


www.elsevier.com/locate/ynimg
NeuroImage 23 (2004) 167–174
Voxel-based morphometry of unilateral temporal lobe epilepsy reveals
abnormalities in cerebral white matter
Alan B. McMillan,a,* Bruce P. Hermann,b Sterling C. Johnson,c Russ R. Hansen,b
Michael Seidenberg,d and Mary E. Meyerande
aDepartment of Medical Physics, University of Wisconsin-Madison, Madison, WI 53706, USAbDepartment of Neurology, University of Wisconsin-Madison, Madison, WI 53706, USAcVA Medical Center and Department of Medicine, University of Wisconsin-Madison, Madison, WI 53706, USAdDepartment of Psychology, Chicago Medical School, North Chicago, IL 60064, USAeDepartment of Medical Physics, University of Wisconsin-Madison, Madison, WI 53706, USA
Received 16 January 2004; revised 22 April 2004; accepted 5 May 2004
Voxel-based morphometric (VBM) investigations of temporal lobe
epilepsy have focused on the presence and distribution of gray matter
abnormalities. VBM studies to date have identified the expected
abnormalities in hippocampus and extrahippocampal temporal lobe, as
well as more diffuse abnormalities in the thalamus, cerebellum, and
extratemporal neocortical areas. To date, there has not been a
comprehensive VBM investigation of cerebral white matter in nonle-
sional temporal lobe epilepsy. This study examined 25 lateralized
temporal lobe epilepsy patients (13 left, 12 right) and 62 healthy
controls in regard to both temporal and extratemporal lobe gray and
white matter. Consistent with prior reports, gray matter abnormalities
were evident in ipsilateral hippocampus and ipsilateral thalamus.
Temporal and extratemporal white matter was affected ipsilateral to
the side of seizure onset, in both left and right temporal lobe epilepsy
groups. These findings indicate that chronic temporal lobe epilepsy is
associated not only with abnormalities in gray matter, but also with
concomitant abnormalities in cerebral white matter regions that may
affect connectivity both within and between the cerebral hemispheres.
D 2004 Elsevier Inc. All rights reserved.
Keywords: Voxel-based morphometry; Temporal lobe epilepsy; White
matter; Gray matter
Introduction
The majority of traditional region-of-interest-based quantitative
volumetric magnetic resonance (MR) imaging studies in temporal
lobe epilepsy have focused on neural regions involved in the
genesis and propagation of seizures. Volumetric abnormalities
(atrophy) are evident in hippocampus (Jack et al., 1992; Quigg et
al., 1997; Tasch et al., 1999; Woermann et al., 1998), associated
1053-8119/$ - see front matter D 2004 Elsevier Inc. All rights reserved.
doi:10.1016/j.neuroimage.2004.05.002
* Corresponding author. Department of Medical Physics, University of
Wisconsin-Madison, 1530 Medical Sciences Center, 1300 University
Avenue, Madison, WI 53706. Fax: +1-608-265-9840.
E-mail address: [email protected] (A.B. McMillan).
Available online on ScienceDirect (www.sciencedirect.com.)
mesial temporal lobe structures including amygdala (Kalviainen et
al., 1997; Martin et al., 1999), fornix (Kuzniecky et al., 1999;
Martin et al., 1999), and entorhinal cortex (Bernasconi et al.,
1999); as well as thalamus and basal ganglia (DeCarli et al.,
1998). In addition, atrophy has been reported in extrahippocampal
temporal lobe regions (Moran et al., 2001) and extratemporal areas
such as the cerebellum (Bohnen et al., 1998; Lawson et al.,
2000a,b; Sandok et al., 2000).
Considerably fewer quantitative MR studies of temporal lobe
epilepsy have examined whole brain volumes or volumes of
extratemporal gray or white matter, but the findings to date suggest
that abnormalities in brain structure extend well outside the
neuronal networks responsible for seizure generation and propa-
gation. Sisodiya et al. (1997) described widespread occult struc-
tural abnormalities occurring in visually normal appearing MRIs in
27 patients with hippocampal sclerosis. Marsh et al. (1997)
reported significant bilateral volumetric reductions in frontoparietal
regions in 14 males with temporal lobe epilepsy. Lee et al. (1998)
reported reduced whole brain volume in 27 patients with temporal
lobe epilepsy, and Theodore et al. (2003) recently described
reduced whole brain volume in patients with temporal lobe
epilepsy with a history of complex febrile convulsions.
Comparing patients with temporal lobe epilepsy (n = 58) to
healthy controls (n = 62), we recently reported that significant
volumetric reductions were particularly evident in cerebral white
matter, both ipsilateral and contralateral to the side of temporal
lobe seizure onset (Hermann et al., 2003a). Closer examination of
the corpus callosum in patients with chronic temporal lobe epilepsy
revealed significant volumetric reduction of this major white matter
tract (Hermann et al., 2003b), as well as lower diffusion anisotropy
and higher diffusivity in directions perpendicular to the axons on
DTI (Arfanakis et al., 2002). However, much remains to be
clarified regarding the nature and distribution of abnormalities
suggested by region-of-interest-based approaches. For instance,
the distribution of white matter abnormality within and between
lobar regions of interest remains unclear. In addition, many specific
and important gray matter structures (such as the thalamus) are not
routinely quantified in standard lobar-based segmentation pro-
Table 1
Demographic and clinical information of study groups
Group Mean SD
Age (years) Control 32.42 12.181
Epilepsy 32.23 11.198
Years of education Control 13.68 2.418
Epilepsy 12.96 2.289
IQ Control 107.67 13.812
Epilepsy 96.42 15.256
Onset age (years) Epilepsy 11.95 9.072
Duration (years) Epilepsy 19.09 12.341
A.B. McMillan et al. / NeuroImage 23 (2004) 167–174168
grams, and potential differences in the patterns of white or gray
matter abnormality remain to be determined.
Voxel-based morphometry (VBM) is a technique used to
examine regional morphological differences in gray or white matter
between groups. Methods of VBM have been described that
include an automated approach to the distribution and localization
of whole-brain morphometric abnormalities that are less restricted
to the limitations associated with traditional region of interest
approaches (Good et al., 2001). To date, VBM studies of temporal
lobe epilepsy have focused on gray matter abnormalities (Keller et
al., 2002a,b; Woermann et al., 1999), and no investigation has
examined the presence or distribution of abnormalities in white
matter using VBM.
The purpose of this investigation is to comprehensively
characterize the distribution of abnormalities in gray and white
matter in patients with unilateral temporal lobe epilepsy. As will
be demonstrated, abnormalities in cerebral white matter in uni-
lateral temporal lobe epilepsy were significant, affected temporal
and extratemporal regions ipsilateral to the side of seizure onset,
and were equal in magnitude to abnormalities detected in gray
matter.
Methods
Subjects
Subjects were patients with temporal lobe epilepsy (n = 25, 13
unilateral left TLE, 12 unilateral right TLE) and healthy controls
(n = 62). Selection criteria for epilepsy patients included the
following: (a) chronological age from 14 to 60 years, (b) complex
partial seizures of unilateral temporal lobe origin demonstrated by
ictal EEG monitoring of spontaneous seizures, (c) absence of
MRI abnormalities other than atrophy on clinical reading, and (d)
no other neurological disorder. The majority of these patients
were candidates for anterior temporal lobectomy and as such
underwent a series of procedures including FDG-PET, Wada Test,
neuropsychological assessment, and extensive EEG monitoring of
spontaneous seizures with scalp or more invasive (e.g., subdural
strip or grid electrodes, depending on the details of the case as
decided by a multidisciplinary team). Patients with bilateral
independent left and right temporal lobe seizure onset were
excluded from the study. The subjects investigated here demon-
strated consistent unilateral temporal lobe onset of their typical
complex partial seizures.
Selection criteria for healthy controls included the following:
(a) chronological age from 14 to 60, (b) either a friend or family
member of the patient, (c) no current substance abuse, medical,
or acute psychiatric condition that could affect cognitive func-
tioning, and (d) no history of loss of consciousness >5 min or
developmental learning disorder. Table 1 provides sociodemo-
graphic and clinical features of the subjects. As can be seen, the
groups were equivalent in age and education, while the epilepsy
patients had significantly lower Full Scale IQ. The epilepsy
patients suffered from chronic epilepsy (mean duration = 19.1
years) of childhood onset (mean onset age = 11.9 years). The
left and right temporal lobe groups were not significantly
different in chronological age, duration of epilepsy, or Full Scale
IQ. The left temporal lobe group had significantly (P = 0.02)
less formal education than the right temporal lobe group (11.9
versus 14.2 years).
Image acquisition
Images were obtained on a 1.5-T GE Signa MR scanner. For
each subject, a T1-weighted, three-dimensional SPGR image was
acquired with the following parameters: TE = 5, TR = 24, NEX =
2, flip angle = 40j, slice plane = coronal, matrix size = 256 � 192,
FOV = 26 cm, slice thickness = 1.5 mm.
Voxel-based morphometry
Analysis was performed on a workstation running MATLAB
6.5 (The Mathworks, Inc., Natick, MA) and the statistical para-
metric mapping software SPM2 (Wellcome Department of Cogni-
tive Neurology, London, UK). The methodology used closely
parallels that of Good et al. (2001). Before the creation of a
study-specific template and morphometric analysis, each image
was visually inspected to ensure that its orientation was compatible
with SPM2, its origin centered on the anterior commissure, and
free of image artifacts. This was accomplished using the MRIcro
software package (Rorden and Brett, 2000).
Template creation
To allow for group comparison, voxel-based morphometry
registers each MR image to a standard template (spatial normaliza-
tion) before the image is automatically segmented into gray and
white matter components (Ashburner and Friston, 2000). While it
has been noted that the use of templates derived from the study
population has been shown to have insignificant consequences on
the quality of spatial normalization (Salmond et al., 2002) when
compared to the templates included with the SPM software, VBM
studies have used templates created from the study population or a
subset thereof to improve the quality of the segmentation step (e.g.,
Good et al., 2001; Karas et al., 2003; Rusch et al., 2003). Thus,
study-specific templates for whole brain volumes, gray matter, and
white matter were created. To accomplish this, images were first
segmented and spatial normalization parameters were calculated to
best match the segmented gray matter image to the SPM gray matter
template image. The whole brain image was then spatially normal-
ized using these calculated parameters and automatically segmented
into gray matter, white matter, and CSF. Note that the templates
were spatially normalized only to the default gray matter template
so that the resultant template images are complementary between
gray matter, white matter, and CSF compartments. Normalizing
each image to the respective gray and white matter template image
is performed in subsequent processing of the images, but at this
stage would have likely resulted in non-overlapping spatial nor-
malization between respective gray and white matter images. The
respective template images were formed from the average voxel

Table 2
Locations of local maximum of volume decreases in gray matter VBM
analysis significant at P < 0.05, corrected for multiple comparisons
Location Size
(voxels)
t P (FDR
corrected)
Left TLE �33 �3 �34 12,140 5.7 0.003
GM < controls �12 �35 9 1260 4.82 0.004
�22 �32 �20 105 3.8 0.019
27 50 �3 339 3.75 0.022
�28 52 �1 76 3.65 0.027
�29 55 �2 1 3.4 0.047
�22 �27 �21 1 3.39 0.048
Right TLE 41 2 �30 16,181 5.47 0.001
GM < controls 3 �24 35 262 4.06 0.008
5 37 9 475 3.83 0.014
43 �25 11 171 3.73 0.019
11 6 12 14 3.67 0.021
28 �35 13 141 3.65 0.022
11 2 14 2 3.64 0.023
11 8 10 2 3.5 0.032
57 �18 �10 2 3.45 0.036
10 7 8 5 3.42 0.039
57 �14 �12 3 3.41 0.039
55 �12 �14 1 3.34 0.046
4 �38 31 1 3.32 0.048
�10 �42 �55 1 3.31 0.049
8 4 8 1 3.31 0.049
A.B. McMillan et al. / NeuroImage 23 (2004) 167–174 169
intensity for each segmented image for all subjects in the study and
smoothed with an 8-mm full width at half maximum (FWHM)
Gaussian kernel.
Image preprocessing
Similar to the template creation step, the images were spatially
normalized to the same coordinate system before group compari-
son. Each image was first segmented and spatial normalization
parameters were calculated for the segmented gray matter image
from the created gray matter template. Because accurate spatial
normalization is crucial for VBM, spatial normalization parameters
for the segmented white matter image were calculated from the
created white matter template. Each whole brain image was then
spatially normalized for each set of normalization parameters
obtained from the previous step and automatically segmented into
gray and white matter components, where the respective images
normalized to the specific template were used in analysis (i.e.,
gray-matter-template-normalized images were used for gray matter
analysis and white-matter-template-normalized images were used
for white matter analysis). To account for the different spatial
normalization parameters applied to each image, as individual
voxels were either shrunk or stretched, the voxel intensities were
multiplied by the Jacobian determinates from the spatial normal-
ization parameters (Ashburner and Friston, 2000). In previous
VBM methods, this process has been named modulation (Good
et al., 2001). The resulting gray and white matter images were
smoothed with a 12-mm FWHM Gaussian kernel.
Statistical analysis
To eliminate voxels outside of the volume of interest (i.e., gray
or white matter), the images were masked before analysis so that
voxels of noninterest (e.g., regions corresponding to white matter
and CSF in a gray matter mask) were not included in statistical
calculations. Masks were created from the study template images. A
gray matter mask was created where voxels in the complementary
image compartments (white matter and CSF) were removed from
the mask. Nonzero voxels from the white matter and CSF template
images with intensity greater than or equal to the mean intensity
plus one standard deviation from the respective white matter and
CSF templates were then removed from the gray matter template
image. Upon smoothing with a small diameter Gaussian kernel, the
statistical comparisons were confined to an area more inclusive of
the gray matter volume. A white matter mask was created and
applied in a similar manner. The mask images are shown in Fig. 1.
To compare groups, analysis of covariance (ANCOVA) was
performed using the total volume of each segmented image after
modulation, with age and gender as confounding covariates for the
Fig. 1. Example of template image used to mask input images. The gray matter m
overlap exists between gray and white matter masks, as the purpose is to restrict th
respective gray and white matter analyses. Total volume of each
segmented and modulated image before smoothing was used to
investigate regional volume changes beyond global gray or white
matter changes. Both left and right temporal lobe epilepsy groups
were incorporated as separate groups into the same statistical model
because it was expected that differences in temporal lobe epilepsy
laterality added more information to the statistical model. Using
SPM2, t-statistic maps were created for each voxel in the standard
atlas space to reflect differences in gray and white matter for the
lateralized (left and right) groups. Resultant t-statistic maps were
thresholded at aP-value of <0.05 corrected for multiple comparisons
using the False Discovery Rate approach (Genovese et al., 2002).
Results
Gray Matter
Table 2 details the regions of gray matter volume decrease that
were apparent at P < 0.05, corrected for multiple comparisons
ask is shown in green and the white matter mask is shown in red. Note that
e respective analysis to regions more representative of gray or white matter.

A.B. McMillan et al. / NeuroImage 23 (2004) 167–174170
across the entire search volume. Cluster size is included for reader
convenience, but all inferences are drawn from voxelwise tests.
Additionally, results will be discussed in relation to their voxelwise
correspondence with anatomical structures. While presented in
tables for completeness, results indicating volume differences of
only a few voxels are difficult to interpret and will not be discussed
in detail. Fig. 2 depicts areas of decreased gray and white matter
volume in the left and right temporal lobe groups. As can be seen
in Fig. 3, left temporal lobe epilepsy patients exhibited significant
abnormalities relative to controls in the thalamus (both ipsilateral
and contralateral to side of seizure onset) and ipsilateral hippo-
campus. The left temporal lobe epilepsy group did not exhibit
significant regions of increased gray matter volume with respect to
the controls. The right temporal lobe epilepsy group exhibited
decreased gray matter volume in the ipsilateral thalamus and
abnormalities near the ipsilateral hippocampus. The right temporal
lobe epilepsy group also did not exhibit significant regions of
increased gray matter volume in comparison to the controls.
White matter
Table 3 details the white matter volume decreases for left and
right TLE groups apparent at P < 0.05, corrected for multiple
comparisons across the entire search volume. In addition to Fig. 2,
Fig. 4 provides a detailed depiction of decreased white matter
volume in the left and right TLE groups. As can be seen, temporal
lobe epilepsy patients exhibited a marked white matter volume
Fig. 2. VBM results at P < 0.05, corrected for multiple comparisons. Top left, regi
gray matter volume reduction for right TLE group; bottom left, regions of white
matter volume reduction for right TLE group.
decrease predominantly focused in ipsilateral temporal pole white
matter. This volume loss extends extratemporally to bilateral
prefrontal white matter in the left temporal lobe epilepsy group,
affecting voxels in the corpus callosum of both left and right TLE
groups, and the fornix of the right TLE group.
The left temporal lobe epilepsy group did not exhibit areas of
increased white matter volume compared to the controls. A
significant amount of white matter increase was found in the right
TLE group in the right hemisphere near the parietal–occipital
fissure. However, the voxels in this region are predominantly gray
matter, likely due to misregistration of tissue during the automated
segmentation, and therefore discounted from further inference.
Discussion
This report confirms and extends previous findings concerning
structural brain abnormalities observed in patients with unilateral
temporal lobe epilepsy. In addition, an extensive degree of tem-
poral lobe white matter abnormality is demonstrated. These find-
ings, their implications, potential significance, and the limitations
of this investigation are reviewed in the material to follow.
Gray matter abnormalities
Overall, the VBM gray matter findings observed in this study
complement previously reported abnormalities in patients with
ons of gray matter volume reduction for left TLE group; top right, regions of
matter volume reduction for left TLE group; bottom right, regions of white
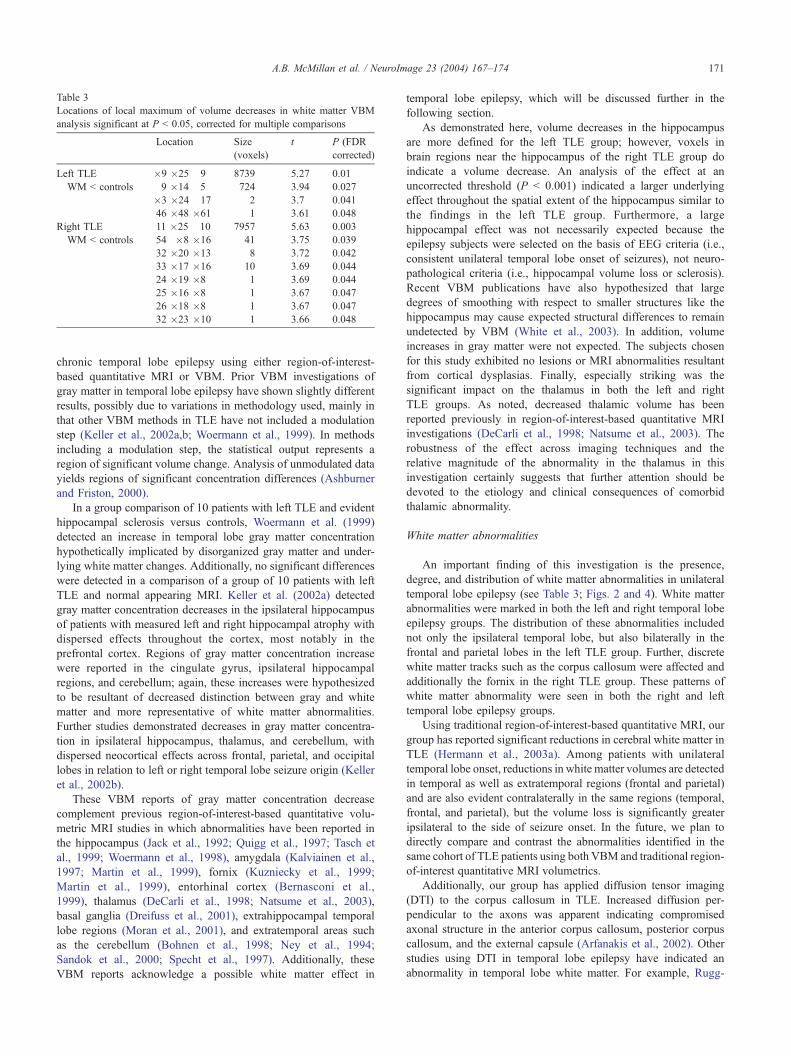
Table 3
Locations of local maximum of volume decreases in white matter VBM
analysis significant at P < 0.05, corrected for multiple comparisons
Location Size
(voxels)
t P (FDR
corrected)
Left TLE �9 �25 9 8739 5.27 0.01
WM < controls 9 �14 5 724 3.94 0.027
�3 �24 17 2 3.7 0.041
46 �48 �61 1 3.61 0.048
Right TLE 11 �25 10 7957 5.63 0.003
WM < controls 54 �8 �16 41 3.75 0.039
32 �20 �13 8 3.72 0.042
33 �17 �16 10 3.69 0.044
24 �19 �8 1 3.69 0.044
25 �16 �8 1 3.67 0.047
26 �18 �8 1 3.67 0.047
32 �23 �10 1 3.66 0.048
A.B. McMillan et al. / NeuroImage 23 (2004) 167–174 171
chronic temporal lobe epilepsy using either region-of-interest-
based quantitative MRI or VBM. Prior VBM investigations of
gray matter in temporal lobe epilepsy have shown slightly different
results, possibly due to variations in methodology used, mainly in
that other VBM methods in TLE have not included a modulation
step (Keller et al., 2002a,b; Woermann et al., 1999). In methods
including a modulation step, the statistical output represents a
region of significant volume change. Analysis of unmodulated data
yields regions of significant concentration differences (Ashburner
and Friston, 2000).
In a group comparison of 10 patients with left TLE and evident
hippocampal sclerosis versus controls, Woermann et al. (1999)
detected an increase in temporal lobe gray matter concentration
hypothetically implicated by disorganized gray matter and under-
lying white matter changes. Additionally, no significant differences
were detected in a comparison of a group of 10 patients with left
TLE and normal appearing MRI. Keller et al. (2002a) detected
gray matter concentration decreases in the ipsilateral hippocampus
of patients with measured left and right hippocampal atrophy with
dispersed effects throughout the cortex, most notably in the
prefrontal cortex. Regions of gray matter concentration increase
were reported in the cingulate gyrus, ipsilateral hippocampal
regions, and cerebellum; again, these increases were hypothesized
to be resultant of decreased distinction between gray and white
matter and more representative of white matter abnormalities.
Further studies demonstrated decreases in gray matter concentra-
tion in ipsilateral hippocampus, thalamus, and cerebellum, with
dispersed neocortical effects across frontal, parietal, and occipital
lobes in relation to left or right temporal lobe seizure origin (Keller
et al., 2002b).
These VBM reports of gray matter concentration decrease
complement previous region-of-interest-based quantitative volu-
metric MRI studies in which abnormalities have been reported in
the hippocampus (Jack et al., 1992; Quigg et al., 1997; Tasch et
al., 1999; Woermann et al., 1998), amygdala (Kalviainen et al.,
1997; Martin et al., 1999), fornix (Kuzniecky et al., 1999;
Martin et al., 1999), entorhinal cortex (Bernasconi et al.,
1999), thalamus (DeCarli et al., 1998; Natsume et al., 2003),
basal ganglia (Dreifuss et al., 2001), extrahippocampal temporal
lobe regions (Moran et al., 2001), and extratemporal areas such
as the cerebellum (Bohnen et al., 1998; Ney et al., 1994;
Sandok et al., 2000; Specht et al., 1997). Additionally, these
VBM reports acknowledge a possible white matter effect in
temporal lobe epilepsy, which will be discussed further in the
following section.
As demonstrated here, volume decreases in the hippocampus
are more defined for the left TLE group; however, voxels in
brain regions near the hippocampus of the right TLE group do
indicate a volume decrease. An analysis of the effect at an
uncorrected threshold (P < 0.001) indicated a larger underlying
effect throughout the spatial extent of the hippocampus similar to
the findings in the left TLE group. Furthermore, a large
hippocampal effect was not necessarily expected because the
epilepsy subjects were selected on the basis of EEG criteria (i.e.,
consistent unilateral temporal lobe onset of seizures), not neuro-
pathological criteria (i.e., hippocampal volume loss or sclerosis).
Recent VBM publications have also hypothesized that large
degrees of smoothing with respect to smaller structures like the
hippocampus may cause expected structural differences to remain
undetected by VBM (White et al., 2003). In addition, volume
increases in gray matter were not expected. The subjects chosen
for this study exhibited no lesions or MRI abnormalities resultant
from cortical dysplasias. Finally, especially striking was the
significant impact on the thalamus in both the left and right
TLE groups. As noted, decreased thalamic volume has been
reported previously in region-of-interest-based quantitative MRI
investigations (DeCarli et al., 1998; Natsume et al., 2003). The
robustness of the effect across imaging techniques and the
relative magnitude of the abnormality in the thalamus in this
investigation certainly suggests that further attention should be
devoted to the etiology and clinical consequences of comorbid
thalamic abnormality.
White matter abnormalities
An important finding of this investigation is the presence,
degree, and distribution of white matter abnormalities in unilateral
temporal lobe epilepsy (see Table 3; Figs. 2 and 4). White matter
abnormalities were marked in both the left and right temporal lobe
epilepsy groups. The distribution of these abnormalities included
not only the ipsilateral temporal lobe, but also bilaterally in the
frontal and parietal lobes in the left TLE group. Further, discrete
white matter tracks such as the corpus callosum were affected and
additionally the fornix in the right TLE group. These patterns of
white matter abnormality were seen in both the right and left
temporal lobe epilepsy groups.
Using traditional region-of-interest-based quantitative MRI, our
group has reported significant reductions in cerebral white matter in
TLE (Hermann et al., 2003a). Among patients with unilateral
temporal lobe onset, reductions in white matter volumes are detected
in temporal as well as extratemporal regions (frontal and parietal)
and are also evident contralaterally in the same regions (temporal,
frontal, and parietal), but the volume loss is significantly greater
ipsilateral to the side of seizure onset. In the future, we plan to
directly compare and contrast the abnormalities identified in the
same cohort of TLE patients using both VBM and traditional region-
of-interest quantitative MRI volumetrics.
Additionally, our group has applied diffusion tensor imaging
(DTI) to the corpus callosum in TLE. Increased diffusion per-
pendicular to the axons was apparent indicating compromised
axonal structure in the anterior corpus callosum, posterior corpus
callosum, and the external capsule (Arfanakis et al., 2002). Other
studies using DTI in temporal lobe epilepsy have indicated an
abnormality in temporal lobe white matter. For example, Rugg-
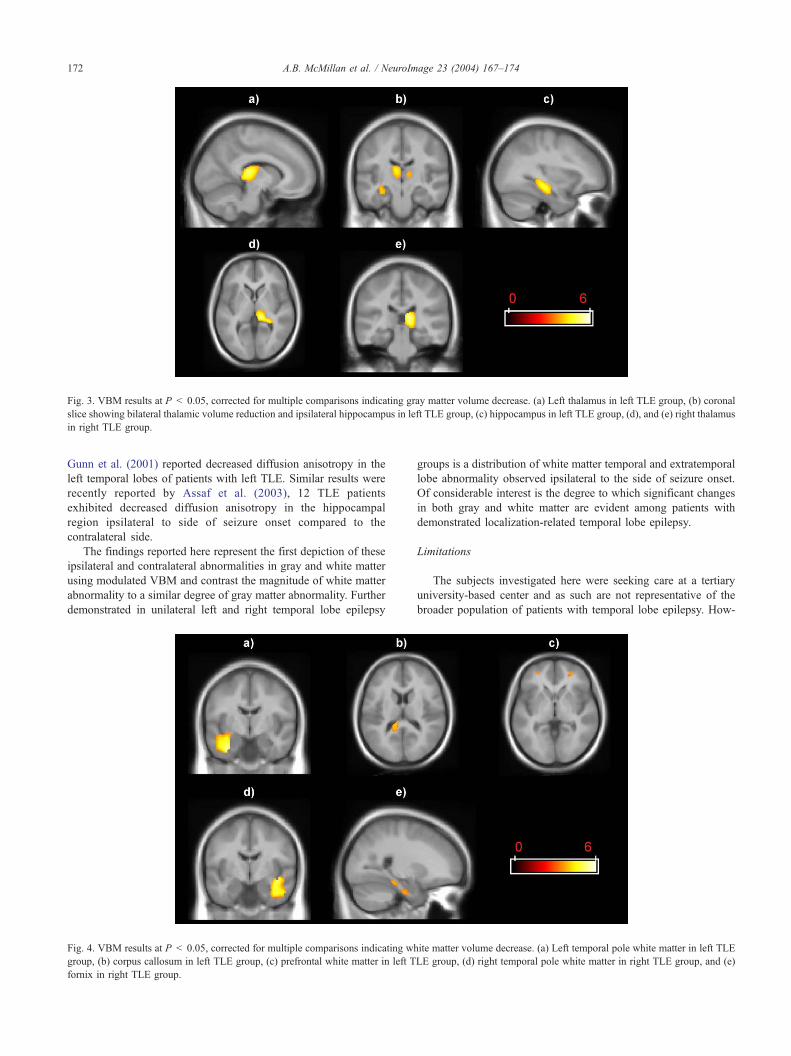
Fig. 3. VBM results at P < 0.05, corrected for multiple comparisons indicating gray matter volume decrease. (a) Left thalamus in left TLE group, (b) coronal
slice showing bilateral thalamic volume reduction and ipsilateral hippocampus in left TLE group, (c) hippocampus in left TLE group, (d), and (e) right thalamus
in right TLE group.
A.B. McMillan et al. / NeuroImage 23 (2004) 167–174172
Gunn et al. (2001) reported decreased diffusion anisotropy in the
left temporal lobes of patients with left TLE. Similar results were
recently reported by Assaf et al. (2003), 12 TLE patients
exhibited decreased diffusion anisotropy in the hippocampal
region ipsilateral to side of seizure onset compared to the
contralateral side.
The findings reported here represent the first depiction of these
ipsilateral and contralateral abnormalities in gray and white matter
using modulated VBM and contrast the magnitude of white matter
abnormality to a similar degree of gray matter abnormality. Further
demonstrated in unilateral left and right temporal lobe epilepsy
Fig. 4. VBM results at P < 0.05, corrected for multiple comparisons indicating wh
group, (b) corpus callosum in left TLE group, (c) prefrontal white matter in left T
fornix in right TLE group.
groups is a distribution of white matter temporal and extratemporal
lobe abnormality observed ipsilateral to the side of seizure onset.
Of considerable interest is the degree to which significant changes
in both gray and white matter are evident among patients with
demonstrated localization-related temporal lobe epilepsy.
Limitations
The subjects investigated here were seeking care at a tertiary
university-based center and as such are not representative of the
broader population of patients with temporal lobe epilepsy. How-
ite matter volume decrease. (a) Left temporal pole white matter in left TLE
LE group, (d) right temporal pole white matter in right TLE group, and (e)

A.B. McMillan et al. / NeuroImage 23 (2004) 167–174 173
ever, a recent population-based study of a heterogeneous group of
epilepsy patients also found substantial presence of both focal and
generalized neocortical atrophy among chronic epilepsy patients
(Liu et al., 2003).
While the automated approach of voxel-based morphometry
has distinct advantages over traditional region-of-interest-based
methods, it is not without limitations due to imperfect spatial
normalization, segmentation, and smoothing of the source images
(Good et al., 2001). Systematic misclassification of structures can
cause volume changes to appear in regions where none truly
exists, such as gray matter changes in brain regions that should
be white matter. This problem is potentially worsened in regions
without distinct gray–white matter boundaries (Ashburner and
Friston, 2000; Keller et al., 2002b) and poor boundaries due to
pathological reasons as previously described. Here, the search
volume for the VBM results was confined to an area more
inclusive of the respective gray or white matter. By eliminating
voxels outside of the tissue type of interest, the results are confined
to areas with greater probabilities of being correctly classified.
Even with a modest sample size, we present gray and white matter
results with findings that are well complemented between the left
and right TLE groups and previous volumetric findings. It is likely
that inclusion of larger numbers of patients would provide in-
creased statistical power resulting in the identification of additional
areas of abnormality.
Implications
The identified changes in gray and especially white matter
affected multiple brain regions and could be expected to adversely
affect cognitive status. Indeed, neuropsychological investigations
of patients with chronic temporal lobe epilepsy have demonstrated
diffuse cognitive dysfunction, the etiology of which has been
difficult to determine (Hermann et al., 1997). The clinical signif-
icance of identified extratemporal gray matter VBM abnormalities
has recently been demonstrated by Keller et al. (2003). They
reported that frontal lobe gray matter abnormalities were evident
in patients with temporal lobe epilepsy, and importantly that these
frontal lobe VBM abnormalities were associated with poorer
performance on measures of frontally dependent executive func-
tions. We have recently reported that whole brain white matter
brain volume abnormalities are also significantly associated with
neuropsychological dysfunction in TLE (Hermann et al., 2003a).
Thus, the presence of extratemporal lobe abnormalities in TLE
may contribute to the cumulative cognitive burden of the disorder.
Future research examining the relationship between VBM identi-
fied abnormalities in cerebral white matter and abnormalities in
specific mental functions and emotional–behavioral status could
provide further clarification of the etiologies underlying important
comorbidities of TLE.
The identified anomalies in cerebral white matter raise the
possibility of compromised connectivity within the temporal lobe
as well as within and between the left and right cerebral hemi-
spheres. The presence of significant disruption in cortical con-
nectivity secondary to abnormalities in cerebral white matter in a
disease traditionally considered a disorder of gray matter repre-
sents a new conceptualization of the etiology underlying some of
the cognitive pathology in epilepsy. Sophisticated functional
imaging research has led to the widely appreciated view that
many cognitive tasks dependent on the coordinated activity of
distributed neuronal network for efficient and successful perfor-
mance. Disruptions in cerebral connectivity could be expected to
adversely affect tasks dependent on such distributed neuronal
systems.
Finally, the pathophysiology and etiology of the identified
abnormalities in cerebral white matter remains to be determined.
Possible causes include the neurodevelopmental impact of epilepsy
and its treatment on white matter development and/or the potential
adverse effects of chronic epilepsy and its treatment with anti-
epilepsy medications on brain structure. Resolution of this issue
has considerable theoretical and treatment implications. Ultimately,
longitudinal studies employing multimodal neuroimaging techni-
ques will be necessary to provide data relevant to this issue.
Acknowledgments
This study was supported by NIH NS 2RO1-37738 and NIH
RO1 RR16591-02.
References
Arfanakis, K., Hermann, B.P., Rogers, B.P., Carew, J.D., Seidenberg, M.,
Meyerand, M.E., 2002. Diffusion tensor MRI in temporal lobe epilepsy.
Magn. Reson. Imaging 20, 511–519.
Ashburner, J., Friston, K.J., 2000. Voxel-based morphometry—The
methods. NeuroImage 11, 805–821.
Assaf, B.A., Mohamed, F.B., Abou-Khaled, K.J., Williams, J.M., Yazeji,
M.S., Haselgrove, J., Faro, S.H., 2003. Diffusion tensor imaging of the
hippocampal formation in temporal lobe epilepsy. Am. J. Neuroradiol.
24, 1857–1862.
Bernasconi, N., Bernasconi, A., Andermann, F., Dubeau, F., Feindel, W.,
Reutens, D.C., 1999. Entorhinal cortex in temporal lobe epilepsy: a
quantitative MRI study. Neurology 52, 1870–1876.
Bohnen, N.I., O’Brien, T.J., Mullan, B.P., So, E.L., 1998. Cerebellar
changes in partial seizures: clinical correlation of quantitative SPECT
and MRI analysis. Epilepsia 39, 640–650.
DeCarli, C., Hatta, J., Fazilat, S., Fazilat, S., Gaillard, W.D., Theodore,
W.H., 1998. Extratemporal atrophy in patients with complex partial
seizures of left temporal origin. Ann. Neurol. 43, 41–45.
Dreifuss, S., Vingerhoets, J.G., Lazeyras, F., Andino, S.G., Spinelli, L.,
Delavelle, J., Seeck, M., 2001. Volumetric measurements of subcortical
nuclei in patents with temporal lobe epilepsy. Neurology 57, 1636–1641.
Genovese, C.R., Lazar, N.A., Nichols, T., 2002. Thresholding of statistical
maps in functional neuroimaging using the false discovery rate. Neuro-
Image 15 (4), 870–878.
Good, C.D., Johnsrude, I.S., Ashburner, J., Henson, R.N., Friston, K.J.,
Frackowiak, R.S., 2001. A voxel-based morphometric study of ageing
in 465 normal adult human brains. NeuroImage 14, 21–36.
Hermann, B.P., Seidenberg, M., Schoenfeld, J., Davies, K., 1997. Neuro-
psychological characteristics of the syndrome of mesial temporal lobe
epilepsy. Arch. Neurol. 54, 369–376.
Hermann, B.P., Seidenberg, M., Bell, B., Rutecki, P., Sheth, R., Sutula, T.,
Wendt, G., O’Leary, D., Magnotta, V., 2003a. Extratemporal quantita-
tive MRI volumetrics and neuropsychological function in temporal lobe
epilepsy. J. Int. Neuropsychol. Soc. 9, 353–362.
Hermann, B.P., Hansen, R., Seidenberg, M., Magnotta, V., O’Leary, D.,
2003b. Neurodevelopmental vulnerability of the corpus callosum to
childhood onset localization-related epilepsy. NeuroImage 18, 284–292.
Jack, C.R, Sharbrough, F.W., Cascino, G.D., Hirschorn, K.A., O’Brien, P.C.,
Marsh,W.R., 1992. Magnetic resonance image-based hippocampal volu-
metry: correlation with outcome after temporal lobectomy. Ann. Neurol.
31, 138–146.
Kalviainen, R., Salmenpera, T., Partanen, K., Vainio, P., Riekkinen, P.,

A.B. McMillan et al. / NeuroImage 23 (2004) 167–174174
Duncan, J.S., 1997. MRI volumetry and T2 relaxometry of the amyg-
dala in newly diagnosed and chronic temporal lobe epilepsy. Epilepsy
Res. 28, 39–50.
Karas, G.B., Burton, E.J., Rombouts, S.A., van Schijndel, R.A., O’Brien,
J.T., Scheltens, P., McKeith, I.G., Williams, D., Ballard, C., Barkhof,
F., 2003. A comprehensive study of gray matter loss in patients with
Alzheimer’s disease using optimized voxel-based morphometry. Neu-
roImage 18, 895–907.
Keller, S.S., Mackay, C.E., Barrick, T.R., Wieshmann, U.C., Howard, M.A.,
Roberts, N., 2002a. Voxel-based morphometric comparison of hippo-
campal and extrahippocampal abnormalities in patients with left and
right hippocampal atrophy. NeuroImage 16, 23–31.
Keller, S.S., Wieshmann, U.C., Mackay, C.E., Denby, C.E., Webb, J.,
Roberts, N., 2002b. Voxel based morphometry of grey matter abnor-
malities in patients with medically intractable temporal lobe epilepsy:
effects of side of seizure onset and epilepsy duration. J. Neurol., Neuro-
surg. Psychiatry 73, 648–656.
Keller, S.S., Baker, G., Weishmann, U.C., Sluming, V., Roberts, N., 2003.
Mapping volume atrophy in patients with temporal lobe epilepsy and
hippocampal atrophy using optimised voxel-based morphometry. Pro-
ceedings of the International Society for Magnetic Resonance in Med-
icine, Toronto, Canada, July 2003.
Kuzniecky, R., Bilir, E., Gilliam, F., Faught, E., Martin, R., Hugg, J., 1999.
Quantitative MRI in temporal lobe epilepsy: evidence for fornix atro-
phy. Neurology 53, 496–501.
Lawson, J.A., Vogrin, S., Bleasel, A.F., Cook, M.J., Bye, A.M., 2000a.
Cerebral and cerebellar volume reduction in children with temporal lobe
epilepsy. Epilepsia 41, 1456–1462.
Lawson, J.A., Vogrin, S., Bleasel, A.F., Cook, M.J., Burns, L., McAnally,
L., Pereira, J., Bye, A.M., 2000b. Predictors of hippocampal, cerebral,
and cerebellar volume reduction in childhood epilepsy. Epilepsia 41,
1540–1545.
Lee, J.W., Andermann, F., Dubeau, F., Bernasconi, A., MacDonald, D.,
Evans, A., Reutens, D.C., 1998. Morphometric analysis of the temporal
lobe in temporal lobe epilepsy. Epilepsia 39, 727–736.
Liu, R.S.N., Lemieux, L., Bell, G.S., Hammers, A., Sisodiya, S.M.,
Bartlett, P.A., Shorvon, S.D., Sander, J., Duncan, J.S., 2003. Progres-
sive neocortical damage in epilepsy. Ann. Neurol. 53, 312–324.
Marsh, L., Morrell, M.J., Shear, P.K., Sullivan, E.V., Freeman, H., Marie,
A., Lim, K.O., Pfefferbaum, A., 1997. Cortical and hippocampal vol-
ume deficits in temporal lobe epilepsy. Epilepsia 38, 576–587.
Martin, R., Hugg, J.W., Roth, D.L., Bilar, E., Gilliam, F.G., Faught, E.,
Kuzneicky, R., 1999. MRI extrahippocampal volumes and visual mem-
ory: correlations independent of MRI hippocampal volumes in temporal
lobe epilepsy. J. Int. Neuropsychol. Soc. 5, 540–548.
Moran, N.F., Lemieux, L., Kitchen, N.D., Fish, D.R., Shorvon, S.D., 2001.
Extrahippocampal temporal lobe atrophy in temporal lobe epilepsy and
mesial temporal sclerosis. Brain 124, 167–175.
Natsume, J., Bernasconi, N., Andermann, F., Bernasconi, A., 2003. MRI
volumetry of the thalamus in temporal, extratemporal, and idiopathic
generalized epilepsy. Neurology 60, 1296–1300.
Ney, G.C., Lantos, G., Barr, W.B., Schaul, N., 1994. Cerebellar atrophy in
patients with long-term phenytoin exposure and epilepsy. Arch. Neurol.
51, 767–771.
Quigg, M., Bertram, E.H., Jackson, T., Laws, E., 1997. Volumetric mag-
netic resonance imaging evidence of bilateral hippocampal atrophy in
mesial temporal lobe epilepsy. Epilepsia 38, 588–594.
Rorden, C., Brett, M., 2000. Stereotaxic display of brain lesions. Behav.
Neurol. 12, 191–200.
Rugg-Gunn, F.J., Eriksson, S.H., Symms, M.R., Barker, G.J., Duncan, J.S.,
2001. Diffusion tensor imaging of cryptogenic and acquired partial
epilepsies. Brain 124, 627–636.
Rusch, N., van Elst, L.T., Ludaescher, P., Wilke, M., Huppertz, H.J., Thiel,
T., Schmahl, C., Bohus, M., Lieb, K., Hesslinger, B., Hennig, J.,
Ebert, D., 2003. A voxel-based morphometric MRI study in female
patients with borderline personality disorder. NeuroImage 20, 385–392.
Salmond, C.H., Ashburner, J., Vargha-Khadem, F., Connelly, A., Gadian,
D.G., Friston, K.J., 2002. The precision of anatomical normalization in
the medial temporal lobe using spatial basis functions. NeuroImage 17,
507–512.
Sandok, E.K., O’Brien, T.J., Jack, C.R., So, E.L., 2000. Significance of
cerebellar atrophy in intractable temporal lobe epilepsy: a quantitative
MRI study. Epilepsia 41, 1315–1320.
Sisodiya, S.M., Moran, N., Free, S.L., Kitchen, N.D., Stevens, J.M.,
Harkness, W.F., Fish, D.R., Shorvon, S.D., 1997. Correlation of
widespread preoperative magnetic resonance imaging changes with
unsuccessful surgery for hippocampal sclerosis. Ann. Neurol. 41,
490–496.
Specht, U., May, T., Schulz, R., Rohde, M., Ebner, A., Schmidt, R.C.,
Schutz, M., Wolf, P., 1997. Cerebellar atrophy and prognosis after tem-
poral lobe resection. J. Neurol., Neurosurg. Psychiatry 62, 501–506.
Tasch, E., Cendes, F., Li, L.M., Dubeau, F., Andermann, F., Arnold, D.L.,
1999. Neuroimaging evidence of progressive neuronal loss and dys-
function in temporal lobe epilepsy. Ann. Neurol. 45, 568–576.
Theodore, W.H., DeCarli, C., Gaillard, W.D., 2003. Total cerebral volume
is reduced in patients with localization-related epilepsy and a history of
complex febrile seizures. Arch. Neurol. 60 (2), 250–252.
White, N.S., Alkire, M.T., Haier, R.J., 2003. A voxel-based morphometric
study of nondemented adults with Down syndrome. NeuroImage 20,
397–403.
Woermann, F.G., Barker, G.J., Birnie, K.D., Meencke, H.J., Duncan, J.S.,
1998. Regional changes in hippocampal T2 relaxation and volume: a
quantitative magnetic resonance imaging study of hippocampal sclero-
sis. J. Neurol., Neurosurg. Psychiatry 65, 656–664.
Woermann, F.G., Free, S.L., Koepp, M.J., Ashburner, J., Duncan, J.S.,
1999. Voxel-by-voxel comparison of automatically segmented cerebral
gray matter—A rater-independent comparison of structural MRI in
patients with epilepsy. NeuroImage 10, 373–384.






























