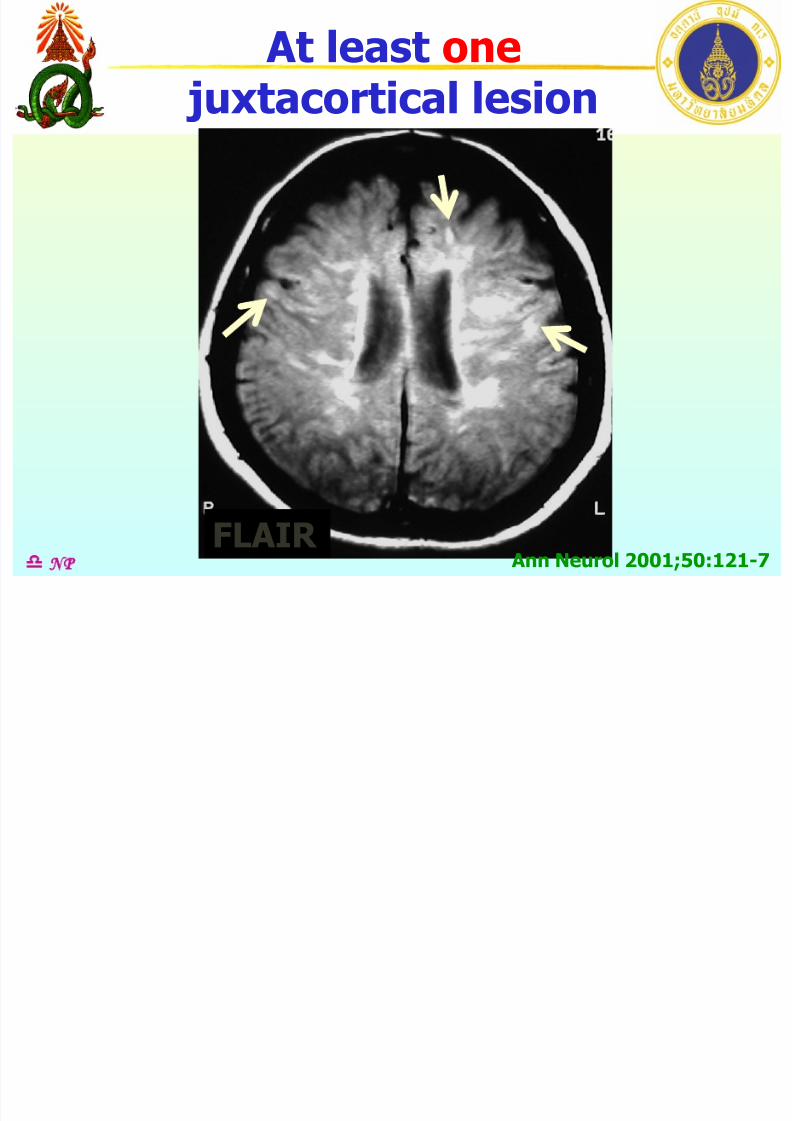
At least one juxtacortical lesion
FLAIR d NP Ann Neurol 2001;50:121-7
At least three

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 66/134
At least three periventricular lesions
FLAIR d NP Ann Neurol 2001;50:121-7
Multiple Sclerosis
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 67/134
Multiple SclerosisMRI Criteria
MRI criteria:• Dissemination in space
brain MRIspinal cord MRI
• Dissemination in time
Barkhof F. Brain 1997;120:2059-69Tintore M. Am J Neuroradiol 2000;21:702-6 NP
Multiple Sclerosis

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 68/134
Multiple SclerosisDissemination in Space
Spinal MRI criteria:• Little or no swelling of cord• T2 hyperintense lesions
- size > 3 mm- length < 2 vertebral segments- partial involvement of cord
(cross section)
d NP Ann Neurol 2001;50:121-7
MRI Criteria for

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 69/134
MRI Criteria for Dissemination in Space
or
3 in 4
2)
>1 Infra-tentorial
3)
>1 Juxta-cortical
4)
> 3 peri-ventricular
Gd+ lesion
1)
> 1 T2W lesions > 9 =
Note
Barkhof F. Brain 1997;120:2059-69Tintore M. Am J Neuroradiol 2000;21:702-6 NP
Little or no cord swelling

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 70/134
Little or no cord swelling
d NP
T1W w GdT2W
Ann Neurol 2001;50:121-7
T2W lesion > 3 mm

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 71/134
T2W lesion > 3 mm
d NP Ann Neurol 2001;50:121-7
T2W
Cervical cord
T2W T2W
Cervical cord
Length <2 vertebral

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 72/134
Length <2 vertebralbody segments
d NP Ann Neurol 2001;50:121-7
T1W w GdT2W
Partial involvement of cord

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 73/134
Partial involvement of cord
d NP Ann Neurol 2001;50:121-7
T2W T2W
Cervical cord
Multiple Sclerosis

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 74/134
Multiple SclerosisDissemination in Space
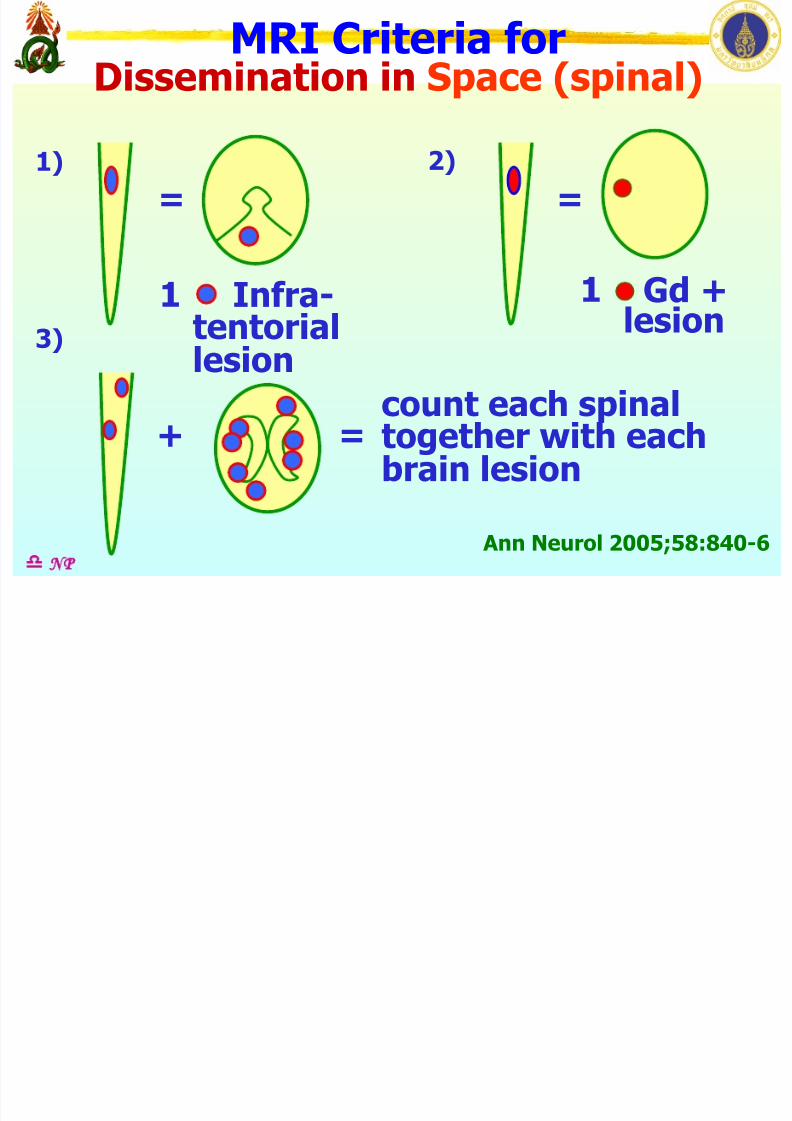
Spinal MRI criteria (revised):• A spinal lesion is equivalent to
a brain infratentorial lesion• An enhancing spinal lesion equals
to an enhancing brain lesion• Individual spinal lesions count
together with individual brain
lesions
d NP Ann Neurol 2005;58:840-6
MRI Criteria for
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 75/134
MRI Criteria for Dissemination in Space (spinal)
1)
3)
2)
count each spinaltogether with eachbrain lesion
Gd +lesion
1 = =
Infra-tentoriallesion
1
Ann Neurol 2005;58:840-6
+ =
d NP
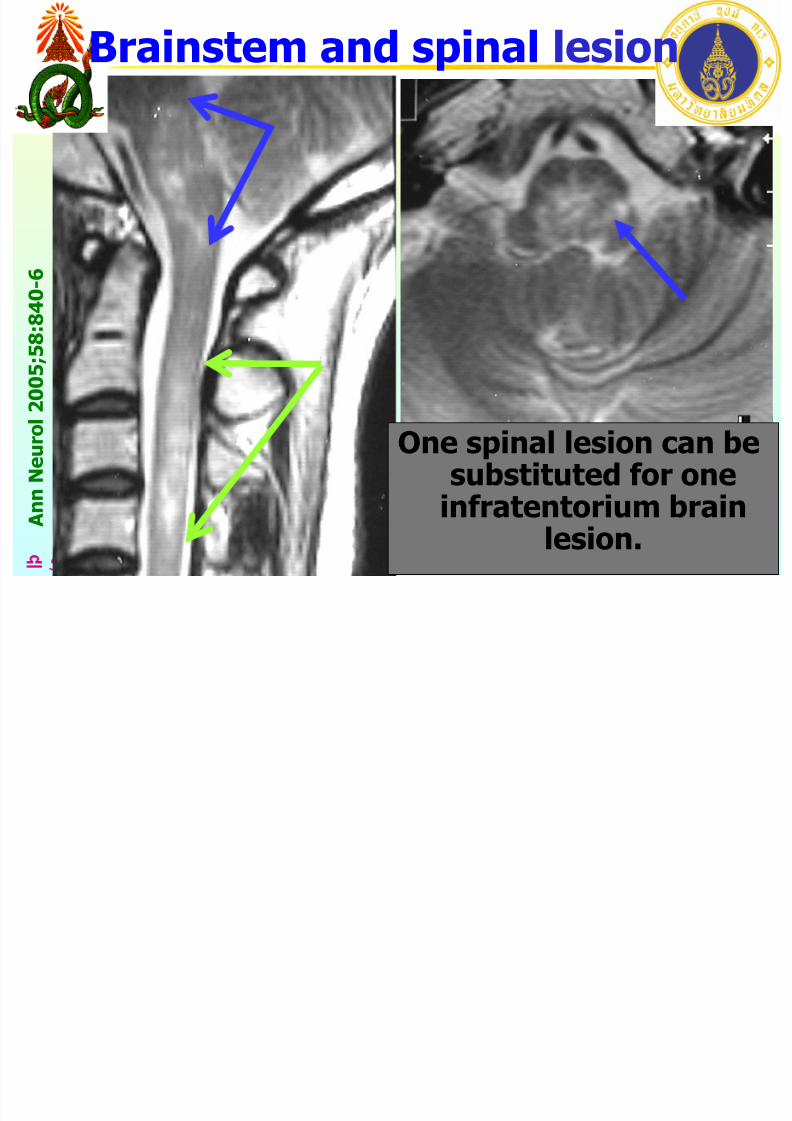
Brainstem and spinal lesion
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 76/134
d NP
T2W
One spinal lesion can besubstituted for one
infratentorium brain
lesion.
A n n
N e u r o l
2 0 0 5 ; 5 8 : 8 4 0 - 6
Brainstem and spinal lesion
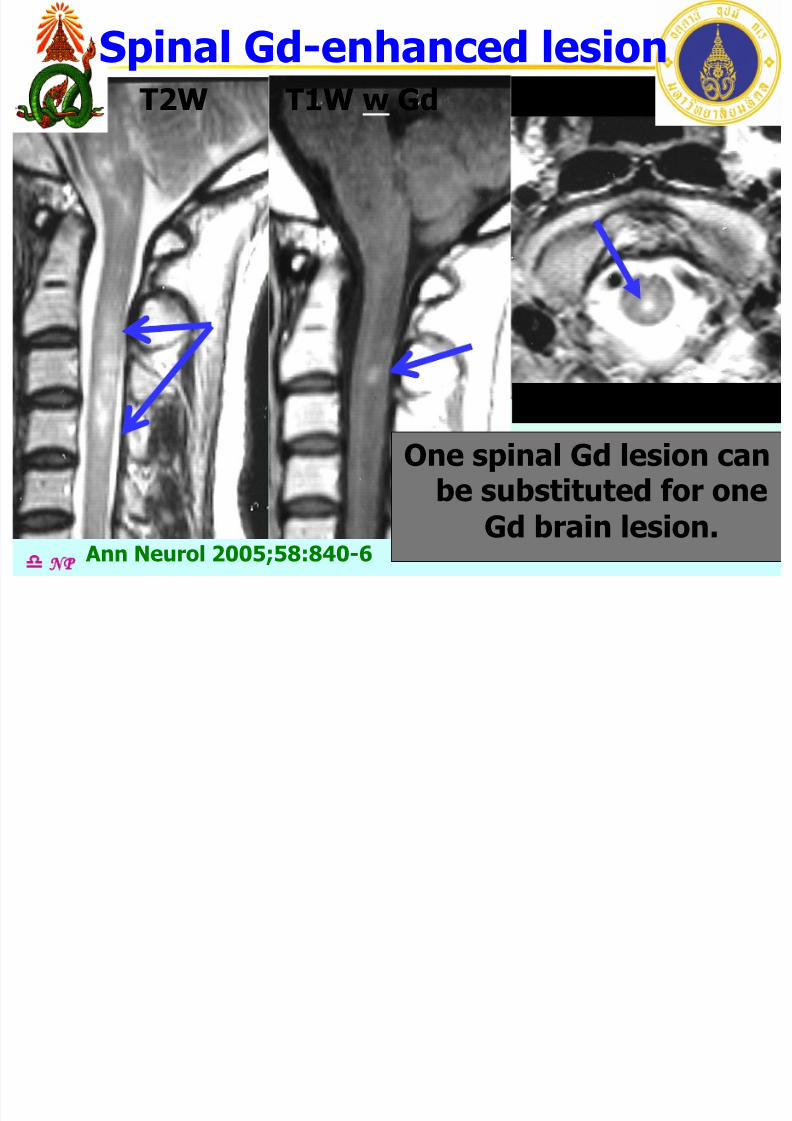
Spinal Gd-enhanced lesion
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 77/134
d NP
T1W w Gd T2WT2W
Cervical cordOne spinal Gd lesion can
be substituted for oneGd brain lesion.
Ann Neurol 2005;58:840-6
Spinal Gd enhanced lesion
Multiple Sclerosis

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 78/134
Multiple SclerosisMRI Criteria
MRI criteria:• Dissemination in space
brain MRIspinal cord MRI
• Dissemination in time
Barkhof F. Brain 1997;120:2059-69Tintore M. Am J Neuroradiol 2000;21:702-6 NP
Multiple Sclerosis

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 79/134
Multiple SclerosisDissemination in Time
a. 1st scan >3 mo of clinical onset:
d NP
• Gd positive lesions; not at the site
implicated in the original clinicalevent
Follow-up scan ~ 3 mo
• New T2 lesion• New Gd positive lesion
2001
Ann Neurol 2001;50:121-7
Multiple Sclerosis
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 80/134
Multiple SclerosisDissemination in Time
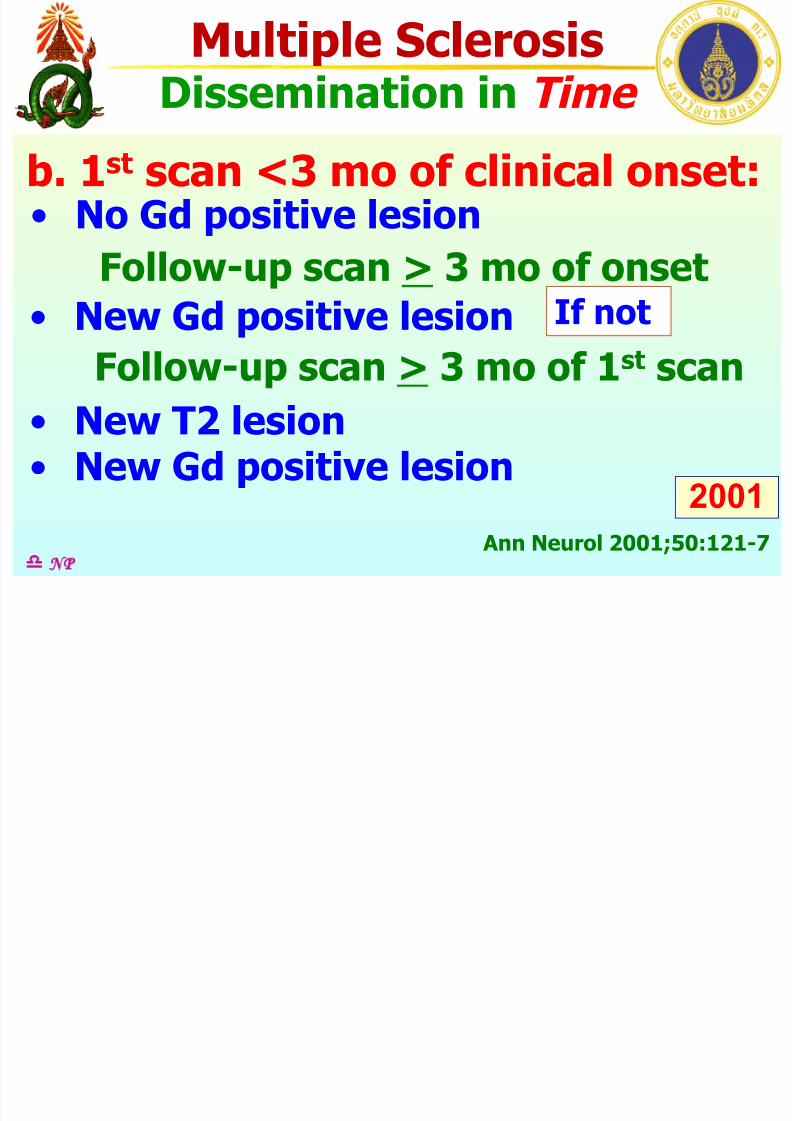
b. 1st scan <3 mo of clinical onset:
d NP
2001
Ann Neurol 2001;50:121-7
• No Gd positive lesion
Follow-up scan > 3 mo of onset• New Gd positive lesion If not
Follow-up scan > 3 mo of 1st scan
• New T2 lesion• New Gd positive lesion
MRI Criteria for

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 81/134
Dissemination in Time Clinical
event
Category 1 yes
yes
yesGd +veNew T2
3 months3 months
Ann Neurol 2001;50:121-7
2001
d NP
Multiple Sclerosis
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 82/134
p oDissemination in Time
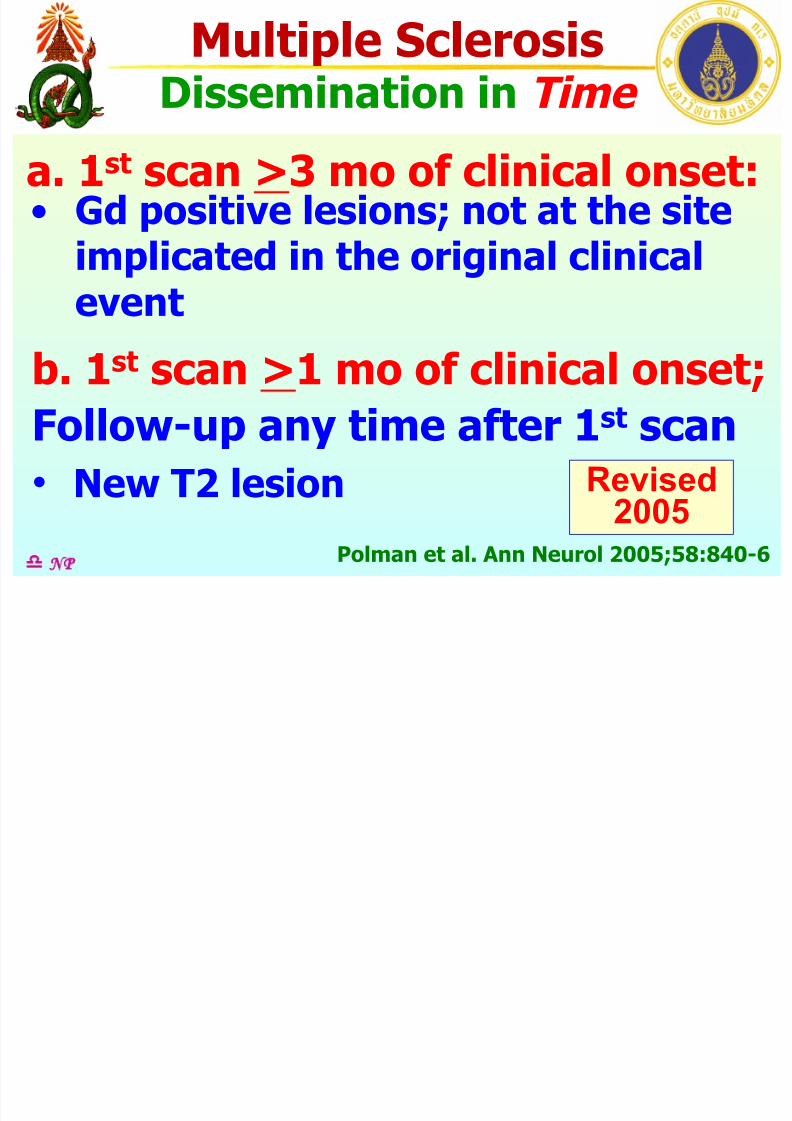
a. 1st scan >3 mo of clinical onset:
d NP
• Gd positive lesions; not at the siteimplicated in the original clinicalevent
b. 1st scan >1 mo of clinical onset;
Follow-up any time after 1st scan• New T2 lesion
Polman et al. Ann Neurol 2005;58:840-6
Revised2005
MRI Criteria for
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 83/134
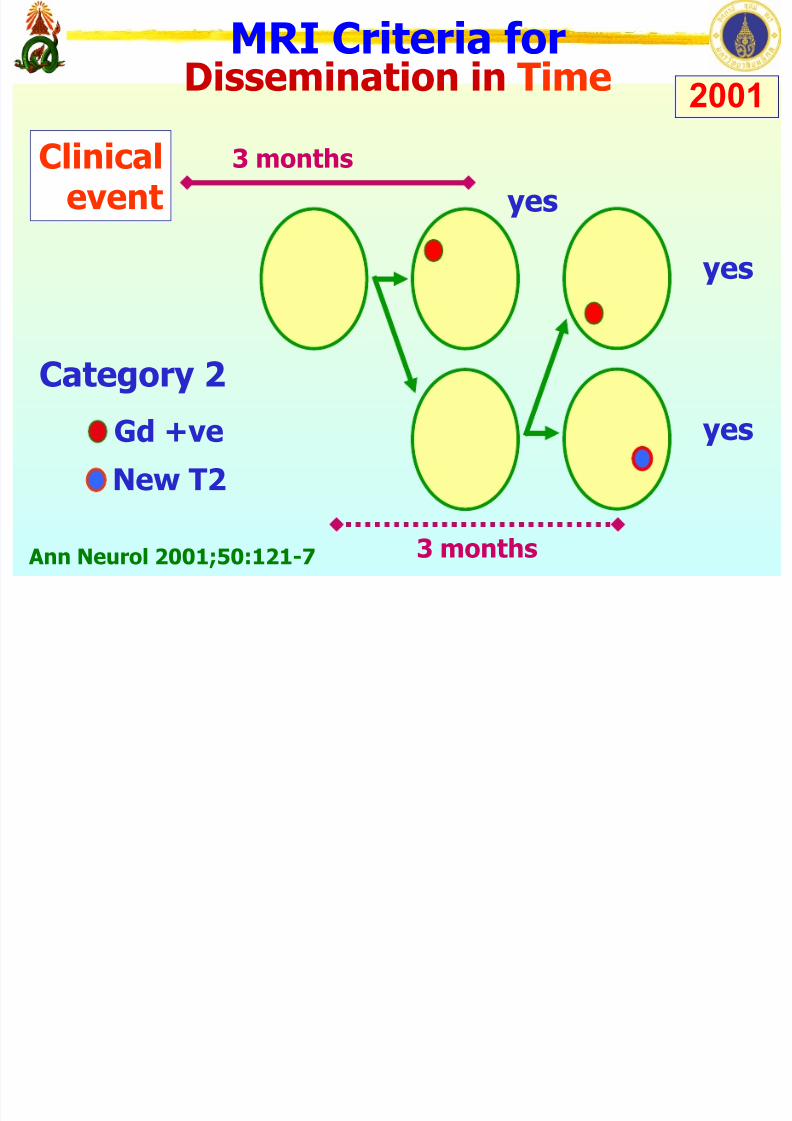
Dissemination in Time Clinical
event
Category 2
yes yes
yesGd +veNew T2
3 months
3 months
Ann Neurol 2001;50:121-7
2001
MRI Criteria for

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 84/134
Dissemination in Time clinicalevent 3 months 3 months
3 months
Category 1
Category 2
yes yes
yes
yes yes yes
Gd +veNew T2
Ann Neurol 2001;50:121-7
2001
d NP
MRI Criteria for
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 85/134
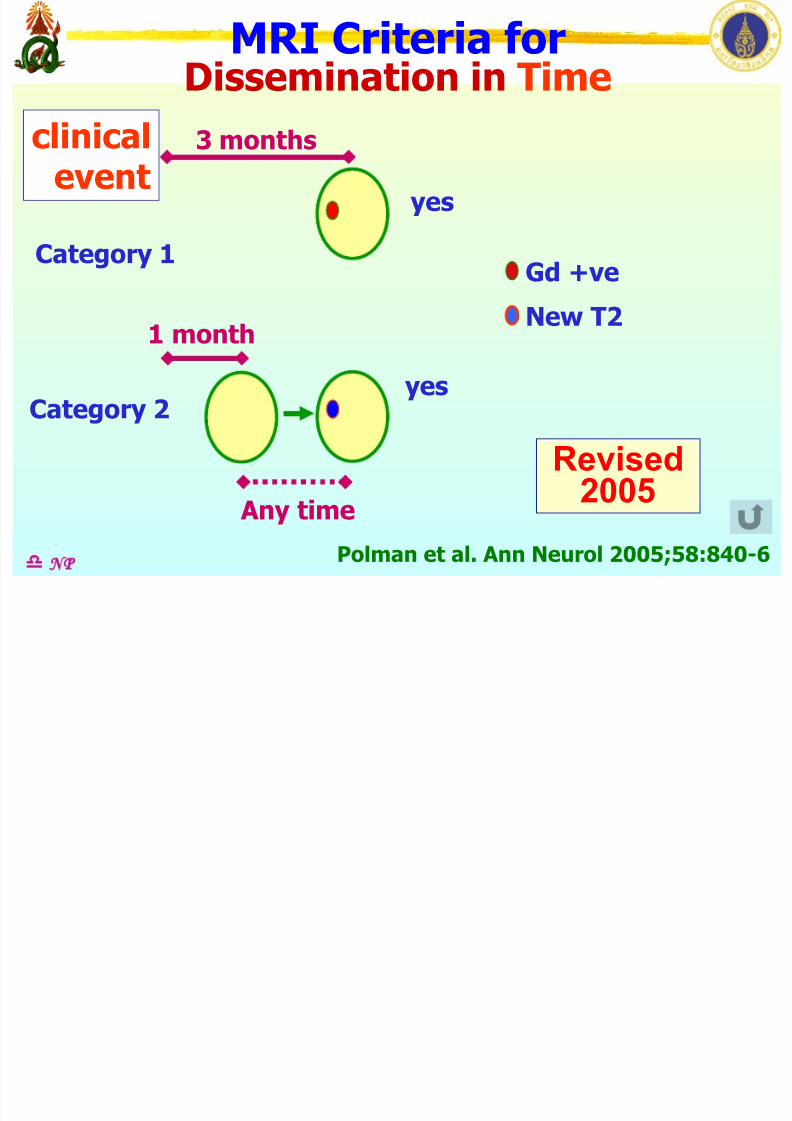
Dissemination in Time clinicalevent 3 months
1 monthCategory 1
Category 2
yes
yes
Gd +ve
New T2
Any timePolman et al. Ann Neurol 2005;58:840-6
Revised2005
d NP
Multiple Sclerosis
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 86/134
pInvestigation
• Magnetic resonance imaging
• Evoked potentials:
visual auditorysomatosensory motor
• CSF analysis
cell count IgG index
oligoclonal band
d NP
Multiple Sclerosis
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 87/134
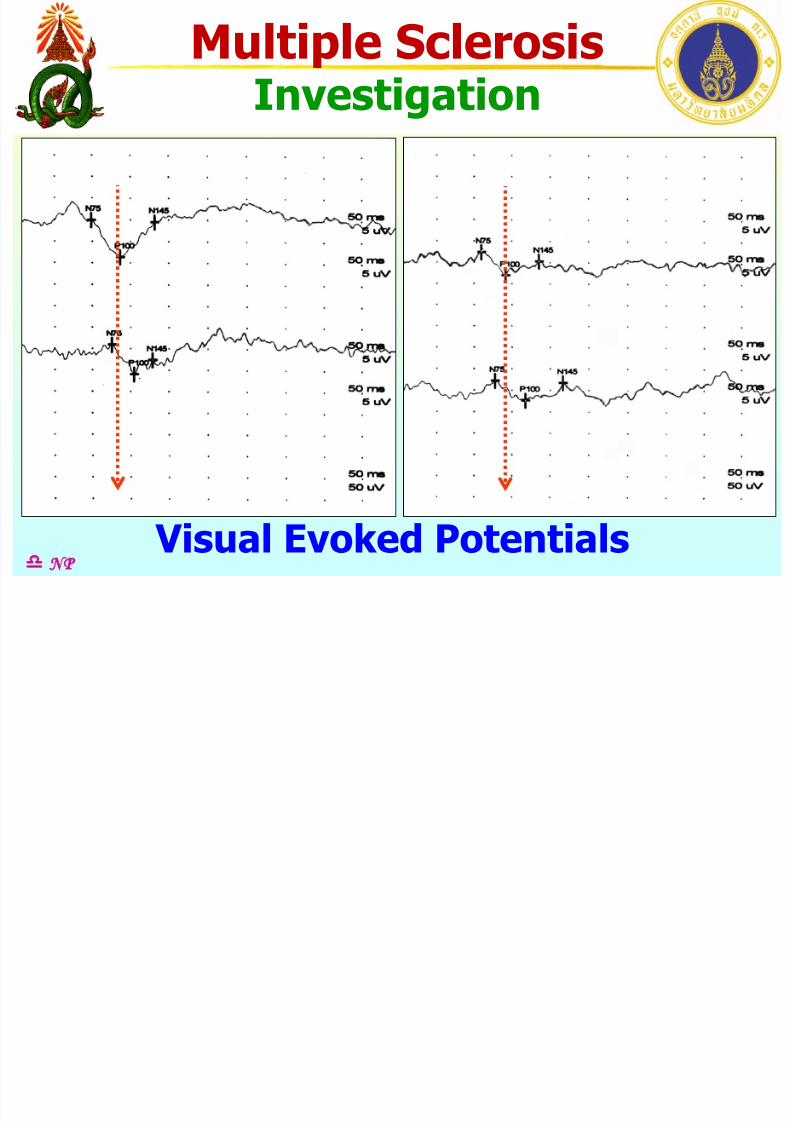
pInvestigation
d NP Visual Evoked Potentials
Multiple Sclerosis
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 88/134
pInvestigations
• Magnetic resonance imaging
• Evoked potentials:
visual auditorysomatosensory motor
• CSF analysis
cell count IgG index
oligoclonal band
d NP
Multiple Sclerosis

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 89/134
pInvestigation
d NP CSF oligoclonal bands
Serum
CSF
Serum: +CSF : ++
Serum: -
CSF : ++
Multiple SclerosisDi i C i i Revised
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 90/134
dNP
Diagnostic Criteria
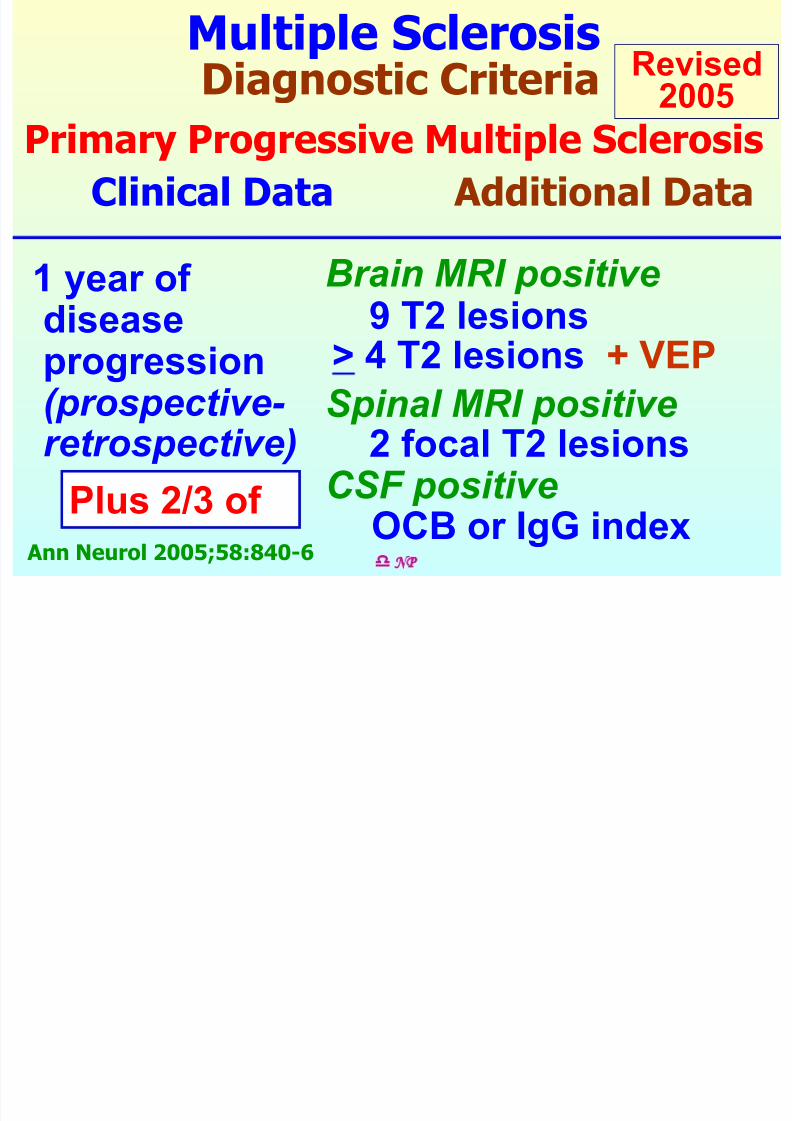
Primary Progressive Multiple SclerosisClinical Data Additional Data
Brain MRI positive1 year of diseaseprogression
(prospective- retrospective)
9 T2 lesions
Spinal MRI positive
> 4 T2 lesions + VEP
2 focal T2 lesionsCSF positive
Ann Neurol 2005;58:840-6
OCB or IgG indexPlus 2/3 of
Revised2005
Criteria: Primary Progressive MS

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 91/134
dNP
y g
Progressive course 1 y
T2W
9 2 >4 Ann Neurol 2005;58:840-6
Revised2005
Brain Spinal CSF
- Oligoclonal
bands
- IgG index
Plus 2/3 of
or + VEP
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 92/134
dNP
Differential Diagnosis
Multiple Sclerosis
Multiple Sclerosis
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 93/134
pDifferential Diagnosis
ADEM APL syndrome
SLE CNS vasculitis
Behcet’s disease 1o Sjogren syndrome
CADASIL Sarcoidosis
CNS infection: HIV, PML, SSPE, Lyme’s disease,
meningovascular syphilis, Whipple’s disease
Mitochondrial 1o CNS lymphomaencephalopathy
d NP
ADEM: acute demyelinating encephalomyelitis, APL: antiphospholipid, SLE: systemic lupuserythematosus, CNS: central nervous system, CADASIL: cerebral autosomal dominant arteriopathy
with subcortical infarcts and leucoencephalopathy, HIV: human immune deficiency virus, PML:
progressive multifocal leucoencephalopathy, SSPE: subacute sclerosing panencephalitis
Multiple Sclerosis
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 94/134
pDifferential Diagnosis
Tabes dorsalis
Familial ataxia
Subacute combined degeneration
(B12 deficiency)
Spinal cord tumor
Cervical spondylosis
d NP
Neuromyelitis Optica
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 95/134
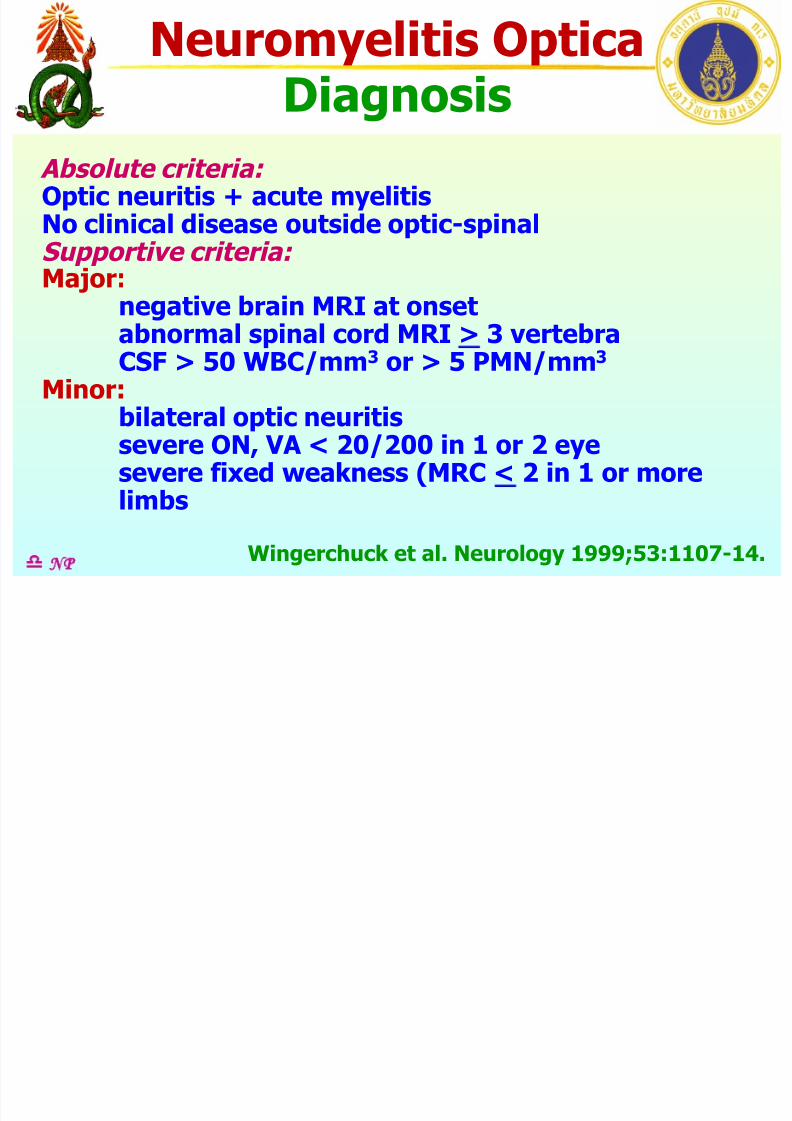
Diagnosis
Absolute criteria: Optic neuritis + acute myelitisNo clinical disease outside optic-spinalSupportive criteria:
Major: negative brain MRI at onsetabnormal spinal cord MRI > 3 vertebraCSF > 50 WBC/mm3 or > 5 PMN/mm3
Minor:
bilateral optic neuritissevere ON, VA < 20/200 in 1 or 2 eyesevere fixed weakness (MRC < 2 in 1 or morelimbs
d NP Wingerchuck et al. Neurology 1999;53:1107-14.
Neuromyelitis Optica
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 96/134
Diagnosis
Absolute criteria: Optic neuritis + acute myelitisNo clinical disease outside optic-spinalSupportive criteria:
Major: negative brain MRI at onsetabnormal spinal cord MRI > 3 vertebraCSF > 50 WBC/mm3 or > 5 PMN/mm3
Minor:
bilateral optic neuritissevere ON, VA < 20/200 in 1 or 2 eyesevere fixed weakness (MRC < 2 in 1 or morelimbs
d NP
Absolute criteria: Optic neuritis + acute myelitisNo clinical disease outside
optic-spinal
Supportive criteria: Major: negative brain MRI at onsetabnormal spinal MRI > 3 vertebra
CSF >50 WBC or >5 PMN per mm3
Supportive criteria: Minor: bilateral optic neuritis
severe ON, VA< 20/200 in 1 or 2 eyesevere fixed weakness (MRC < 2
in 1 or more limbs
Wingerchuck et al. Neurology 1999;53:1107-14.
Neuromyelitis Optica

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 97/134
Diagnosis
Definite NMO:
Optic neuritis
acute myelitis
Supportive criteria: 2 in 3Brain MRI not compatible with Barkhof’s criteria
Spinal MRI > 3 vertebral body segments
NMO IgG antibody positive
d NP Wingerchuck et al. Neurology 2006;66:1485-9.
Definite NMO: • Optic neuritis• acute myelitis
Supportive criteria: 2 in 3• Brain MRI not compatible with
Barkhof’s criteria
• Spinal MRI > 3 vertebral bodysegments
• NMO IgG antibody positive
Multiple Sclerosis

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 98/134
Multiple Sclerosis
Scope:
Clinical manifestations
PathologyPathogenesis
Diagnosis
Treatment
d NP

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 99/134
dNP
Treatment
Multiple Sclerosis
Multiple Sclerosis
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 100/134
Treatment
Acute relapses
Disease modifying therapies (DMT)
Symptom control
d NP
Multiple Sclerosis
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 101/134
Treatment
Acute relapses
Disease modifying therapies (DMT)
Symptom control
d NP

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 102/134
Multiple Sclerosis
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 103/134
Acute Relapses Rx
2. Plasma exchange
Rational: To remove circulating
autoantibodies, complimentsIndication: Severe steroid-resistant
relapses, neuromyelitis optica (NMO),
acute disseminated encephalomyelitis(ADEM) within 1 month of onset of
symptom
d NP Kieseier BC, et al. Curr Opion Neurol 2007;20:286-93
Multiple Sclerosis

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 104/134
Acute Relapses Rx
2. Plasma exchange
Rx: 1 plasma volume
7 exchanges alternate day
d NP Kieseier BC, et al. Curr Opion Neurol 2007;20:286-93
Multiple Sclerosis

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 105/134
Treatment
Acute relapses
Disease modifying therapies (DMT)
Symptom control
d NP
Multiple Sclerosis

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 106/134
Disease Modifying Therapy
Disease modifying therapies DMT
1. Interferon beta
2. Glatiramer acetate
3. Mitoxantrone
4. Monoclonal antibodies
5. Oral therapies
De Angelis T, Lublin F. Curr Opion Neurol 2007;20:261-71
Costello FC, Stuve O, Weber M, et al. Curr Opion Neurol 2007;20:281-5
Kieseier BC, Weindl H, Hemmer B, et al. Curr Opion Neurol 2007;20:286-93dNP
Multiple Sclerosis

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 107/134
Disease Modifying Therapy
1. Interferon beta IFN β
Mechanism: Anti-inflammatory effect by
- inhibit cytokine production- limit access of immune cell infiltration
to CNS
De Angelis T, Lublin F. Curr Opion Neurol 2007;20:261-71
Costello FC, Stuve O, Weber M, et al. Curr Opion Neurol 2007;20:281-5
Kieseier BC, Weindl H, Hemmer B, et al. Curr Opion Neurol 2007;20:286-93dNP
Multiple Sclerosis
f

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 108/134
Disease Modifying Therapy
De Angelis T, Lublin F. Curr Opion Neurol 2007;20:261-71
Costello FC, Stuve O, Weber M, et al. Curr Opion Neurol 2007;20:281-5
Kieseier BC, Weindl H, Hemmer B, et al. Curr Opion Neurol 2007;20:286-93dNP
IM: intramuscular, Sc: subcutaneous, wk: week, AD: alternate day
Type Drug Company µg Route Dose
IFN β 1a AvonexR Biogen Idec 30 IM 1/wk Rebif R Merck Serono 22, 44 Sc 3/wk
IFN β 1b BetaseronR Bayer Schering
Pharma
250 Sc AD
1. IFN β 1
Multiple Sclerosis
i dif i h
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 109/134
Disease Modifying Therapy
2. Glatiramer acetate (Copolymer-1)
Mechanism: Anti-inflammatory effect by
- induce changes in phenotypicexpression of T helper cell
- modify central effects of inflammation
De Angelis T, Lublin F. Curr Opion Neurol 2007;20:261-71
Costello FC, Stuve O, Weber M, et al. Curr Opion Neurol 2007;20:281-5
Kieseier BC, Weindl H, Hemmer B, et al. Curr Opion Neurol 2007;20:286-93dNP
Multiple Sclerosis
Di M dif i Th
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 110/134
Disease Modifying Therapy
3. Mitoxantrone
Mechanism:
- reduce Th1 cytokines- eliminate lymphocytes
Indication: SP MS, PR MS,
refractory RR MS
De Angelis T, Lublin F. Curr Opion Neurol 2007;20:261-71
Costello FC, Stuve O, Weber M, et al. Curr Opion Neurol 2007;20:281-5
Kieseier BC, Weindl H, Hemmer B, et al. Curr Opion Neurol 2007;20:286-93dNP
Multiple Sclerosis
Di M dif i Th
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 111/134
Disease Modifying Therapy
4. Monoclonal antibodies
Mechanism: Targeted therapies of
molecules involved in pathogenesis
De Angelis T, Lublin F. Curr Opion Neurol 2007;20:261-71
Costello FC, Stuve O, Weber M, et al. Curr Opion Neurol 2007;20:281-5
Kieseier BC, Weindl H, Hemmer B, et al. Curr Opion Neurol 2007;20:286-93dNP
Multiple Sclerosis
DMT M l l A tib d

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 112/134
DMT: Monoclonal Antibody
dNP
Type Drug Company Target
Natalizumab TysabriR Biogen Idec α-4 integrins
Alemtuzumab CampathR Bayer Schering
Pharma
CD52 NK, B cell
Rituximab MabTheraR Roche CD20 B cell
Daclizumab ZenapaxR Biogen Idec CD25, IL 2
De Angelis T, Lublin F. Curr Opion Neurol 2007;20:261-71
Costello FC, Stuve O, Weber M, et al. Curr Opion Neurol 2007;20:281-5
Kieseier BC, Weindl H, Hemmer B, et al. Curr Opion Neurol 2007;20:286-93
Multiple Sclerosis
Di M dif i Th

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 113/134
Disease Modifying Therapy
Disease modifying therapies DMT
1. Interferon beta
2. Glatiramer acetate
3. Mitoxantrone
4. Monoclonal antibodies
5. Oral therapies
De Angelis T, Lublin F. Curr Opion Neurol 2007;20:261-71
Costello FC, Stuve O, Weber M, et al. Curr Opion Neurol 2007;20:281-5
Kieseier BC, Weindl H, Hemmer B, et al. Curr Opion Neurol 2007;20:286-93dNP
Multiple Sclerosis
O l Th

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 114/134
Oral Therapy
5.1 Cladribine (Merck Serono)
5.2 Fingolimod (Novartis)
5.3 Fumaric acid ester (Biogen Idec)
5.4 Laquinimod (Teva Neurosci.)
5.5 Teriflunamide (Sanofi Aventis)
5.6 Glatiramer acetate (Teva Neurosci.)5.7 statin
De Angelis T, Lublin F. Curr Opion Neurol 2007;20:261-71
Costello FC, Stuve O, Weber M, et al. Curr Opion Neurol 2007;20:281-5
Kieseier BC, Weindl H, Hemmer B, et al. Curr Opion Neurol 2007;20:286-93dNP
Multiple SclerosisT t t
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 115/134
Treatment
Acute relapses
Disease modifying therapies (DMT)
Symptom control
d NP
Multiple SclerosisS t C t l
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 116/134
Symptom Control
Weakness
Spasticity
PainFatigue
Psychological disorders
d NP
Multiple SclerosisS t C t l

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 117/134
Symptom Control
Weakness
Rehabilitation:
increase strengthincrease endurance
d NP
Multiple SclerosisS t C t l
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 118/134
Symptom Control
Spasticity
Exercise
MassageCentral muscle relaxant:
baclofen, tizanidine
Botulinum toxin injection
d NP
Multiple SclerosisS t C t l

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 119/134
Symptom Control
Pain
neuropathic pain
- antidepressant: TCAs, SSRIs- anticonvulsant: carbamazepine,
gabapentin, oxcarbazepine,
pregabalin
NP
Multiple SclerosisS mptom Cont ol
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 120/134
Symptom Control
Pain
tonic spasm: spontaneous, action
- behavior adjustment: slow, steadymovement
- antidepressant: TCAs, SSRIs
- central muscle relaxant:
baclofen, tizanidine
NP
Multiple SclerosisSymptom Control

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 121/134
Symptom Control
Fatigue: feeling lack of ‘energy’
- not weakness or depressive mood
- improve with exercise- balance between rest and exercise
- keep cool while exercise
d NP
Multiple SclerosisSymptom Control
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 122/134
Symptom Control
Psychological disorders:
Depressive mood
- psychological support- antidepressant: TCAs, SSRI
Anxiety
- psychological support
- anxiolytic
NP
Multiple SclerosisTreatment
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 123/134
Treatment
Acute relapses
Disease modifying therapies (DMT)
Symptom control
d NP
Multiple Sclerosis
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 124/134
p
Scope:
Clinical manifestations
PathologyPathogenesis
Diagnosis
Treatment in MS
d NP
Case Presentation

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 125/134
Diagnosis: optic neuritisRx: high dose steroids
A young woman had dimmed
vision of the left eye for 2 days. Eyedrop tried without improvement.
d NP
Eye:
Vision got worse. Pain on eye
movement was noted.
Case Presentation
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 126/134
A young woman felt spinning for
a few days, getting worse withmotion. There was no hearing lossor visual blurring.
d NP
ENT:
Few days later she had double
vision, nystagmus and ataxia.MRI: brainstem lesion
Diagnosis: clinically isolated synd.Rx: high dose steroids
Case Presentation

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 127/134
A young woman difficulty in
voiding for 3 days.Urinalysis: WBC 3-5, RBC 5-10, fewbacteria
d NP
Urology:
One day later she developed
numbness and weakness of bothlegs.
LP: h WBC
MRI: intrinsic cord lesion T level
Diagnosis: acute myelitis
Case Presentation

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 128/134
A young woman had nausea and
vomiting for 5 days. He had veryfrequent hiccoughs for 1 day.
EGD: showed mild gastritis
d NP
Rx: iv methylprednisolone (MP)
GI:
Past history: visual loss (optic
neuritis) left eye
Case Presentation
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 129/134
A middle age woman had gait
difficulty 2-3 weeks. She could notproperly lift her feet above theground. There was some numbness
at the lower legs.
d NP
Diagnosis: lumbar spondylosisCT myelogram: disc herniation
Orthopedics:
Rx: laminectomy
Few months later she had bilateralvisual loss.
Dx: RR MS
Case Presentation

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 130/134
A middle age man experienced
itching at the anterior chest left sidefor 1 week. No rash was noted.
d NP
Diagnosis: dermatitisRx: topical steriods
Skin:
Few weeks later he had numbness
at the left chest down to the leftleg and weakness of both legs.
MRI: intrinsic cord lesionRx: IV MP
Case Presentation

8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 131/134
A middle age woman had
headache for 1-2 months. She couldnot do her routine work, was slow inresponse. Mild weakness was noted.
d NP
Inx: CT brain with contrast -massDiagnosis: brain tumor
Surgery:
Brain biopsy: chronic demyelination
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 132/134
dNP
MS
Q&A
Acute Optic NeuritisInvestigations
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 133/134
Investigations
1. Demonstrate the lesion
2. Look for other site involved
3. Look for other causes
d NP
Optic nerve MRI, VEPs Brain, whole cord MRI,
CSF oligoclonal bands Immune profile, (anti HIV)
Acute MyelitisInvestigations
8/6/2019 MS-KKU 24-09-2009
http://slidepdf.com/reader/full/ms-kku-24-09-2009 134/134
Investigations
1. Demonstrate the lesion
2. Look for other site involved
3. Look for other causes
Whole cord MRI
Brain MRI, VEPs, CSF
oligoclonal bands