American Journal of Pathology, Vol. 145, No. 6, December 1994 Copyright © American Society for Investigative Pathology Hepatic Microcirculatory Perfusion Failure Is a Determinant of Liver Dysfunction in Warm Ischemia-Reperfusion Brigitte Vollmar,*t Julia Glasz,* Rosemarie Leiderer,* Stefan Post,t and Michael D. Menger*t From the Institute for Surgical Research,* University of Munich, the Institute for Clinical and Experimental Surgery,t University of Saarland, Homburg/Saar, and the Department of Surgery,* University of Heidelberg, Germany Hepatic ischemia-reperfusion (I/R) is character- ized by circulatory and metabolic derangements, liver dysfunction, and tissue damage. However, little is known about the causative role of I/R- induced microcirculatory disturbance on the manifestation of postischemic reperfusion in- jury. Therefore, the intention of the study was to assess changes of hepatic microvascular perfu- sion (intravital fluorescence microscopy) as related to hepatic morphology (light/electron mi- croscopy), hepatocelular integrity (serum as- partate aminotransferase (AST) and alanine ami- notransferase (ALI) activities), and excretory function (bile flow). Sprague-Dawley rats were subjected to 20 minutes (group B, n = 9) and 60 minutes (group C, n = 9) of left hepatic lobar is- chemia folowed by 60 minutes of reperfusion. Sham-operated animals without ischemia served as controls (group A, n = 10). Lobar ischemiafor 20 minutes folowed by reperfusion resulted in a significant reduction ofsinusoidalperfusion rate (93.9 ± 1.4%; P < 0.05) and a decrease in eryth- rocyte flux (90.0 + 5.6%) when compared with controls (99.4 ± 0.2 and 97.9 ± 2.7%). This was accompanied by a significant increase of serum AST and ALT activities (P < 0.05) and a reduction of bile flow (P < 0.05). Prolongation of lobar is- chemia (group C, 60 minutes) aggravated post- ischemic reperfusion injury (sinusoidal perfu- sion rate: 87.4 ± 2.9%; erythrocyte flux: 62.1 + 8.4%) and was paraUeled by severed hepatocel- lular damage. Electron microscopy ofpostische- mic tissue demonstrated alteration of nonparen- chymal ceUs (swelling of sinusoidal lining ceUs and widening of Disse's space) and substantial parenchymal ceU damage (sweUing of mitochon- dnia, disarrangement ofrough endoplasmatic re- ticulum, vacuolization, complete cytoplasmic de- generation). Initial postiscbemic increase in serumASTandALTactivities and reduction ofbile flow directly correlated with the extent of micro- circulatory failure (P < 0.01), ie, impairment of sinusoidalperfusion and decrease oferythrocyte flux, indicating the decisive role ofmicrovascular perfusionfailurefor the manifestation ofhepatic tissue damage and liver dysfunction. (Am J Pathol 1994, 145:1421-1431) Temporary interruption of blood flow to the liver is of- ten unavoidable during operations for extensive injury of the liver or for major liver resection.1-3 Following ischemia and reperfusion (I/R), transient dysfunction of the liver occurs, presumably due to the high sus- ceptibility of the liver to ischemia and cell injury ad- ditionally induced by reperfusion.4 While the effects of ischemia/hypoxia on liver metabolism and hepatocel- lular damage have been extensively studied during the last decade,4'5 only recently the focus of interest has turned toward postischemic reperfusion and its impact on l/R-induced hepatic injury. A variety of ex- perimental studies have shown that postischemic re- perfusion is associated with insufficient energy sup- ply and subsequent decline of hepatic tissue oxygenation,6 impaired ATP regeneration,7'8 and in- complete recovery of hepatocellular excretory func- tion.9'10 However, little is known about the causative role of I/R-induced microcirculatory disturbances on the development of postischemic liver damage.5 Supported by grants from the Deutsche Forschungsgemeinschaft (DFG Me 900/1-2) and the Friedrich-Baur Stiftung. Accepted for publication August 15, 1994. Address reprint requests to M. D. Menger, M.D., Institute for Clinical and Experimental Surgery, University of Saarland, Oscar- Orth-Strasse, D-66421 Homburg/Saar, Germany. 1421

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
American Journal ofPathology, Vol. 145, No. 6, December 1994Copyright © American Societyfor Investigative Pathology
Hepatic Microcirculatory Perfusion Failure Is aDeterminant of Liver Dysfunction in WarmIschemia-Reperfusion
Brigitte Vollmar,*t Julia Glasz,*Rosemarie Leiderer,* Stefan Post,t andMichael D. Menger*tFrom the Institutefor Surgical Research,* University ofMunich, the Institute for Clinical and ExperimentalSurgery,t University of Saarland, Homburg/Saar, and theDepartment of Surgery,* University ofHeidelberg, Germany
Hepatic ischemia-reperfusion (I/R) is character-ized by circulatory and metabolic derangements,liver dysfunction, and tissue damage. However,little is known about the causative role of I/R-induced microcirculatory disturbance on themanifestation of postischemic reperfusion in-jury. Therefore, the intention ofthe study was toassess changes of hepatic microvascular perfu-sion (intravital fluorescence microscopy) asrelated to hepatic morphology (light/electron mi-croscopy), hepatocelular integrity (serum as-partate aminotransferase (AST) and alanine ami-notransferase (ALI) activities), and excretoryfunction (bile flow). Sprague-Dawley rats weresubjected to 20 minutes (group B, n = 9) and 60minutes (group C, n = 9) of left hepatic lobar is-chemia folowed by 60 minutes of reperfusion.Sham-operated animals without ischemia servedas controls (group A, n = 10). Lobar ischemiafor20 minutesfolowed by reperfusion resulted in asignificant reduction ofsinusoidalperfusion rate(93.9 ± 1.4%; P < 0.05) and a decrease in eryth-rocyte flux (90.0 + 5.6%) when compared withcontrols (99.4 ± 0.2 and 97.9 ± 2.7%). This wasaccompanied by a significant increase of serumASTandALT activities (P < 0.05) and a reductionof bile flow (P < 0.05). Prolongation of lobar is-chemia (group C, 60 minutes) aggravated post-ischemic reperfusion injury (sinusoidal perfu-sion rate: 87.4 ± 2.9%; erythrocyte flux: 62.1 +
8.4%) and was paraUeled by severed hepatocel-lular damage. Electron microscopy ofpostische-mic tissue demonstrated alteration ofnonparen-
chymal ceUs (swelling of sinusoidal lining ceUsand widening of Disse's space) and substantialparenchymal ceU damage (sweUing ofmitochon-dnia, disarrangement ofrough endoplasmatic re-ticulum, vacuolization, complete cytoplasmic de-generation). Initial postiscbemic increase inserumASTandALTactivities andreduction ofbileflow directly correlated with the extent ofmicro-circulatory failure (P < 0.01), ie, impairment ofsinusoidalperfusion and decrease oferythrocyteflux, indicating the decisive roleofmicrovascularperfusionfailurefor the manifestation ofhepatictissue damage and liver dysfunction. (Am JPathol 1994, 145:1421-1431)
Temporary interruption of blood flow to the liver is of-ten unavoidable during operations for extensive injuryof the liver or for major liver resection.1-3 Followingischemia and reperfusion (I/R), transient dysfunctionof the liver occurs, presumably due to the high sus-ceptibility of the liver to ischemia and cell injury ad-ditionally induced by reperfusion.4 While the effects ofischemia/hypoxia on liver metabolism and hepatocel-lular damage have been extensively studied duringthe last decade,4'5 only recently the focus of interesthas turned toward postischemic reperfusion and itsimpact on l/R-induced hepatic injury. A variety of ex-perimental studies have shown that postischemic re-perfusion is associated with insufficient energy sup-ply and subsequent decline of hepatic tissueoxygenation,6 impaired ATP regeneration,7'8 and in-complete recovery of hepatocellular excretory func-tion.9'10 However, little is known about the causativerole of I/R-induced microcirculatory disturbances onthe development of postischemic liver damage.5
Supported by grants from the Deutsche Forschungsgemeinschaft(DFG Me 900/1-2) and the Friedrich-Baur Stiftung.Accepted for publication August 15, 1994.Address reprint requests to M. D. Menger, M.D., Institute for
Clinical and Experimental Surgery, University of Saarland, Oscar-Orth-Strasse, D-66421 Homburg/Saar, Germany.
1421
1422 Vollmar et alAJP December 1994, Vol. 145, No. 6
Therefore, the present study was performed to assessquantitatively hepatic microvascular perfusion failureinduced by I/R as related to liver dysfunction andhepatocellular disintegration, including alterations ofultrastructure of both parenchymal and nonparenchy-mal cells.
Materials and Methods
Animals and Preparation
In accordance with the German legislation on pro-tection of animals and the "Guide for the Care andUse of Laboratory Animals" (NIH publication no. 86-23, revised 1985), 36 male Sprague-Dawley ratsweighing 170-265 g (mean body weight (bw) 203 ±7 g) were used. After overnight fasting but with freeaccess to tap water the animals were anesthetized bychloralhydrate (36 mg-100 g bw-1 intraperitoneal)and atropine (0.25 mg subcutaneous). Tracheotomywas performed to facilitate spontaneous respiration(room air, flow rate 2 1-min-1). The animals wereplaced in supine position on a heating pad for main-tenance of body temperature between 36 and 37 C.Polyethylene catheters (PE-50, 0.58 mm inner diam-eter, Portex, Lythe, Kent, UK) were placed into thecarotid artery and jugular vein for assessment of mac-rohemodynamic parameters (mean arterial bloodpressure, MAP; heart rate, HR) as well as for with-drawal of arterial blood samples and injection of fluo-rescent dyes for in vivo microscopy. Supplementarychloralhydrate (3.6 mg-100 g bw-1) was given intra-peritoneally if required.
Laparotomy was performed via a transverse inci-sion. Ligamentous attachments from the liver to thediaphragm and abdominal wall were dissected. Forthe collection of bile the common bile duct was can-nulated with a PE-50 catheter. Left hepatic lobar is-chemia was induced by clamping the left hepatic ar-tery and the left portal branch. The ischemic periodof either 20 or 60 minutes was followed by reperfusionfor a total of 60 minutes. After 45 minutes reperfusion,the animals were positioned on their left side and theleft liver lobe was exteriorized and placed on a me-chanical stage for intravital fluorescence microscopy(IVM). The stage was adjusted to minimize tension onthe lobe, to provide a flat surface for microscopic vis-ualization, and to minimize respiratory movement.The liver surface was moistened with saline and cov-ered with Saran wrap to prevent evaporation and theinfluence of the ambient air. Sham-operated animals,undergoing the same procedures without induction ofischemia, served as controls.
IVM
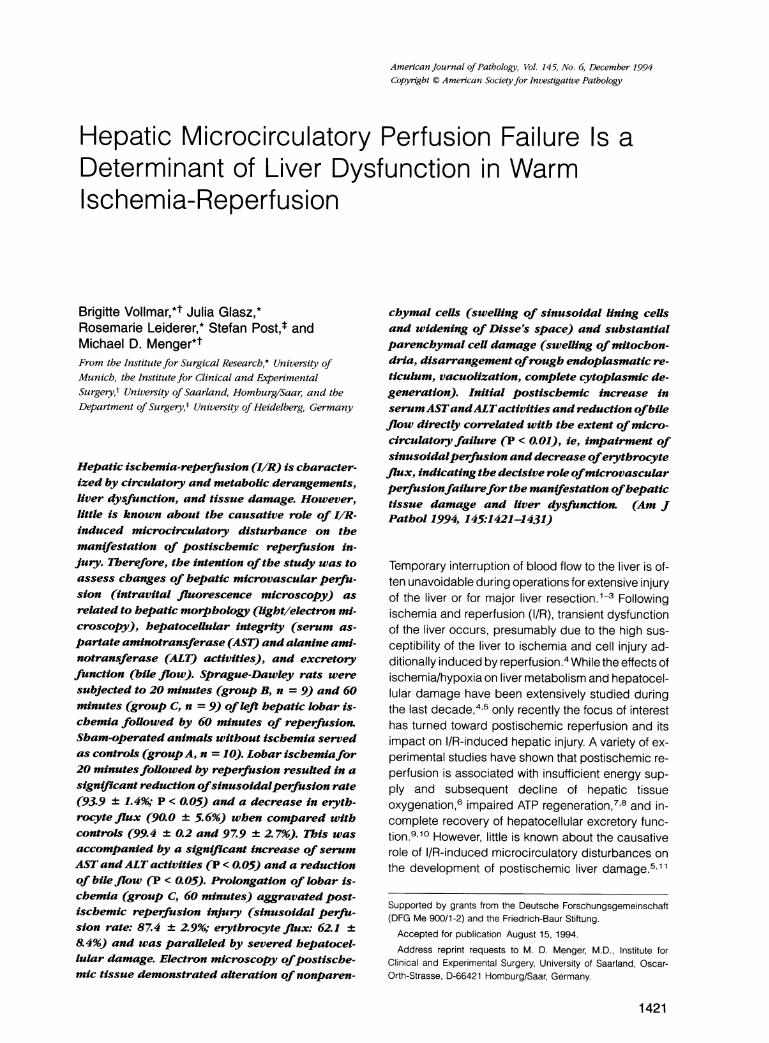
After 45 to 60 minutes of postischemic reperfusion,IVM was performed using a modified Leitz-Orthoplanmicroscope (Leitz, Wetzlar, FRG) and epi-illuminationtechnique.12-14 Microscopic images were registeredby a charge coupled device video camera (FK 6990;Prospective Measurements Inc., San Diego, CA) andrecorded on videotape (VO-5800 PS; Sony GmbH,Munich, FRG). Using long-distance and water-immersion objectives (Fluotar 1 0x/0.30; W 25x/0.60,Leitz, Wetzlar, FRG) magnifications of X280 andx700 were achieved on the video screen (PVM-1442QM, diagonal: 330 mm, Sony GmbH, Munich, FRG).For contrast enhancement sodium fluorescein (2pmol*kg-1; Fa. Merck, Darmstadt, FRG) was injectedintravenously and visualized by an 12/3 filter (450 to490 nm/>515 nm, excitation/emission wavelength) toassess lobular and sinusoidal perfusion (Figure 1, Aand B).
Quantification of microhemodynamic parameterswas performed offline by frame-to-frame analysis ofthe videotaped images. Lobular perfusion was ana-lyzed by scanning a region of interest containing atotal of 100 lobules at a magnification of x280 (Figure1A). According to hepatocellular uptake of fluores-cent dye, lobules were graded in three categories: not
Figure 1. Epi-illumination in vivo microscopy of the rat liver undercontrol conditions: (A) lobular perfusion and (B) sinusoidal perfu-sion after contrast enhancement with sodium fluorescein (2jmol kg-' i.v.). Bloodflow is directedfrom periportal (*) to midzonaland pericentral sinusoids and drains into postsinusoidal venules (v).Bars represent 100u and 504i, respectively.
Hepatic Reperfusion Injury 1423AJP December 1994, Vol. 145, No. 6
perfused (no staining), irregularly perfused (patchystaining), and well perfused (homogeneous stainingwith typical periportal enhancement), and lobular per-fusion was expressed by an index calculated by(Ng + 0.5 Ni)/Nt, where Ng represents the number ofwell perfused, N, the number of irregularly perfused(perfused area of the lobule <50%), and Nt the totalnumber of lobules analyzed. This index equals 1 if alllobules are well perfused and 0 in case of no perfu-sion at all.
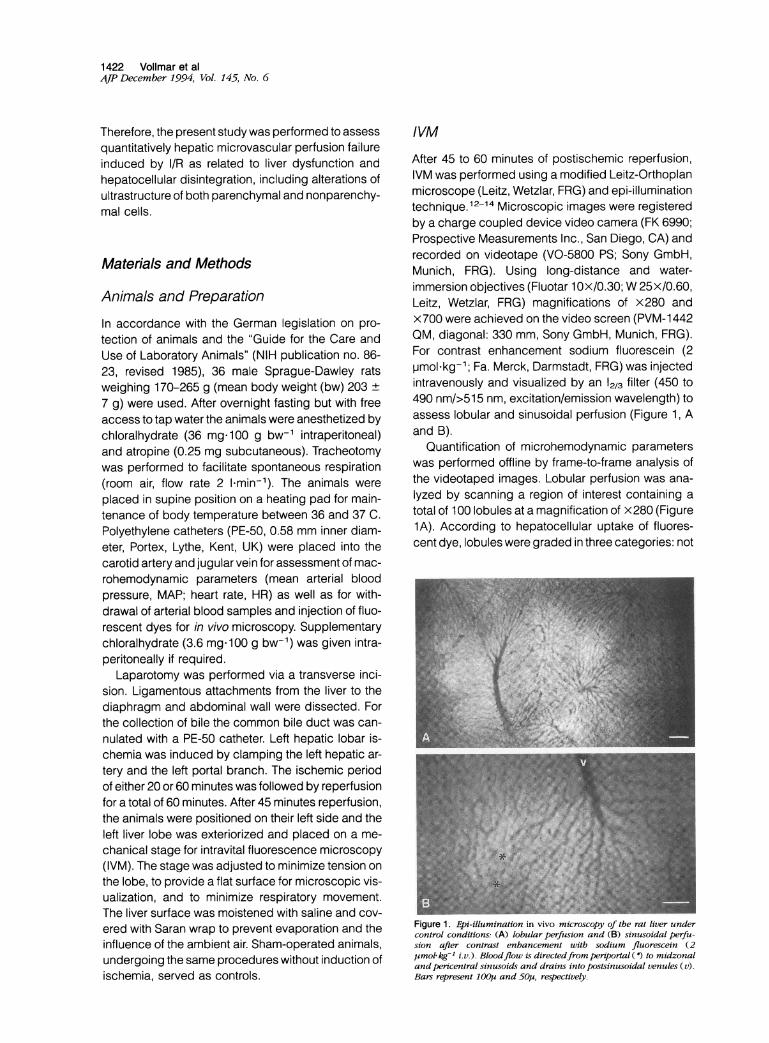
At a magnification of x700 sinusoidal perfusionwas assessed from 10 to 15 liver lobules within theregion of interest over a time period of 30 to 60 sec-onds each (Figure 1 B). Sinusoidal perfusion rate wasdetermined by counting the number of perfused si-nusoids and is expressed as percentage of all sinu-soids visible (Figure 2). A sinusoid was defined as aperfused sinusoid if red blood cells (visualized bytheir negative contrast) passed the sinusoid withinthe observation period of 30 to 60 seconds. In addi-tion, sinusoidal perfusion rate was determined forperiportal, midzonal, and pericentral zones by divid-ing the sinusoids into three segments of equal length(Figure 2).14
Laser Doppler Flowmetry (LDF)
Erythrocyte flux (aU, arbitrary units) was assessed bymeans of LDF (MBF 3D, semiconductor laser diode,780 to 820 nm, 2 mW; Moor Instruments, Axminster,
- - - - - -
peiiortal
- - - - - -
Figure 2. Schematic drawing of a video image of heptvisualized by IVM. Sinusoidal bloodflow is directedfronmidzonal and pericentral and is drained into the avenule. Sinusoidal perfusion rate was determined bynumber ofperfused sinusoids and is expressed as percetnusoids visible. A sinusoid was defined as a perfused siblood cells passed the sinusoid within the observation p60 seconds. Analyses were performed in peniportal, m
pericentral zones by dividing the sinusoids into thresequal length. The drawing displays perfusion failure inand midzonal segments ofone sinusoid (-), while all oare perfused (0). Therefore, the example given in this d.sents sinusoidal perfusion rates of80% (4/5 perfused si;portal), 86% (617, midzonal), and 100% (7/7, pericentively.
UK) at five sites of interest on the surface of the leftliver lobe. The LDF technique was previously shownto be suitable for estimation of hepatic microvascularperfusion. 15'16 Calculation of erythrocyte flux wasbased on the product of erythrocyte velocity and con-centration within the tissue unit under investigation.Measurements were performed during baseline, atthe end of the ischemic period, and after 60 minutesof reperfusion. Values are given in % baseline.
Hepatocellular Excretory Function
Bile flow, as an indicator of ischemic injury,17 wasassessed via a catheter in the common bile ductduring baseline, ischemia and reperfusion, respec-tively. Average bile production is given in pl-ming-1liver tissue.
Sampling and Assays
Arterial blood samples were taken for analysis ofblood gases (ABL 300 Radiometer, Copenhagen,Denmark), hematocrit, and leukocyte count (CoulterCounter, T540, Hialeah, Florida). Serum aspartateaminotransferase (AST) and alanine aminotrans-ferase (ALT) activities, which reflect hepatocellulardamage,18 were determined by standard spectro-photometric procedures in samples collected fromthe aorta at the end of reperfusion (60 minutes). Aftercollection of arterial blood samples, rats were sacri-ficed and the livers removed for determination of wetweight.
Experimental Groups and Protocol
The animals were divided into three groups: Nonis-midzonal chemic animals served as controls (group A, n = 10)
-_
- - - - -and underwent the identical experimental protocolexcept for clamping of the hepatic vessels (60 min-
perkentral utes sham-ischemia). Animals of group B and C un-- _- - - - - derwent left hepatic lobar ischemia for 20 minutes
(n = 9) and 60 minutes (n = 9), respectively, followedby a 60-minute reperfusion period.
atic sinusoids After a 30-minute stabilization period, baseline re-n peiportal to,ostsinusoidal cording of macrohemodynamics (MAP, HR) and LDFcounting the was performed. Arterial blood samples were taken for,itage of all si-inusoid if red determination of blood gases, hematocrit, and leu-eriod of30 to kocyte count. Ischemia was followed by 60 minutes oficdzonal, and? segments of reperfusion with assessment of macrohemodynamicthepenportal parameters, IVM, and LDF within the last 15 minutesther sinusoids'rawing repre- of reperfusion. The animals were sacrificed by arterialnusoids, pen- exsanguination for sampling of blood (blood gases,itral, respec-
hematocrit, leukocyte count, and enzymes).

1424 Vollmar et alAJP December 1994, Vol. 145, No. 6
Light/Electron Microscopy
In additional animals aorta and portal vein were can-nulated after 60 minutes of reperfusion following 60minutes of left lobar ischemia (n = 5) or sham-ischemia (n = 3, control). Perfusion-fixation of hepatictissue was performed using a 5% glutaraldehyde/4%paraformaldehyde mixture in phosphate buffer (pH7.4) at a constant pressure <15 cm H20. Specimenswere cut from the left liver lobe and blocks were dicedinto 1-mm cubes. The samples were stored in fixativefor 2 to 3 days prior to further processing. Specimenswere postfixed with osmium tetroxide, dehydrated ingraded alcohol, and embedded in Epon 812. Ultra-thin sections were cut on the Reichert-ultramicrotomeand contrasted with uranyl acetate and lead citrate forelectron microscopy. Stained sections were reviewedin a Zeiss EM900 electron microscope operating atKV 80. Semithin (1 -p) sections were stained with 0. 1%toluidine blue for light microscopy. A total of 200 sec-tions were examined by light and electron micros-copy, respectively.
Statistics
All data are expressed as mean ± SEM. Differencesbetween groups were assessed by use of theKruskal-Wallis analysis of variance (overall differ-ence) and the Mann-Whitney U-test (pairwise com-parison). To test for time effects in each group sepa-rately, Friedman rank analysis of variance followed byWilcoxon matched pairs test was applied. The level ofthe tests was adjusted to take account for multiplecomparisons. Overall statistical significance was setat P < 0.05. Correlations between enzyme activities,bile flow, and hepatic microcirculation were testedusing linear regression analysis. Statistics were per-formed using the software package CSS (CompleteStatistical System, StatSoft, Inc., Tulsa, OK).
Results
Systemic Circulatory Parameters
Sham-operated animals (controls, group A) as well asanimals subjected to lobar ischemia (groups B and C)maintained stable macrohemodynamic conditionsthroughout the experiment (MAP, 82 to 99 mm Hg; HR,390 to 417 minutes-1). Hematocrit remained un-changed in animals of groups A and B (43.5 + 1.5%and 44.8 + 1.9% versus baseline: 44.3 ± 1.2% and44.5 + 0.9%), whereas animals of group C showed asignificant (P< 0.05) increase of systemic hematocrit
after reperfusion (48.6 + 1.2%) when compared withpreischemic values (43.9 + 1.0%). Arterial bloodgases (PaO2: 93 to 118 mm Hg; PaCO2: 34 to 46 mmHg) and systemic leukocyte count (10.3 to 12.9 x 103mm3) did not change significantly in either of thegroups over the observation period.
IVM
Control animals (group A) revealed intact hepatic mi-crocirculation with regularly perfused lobules (indexof lobular perfusion: 1.0) and sinusoids (Figure 1, Aand B). Ischemia of 20 minutes (group B) or 60 min-utes (group C) did not result in lobular perfusion fail-ure after the 60-minute reperfusion period, as indi-cated by an index of lobular perfusion of 1.0 in bothgroups. However, hepatic I/R led to perfusion failureof individual sinusoids (Figure 3A) and loss of the in-tegrity of sinusoidal lining cells, as indicated by theextravasation of erythrocytes and, ultimately, pete-chial bleedings (Figure 3B).
Quantitative analysis of the hepatic microcircula-tion of sham-operated animals (group A) revealed asinusoidal perfusion rate of almost 100% (Figure 4).
Figure 3. Epi-illumination in vivo microscopy of the rat liver in is-chemia-reperfusion. Hepatic microcirculation is characterized by in-dividual sinusoids presenting with cessation of blood flow (*) (A).Prolongation of ischemia results in aggravation of microvascular I/Rinjury as evidenced by extravasation of erythrocytes/petechial bleed-ings (-) (B). Bars represent 50 , and 100 ,u respectively.
Hepatic Reperfusion Injury 1425AJP December 1994, Vol. 145, No. 6
_~~~~~~periportal midzonol pericentral (A
A B C A B C A B C A BC
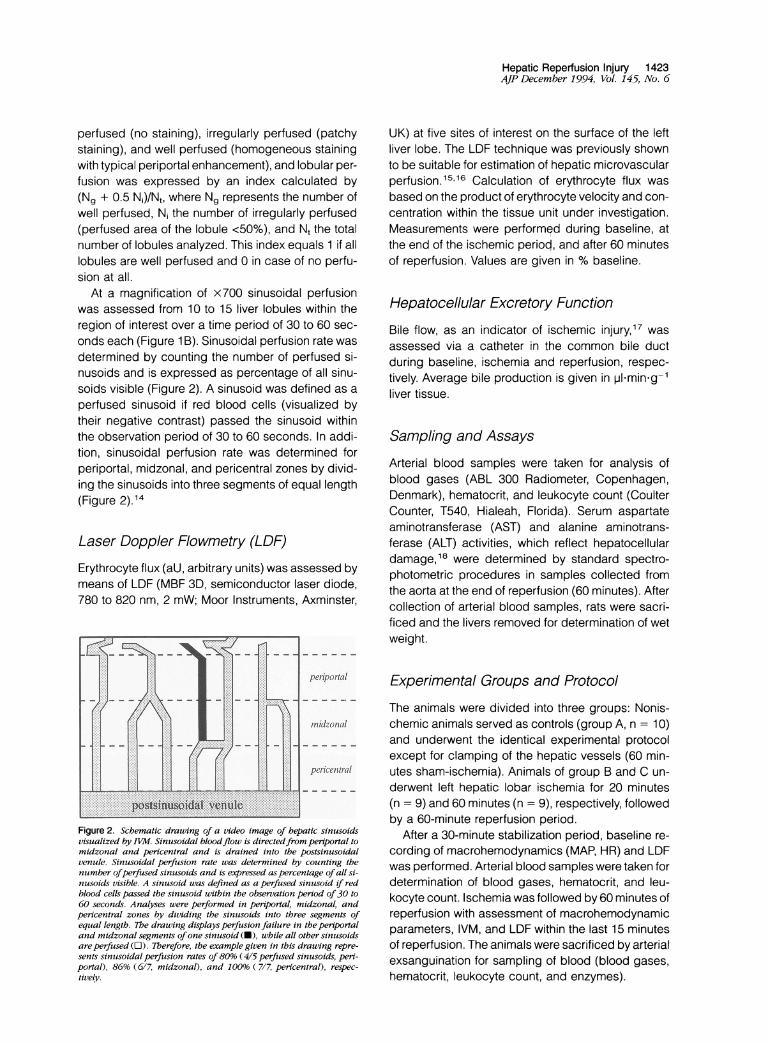
Figure 4. Hepatic sinuesoidal perfusion rate after 60 minuxtes of re-perfusion follouing 20 minutes (group B, n - 9) and 60 Cinutes(group C, n 9) of left lobar ischemia. Sham-operated animalsserved as Contro)ls (group A, n =10). Mlean + SFM. Mann-WhitneytJ test. P < 0.05 versus groop A.
Lobar isohemia of 20 and 60 minutes reperfusion re-sulted in a significant reduction (P < 0.05) of sinu-soidal perfusion rate to 93.9 ± 1.4%. Prolongation oflobar ischemia to 60 minutes (group C) aggravatedsinusoidal perfusion failure with only 87.4 ± 2.9% ofthe sinusoids being reperfused. Perfusion failure wasfound most pronounced in the periportal and mid-zonal segments of the sinusoids (Figure 4).
LDF
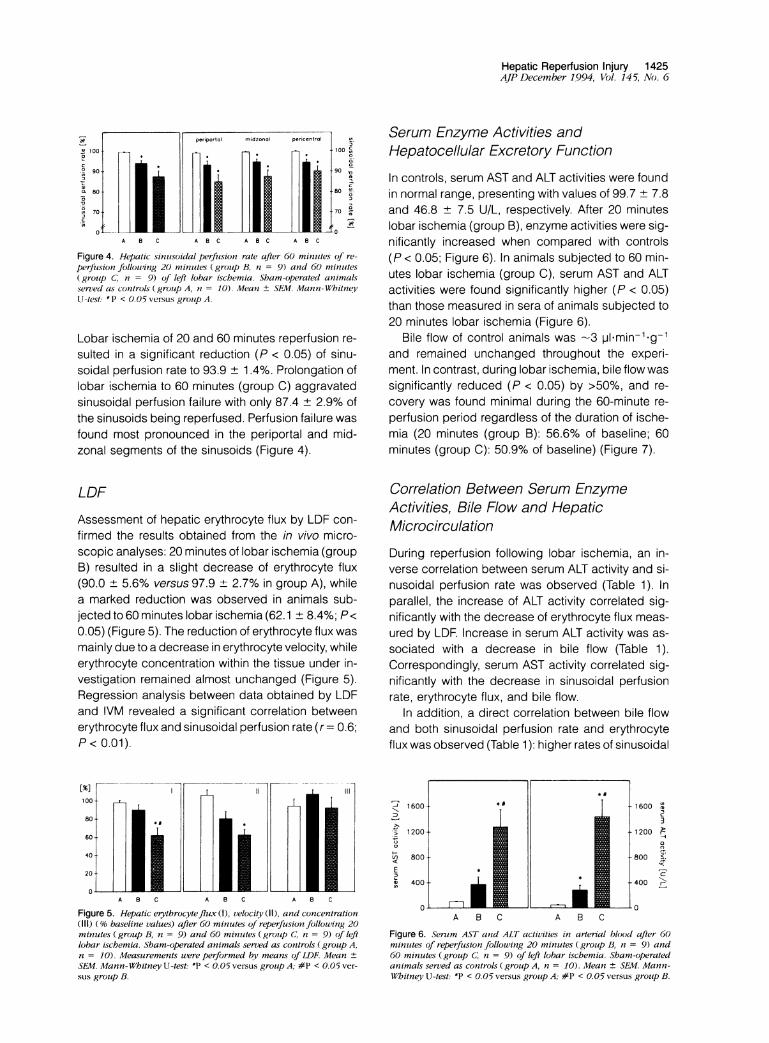
Assessment of hepatic erythrocyte flux by LDF con-firmed the results obtained from the in vivo micro-scopic analyses: 20 minutes of lobar ischemia (groupB) resulted in a slight decrease of erythrocyte flux(90.0 ± 5.6% versus 97.9 + 2.7% in group A), whilea marked reduction was observed in animals sub-jected to 60 minutes lobar ischemia (62.1 + 8.4%; P<0.05) (Figure 5). The reduction of erythrocyte flux wasmainly due to a decrease in erythrocyte velocity, whileerythrocyte concentration within the tissue under in-vestigation remained almost unchanged (Figure 5).Regression analysis between data obtained by LDFand IVM revealed a significant correlation betweenerythrocyte flux and sinusoidal perfusion rate (r= 0.6;P< 0.01).
lo
A C A B C A B C
Figure 5. Hepatic erythrocyteflux (1), velocity (II), and concentration(111) (0% baseline values) after 60 minutes of reperfusion following 20minutes (group B, n = 9) and 60 minutes (grouip C; n = 9) of leftlobar ischemia. Sham-operated animals served as controls (group A,n = 10). Measurements were performed by means of LDF. Mean +
SEM. Mann-Whitney U-test: *P < 0.05 versus grotup A; #P < 0.05 ver-
sus group B.
Serum Enzyme Activities andHepatocellular Excretory Function
In controls, serum AST and ALT activities were foundin normal range, presenting with values of 99.7 + 7.8and 46.8 ± 7.5 U/L, respectively. After 20 minuteslobar ischemia (group B), enzyme activities were sig-nificantly increased when compared with controls(P < 0.05; Figure 6). In animals subjected to 60 min-utes lobar ischemia (group C), serum AST and ALTactivities were found significantly higher (P < 0.05)than those measured in sera of animals subjected to20 minutes lobar ischemia (Figure 6).
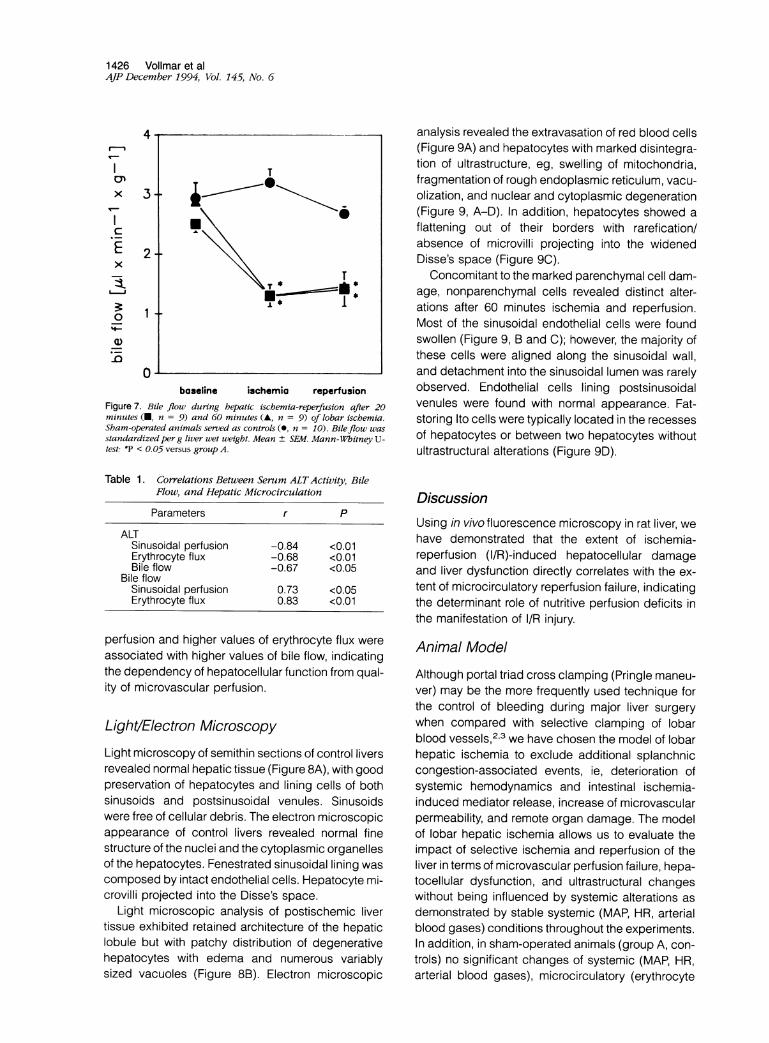
Bile flow of control animals was -3 pI*min-'-g-1and remained unchanged throughout the experi-ment. In contrast, during lobar ischemia, bile flow wassignificantly reduced (P < 0.05) by >50%, and re-covery was found minimal during the 60-minute re-perfusion period regardless of the duration of ische-mia (20 minutes (group B): 56.6% of baseline; 60minutes (group C): 50.9% of baseline) (Figure 7).
Correlation Between Serum EnzymeActivities, Bile Flow and HepaticMicrocirculation
During reperfusion following lobar ischemia, an in-verse correlation between serum ALT activity and si-nusoidal perfusion rate was observed (Table 1). Inparallel, the increase of ALT activity correlated sig-nificantly with the decrease of erythrocyte flux meas-ured by LDF. Increase in serum ALT activity was as-sociated with a decrease in bile flow (Table 1).Correspondingly, serum AST activity correlated sig-nificantly with the decrease in sinusoidal perfusionrate, erythrocyte flux, and bile flow.
In addition, a direct correlation between bile flowand both sinusoidal perfusion rate and erythrocyteflux was observed (Table 1): higher rates of sinusoidal
= 9
A9NHC
D! Wllib Mi Mim II!HIF1911mffl 9YIDffl WH9! Wg iimmffl
* fflfflr W_
__
A B C
1600 X
3
2.e-1200 r
-800 <.lc
-400 \
-0
Figure 6. Senrm AST and ALT activities in arterial blood after 60minuites of reperfusion following 20 minutes (group B, n = 9) and60 minutes (group C; n = 9) of left lobar ischemia. Sham-operatedanimals served as conttrols (group A, n = 10). Mean ± SEM. Mann-Whitney U-test:- P < 0.05 versus group A; #P < 0.05 versus group B.
1426 Vollmar et alAJP December 1994, Vol. 145, No. 6
4
I
x
Ex
0'4--
Q1)
3-
1
0baseline ichemia reperfusion
Figure 7. Bile flow during hepatic ischemia-reperfusion after 20minutes (U, n = 9) and 60 minutes (A, n = 9) of lobar ischemia.Sham-operated animals served as controls (0, n = 10). Bileflow wasstandardized perg liver wet weight. Mean ± SEM. Mann-Whsitney U-test. *P < 0.05 versus group A.
Table 1. Correlations Between Serum ALTActivity, BileFlow, and Hepatic Microcirculation
Parameters r P
ALTSinusoidal perfusion -0.84 <0.01Erythrocyte flux -0.68 <0.01Bile flow -0.67 <0.05
Bile flowSinusoidal perfusion 0.73 <0.05Erythrocyte flux 0.83 <0.01
perfusion and higher values of erythrocyte flux wereassociated with higher values of bile flow, indicatingthe dependency of hepatocellular function from qual-ity of microvascular perfusion.
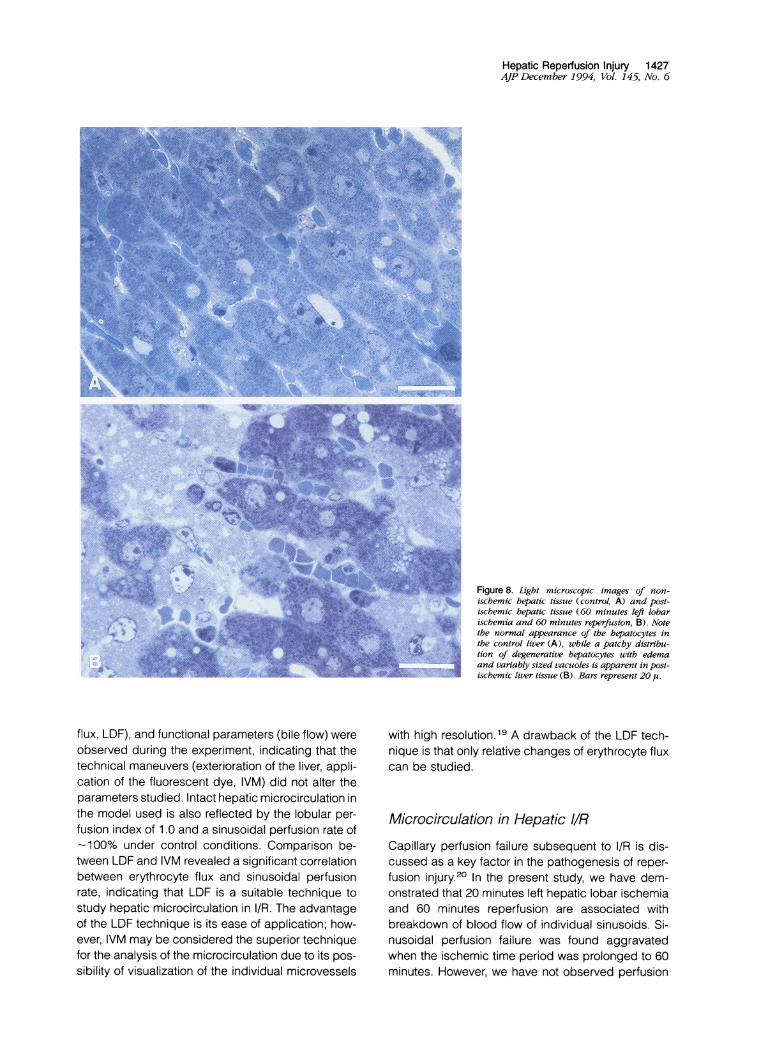
Light/Electron MicroscopyLight microscopy of semithin sections of control liversrevealed normal hepatic tissue (Figure 8A), with goodpreservation of hepatocytes and lining cells of bothsinusoids and postsinusoidal venules. Sinusoidswere free of cellular debris. The electron microscopicappearance of control livers revealed normal finestructure of the nuclei and the cytoplasmic organellesof the hepatocytes. Fenestrated sinusoidal lining wascomposed by intact endothelial cells. Hepatocyte mi-crovilli projected into the Disse's space.
Light microscopic analysis of postischemic livertissue exhibited retained architecture of the hepaticlobule but with patchy distribution of degenerativehepatocytes with edema and numerous variablysized vacuoles (Figure 8B). Electron microscopic
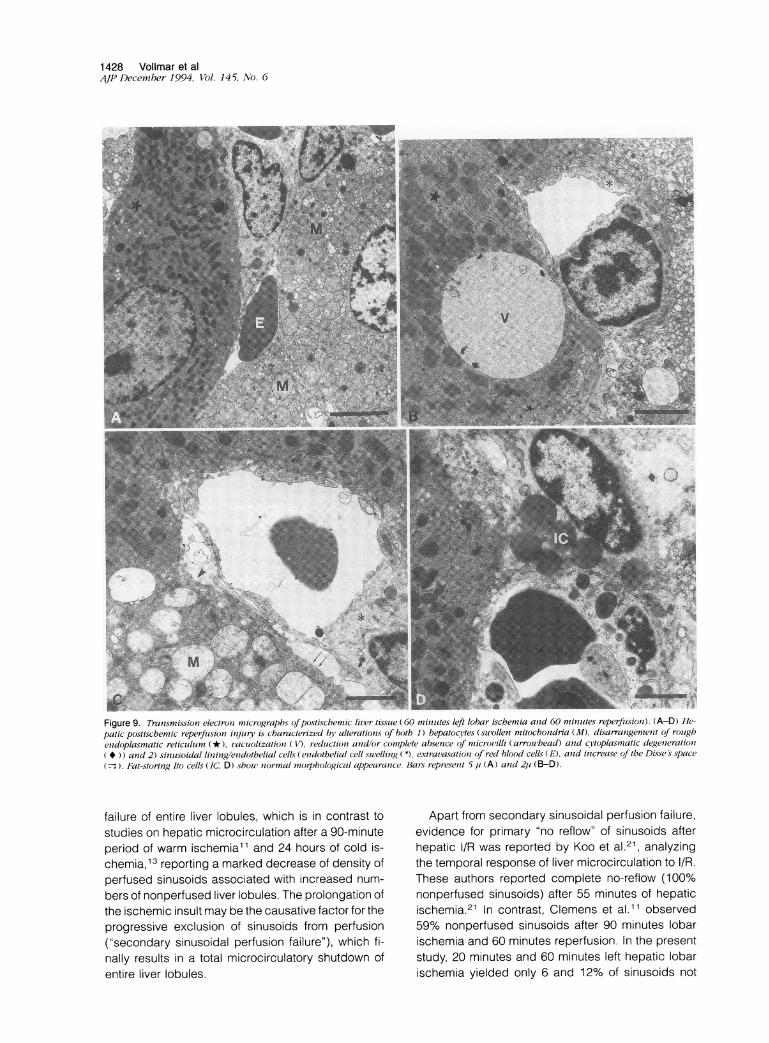
analysis revealed the extravasation of red blood cells(Figure 9A) and hepatocytes with marked disintegra-tion of ultrastructure, eg, swelling of mitochondria,fragmentation of rough endoplasmic reticulum, vacu-olization, and nuclear and cytoplasmic degeneration(Figure 9, A-D). In addition, hepatocytes showed aflattening out of their borders with rarefication/absence of microvilli projecting into the widenedDisse's space (Figure 9C).
Concomitant to the marked parenchymal cell dam-age, nonparenchymal cells revealed distinct alter-ations after 60 minutes ischemia and reperfusion.Most of the sinusoidal endothelial cells were foundswollen (Figure 9, B and C); however, the majority ofthese cells were aligned along the sinusoidal wall,and detachment into the sinusoidal lumen was rarelyobserved. Endothelial cells lining postsinusoidalvenules were found with normal appearance. Fat-storing Ito cells were typically located in the recessesof hepatocytes or between two hepatocytes withoutultrastructural alterations (Figure 9D).
DiscussionUsing in vivo fluorescence microscopy in rat liver, wehave demonstrated that the extent of ischemia-reperfusion (I/R)-induced hepatocellular damageand liver dysfunction directly correlates with the ex-tent of microcirculatory reperfusion failure, indicatingthe determinant role of nutritive perfusion deficits inthe manifestation of I/R injury.
Animal Model
Although portal triad cross clamping (Pringle maneu-ver) may be the more frequently used technique forthe control of bleeding during major liver surgerywhen compared with selective clamping of lobarblood vessels,2 we have chosen the model of lobarhepatic ischemia to exclude additional splanchniccongestion-associated events, ie, deterioration ofsystemic hemodynamics and intestinal ischemia-induced mediator release, increase of microvascularpermeability, and remote organ damage. The modelof lobar hepatic ischemia allows us to evaluate theimpact of selective ischemia and reperfusion of theliver in terms of microvascular perfusion failure, hepa-tocellular dysfunction, and ultrastructural changeswithout being influenced by systemic alterations asdemonstrated by stable systemic (MAP, HR, arterialblood gases) conditions throughout the experiments.In addition, in sham-operated animals (group A, con-trols) no significant changes of systemic (MAP, HR,arterial blood gases), microcirculatory (erythrocyte
T
T
1*
;~~~~~J \
Hepatic Reperfusion Injury 1427AJP December 1994, Vol. 145, No. 6
Figure 8. Light microscopic images of non-ischemic hepatic tissue (control, A) and post-ischemic hepatic tissue (60 minutes left lobarischemia and 60 minutes reperfusion, B). Notethe normal appearance of the hepatocytes inthe control liver (A), while a patchy distribu-tion of degenerative hepatocytes with edemaand variably sized vacuoles is apparent in post-ischemic liver tissue (B). Bars represent 20 jc.
flux, LDF), and functional parameters (bile flow) wereobserved during the experiment, indicating that thetechnical maneuvers (exterioration of the liver, appli-cation of the fluorescent dye, IVM) did not alter theparameters studied. Intact hepatic microcirculation inthe model used is also reflected by the lobular per-fusion index of 1.0 and a sinusoidal perfusion rate of-100% under control conditions. Comparison be-tween LDF and IVM revealed a significant correlationbetween erythrocyte flux and sinusoidal perfusionrate, indicating that LDF is a suitable technique tostudy hepatic microcirculation in I/R. The advantageof the LDF technique is its ease of application; how-ever, IVM may be considered the superior techniquefor the analysis of the microcirculation due to its pos-sibility of visualization of the individual microvessels
with high resolution.19 A drawback of the LDF tech-nique is that only relative changes of erythrocyte fluxcan be studied.
Microcirculation in Hepatic IIRCapillary perfusion failure subsequent to l/R is dis-cussed as a key factor in the pathogenesis of reper-fusion injury.20 In the present study, we have dem-onstrated that 20 minutes left hepatic lobar ischemiaand 60 minutes reperfusion are associated withbreakdown of blood flow of individual sinusoids. Si-nusoidal perfusion failure was found aggravatedwhen the ischemic time period was prolonged to 60minutes. However, we have not observed perfusion
1428 Vollmar et al,jP December 1994, Vol. 145, No. 6
Figure 9. Transmission electroni micrographs ofpostischemic liver tissue (60 minutes left lobar ischemia and 60 minutes reperfiisioni). (A-D) He-patic postiscbebmic reperfusion in ury is characterized bl, alterations of both 1) hepatocntes (swollen mitochondnia (M), disarr^angement ofJ roiughenidoplasmatic reticulum (*), tacuolization (V, reduction and/or complete absence of micro/illi (arrouhead) anid cvtoplasmnatic degeneration( * )) and 2) sinusoidal lining/endothelial cells (endotbelial cell swelling (*), extravasation of red blood cells (F), and increase of the Disse s space( P)Fat-storing Ito cells (IC, D) shouw niormal ?notpbological appearanice. Bars represent 5 u (A) anid 2;i (B-D).
failure of entire liver lobules, which is in contrast tostudies on hepatic microcirculation after a 90-minuteperiod of warm ischemia11 and 24 hours of cold is-chemia,13 reporting a marked decrease of density ofperfused sinusoids associated with increased num-
bers of nonperfused liver lobules. The prolongation ofthe ischemic insult may be the causative factor for theprogressive exclusion of sinusoids from perfusion("secondary sinusoidal perfusion failure"), which fi-
nally results in a total microcirculatory shutdown ofentire liver lobules.
Apart from secondary sinusoidal perfusion failure,evidence for primary "no reflow" of sinusoids afterhepatic I/R was reported by Koo et al.21, analyzingthe temporal response of liver microcirculation to I/R.These authors reported complete no-reflow (100%nonperfused sinusoids) after 55 minutes of hepaticischemia.21 In contrast, Clemens et al.11 observed59% nonperfused sinusoids after 90 minutes lobarischemia and 60 minutes reperfusion. In the presentstudy, 20 minutes and 60 minutes left hepatic lobarischemia yielded only 6 and 12% of sinusoids not

Hepatic Reperfusion Injury 1429AJP December 1994, Vol. 145, No. 6
perfused after a 60-minute reperfusion period. Be-sides variations of the ischemia and reperfusion timeperiods studied, the different models and methodsused may account for these conflicting results. Inparticular, the use of appropriate fluorescent dyesfor the visualization of sinusoidal perfusion (sodiumfluorescein, fluorescein isothiocyanate conjugatedalbumin) may provide a more accurate analysis ofsinusoidal perfusion when compared with epi-illumi-nation microscopy without contrast enhancement(autofluorescence).
The extent of sinusoidal perfusion failure after 1hour warm hepatic I/R (12% nonperfused sinusoids)was found to be in a similar range when comparedwith the extent of perfusion failure after 1 hour coldI/R (16% nonperfused sinusoids; storage in Euro-Collins solution (EC)),22 although the experimentswith cold ischemia included the transplantation pro-cedure and a short warm ischemic period duringimplantation. In parallel to the results of the presentstudy (warm I/R), prolongation of cold ischemia (8hours EC) resulted in a marked reduction of sinusoi-dal perfusion (52% nonperfused sinusoids),22 indi-cating that also in cold I/R the extent of postischemicperfusion failure depends on the ischemic time pe-riod applied. However, the quality of sinusoidal per-fusion in liver transplants depends mainly on thepreservation conditions. With the use of University ofWisconsin solution and Carolina rinse microvascularinjury after 24 hours cold ischemia can be effectivelyattenuated to 8.5% of nonperfused sinusoids,13 indi-cating superior microvascular perfusion conditionswhen compared with 60 minutes of warm I/R.
Several mechanisms may be proposed to contrib-ute to postischemic sinusoidal perfusion failure, in-cluding microvascular accumulation and adherenceof leukocytes, intracellular edema formation, and in-travascular hemoconcentration. Postischemic accu-mulation of leukocytes in outflow (postsinusoidal)venules23,24 may alter sinusoidal perfusion due to anincrease in blood viscosity,25 and hence vascular re-sistance.26 In addition, the increased incidence of in-travascular plugging by leukocytes has been re-ported to cause complete cessation of blood flow insome liver sinusoids.27 However, Ferguson and co-workers28 have demonstrated that, although at thewhole organ level leukocyte accumulation appears tocorrelate well with microvascular damage, this doesnot necessarily reflect accumulation at sites present-ing with nonperfused sinusoids. Therefore, these au-thors conclude that leukocyte-independent factorsare likely to be of considerable quantitative impor-tance in the manifestation of microvascular injury dur-ing hepatic I/R.28
In fact, in the present study we could demonstrateintracellular edema formation and intravascularhemoconcentration (increase of hematocrit), whichhave to be considered to adversely affect postische-mic nutritive perfusion. The ischemia-induced energydeficiency and the consecutive failure of active trans-membrane ion transport result in intracellularedema5,29 with swelling of sinusoidal lining (endothe-lial) cells and, hence, lumenal narrowing, which thenalters the microcirculation during reperfusion. Thishypothesis is supported by the fact that treatment withATP-MgCI2 normalizes both transmembrane iontransport and hepatic intracellular water content30and attenuates postischemic sinusoidal perfusionfailure. 11
Although cellular damage due to ischemia isknown to be most pronounced in the pericentral area,this ischemia/hypoxia-dependent hepatocellularevent must not spatially correlate with reperfusion-induced microcirculatory deteriorations. There maybe several causative factors responsible for the mostprominent sinusoidal perfusion failure in the periportalarea. The lumenal narrowing due to swelling of endo-thelial cells will primarily result in perfusion deficits insinusoids of the periportal areas, since periportal si-nusoids have, already under physiological condi-tions, smaller diameters with a more tortuous path andhigher flow resistance with the consequence of lowerblood flow when compared with sinusoids of the mid-zonal and pericentral areas.31 In addition, about two-thirds of the Kupffer cells are located in the periportalarea, and these macrophages are generally of largersize than pericentrally located macrophages. I/R isknown to activate Kupffer cells with subsequent re-lease of inflammatory mediators (oxygen radicals, cy-tokines, arachidonic acid metabolites, platelet acti-vating factor), which themselves can causeendothelial damage and thus impairment of micro-vascular perfusion.5 This view is further supported bythe findings of Suematsu and coworkers,32 demon-strating in a low-flow hypoxia model in the perfusedrat liver the onset of oxidative stress in the upstreamregions of the hepatic microcirculatory unit.
Correlation Between Serum EnzymeActivities, Bile Flow, and Microcirculationin Hepatic l/R
l/R-induced hepatocellular damage was associatedwith reduction of liver function, demonstrated by thesignificant correlation between the impairment of bileflow and the elevation of serum AST and ALT activi-ties. This finding parallels previous observations9"'0

1430 Vollmar et alAJP December 1994, Vol. 145, No. 6
demonstrating a linear relationship between bile flowand hepatocellular level of ATP. In addition, the abilityof the liver to regenerate ATP during postischemicrestoration of hepatic blood flow has been reported todetermine tissue viability and survival rate.7 Interre-lation between insufficient energy supply via alteredperfusion and hepatocellular damage was hypoth-esized by Goto et al.6 Using reflectance spectropho-tometry in hepatic I/R, they observed a significant cor-relation between the increase of serum ALT levels andthe reduction of the index of blood oxygenation, whichwas suggested to reflect decreased blood flow and,consecutively, insufficient oxygen supply.6 This hy-pothesis is now verified by the results of the presentstudy, demonstrating significant correlation betweenthe extent of hepatocellular damage (increase in en-zyme activities) as well as hepatocellular dysfunction(decrease in bile flow) and hepatic microvascular per-fusion failure.
Alterations of Ultrastructure in Hepatic I/R
Ultrastructural analysis (electron microscopy) afterhepatic I/R revealed alterations of both parenchymaland nonparenchymal (endothelial) cells. Within thesinusoidal lining ultrastructural changes characteris-tically consisted of swelling of endothelial cells andwidening of the Disse's space. Loss of endothelialintegrity was indicated by the extravasation of redblood cells. These findings are consistent and extendobservations of previous studies, which have indi-cated by use of indirect techniques (release of purinenucleoside phosphorylase,33 formation of conju-gated dienes in nonparenchymal cell fractions34) theinvolvement of endothelial cell injury in the manifes-tation of postischemic liver failure. However, detach-ment of endothelial cells, characteristically seen aftercold I/R, was not observed. In addition, while injuryafter cold ischemia is known to involve primarily non-parenchymal cells, whereas parenchymal cells arerelatively spared,35 we could now demonstrate thatafter warm I/R the alterations of nonparenchymal cellsare accompanied by marked disintegration of theultrastructure of hepatocytes including swelling of mi-tochondria, disarrangement of the rough endoplas-matic reticulum, vacuolization, and complete cyto-plasmic degeneration.
In summary, reperfusion injury of the liver afterwarm ischemia is characterized by impaired sinusoi-dal perfusion with reduction of erythrocyte flux, hepa-tocellular damage, and excretory dysfunction. Pro-longation of ischemia aggravates h/R-inducedhepatic injury, which is characterized by ultrastruc-
tural changes including not only nonparenchymal butalso parenchymal cells. Significant correlation of l/R-induced hepatocellular damage and dysfunction withmicrocirculatory disturbances indicates the determi-nant role of intact microcirculation for postischemicrecovery of organ function.
References1. Pachter HL, Spencer FC, Hofstetter SR, Coppa GF:
Experience with the finger fracture technique toachieve intra-hepatic hemostasis in 75 patients withsevere injuries of the liver. Ann Surg 1983, 197:771-777
2. Delva E, Camus Y, Nordlinger B, Hannoun L, Parc R,Deriaz H, Lienhart A, Huguet C: Vascular occlusionsfor liver resections. Operative management and toler-ance to hepatic ischemia: 142 cases. Ann Surg 1989,209:211-218
3. Huguet C, Gavelli A, Chieco A, Bona S, Harb J, Jo-seph JM, Jobard J, Gramaglia M, Lassere M: Liver is-chemia for hepatic resection: where is the limit? Sur-gery 1992, 111:251-259
4. Hasselgren PO: Prevention and treatment of ischemiaof the liver. Surg Gynecol Obstet 1987, 164:187-196
5. Chaudry IH: Cellular mechanisms in shock and ische-mia and their correction. Am J Physiol 1983, 245:Rl 17-R134
6. Goto M, Kawano S, Yoshihara H, Takei Y, Hijioka T,Fukui H, Matsunaga T, Oshita M, Kashiwagi T,Fusamoto H, Kamada T, Sato N: Hepatic tissue oxy-genation as a predictive indicator of ischemia-reperfusion liver injury. Hepatology 1992, 15:432-437
7. Marubayashi S, Takenaka M, Dohi K, Ezaki H, Ka-wasaki T: Adenine nucleotide metabolism during he-patic ischemia and subsequent blood reflow periodsand its relation to organ viability. Transplantation 1980,30:294-296
8. Wang WY, Taki Y, Morimoto T, Nishihira T, Yokoo N,Jikko A, Nishikawa K, Tanaka J, Kamiyama Y, OzawaK: Effects of partial ischemia and reflow on mitochon-drial metabolism in rat liver. Eur Surg Res 1988, 20:181-189
9. Kamiike W, Nakahara M, Nakao K, Koseki M, NishidaT, Kawashima Y, Watanabe F, Tagawa K: Correlationbetween cellular ATP level and bile excretion in the ratliver. Transplantation 1985, 39:50-55
10. Karwinski W, Husoy A-M, Farstad M, Soreide 0: Sixtyminutes of normothermic ischemia in the rat liver: cor-relation between adenine nucleotides and bile excre-tion. J Surg Res 1989, 46:99-103
11. Clemens MG, McDonagh PF, Chaudry IH, Baue AE:Hepatic microcirculatory failure following ischemiaand reperfusion: improvement with ATP-MgCI2. Am JPhysiol 1985, 248:H804-H811
12. Menger MD, Marzi I, Messmer K: In vivo fluorescencemicroscopy for quantitative analysis of the hepatic mi-
Hepatic Reperfusion Injury 1431AJP December 1994, Vol. 145, No. 6
crocirculation in hamsters and rats. Eur Surg Res1991, 23:158-169
13. Post S, Palma P, Rentsch M, Gonzalez AP, MengerMD: Differential impact of Carolina rinse and Univer-sity of Wisconsin solutions on microcirculation, leuko-cyte adhesion, Kupffer cell activity and biliary excre-tion after liver transplantation. Hepatology 1993, 18:1490-1497
14. Vollmar B, Lang G, Menger MD, Messmer K: Hyper-tonic hydroxyethyl starch restores hepatic microvas-cular perfusion in hemorrhagic shock. Am J Physiol1994, 266:H1927-H1934
15. Arvidsson D, Svensson H, Haglund U: Laser-Dopplerflowmetry for estimating liver blood flow. Am J Physiol1988, 254:G471-G476
16. Almond NE, Wheatley AM: Measurement of hepaticperfusion in rats by laser Doppler flowmetry. Am JPhysiol 1992, 262:G203-G209
17. Bowers BA, Branum GD, Rotolo FS, Watters CR, Mey-ers WC: Bile flow: an index of ischemic injury. J SurgRes 1987, 42:565-569
18. Nishimura T, Yoshida Y, Watanabe F, Koseki M,Nishida T, Tagawa K, Kawashima Y: Blood level of mi-tochondrial aspartate aminotransferase as an indica-tor of the extent of ischemic necrosis of the rat liver.Hepatology 1986, 6:701-707
19. Menger MD, Barker JH, Messmer K: Capillary bloodperfusion during postischemic reperfusion in striatedmuscle. Plast Reconstr Surg 1992, 89:1104-1114
20. Menger MD, Steiner D, Messmer K: Microvascularischemia/reperfusion injury in striated muscle: signifi-cance of "no-reflow". Am J Physiol 1992, 263:H1892-H1900
21. Koo A, Komatsu H, Tao G, Inoue M, Guth PH, KaplowitzN: Contribution of no-reflow phenomenon to hepaticinjury after ischemia-reperfusion: evidence for a role forsuperoxide anion. Hepatology 1992, 15:507-514
22. Marzi I, Knee J, Buhren V, Menger MD, Trentz 0: Re-duction of superoxide dismutase of leukocyte-endothelial adherence after liver transplantation. Sur-gery 1992, 111:90-97
23. Menger MD, MOller MJ, Friedl HP, Trentz 0, MessmerK: Ischemia-reperfusion injury of the liver: role of neu-trophils and xanthine oxidase. Host Defense Dysfunc-tion in Trauma, Shock and Sepsis. Edited by E Faist,JL Meakins, FW Schildberg. New York, Springer Pub-lishing, 1992, pp 539-544
24. Menger MD, Pelikan S, Steiner D, Messmer K: Micro-vascular ischemia/reperfusion injury in striated muscle:significance of "reflow-paradox". Am J Physiol 1992,263:H 1901-H 1906
25. Chien S: Role of blood cells in microcirculatory regula-tion. Microvasc Res 1985, 29:129-151
26. Braide M, Amundson B, Bagge U: Quantitative stud-ies on the influence of leukocytes on the vascular re-sistance in a skeletal muscle preparation. MicrovascRes 1984, 27:331-352
27. Koo A, Breit G, Intaglietta M: Leukocyte adherence inthe hepatic microcirculation in ischemia-reperfusion.Microcirculation in Circulatory Disorders. Edited by HManabe, BW Zweifach, K Messmer New York,Springer Publishing, 1988, pp 205-213
28. Ferguson D, McDonagh PF, Biewer J, Paidas CN, Cle-mens MG: Spatial relationship between leukocyte ac-cumulation and microvascular injury during reperfu-sion following hepatic ischemia. Int J Microcirc ClinExp 1993, 12:45-60
29. Leaf A: Cell swelling. A factor in ischemic tissue injury.Circulation 1973, 48:455-458
30. Ohkawa M, Chaudry IH, Clemens MG, Baue AE: Im-provement in water and electrolyte homeostasis byATP-MgCI2 after ischemia (abstract). Circ Shock 1982,9:162
31. Komatsu H, Koo A, Guth PH: Leukocyte flow dynam-ics in the rat liver microcirculation Microvasc Res1990, 40:1-13
32. Suematsu M, Suzuki H, Ishii H, Tsuchiya M: Paradoxof oxygen-radical-dependent cell injury in the hypoxicliver microcirculation. Prog Appl Microcirc 1993: 19:127-138
33. Rao PN, Walsh TR, Makowka L, Rubin RS, Weber T,Snyder JT, Starzl E: Purine nucleoside phosphorylase:a new marker for free oxygen radical injury to theendothelial cell. Hepatology 1990, 11:193-198
34. Walsh TR, Rao PN, Makowka L, Starzl TE: Lipid per-oxidation is a nonparenchymal cell event with reperfu-sion after prolonged liver ischemia. J Surg Res 1990,49:18-22
35. McKeown CMB, Edwards V, Phillips J, Harvey PRC,Petrunka CN, Strasberg SM: Sinusoidal lining celldamage: the critical injury in cold preservation of liverallografts in the rat. Transplantation 1988, 46:178-191
Related Documents











