The Pediatric Central Skull Base Gary L. Hedlund, D.O. Primary Children’s Medical Center Salt Lake City, Utah

The Pediatric Central Skull Base Gary L. Hedlund, D.O. Primary Children’s Medical Center Salt Lake City, Utah.
Dec 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

The Pediatric Central Skull Base
Gary L. Hedlund, D.O.Primary Children’s Medical Center
Salt Lake City, Utah
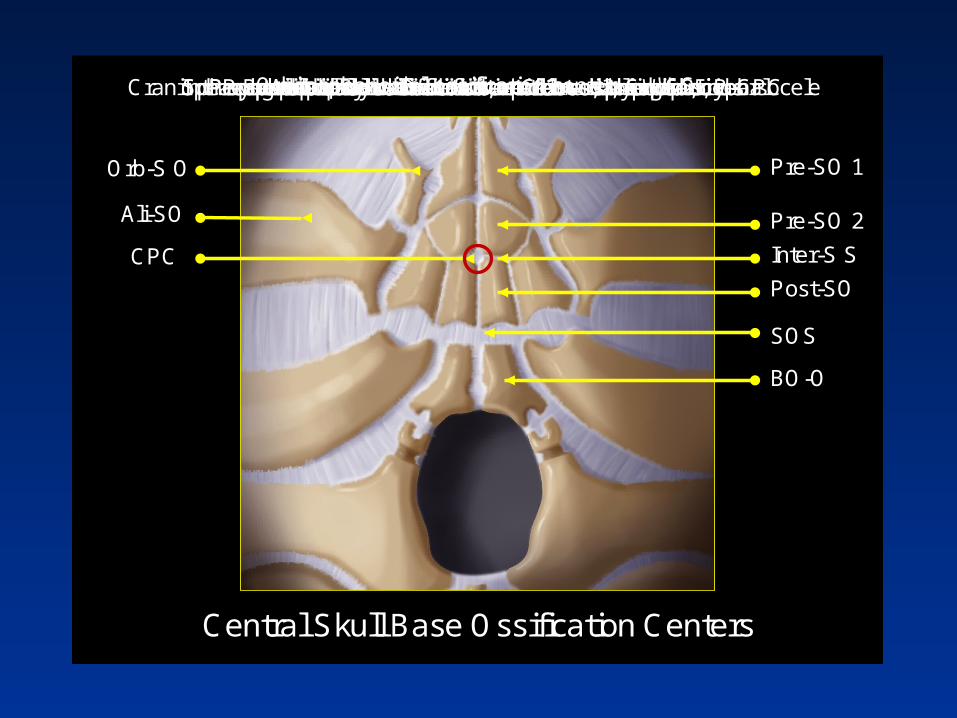
Pre-SO 1
Pre-SO 2
Inter-S S
Post-SO
SOS
BO-O
CPC
Ali-SO
Orb-S O
Central Skull Base Ossification Centers
Presphenoidal ossification center 1 → sphenoid sinusPresphenoidal ossification center 2 → sphenoid sinusIntersphenoidal synchondrosis → Closes, 3mo; if no, P-CPCPostsphenoidal ossification center → basisphenoidSphenooccipital synchondrosis → Closes by age 25 yearsBasioccipital ossification center → basiocciputOrbitosphenoidal ossification center → LWSAlisphenoidal ossification center → GWSCraniopharyngeal canal → Dermoid, epidermoid, lipoma, cephalocele


The Chondrocranium
• Portion of the neocranium formed by endochondral ossification
• 25 centers of ossification
• 18 sutures and/or synchondroses
• Anatomic variants and developmental anomalies abound
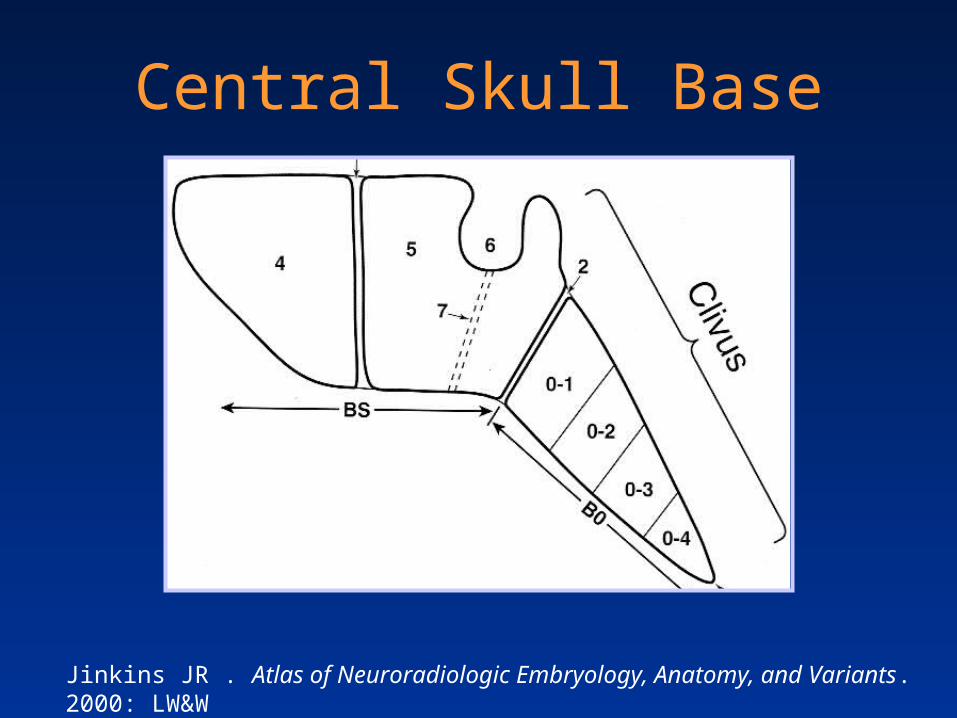
Central Skull Base
Jinkins JR . Atlas of Neuroradiologic Embryology, Anatomy, and Variants. 2000: LW&W

Newborn Central Skull Base
Newborn
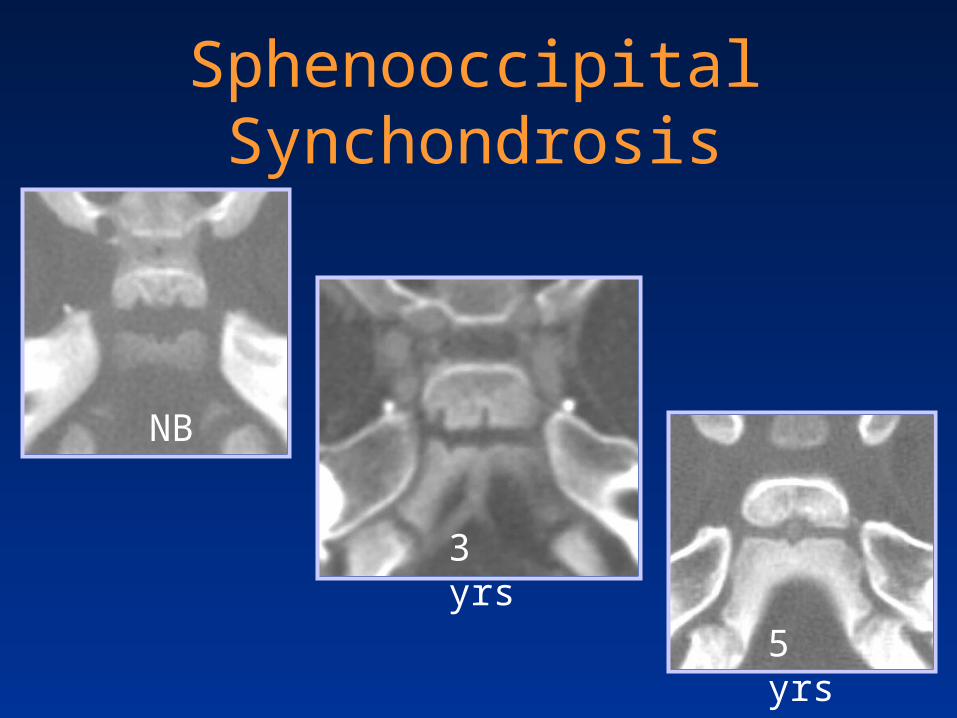
Sphenooccipital Synchondrosis
NB
3 yrs
5 yrs
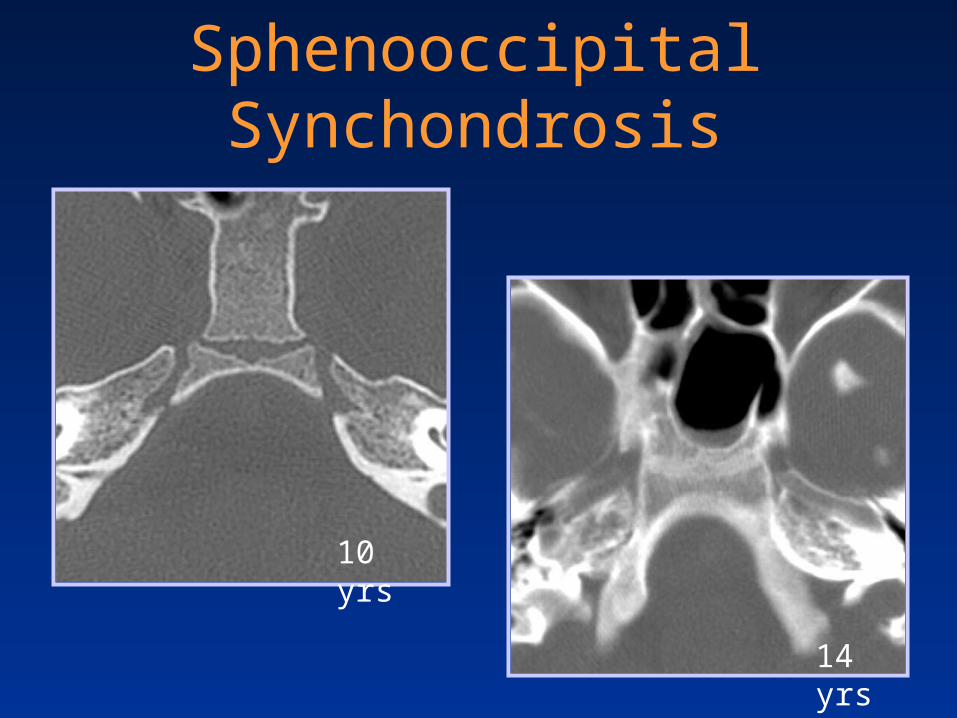
Sphenooccipital Synchondrosis
10 yrs
14 yrs

18-year-old female with closed head trauma
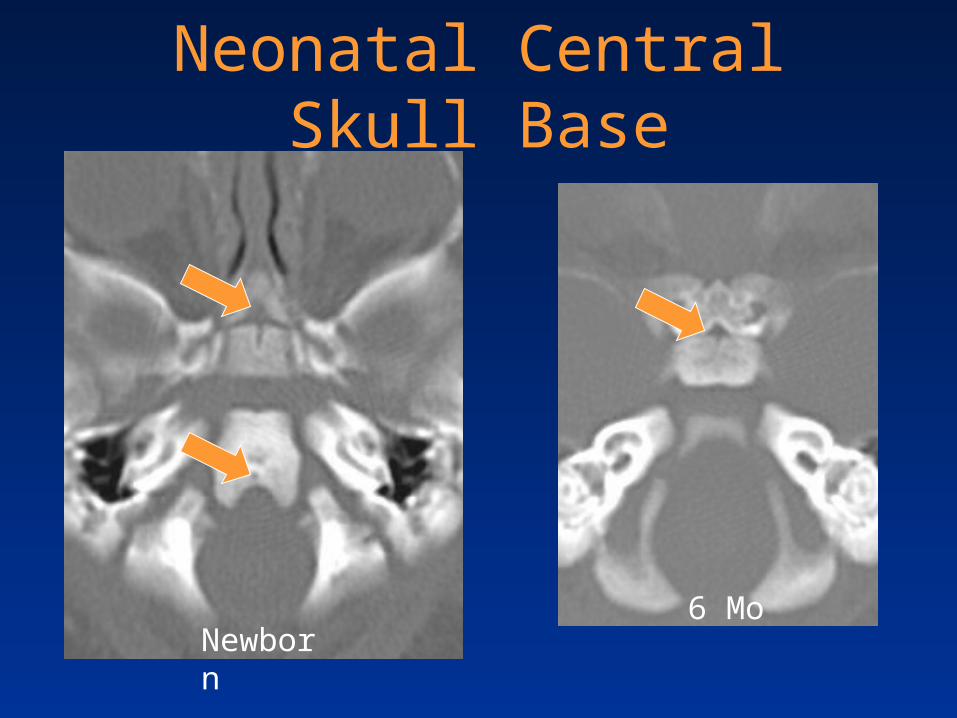
Neonatal Central Skull Base
Newborn6 Mo
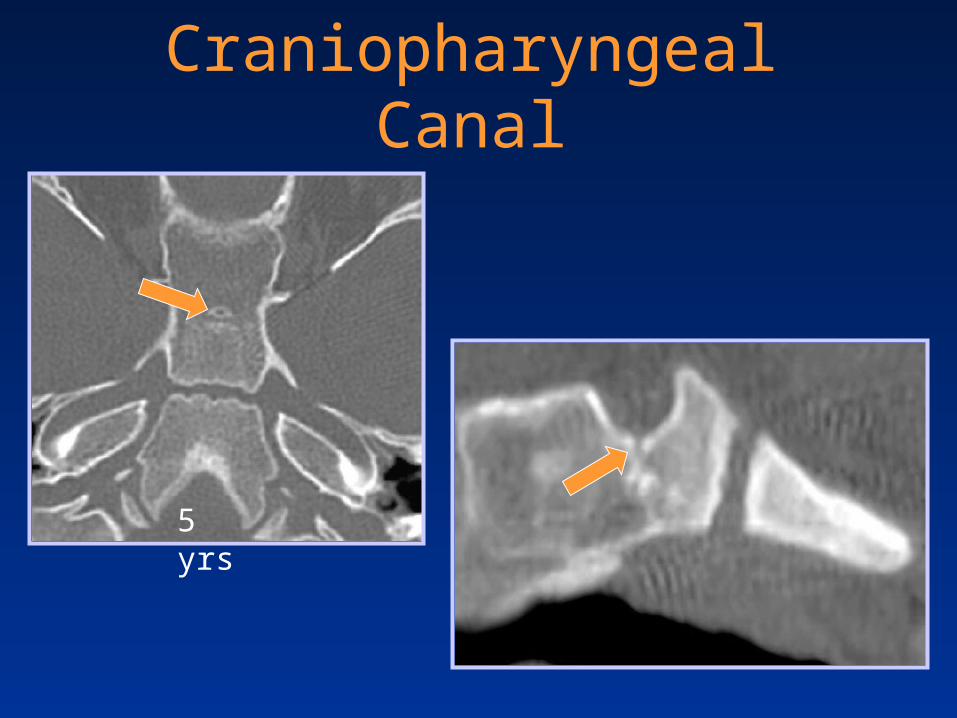
Craniopharyngeal Canal
5 yrs

Craniopharyngeal Canal
Larsen WJ. Human Embryology, 2ND ed. Saunders; 1997

Craniopharyngeal Canal
Courtesy Bronwyn E. Hamilton, MD

Infant Central Skull Base

Age Related T1WI Marrow Changes
Newborn
3 yrs
7 yrs
Sphenoid Bone Pneumatization
• Follows marrow conversion
• Begins at about 1 – 2 years
• Reaches the sella by about 7 years
• Mature by 15 years
• Asymmetric pneumatization is common
• Lateral recess pneumatization– Splays distance between f. rotundum & vidian canal

11-year-old boy with headache and lethargy
Leukemic marrow infiltration - ALL

Three-year-old with nasal congestion
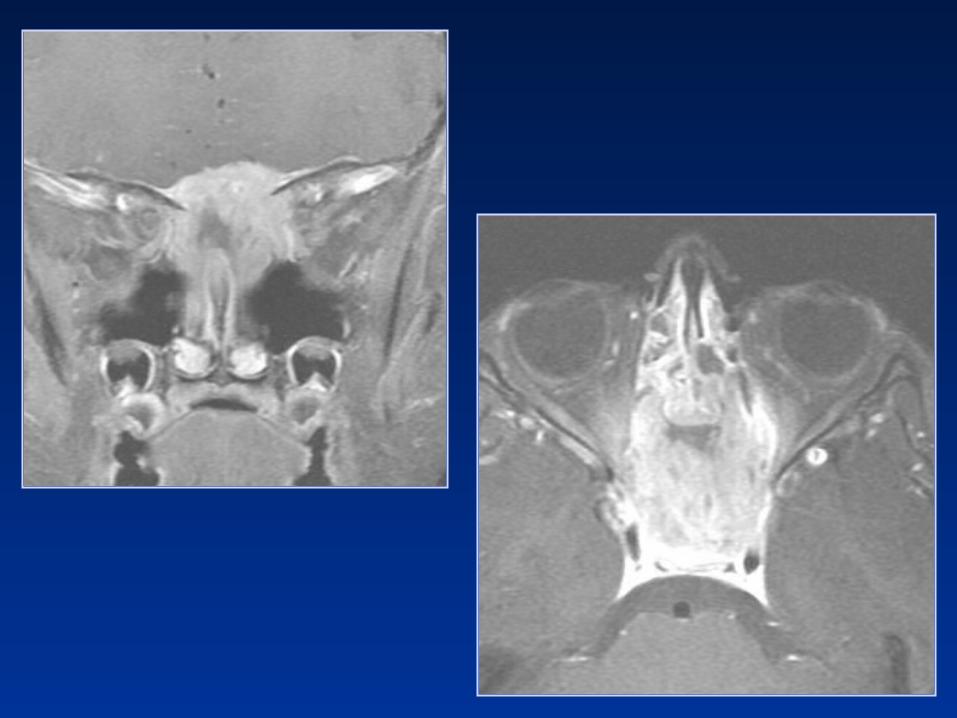
Diagnostic Considerations?
1. Metastasis
2. Rhabdomyosarcoma
3. LCH
4. Chordoma
5. Chondrosarcoma

Langerhans’ Cell Histiocytosis
• Denditic cell proliferation
• Skull (calvarium>orbit>skullbase)– Mandible> ribs> femur> pelvis> spine
• Imaging– Punched-out, beveled, lack of sclerosis – Sequestration +/-– T1 hyper - isointensity ~ lipid laiden histiocytes– T2 signal variable
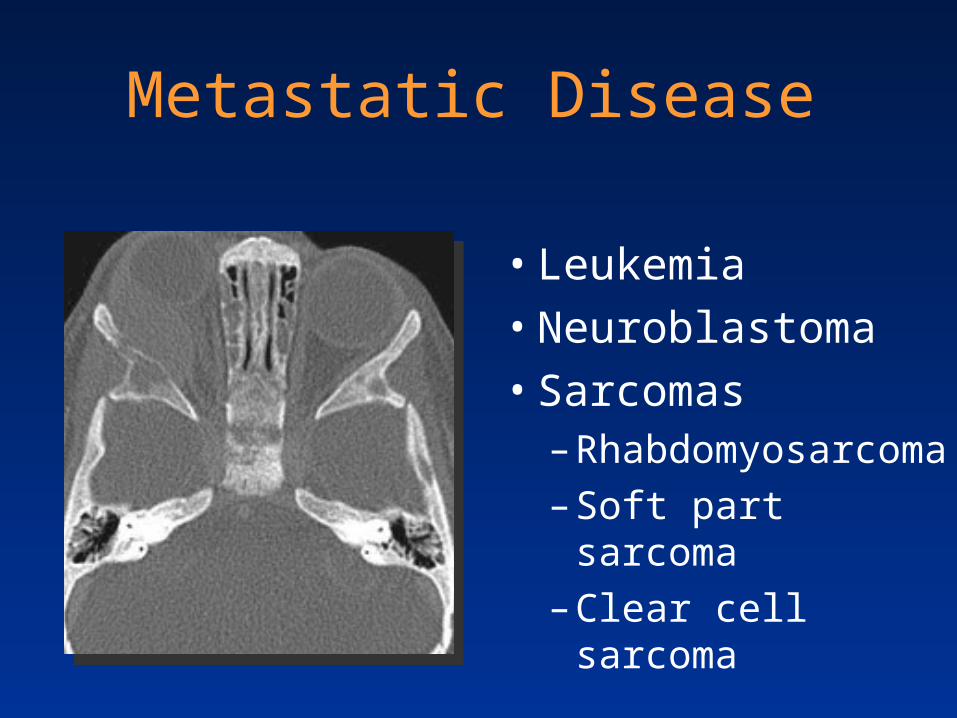
Metastatic Disease
• Leukemia
• Neuroblastoma
• Sarcomas– Rhabdomyosarcoma
– Soft part sarcoma
– Clear cell sarcoma

Seven-year-old female with headache and nasal congestion
Rhabdomyosarcoma• Most common childhood soft tissue sarcoma• More common in African American children • H&N involvement in 50%
– Orbit– Parameningeal
• Nasal cavity, NP, sinuses, parapharyngeal, masticator, pterygopalatine fossa, middle ear
– Other • Cervical nonparameningeal

Imaging of Rhabdomyosarcoma
• CT– Bony lysis – ST attenuation
• MR
T1 hypo to isointense
T2 hyperintense
Variable enhancement
NonrhabdomyosarcomaSoft Tissue Sarcomas (NRSTSs)
• Fibrosarcoma
• Primitive neuroectodermal tumor (PNET)
• Malignant peripheral nerve sheath tumor
• Ewing sarcoma
• Synovial sarcoma
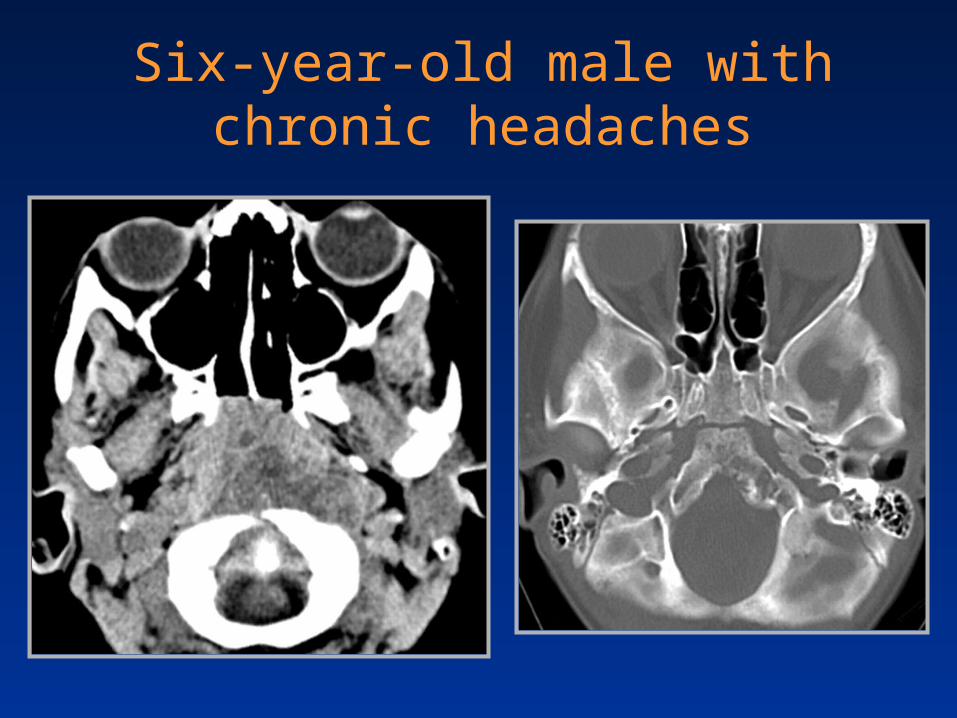
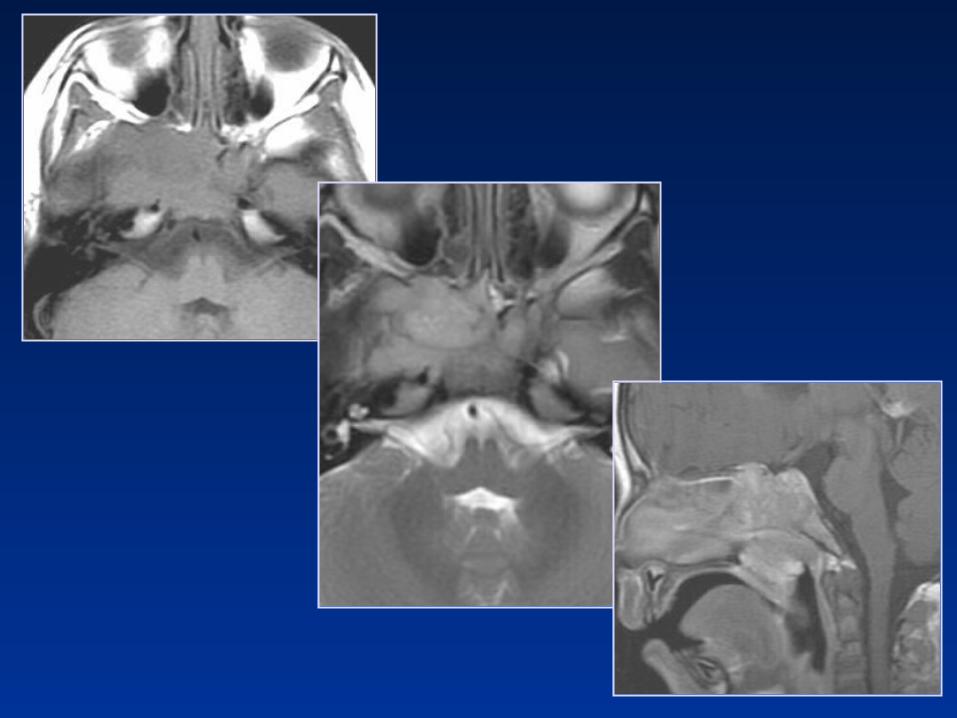
Six-year-old male with chronic headaches


Clival Chordoma
• Primitive notocord remnant
• Location– 35% skull base– 50% sacrococcygeal– 15% vertebral body

Clival Chordoma
• T1WI– Intermediate to low
signal– Focal hemorrhage
• T2WI– High signal intensity– Heterogeneous
• T1 C+– Honeycomb
enhancement
Hemorrhage ~ 30%

Chordoma and TSC
• TSC is a harmatoneoplastic syndrome
• Autosomal dominant trait
• Nonsense mutations in TSC1 (9q34)– Found in:
• Symptomatic father • Clival chordoma of the son
Borgel J et al. Eur J Pediatr (2001) 160:138

Fourteen-year-old female with frontal headaches

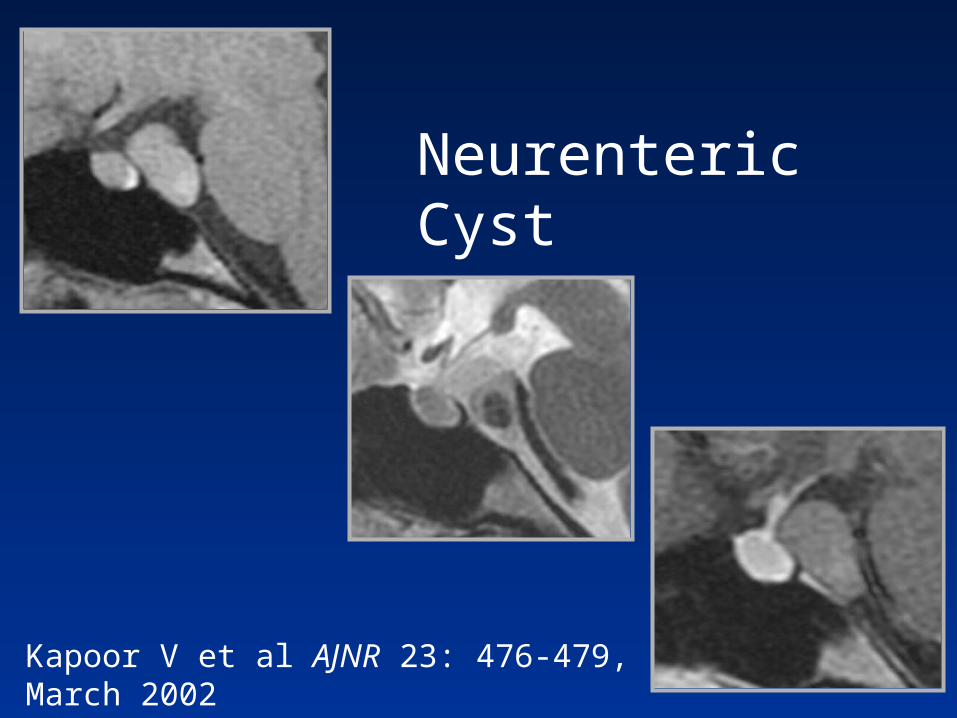
Kapoor V et al AJNR 23: 476-479, March 2002
Neurenteric Cyst
Paraclival Neurenteric Cyst
• Dysgenesis of notocord & neurenteric canal. Similar to Rathke cleft and colloid cysts
• Most involve – Craniovertebral junction and posterior fossa
• Histopathiology– Type A, resemble respiratory or GI epithelium– Type B, smooth muscle, glandular, and lymphoid– Type C, like Type B + glial elements

Summary
• Review age related ossification and maturation
• Identify anatomic variants
• Review anomalies of development
• Highlight pseudolesions and tumefactions of the central skull base

Related Documents