INTESTINAL OBSTRUCTION TEN-YEAR STATISTICAL SURVEY AT THE HOSPITAL OF THE UNIVERSITY OF PENNSYLVANIA* PAUL NEMIR, JR., M.D. PHILADELPHIA, PENNSYLVANIA FROM THE HARRISON DEPARTMENT OF SURGICAL RESEARCH SCHOOL OF MEDICINE, UNIVERSITY OF PENNSYLVANIA. AND THE HOSPITAL OF THE UNIVERSITY OF PENNSYLVANIA, PHII4DELPHIA THIS REPORT represents the fourth in a series of statistical studies on intestinal ob- struction in the Hospital of the University of Pennsylvania. In 1929, North10 reported a mortality of 30.5 per cent between 1905 and 1922. Brill3 reported a mortality of 36.3 per cent between 1922 and 1928. Eliason and Welty5 recorded a mortality of 11 per cent in cases of intestinal obstruction ad- mitted to Surgical Service A between 1934 and 1943. This fourth report was undertaken for the following reasons: 1. To have a progress report on all cases of intestinal obstruction, as later defined, admitted to this hospital between 1940 and 1950. 2. To determine if there has been any further decrease in mortality with the use of penicillin and the other antibiotics. For this purpose, January 1, 1945, offered a con- venient dividing line. Whereas prior to 1945 penicillin was used only in several instances, from 1945 to 1950 the antibiotics were freely available for use and have been freely utilized. This study seemed indicated from the significant work of Blain and his group1' 2 and Calihan, Kennedy and Blain.4 3. To determine as far as possible whether there was any correlation between the deaths in clinical strangulation obstruc- tion, with our experimental observations.7 8 MATERIAL Between January 1, 1940, and January 1, 1950, 430 cases of mechanical intestinal obstruction were treated on the surgical service of the University Hospital. In every case obstruction was definitely found to be present by physical examination and roentgen ray examination (in the cases treated conservatively), or by physical ex- amination, roentgen ray, and operation. Of this number, 358 cases comprise the group treated by operation, and 72 cases comprise the group treated conservatively. Not in- cluded in the study were the following: 1. Sixty-eight cases diagnosed as intes- tinal obstruction but not confirmed by our criteria on physical examination, roentgen ray, or operation. Most of these patients had chronic intermittent recurrent bouts of obstruction, and were admitted during an interval period. However, as there was no definite evidence of obstruction on admis- sion, they were not included. 2. Sixteen cases of external hernias in which omentum only was found at oper- ation. Unless the intestine was definitely in- carcerated in the sac at operation, the case was not included. 3. Twelve cases of duodenal ulcer with obstruction at the pylorus or first portion of the duodenum. 4. Ten cases of postoperative paralytic ileus in which conservative treatment was successfully carried out. Obviously there were more than ten cases of paralytic ileus 367 * Submitted for publication April, 1951.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

INTESTINAL OBSTRUCTIONTEN-YEAR STATISTICAL SURVEY AT THE HOSPITAL OF THE UNIVERSITY OF PENNSYLVANIA*
PAUL NEMIR, JR., M.D.PHILADELPHIA, PENNSYLVANIA
FROM THE HARRISON DEPARTMENT OF SURGICAL RESEARCH SCHOOL OF MEDICINE, UNIVERSITY OF PENNSYLVANIA.AND THE HOSPITAL OF THE UNIVERSITY OF PENNSYLVANIA, PHII4DELPHIA
THIS REPORT represents the fourth in aseries of statistical studies on intestinal ob-struction in the Hospital of the Universityof Pennsylvania. In 1929, North10 reporteda mortality of 30.5 per cent between 1905and 1922. Brill3 reported a mortality of 36.3per cent between 1922 and 1928. Eliasonand Welty5 recorded a mortality of 11 percent in cases of intestinal obstruction ad-mitted to Surgical Service A between 1934and 1943.
This fourth report was undertaken for thefollowing reasons:
1. To have a progress report on all casesof intestinal obstruction, as later defined,admitted to this hospital between 1940 and1950.
2. To determine if there has been anyfurther decrease in mortality with the useof penicillin and the other antibiotics. Forthis purpose, January 1, 1945, offered a con-venient dividing line. Whereas prior to 1945penicillin was used only in several instances,from 1945 to 1950 the antibiotics werefreely available for use and have been freelyutilized. This study seemed indicated fromthe significant work of Blain and hisgroup1' 2 and Calihan, Kennedy and Blain.4
3. To determine as far as possiblewhether there was any correlation betweenthe deaths in clinical strangulation obstruc-tion, with our experimental observations.7 8
MATERIALBetween January 1, 1940, and January 1,
1950, 430 cases of mechanical intestinalobstruction were treated on the surgicalservice of the University Hospital. In everycase obstruction was definitely found to bepresent by physical examination androentgen ray examination (in the casestreated conservatively), or by physical ex-amination, roentgen ray, and operation. Ofthis number, 358 cases comprise the grouptreated by operation, and 72 cases comprisethe group treated conservatively. Not in-cluded in the study were the following:
1. Sixty-eight cases diagnosed as intes-tinal obstruction but not confirmed by ourcriteria on physical examination, roentgenray, or operation. Most of these patientshad chronic intermittent recurrent bouts ofobstruction, and were admitted during aninterval period. However, as there was nodefinite evidence of obstruction on admis-sion, they were not included.
2. Sixteen cases of external hernias inwhich omentum only was found at oper-ation. Unless the intestine was definitely in-carcerated in the sac at operation, the casewas not included.
3. Twelve cases of duodenal ulcer withobstruction at the pylorus or first portion ofthe duodenum.
4. Ten cases of postoperative paralyticileus in which conservative treatment wassuccessfully carried out. Obviously therewere more than ten cases of paralytic ileus
367* Submitted for publication April, 1951.
PAUL NEMIR, JR.
postoperatively during the ten-year period,but usually it was not recorded on the diag-nosis sheets unless it was of severe pro-
portions.5. Twelve cases of postoperative intes-
tinal obstruction, thought to be on amechanical basis by examination androentgen ray, which were relieved with a
Miller-Abbott tube. If re-operation was
necessary in the postoperative period, thenthe case was included in the series. Becauseof the difficulty in determining whetherpostoperative ileus was on the basis ofparalytic or an actual mechanical obstruc-tion, it was felt that only those cases provedto have a mechanical block at a secondoperation should be included.
6. Two cases of mesenteric thrombosis.7. One case of external hernia treated
conservatively because of age and severe
heart disease. Decompression and reduc-tion was successfully accomplished.The overall mortality for cases of intes-
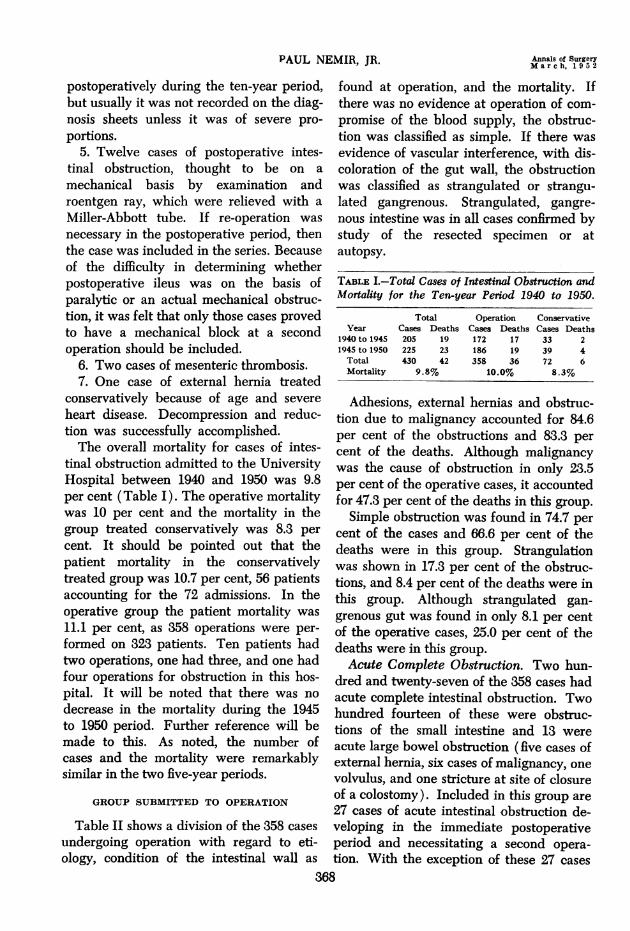
tinal obstruction admitted to the UniversityHospital between 1940 and 1950 was 9.8per cent (Table I). The operative mortalitywas 10 per cent and the mortality in thegroup treated conservatively was 8.3 per
cent. It should be pointed out that thepatient mortality in the conservativelytreated group was 10.7 per cent, 56 patientsaccounting for the 72 admissions. In theoperative group the patient mortality was
11.1 per cent, as 358 operations were per-formed on 323 patients. Ten patients hadtwo operations, one had three, and one hadfour operations for obstruction in this hos-pital. It will be noted that there was no
decrease in the mortality during the 1945to 1950 period. Further reference will bemade to this. As noted, the number ofcases and the mortality were remarkablysimilar in the two five-year periods.
GROUP SUBMITTED TO OPERATION
Table II shows a division of the 358 cases
undergoing operation with regard to eti-ology, condition of the intestinal wall as
found at operation, and the mortality. Ifthere was no evidence at operation of com-
promise of the blood supply, the obstruc-tion was classified as simple. If there wasevidence of vascular interference, with dis-coloration of the gut wall, the obstructionwas classified as strangulated or strangu-lated gangrenous. Strangulated, gangre-nous intestine was in all cases confirmed bystudy of the resected specimen or atautopsy.
TABLE I.-Total Cases of Intestinal Obstruction andMortality for the Ten-year Period 1940 to 1950.
Total Operation ConservativeYear Cases Deaths Cases Deaths Cases Deaths
1940 to 1945 205 19 172 17 33 21945 to 1950 225 23 186 19 39 4Total 430 42 358 36 72 6Mortality 9.8% 10.0% 8.3%
Adhesions, external hernias and obstruc-tion due to malignancy accounted for 84.6per cent of the obstructions and 83.3 per
cent of the deaths. Although malignancywas the cause of obstruction in only 23.5per cent of the operative cases, it accountedfor 47.3 per cent of the deaths in this group.
Simple obstruction was found in 74.7 per
cent of the cases and 66.6 per cent of thedeaths were in this group. Strangulationwas shown in 17.3 per cent of the obstruc-tions, and 8.4 per cent of the deaths were inthis group. Although strangulated gan-
grenous gut was found in only 8.1 per centof the operative cases, 25.0 per cent of thedeaths were in this group.Acute Complete Obstruction. Two hun-
dred and twenty-seven of the 358 cases hadacute complete intestinal obstruction. Twohundred fourteen of these were obstruc-tions of the small intestine and 13 were
acute large bowel obstruction (five cases ofexternal hernia, six cases of malignancy, one
volvulus, and one stricture at site of closureof a colostomy). Included in this group are
27 cases of acute intestinal obstruction de-veloping in the immediate postoperativeperiod and necessitating a second opera-
tion. With the exception of these 27 cases
368
Annals of SurgeryMarch, 1952

INTESTINAL OBSTRUCTION
subsequently discussed, all of this group^., vious operations. Both patients who hadwere operated upon within one to six hours five previous operations died following op-
after admission to the hospital. Of the 27 eration. Two more of the deaths occurredcases of postoperative obstruction, 11 were in patients having three previous operations,operated upon less than 24 hours after and the remaining two deaths occurred insymptoms developed, with no deaths, two patients having one previous operation. Itbetween 24-48 hours with two deaths, and will be noted, Table IV, that 103 (73 per
14 after 72 hours with one death. cent) of the 142 cases had adhesions or
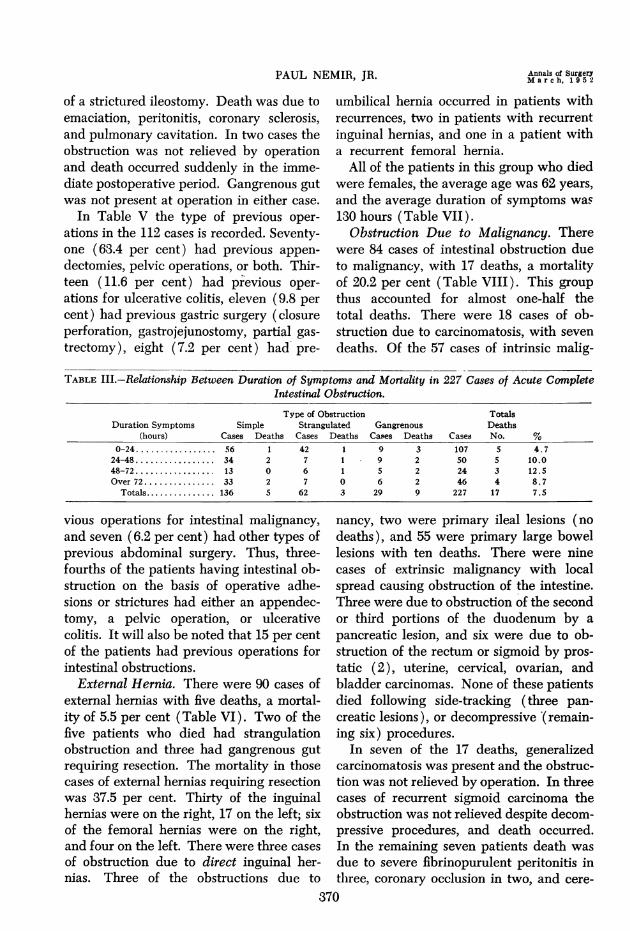
Table III shows the relationship between strictures secondary to previous operations.the duration of symptoms and the mortality Of the ten cases of inflammatory strictures,in the cases of acute obstruction. It will be five occurred in patients with ulcerativenoted that all of the strangulated and all of colitis and one of these patients died.the gangrenous cases in the entire operative Three of the ten patients who died had
TABLE II.-Etiology, Type of Obstruction, and Mortality in 358 Cases of Intestinal Obstruction Under-going Operation With 36 Deaths.
Type of Obstruction TotalsSimple Strangulated Gangrenous Deaths
Cause Cases Deaths Cases Deaths Cases Deaths Cases No. %
Adhesions .............. 110 5 8 0 11 3 129 8 6.2External hernia......... 38 0 44 2 8 3 90 5 5.5Malignancy ............ 83 17 1 0 0 0 84 17 20.2Internal hernia......... 5 0 2 0 2 2 9 2 22.2Volvulus ............... 3 0 4 0 6 0 13 0 0.0Intussusception ......... 4 1 2 0 1 0 7 1 14.3Stricture ............... 12 1 1 1 0 0 13 2 15.4Foreignbody ........... 6 0 0 0 1 1 7 1 14.3Congenital defect....... 1 0 0 0 0 0 1 0 0.0Others ................. 5 0 0 0 0 0 5 0 0O0
Totals ............... 267 24 62 3 29 9Mortality .9.0% 4.8% 31.0%
series were in this group of 227 cases. Theincrease in mortality in those cases wherethe obstructive symptoms were present forover 24 hours is apparent. The overall mor-
tality in this group was 7.5 per cent. It isinteresting to note that although gangre-nous gut was found in only 13 per cent ofthe 227 cases the number of deaths in thisgroup, however, accounted for 53 per centof the total of 17 deaths.
Adhesions. In the group of 358 cases,
there were 142 cases of intestinal obstruc-tion due to adhesions and stricture with tendeaths, a mortality of 7.0 per cent. Of thisgroup 30 (21 per cent) had no previousoperations and four died. The remaining112 had from one to five operations, 59 (53per cent) had one operation, 31 (28 per
cent) had two operations, 16 (14 per cent)had three operations, four patients had fourprevious operations and two had five pre-
gangrenous gut requiring resection andlarge amounts of dark bloody fluid in theperitoneal cavity. Death occurred at 36, 66,and 100 hours respectively. Perforation hadoccurred in the patient who died at 36hours. A 72-year-old male died on the six-teenth day following lysis of adhesions, andnecropsy revealed a coronary thrombosis.An 82-year-old female died on the eighthday following lysis of adhesions and threemajor anastomoses. Death was due toauricular fibrillation, cardiovascular failure,and uremia. One patient developed jejunalfistulas following his fourth operation forrelease of adhesions and died of inanitionon the sixtieth postoperative day. Anotherdied 35 days following resection of severelymatted loops and an ileostomy. Attemptsto close the ileostomy were unsuccessful.One patient with severe ulcerative colitisdied seven days after operation for revision
369
Volume 135Number 3
PAUL NEMIR, JR.
of a strictured ileostomy. Death was due toemaciation, peritonitis, coronary sclerosis,and pulmonary cavitation. In two cases theobstruction was not relieved by operationand death occurred suddenly in the imme-diate postoperative period. Gangrenous gutwas not present at operation in either case.
In Table V the type of previous oper-
ations in the 112 cases is recorded. Seventy-one (63.4 per cent) had previous appen-
dectomies, pelvic operations, or both. Thir-teen (11.6 per cent) had previous oper-
ations for ulcerative colitis, eleven (9.8 per
cent) had previous gastric surgery (closureperforation, gastrojejunostomy, partial gas-
trectomy), eight (7.2 per cent) had pre-
umbilical hernia occurred in patients withrecurrences, two in patients with recurrentinguinal hernias, and one in a patient witha recurrent femoral hernia.
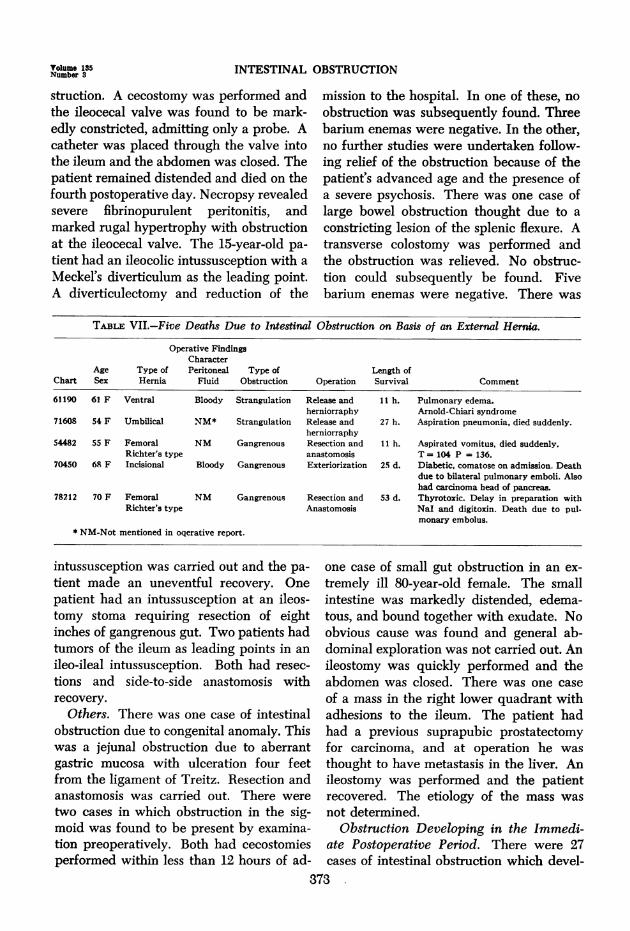
All of the patients in this group who diedwere females, the average age was 62 years,
and the average duration of symptoms was130 hours (Table VII).
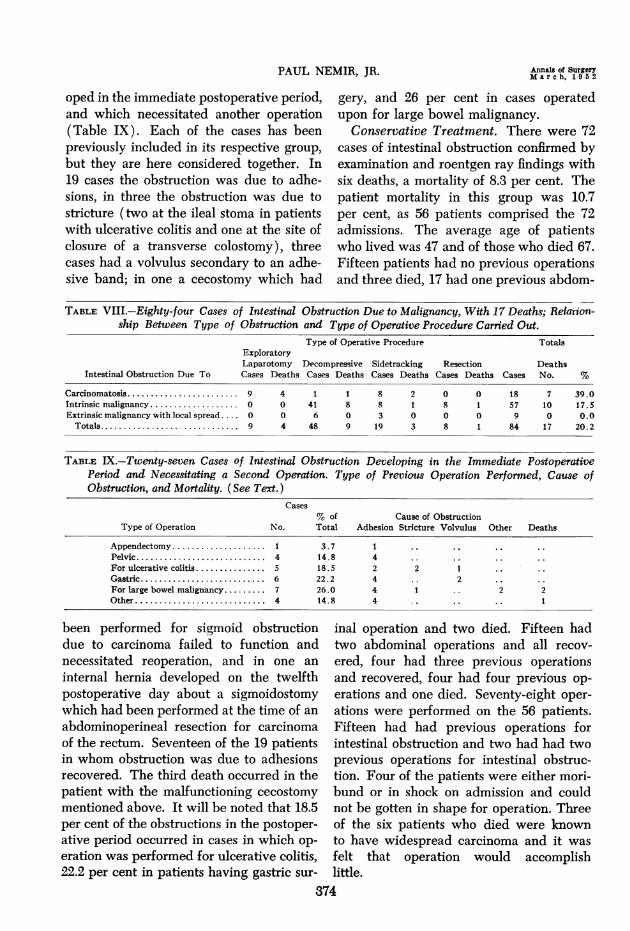
Obstruction Due to Malignancy. Therewere 84 cases of intestinal obstruction dueto malignancy, with 17 deaths, a mortalityof 20.2 per cent (Table VIII). This groupthus accounted for almost one-half thetotal deaths. There were 18 cases of ob-struction due to carcinomatosis, with seven
deaths. Of the 57 cases of intrinsic malig-
TABLE III.-Relationship Between Duration of Symptoms and Mortality in 227 Cases of Acute CompleteIntestinal Obstruction.
Duration Symptoms SimpleType of Obstruction
Strangulated GangrenousTotalsDeaths
(hours) Cases Deaths Cases Deaths Cases Deaths Cases No. %0-24 ............ 56 1 42 1 9 3 107 5 4.7
24-48 ................. 34 2 7 1 9 2 50 5 10.048-72 ................. 13 0 6 1 5 2 24 3 12.5Over 72 ............... 33 2 7 0 6 2 46 4 8.7
Totals ............... 136 5 62 3 29 9 227 17 7.5
vious operations for intestinal malignancy,and seven (6.2 per cent) had other types ofprevious abdominal surgery. Thus, three-fourths of the patients having intestinal ob-struction on the basis of operative adhe-sions or strictures had either an appendec-tomy, a pelvic operation, or ulcerativecolitis. It will also be noted that 15 per centof the patients had previous operations forintestinal obstructions.
External Hernia. There were 90 cases ofexternal hernias with five deaths, a mortal-ity of 5.5 per cent (Table VI). Two of thefive patients who died had strangulationobstruction and three had gangrenous gutrequiring resection. The mortality in thosecases of external hernias requiring resectionwas 37.5 per cent. Thirty of the inguinalhernias were on the right, 17 on the left; sixof the femoral hernias were on the right,and four on the left. There were three cases
of obstruction due to direct inguinal her-nias. Three of the obstructions due to
nancy, two were primary ileal lesions (nodeaths), and 55 were primary large bowellesions with ten deaths. There were ninecases of extrinsic malignancy with localspread causing obstruction of the intestine.Three were due to obstruction of the secondor third portions of the duodenum by a
pancreatic lesion, and six were due to ob-struction of the rectum or sigmoid by pros-
tatic (2), uterine, cervical, ovarian, andbladder carcinomas. None of these patientsdied following side-tracking (three pan-creatic lesions), or decompressive ( remain-ing six) procedures.
In seven of the 17 deaths, generalizedcarcinomatosis was present and the obstruc-tion was not relieved by operation. In threecases of recurrent sigmoid carcinoma theobstruction was not relieved despite decom-pressive procedures, and death occurred.In the remaining seven patients death was
due to severe fibrinopurulent peritonitis intlhree, coronary occlusion in two, and cere-
370
Annals of SurgeryMarch, 195 2

INTESTINAL OBSTRUCTION
bral vascular accident in one; the seventhpatient died suddenly and no autopsy was
obtained.Internal Hernia. There were nine cases
of intestinal obstruction due to internalhernia with two deaths, a mortality of 22.2per cent. All cases were acute and all wereoperated upon shortly after admission. Fourpatients had herniations of the ileum be-tween the cecum and the lateral abdominalwall underneath a band of adhesions (threecongenital, and one probably operative). Inone, a Meckel's diverticulum was in thehernia and a diverticulectomy was per-
not resected due to the poor condition ofthe patient. Diagnosis was delayed so thatthere were around six hours between admis-sion to the hospital and operation, and thepatient went into shock before operation.The other death was in a one-day-old babywith small and large gut, stomach andspleen herniated through a small diaphrag-matic hernia, with strangulated, gangrenousgut. After the hernia was reduced the gutstill remained blue but it was felt that noth-ing more could be done. Both patients haddark bloody fluid in the peritoneal cavityat operation.
TABLE IV.-One Hundred and Forty-two Cases of Intestinal Obstruction Due to Adhesions or Stric-tures, With Ten Deaths.
Previous Operations Inflammation Congenital Band OthersCases Deaths Cases Deaths Cases Deaths Cases Deaths
Adhesions due to.......... 102 6 19 0 7 1 1 1Stricturesdt-o.-;....... 1 0 10 1 1 0 1 1
Totals ... .. .. 103 6 29 1 8 1 2 2
formed. All four survived following lysis ofthe adhesion and reduction of the hernia. Intwo cases herniation occurred about enter-ostomies. One was a longitudinal twist ofthe ileum over an ileostomy into the cecalfossa and thence into the pelvis in a patientwho had had previous ileostomy and totalcolectomy in four stages for ulcerative co-
litis. Another was a longitudinal twistthrough the sigmoid mesentery around a
sigmoidostomy occurring on the twelfthpostoperative day in a patient with a pre-
vious abdominoperineal resection. Bothpatients lived following reduction of thehernia and repair of the defect. In one case
there was an ileal herniation through an
omental rent, the omentum being attachedto the internal inguinal ring following a
previous herniorrhaphy. The intestine was
strangulated but normal color returnedafter 45 minutes and the intestine was re-
placed without resection. There was one
death due to strangulated gangrenous gut ina paraduodenal hernia. Although the gutviability was questioned at operation, it was
Volvulus. There were 13 cases of intes-tinal obstruction due to volvulus with no
deaths. Eleven of these were due to post-operative adhesions, one was due to malro-tation of the gut, and one was due to sig-moid volvulus. Three of the cases due toadhesions developed in the immediate post-operative period. One was in a patient pre-
viously operated upon for ulcerative colitis,and two were in patients having a partialgastrectomy. Of the 11 patients with pre-
vious operations, two had had previous sur-
gery for ulcerative colitis, three had hadsome type of gastric operation, three hadhad previous hysterectomies, and three pre-
vious appendectomies. The other two pa-
tients had no previous operations. Six ofthe 13 cases had gangrenous gut requiringresection, and all recovered.The average time lapse from onset of
symptoms to operation was 50 hours in thepatients having gangrenous intestine re-
quiring resection and 41 hours in the otherseven cases. The average leukocyte countwas 14,000, ranging from 6800 to 19,600.
371
Volume 135Number 3

PAUL NEMIR, JR.
TABLE V.-Types of OpeHaving Intestinal Obsions or StricturesOperation.
Type of Previous Operationor Operations
AppendectomyPelvicBoth appendectomy and
pelvicFor ulcerative colitis
GastricFor intestinal malignancy
OthersPrevious operation for intes-
tinal obstruction* Fifteen patients in this gro
operations, i.e., one for one of tIand one for intestinal obstructitherefore included twice. Three c
tion. Two patients had a previoistruction, but no other abdomii
aratio in 112 Pa s baby who began showing evidence of)struction Due to Adhe- marked intestinal distention less than 24Secondary to Previous hours after birth. The abdomen was
opened approximately 40 hours after onsetCases of the distention and there was immediate
No. % of Total Deaths release of air. Exploration revealed a loop21 18.7 2 of ileum which was trapped in the right lat-33 29.5 0 eral gutter with impairment of the blood17 15.2 1 supply and perforation. The loop was mo-13 11.6 1 bilized and the gangrenous area around the11 9.8 0
8 7.2 1 perforation quickly oversewn. There7 6.2 1 seemed to be a satisfactory lumen and gas
17* 15.2 3* and fluid feces passed over the area. Post-tup had at least two previous operatively, distention was not relieved, shehe conditions mentioned aboveion. Each of these patients is continued to vomit, there was obstipationDf the 15 died following opera- and she suddenly expired on the seventhlus operation for intestinal ob-nal surgery. postoperative day. At autopsy there was
generalized peritonitis, a section of gan--remnnmis ilt-im onn hintAoer nf th1P benvWPIAbdominal tenderness and guarding was
present in all of the gangrenous cases.
Foreign Body. There were seven cases
of obstruction due to foreign body, with one
death, a mortality of 14.3 per cent. Five ofthe obstructions were due to gallstones withno deaths and two were due to fecal impac-tions with one death.The five cases of gallstone ileus are being
combined with three other cases treated inthis hospital in 1939, 1950, and 1951, andare being reported in another communica-tion.9 All were simple obstruction, all oc-
curred in elderly females, and all were
acute cases. In two of the five cases thestone was obstructing in the jejunum andin the three others, in the ileum. Enterot-omy with removal of the stone was carriedout in every case. In one, a Witzel enteros-tomy was performed above the site of ob-struction. In two cases, cholecystectomy,choledochostomy, and repair of the fistu-lous tract was performed about two weeksafter operation.Of the remaining two cases one was a
78-year-old man who had a large fecal im-paction in the ascending colon which was
successfully removed through a cecostomy.The patient who died was a three-day-old
TABLE VI.-Ninety Cases of Intestinal ObstructionDue to External Hernias, With Five Deaths.
Type of ObstructionType of Simple Strangulated GangrenousHernia Cases Deaths Cases Deaths Cases Deaths
Inguinal 17 0 28 0 2 0Incisional 10 0 6 0 1 1Femoral 3 0 3 0 4 2Umbilical 7 0 6 1 1 0Ventral 0 0 1 1 0 0Sliding 1 0 0 0 0 0TotalsCases 38 0 44 2 8 3% Mortality 0.0 4.5 37.5
in the region of closure with meconium.There was no mention of peritoneal fluid.
Intussusception. There were seven casesof obstruction due to intussusception withone death, a mortality of 14.3 per cent. Allwere acute and all but one were operatedupon less than 12 hours after admission.There were four cases of ileocolic intussus-ception. The patients were three weeks,four weeks, 22 months, and 15 years old,respectively. In two of the infants theintussusception was reduced and recoveryoccurred. In the three-week-old infant thesmall gut was found to be markedly dis-tended, though viable, and the ileal mucosahad intussuscepted into the cecum with ob-
372
Annals of SurgeryMarch, 1952
6.L%,.Ll%jua iLiLq-luljLl , aAiu uivt;Ka6v ujL tium; uuwt;i
INTESTINAL OBSTRUCTION
struction. A cecostomy was performed andthe ileocecal valve was found to be mark-edly constricted, admitting only a probe. Acatheter was placed through the valve intothe ileum and the abdomen was closed. Thepatient remained distended and died on thefourth postoperative day. Necropsy revealedsevere fibrinopurulent peritonitis, andmarked rugal hypertrophy with obstructionat the ileocecal valve. The 15-year-old pa-
tient had an ileocolic intussusception with a
Meckel's diverticulum as the leading point.A diverticulectomy and reduction of the
mission to the hospital. In one of these, no
obstruction was subsequently found. Threebarium enemas were negative. In the other,no further studies were undertaken follow-ing relief of the obstruction because of thepatient's advanced age and the presence ofa severe psychosis. There was one case oflarge bowel obstruction thought due to a
constricting lesion of the splenic flexure. Atransverse colostomy was performed andthe obstruction was relieved. No obstruc-tion could subsequently be found. Fivebarium enemas were negative. There was
TABLE VII.-Five Deaths Due to Intestinal Obstruction on Basis of an External Hernia.
Operative FindingsCharacter
Age Type of Peritoneal Type of Length ofChart Sex Hernia Fluid Obstruction Operation Survival Comment
61190 61 F Ventral Bloody Strangulation Release and 11 h. Pulmonary edema.herniorraphy Arnold-Chiari syndrome
71608 54 F Umbilical NM* Strangulation Release and 27 h. Aspiration pneumonia, died suddenly.herniorraphy
54482 55 F Femoral NM Gangrenous Resection and 11 h. Aspirated vomitus, died suddenly.Richter's type anastomosis T = 104 P = 136.
70450 68 F Incisional Bloody Gangrenous Exteriorization 25 d. Diabetic, comatose on admission. Deathdue to bilateral pulmonary emboli. Alsohad carcinoma head of pancreas.
78212 70 F Femoral NM Gangrenous Resection and 53 d. Thyrotoxic. Delay in preparation withRichter's type Anastomosis Nal and digitoxin. Death due to pul-
monary embolus.* NM-Not mentioned in oqerative report.
intussusception was carried out and the pa-
tient made an uneventful recovery. Onepatient had an intussusception at an ileos-tomy stoma requiring resection of eightinches of gangrenous gut. Two patients hadtumors of the ileum as leading points in an
ileo-ileal intussusception. Both had resec-
tions and side-to-side anastomosis withrecovery.
Others. There was one case of intestinalobstruction due to congenital anomaly. Thiswas a jejunal obstruction due to aberrantgastric mucosa with ulceration four feetfrom the ligament of Treitz. Resection andanastomosis was carried out. There were
two cases in which obstruction in the sig-moid was found to be present by examina-tion preoperatively. Both had cecostomiesperformed within less than 12 hours of ad-
one case of small gut obstruction in an ex-
tremely ill 80-year-old female. The smallintestine was markedly distended, edema-tous, and bound together with exudate. Noobvious cause was found and general ab-dominal exploration was not carried out. Anileostomy was quickly performed and theabdomen was closed. There was one case
of a mass in the right lower quadrant withadhesions to the ileum. The patient hadhad a previous suprapubic prostatectomyfor carcinoma, and at operation he was
thought to have metastasis in the liver. Anileostomy was performed and the patientrecovered. The etiology of the mass was
not determined.Obstruction Developing in the Immedi-
ate Postoperative Period. There were 27cases of intestinal obstruction which devel-
373
Volume 135Number 3
PAUL NEMIR, JR.
oped in the immediate postoperative period,and which necessitated another operation(Table IX). Each of the cases has beenpreviously included in its respective group,
but they are here considered together. In19 cases the obstruction was due to adhe-sions, in three the obstruction was due tostricture (two at the ileal stoma in patientswith ulcerative colitis and one at the site ofclosure of a transverse colostomy), threecases had a volvulus secondary to an adhe-sive band; in one a cecostomy which had
gery, and 26 per cent in cases operatedupon for large bowel malignancy.
Conservative Treatment. There were 72cases of intestinal obstruction confirmed byexamination and roentgen ray findings withsix deaths, a mortality of 8.3 per cent. Thepatient mortality in this group was 10.7per cent, as 56 patients comprised the 72admissions. The average age of patientswho lived was 47 and of those who died 67.Fifteen patients had no previous operationsand three died, 17 had one previous abdom-
TABLE VIII.-Eighty-four Cases of Intestinal Obstruction Due to Malignancy, With 17 Deaths; Relarion-ship Between Type of Obstruction and Type of Operative Procedure Carried Out.
Type of Operative Procedure TotalsExploratoryLaparotomy Decompressive Sidetracking Resection Deaths
Intestinal Obstruction Due To Cases Deaths Cases Deaths Cases Deaths Cases Deaths Cases No. %
Carcinomatosis ........................ 9 4 1 1 8 2 0 0 18 7 39.0Intrinsic mialignancy ................... 0 0 41 8 8 1 8 1 57 10 17.5Extrinsic malignancy with local spread... 0 0 6 0 3 0 0 0 9 0 0.0Totals ............... 9 4 48 9 19 3 8 1 84 17 20.2
TABLE IX.-Twenty-seven Cases of Intestinal Obstruction Developing in the Immediate PostoperativePeriod and Necessitating a Second Operation. Type of Previous Operation Performed, Cause ofObstruction, and Mortality. (See Text.)
Cases% of Cause of Obstruction
Type of Operation No. Total Adhesion Stricture Volvulus Other Deaths
Appendectomy ........... ......... 1 3.7 1 ..Pelvic ............ ............... 4 14.8 4 ..For ulcerative colitis ....... ........ 5 18.52 2 1Gastric ........................... 6 22.2 4 .. 2For large bowel malignancy......... 7 26.0 4 1 .. 2 2Other ............................ 4 14.8 4 .. .. .. 1
been performed for sigmoid obstructiondue to carcinoma failed to function andnecessitated reoperation, and in one an
internal hernia developed on the twelfthpostoperative day about a sigmoidostomywhich had been performed at the time of an
abdominoperineal resection for carcinomaof the rectum. Seventeen of the 19 patientsin whom obstruction was due to adhesionsrecovered. The third death occurred in thepatient with the malfunctioning cecostomymentioned above. It will be noted that 18.5per cent of the obstructions in the postoper-ative period occurred in cases in which op-eration was performed for ulcerative colitis,22.2 per cent in patients having gastric sur-
inal operation and two died. Fifteen hadtwo abdominal operations and all recov-
ered, four had three previous operationsand recovered, four had four previous op-
erations and one died. Seventy-eight oper-
ations were performed on the 56 patients.Fifteen had had previous operations forintestinal obstruction and two had had twoprevious operations for intestinal obstruc-tion. Four of the patients were either mori-bund or in shock on admission and couldnot be gotten in shape for operation. Threeof the six patients who died were knownto have widespread carcinoma and it was
felt that operation would accomplishlittle.
374
Annals of SurgeryMarch, 1952
Volume 135 INTESTINAL OBSTRUCTIONNumber 3
DISCUSSION
There has been a progressive decline inthe mortality of intestinal obstruction inthe Hospital of the University of Pennsyl-vania. Factors responsible for the loweredmortality have been discussed elsewhere.5 6The high mortality still existing in strangu-lation obstruction with gangrenous bowelindicates that factors other than thoseamenable to present improved methods ofmanagement continue to exist. There wasno decrease in mortality from 1945 to 1950when penicillin and other antibiotics werewidely used. This is not to be interpretedthat we feel the antibiotics are of no use.Blain and his group1' 2 have shown the pro-tective action of penicillin in experimentalstrangulation obstruction. Its mechanismof action is not known but in the experi-mental animal it would appear that it exertsits protective effect by delaying the actionof the bacteria on the gut wall, therebylengthening the time before the gut wallbecomes permeable to its intraluminal con-tents.6 Obviously, the outpouring of toxicintraluminal contents through a permeablegut wall into the peritoneal cavity andthence into the blood stream cannot be in-criminated as the cause of death in all thecases of strangulated gangrenous obstruc-tion. However, dark bloody fluid similar tothat which has been described in strangula-tion obstruction in the experimental animalwas present in the peritoneal cavity of eightof 12 patients at either operation or autopsyand could have conceivably contributed tothe demise.
CONCLUSIONS
1. The operative mortality in intestinalobstruction at the University Hospital forthe ten-year period, 1940 to 1950, was 10.0per cent.
2. There was no further decrease in themortality in this series during that periodwhen penicillin and the other antibioticswere freely utilized.
3. The mortality in cases where gangre-
nous bowel was found at operation was 31per cent.
4. Intestinal obstruction due to malig-nancy accounted for almost one-half thetotal deaths.
5. Peritoneal fluid which grossly resem-bled that previously described in the ex-perimental animal subjected to strangula-tion obstruction was found in the peritonealcavity of eight of the 12 patients who diedwith gangrenous bowel and could have con-ceivably contributed to the demise.
BIBLIOGRAPHY1 Blain, A., III, and J. D. Kennedy: Effect of
Penicillin in Experimental Intestinal Obstruc-tions; Studies on Strangulated Low Ileal Ob-structions. Bull. Johns Hopkins Hosp., 79: 1,1946.
2 Blain, A., III, J. D. Kennedy, R. J. Calihan andH. N. Harkins: Effect of Penicillin in Experi-mental Intestinal Obstruction; Cure of Stran-gulated Ileal Obstructions Treated with Peni-cillin Prior to Late Resections. Arch. Surg.,53: 378, 1946.
3 Brill, S.: The Mortality of Intestinal Obstruction;Analysis of 124 Cases Operated Upon at theHospital of the University of Pennsylvania.Ann. Surg., 89: 541, 1929.
4 Calihan, R. J., J. D. Kennedy and A. Blain, III:Intestinal Obstruction: Study of 204 AcuteCases with Reference to Possible Efficacy ofAnti-bacterial Therapy. Bull. Johns HopkinsHosp., 79: 21, 1946.
5 Eliason, E. L., and R. F. Welty: Ten Year Sur-vey of Intestinal Obstruction. Ann. Surg.,125: 57, 1947.
6 Hawthorne, H. R., and P. Nemir, Jr.: The Man-agement of Intestinal Obstruction. Med. Clin.North America, Mass. Gen. Hosp. Number,p. 1455, 1949.
7 Nemir, P., Jr., H. R. Hawthorne, I. Cohn, Jr.,and D. L. Drabkin: The Cause of Death inStrangulation Obstruction; An ExperimentalStudy. I. Clinical Course, Chemical, Bacterio-logic, and Spectrophotometric Studies. Ann.Surg., 130: 857, 1949.
8 Nemir, P., Jr., H. R. Hawthorne, I. Cohn, Jr.,and D. L. Drabkin: The Cause of Death inStrangulation Obstruction; An ExperimentalStudy. II. Lethal Action of the PeritonealFluid. Ann. Surg., 130: 874, 1949.
9 Nemir, P., Jr.: Gallstone Ileus: Report of EightCases: Surg., Gynec. & Obst.; to be pubished.
10 North, J. P.: Acute Intestinal Obstruction. Inter-nat. Clin.. 3: 206. 1929.
375
Related Documents











