A MODEL OF CHILD UNINTENTIONAL INJURY 1
‘The Interrelations between Toddler Temperament, Risky Behaviour, and Unintentional
Injury: A model and pilot study’ Ashleigh M. Barber
Supervisor: Dr. Merrilyn Hooley
Deakin University
2013
213080375
“I, the undersigned, declare that this Empirical Report is less than the specified word limit, and that it comprises original work and writing by me, and that due acknowledgement has been made to all other material used.
Signed: A.M. Barber
Dated: 9/11/13

A MODEL OF CHILD UNINTENTIONAL INJURY 2
Abstract
There is a paucity of research investigating multivariate factors in paediatric unintentional injury, yet uni- or bivariate risk factors do not suffice in explicating complex aetiological pathways. A first-phase pilot study was conducted to explore relations and structure of three toddler-variables proposed in a model of unintentional injury. The study aimed to determine the psychometric properties of measures and assess feasibility of methods. Forty-eight toddlers (15-26 months) comprised the sample, and were observed for 10 minutes in a playroom (a parent was present but facing away). The room was fit out with pseudo-risky items (e.g., plastic knife and fork, water-filled cleaning bottle) to mirror real-world environmental hazards. Parents completed questionnaires about child’s temperament and injury history prior to testing. Sound reliability and validity was found for the five observed Risky Behaviours (latency to engage with risky item; proximity to parent; visual-verbal interactions; innocuous engagement; hazardous engagement). Parent-report temperament and Injury Scores, derived from a novel, post-data collection rating scale for injury histories, revealed good internal consistency and convergent validity. Results revealed only one of five temperament factors (comprised of three traits: positive anticipation, low intensity pleasure, and sociability), was significant, revealing an interaction with toddler’s sex to produce differential risk of unintentional injury in girls and boys. It is concluded that multivariate investigations reveal important interactions that are cannot be intuitively or statistically discerned through single or dual variables alone.
A MODEL OF CHILD UNINTENTIONAL INJURY 3
‘The Interrelations between Toddler Temperament, Risky Behaviour, and Unintentional
Injury: A model and pilot study’
Each child injury event is underpinned by a chronology of factors that engage in a
bidirectional interplay long before an injury even occurs. This makes it difficult to
discern a child who is definitively ‘at-risk’, because risk by definition is asymptomatic
before an injury occurs. Schwebel and Barton (2005) allude to the idea of explicating
the phenomena that places children at risk of injury, which would allow aetiological
processes to be better understood, and in turn, effective preventative methods be
developed. However, research in the area of paediatric unintentional injury has long
explored individual risk factors, such as being male (Sorenson, 2011), having a difficult
temperament (i.e., negative emotionality; irritability) (Schwebel, Brezausek, Ramey, &
Ramey, 2004), prior injuries (Johnston & Martin-Herz, 2010; Ramsay et al., 2003) and
showing externalising behaviour such as hyperactivity (Karazsia, Guilfoyle, &
Wildman, 2012). These are too general to be useful identifiers of children at risk.
Furthermore, developmental outcomes are the product of child-environment interplay,
indicating that extant univariate models lack the explanatory capacity to discern the
latent multivariate processes in paediatric injury (Allegrante, Hanson, Sleet, & Marks,
2010).
The purpose of this research project is therefore to develop a model exploring the
multiple pathways involved in child injury risk, which involve factors at the child,
parent and environmental levels. In this thesis, a model is proposed that involves two
tiers, the first of parent factors (parental personality, style, and behaviour) and the
second of child factors (temperament, behaviour, injury) which interact in a
bidirectional manner. In this first stage of pilot testing, preliminary testing of the
second, toddler tier is undertaken. First, measures of temperament are analysed to
confirm factor structure. Second, the psychometric properties of a novel Injury History
Rating Scale, and of observed risky behaviours are assessed. Finally, initial regression
analyses are undertaken to explore the combinations of factors involved in unintentional
injury. In order to orient the reader to the importance of developing a model of child
injury, a brief summary of research taking a univariate approach to injury risk factors if
presented. This is followed by an introduction to the model, and an explication of the
A MODEL OF CHILD UNINTENTIONAL INJURY 4
second tier, toddler factors, which will be the focus of pilot testing in this thesis.
Preschool children aged 1 to 4-years are particularly at risk of injury, since their
development renders them limited in their capacity to first discern unsafe situations, and
second safely manipulate them if they arise. As such, young children rely on caregivers
to maintain their safety (Simpson, Turnball, Ardagh, & Richardson, 2009). Parents are
suggested to moderate child injury risk via three fundamental mechanisms; supervision,
teaching safety rules, and modifying the environment (Morrongiello, Ondejko, &
Littlejohn, 2004a; Morrongiello, Ondejko, & Littlejohn, 2004b). Many complex factors
are implicated in determining the quality and quantity of which a parent might
implements these (Schwebel, Brezausek, Ramey, & Ramey, 2004). For example,
assessing environmental risks (Schwebel et al., 2004), accurately predicting the child’s
behaviour (Wells, Morrongiello, & Kane, 2012), and modifying such parental behaviour
as supervision according to the perceived fit between behaviour prediction and risk
assessment (Munro, Van Niekerk, & Seedat, 2006). Patently, several factors determine
how successfully parents perform each of these, with both parent- and child-oriented
factors being important. A set of factors such as the aforementioned parenting
behaviours are more fitting to the phenomena which places or protects against a child at
risk of injury.
Aforementioned factors that have been shown to be fundamental in moderating
child injury risk (e.g., supervision, teaching about safety and hazards), are indeed
important to add to the understanding of injury but being able to predict why some
parents engage in positive levels of these behaviours and others do not is more
important. Morrongiello (2005) highlighted this, by stating the importance of
identifying predictors of specific caregiver behaviours because behaviours vary
according to the context they appear in. There is a paucity of research on the factors that
might explain the differences found in parent-child interactions, even when outward
characteristics appear to be similar. Specifically, what factors could provide an
explanation at a more stable level than behaviour, such as why children have high and
low injury histories when their temperaments are similar and their parents have similar
parenting styles. Personality is a psychobiological characteristic that has been found to
be a sound determinant of behaviour. Likewise, temperament has strong biological
components but due to the plasticity associated with early childhood development, is
A MODEL OF CHILD UNINTENTIONAL INJURY 5
not as stable as personality, but is the most stable predictor of child behaviour
(Schwebel & Plumert, 1999).
Toddler temperament is thus always referenced as a leading risk or protective
factor in injury. The three strongest predictor traits of injury risk in toddlers are reported
as (high) activity level, (high) impulsivity, and (low) inhibitory control (Schwebel &
Barton, 2006; Schwebel & Gaines, 2007). High activity and impulsivity have been
found to strongly link with externalised problem behaviours (De Pauw et al., 2009) such
as hyperactivity and low compliance with parental demands (Cole, Koulouglioti,
Kitzman, Sidora-Arcoleo, & Anson, 2009; Morrongiello, Midgett, & Shields, 2001).
Since externalising behaviour is consistently found to relate to increased injury risk
(Van Aken, Junger, Verhoeven, Van Aken, & Deković, 2007; Williams et al., 2009),
and high levels of activity and impulsivity predict greater externalised than internalised
behaviour (Prinzie et al., 2012), children high on these traits are considered to be at a
greater risk of injury. Research has found significant relationships between
temperament and both risk-taking behaviour and the number of injuries endured
(Bijttebier, Vertommen, & Florentie, 2003). One tentative explanation for the pathway
between overestimation of physical abilities and temperament might be that children
with high impulsivity and poor inhibitory control overestimate their ability to complete
a task by way of rapid and incautious judgments about their physical abilities
(Schwebel, 2004a). However, these studies included school-aged children who have
enough cognitive maturity to engage in risk taking consciously.
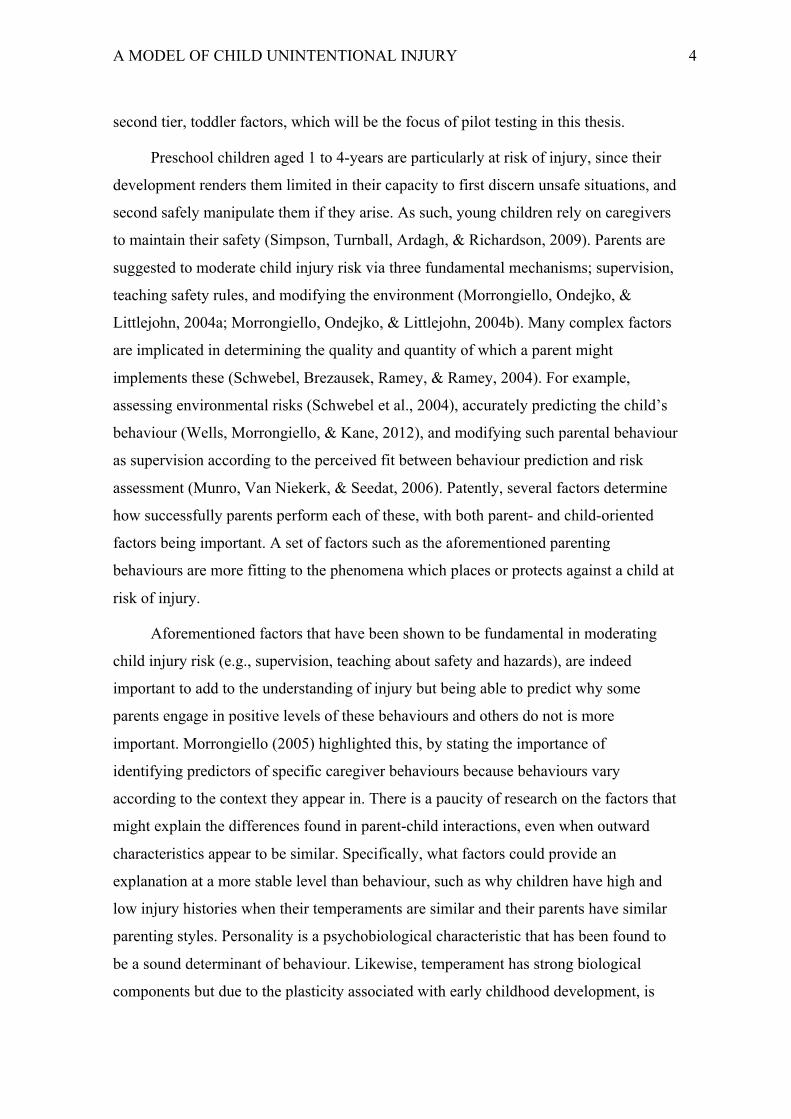
Figure 1: A Conceptual Risk-Protection model of Childhood Injury.
A MODEL OF CHILD UNINTENTIONAL INJURY 6
The conceptual model proposed in this pilot study was developed in response to a
few of the discerned gaps in the child injury literature. The six-variable model is nested
within the framework of developmental theory (Bronfenbrenner’s Bioecological
systems), and thus supports cross-tier interplay or interactional effects between any
combinations of its variables. One of the leading gaps discovered in extant research is
the limited research with a multivariate-focus, especially in child injury and parenting.
That is, the extensive research that has been done on uni- or bivariate relations is likely
to have missed important mutual influences and interaction effects, perhaps leading to
spurious results. This explains why there is no definitive answer to why personality
dimensions as predictors are not consistent across studies when they so reliability and
validly measure the construct, and why studies exploring temperament dimensions do
not consistently derive the same conclusions about the same traits. Parental personality
and Temperament are predictors of emotional climate (warmth, responsiveness, control)
and risky behaviour respectively, while personality also predicts parenting behaviour
but is mediated by emotional climate. That is, parenting behaviour must always be
presented in an emotional context such as a tone of voice or body language, and this
interacts with toddler temperament to influence toddler behaviour. Parenting behaviour
is comprised of supervision, teaching, and modification of the environment, which have
the opportunity to moderate risk twice in the process towards injury. First, it may
moderate the relationship between temperament and risky behaviour, by reducing the
effects of risky traits, and second, by moderating the relationship between risky
behaviour and injury, for example by removing hazards from the environment.
The purpose of this pilot study is to determine the feasibility, reliability, and
validity of the measures (questionnaires) and methods (observation) in order to test the
proposed model of childhood injury. The aims are two-fold, first, to identify the most
influential clusters of temperamental and behavioural factors in unintentional injury,
and secondly to explore and describe interrelations between toddler temperamental,
behavioural and injury variables. Specific hypotheses concerning the variable relations
are not presented as robust extant evidence is lacking. All analyses in this pilot study are
considered exploratory.
Method.
A MODEL OF CHILD UNINTENTIONAL INJURY 7
Participants.
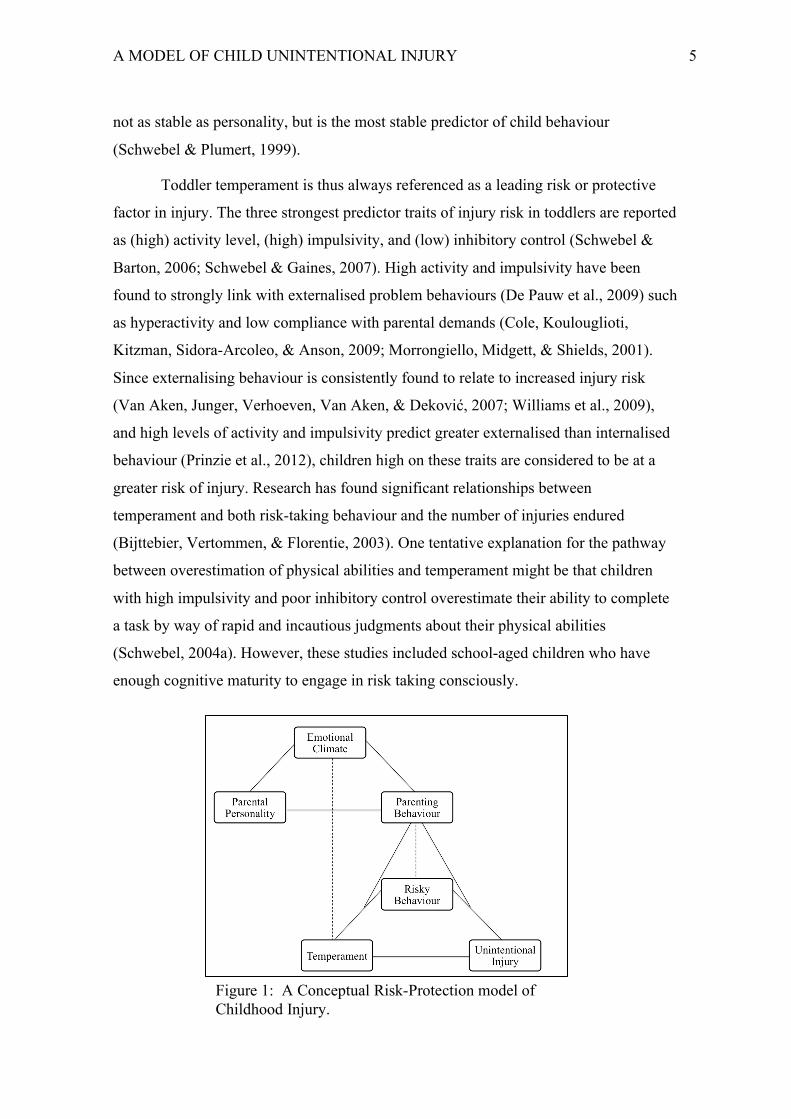
The sample included 62 parent-child dyads (56% female, 44% male), who
volunteered to participate either in the survey and observation (n = 48, 77.4%) or online
surveys (no observation; n = 14, 22.6%). Toddlers ranged in age from 16 and 25 months
(M = 21.31, SD = 3.56). Participants were recruited from local relevant sites such as toy
libraries, playgroups, swimming pools, and kindergyms by leaving flyers and promoting
the study in-person. Sociodemographic information about the sample is presented in
Table 1, which shows that toddlers were primarily Australian (61.3%), from dual-parent
families (93.5%), had caregivers who were tertiary educated (61.3%), and from a
residential area associated with a high socioeconomic background (59.7%), according to
Australian Bureau of Statistics’ (ABS) postcode-to-socioeconomic status concordance
(ABS, 2006).
Table 1 Sample sociodemographic characteristics
Males Females Total n % n % n % Cultural background Australian 19 54.3 20 74.1 39 62.9 Australian-other 7 20 3 11.1 10 16.1 Other 9 25.7 4 14.8 13 21.0 Family composition Dual-parent 33 94.3 25 92.6 58 93.5 Single-parent 2 5.7 2 7.4 4 6.5 Postcode socioeconomic status Low 3 8.6 5 18.5 8 12.9 Middle 10 28.6 7 25.9 17 27.4 High 22 62.9 15 55.6 37 59.7 Primary caregivers highest level of education Bachelor/Postgraduate 22 62.8 16 40.7 38 61.3 Diploma or school 13 37.2 11 59.2 24 38.7
Measures.
Questionnaires.
Demographics
The parent-report demographics questionnaire requested information about the
child’s developmental history and familial background such as toddler age, parent’s
education level, and family cultural identity and composition (see Appendix B).

A MODEL OF CHILD UNINTENTIONAL INJURY 8
Toddler Temperament.
The Early Childhood Behaviour Questionnaire (ECBQ; Putnam, Ellis, &
Rothbart, 2001) is a 201-item parent-report instrument, which was used to measure
temperament (Appendix B). The measure produces 18 temperament dimension scores
by averaging item scores, with higher scores indicating greater levels of that trait. A 7-
item response scale (1, never to 7, always) gauged the incidence of behavioural displays
of each trait in various situations over the past two weeks. For example, items from the
High Intensity Pleasure (HIP) subscale (HIP is feeling enjoyment at times of intense,
novel, or complex sensory stimuli), ask such questions as “While playing outdoors
[situation], how often did your child, want to climb to high places (for example, up a
tree or on the jungle gym) [behaviour]” The internal consistency of the ECBQ in this
sample was very good, Cronbach’s alpha for 18 dimensions were very good (all α =
>.99). Sound internal consistency is also reported by the original authors’, with α
ranging from .57 for impulsivity to .90 for perceptual sensitivity (Putnam, Ellis, &
Rothbart, 2006).
Injury history.
Injury data were collected from parents retrospectively via the Injury History
Survey (Appendix B), which was developed for an associated project. It is a qualitative
5-columned grid with the following headers: Frequency in past month (e.g., 7 times),
Injury-related activity (e.g., climbing), Injury Description (e.g., bump), Severity (e.g.,
no medical attention), Location/circumstances (e.g., at home). Each row corresponded
to a particular injury type, not an individual event (i.e., frequency of each type were
recorded).
Injury behaviours.
The Injury Behaviour Checklist (IBC; Speltz, Gonzales, Sulzbacher, & Quan,
1990) (Appendix B) is a 24-item parent-report questionnaire, which measures toddlers’
risk of subsequent injuries, based on their risky behaviour and injuries within the past 6
months. Scoring uses a Likert scale from 0 (not at all) to 5 (very often/more than once a
week), and higher scores indicate greater habitual risky behaviour. Of the 24 items, 18
pertain to behaviours that increase risk of injury (e.g., ‘tries to climb on top of furniture
etc.’), while 4 items relate to injuries (e.g., ‘falls down’, ‘burns self with hot objects’).
A MODEL OF CHILD UNINTENTIONAL INJURY 9
Internal consistency is found to be very good (.89) (Speltz et al., 1990).
Apparatus
Timers that were used were DSE Digital LCD stopwatches, while Sony
HandyCam (DVDRDVD653) filmed the freeplay sessions, which were recorded onto
an attached Tevion DVD recorder (TEV-605).
Procedures.
Recruitment.
Ethics approval for this research project was granted by the Human Ethics
Research Unit at Deakin University (Appendix A). This study is part of a larger project,
for which invitations to participate were distributed over the first six months of the
years 2010 through 2013. Local toy libraries, kindergyms, and swimming centres in
Victoria, Australia were approached and invited to support the research by promoting
participation. One or two researchers attended consenting sites and conducted short (i.e.,
5 to 10 minute) information sessions about child injury in Australia, and what
participation in the study would entail. If this was not possible, flyers were left on-site
for potential parents. To increase participation rates and allow parents who could not
partake in the observation component to still contribute, the 2013 flyer included a web-
link to online versions of the surveys in the questionnaire pack, which was typically
mailed to participants’ residential address.
Data Collection
Questionnaires
Survey data from parents of toddlers partaking in the observation were collected
by mailing them a questionnaires pack before the observation date for return on testing
day. These packs included the Plain Language Statement and Consent Forms (Appendix
A), and the questionnaires described above (ECBQ, IBC, Injury History, and
demographics). Consent was obtained by signed consent or assumed when they
completed and submitted the survey online.
Observation
The coding protocol for the observation data was designed to measure risky
A MODEL OF CHILD UNINTENTIONAL INJURY 10
behaviour using the following five variables: Proximity from parent (seconds), Visual
references (frequency), Verbal bids for attention (frequency), Risky and Innocuous
engagement with hazardous items (seconds), which respectively refer to using items for
their intended purpose or hazardously. To control for experimenter biases, all risky
behaviour variables were either double or tripled coded, in such cases the mean was
used as the raw value.
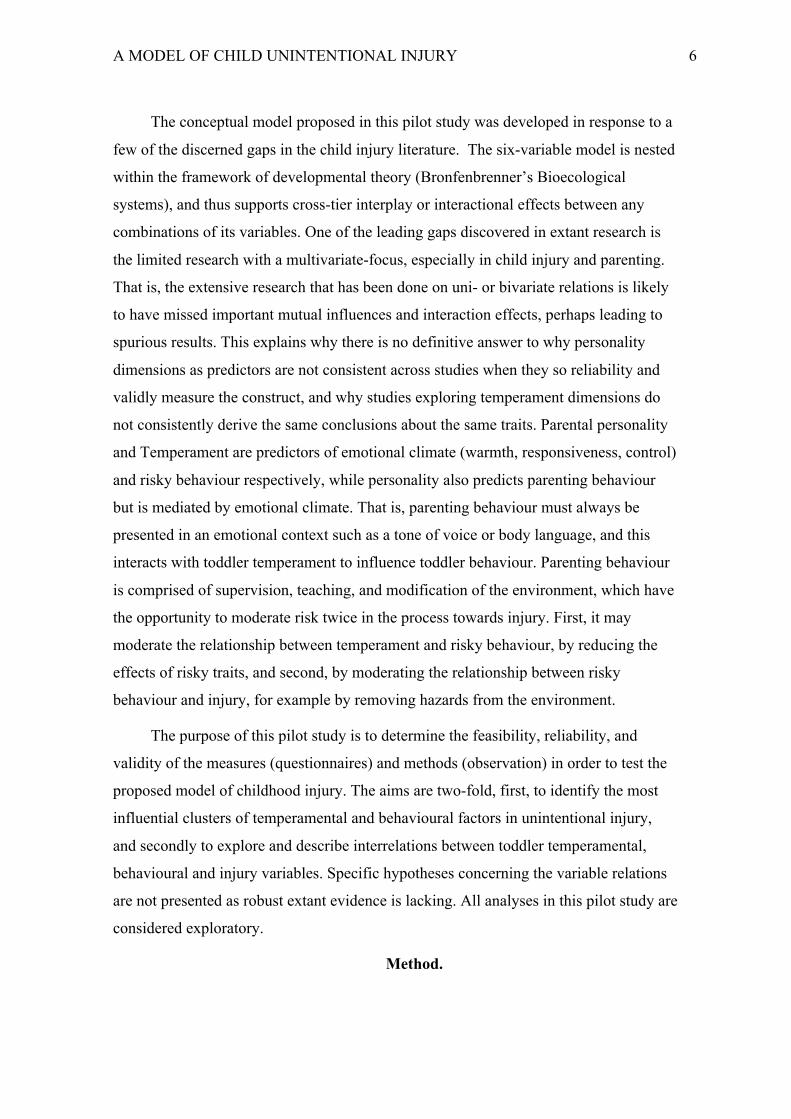
Toddlers’ risky behaviour observations took place in contrived play area (a 600cm
by 170cm corridor) within the University. Prior to beginning the observation,
questionnaires were collected from parents and the procedure for the session was
explained. Instructions to parents were to try to not interact with their child (i.e.,
interfere with child’s natural behaviour) but also to attend to the child if necessary. The
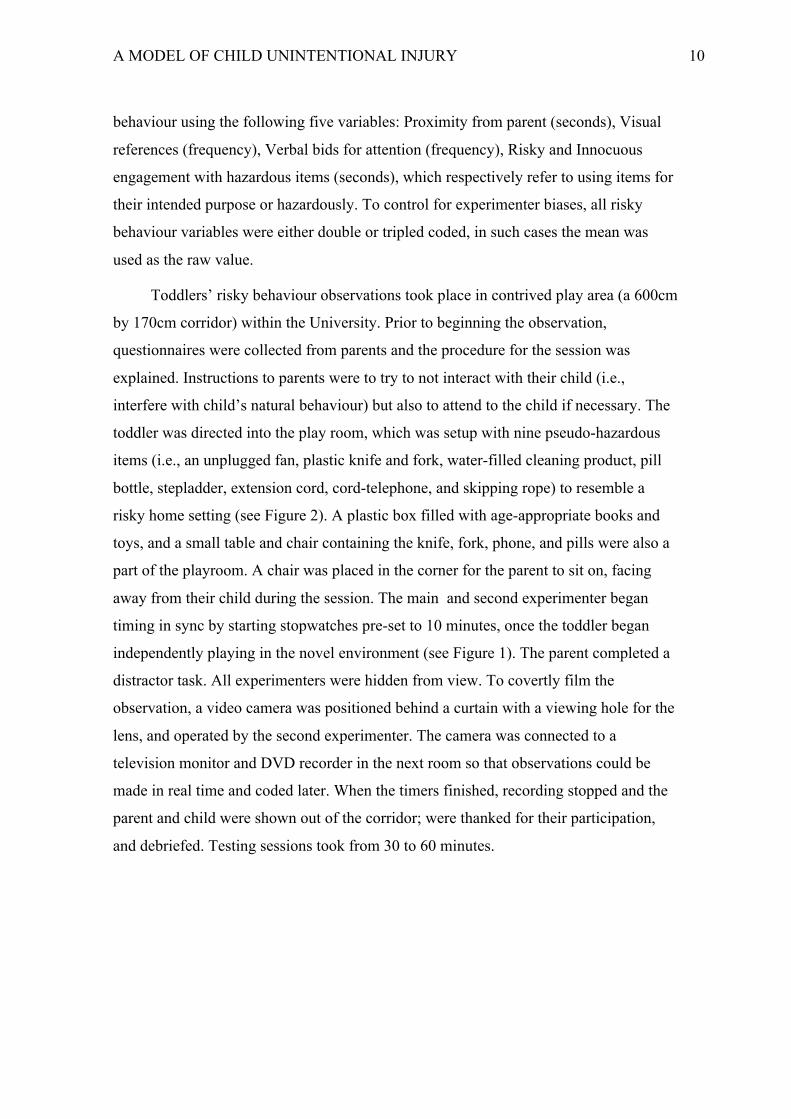
toddler was directed into the play room, which was setup with nine pseudo-hazardous
items (i.e., an unplugged fan, plastic knife and fork, water-filled cleaning product, pill
bottle, stepladder, extension cord, cord-telephone, and skipping rope) to resemble a
risky home setting (see Figure 2). A plastic box filled with age-appropriate books and
toys, and a small table and chair containing the knife, fork, phone, and pills were also a
part of the playroom. A chair was placed in the corner for the parent to sit on, facing
away from their child during the session. The main and second experimenter began
timing in sync by starting stopwatches pre-set to 10 minutes, once the toddler began
independently playing in the novel environment (see Figure 1). The parent completed a
distractor task. All experimenters were hidden from view. To covertly film the
observation, a video camera was positioned behind a curtain with a viewing hole for the
lens, and operated by the second experimenter. The camera was connected to a
television monitor and DVD recorder in the next room so that observations could be
made in real time and coded later. When the timers finished, recording stopped and the
parent and child were shown out of the corridor; were thanked for their participation,
and debriefed. Testing sessions took from 30 to 60 minutes.
A MODEL OF CHILD UNINTENTIONAL INJURY 11
Data Analysis Procedures
Injury history score
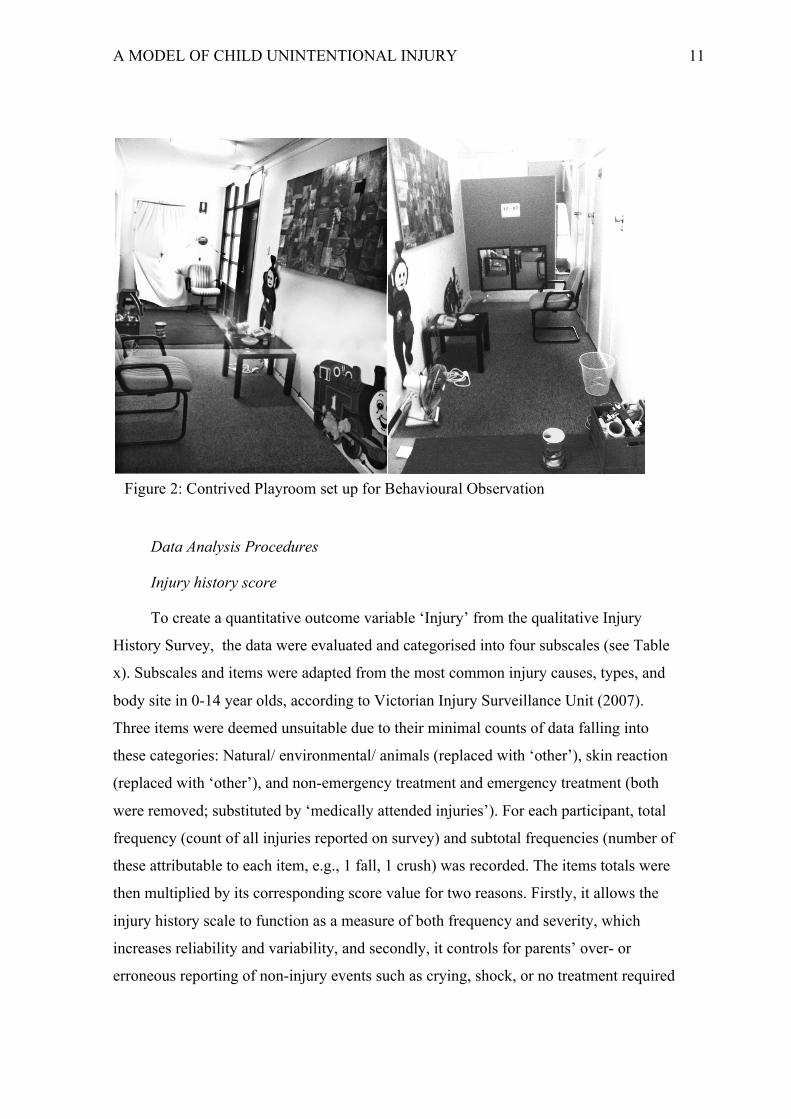
To create a quantitative outcome variable ‘Injury’ from the qualitative Injury
History Survey, the data were evaluated and categorised into four subscales (see Table
x). Subscales and items were adapted from the most common injury causes, types, and
body site in 0-14 year olds, according to Victorian Injury Surveillance Unit (2007).
Three items were deemed unsuitable due to their minimal counts of data falling into
these categories: Natural/ environmental/ animals (replaced with ‘other’), skin reaction
(replaced with ‘other’), and non-emergency treatment and emergency treatment (both
were removed; substituted by ‘medically attended injuries’). For each participant, total
frequency (count of all injuries reported on survey) and subtotal frequencies (number of
these attributable to each item, e.g., 1 fall, 1 crush) was recorded. The items totals were
then multiplied by its corresponding score value for two reasons. Firstly, it allows the
injury history scale to function as a measure of both frequency and severity, which
increases reliability and variability, and secondly, it controls for parents’ over- or
erroneous reporting of non-injury events such as crying, shock, or no treatment required
Figure 2: Contrived Playroom set up for Behavioural Observation
A MODEL OF CHILD UNINTENTIONAL INJURY 12
(multiplying by zero eliminates them from the score). Importantly, non-injury events
like near misses do not indicate injury but risk of injury, and including them would
affect construct validity, and create a circular argument within the model. Scores were
determined by using Department of Communities, Child Safety and Disability Services’
(CCDS, 2013) severity indicators, with higher scores indicating greater potential for an
injury item to result in extensive injury, lasting damage, or significantly impact
development.
Table 2.
Injury History Subscales and Items n % Subscale
Score value
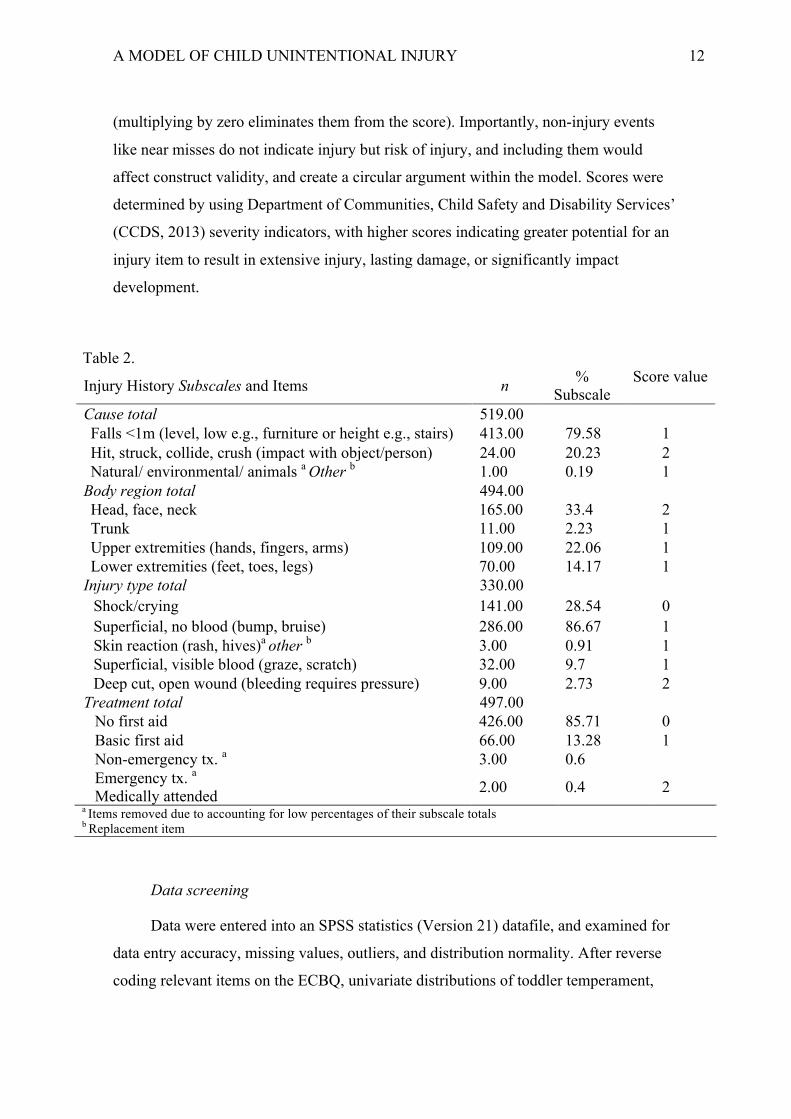
Cause total 519.00 Falls <1m (level, low e.g., furniture or height e.g., stairs) 413.00 79.58 1 Hit, struck, collide, crush (impact with object/person) 24.00 20.23 2 Natural/ environmental/ animals a Other b 1.00 0.19 1
Body region total 494.00 Head, face, neck 165.00 33.4 2 Trunk 11.00 2.23 1 Upper extremities (hands, fingers, arms) 109.00 22.06 1 Lower extremities (feet, toes, legs) 70.00 14.17 1
Injury type total 330.00 Shock/crying 141.00 28.54 0 Superficial, no blood (bump, bruise) 286.00 86.67 1 Skin reaction (rash, hives)a other b 3.00 0.91 1 Superficial, visible blood (graze, scratch) 32.00 9.7 1 Deep cut, open wound (bleeding requires pressure) 9.00 2.73 2
Treatment total 497.00 No first aid 426.00 85.71 0 Basic first aid 66.00 13.28 1 Non-emergency tx. a 3.00 0.6 Emergency tx. a
Medically attended 2.00 0.4 2 a Items removed due to accounting for low percentages of their subscale totals b Replacement item
Data screening
Data were entered into an SPSS statistics (Version 21) datafile, and examined for
data entry accuracy, missing values, outliers, and distribution normality. After reverse
coding relevant items on the ECBQ, univariate distributions of toddler temperament,
A MODEL OF CHILD UNINTENTIONAL INJURY 13
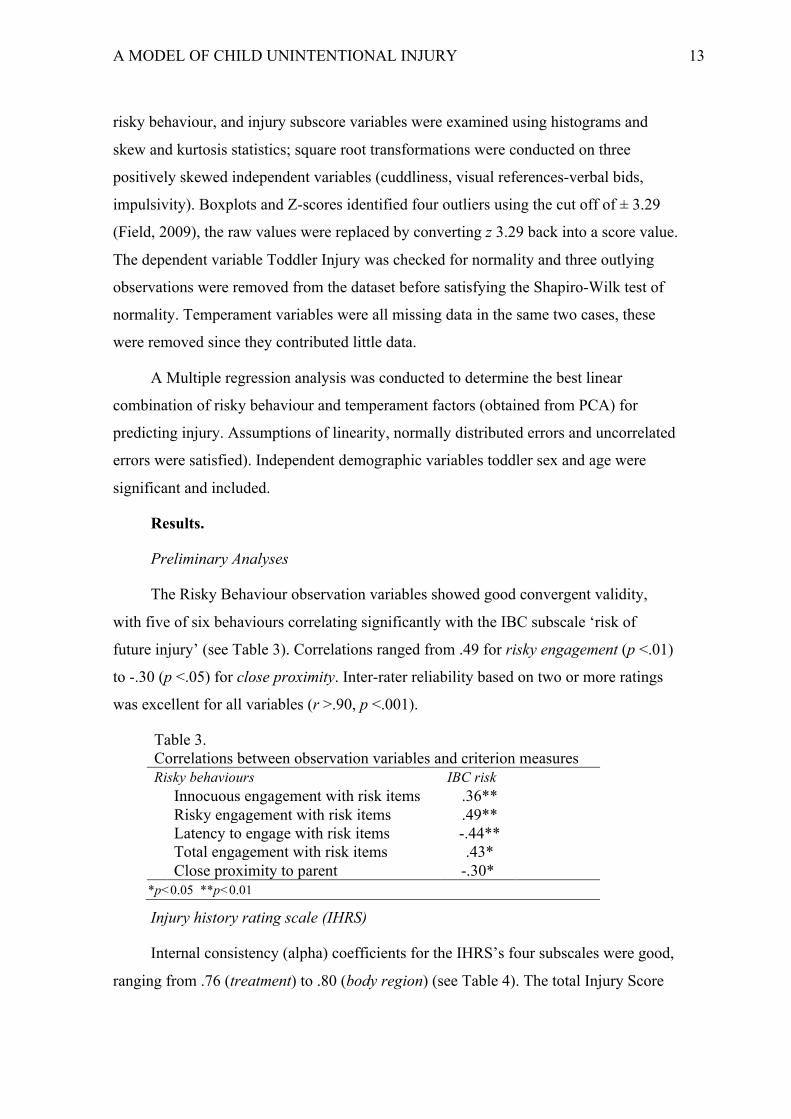
risky behaviour, and injury subscore variables were examined using histograms and
skew and kurtosis statistics; square root transformations were conducted on three
positively skewed independent variables (cuddliness, visual references-verbal bids,
impulsivity). Boxplots and Z-scores identified four outliers using the cut off of ± 3.29
(Field, 2009), the raw values were replaced by converting z 3.29 back into a score value.
The dependent variable Toddler Injury was checked for normality and three outlying
observations were removed from the dataset before satisfying the Shapiro-Wilk test of
normality. Temperament variables were all missing data in the same two cases, these
were removed since they contributed little data.
A Multiple regression analysis was conducted to determine the best linear
combination of risky behaviour and temperament factors (obtained from PCA) for
predicting injury. Assumptions of linearity, normally distributed errors and uncorrelated
errors were satisfied). Independent demographic variables toddler sex and age were
significant and included.
Results.
Preliminary Analyses
The Risky Behaviour observation variables showed good convergent validity,
with five of six behaviours correlating significantly with the IBC subscale ‘risk of
future injury’ (see Table 3). Correlations ranged from .49 for risky engagement (p <.01)
to -.30 (p <.05) for close proximity. Inter-rater reliability based on two or more ratings
was excellent for all variables (r >.90, p <.001).
Table 3.
Correlations between observation variables and criterion measures Risky behaviours IBC risk
Innocuous engagement with risk items .36** Risky engagement with risk items .49** Latency to engage with risk items -.44** Total engagement with risk items .43* Close proximity to parent -.30*
*p<0.05 **p<0.01
Injury history rating scale (IHRS)
Internal consistency (alpha) coefficients for the IHRS’s four subscales were good,
ranging from .76 (treatment) to .80 (body region) (see Table 4). The total Injury Score
A MODEL OF CHILD UNINTENTIONAL INJURY 14
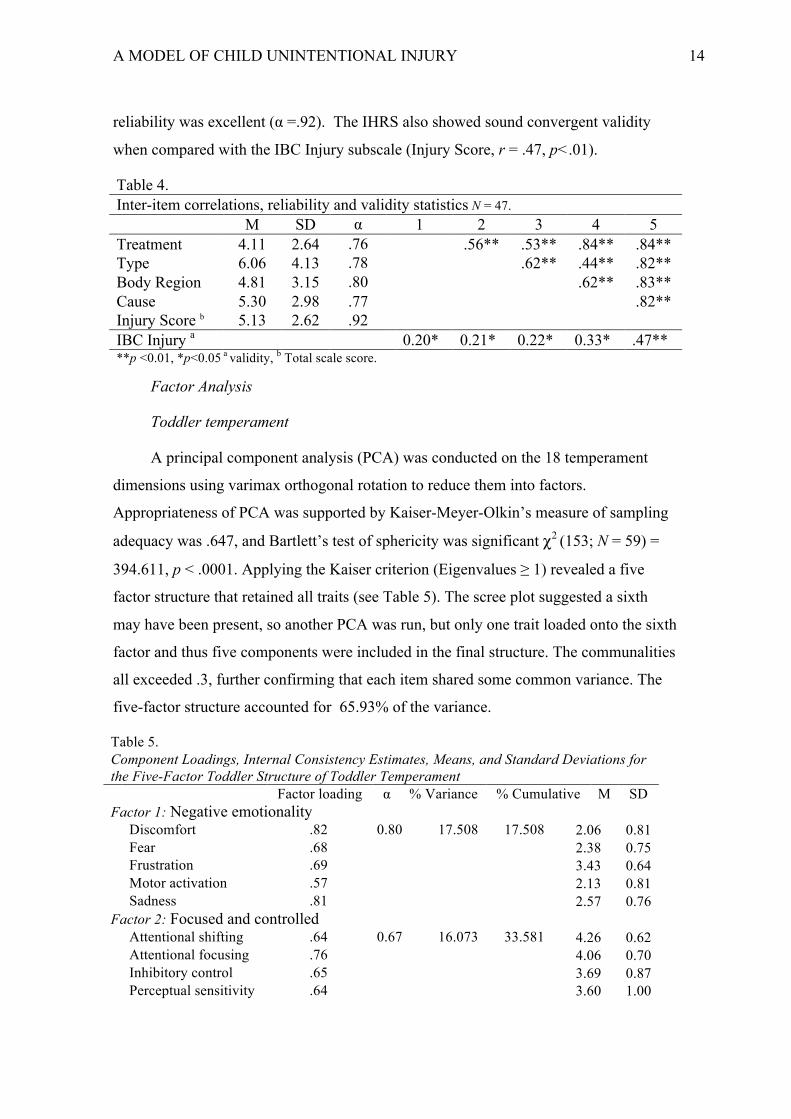
reliability was excellent (α =.92). The IHRS also showed sound convergent validity
when compared with the IBC Injury subscale (Injury Score, r = .47, p<.01).
Table 4. Inter-item correlations, reliability and validity statistics N = 47.
M SD α 1 2 3 4 5 Treatment 4.11 2.64 .76 .56** .53** .84** .84** Type 6.06 4.13 .78 .62** .44** .82** Body Region 4.81 3.15 .80 .62** .83** Cause 5.30 2.98 .77 .82** Injury Score b 5.13 2.62 .92 IBC Injury a 0.20* 0.21* 0.22* 0.33* .47** **p <0.01, *p<0.05 a validity, b Total scale score.
Factor Analysis
Toddler temperament
A principal component analysis (PCA) was conducted on the 18 temperament
dimensions using varimax orthogonal rotation to reduce them into factors.
Appropriateness of PCA was supported by Kaiser-Meyer-Olkin’s measure of sampling
adequacy was .647, and Bartlett’s test of sphericity was significant χ2 (153; N = 59) =
394.611, p < .0001. Applying the Kaiser criterion (Eigenvalues ≥ 1) revealed a five
factor structure that retained all traits (see Table 5). The scree plot suggested a sixth
may have been present, so another PCA was run, but only one trait loaded onto the sixth
factor and thus five components were included in the final structure. The communalities
all exceeded .3, further confirming that each item shared some common variance. The
five-factor structure accounted for 65.93% of the variance.
Table 5. Component Loadings, Internal Consistency Estimates, Means, and Standard Deviations for the Five-Factor Toddler Structure of Toddler Temperament
Factor loading α % Variance % Cumulative M SD Factor 1: Negative emotionality
Discomfort .82 0.80 17.508 17.508 2.06 0.81
Fear .68 2.38 0.75
Frustration .69 3.43 0.64
Motor activation .57 2.13 0.81 Sadness .81 2.57 0.76 Factor 2: Focused and controlled
Attentional shifting .64 0.67 16.073 33.581 4.26 0.62
Attentional focusing .76 4.06 0.70
Inhibitory control .65 3.69 0.87 Perceptual sensitivity .64 3.60 1.00
A MODEL OF CHILD UNINTENTIONAL INJURY 15
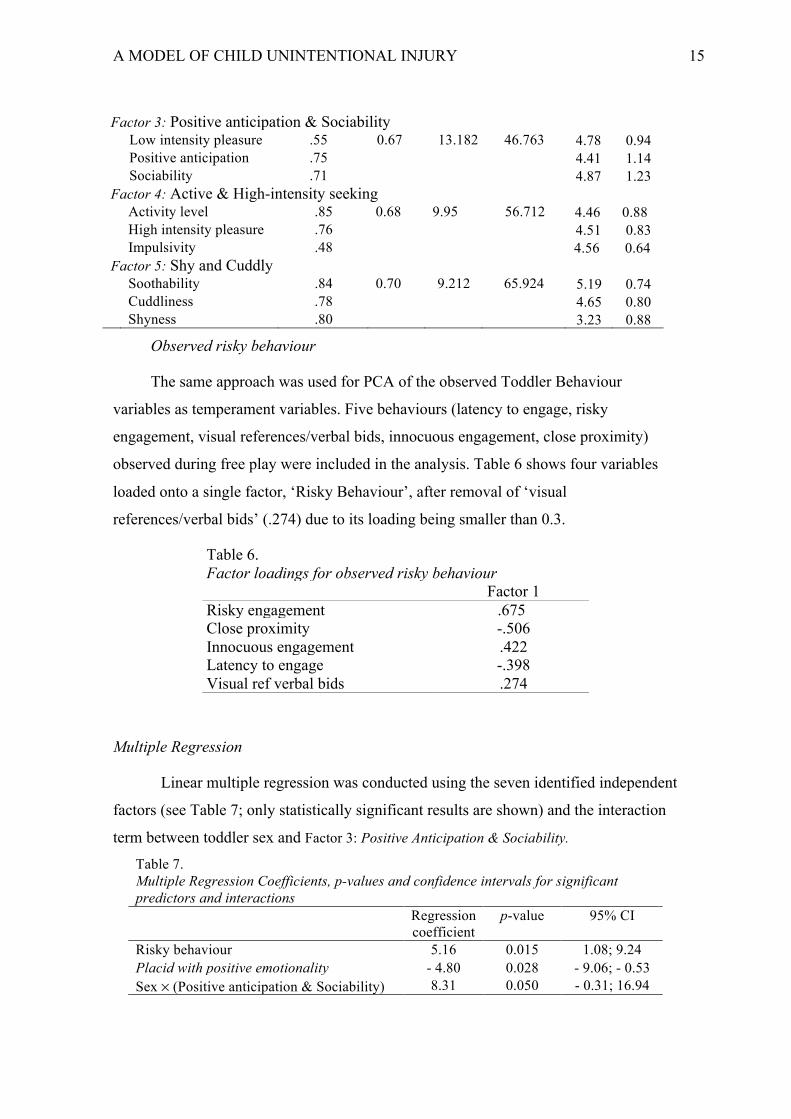
Factor 3: Positive anticipation & Sociability
Low intensity pleasure .55 0.67 13.182 46.763 4.78 0.94
Positive anticipation .75 4.41 1.14 Sociability .71 4.87 1.23 Factor 4: Active & High-intensity seeking
Activity level .85 0.68 9.95 56.712 4.46 0.88 High intensity pleasure .76 4.51 0.83
Impulsivity .48 4.56 0.64 Factor 5: Shy and Cuddly
Soothability .84 0.70 9.212 65.924 5.19 0.74 Cuddliness .78 4.65 0.80 Shyness .80 3.23 0.88
Observed risky behaviour
The same approach was used for PCA of the observed Toddler Behaviour
variables as temperament variables. Five behaviours (latency to engage, risky
engagement, visual references/verbal bids, innocuous engagement, close proximity)
observed during free play were included in the analysis. Table 6 shows four variables
loaded onto a single factor, ‘Risky Behaviour’, after removal of ‘visual
references/verbal bids’ (.274) due to its loading being smaller than 0.3.
Multiple Regression
Linear multiple regression was conducted using the seven identified independent
factors (see Table 7; only statistically significant results are shown) and the interaction
term between toddler sex and Factor 3: Positive Anticipation & Sociability. Table 7. Multiple Regression Coefficients, p-values and confidence intervals for significant predictors and interactions Regression
coefficient p-value 95% CI
Risky behaviour 5.16 0.015 1.08; 9.24 Placid with positive emotionality - 4.80 0.028 - 9.06; - 0.53 Sex × (Positive anticipation & Sociability) 8.31 0.050 - 0.31; 16.94
Table 6. Factor loadings for observed risky behaviour
Factor 1 Risky engagement .675 Close proximity -.506 Innocuous engagement .422 Latency to engage -.398 Visual ref verbal bids .274
A MODEL OF CHILD UNINTENTIONAL INJURY 16
The signs of the presented regression coefficients (Table 7) indicate the direction
of the impact of the corresponding variables on the risk of injuries. For example, the
variable with the highest significance is the observation variable Risky behaviour. The
positive sign of the coefficient corresponding to this variable (factor) means that, as
expected, increasing risky behaviour results in increasing injury probability.
The model coefficient adjusted to the sample size R2 = 0.22 means that ~ 22% of
the overall variance of Toddler Injury Score can be explained by the considered
multiple regression model (i.e., by toddler temperament and behaviour adjusted to sex
and age). While this is not a great amount of variance, it satisfies a preliminary purpose
in this pilot study that there are significant interactions, even with a sample that is
relatively small and homogeneous, and using pilot measures.
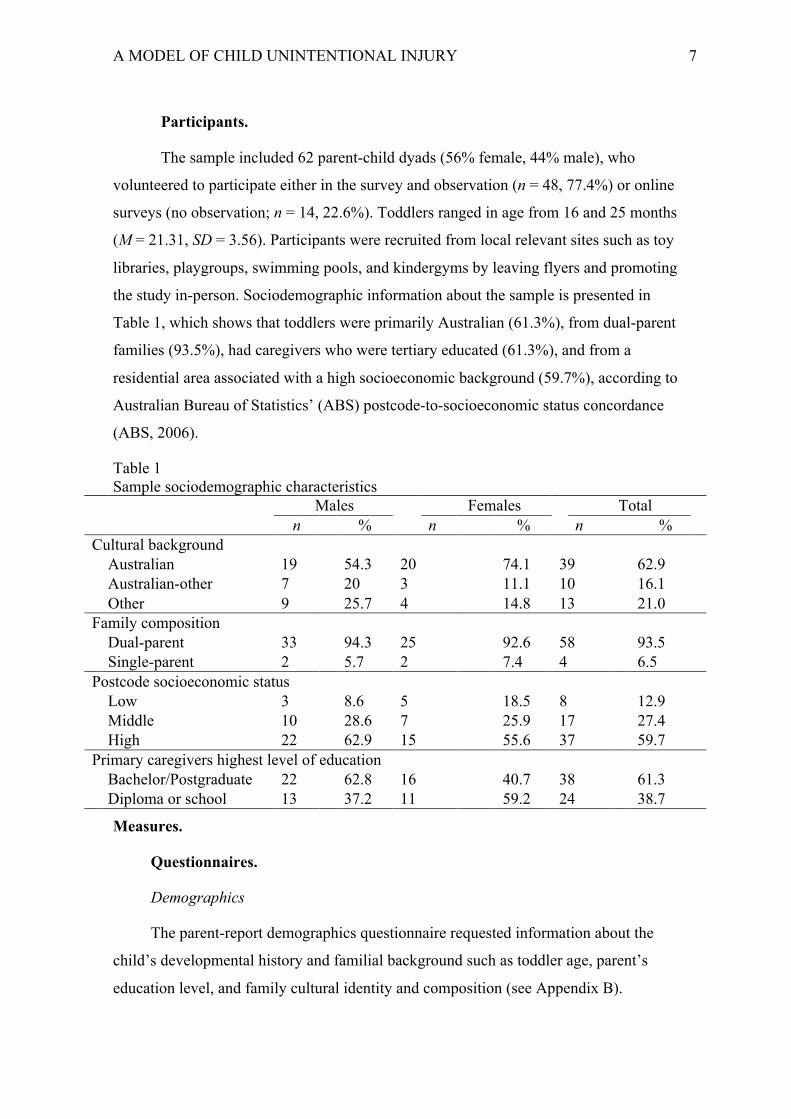
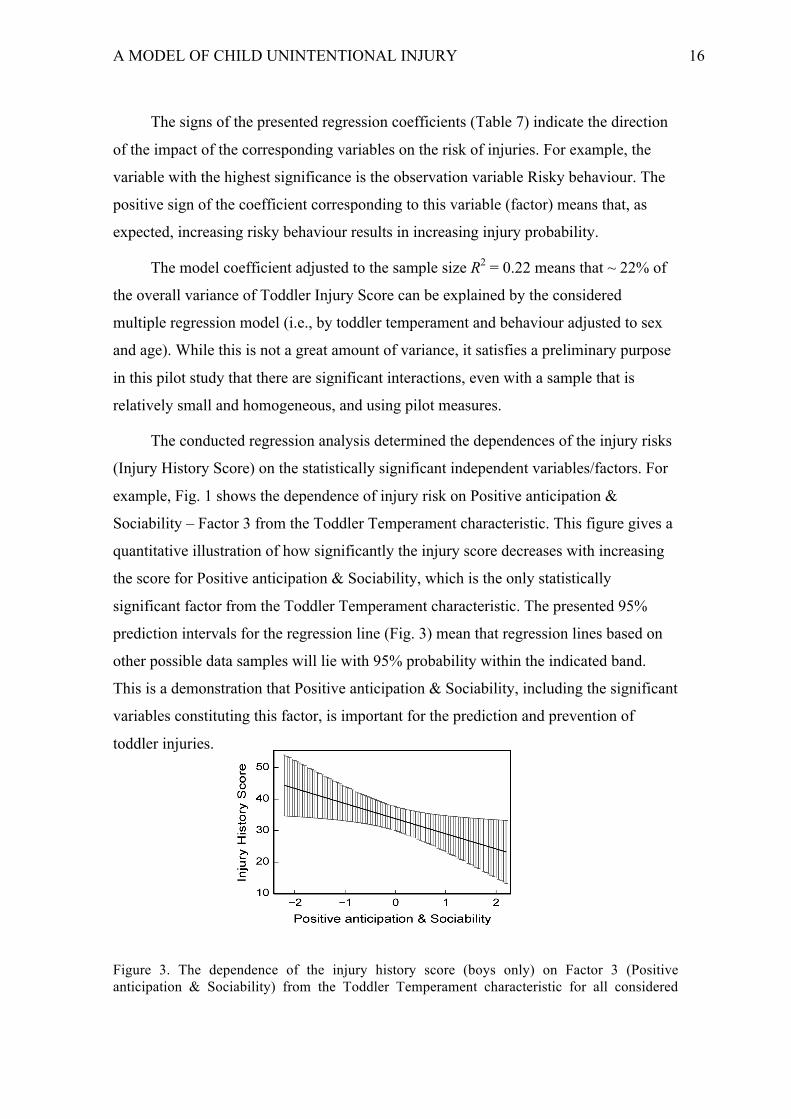
The conducted regression analysis determined the dependences of the injury risks
(Injury History Score) on the statistically significant independent variables/factors. For
example, Fig. 1 shows the dependence of injury risk on Positive anticipation &
Sociability – Factor 3 from the Toddler Temperament characteristic. This figure gives a
quantitative illustration of how significantly the injury score decreases with increasing
the score for Positive anticipation & Sociability, which is the only statistically
significant factor from the Toddler Temperament characteristic. The presented 95%
prediction intervals for the regression line (Fig. 3) mean that regression lines based on
other possible data samples will lie with 95% probability within the indicated band.
This is a demonstration that Positive anticipation & Sociability, including the significant
variables constituting this factor, is important for the prediction and prevention of
toddler injuries.
Figure 3. The dependence of the injury history score (boys only) on Factor 3 (Positive anticipation & Sociability) from the Toddler Temperament characteristic for all considered

A MODEL OF CHILD UNINTENTIONAL INJURY 17
ages. The error bars show the 95% prediction intervals. For girls, the dependence of the injury score on Positive anticipation & Sociability is not significant – not presented here.

A MODEL OF CHILD UNINTENTIONAL INJURY 18
Discussion
The findings of this exploratory pilot study determined the feasibility of data
collection methods (observed Risky Behaviour) and measures (Injury History Rating
Scale; Early Childhood Behaviour Questionnaire), and assessed their psychometric
properties. The 18 toddler temperament dimensions were reduced to five factors that
explain almost 70% of the variance, and all other than impulsivity had sound
coefficients over .55. Similarly, the five behavioural observation variables, or Risky
Behaviours, all reduced onto the same factor, allowing analysis to include a single
measure of toddler behaviour. Finally, the Injury History Rating Scale, which produces
four subscale scores (cause, type, body, and treatment) and a total Injury Score, was
developed as a post data collection tool for quantifying qualitatively reported injury
histories. The overall score had excellent validity with another measure of past injuries
(IBC injuries subscale). Moreover, to support the scale’s psychometric robustness in
this sample, patterns such as most common causes in the 1 to 4 years age group were
congruent (i.e., falls most common; location is often home).
The primary analyses strongly underscore the importance of multivariate
investigations. For example, toddler sex was not statistically significant as a separate
variable in multiple regression, however, it appeared as a significant moderating
variable affecting the risk of injuries through its interaction with Factor 3: Positive
anticipation & Sociability (Table 7). Thus, has two different channels of impact on the
injury score – the direct impact with the negative regression coefficient – 4.80, and the
impact through the interaction term with the regression coefficient + 8.31 (Table 7). As
a result, risk of injury for boys is significantly reduced with increasing the Positive
anticipation & Sociability factor, because the interaction term with the positive
regression coefficient is cancelled by the value boys = 0 for the categorical variable
toddler sex. The findings are very different for girls, corresponding to the value girls ≡ 1
for the sex categorical variable. In this case, the contribution of the interaction term with
the positive regression coefficient is not cancelled, and the impact of Positive
anticipation & Sociability on the risk of injury in girls is significantly reduced. In turn,
the overall impact of the Positive anticipation & Sociability Sex factor on risk of
injuries in girls is not statistically significant (with p = 0.35 > 0.05). These contradictory
outcomes for the Positive anticipation & Sociability factor and its impact on the risk of

A MODEL OF CHILD UNINTENTIONAL INJURY 19
injuries in boys and girls are important preliminary findings for this study. Nonetheless,
they are disparate to the large body of research suggesting that the most important ‘risk
traits’ are those like activity level and impulsivity (Prinzie et al., 2012; Van Aken,
Junger, Verhoeven, Van Aken, & Deković, 2007; Williams et al., 2009).
Further contradiction to the wealth of research on Activity level as a risk factor for
injury (e.g., Schwebel & Barton, 2006a; Schwebel & Gaines, 2007), toddler boys in this
study with enhanced Activity level and High-intensity pleasure are actually at a lesser
risk of sustaining unintentional injuries (p = 0.042). Although higher levels of activity
and high-intensity pleasure theoretically should increase the risk of injuries, these traits
might also be associated with better developed social skills or better control over
inappropriate responses and behaviour. One explanation is that elevated activity levels
cause a child to experience more environments, and thus develop advanced cognitive
and physical skills that allow them to better manipulate the environment than those
without experience (Plumert, 1995; Plumert and Schwebel, 1997). Therefore, despite
the expectation of higher injury risks with increasing level of activity, the opposite co-
existing tendency towards improved control and satisfaction (positive anticipation)
appears to dominate the increased exposure to potential risks and cause the overall
reduction of injury probability. No such significant dependence has been derived for
girls (p = 0.27).
A Positive toddler’s attitude to the environment and good social skills are
suggested to be a safeguard against potential injuries even though these traits tend to
increase social contact and activity (and in turn, more opportunities for risk; Schwebel,
2001). It may be hypothesised that such increase of the social skills and contact, as well
as positive anticipation from the environment and surrounding people, cause more
compliance with parents and less risky behaviour, for example, due to and thus lesser
incentives towards breaking the existing boundaries and safety limitations. This relates
to evidence of children with externalising behavioural problems or disorders, such as to
non-compliance, poor social skills, or negative emotionality towards their environments
(conversely to these proposed protective traits), for example children with ADHD or
conduct disorder are reported to have experienced more injuries than their unaffected
siblings Shilon, Pollak, Aran, Shaked, & Gross-Tsur, 2011)

A MODEL OF CHILD UNINTENTIONAL INJURY 20
Recommendations for follow up study
‘Time constraints’ was the most commonplace reason given by parents of young
children for not participating in the behavioural observation. An online version of the
questionnaires was created in an attempt to counteract this, however, for such reasons as
anonymity (no accountability), and abandonment, participation rates were very low (14
out of >400 parents saw the online advertisement). It is therefore suggested for that
interested participants register and receive a single-user login that allows their survey to
be left and returned to. Registration could also allow for email reminders to be sent. In
addition, a proposed new version of the injury history scale is included in Appendix C,
and is based on the data collected in this pilot.
Conclusion
This pilot study used both observational and survey data, online and face-to-face
participants, and both novel and well-established measures and methods, and rigorously
analysed each to ensure that the follow up studies are both methodologically and
conceptually sound. As such, the aims of the study pertaining to preliminary analyses
was addressed. The overarching model furthermore was developed in response to a gap
in both literature and thus knowledge concerning the aetiological pathways
underpinning paediatric injury. In such an important line of developmental research, it
is crucial to undertake such pilot studies as this one so as to ensure findings and
conclusions are not accepted or rejected erroneously.
A MODEL OF CHILD UNINTENTIONAL INJURY 21
References . Practice guide: The assessment of harm and risk of harm. (2013). Queensland, Australia:
Retrieved from http://www.communities.qld.gov.au/resources/childsafety/practice-manual/pg-assess-risk-of-harm.pdf.
Wells, M., Morrongiello, B. A., & Kane, A. (2012). Unintentional injury risk in school-age
children: Examining interrelations between parent and child factors. Journal of Applied Developmental Psychology, 33 189–196.
Shilon, Y., Pollak, Y., Aran, A., Shaked, S., & Gross‐Tsur, V. (2012). Accidental injuries are more common in children with attention deficit hyperactivity disorder compared with their non‐affected siblings. Child: Care, Health and Development, 38(3), 366-370.
Prinzie, P., Deković, M., van den Akker, A. L., de Haan, A. D., Stoltz, S. E., & Jolijn Hendriks, A. (2012). Fathers’ personality and its interaction with children’s personality as predictors of perceived parenting behavior six years later. Personality and Individual Differences, 52(2), 183-189.
Karazsia, B. T., Guilfoyle, S. M., & Wildman, B. G. (2012). The mediating role of hyperactivity and inattention on sex differences in paediatric injury risk. Child Care Health Development, 38(3), 358-365. doi: 10.1111/j.1365-2214.2011.01243.x
Sorenson, S. B. (2011). Gender disparities in injury mortality: consistent, persistent, and larger
than you'd think. Am J Public Health, 101 Suppl 1, S353-358. doi: 10.2105/AJPH.2010.300029
Williams, L. R., Degnan, K. A., Perez-Edgar, K. E., Henderson, H. A., Rubin, K. H., Pine, D.
S., . . . Fox, N. A. (2009). Impact of behavioral inhibition and parenting style on internalizing and externalizing problems from early childhood through adolescence. Journal of abnormal child psychology, 37(8), 1063-1075.
Simpson, J. C., Turnbull, B. L., Ardagh, M., & Richardson, S. (2009). Child home injury prevention: understanding the context of unintentional injuries to preschool children. International Journal of Injury Control and Safety Promotion, 16(3), 159-167.
Field, A. (2009). Discover statistics using SPSS: SAGE Publications Ltd, London, UK. Cole, R., Koulouglioti, C., Kitzman, H., Sidora-Arcoleo, K., & Anson, E. (2009). Maternal
rules, compliance, and injuries to preschool children. Family & Community Health, 32(2), 136.
Van Aken, C., Junger, M., Verhoeven, M., Van Aken, M., & Deković, M. (2007). Externalizing behaviors and minor unintentional injuries in toddlers: common risk factors? Journal of pediatric psychology, 32(2), 230-244.
Schwebel, D. C., & Gaines, J. (2007). Pediatric unintentional injury: behavioral risk factors and implications for prevention. Journal of Developmental & Behavioral Pediatrics, 28(3), 245-254.
Cassell, E., & Clapperto, A. (2007). Preventing unintentional injury in Victorian children aged 0-14 years: a call to action. Melbourne, VIC.: Monash University Accident Research Centre Retrieved from www.monash.edu.au/muarc/visu.
Schwebel, D. C., Hodgens, J. B., & Sterling, S. (2006). How mothers parent their children with
behavior disorders: Implications for unintentional injury risk. Journal of safety
A MODEL OF CHILD UNINTENTIONAL INJURY 22
research, 37(2), 167-173. Schwebel, D. C., & Barton, B. K. (2006). Temperament and children’s unintentional injuries.
Handbook of personality and health, 51-71. Putnam, S. P., Gartstein, M. A., & Rothbart, M. K. (2006). Measurement of fine-grained
aspects of toddler temperament: The Early Childhood Behavior Questionnaire. Infant Behavior and Development, 29(3), 386-401.
Munro, S. A., Van Niekerk, A., & Seedat, M. (2006). Childhood unintentional injuries: the perceived impact of the environment, lack of supervision and child characteristics. Child: care, health and development, 32(3), 269-279.
Schwebel, D. C., & Barton, B. K. (2005). Contributions of multiple risk factors to child injury. Journal of pediatric psychology, 30(7), 553-561.
Morrongiello, B. A. (2005). Caregiver supervision and child-injury risk: I. Issues in defining and measuring supervision; II. Findings and directions for future research. Journal of Pediatric Psychology, 30(7), 536-552.
Schwebel, D. C., Brezausek, C. M., Ramey, S. L., & Ramey, C. T. (2004). Interactions between child behavior patterns and parenting: Implications for children's unintentional injury risk. Journal of Pediatric Psychology, 29(2), 93-104.
Schwebel, D. C. (2004). Interactions Between Child Behavior Patterns and Parenting: Implications for Children's Unintentional Injury Risk. Journal of Pediatric Psychology, 29(2), 93-104. doi: 10.1093/jpepsy/jsh013
Morrongiello, B. A., Ondejko, L., & Littlejohn, A. (2004). Understanding toddlers’ in-home
injuries: II. Examining parental strategies, and their efficacy, for managing child injury risk. Journal of pediatric psychology, 29(6), 433-446.
Morrongiello, B. A., Ondejko, M. A., & Littlejohn, A. . (2004). Understanding Toddlers' In-Home Injuries: 1. Context, Correlates, and Determinants. Journal of Pediatric Psychology, 29(6), 16. doi: 10.1093
Ramsay, L., Moreton, G., Gorman, D., Blake, E., Goh, D., Elton, R., & Beattie, T. (2003).
Unintentional home injury in preschool-aged children: looking for the key—an exploration of the inter-relationship and relative importance of potential risk factors. Public health, 117(6), 404-411.
Bijttebier, P., Vertommen, H., & Florentie, K. (2003). Risk-taking behavior as a mediator of the relationship between children's temperament and injury liability. Psychology and Health, 18(5), 645-653.
Schwebel, D. C. (2001). Relations between children's temperament, ability estimation, and unintentional injuries. ProQuest Information & Learning.
Putnam, S. P., Ellis, L. K., & Rothbart, M. K. (2001). The structure of temperament from infancy through adolescence. Advances in research on temperament, 165-182.
Morrongiello, B. A., Midgett, C., & Shields, R. (2001). Don't run with scissors: young children's knowledge of home safety rules. Journal of Pediatric Psychology, 26(2), 105-115.
Schwebel, D. C., & Plumert, J. M. (1999). Longitudinal and concurrent relations among temperament, ability estimation, and injury proneness. Child development, 70(3), 700-712.
Plumert, J. M., & Schwebel, D. C. (1997). Social and temperamental influences on children's overestimation of their physical abilities: Links to accidental injuries. Journal of Experimental Child Psychology, 67(3), 317-337.

A MODEL OF CHILD UNINTENTIONAL INJURY 23
Plumert, J. M. (1995). Relations between children's overestimation of their physical abilities and accident proneness. Developmental Psychology, 31(5), 866.
Speltz, M. L., Gonzales, N., Sulzbacher, S., & Quan, L. (1990). Assessment of injury risk in young children: A preliminary study of the Injury Behavior Checklist. Journal of Pediatric Psychology, 15(3), 373-383.
Plain&Language&Statement&&&Consent&Form&to&Parents&of&toddlers& &2013-031: Individual difference in toddlers' water-play behaviour:&version&1:&14th&March,&2013& & Page&1&of&5 &
!!PLAIN!LANGUAGE!STATEMENT!AND!CONSENT!FORM!!TO:!!Parents of toddlers aged 16-25 months! !&&
Plain!Language!Statement!!
Date:!16th!April,!2013!
Full!Project!Title:!Individual!differences!in!toddlers’!waterNplay!behaviour!
Principal!Researcher:!Dr.!Merrilyn!Hooley!Student!Researchers:!Ashleigh!Barber,!Manuela!Barichello,!Mei!Kee!Chun,!Krystal!!Kelley,!Karen!Lim,!Cassandra!Whelan!&
&
1. Your Consent
You are invited to take part in this research project.
This Plain Language Statement contains detailed information about the research project. Its purpose is to explain to you as openly and clearly as possible all the procedures involved in this project so that you can make a fully informed decision whether you are going to participate.
Please read this Plain Language Statement carefully. Feel free to ask questions about any information in the document. You may also wish to discuss the project with a relative or friend or your local health worker. Feel free to do this.
Once you understand what the project is about and if you agree to take part in it, you will be asked to complete the linked Survey. By completing and submitting the survey you indicate that you understand the information provided and that you give your consent to participate in the research project.
You are welcome to print a copy of the Plain Language Statement for your records.
2. Purpose and Background
The purpose of this project is to identify factors (such as parent personality/parenting style, and toddlers’ temperament) that are associated with toddlers’ risk of accidental injury. A number of student researchers are involved in this project; they are all post-graduate students in the School of Psychology, working towards a Graduate Diploma in Psychology.
A total of approximately 300 parents will participate in this project.
Plain&Language&Statement&&&Consent&Form&to&Parents&of&toddlers& &2013-031: Individual difference in toddlers' water-play behaviour:&version&1:&14th&March,&2013& & Page&2&of&5 &
Previous experience has shown that accidental injury is the leading cause of death for children aged 0-4 years with male children suffering higher rates of injury than female children. Our research is designed to help identify some characteristics of the environment and of toddlers, and explore how these factors interact to influence toddlers’ injury history. Some aspects of our research involve observing toddlers aged 16-25 months exploring in a play area at Deakin University; if you would like to be involved in these experiments please contact the researchers. Other aspects of our research involve surveying a large number of parents of toddlers to see how parent/child interactions might be associated with risk. You are invited to participate in the online survey.
3. Methods and Participant demands
The online survey can be accessed by clicking on the link below. Completing, and submitting the survey will be taken as consent to participate. Participation in the survey should take approximately 20 minutes. In completing the survey you will be asked to provide some background information about your child and provide information about you and your child’s personalities and your child’s recent injury history. The survey information we are collecting will provide us with background information about your child that might help us to understand individual differences in the ways different children explore the environment, and the types and rates of injuries that these different children suffer. Examples of questions you will be asked about your child are:
“How quickly does your child adapt to new surroundings?”
“How often does your child suffer accidental injuries that require some attention?”
“Has your child ever had an accident that required a visit to a hospital? If so, describe the accident, or accidents, if more than one?”
We will also ask you some questions about yourself. This is because we are studying the relationship between the approach that parents use in the way they raise children, and the way that children behave in the Perception and Action Laboratory. Examples of questions that you will be asked are:
“How quickly do you adapt to new surroundings?”
How strongly do you agree with the following statement: “As a parent, I consistently give my children direction and guidance in rational and objective ways”
How strongly do you agree with the following statement: “It is easy for me to understand what my child wants or needs”
4. Possible Benefits and risks to participants
There are no direct benefits to you for participating in this research however your contribution will help us to better understand the factors that contribute to child injury and inform targeted interventions.
5. Possible Risks and risks to the wider community
Possible benefits of this research include improvements to evidence-based injury interventions and educational programs which may help to reduce the rate of injuries in toddlers within the general community.
6. Privacy, Confidentiality and Disclosure of Information
No identifying information will be collected as part of the survey so you will not be able to be identified. The overall results of the research will be made public at conferences and by publication in journals.
7. Results of Project
The results of the project will be disseminated via articles in peer-review journals and conferences. A website will be set up which will summarise the results of the first phase of the research at the
Plain&Language&Statement&&&Consent&Form&to&Parents&of&toddlers& &2013-031: Individual difference in toddlers' water-play behaviour:&version&1:&14th&March,&2013& & Page&3&of&5 &
completion of the project for participants. You will be provided a URL when you submit the survey. A summary of results should be available after November.
8. Participation is Voluntary
9. Ethical Guidelines
This project will be carried out according to the National Statement on Ethical Conduct in Human Research (2007) produced by the National Health and Medical Research Council of Australia. This statement has been developed to protect the interests of people who agree to participate in human research studies.
The ethics aspects of this research project have been approved by the Human Research Ethics Committee of Deakin University.
10. Complaints
If you have any complaints about any aspect of the project, the way it is being conducted or any questions about your rights as a research participant, then you may contact:
The Manager, Research Integrity, Deakin University, 221 Burwood Highway, Burwood Victoria 3125, Telephone: 9251 7129, [email protected]
Please quote project number 2013-031.
11. Further Information, Queries or Any Problems
If you require further information, wish to withdraw your participation or if you have any problems concerning this project, you can contact the principal researcher.
The researcher responsible for this project is:
Dr. Merrilyn Hooley PhD
School of Psychology,
Deakin University
221 Burwood Highway,
Burwood, 3125
Ph: B/H 92446499
Email: [email protected]
Plain&Language&Statement&&&Consent&Form&to&Parents&of&toddlers& &2013-031: Individual difference in toddlers' water-play behaviour:&version&1:&14th&March,&2013& & Page&4&of&5 &
!!PLAIN!LANGUAGE!STATEMENT!AND!CONSENT!FORM!!TO:!!Parents of toddlers aged 16-25 months!&
Third!Party!Consent!Form!
(To!be!used!by!parents/guardians!of!minor!children,!or!carers/guardians!consenting!on!behalf!of!adult!participants!who!do!not!have!the!capacity!to!give!informed!consent)!
!
Date:!
Full!Project!Title:!Individual!differences!in!toddlers’!waterNplay!behaviour!
Principal!Researcher:!Dr.!Merrilyn!Hooley!Student!Researchers:!Ashleigh!Barber,!Manuela!Barichello,!Mei!Kee!Chun,!Krystal!!Kelley,!Karen!Lim,!Cassandra!Whelan!&
&I&have&read&and&I&understand&the&attached&Plain&Language&Statement.!
I&give&my&permission&for&……………………………………………………(name&of&participant)&to&participate&in&this&project&according&to&the&conditions&in&the&Plain&Language&Statement.&&&I&have&been&given&a©&of&Plain&Language&Statement&and&Consent&Form&to&keep.&
The&researcher&has&agreed¬&to&reveal&my&identity&and&personal&details,&including&where&information&about&this&project&is&published,&or&presented&in&any&public&form.&&&
&&!&&Participant’s&Name&(printed)&……………………………………………………&
Name&of&Person&giving&Consent&(printed)&……………………………………………………&&&
Relationship&to&Participant:&………………………………………………………&&
Signature&………………………………………………………& Date&&…………………………&
& &
Plain&Language&Statement&&&Consent&Form&to&Parents&of&toddlers& &2013-031: Individual difference in toddlers' water-play behaviour:&version&1:&14th&March,&2013& & Page&5&of&5 &
!!PLAIN!LANGUAGE!STATEMENT!AND!CONSENT!FORM!!TO:! Parents of toddlers!!
Release!Consent!Form!
(To!be!used!by!parents/guardians!of!minor!children,!or!carers/guardians!consenting!on!behalf!of!adult!participants!who!do!not!have!the!capacity!to!give!informed!consent)!
Date:!
Full!Project!Title:!Individual!differences!in!toddlers’!waterNplay!behaviour!
Principal!Researcher:!Dr.!Merrilyn!Hooley!Student!Researcher:! Ashleigh!Barber,!Manuela!Barichello,!Mei!Kee!Chun,!Krystal!!Kelley,!Karen!Lim,!Cassandra!Whelan!
I have read and I understand the attached Plain Language Statement and understand that my child will be videotaped while they explore and play in two novel environments. I also understand that I will also appear in some of this video when I am in proximity to my child.
I give my permission for the image of my child to be used during the presentation of the results of this research FOR EDUCATIONAL PURPOSES ONLY (e.g. in research conference presentation). I understand that my image may also appear in the background of my child’s image. I understand that my child’s (and in cases my) images will ONLY be used in restricted environments, and will remain under the control of the Principal Investigator who will NOT release the images for use by other individuals. I give my consent to the restricted use of my child’s …………………………………………………… (name of participant) and my images for use for educational purposes. The researcher has agreed not to reveal my identity and personal details.
Participant’s Name (printed) ……………………………………………………
Name of Person giving Consent (printed) ……………………………………………………
Relationship to Participant: ………………………………………………………
Signature ……………………………………………………… Date …………………………
Memorandum
To:
From:
Date:
Subject: 2013-031
Individual difference in toddlers' water-play behaviour
Dr Merrilyn Hooley
School of Psychology
B
Deakin University Human Research Ethics Committee (DUHREC)
13 May, 2013
Please quote this project number in all future communications
The modification to this project, submitted on 1/05/2013 has been approved by the committee executive on13/05/2013.
cc:
Human Research Ethics
Deakin Research Integrity 70 Elgar Road Burwood Victoria Postal: 221 Burwood Highway Burwood Victoria 3125 Australia Telephone 03 9251 7123 Facsimile 03 9244 6581 [email protected]
Approval has been given for Dr Merrilyn Hooley, School of Psychology, to continue this project as modified to14/03/2017.
In addition you will be required to report on the progress of your project at least once every year and at theconclusion of the project. Failure to report as required will result in suspension of your approval to proceed withthe project.
DUHREC may need to audit this project as part of the requirements for monitoring set out in the NationalStatement on Ethical Conduct in Human Research (2007).
• Serious or unexpected adverse effects on the participants• Any proposed changes in the protocol, including extensions of time.• Any events which might affect the continuing ethical acceptability of the project.• The project is discontinued before the expected date of completion.• Modifications are requested by other HRECs.
The approval given by the Deakin University Human Research Ethics Committee is given only for the project andfor the period as stated in the approval. It is your responsibility to contact the Human Research Ethics Unitimmediately should any of the following occur:
Human Research Ethics [email protected]: 03 9251 7123
1
Some information about your child Would you please provide some background information about your child and your household. The purpose of this information is to allow us to describe our sample, as well as identify aspects of your child’s stage of development. 1. Please circle your child’s gender? Male / Female 2. What is your child date of birth? ______/________/______ 3. Please indicate you child’s height ___________________ (cm) 4. Please indicate you child’s weight ____________________(kg) 5. How long has your child been crawling? _______________ Months 6. How long has your child been standing? ________________ Months 7. How long has your child been walking using supports? ______________ Months 8. How long has your child been walking without supports? ____________ Months 9. Does your child, or has your child ever participated in any of the following structured activities? If yes, please note for how long they have been involved and how often participation occurs. Leave blank if No. Activity Yes Duration (months) Daily / Weekly / Fortnightly / Monthly Swimming Lessons Kiddy gym Play group Music Other 10. Does your child attend child care or have regular formal or informal care? Carer Yes Daily/ Weekly / Fortnightly/ Monthly Child Care Nanny Family Friends / Neighbours 11. Does your child have a disability or special needs? Yes / No Please describe ___________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
2
Household information 12. What is your cultural identity? ________________________________________ 13. What is your postcode? _____________________________ 14. Do you own a swimming pool or spa? Yes / No 15. If yes, is the water site fenced to Australian standards? Yes / No 16. Please indicate the primary carer for your child. Primary Caregiver Tick Myself My Partner Myself and My partner Other Family member Friend / Neighbour Nanny / Professional Other (please note) 17. Does your child have any siblings? If yes, please circle their gender and note their year of birth Sibling Gender Year of birth 1 Male / Female 2 Male / Female 3 Male / Female 4 Male / Female 18. Are you a single parent family? No / Yes Female / Yes Male 19. What is your highest level of education? Please include your partner if applicable. Level of Education You Your Partner Primary / secondary school Diploma Degree Post-graduate 20. What is your labour force status? Please include your partner if applicable. Labour force status You Your Partner ‘Stay-at-home’ carer Unemployed Employed Casual Employed Part time Employed Full time Thank you
Early Childhood behaviour QuestionnaireChild’s name: ______________________ Child’s birthdate: Mo:____ Day:____ Yr:____
Today’s date: Month:____ Day:____ Year:____ Child’s Age: ______ Years, ______Months
Relation to child: ______________________ Sex of child (circle one): Male Female
INSTRUCTIONS: Please read carefully before starting.
As you read each description of the child’s behaviour below, please indicate how often the child did this during the last two weeks by circling one of the numbers in the right column. These numbers indicate how often you observed the behaviour described during the last two weeks.
less about morevery than half half than half almost does not
never rarely the time the time the time always always apply1 2 3 4 5 6 7 NA
The “Does Not Apply” column (NA) is used when you did not see the child in the situation described during the last two weeks. For example, if the situation mentions the child going to the doctor and there was no time during the last two weeks when the child went to the doctor, circle the (NA) column. “Does Not Apply” (NA) is different from “NEVER” (1). “Never” is used when you saw the child in the situation but the child never engaged in the behaviour mentioned in the last two weeks. Please be sure to circle a number or NA for every item.
When told that it was time for bed or a nap, how often did your child react with anger? 1 2 3 4 5 6 7 NAget irritable? 1 2 3 4 5 6 7 NA
When approached by an unfamiliar person in a public place (for example, the grocery store), how often did your child remain calm? 1 2 3 4 5 6 7 NApull back and avoid the person? 1 2 3 4 5 6 7 NAcling to a parent? 1 2 3 4 5 6 7 NA
During everyday activities, how often did your childstartle at loud noises (such as a fire engine siren)? 1 2 3 4 5 6 7 NAtap or drum with fingers on tables or other objects? 1 2 3 4 5 6 7 NAget irritated by scratchy sounds? 1 2 3 4 5 6 7 NAbecome uncomfortable when his/her socks were not
aligned properly on his/her feet? 1 2 3 4 5 6 7 NA
After getting a bump or scrape, how often did your child forget about it in a few minutes? 1 2 3 4 5 6 7 NA
While playing outdoors, how often did your childlike making lots of noise? 1 2 3 4 5 6 7 NAenjoy sitting quietly in the sunshine? 1 2 3 4 5 6 7 NAwant to climb to high places (for example, up a tree
or on the jungle gym)? 1 2 3 4 5 6 7 NA
When s/he was carried, how often did your childlike to be held? 1 2 3 4 5 6 7 NApush against you until put down? 1 2 3 4 5 6 7 NAsquirm? 1 2 3 4 5 6 7 NAstruggle to get away? 1 2 3 4 5 6 7 NAsnuggle up next to you? 1 2 3 4 5 6 7 NA
While having trouble completing a task (e.g., building, drawing, dressing), how often did your childget easily irritated? 1 2 3 4 5 6 7 NAbecome sad? 1 2 3 4 5 6 7 NA
When a familiar child came to your home, how often did your childengage in an activity with the child? 1 2 3 4 5 6 7 NAseek out the company of the child? 1 2 3 4 5 6 7 NA
When offered a choice of activities, how often did your childstop and think before deciding? 1 2 3 4 5 6 7 NAdecide what to do very quickly and go after it? 1 2 3 4 5 6 7 NAseem slow and unhurried about what to do next? 1 2 3 4 5 6 7 NA
When asked NOT to, how often did your childrun around your house or apartment anyway? 1 2 3 4 5 6 7 NA
touch an attractive item (such as an ornament) anyway? 1 2 3 4 5 6 7 NAplay with something anyway? 1 2 3 4 5 6 7 NA
During daily or evening quiet time with you and your child, how often did your childenjoy just being quietly sung to? 1 2 3 4 5 6 7 NAsmile at the sound of words, as in nursery rhymes? 1 2 3 4 5 6 7 NAenjoy just being talked to? 1 2 3 4 5 6 7 NAenjoy rhythmic activities, such as rocking or swaying? 1 2 3 4 5 6 7 NA
During everyday activities, how often did your childbecome distressed when his/her hands were dirty and/or sticky? 1 2 3 4 5 6 7 NAnotice that material was very soft (cotton) or rough (wool)? 1 2 3 4 5 6 7 NAnotice low-pitched noises such as the air-conditioner, heater,
or refrigerator running or starting up? 1 2 3 4 5 6 7 NAblink a lot? 1 2 3 4 5 6 7 NAget very enthusiastic about the things s/he was going to do? 1 2 3 4 5 6 7 NA
While at home, how often did your childshow fear at a loud sound (blender, vacuum cleaner, etc.)? 1 2 3 4 5 6 7 NAseem afraid of the dark? 1 2 3 4 5 6 7 NA
When visiting the home of a familiar adult, such as a relative or friend, how often did your childwant to interact with the adult? 1 2 3 4 5 6 7 NA
While bathing, how often did your childsit quietly? 1 2 3 4 5 6 7 NAsplash, kick, or try to jump? 1 2 3 4 5 6 7 NA
While playing outdoors, how often did your childlook immediately when you pointed at something? 1 2 3 4 5 6 7 NAchoose to take chances for the fun and excitement of it? 1 2 3 4 5 6 7 NAnot like going down high slides at the amusement park
or playground? 1 2 3 4 5 6 7 NA
When s/he was upset, how often did your childchange to feeling better within a few minutes? 1 2 3 4 5 6 7 NAsoothe only with difficulty? 1 2 3 4 5 6 7 NAstay upset for 10 minutes or longer? 1 2 3 4 5 6 7 NA
When engaged in play with his/her favourite toy, how often did your childplay for 5 minutes or less? 1 2 3 4 5 6 7 NAplay for more than 10 minutes? 1 2 3 4 5 6 7 NAcontinue to play while at the same time responding
to your remarks or questions? 1 2 3 4 5 6 7 NA
When approaching unfamiliar children playing, how often did your childwatch rather than join? 1 2 3 4 5 6 7 NAapproach slowly? 1 2 3 4 5 6 7 NAseem uncomfortable? 1 2 3 4 5 6 7 NA
During everyday activities, how often did your childcomplain about odors on others, such as perfume? 1 2 3 4 5 6 7 NAseem to be bothered by bright light? 1 2 3 4 5 6 7 NA move quickly from one place to another? 1 2 3 4 5 6 7 NA notice the smoothness or roughness of objects s/he touched? 1 2 3 4 5 6 7 NA become sad or blue for no apparent reason? 1 2 3 4 5 6 7 NA
After having been interrupted, how often did your childreturn to a previous activity? 1 2 3 4 5 6 7 NA have difficulty returning to the previous activity? 1 2 3 4 5 6 7 NA
While watching TV or hearing a story, how often did your childseem frightened by ‘monster’ characters? 1 2 3 4 5 6 7 NA
When you suggested an outdoor activity that s/he really likes, how often did your childrespond immediately? 1 2 3 4 5 6 7 NA run to the door before getting ready? 1 2 3 4 5 6 7 NA
When told that loved adults would visit, how often did your childget very excited? 1 2 3 4 5 6 7 NA become very happy? 1 2 3 4 5 6 7 NA
When taking a quiet, warm bath, how often did your childseem to relax and enjoy him/herself? 1 2 3 4 5 6 7 NA
When s/he couldn’t find something to play with, how often did your childget angry? 1 2 3 4 5 6 7 NA During sleep, how often did your childtoss about in the bed? 1 2 3 4 5 6 7 NA sleep in one position only? 1 2 3 4 5 6 7 NA
During quiet activities, such as reading a story, how often did your childswing or tap his/her foot? 1 2 3 4 5 6 7 NAfiddle with his/her hair, clothing, etc.? 1 2 3 4 5 6 7 NA show repeated movements like squinting, hunching up
the shoulders, or twitching the facial muscles? 1 2 3 4 5 6 7 NA
While playing indoors, how often did your childlike rough and rowdy games? 1 2 3 4 5 6 7 NAenjoy playing boisterous games like ‘chase’? 1 2 3 4 5 6 7 NA enjoy vigorously jumping on the couch or bed? 1 2 3 4 5 6 7 NA
In situations where s/he is meeting new people, how often did your childturn away? 1 2 3 4 5 6 7 NA become quiet? 1 2 3 4 5 6 7 NA seem comfortable? 1 2 3 4 5 6 7 NA
When being gently rocked or hugged, how often did your childseem eager to get away? 1 2 3 4 5 6 7 NAmake protesting noises? 1 2 3 4 5 6 7 NA
When encountering a new activity, how often did your childsit on the sidelines and observe before joining in? 1 2 3 4 5 6 7 NAget involved immediately? 1 2 3 4 5 6 7 NA
When visiting the home of a familiar child, how often did your childengage in an activity with the child? 1 2 3 4 5 6 7 NA seek out the company of the child? 1 2 3 4 5 6 7 NA
When another child took away his/her favorite toy, how often did your childscream with anger? 1 2 3 4 5 6 7 NA not become angry? 1 2 3 4 5 6 7 NA sadly cry? 1 2 3 4 5 6 7 NA not react with sadness? 1 2 3 4 5 6 7 NA
When engaged in an activity requiring attention, such as building with blocks, how often did your childmove quickly to another activity? 1 2 3 4 5 6 7 NA stay involved for 10 minutes or more? 1 2 3 4 5 6 7 NA tire of the activity relatively quickly? 1 2 3 4 5 6 7 NA
During everyday activities, how often did your childpay attention to you right away when you called
to him/her? 1 2 3 4 5 6 7 NAseem to be disturbed by loud sounds? 1 2 3 4 5 6 7 NAstop going after a forbidden object (such as a VCR)
when you used a toy to distract her/him? 1 2 3 4 5 6 7 NAnotice small things, such as dirt or a stain, on
his/her clothes? 1 2 3 4 5 6 7 NA
While in a public place, how often did your childseem uneasy about approaching an elevator or escalator? 1 2 3 4 5 6 7 NA cry or show distress when approached by an unfamiliar animal? 1 2 3 4 5 6 7 NA seem afraid of large, noisy vehicles? 1 2 3 4 5 6 7 NA show fear when the caregiver stepped out of sight? 1 2 3 4 5 6 7 NA
When playing outdoors with other children, how often did your child seem to be one of the most active children? 1 2 3 4 5 6 7 NA sit quietly and watch? 1 2 3 4 5 6 7 NA
During daily or evening quiet time with you and your child, how often did your child want to be cuddled? 1 2 3 4 5 6 7 NA
During everyday activities, how often did your child seem frightened for no apparent reason? 1 2 3 4 5 6 7 NA seem to be irritated by tags in his/her clothes? 1 2 3 4 5 6 7 NA notice when you were wearing new clothing? 1 2 3 4 5 6 7 NA react to beeping sounds (such as when the microwave
or oven is done cooking)? 1 2 3 4 5 6 7 NA show repeated movements like squinting, hunching up
the shoulders, or twitching the facial muscles? 1 2 3 4 5 6 7 NA
When being dressed or undressed, how often did your child squirm and try to get away? 1 2 3 4 5 6 7 NA stay still? 1 2 3 4 5 6 7 NA
When told “no”, how often did your child stop an activity quickly? 1 2 3 4 5 6 7 NA stop the forbidden activity? 1 2 3 4 5 6 7 NA ignore your warning? 1 2 3 4 5 6 7 NA become sadly tearful? 1 2 3 4 5 6 7 NA
Following an exciting activity or event, how often did your child calm down quickly? 1 2 3 4 5 6 7 NA have a hard time settling down? 1 2 3 4 5 6 7 NA seem to feel down or blue? 1 2 3 4 5 6 7 NA become sadly tearful? 1 2 3 4 5 6 7 NA
When given something to eat that s/he didn’t like, how often did your child become angry? 1 2 3 4 5 6 7 NA
During everyday activities, how often did your child seem able to easily shift attention from one activity to another? 1 2 3 4 5 6 7 NA do more than one thing at a time (such as playing with
a toy while watching TV)? 1 2 3 4 5 6 7 NA
While playing indoors, how often did your child run through the house? 1 2 3 4 5 6 7 NA climb over furniture? 1 2 3 4 5 6 7 NA not care for rough and rowdy games? 1 2 3 4 5 6 7 NA enjoy activities such as being spun, etc.? 1 2 3 4 5 6 7 NA
When playing alone, how often did your child become easily distracted? 1 2 3 4 5 6 7 NA play with a set of objects for 5 minutes or longer at
a time? 1 2 3 4 5 6 7 NA scratch him/herself? 1 2 3 4 5 6 7 NA tear materials close at hand? 1 2 3 4 5 6 7 NA
Before an exciting event (such as receiving a new toy), how often did your child get so worked up that s/he had trouble sitting still? 1 2 3 4 5 6 7 NA get very excited about getting it? 1 2 3 4 5 6 7 NA remain pretty calm? 1 2 3 4 5 6 7 NA seem eager to have it right away? 1 2 3 4 5 6 7 NA
When s/he asked for something and you said “no”, how often did your child become frustrated? 1 2 3 4 5 6 7 NA protest with anger? 1 2 3 4 5 6 7 NA have a temper tantrum? 1 2 3 4 5 6 7 NA become sad? 1 2 3 4 5 6 7 NA
While playing or walking outdoors, how often did your child notice sights or sounds (for example, wind chimes
or water sprinklers)? 1 2 3 4 5 6 7 NA notice flying or crawling insects? 1 2 3 4 5 6 7 NA
When you gave your child an attractive toy, how often did your child grab the object as soon as it was set down? 1 2 3 4 5 6 7 NA look the object over before touching it? 1 2 3 4 5 6 7 NA
When asked to wait for a desirable item (such as ice cream), how often did your child seem unable to wait for as long as 1 minute? 1 2 3 4 5 6 7 NA go after it anyway? 1 2 3 4 5 6 7 NA wait patiently? 1 2 3 4 5 6 7 NA whimper and cry? 1 2 3 4 5 6 7 NA
When being gently rocked, how often did your child smile? 1 2 3 4 5 6 7 NA make sounds of pleasure? 1 2 3 4 5 6 7 NA
While visiting relatives or adult family friends s/he sees infrequently, how often did your child stay back and avoid eye contact? 1 2 3 4 5 6 7 NA hide his/her face? 1 2 3 4 5 6 7 NA “warm up” to the person within a few minutes? 1 2 3 4 5 6 7 NA
When you removed something s/he should not have been playing with, how often did your child become sad? 1 2 3 4 5 6 7 NA
During everyday activities, how often did your child become bothered by sounds while in noisy environments? 1 2 3 4 5 6 7 NA become bothered by scratchy materials like wool? 1 2 3 4 5 6 7 NA notice changes in your appearance (such as wet hair,
a hat, or jewellery)? 1 2 3 4 5 6 7 NA appear to listen to even very quiet sounds? 1 2 3 4 5 6 7 NA seem full of energy, even in the evening? 1 2 3 4 5 6 7 NA
When interrupted during a favuorite TV show, how often did your child immediately return to watching the TV program? 1 2 3 4 5 6 7 NA not finish watching the program? 1 2 3 4 5 6 7 NA
While being held on your lap, how often did your child pull away and kick? 1 2 3 4 5 6 7 NA seem to enjoy him/herself? 1 2 3 4 5 6 7 NA mould to your body? 1 2 3 4 5 6 7 NA seek hugs and kisses? 1 2 3 4 5 6 7 NA
While a story was being read to your child, how often did s/he enjoy listening to the story? 1 2 3 4 5 6 7 NA
When hearing about a future family outing (such as a trip to the playground), how often did your child become very enthusiastic? 1 2 3 4 5 6 7 NA look forward to it? 1 2 3 4 5 6 7 NA remain pretty calm? 1 2 3 4 5 6 7 NA
While looking at picture books on his/her own, how often did your child stay interested in the book for 5 minutes or less? 1 2 3 4 5 6 7 NA stay interested in the book for more than 10 minutes
at a time? 1 2 3 4 5 6 7 NA become easily distracted? 1 2 3 4 5 6 7 NA enjoy looking at the books? 1 2 3 4 5 6 7 NA
When tired after a long day of activities, how often did your child become easily frustrated? 1 2 3 4 5 6 7 NA
When a familiar adult, such as a relative or friend, visited your home, how often did your child want to interact with the adult? 1 2 3 4 5 6 7 NA
When asked to do so, how often was your child able to stop an ongoing activity? 1 2 3 4 5 6 7 NA lower his or her voice? 1 2 3 4 5 6 7 NA be careful with something breakable? 1 2 3 4 5 6 7 NA
When visiting a new place, how often did your child not want to enter? 1 2 3 4 5 6 7 NA go right in? 1 2 3 4 5 6 7 NA
While you were showing your child how to do something, how often did your child jump into the task before it was fully explained? 1 2 3 4 5 6 7 NA
While you were talking with someone else, how often did your child easily switch attention from speaker to speaker? 1 2 3 4 5 6 7 NA
During everyday activities, how often did your child become irritated when his/her clothes were tight? 1 2 3 4 5 6 7 NA notice smells from cooking? 1 2 3 4 5 6 7 NA crock back and forth while sitting? 1 2 3 4 5 6 7 NA notice sirens from fire trucks or ambulances at a distance? 1 2 3 4 5 6 7 NA When you mildly criticised or corrected her/his behaviour, how often did your child get mad? 1 2 3 4 5 6 7 NA have hurt feelings? 1 2 3 4 5 6 7 NA
When s/he was upset, how often did your child cry for more than 3 minutes, even when being comforted? 1 2 3 4 5 6 7 NA cheer up within a minute or two when being comforted? 1 2 3 4 5 6 7 NA become easily soothed? 1 2 3 4 5 6 7 NA
When you were busy, how often did your child find another activity to do when asked? 1 2 3 4 5 6 7 NA
While playing outdoors, how often did your child want to jump from heights? 1 2 3 4 5 6 7 NA
want to go down the slide in unusual ways (for example, head first)? 1 2 3 4 5 6 7 NA
enjoy being pushed fast on a wheeled vehicle? 1 2 3 4 5 6 7 NA enjoy sitting down and playing quietly? 1 2 3 4 5 6 7 NA
When playing alone, how often did your child chew his/her lower lip? 1 2 3 4 5 6 7 NA stick out his/her tongue when concentrating? 1 2 3 4 5 6 7 NA move from one task or activity to another without
completing any? 1 2 3 4 5 6 7 NA have trouble focusing on a task without guidance? 1 2 3 4 5 6 7 NA
When given a wrapped present, how often did your child become extremely animated? 1 2 3 4 5 6 7 NA
When around large gatherings of familiar adults or children, how often did your child want to be involved in a group activity? 1 2 3 4 5 6 7 NA enjoy playing with a number of different people? 1 2 3 4 5 6 7 NA
When s/he was asked to share his/her toys, how often did your child become sad? 1 2 3 4 5 6 7 NA
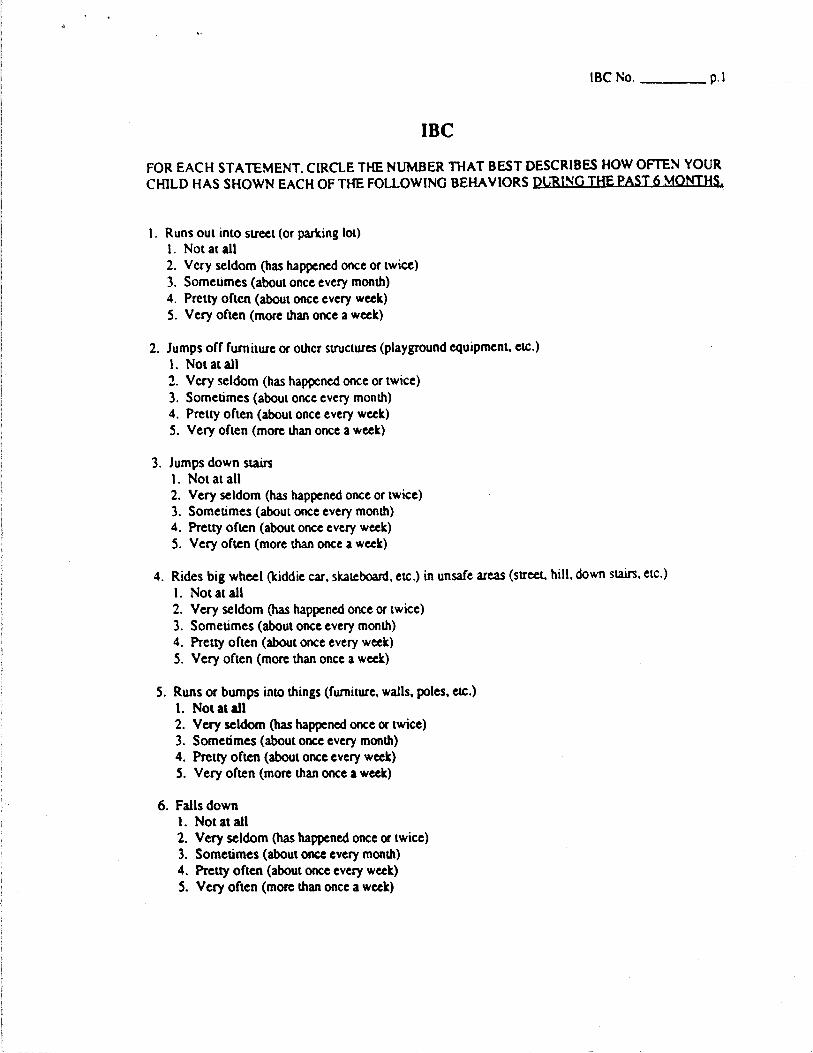
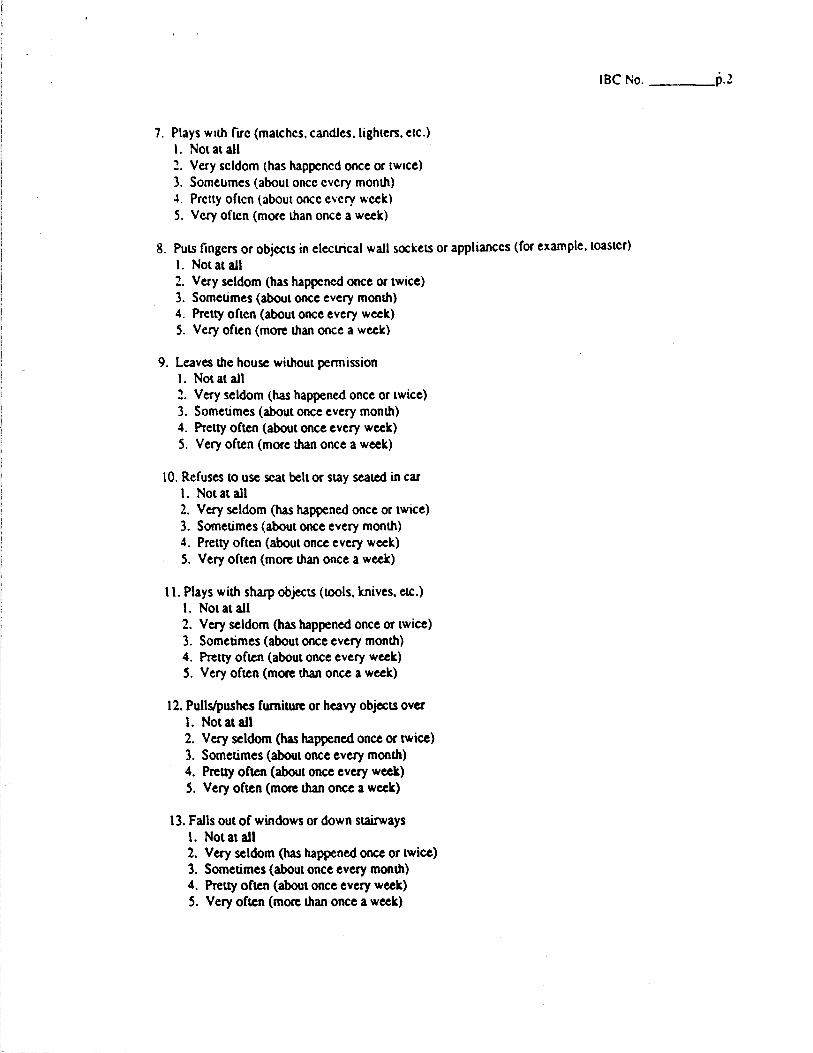
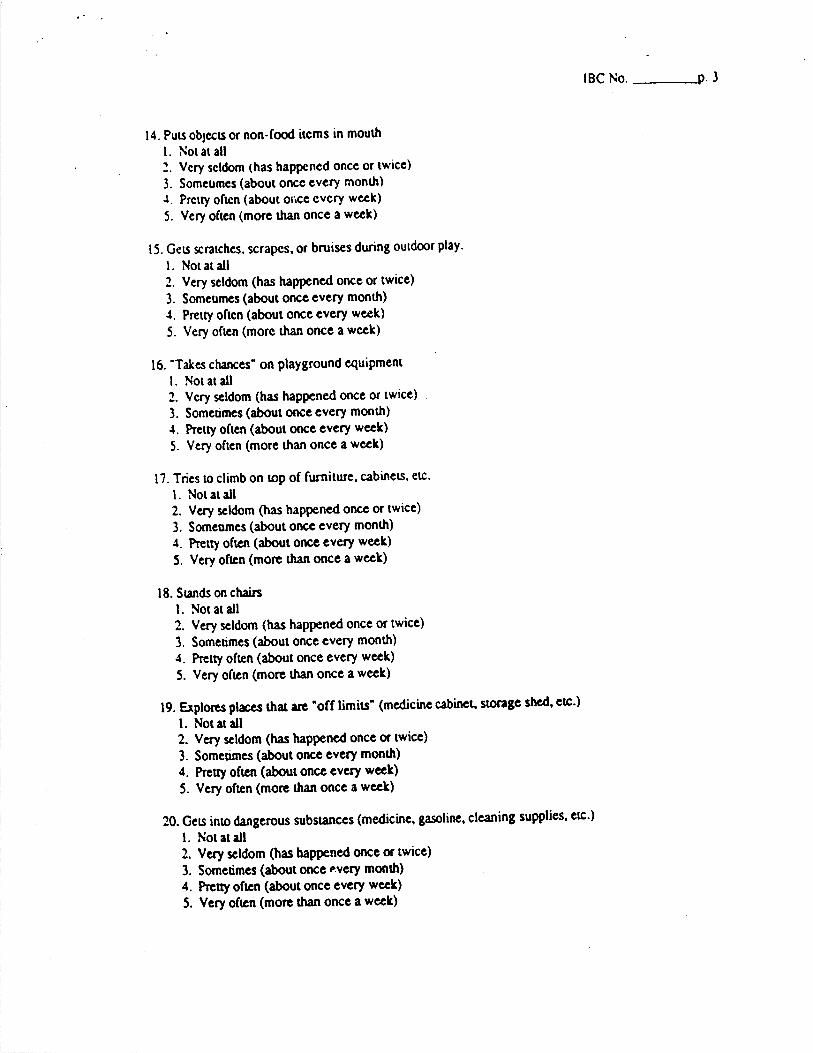
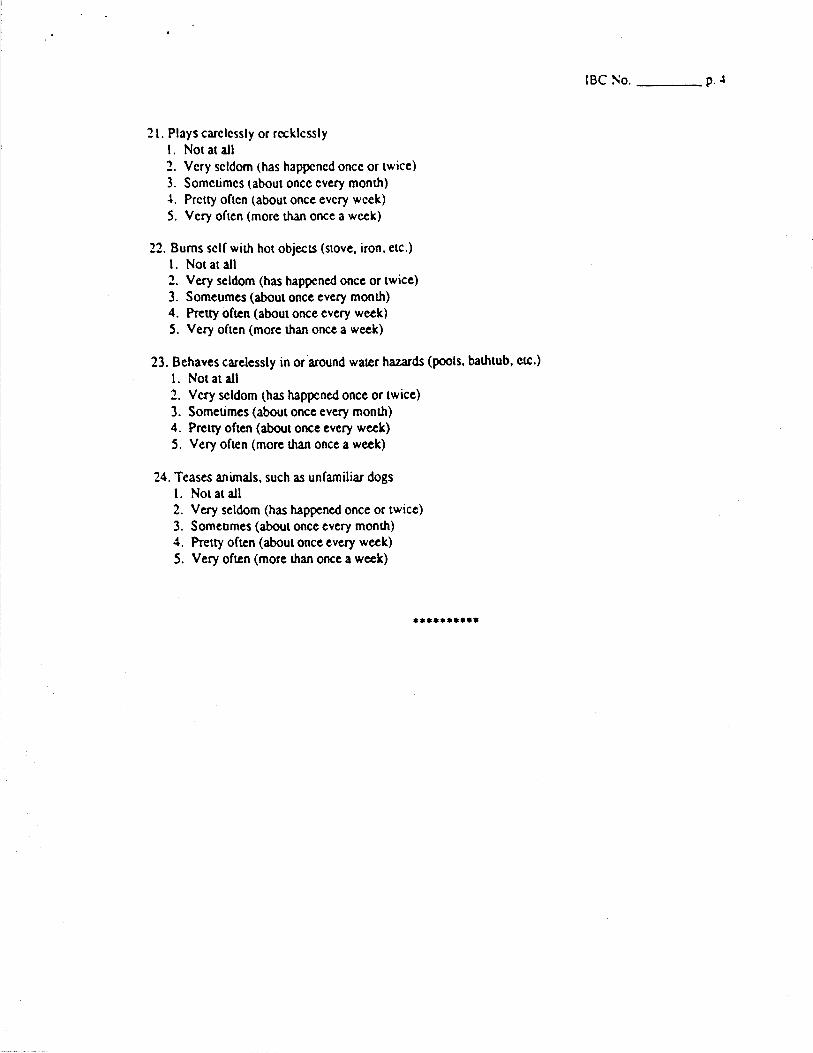
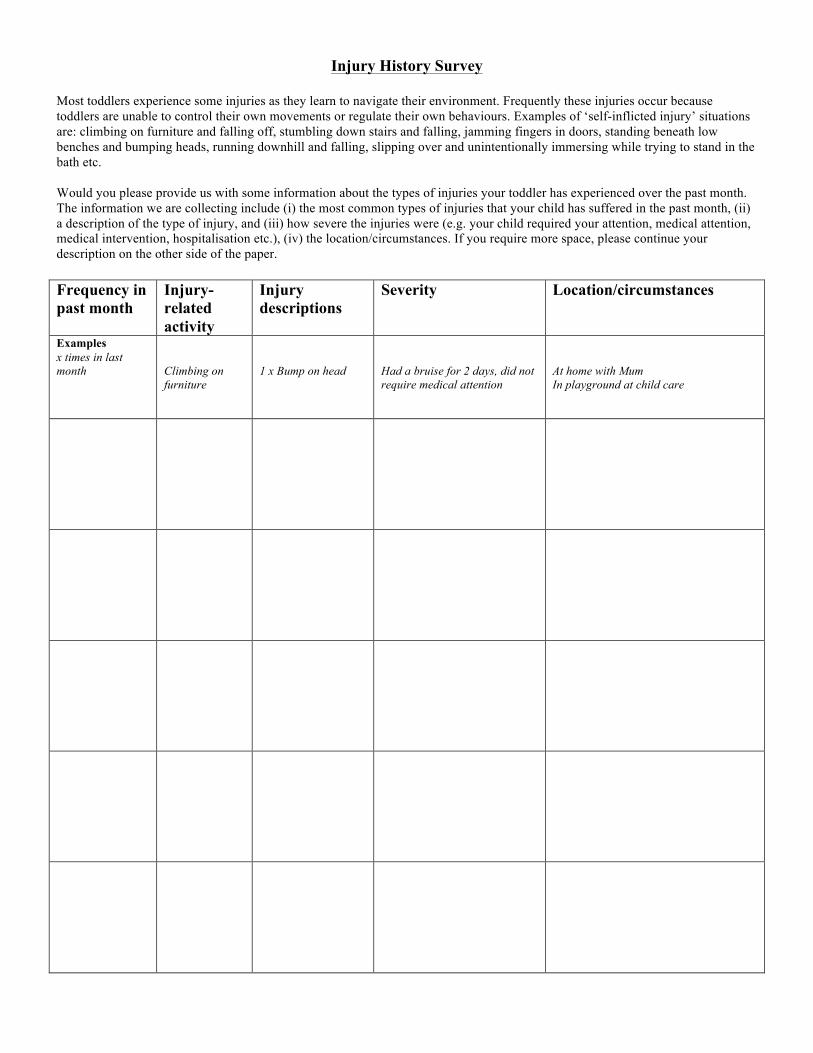
Injury History Survey
Most toddlers experience some injuries as they learn to navigate their environment. Frequently these injuries occur because toddlers are unable to control their own movements or regulate their own behaviours. Examples of ‘self-inflicted injury’ situations are: climbing on furniture and falling off, stumbling down stairs and falling, jamming fingers in doors, standing beneath low benches and bumping heads, running downhill and falling, slipping over and unintentionally immersing while trying to stand in the bath etc. Would you please provide us with some information about the types of injuries your toddler has experienced over the past month. The information we are collecting include (i) the most common types of injuries that your child has suffered in the past month, (ii) a description of the type of injury, and (iii) how severe the injuries were (e.g. your child required your attention, medical attention, medical intervention, hospitalisation etc.), (iv) the location/circumstances. If you require more space, please continue your description on the other side of the paper. Frequency in past month
Injury-related activity
Injury descriptions
Severity Location/circumstances
Examples x times in last month
Climbing on furniture
1 x Bump on head
Had a bruise for 2 days, did not require medical attention
At home with Mum In playground at child care
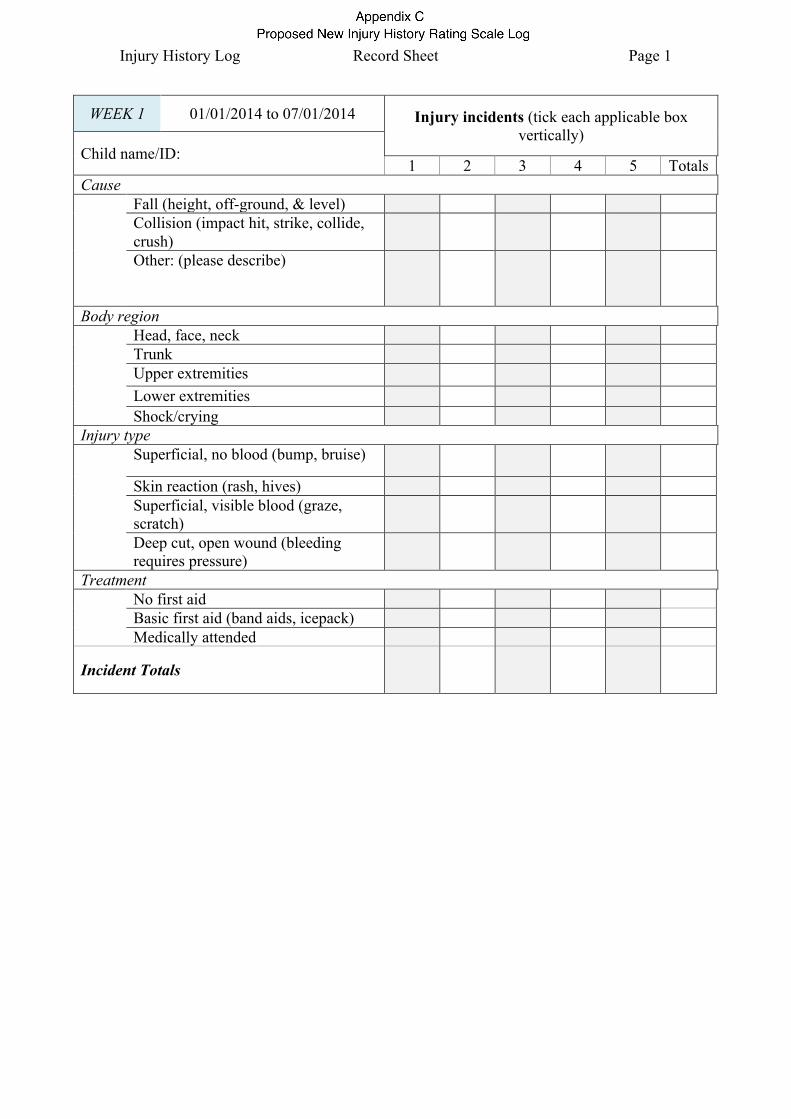
Injury History Log Record Sheet Page 1
WEEK 1 01/01/2014 to 07/01/2014 Injury incidents (tick each applicable box vertically)
Child name/ID: 1 2 3 4 5 Totals
Cause Fall (height, off-ground, & level) Collision (impact hit, strike, collide,
crush)
Other: (please describe)
Body region Head, face, neck Trunk Upper extremities Lower extremities Shock/crying Injury type Superficial, no blood (bump, bruise)
Skin reaction (rash, hives) Superficial, visible blood (graze,
scratch)
Deep cut, open wound (bleeding requires pressure)
Treatment No first aid Basic first aid (band aids, icepack) Medically attended
Incident Totals
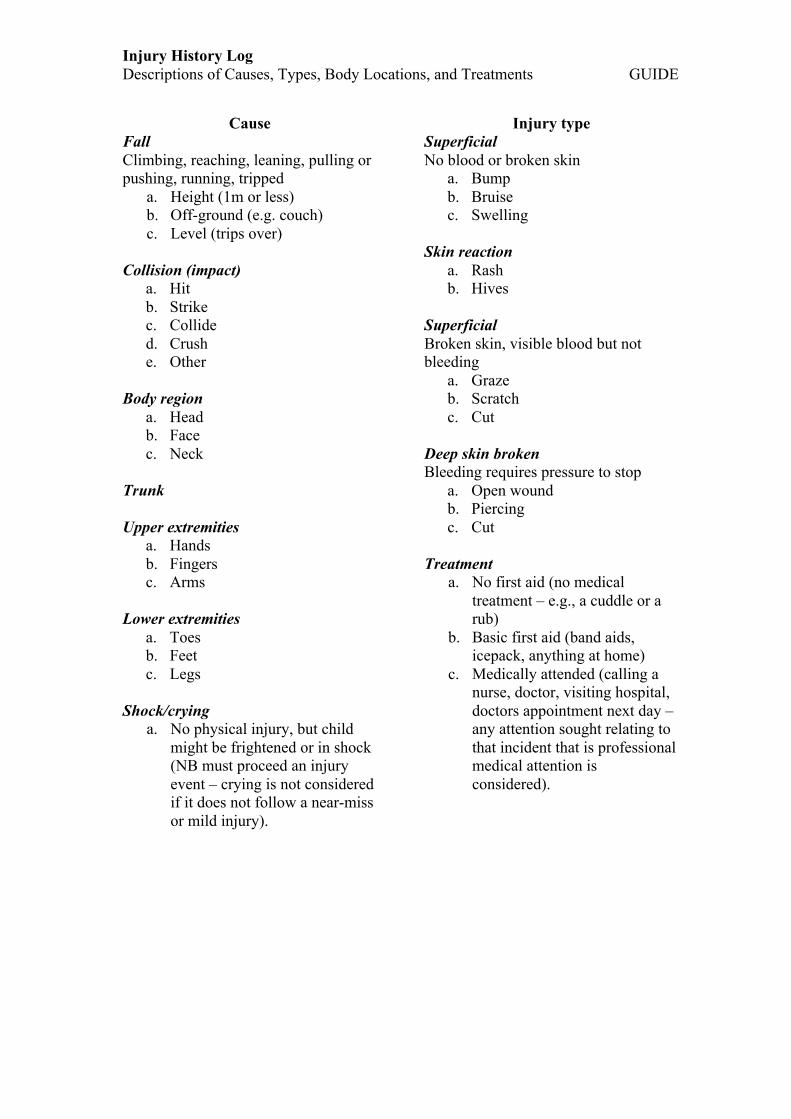
Injury History Log Descriptions of Causes, Types, Body Locations, and Treatments GUIDE
Cause Fall Climbing, reaching, leaning, pulling or pushing, running, tripped
a. Height (1m or less) b. Off-ground (e.g. couch) c. Level (trips over)
Collision (impact)
a. Hit b. Strike c. Collide d. Crush e. Other
Body region
a. Head b. Face c. Neck
Trunk Upper extremities
a. Hands b. Fingers c. Arms
Lower extremities
a. Toes b. Feet c. Legs
Shock/crying
a. No physical injury, but child might be frightened or in shock (NB must proceed an injury event – crying is not considered if it does not follow a near-miss or mild injury).
Injury type Superficial No blood or broken skin
a. Bump b. Bruise c. Swelling
Skin reaction
a. Rash b. Hives
Superficial Broken skin, visible blood but not bleeding
a. Graze b. Scratch c. Cut
Deep skin broken Bleeding requires pressure to stop
a. Open wound b. Piercing c. Cut
Treatment
a. No first aid (no medical treatment – e.g., a cuddle or a rub)
b. Basic first aid (band aids, icepack, anything at home)
c. Medically attended (calling a nurse, doctor, visiting hospital, doctors appointment next day – any attention sought relating to that incident that is professional medical attention is considered).