An interview study of 246 Negro and white mothers of children enrolled in a well-baby clinic identified deterrents to well-child supervision that were related to social and sociopsychological characteristics. The study also showed, however, that individual mothers have a consistent pattern in seeking maternal and child health care. DETERRENTS TO WELL-CHILD SUPERVISION Naomi M. Morris, M.D., M.P.H.; Martha H. Hatch, BA.; and Sidney S. Chipman, M.D., M.P.H., F.A.P.H.A. THIS study grew out of concern over the large number of children who did not appear for their scheduled appoint- ments in the North Carolina Memorial Hospital Well-Baby Clinic, a clinic car- ing for children born on the staff (med. ically indigent) service of the hospital and operating for the education of med- ical and nursing students, interns and residents. Reasons for this concern were the inconvenience to the clinic of missed appointments, and the possible loss of health supervision for those children whose parents failed to bring them as scheduled. Previous studies on appointment- breaking in pediatric clinics have cited reasons for missed appointments as bad weather,l illness of the child or family,.12 no baby sitter, no transportation, lack of money,2 dissatisfaction with medical care,2 ill-defined need to see a physi- cian,2 and lack of urgency., These studies have characterized "appoint- ment-breakers" as more often using "multiphysician" clinics,1'2 being lower class,2 and from broken or socially dis- organized homes.2 Studies focusing on health practices and health supervision of mothers and children have shown correlations be- tween early prenatal care, number of visits for well-child supervision, and so- cial class.4' Deterrents to prenatal care are similar to those given for pediatric appointment-breaking.6 The North Carolina Memorial Hos- pital Well-Baby Clinic is a clinic where, unfortunately, few patients see the same doctor twice. The children brought in are "well," a condition associated with "lack of urgency."3 The families are largely lower class; the majority are Negro. About one-fifth of the Negro mothers are unmarried. Unpaved roads in some rural areas make access diffi- cult in wet weather, and public trans- portation is extremely limited. Despite this concentration of factors contribut- ing to appointment-breaking, many mothers keep appointments regularly. Purpose The purpose of this study was to examine the background, care-seeking behavior, and certain social-psycholog- ical characteristics of medically indi- gent mothers enrolled in the Memorial Hospital Well-Baby Clinic, in order to learn more about factors acting as deterrents to well-child care and to pro- VOL. 56, NO. 8, A.J.P.H. 1232

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
An interview study of 246 Negro and white mothers of children enrolledin a well-baby clinic identified deterrents to well-child supervision thatwere related to social and sociopsychological characteristics. The studyalso showed, however, that individual mothers have a consistentpattern in seeking maternal and child health care.
DETERRENTS TO WELL-CHILD SUPERVISION
Naomi M. Morris, M.D., M.P.H.; Martha H. Hatch, BA.; and Sidney S. Chipman, M.D.,M.P.H., F.A.P.H.A.
THIS study grew out of concern overthe large number of children who did
not appear for their scheduled appoint-ments in the North Carolina MemorialHospital Well-Baby Clinic, a clinic car-ing for children born on the staff (med.ically indigent) service of the hospitaland operating for the education of med-ical and nursing students, interns andresidents. Reasons for this concern werethe inconvenience to the clinic of missedappointments, and the possible loss ofhealth supervision for those childrenwhose parents failed to bring them asscheduled.
Previous studies on appointment-breaking in pediatric clinics have citedreasons for missed appointments as badweather,l illness of the child or family,.12no baby sitter, no transportation, lackof money,2 dissatisfaction with medicalcare,2 ill-defined need to see a physi-cian,2 and lack of urgency., Thesestudies have characterized "appoint-ment-breakers" as more often using"multiphysician" clinics,1'2 being lowerclass,2 and from broken or socially dis-organized homes.2
Studies focusing on health practicesand health supervision of mothers andchildren have shown correlations be-
tween early prenatal care, number ofvisits for well-child supervision, and so-cial class.4' Deterrents to prenatal careare similar to those given for pediatricappointment-breaking.6The North Carolina Memorial Hos-
pital Well-Baby Clinic is a clinic where,unfortunately, few patients see the samedoctor twice. The children brought inare "well," a condition associated with"lack of urgency."3 The families arelargely lower class; the majority areNegro. About one-fifth of the Negromothers are unmarried. Unpaved roadsin some rural areas make access diffi-cult in wet weather, and public trans-portation is extremely limited. Despitethis concentration of factors contribut-ing to appointment-breaking, manymothers keep appointments regularly.
PurposeThe purpose of this study was to
examine the background, care-seekingbehavior, and certain social-psycholog-ical characteristics of medically indi-gent mothers enrolled in the MemorialHospital Well-Baby Clinic, in order tolearn more about factors acting asdeterrents to well-child care and to pro-
VOL. 56, NO. 8, A.J.P.H.1232
DETERRENTS TO WELL-CHILD SUPERVISION
vide information which could be usedto decrease missed appointments in theclinic.
Method
Home interviews were held with 246Negro and white mothers of ten-month-old children enrolled in the Well-BabyClinic. Names were obtained fromnursery records and cohorts were col-lected over an 11-month period. In-fants of college student families, thosenot living with their own mothers, pre-matures, multiple births, and those withsevere congenital anomalies or neonatalillnesses were excluded.
Seventeen otherwise eligible motherswere not interviewed because they hadmoved too far away, could not be lo-cated, or were located too late to be in-terviewed while the child was still inthe ten-month age group. As far ascould be determined from the children'smedical records, these mothers did notdiffer in race, marital status, or care-seeking behavior from those interviewed.No refusals to participate were encoun-tered.Memorial Hospital medical records
were reviewed after the child reachednine months of age to extract informa-tion concerning clinlic attendance andother data. Structured questionnaireswere used to seek information fromthe mothers. Along with backgroundinformation including marital status,age, education, occupation, householdstructure, and pregnancy history, datawere recorded concerning the mother'sagreement with a series of statementsabout the purposes and potentialities ofchild health supervision; her reactionsto a series of hypothetical problems ina nine-month-old child; her attitudesabout doctors, clinics and clinic per-sonnel; her reactions to a scale testingher degree of alienation; her opinionsabout prenatal and maternity care inMemorial Hospital and about the Well-
Baby Clinic; her sources of child-careknowledge; how the mother felt thechild was getting along; sources ofpediatric care besides Memorial- Hos-pital; and family decision-making whenthe child was sick.
Scales for assessing the mother's atti-tudes, agreement with purposes of well-child supervision and reactions to hypo-thetical problems were constructed bythe investigators. The scale for meas-uring alienation was adapted from aninstrument developed by Dr. DwightDean, a sociologist at Dension Univer-sity.7The father's occupational status was
dlassified, utilizing a method developedby the University of North CarolinaDepartment of Sociology.8 Farm andnonfarm occupations are separated, andeach category is grouped into four strata.Education, job training, skill, and re-sponsibility are considered. The data wereanalyzed against the number of certainimmunizing inoculations received by thechild during the first nine months oflife.* This measure has been used inthe past5 and has the advantages of giv-ing credit for preventive care receivedoutside the hospital clinic when morethan one source of care is utilized by afamily, and not being unduly influencedby a specific doctor's re-visit scheduling.The number of immunizing inocula-
tions received,t scale scores, years ofeducation, numbers of pregnancies andother data collected in this study werecounted (metric) values or at leastrank-ordered Since it is especially de-signed for the analysis of nonparametricrank-ordered data, much use was made
*By nine months of age, consistent withpractice common in North Carolina at thetime of the study, the basic series of threediphtheria, pertussis, and tetanus inoculationsand one smallpox inoculation would have beencompleted if the children had received regularcare from any medical source.
t One inoculation against diphtheria, per-tussis, and tetanus counted as "1"; one inocu-lation of smallpox vaccine counted as "1." SeeResults.
AUGUST, 1966 1233
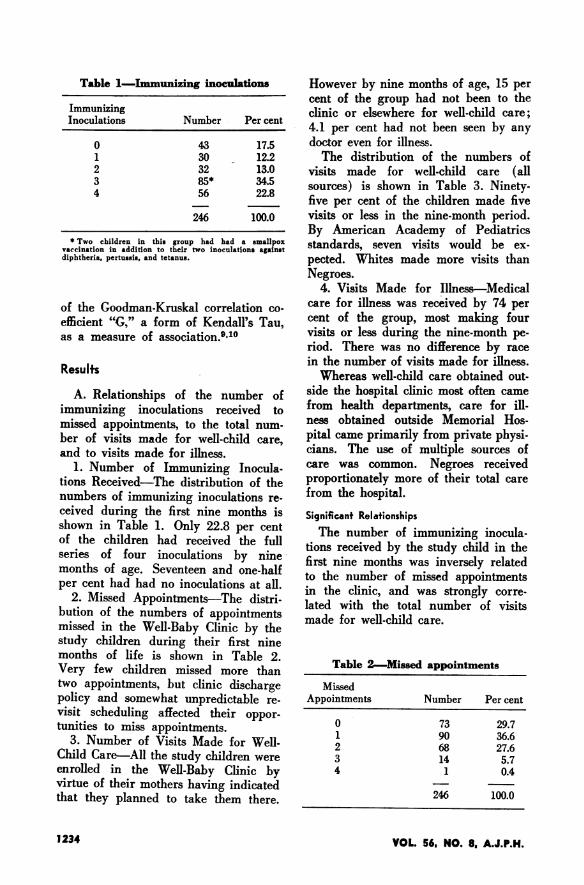
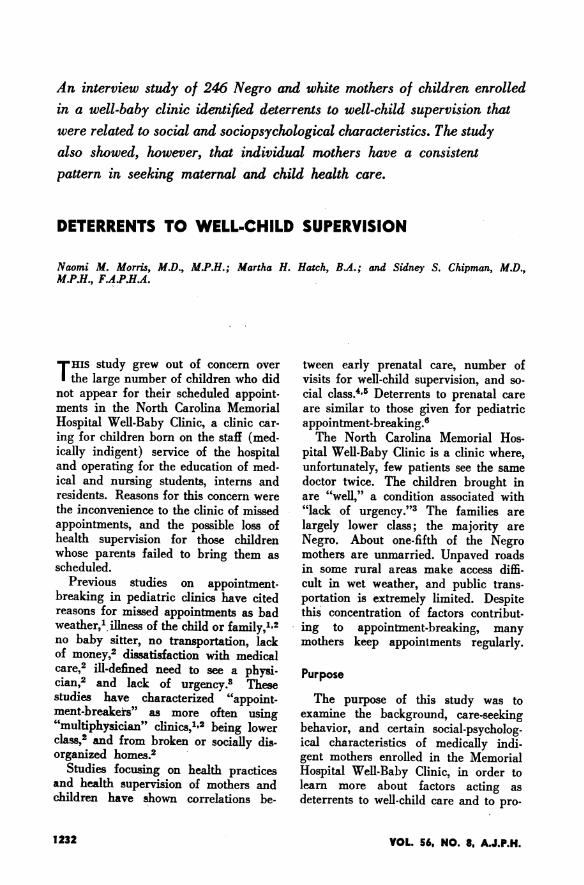
Table 1-Immunizing inoculations
ImmunizingInoculations Number Per cent
0 43 17.51 30 12.22 32 13.03 85* 34.54 56 22.8
246 100.0
* Two children in this group had had a smallpoxvaccination in addition to their two inoculations againstdiphtheria, pertussis, and tetanus.
of the Goodman-Kruskal correlation co-efficient "G," a form of Kendall's Tau,as a measure of association.910
Results
A. Relationships of the number ofimmunizing inoculations received tomissed appointments, to the total num-ber of visits made for well-child care,and to visits made for illness.
1. Number of Immunizing Inocula-tions Received-The distribution of thenumbers of immunizing inoculations re-ceived during the first nine months isshown in Table 1. Only 22.8 per centof the children had received the fullseries of four inoculations by ninemonths of age. Seventeen and one-halfper cent had had no inoculations at all.
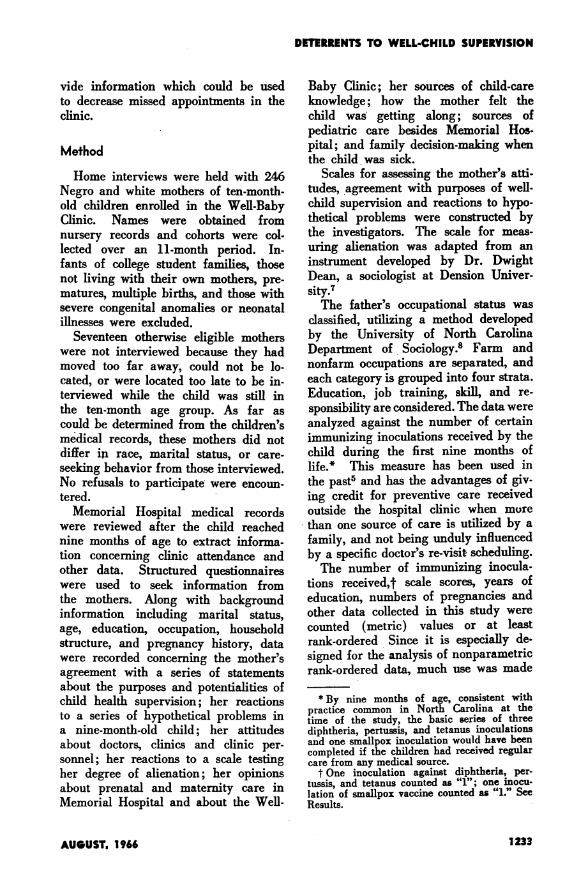
2. Missed Appointments-The distri-bution of the numbers of appointmentsmissed in the Well-Baby Clinic by thestudy children during their first ninemonths of life is shown in Table 2.Very few children missed more thantwo appointments, but clinic dischargepolicy and somewhat unpredictable re-visit scheduling affected their oppor-tunities to miss appointments.
3. Number of Visits Made for Well-Child Care-All the study children wereenrolled in the Well-Baby Clinic byvirtue of their mothers having indicatedthat they planned to take them there.
However by nine months of age, 15 percent of the group had not been to theclinic or elsewhere for well-child care;4.1 per cent had not been seen by anydoctor even for illness.The distribution of the numbers of
visits made for well-child care (allsources) is shown in Table 3. Ninety-five per cent of the children made fivevisits or less in the nine-month period.By American Academy of Pediatricsstandards, seven visits would be ex-pected. Whites made more visits thanNegroes.
4. Visits Made for Illness-Medicalcare for illness was received by 74 percent of the group, most making fourvisits or less during the nine-month pe-riod. There was no difference by racein the number of visits made for illness.Whereas well-child care obtained out-
side the hospital clinic most often camefrom health departments, care for ill-ness obtained outside Memorial Hos-pital came primarily from private physi-cians. The use of multiple sources ofcare was common. Negroes receivedproportionately more of their total carefrom the hospital.
Significant RelationshipsThe number of immunizing inocula-
tions received by the study child in thefirst nine months was inversely relatedto the number of missed appointmentsin the clinic, and was strongly corre-lated with the total number of visitsmade for well-child care.
Table 2-Missed appointments
MissedAppointments Number Per cent
0 73 29.71 90 36.62 68 27.63 14 5.74 1 0.4
246 100.0
VOL. 56, NO. 8. A.J.P.H.1234

DETERRENTS TO WELL-CHILD SUPERVISION
The total number of visits made forillness was not associated with the de-pendent variable but considering visitsmade only to Memorial Hospital, thelarger the proportion of visits madefor illness the smaller the number ofimmunizing inoculations received. Cor-relation values are given in Table 4.
B. Relationships of the dependentvariable to background characteristics,pregnancy histories, and past preven-tive care-seeking histories of themothers.
1. Race, Age, Education, Occupa-tion, Family, and Household Structure-Over three-quarters of the studygroup were Negro. The median age ofthe mothers was 24 years, of the mar-ried fathers 28 years. The medianlevel of completed school years was tenfor both mothers and fathers. Two-thirds of the married fathers were un-skilled laborers; almost one-third wereskilled laborers, the small remainderwere white collar workers. About two-thirds of the Negro mothers were work-ing and one-third of the whites. Themajority of the working mothers wereemployed full-time.The families resided largely in rural
non-farm areas or in small communi-ties. The median household size wasbetween five and six persons, with just
Table 3-Number of visits for well-childcare (to all sources)
Visits Number Per cent
0 37 15.01 29 11.82 29 11.83 53 21.64 56 22.85 28 11.46 7 2.87 4 1.68 2 0.89 1 0.4
246 100.0
Table 4*-Relationships of the depend-ent variable to missed appointments,and to visits made for well-child careand illness, values for "G" given
Number ofImmunizingInoculations
Missed appointments - 0.26**Total number of well-child care
visits (all sources) +0.84**Proportion of visits for sickness
(Memorial Hospital) -0.28**
* In Table 4 and subsequent tables, asterisks in-dicate the level of significance; * means P is equal toor less than 0.05; ** means P is equal to or less than0.01. Direct relationships are indicated by a plus sign,inverse relationships by a minus sign. "NS" in a tableindicates that the value for "G" was not significantat the 0.05 level or less.
under three children per household.The median number of children forwhom an individual mother was re-sponsible was just over two. Negroeslived in larger households than whites,with more children in them, but withno more children per mother. Almostone-third of the households includedmore than one adult woman; 35 percent of the families were "extended"(adult relatives, male or female presentin addition to parent(s) of child).Negroes were more often living in ex-tended family groups. Seventy-six percent of the mothers were married andliving with their husbands; 17 per centof the mothers had never been mar-ried. The unmarried mothers all hap-pened to be Negroes, younger than therest (median age 20 years) and 98 percent were living in extended families,usually with their parents and siblings.The distributions of some of these
characteristics are shown in greater de-tail in Tables 5 through 11.
Significant RelationshipsTable 12 shows that the number of
immunizing inoculations received bynine months of age was directly asso-ciated with mother's education, father's
AUGUST. 1966 1235
Table 5-Race
Number Per cent
Negro 192 78.0White 54 22.0
246 100.0
Table 6-Age of parents
Mothers FathersAge No. % No. %
Unknown 45 18.3
15-19 36 14.6 2 0.820-24 99 40.3 61 24.825-29 52 21.1 57 23.230.34 30 12.2 33 13.435-39 20 8.1 23 9.4
40-44 9 3.7 15 6.145-49 4 1.650.54 5 2.055-5960-64 1 0.4
246 100.0 246 100.0
education, and father's occupationalstratum. As the number of children forwhom a mother was responsible in-creased, the number of immunizinginoculations achieved by the study childdecreased. Significant correlations werenot found with other characteristicsmentioned above.
2. Pregnancy Histories and Past Pre-ventive Care-Seeking-The 246 mothersinterviewed had had from 1 to 15 preg-nancies; at least one pregnancy had re-sulted in miscarriage (fetus lost before20 weeks' gestation), stillbirth (still-born fetus delivered after 20 weeks'gestation), or liveborn child who subse-quently died, in the histories of 31 percent of the mothers. Negroes reportedsignificantly more live births now dead.With reference to the pregnancy
which produced the study child, 40per cent of the mothers initiated pre-
natal care during the first trimester, 38per cent during the second trimester.Four per cent of the mothers had noprenatal care at all; 18 per cent initiatedprenatal care during the third trimester.Negroes tended to initiate prenatal carelater in pregnancy than whites. Motherswith husbands in lower occupationalstrata similarly initiated prenatal carelater.
Twenty-nine per cent of the motherswho received prenatal care and forwhom the source is known (n=220)sought care from a private physicianbefore enrolling in the Memorial Hos-pital staff (medically indigent) pre-natal clinic. The rest of the mothersreceived clinic care only.A postpartum examination was ob-
tained by 61 per cent of the mothers.At the time of the interviews, 24 per
cent of the mothers had had no poliovaccine. Twenty-two per cent had had
Table 7-Education
Mothers FathersYears No. % No. %
Unknown 1 0.4 46 18.7Under 4 2 0.8 8 3.24-6 11 4.5 25 10.27-9 83 33.8 61 24.810-11 64 26.0 59 24.0High Grad. 69 28.0 36 14.61-3 college 14 5.7 9 3.7Coll. Grad. 2 0.8 2 0.8
246 100.0 246 100.0
Table 8-Occupation of father
Stratum Number Per cent
Unknown 46 18.71 (High) 1 0.42 10 4.13 57 23.24 (Low) 132 53.6
246 100.0
VOL. 56. NO. 8. A.J.P.H.1 236

DETERRENTS TO WELL-CHILD SUPERVISION
one or two Salk inoculations; 45 percent had had three or more; the rest (9per cent) did not know whether theyhad had any. White mothers had re-ceived more polio inoculations thanNegro mothers.Among the living siblings of the
study children (175 families had morethan one child), only 51 per cent hadhad three or more diphtheria, pertussis,and tetanus inoculations. In 24 fami-lies there were 44 siblings with noinoculations.The mothers reported learning what
to do for their babies in sickness andhealth from family members and theirown experiences; very few assignedmuch importance to the role of formaleducation, including parents' classes,or mass media.
Significant Relationships
Table 13 shows that the number ofimmunizing inoculations received inthe nine-month period was inversely re-
Table 9-Place of residence
Number Per cent
Unknown 1 0.410,000 and over 42 17.12,500-10,000 14 5.7Under 2,500 35 14.2Suburb of city 13 5.3Rural, nonfarm 112 45.5Farm 29 11.8
246 100.0
Table 10-Number of other adult womenin household
Number Per cent
None 170 69.01 62 25.32 10 4.13 4 1.6
246 100.0
Table 11-Marital status
Number Per cent
Married andliving together 186 75.6
Separated 14 5.7Legally divorced 4 1.6Widowed 1 0.4Not married 41 16.7
246 100.0
Table 19- Relationships of the depend-ent variable to significant backgroundfactors of the mothers, values for "G"given
Number ofImmunizingInoculations
Mother's education +0.26**Father's education +0.19*Father's occupational stratum +0.21*Number of children for whomeach mother responsible -0.21**
lated to the number of pregnancies themother had had and to the number oflive births now living. The study child
- had received more immunzing inocu-lations if the mother had initiated pre-natal care early or obtained a post-partum examination. The number ofimmunizing inoculations received by thestudy child was also directly relatedto the number of polio-inoculations re-
ceived by his mother and to the pro-portion of his siblings who had receivedat least three diphtheria, pertussis, andtetanus inoculations.No associations emerged with the
mothers' sources of baby care informa-tion.
C. Specific factors affecting the num-ber of immunizing inoculitions received.
1. External factors-A group of eco-nomically-based factors were exploredand examined against the dependentvariable. It was seen that the farther
AUGUST. 1966 1237
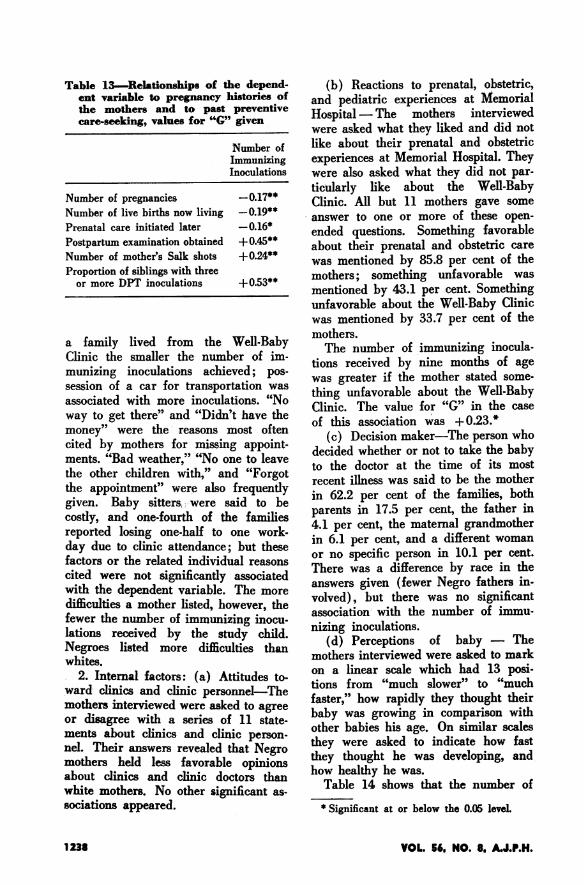
Table 13-Relationships of thent variable to pregnancy hithe mothers and to past ]care-seeking, values for "'G"
IIi
Number of pregnanciesNumber of live births now livingPrenatal care initiated laterPostpartum examination obtainedNumber of mother's Salk shotsProportion of siblings with three
or more DPT inoculations
a family lived from the I
Clinic the smaller the numb4munizing inoculations achieisession of a car for transportassociated with more inoculatway to get there" and "Didn'tmoney" were the reasons ncited by mothers for missingments. "Bad weather," "No onthe other children with," an(the appointment" were also Igiven. Baby sitters, were sacosdy, and one-fourth of thEreported losing one-half to cday due to clinic attendance;factors or the related individu,cited were not significantlywith the dependent variable.difficulties a mother listed, hoifewer the number of immunizilations received by the stuNegroes listed more difficulwhites.
2. Internal factors: (a) Atiward clinics and clinic persoxmothers interviewed were askeoor disagree with a series ofments about clinics and clininel. Their answers revealed timothers held less favorableabout clinics and clinic doewhite mothers. No other signisociations appeared.
e depend- (b) Reactions to prenatal, obstetric,istories of and pediatric experiences at Memorialpreventive Hospital -The mothers interviewedgiven were asked what they liked and did notNlumber of like about their prenatal and obstetricmmunizing experiences at Memorial Hospital. Theynoculations were also asked what they did not par-
ticularly like about the Well-Baby- 0.17** Clinic. All but 11 mothers gave some
-0.19* answer to one or more of these open-0.45** ended questions. Something favorable
+0A5** about their prenatal and obstetric care+0.24** was mentioned by 85.8 per cent of the
+0.53** mothers; something unfavorable was+_____* mentioned by 43.1 per cent. Something
unfavorable about the Well-Baby Clinicwas mentioned by 33.7 per cent of themothers.WVell-Baby The number of immunizing inocula-
er of im- tions received by nine months of ageired; pos was greater if the mother stated some-
ions. "No thing unfavorable about the Well-Babyhave. the Clinic. The value for "G" in the case
iost often of this association was + 0.23.*lOStponten (c) Decision maker-The person who,appoint- decided whether or not to take the baby.e to leave to the doctor at the time of its most
I "Forgot recent illness was said to be the motherfrequently in 62.2 per cent of the families, bothId to befd tole parents in 17.5 per cent, the father inewamlrkes 4.1 per cent, the maternal grandmother
but these in 6.1 per cent, and a different womanbtrheason or no specific person in 10.1 per cent.al reasons There was a difference by race in the
Thsoriated answers given (fewer Negro fathers in-The more volved), but there was no significantngverinou association with the number of immu-dy child. nizing inoculations.ties than (d) Perceptions of baby - Themothers interviewed were asked to markitudes to- on a linear scale which had 13 posi-
tions from "much slower" to "muchmto agree faster," how rapidly they thought their
11 statee baby was growing in comparison with11 state- other babies his age. On similar scalesPpegro they were asked to indicate how fastatpNnegro they thought he was developing, andopinions how healthy he was.
tors than Table 14 shows that the number ofificant as-* Significant at or below the 0.05 leveL
VOL. 56, NO. 8, A.J.P.H.1 23S
DETERRENTS TO WELL-CHILD SUPERVISION
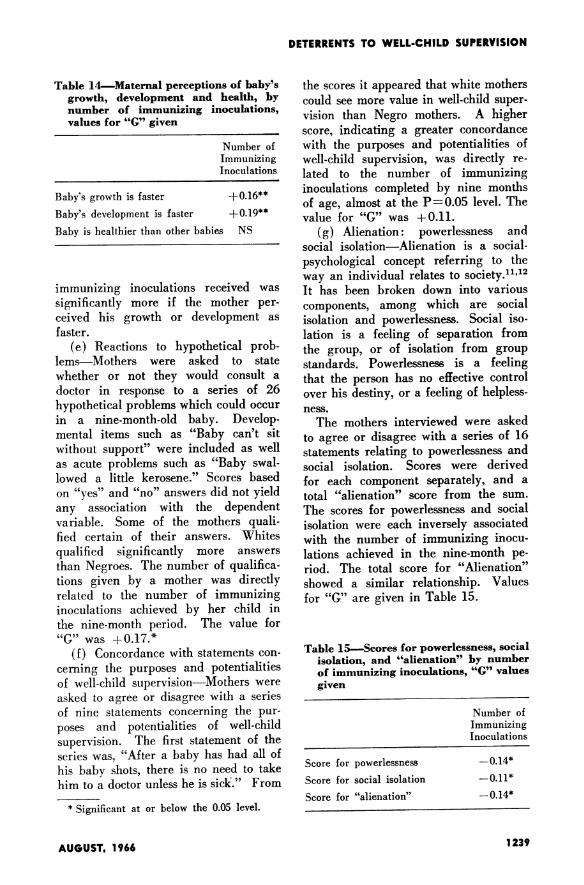
Table 14-Maternal perceptions of baby'sgrowth, development and health, bynumber of immunizing inoculations,values for "G" given
Number ofImmunizingInoculations
Baby's growth is faster +0.16**Baby's development is faster +0.19**
Baby is healthier than other babies NS
immunizing inoculations received wassignificantly more if the mother per-ceived his growth or development asfaster.
(e) Reactions to hypothetical prob-lems-Mothers were asked to statewhether or not they would consult adoctor in response to a series of 26hypothetical problems which could occurin a nine-month-old baby. Develop-mental items such as "Baby can't sitwithout support" were included as wellas acute problems such as "Baby swal-lowed a little kerosene." Scores basedon "yes" and "no" answers did not yieldany association with the dependentvariable. Some of the mothers quali-fied certain of their answers. Whitesqualified significantly more answersthan Negroes. The number of qualifica-tions given by a mother was directlyrelated to the number of immunizinginoculations achieved by her child inthe nine-month period. The value for"G" was +0.17.*
(f) Concordance with statements con-cerning the purposes and potentialitiesof well-child supervision-Mothers wereasked to agree or disagree with a seriesof nine statements concerning the pur-poses and potentialities of well-childsupervision. The first statement of theseries was, "After a baby has had all ofhis baby shots, there is no need to takehim to a doctor unless he is sick." From
* Significant at or below the 0.05 level.
the scores it appeared that white motherscould see more value in well-child super-vision than Negro mothers. A higherscore, indicating a greater concordancewith the purposes and potentialities ofwell-child supervision, was directly re-lated to the number of immunizinginoculations completed by nine monthsof age, almost at the P= 0.05 level. Thevalue for "G" was +0.11.
(g) Alienation: powerlessness andsocial isolation-Alienation is a social-psychological concept referring to theway an individual relates to society.11 12
It has been broken down into variouscomponents, among which are socialisolation and powerlessness. Social iso-lation is a feeling of separation fromthe group, or of isolation from groupstandards. Powerlessness is a feelingthat the person has no effective controlover his destiny, or a feeling of helpless-ness.The mothers interviewed were asked
to agree or disagree with a series of 16statements relating to powerlessness andsocial isolation. Scores were derivedfor each component separately, and atotal "alienation" score from the sum.The scores for powerlessness and socialisolation were each inversely associatedwith the number of immunizing inocu-lations achieved in the nine-month pe-riod. The total score for "Alienation"showed a similar relationship. Valuesfor "G" are given in Table 15.
Table 15-Scores for powerlessness, socialisolation, and "alienation" by numberof immunizing inoculations, "G" valuesgiven
Number ofImmunizingInoculations
Score for powerlessness - 0.14*
Score for social isolation -0.11*
Score for "alienation" -0.14*
1239AUGUST. 1966
Discussion
The data supported the use of thenumber of immunizing inoculations re-ceived by the child during the firstnine months of life as a measure of theamount of well-child care sought, andshowed an inverse relationship betweenthat measure and the number of ap-pointments missed in the Memorial Hos-pital Clinic, a more limited variable.The number of immunizing inocula-
tions received was greater with earlierinitiation of prenatal care by the motherand with a larger proportion of thestudy child's siblings having received atleast three inoculations against diph-theria, pertussis, and tetanus. Directassociations between the number of polioshots the mother had had, and the factthat she had obtained a postpartumexamination after the birth of the studychild, added to the impression of theconsistency of maternal care-seekingbehavior.What is it about being lower class
that causes in some mothers a kindof care-seeking behavior consistentlydifferent from that desired by the stand-ard-setting purveyors of health care?
According to this study of medicallyindigent mothers, those who seek lesspreventive care are less educated, andare married to less educated men in thelowest occupational stratum; they havehad more pregnancies than othermothers and have more children to carefor; and they live farther from theclinic (which is located on the univer-sity campus in a small residential com-munity), do not own a car, and listmore difficulties, many based in eco-nomics, encountered in past efforts toattend clinic. This largely indicates thatthe lower a mother is in the lower class,the less preventive care she seeks.
In the medically indigent mothersstudied, the social-psychological factorsexamined provided more answers tothe question of what it is about lower
class status that produces less preven-tive care-seeking.
Mothers who achieved fewer immuniz-ing inoculations for their children wereless impressed with the purposes andpotentialities of well-child supervision;they felt more powerless and socially iso-lated; and they perceived the growthand development of their children asless rapid. The latter may be a re-flection of the mothers' feelings aboutthemselves, rather than accurate ob-servations. In addition they were lessspecifically critical of the clinic, andqualified fewer answers during the in-terview. Although difficult to interpret,these last traits demonstrate a differ-ence in communication behavior orthought in the mothers.To what extent these social-psycho-
logical characteristics are independentof race or stratum within the lowersocial class is beyond the scope of thispaper, but future data analysis willcarry further the exploration of both.
Conclusions
Conclusions drawn in this report are:(1) The amount of preventive child
care sought among the medically indi-gent is related to social class stratumand to social-psychological factors,among which are the mother's concord-ance with the purposes and potentialitiesof well-child supervision; her feelings ofpowerlessness and social isolation; andher perceptions of her baby's well-being(and therefore probably of herself).
(2) Maternal and child health care-seeking tends to form a consistent pat-tern for individual mothers.
SummaryAn interview study of 246 Negro and
white mothers of 10-month-old childrenenrolled in the well-baby clinic of asouthern university hospital has identi-fied certain deterrents to well-child su-
VOL. 56. NO. 8. A.J.P.H.1240
DETERRENTS TO WELL-CHILD SUPERVISION
pervision related to social class and tosocial-psychological characteristics.
Mothers whose children received lesspreventive care were less educated, mar-ried to less educated men in the low-est occupational stratum, of higher par-ity, and living farther away from theclinic (which is located on the uni-versity campus). They owned fewerautomobiles, and listed more difficultiesinterfering with attendance at the clinic.They were less impressed with the
purposes and potentialities of well-childcare, felt more powerless and sociallyisolated, and perceived the growth anddevelopment of their children as lessrapid than that of others. They were lessapt to qualify their answers to questions,and less specifically critical of the clinic.
It was also demonstrated in the studythat maternal and child health care-seeking tends to form a consistent pat-tern for individual mothers.
ACKNOWLEDGMENTS-The authors gratefullyacknowledge the assistance of Dana Quade,Ph.D., assistant professor of biostatistics, Uni-versity of North Carolina School of PublicHealth, who acted as biostatistical consultantfor this study. We also wish to thank DwightG. Dean, Ph.D., for making available his
Alienation Scale, and Drs. Floyd Denny, LorenMacKinney, and Charles Sheaffer of the De-partment of Pediatrics, University of NorthCarolina School of Medicine, whose friendlycooperation made the study possible.
REFERENCES1. Hansen, Ann C. Broken Appointments in a Child
Health Conference. Nursing Outlook Vol 1 (July),1953.
2. Alpert, Joel J. Broken Appointments. Pediatrics 34:127-132 (July), 1964.
3. Ambuel, J. Phillip, et al. Urgency as a Factor inClinic Attendance. Am. J. Dis. Child. 4:394-398(Oct.), 1964.
4. Yankauer, Alfred; Boek, Walter E.; Lawson, EdwinD.; and lanni, Francis A. J. Social Stratificationand Health Practices in Child-Bearing and Child-Rearing. A.J.P.H. 48,6:732-741 (June), 1958.
5. Schonfield, Jacob; Schmidt, William M.; andSternfeld, Leon. Variations in Prenatal Care andWell-Child Supervision in a New England City.J. Pediat. 61,3:430-437 (Sept.), 1962.
6. Monahan, Howard B., and Spencer, Esther C.Deterrents to Prenatal Care. Children (May-June),1962.
7. Dean, Dwight. Alienation Scales. Original materialin mimeograph form, from studies done at DenisonUniversity.
8. Pope, Hal. Original material in mimeograph form,from studies done by the University of North Caro-lina Department of Sociology on unwed mothers inNorth Carolina.
9. Kendall, Maurice G. Rank Correlation Methods (3rded.). New York: Hafner Publishisg Company, 1963.
10. Goodman, Leo A., and Kruskal, William H. Meas-ures of Association for Cross Classifications. IHI. Ap-proximate Sampling Theory. J. Am. Statist. A. 58:310-364, 1963.
11. Dean, Dwight G. Alienation: Its Meaning and Meas-urement. Am. Sociol. Rev. 26,5:753-758 (Oct.), 1961.
12. Seeman, Melvin, and Evans, John W. Alienation andLearning in a Hospital Setting. Ibid. 27,6:772-782(Dec.), 1962.
Dr. Morris is assistant professor of maternal and child health; Miss Hatchwas formerly research associate; and Dr. Chipman is professor of maternal andchild health, School of Public Health, University of North Carolina, Chapel Hill.
This paper was presented in part at the meeting of Maternal and Child HealthProfessors and Maternal and Child Health and Crippled Children's ServicesDirectors, Baltimore, Md., April 23, 1965, and submitted for publication onDecember 7, 1965.
AUGUST. 1966 1241
Related Documents











