Surveillance of Fetal Alcohol
Syndrome
Why Healthy People gave up
counting

Healthy People
• Healthy People 2000 objective was to
reduce the occurrence of FAS to 1.2 per
10,000 (0.12 per 1,000)
• Healthy People 2010 objective was to
reduce the occurrence of FAS – why?

FAS Prevalence Rates*
1.7
4.2
2.97
0.8.6120.0
0.9 2.2
2.0
3.1
30.0
.37
2.9
.33
8.51.3
.23 3.9
1.4
.67
* Per 1,000 live births

Issues in FAS Surveillance
• Diagnosis is difficult – depends on several
factors
• Diagnosis is difficult in the newborn (>3 yrs)
– facial features may not be evident
– CNS difficult to evaluate
• Lack of training, inconsistent diagnostic criteria
• Clinicians reluctant to make the diagnosis
– Do not want to stigmatize the mothers
– Do not know what to do or where to refer


Assessing Palpebral Fissure
Length
Courtesy of Dr. Luther Robinson

Prevalence of FAS from Various Methods*
Method Pop Years Ages Rate**BMDP US 1981-86 nb 0.07
BDMP US 1992 nb 0.52
MACDP Atlanta 1992 nb 0.33
Multiple Alaska 1977-1992 3-18 yrs 0.3 (3-5)
Clinic-based US-Low SES 70s-90s nb ~2.0
Special Studies Native AM 60s-90s 0-18 2-120
Special Studies South Africa 1990s 6-7 39
School-Based Washington 2001 1st grade 3.1
* Adapted from May et al. Dev Dis Res Rev. 2009;15:176-192) ** per 1,000

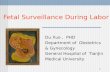
Fetal Alcohol Syndrome Surveillance Network
(FASSNet) States
CO
AZ
WI NY
AK


FASSNet Surveillance Region
•Allegany
•Cattaraugus
•Chautauqua
•Erie
•Genesee
•Monroe
•Niagara
•Orleans
•Wyoming

• Genetics clinics (Buffalo & Rochester)
• Early Intervention programs
• Hospitals
• Congenital Malformations Registry (CMR)
• Birth defect surveillance program (NBDPS)
• Developmental Disabilities Clinic in Rochester
• Hospital Discharge Data (SPARCS)
• NYS Vital Records
• Parents and Children Together Clinic; Foster
Care Pediatric Clinic
Data Sources

FAS Prevalence by Race/Ethnicity, 1995-1999,
Using FAS Surveillance Network Methodology
Western New York Erie County Urban Buffalo
Race/
EthnicityLive
Births Cases
Rate
per
1000
Live
Births Cases
Rate
per
1000
Live
Births Cases
Rate
per
1000
Non-Hispanic
White 111,802 33 0.30 44,364 15 0.34 12,047 10 0.83
Black 22,574 43 1.90 10,862 36 3.31 10,165 35 3.44
Hispanic 6,117 1 0.16 1,856 1 0.54 1,530 1 0.65
Amer. Indian/
Native
Alaskan 1,081 2 1.85 366 1 2.73 145 1 6.90
Total ** 145,260 79 0.54 58,757 53 0.90 24,431 47 1.92
* Per 1,000 live births, based on maternal residence at birth
** Includes all racial groups including Asian and Other

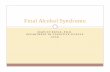
NYS FAS prevalence rates with different
methods of detection (3-yr moving average)
a per 1,000 live births
b Congenital Malformations Registry (CMR)
c Fetal Alcohol Syndrome Surveillance Network (FASSNet)
0.00
0.10
0.20
0.30
0.40
0.50
0.60
90-92 91-93 92-94 93-95 94-96 95-97 96-98
3 Year Time Period
P
revale
nce R
ate
(per
1,0
00 b
irth
s)
760.71 by CMR (NYS
excluding Western
NY)
760.71 by CMR (9-
County Western NY)
FASSNet

Initial Ascertainment Source, Erie and Monroe Counties,
New York FASSNet, 1995-1999
Source All Children Children with FAS
Erie Monroe Erie Monroe
Directly Accessible
SPARCS
CMR/NBDPS
Birth Certificates
248 (45.7%)
36 (6.6%)
73 (13.5%)
155 (69.8%)
5 (2.2%)
37 (16.7%)
32 (29.1%)
21 (19.1%)
8 (7.3%)
3 (27.3%)
1 (9.0%)
0 (0%)
Source Provided
Genetics clinic
Early Intervention
Other (physicians,
developmental
clinics, other
clinics)
75 (13.9%)
65 (12.0%)
45 (8.3%)
5 (2.3%)
12 (5.4%)
8 (3.6%)
36 (32.7%)
9 (8.2%)
4 (3.6%)
2 (18.2%)
2 (18.2%)
3 (27.3%)
Total*
Total Children
542 (100%)
420
222 (100%)
208
110 (100%)
53
11 (100%)
10
* Total greater than # of children as they were independently ascertained at more than one source

FAS Abstractions With "Face" Data
by Source, 1995-1999
Source Erie MonroeDirectly Accessible
Hospital Record
CMR/NBDPS
42 (37%)
1 (1%)
6 (30%)
0 (0%)
Source Provided
Genetic Clinic
Early Intervention
Other
43 (38%)
0 (0%)
27 (24%)
3 (15%)
1 (5%)
10 (50%)
Total Children 113 (100%) 20 (100%)

What Might Account for the Differences?
In Monroe county, anecdotal reports that clinicians do not diagnose
FAS and few referrals are made to the geneticist
In Erie county, Dr Robinson, a nationally known expert in FAS,
has established an FAS clinic and performs outreach education and
training
In Monroe county, most referrals come from ‘passive sources’,
fewer referrals come from genetics clinics

Improving Methods for population-based FAS
surveillance, Feb 2008 – Action Items
• Streamline Data Collection items
• Develop QA/Qc measures
• System should use high risk populations
but also broader data collection
• Expand databases – Medicaid, schools..

Improving Methods for population-based FAS
surveillance, Feb 2008 – Action Items
Continued
• Develop and disseminate a clear message
to providers and families on the benefits of
diagnosing FAS (Incentivize the diagnosis)
• Consider focusing on a peak age of
diagnosis
• Increase diagnostic capacity

FASSNet II!!!!• Use a multiple source surveillance methodology to determine the
prevalence of FAS
– Study cohort: 7-9 year olds; Study year: 2010
• Develop a standardized clinical review procedure that will be implemented uniformly by all sites
• Improve or build upon an existing surveillance system to ascertain infants and children with FAS and generate population-based surveillance data
• Establish or expand relationships with facilities where children with FAS are likely to be diagnosed or received services
• Evaluate the surveillance system methodology
– Quality assurance procedures
• Implement provider training and education on FAS to improve case ascertainment

FASSnet II
• Three Sites
– Arizona
– Colorado
– New York
• Building on FASSnet and FASlink
• Adding CNS expertise
• Began abstraction Fall 2010!!

• Clinic-Plus programs, Office of Mental Health
• ECCPASA’s Fetal Alcohol & Drug Effects Program
• Robert Warner Rehabilitation Center
• Special Needs Clinic of WCHOB
• Hodge Pediatrics
• Early Childhood Direction Center
• Native American Community Services
• Hopevale, Inc.
• DePaul Developmental Services (Rochester)
• NYS Office of Children & Family Services
• Unified Court System
• Division of Juvenile Justice & Opportunities for Youth
New York New Data Sources

Closing Thoughts
FAS Surveillance is sensitive to clinician education, interest
and cooperation
Clinicians need to be educated not only in how to make the
diagnosis but why it is important
If you are going to do FAS surveillance, it really helps to have
Dr. Robinson!!!
The more carefully you look for FAS, the more you find