HEAD CT SCAN Dr. Risda Fitriyani

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

8/10/2019 Head Ct Koass Ri
http://slidepdf.com/reader/full/head-ct-koass-ri 1/35
HEAD CT SCAN Dr. Risda Fitriyani

8/10/2019 Head Ct Koass Ri
http://slidepdf.com/reader/full/head-ct-koass-ri 2/35
ANATOMY

8/10/2019 Head Ct Koass Ri
http://slidepdf.com/reader/full/head-ct-koass-ri 3/35

8/10/2019 Head Ct Koass Ri
http://slidepdf.com/reader/full/head-ct-koass-ri 4/35

8/10/2019 Head Ct Koass Ri
http://slidepdf.com/reader/full/head-ct-koass-ri 5/35

8/10/2019 Head Ct Koass Ri
http://slidepdf.com/reader/full/head-ct-koass-ri 6/35
VASCULAR
SUPPLY

8/10/2019 Head Ct Koass Ri
http://slidepdf.com/reader/full/head-ct-koass-ri 7/35
Ekspertise CT scan kepala noral (yang dinilai pada CT scan kepala)
• Tak tampak lesi hipodens maupun hiperdens padaintrakranial
• Differensiasi substantia alba dan grisea tampak normal
• Sulkus kortikalis dan fissura sylvii kanan kiri normal
• Ventrikel lateralis kanan kiri, III dan IV tampak normal• Cisterna perimescecephalic tampak normal
• Tak tampak midline shifting
• Pons dan cerebellum tampak normal
!S"# $• TAK TAMPAK INFARK, PERDARAHAN MAPN !O" PADA
INTRAKRANIA"
• TAK TAMPAK TANDA#TANDA PENIN$KATAN TEKANAN INTRAKRANIA"

8/10/2019 Head Ct Koass Ri
http://slidepdf.com/reader/full/head-ct-koass-ri 8/35
CT CR!SS"SECT#!NAL ANAT!$Y

8/10/2019 Head Ct Koass Ri
http://slidepdf.com/reader/full/head-ct-koass-ri 9/35
• Cerebral hemispher separated by falk cerebri % interhemispheric fissure
• &ray matter appears lighter $ 'hite matter
• Centrum semiovale ( hemispheric subcortical 'hite matter

8/10/2019 Head Ct Koass Ri
http://slidepdf.com/reader/full/head-ct-koass-ri 10/35
The slice sho's the bodies of the lateral ventricles,
'hich appear as paired crescent)shaped CS*
spaces +t'in bananas-.

8/10/2019 Head Ct Koass Ri
http://slidepdf.com/reader/full/head-ct-koass-ri 11/35

8/10/2019 Head Ct Koass Ri
http://slidepdf.com/reader/full/head-ct-koass-ri 12/35

8/10/2019 Head Ct Koass Ri
http://slidepdf.com/reader/full/head-ct-koass-ri 13/35

8/10/2019 Head Ct Koass Ri
http://slidepdf.com/reader/full/head-ct-koass-ri 14/35

8/10/2019 Head Ct Koass Ri
http://slidepdf.com/reader/full/head-ct-koass-ri 15/35

8/10/2019 Head Ct Koass Ri
http://slidepdf.com/reader/full/head-ct-koass-ri 16/35

8/10/2019 Head Ct Koass Ri
http://slidepdf.com/reader/full/head-ct-koass-ri 17/35
Head CT A%&i'ac&s

8/10/2019 Head Ct Koass Ri
http://slidepdf.com/reader/full/head-ct-koass-ri 18/35
CT Ce''icien&s ' #%ay A&&en*a&in in
H*ns'ield ni&s

8/10/2019 Head Ct Koass Ri
http://slidepdf.com/reader/full/head-ct-koass-ri 19/35
HEAD TRAMA

8/10/2019 Head Ct Koass Ri
http://slidepdf.com/reader/full/head-ct-koass-ri 20/35
FRACTRE!
• Linear %ract&re
• Depressed %ract&re
• /asilar skull fracture• *rontal sinus fracture
• Pneumocephalus
• &ro'ing fracture

8/10/2019 Head Ct Koass Ri
http://slidepdf.com/reader/full/head-ct-koass-ri 21/35
0inear fracture
• "1ial CT scan 'ith
bone algorithm sho's
multiple fractures of
the right frontal andparietal bones
(arrows).

8/10/2019 Head Ct Koass Ri
http://slidepdf.com/reader/full/head-ct-koass-ri 22/35
Depressed *racture
• " fragment is
considered depressed
'hen its outer table is
displaced belo' thelevel of the inner table
of the skull

8/10/2019 Head Ct Koass Ri
http://slidepdf.com/reader/full/head-ct-koass-ri 23/35
Pneumocephalus
• "ir loculi in thee1tracerebral spaces
typically indicate traumatic
air entry resulting from
fracture of a paranasalsinus or mastoid air cells
• 2ay be complicated by
CS* leakage, empyema,
meningitis, or brainabscess
Pneumocephalus3 Collections of air
overlie the frontal lobes and e1tend
along the anterior interhemispheric fi
ssure (arrows).

8/10/2019 Head Ct Koass Ri
http://slidepdf.com/reader/full/head-ct-koass-ri 24/35
4ematomas
• Cephalhematoma• Intracerebral hematoma +IC4.
• !pidural hematoma +!D4.
• Subdural hematoma +SD4.
• Subarachnoid hemorrhage +S"4.
• Contusion
• Diffuse a1onal in5ury
• /rain stem in5ury• /rain s'elling % edema
• Penetrating in5ury
• Vascular in5ury

8/10/2019 Head Ct Koass Ri
http://slidepdf.com/reader/full/head-ct-koass-ri 25/35
Intracerebral 4ematoma
• 4omogeneously
hyperdense
• Sharply marginated lesions
surrounded by a rim of
decreased density
• 2ass effect may be present• 66 sites $ frontal and
temporal lobes, basal
ganglia, posterior fossa
• 66 associated '7 othertraumatic lesions, e1 $ S"4,
SD4, IV4Intraparenchymal hematoma3 0arge,
'ell)marginated intraparenchymal
hematoma in the right parietal lobe 'ith
rupture into the ventricular system3

8/10/2019 Head Ct Koass Ri
http://slidepdf.com/reader/full/head-ct-koass-ri 26/35
!pidural 4ematoma• Damage to the middle meningeal artery
• /iconve1 or lentiform shape• 66 *racture of the ad5acent bone +8.
• 0ocation $ temporal lobe +66.3 Parietal, frontal, occipital, posterior fossa
• The shape is determined by the dura Perdara'an tidak ele(ati s&t&ra

8/10/2019 Head Ct Koass Ri
http://slidepdf.com/reader/full/head-ct-koass-ri 27/35
Subdural 4ematoma
• Tear the )rid*in* +eins
• The degree of mass effect seen 'ith an
SD4 is often disproportionate to the si9e
of the SD4
• 4yperdense Crescent"s'aped collection
'ith a conve1 lateral border and concave
medial border overlying the cerebral
conve1ity
• /iconcavity can be seen particularly 'henthe SD4 is large
• "cute, subacute +:); 'eeks post trauma.,
chronic +6; 'eeks post trauma.

8/10/2019 Head Ct Koass Ri
http://slidepdf.com/reader/full/head-ct-koass-ri 28/35
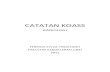
!*+d*%al e-a&-a
Ac*&e !DH !*+ac*&e !DH C%nic !DH
Perdara'an ele(ati *aris s&t&ra

8/10/2019 Head Ct Koass Ri
http://slidepdf.com/reader/full/head-ct-koass-ri 29/35
!*+a%acnid He-%%age
• 66 acutely in5ured patient % associated
'7 other lesions, e1 $ IC4
• Damage to blood vessels on the pia)
arachnoid• hyperdensity representing acute
hemorrhage is visuali9ed in t'e s&lci
overlying the cerebral conve1ities,
(it'in t'e syl+ian %iss&res, )asal
cisterns, - inter'eisp'eric %iss&re

8/10/2019 Head Ct Koass Ri
http://slidepdf.com/reader/full/head-ct-koass-ri 30/35
!*+a%acnid He-%%age
• S"4 is present in the
interhemispheric and left
sylvian fi ssures, as 'ell
as in the cortical sulci of
the left frontal andtemporal lobes3
• /lood in the frontal lobe
sulci is responsible for the
i*a* appearance ofthe subarachnoid
hemorrhage3

8/10/2019 Head Ct Koass Ri
http://slidepdf.com/reader/full/head-ct-koass-ri 31/35
He-%%agic Cn&*sin
•4eterogeneous increased densitymi1ed 'ith or surrounded by areas
of decreased or normal density
• 2ass effect +87).
• *rontal lobe conve1ity and the
lateral temporal areas are the most
common sites
A%ea dengan a&en*asi %enda +e%si'a& 'kal,
-*l&i'kal yang +eca-p*% dengan a%ea#a%ea
kecil +e%densi&as &inggi yang -engga-+a%kan
s*a& pe%da%aan

8/10/2019 Head Ct Koass Ri
http://slidepdf.com/reader/full/head-ct-koass-ri 32/35
He-%%agic Cn&*sin
"1ial CT scan demonstrates multiple
hemorrhagic contusions in the temporal
lobes3 #ote the small left occipital lobe
conve1ity subdural hematoma (arrow).
4emorrhagic contusions 'ith
surrounding edema are evident in the
inferior left frontal and anterior right
temporal lobe(arrowheads).

8/10/2019 Head Ct Koass Ri
http://slidepdf.com/reader/full/head-ct-koass-ri 33/35
.%ain s/elling 0 ede-a
• Cerebral edema may becytoto1ic, interstitial, or
vasogenic in origin
• CT findings consist of
compression of thelateral and third
ventricles and
perimesencephalic
cistern

8/10/2019 Head Ct Koass Ri
http://slidepdf.com/reader/full/head-ct-koass-ri 34/35
$%ading Di''*se A1nal In2*%y('%- Ma%sall "F, e& al 3443)

8/10/2019 Head Ct Koass Ri
http://slidepdf.com/reader/full/head-ct-koass-ri 35/35
TERIMAKA!IH
Related Documents