BRIEF REPORT • CID 2010:51 (15 July) • e7
B R I E F R E P O R T
Successful Treatment of Balamuthiamandrillaris Amoebic Infectionwith Extensive Neurologicaland Cutaneous Involvement
Dalila Y. Martınez,1 Carlos Seas,1,2 Francisco Bravo,1,2 Pedro Legua,1,2
Cesar Ramos,2 Alfonso M. Cabello,1 and Eduardo Gotuzzo1,2
1Instituto de Medicina Tropical “Alexander von Humboldt,” Universidad PeruanaCayetano Heredia, and 2Departamento de Enfermedades Infecciosas, Tropicalesy Dermatologicas, Hospital Nacional Cayetano Heredia, Lima, Peru
Granulomatous amoebic encephalitis caused by Balamuthia
mandrillaris is an uncommon infection for which there is
no optimal therapy. We describe a young, female patient who
presented with extensive cutaneous and neurological involve-
ment and who recovered after receiving prolonged treatment
with miltefosine, fluconazole, and albendazole.
Balamuthia mandrillaris is a free-living amoeba that has been
recognized as an uncommon human pathogen since 1990 [1].
More than 150 cases of human encephalitis due to B. man-
drillaris have been reported worldwide; most have been re-
ported from Latin America and from the southwestern region
of the United States [2]. The disease induced by this amoeba
is characterized by involvement of the skin, especially around
the central face following a chronic course, with subsequent
extension to the central nervous system (CNS), where it causes
multifocal granulomatous encephalitis, leading almost invari-
ably to a fatal outcome [3–5].
No specific treatment is available to manage this lethal con-
dition. A number of antimicrobials (alone and in combination)
have been tried with unsuccessful results, including ampho-
tericin B, azoles, paromomycin, albendazole, pentamidine is-
ethionate, macrolides, metronidazole, sulfadiazine, and some
others [5–7]. However, 6 patients (4 in the United States and
2 in Peru) who presented with extensive CNS involvement
survived after receiving several antimicrobial regimens [4–6, 8].
We report, to our knowledge, the first successful treatment of
Received 22 December 2009; accepted 7 April 2010; electronically published 15 June 2010.Reprints or correspondence: Dr Dalila Y. Martınez, Universidad Peruana Cayetano Heredia,
Av. Honorio Delgado 430, Lima 31, Peru ([email protected]).
Clinical Infectious Diseases 2010; 51(2):e7–e11� 2010 by the Infectious Diseases Society of America. All rights reserved.1058-4838/2010/5102-00E1$15.00DOI: 10.1086/653609
a young patient with Balamuthia encephalitis with a combi-
nation regimen of miltefosine, fluconazole, and albendazole.
Case report. A 21-year-old woman presented in August
2006 with a long-term history of cutaneous lesions on her right
knee. Four years before admission, she had noticed several
papular, erythematous, and painless lesions that had appeared
2 weeks after a fall in front of her house. The lesions coalesced
to form a violaceus and indurate plaque covering the entire
right knee. Empirical therapy was started at another institution
with topical antifungal creams that contained fluconazole and
clotrimazole plus topical steroids, which were administered for
almost 1 year, followed by a combination of oral fluconazole
(150 mg per day for ∼45 days) and subsequent addition of
clarithromycin (1500 mg per day) and trimethoprim-sulfa-
methoxazole (TMP-SMX; 320 mg/1600 mg per day) for 8
months, without improvement.
The patient was born in Lima, Peru, and has resided there
for her entire life. She denied travel or specific occupational
exposure, including gardening and swimming in brackish, fresh,
or sea water. She noticed enlargement of the lesion on the right
knee and the appearance of 3 new papular lesions—2 of them
around the plaque on the right knee, and the third on the left
thigh—in February 2006. Both lesions subsequently evolved
into violaceus plaques. She was first seen at our institution 4
months later, where a skin biopsy of the lesion on the right
knee was performed (Figure 1A). Histopathologic examination
revealed a dense inflammatory infiltrate of the dermis com-
posed of lymphocytes, plasma cells, and ill-defined granulomas,
with great number of multinucleated giant cells located inside
and outside the granulomas. A microorganism with a nucleus
that has a large, central karyosome and a vacuolated cytoplasm,
compatible with an amoebic trophozoite, was observed (Figure
1B). In addition, B. mandrillaris was isolated from a skin sample
cultivated in an axenic culture prepared with monkey kidney
cells [7]. Polymerase chain reaction of a skin sample also yielded
positive results for B. mandrillaris (the amplification was per-
formed using the primer mitochondrial 16S rRNA gene from
B. mandrillaris as a target) [9]. A skin biopsy sample was sent
to the Public Health Department of California (Sacramento)
and to the Centers for Disease Control and Prevention (Atlanta,
GA), where B. mandrillaris infection was confirmed by im-
munohistochemical staining in September 2006. A brain com-
puted tomograph, without contrast enhancement, yielded nor-
mal findings at this time. Empirical therapy was started with
itraconazole (200 mg per day), and albendazole (400 mg per
day).
by guest on September 26, 2013
http://cid.oxfordjournals.org/D
ownloaded from
by guest on Septem
ber 26, 2013http://cid.oxfordjournals.org/
Dow
nloaded from
by guest on September 26, 2013
http://cid.oxfordjournals.org/D
ownloaded from
by guest on Septem
ber 26, 2013http://cid.oxfordjournals.org/
Dow
nloaded from
by guest on September 26, 2013
http://cid.oxfordjournals.org/D
ownloaded from

e8 • CID 2010:51 (15 July) • BRIEF REPORT
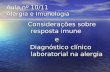
Figure. 1. A, Cutaneous lesion on the right knee observed in February 2006 showing an indurated and violaceous plaque covering the entire kneewith 2 papular lesions. B, Skin biopsy specimen showing a dense inflammatory infiltrate of the dermis with granulomas (hematoxylin and eoisin stain).An amoebic trophozoite is observed, with a nucleus that has a large, central karyosome and vacuolated cytoplasm. C, Fluid-attenuated inversionrecovery (FLAIR) magnetic resonance image (MRI) obtained 7 days after the onset of neurologic symptoms (June 2007) showing hypersignal in theleft temporal lobe. D, Axial gadolinium-enhanced T1-weighted sequence (June 2007) showing a ring-enhancing lesion in the left temporal lobe. E,Follow-up of the left knee lesion 1 week after the patient had commenced treatment with miltefosine, albendazole, and fluconazole. The lesionsabruptly changed, developing a scaly and crusty surface. F, Axial gadolinium-enhanced MRI obtained 5 months after the start of treatment, showingsignificant improvement on the neurological lesions without evidence of contrast enhancing. G, Gadolinium-enhanced MRI image 4 months aftercompletion of treatment, showing the disappearance of the brain lesions. H, Follow-up of the healed left knee lesions (May 2008).
The enlargement of the lesions continued despite medical
treatment, and the patient was hospitalized in October 2006 to
receive amphotericin B (cumulative dose, 1.5 g), in addition
to itraconazole and albendazole. The lesions improved initially,
but reactivation of the lesion on the left thigh and the ap-
pearance of 2 new small papular lesions (one on the left breast
and the other one on her back) were observed in February
2007. Biopsy of the lesion on the back was performed; the
biopsy findings were the same as described above. A surgical
resection of the new lesions was performed, and TMP-SMX
(320 mg/1600 mg by day) was added to the treatment regimen,
without improvement.
The patient was readmitted to the hospital in May 2007
because of reactivation of the lesion on the surgical wound on

Tabl
e.1.
Dem
ogra
phic
Char
acte
ristic
s,Cl
inic
alD
ata,
and
Ther
apeu
ticRe
gim
ens
for
7Su
rviv
ors
ofB
alam
uthi
am
andr
illar
isIn
fect
ion
Pat
ient
Age
,ye
ars
Sex
Reg
ion
Type
ofle
sion
(s)
Trea
tmen
tre
gim
enO
utco
me
Dur
atio
nof
follo
w-u
pR
efer
ence
164
MC
alifo
rnia
Ski
n:ra
ised
lesi
onon
the
right
fore
arm
;C
NS
:4
ring-
enha
ncin
gle
sion
s(p
arie
tala
ndoc
cipi
tal
lobe
s)
Fluc
ytos
ine
(8g
per
day)
,flu
cona
zole
(400
mg
per
day)
,an
dsu
lfadi
azin
e(6
gpe
rda
y)fo
r5
year
s;cl
arith
rom
y-ci
n(5
00m
gpe
rda
y)fo
r2
year
s;an
dpe
ntam
idin
eis
e-th
iona
te(4
mg/
kgpe
rda
y)an
dtr
ifluo
pera
zine
(20
mg
per
day)
for
18da
ys
Per
form
ing
alla
ctiv
ities
ofda
ilyliv
ing,
with
good
com
mun
icat
ion
skill
s5
year
s[5
]
25
FC
alifo
rnia
CN
S:
2rin
g-en
hanc
ing
le-
sion
s(t
empo
rala
ndpa
-rie
tall
obes
)
Fluc
ytos
ine
(110
mg/
kgpe
rda
y)an
dflu
cona
zole
(4m
g/kg
per
day)
for
2.4
year
s;pe
ntam
idin
eis
ethi
onat
e(1
mg/
kgpe
rda
y)fo
r34
days
;cl
arith
rom
ycin
(14
mg/
kgpe
rda
y)fo
r2.
4ye
ars;
and
thio
ridaz
ina
(1m
g/kg
per
day)
for
1.8
year
s
Typi
cals
choo
lper
form
ance
,w
ithou
tgr
oss
neur
olog
icse
quel
a2.
4ye
ars
[5]
372
FN
ewYo
rkC
NS
:2
ring-
enha
ncin
gle
-si
ons
(fro
ntal
and
tem
-po
rall
obes
)
Fluc
onaz
ole
(400
mg
per
day)
,su
lfadi
azin
e(6
gpe
rda
y),
clar
ithro
myc
in(1
500
mg
per
day)
,an
dpe
ntam
idin
eis
ethi
onat
e(3
00m
gpe
rda
y);
dura
tion
ofth
erap
yis
unkn
own
No
sign
ifica
ntne
urol
ogic
alse
quel
a6
mon
ths
[6]
435
MC
alifo
rnia
CN
S:
foca
lenh
anci
ngle
sion
sN
AA
live
and
ingo
odco
nditi
ons
3m
onth
s[8
]
58
MP
iura
,P
eru
Ski
n:la
rge
plaq
ueon
the
cent
ralf
ace;
CN
S:
mul
ti-pl
efo
call
esio
ns(b
oth
hem
isph
eres
)
Alb
enda
zole
(400
mg
per
day)
and
itrac
onaz
ole
(200
mg
per
day)
for
14m
onth
sS
kin
and
CN
Sle
sion
she
aled
;be
low
-ave
r-ag
eto
aver
age
scho
olpe
rfor
man
ce;
mild
left
hem
ipar
esis
3ye
ars
[4]
610
FP
iura
,P
eru
Ski
n:la
rge
plaq
ueon
the
cent
ralf
ace;
CN
S:
2rin
g-en
hanc
ing
lesi
ons
(rig
htfr
onta
llob
e)
Alb
enda
zole
(600
mg
per
day)
,itr
acon
azol
e(1
00m
gpe
rda
y),
and
TMP
-SM
X(3
20m
g/16
00m
gpe
rda
y)fo
r6
mon
ths;
surg
ical
rese
ctio
n
No
neur
olog
ical
sequ
elae
18m
onth
s[4
]
721
FLi
ma,
Per
uS
kin:
mul
tiple
plaq
ues
(rig
htkn
ee,
left
thig
h,br
east
,an
dba
ck);
CN
S:
1en
hanc
ing
lesi
on(t
empo
rall
obe)
Itra
cona
zole
(200
mg
per
day)
and
albe
ndaz
ole
(400
mg
per
day)
for
10m
onth
s;am
phot
eric
inB
(cum
ulat
ive
dose
,1.
50g)
was
adde
dw
ithou
tim
prov
emen
t;TM
P-
SM
X(3
20m
g/16
00m
gpe
rda
y)w
asad
ded
for
3m
onth
s;su
rgic
alre
sect
ion
ofsm
alll
esio
nsw
ithpo
ste-
rior
reac
tivat
ion;
anad
ditio
nalc
ours
eof
amph
oter
icin
B(c
umul
ativ
edo
se,
1.35
g),
itrac
onaz
ole
(300
mg
per
day)
,TM
P-S
MX
(640
mg/
3200
mg
per
day)
and
albe
n-da
zole
(800
mg
per
day)
was
give
nfo
r45
days
and
did
not
yiel
dim
prov
emen
t;cl
arith
rom
ycin
(150
0m
gpe
rda
y)an
dar
tesu
nate
(100
mg
per
day)
wer
ead
ded
for
2w
eeks
,w
ithou
tim
prov
emen
t,an
d1
CN
Sle
sion
appe
ared
inth
ebr
ain
MR
I;th
erap
yw
asch
ange
dto
al-
bend
azol
e(8
00m
gpe
rda
y)an
dflu
cona
zole
(450
mg
per
day)
for
7.5
mon
ths,
asw
ella
sm
iltef
osin
e(1
50m
gpe
rda
yfo
r12
days
,fo
llow
edby
100
mg
per
day
for
7m
onth
s),
atw
hich
time
skin
and
CN
Sle
sion
she
aled
Ski
nan
dC
NS
lesi
ons
heal
ed30
mon
ths,
incl
udin
g12
with
out
ther
apy
and
nore
curr
ence
PR
NO
TE
.C
NS
,ce
ntra
lner
vous
syst
em(c
onfir
med
byM
RI);
MR
I,m
agne
ticre
sona
nce
imag
ing;
NA
,no
tav
aila
ble;
PR
,pr
esen
tre
port
;TM
P-S
MX
,tr
imet
hopr
im-s
ulfa
met
hoxa
zole
.

e10 • CID 2010:51 (15 July) • BRIEF REPORT
the left thigh. A second course of amphotericin B was started
(cumulative dose, 1.350 g), in addition to an oral regimen of
itraconazole (300 mg per day), albendazole (800 mg per day),
and TMP-SMX (640 mg/3200 mg per day), for 1 month with-
out improvement. In June 2007, clarithromycin (1500 mg per
day) and oral artesunate (100 mg per day) were added to the
regimen. At this time, the patient developed fever, headache,
and childish behavior, with no other neurologic complaints.
The results of serological tests for human immunodeficiency
virus and human T lymphotropic virus–1 were negative. Mag-
netic resonance imaging of the brain performed 7 days after
the beginning of neurologic symptoms demonstrated hyper-
signal in the left temporal lobe in the fluid-attenuated inversion
recovery (FLAIR) sequence and a ring-enhancement lesion with
gadolinium in the temporal lobe (Figure 1C and 1D). Treatment
with amphotericin B, TMP-SMX, clarithromycin, and artesu-
nate was discontinued; itraconazole was changed to fluconazole
to optimize the penetration of the azole into the CNS; alben-
dazole treatment was continued, and oral miltefosine (150 mg
per day for 12 days and 100 mg per day thereafter) was added
in mid-June 2007. The cutaneous lesions on the knee abruptly
changed, developing a scaly, crusty surface (Figure 1E 1 week
after the patient started this regimen. The headache disappeared
by the second week of this regimen, and fever waned by the
fourth week. The skin lesion improved, becoming less scaly and
flat, until it eventually disappeared. The patient did well, with
regression of all neurological symptoms. She was discharged
home with the prescribed antibiotics in August 2007.
Significant improvement on the size of the neurological le-
sions was documented after 5 months of treatment (Figure 1F).
The patient continued to take miltefosine, albendazole, and
fluconazole for 7 months. The intracerebral lesions disappeared,
as documented by magnetic resonance imaging performed in
May 2008 (Figure 1G). She remains asymptomatic, all cuta-
neous lesions have healed (Figure 1H), and no recurrence has
been recognized as of May 2010.
Discussion. Since the first report of a Balamuthia man-
drillaris amoebic infection affecting a baboon in the San Diego
Wild Animal Park in 1986 [1], 1100 human cases have been
reported worldwide, with only 6 survivors [4–8]. In 2003, Deetz
et al [5] described 2 patients with extensive CNS involvement
who responded to a prolonged treatment regimen (up to 5
years) that included fluocytosine, pentamidine isethionate, flu-
conazole, sulfadiazine, and a macrolide. A third patient with
CNS involvement who responded to a regimen similar to the
one described above, but without fluocytosine, was described
by Jung et al [6]. A fourth patient from the California En-
cephalitis Project (CEP) was reported alive and in good health
condition three months after diagnosis, details about his treat-
ment were not provided however [8]. Two additional Peruvian
patients survived this infection: one patient with CNS involve-
ment survived long-term therapy (6 months) with albendazole
and itraconazole, and another patient, who demonstrated cu-
taneous involvement alone, was treated with surgical resection
plus a combination of itraconazole, albendazole and ampho-
tericin B (cumulative dose, 2 g) [3, 4]. A description of the 7
patients who survived Balamuthia infection of the CNS, in-
cluding the patient in our study, is presented in Table 1.
Very few drugs have shown in vitro amebicidal activity
against B. mandrillaris, including miltefosine [10], propami-
dine, and gramicidin S [7]. The amebicidal activity was dem-
onstrated by drug efficacy test using axenic cultures inoculated
in tissue culture flasks with growing concentrations of anti-
microbials. Most of the available drugs are amebistatic: phe-
nothiazine compounds, pentamidine isethionate, macrolides,
azoles, TMP-SMX, and amphotericin B [7]. In addition, B.
mandrillaris escapes the effect of antimicrobials by encysting in
tissues, establishing chronic infections that may reactivate later
[11]. Use of amebicidal drugs for treating this condition may
not only kill trophozoites in active lesions, but may also prevent
the further dissemination of the infection to the CNS and other
organs, which has been invariably observed when amebistatic
drugs are used.
Miltefosine is an alkylphosphocholine compound originally
developed as an anticancer drug, which is now established as
an effective anti-leishmanial therapy. It acts on key enzymes
involved in phospholipid and sterol biosynthesis, suggesting
that the cell membrane is its main target [12]. In vitro, it
stimulates T cells and macrophages to secrete activating cyto-
kines, including interferon-g, and induces production of mi-
crobicidal reactive nitrogen and oxygen intermediates, caus-
ing cell death by an apoptosis-like effect [13]. A recent report
showed good in vitro activity of miltefosine against Balamuthia,
Acanthamoeba, and Naegleria species [10]. Miltefosine achieves
a high concentration of the active drug in the brain tissue as
a result of excellent passage through the brain-blood barrier.
In addition, miltefosine carries an acceptable safety profile [10].
This is a potentially critical property of any drug to be successful
in treating CNS involvement by free-living amebas.
Although the prognosis of amebic encephalitis caused by B.
mandrillaris is still ominous, it may not be invariably fatal. This
report on the successful use of a combination regimen that
includes 1 amebicidal drug (miltefosine) along with 2 amebi-
static drugs capable of crossing the brain-blood barrier (flu-
conazole and albendazole) provides hope for attaining clinical
cure for an otherwise lethal condition. More clinical experience
is needed before miltefosine can be recommended as the de-
finitive first-line treatment for amebic encephalitis.
Acknowledgments
We thank the Dermatology staff of the Hospital Nacional CayetanoHeredia for their assistance in the diagnosis and follow-up of the patient.We specially thank Dr Juan Cabrera (Universidad Peruana Cayetano He-

BRIEF REPORT • CID 2010:51 (15 July) • e11
redia) for his advice in this case and permanent inspiration. Sadly, DrCabrera passed away on 25 May 2009.
Potential conflicts of interest. C.S. has received recent research fundingfrom Schering-Plough and has served on the speakers’ bureau for Pfizer.All other authors: no conflicts.
References
1. Visvesvara GS, Martinez A, Schuster FL, et al. Leptomyxid ameba, anew agent of amebic meningoencephalitis in humans and animals. JClin Microbiol 1990; 28:2750–2756.
2. Matin A, Siddiqui R, Jayasekera S, Khan NA. Increasing Importanceof Balamuthia mandrillaris. Clin Microbiol Rev 2008; 21:435–448.
3. Bravo FG, Cabrera J, Gotuzzo E. Cutaneous manifestations of infectionby free living amebas, with special emphasis on Balamuthia mandril-laris. In: Tyring SK, Lupi O, Henage UR, eds. Tropical dermatology.Philadelphia: Churchill Livingstone, 2005:49–56.
4. Seas C, Bravo FG. Encefalitis amebiana granulomatosa por Balamuthiamandrillaris: una enfermedad fatal reconocida cada vez mas frecuen-temente en America Latina. Rev Chil Infect 2006; 23:197–199.
5. Deetz TR, Sawyer MH, Billman G, et al. Successful treatment of Bal-amuthia amoebic encephalitis: presentation of 2 cases. Clin Infect Dis2003; 37:1304–1312.
6. Jung S, Schelper RL, Visvesvara GS, Chang HT. Balamuthia mandrillarismeningoencephalitis in an immunocompetent patient. an unusual clin-
ical course and a favorable outcome. Arch Pathol Lab Med 2004; 128:466–468.
7. Schuster FL, Visvesvara GS. Axenic growth and drug sensitivity studiesof Balamuthia mandrillaris, an agent of amebic meningoencephalitisin humans and other animals. J Clin Microbiol 1996; 34:385–388.
8. Centers for Disease Control and Prevention. Balamuthia amebic en-cephalitis—California 1999- 2007. MMWR Morb Mortal Wkly Rep2008; 57:768–771.
9. Booton, GC, Carmichael JR, Visvesvara GS, et al. Identification ofBalamuthia mandrillaris by PCR assay using the mitochondrial 16SrRNA gene as a target. J Clin Microbiol 2003; 41:453–455.
10. Schuster FL, Guglielmob ABJ, Visvesvara GS. In-vitro activity of mil-tefosine and voriconazole on clinical isolates of free-living amebas:Balamuthia mandrillaris, Acanthamoeba spp., and Naegleria fowleri. JEukaryot Microbiol 2006; 53:121–126.
11. Siddiqui R, Matin A, Warhurst D, et al. Effect of antimicrobial com-pounds on Balamuthia mandrillaris encystment and human brain mi-crovascular endothelial cell cytopathogenicity. Antimicrob Agents Che-mother 2007; 51:4471–4473.
12. Walochnik J, Duchene M, Seifert K, et al. Cytotoxic activity of alkyl-phosphocholines against clinical isolates of Acanthamoeba spp. Anti-microb Agents Chemother 2002; 46:695–701.
13. Verma NK, Dey CS. Possible mechanism of miltefosine mediated deathof Leishmania donovani. Antimicrob Agents Chemother 2004; 48:3010–3015.