The Pediatric Central Skull Base
Gary L. Hedlund, D.O.Primary Children’s Medical Center
Salt Lake City, Utah
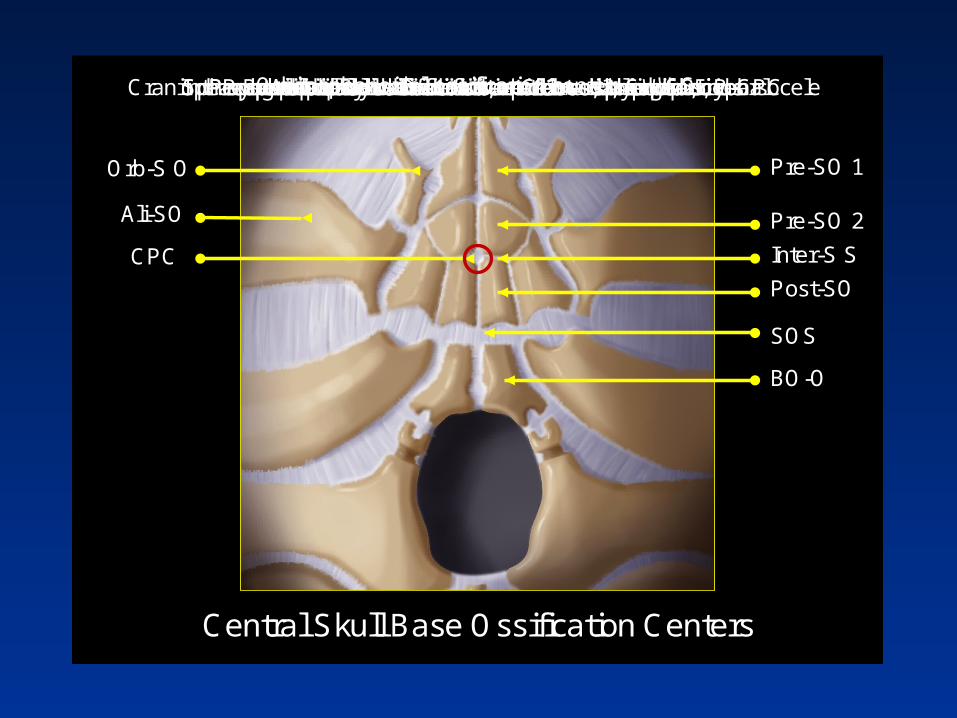
Pre-SO 1
Pre-SO 2
Inter-S S
Post-SO
SOS
BO-O
CPC
Ali-SO
Orb-S O
Central Skull Base Ossification Centers
Presphenoidal ossification center 1 → sphenoid sinusPresphenoidal ossification center 2 → sphenoid sinusIntersphenoidal synchondrosis → Closes, 3mo; if no, P-CPCPostsphenoidal ossification center → basisphenoidSphenooccipital synchondrosis → Closes by age 25 yearsBasioccipital ossification center → basiocciputOrbitosphenoidal ossification center → LWSAlisphenoidal ossification center → GWSCraniopharyngeal canal → Dermoid, epidermoid, lipoma, cephalocele


The Chondrocranium
• Portion of the neocranium formed by endochondral ossification
• 25 centers of ossification
• 18 sutures and/or synchondroses
• Anatomic variants and developmental anomalies abound
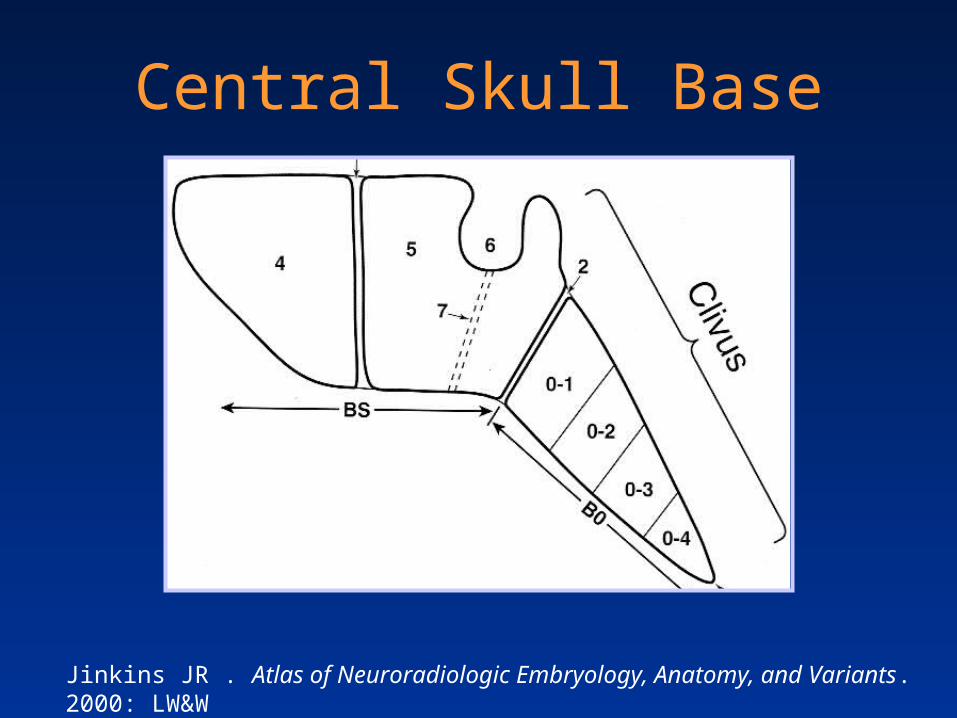
Central Skull Base
Jinkins JR . Atlas of Neuroradiologic Embryology, Anatomy, and Variants. 2000: LW&W

Newborn Central Skull Base
Newborn
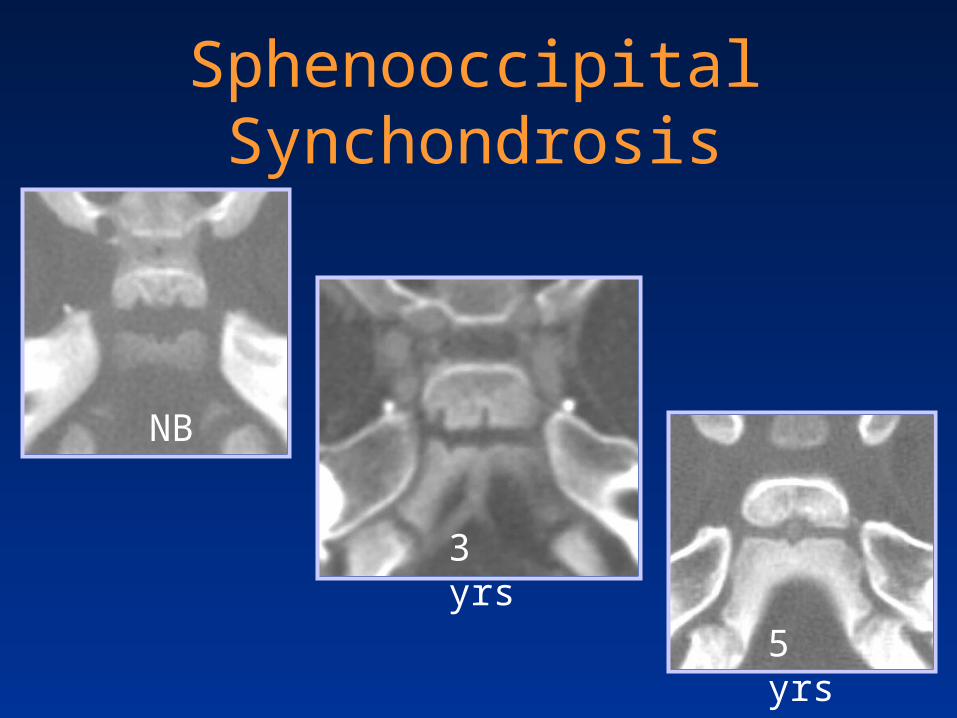
Sphenooccipital Synchondrosis
NB
3 yrs
5 yrs
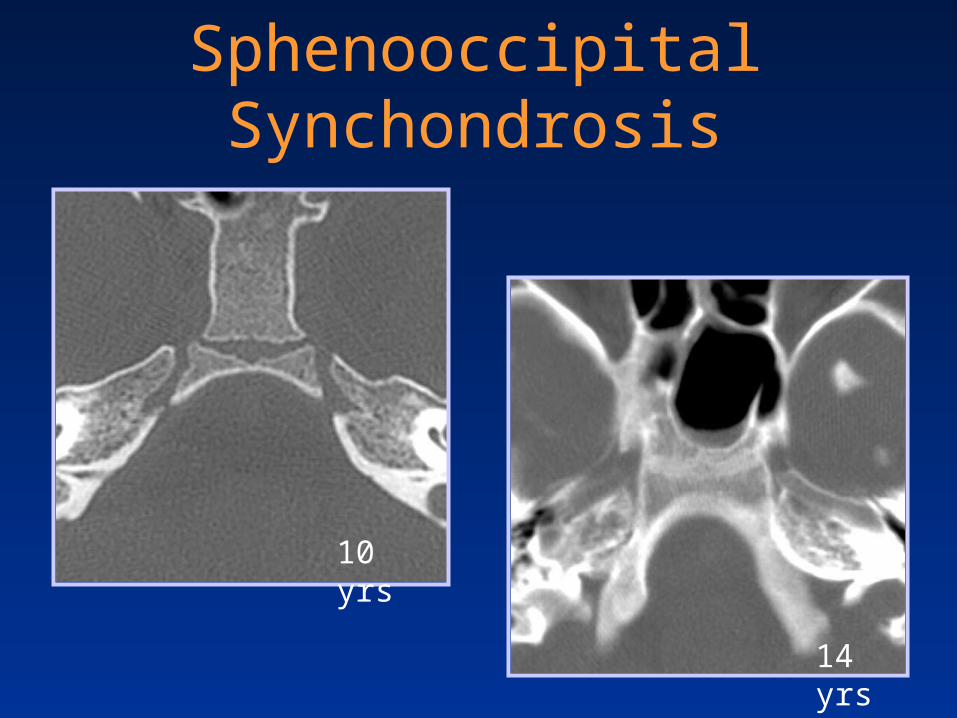
Sphenooccipital Synchondrosis
10 yrs
14 yrs

18-year-old female with closed head trauma
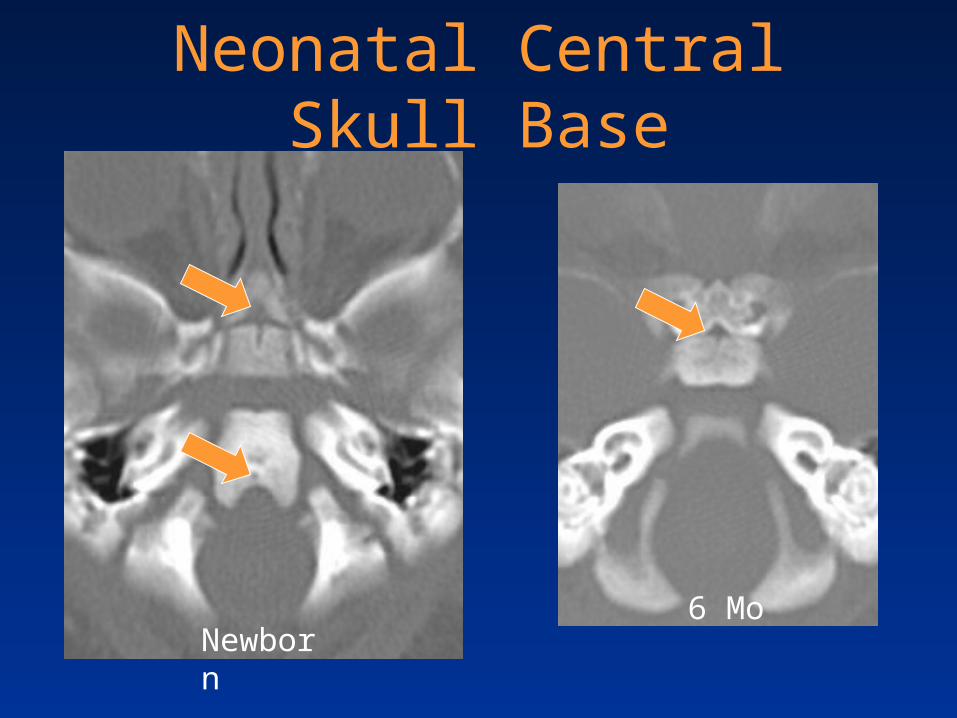
Neonatal Central Skull Base
Newborn6 Mo
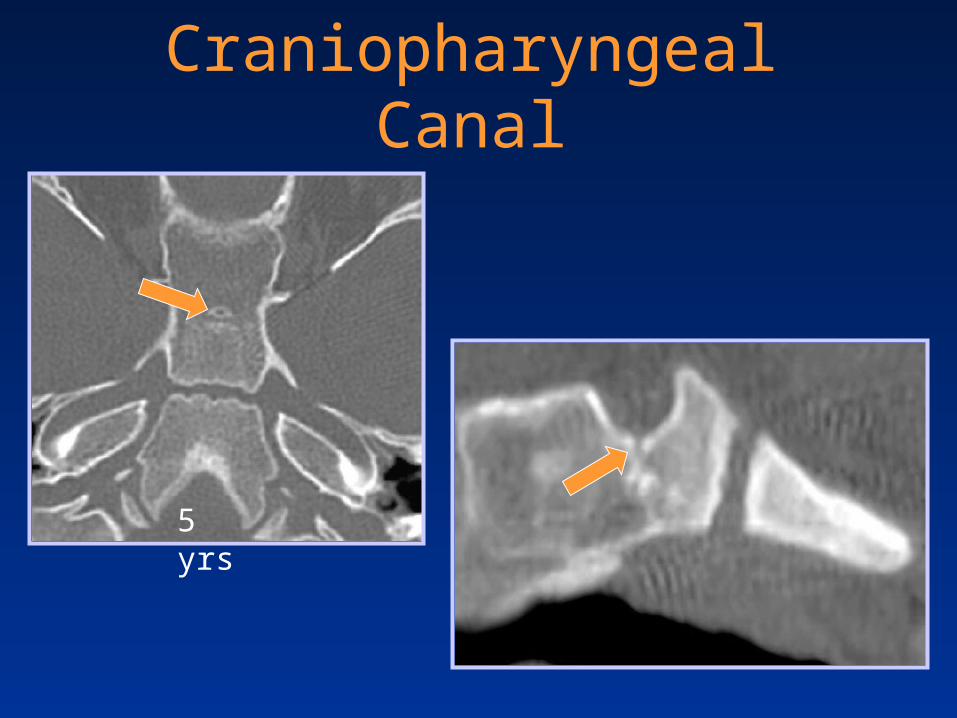
Craniopharyngeal Canal
5 yrs

Craniopharyngeal Canal
Larsen WJ. Human Embryology, 2ND ed. Saunders; 1997

Craniopharyngeal Canal
Courtesy Bronwyn E. Hamilton, MD

Infant Central Skull Base

Age Related T1WI Marrow Changes
Newborn
3 yrs
7 yrs
Sphenoid Bone Pneumatization
• Follows marrow conversion
• Begins at about 1 – 2 years
• Reaches the sella by about 7 years
• Mature by 15 years
• Asymmetric pneumatization is common
• Lateral recess pneumatization– Splays distance between f. rotundum & vidian canal

11-year-old boy with headache and lethargy
Leukemic marrow infiltration - ALL

Three-year-old with nasal congestion
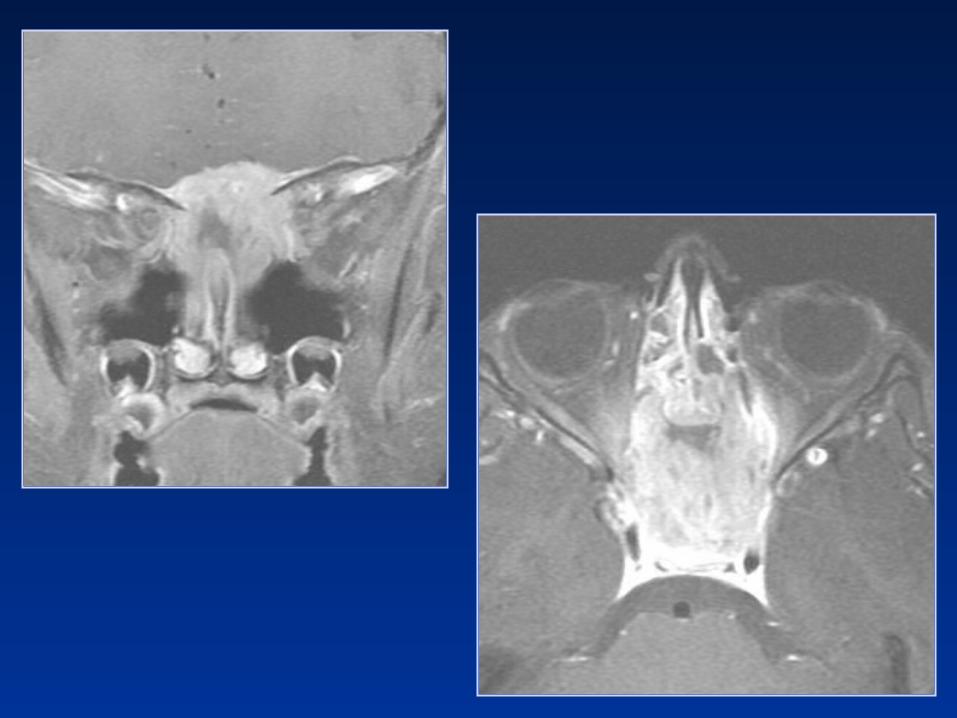
Diagnostic Considerations?
1. Metastasis
2. Rhabdomyosarcoma
3. LCH
4. Chordoma
5. Chondrosarcoma

Langerhans’ Cell Histiocytosis
• Denditic cell proliferation
• Skull (calvarium>orbit>skullbase)– Mandible> ribs> femur> pelvis> spine
• Imaging– Punched-out, beveled, lack of sclerosis – Sequestration +/-– T1 hyper - isointensity ~ lipid laiden histiocytes– T2 signal variable
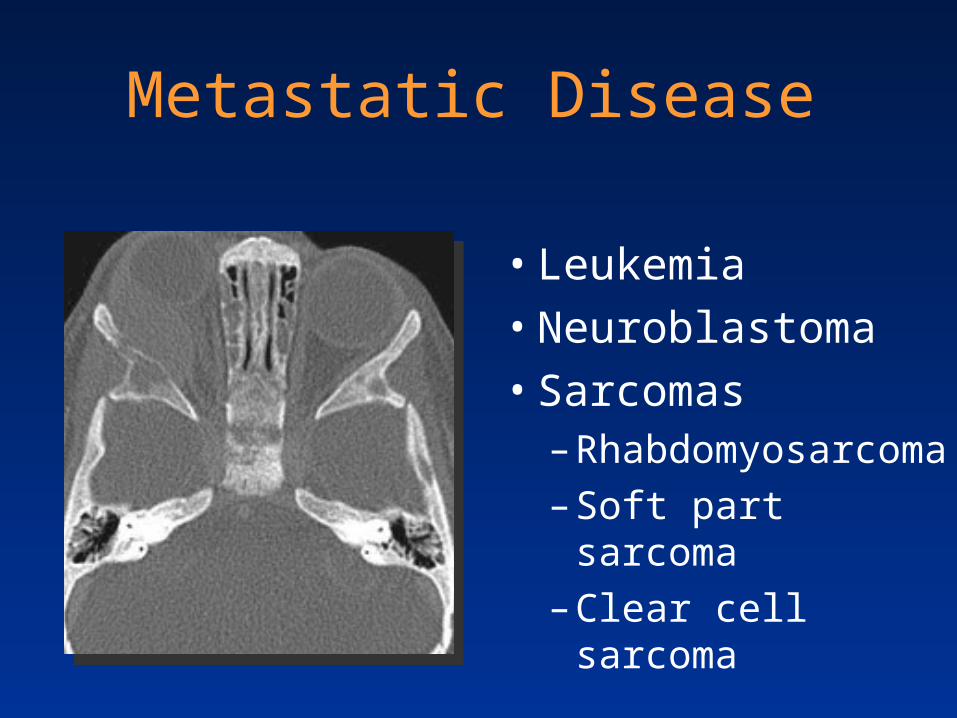
Metastatic Disease
• Leukemia
• Neuroblastoma
• Sarcomas– Rhabdomyosarcoma
– Soft part sarcoma
– Clear cell sarcoma

Seven-year-old female with headache and nasal congestion
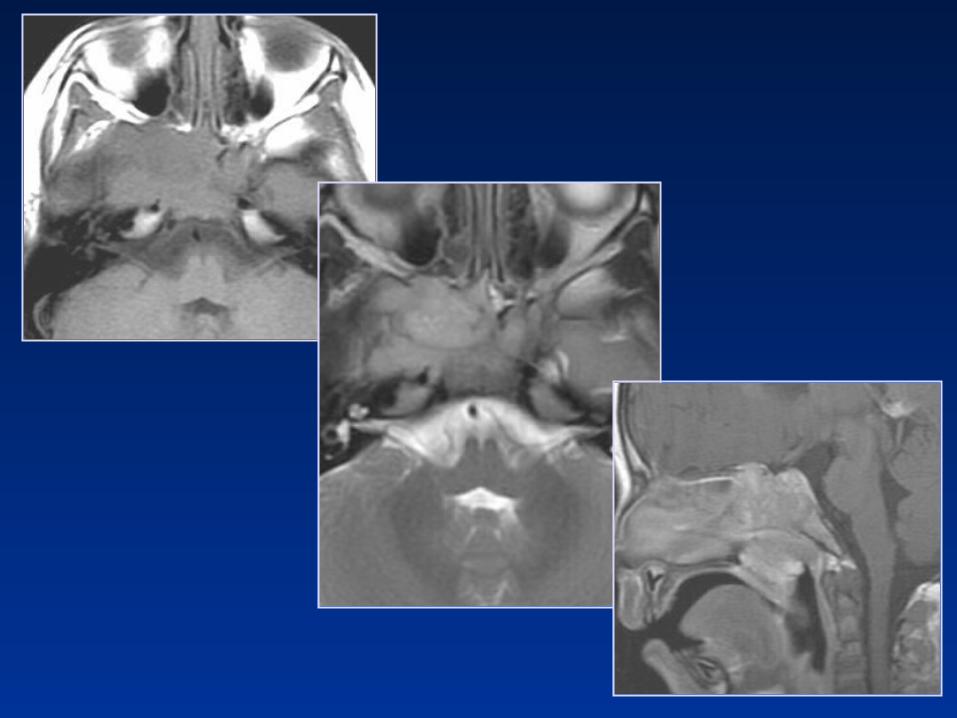
Rhabdomyosarcoma• Most common childhood soft tissue sarcoma• More common in African American children • H&N involvement in 50%
– Orbit– Parameningeal
• Nasal cavity, NP, sinuses, parapharyngeal, masticator, pterygopalatine fossa, middle ear
– Other • Cervical nonparameningeal

Imaging of Rhabdomyosarcoma
• CT– Bony lysis – ST attenuation
• MR
T1 hypo to isointense
T2 hyperintense
Variable enhancement
NonrhabdomyosarcomaSoft Tissue Sarcomas (NRSTSs)
• Fibrosarcoma
• Primitive neuroectodermal tumor (PNET)
• Malignant peripheral nerve sheath tumor
• Ewing sarcoma
• Synovial sarcoma
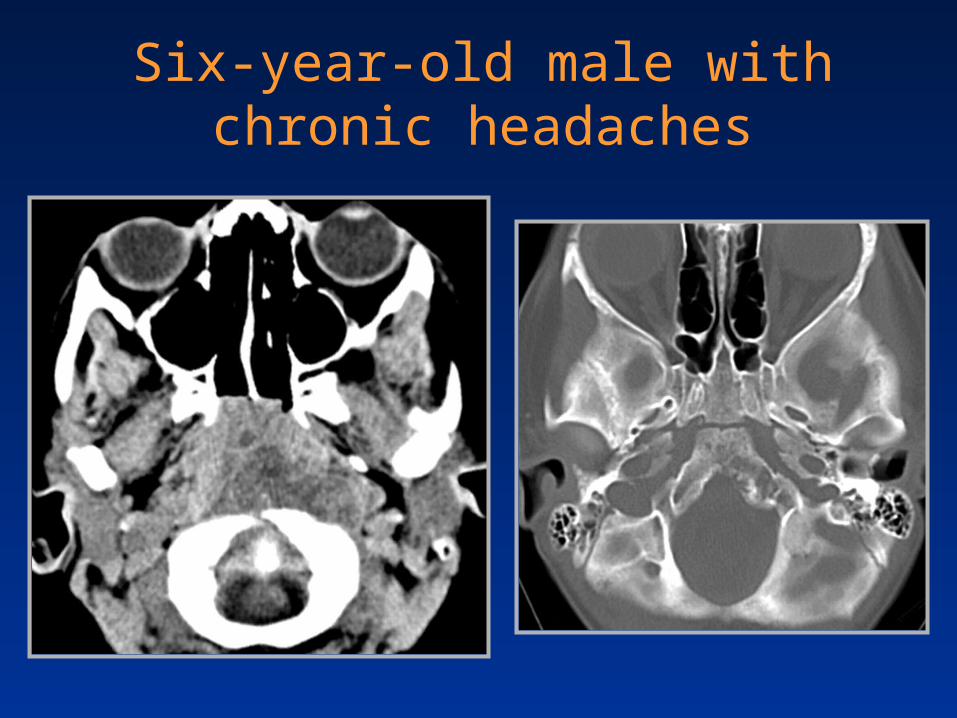
Six-year-old male with chronic headaches


Clival Chordoma
• Primitive notocord remnant
• Location– 35% skull base– 50% sacrococcygeal– 15% vertebral body

Clival Chordoma
• T1WI– Intermediate to low
signal– Focal hemorrhage
• T2WI– High signal intensity– Heterogeneous
• T1 C+– Honeycomb
enhancement
Hemorrhage ~ 30%

Chordoma and TSC
• TSC is a harmatoneoplastic syndrome
• Autosomal dominant trait
• Nonsense mutations in TSC1 (9q34)– Found in:
• Symptomatic father • Clival chordoma of the son
Borgel J et al. Eur J Pediatr (2001) 160:138

Fourteen-year-old female with frontal headaches

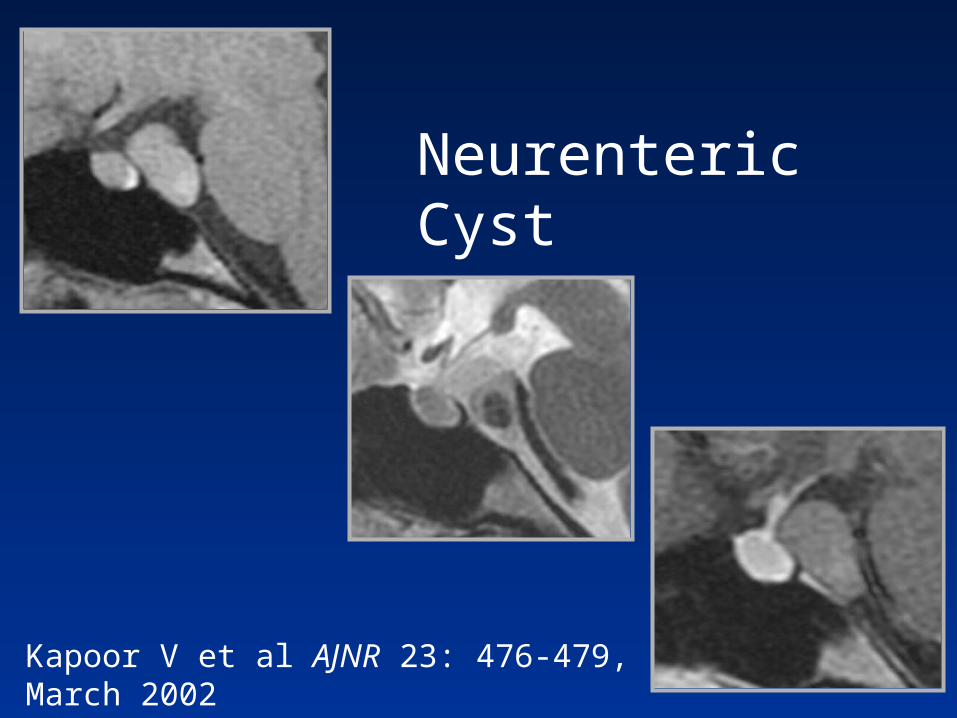
Kapoor V et al AJNR 23: 476-479, March 2002
Neurenteric Cyst
Paraclival Neurenteric Cyst
• Dysgenesis of notocord & neurenteric canal. Similar to Rathke cleft and colloid cysts
• Most involve – Craniovertebral junction and posterior fossa
• Histopathiology– Type A, resemble respiratory or GI epithelium– Type B, smooth muscle, glandular, and lymphoid– Type C, like Type B + glial elements

Summary
• Review age related ossification and maturation
• Identify anatomic variants
• Review anomalies of development
• Highlight pseudolesions and tumefactions of the central skull base