Fetal Alcohol Syndrome Arunraj Group-10

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Fetal Alcohol Syndrome
ArunrajGroup-10

Definition:Fetal alcohol syndrome is growth, mental, and
physical problems that may occur in a baby when a mother drinks alcohol during pregnancy.
In the United States, alcohol is the leading known preventable cause of birth defects, both physical and developmental.Many women drink alcohol while pregnant. It is estimated that each year in the US, 1 in every 750 infants are born with FAS, while another 40,000 are born with fetal alcohol effects (FAE).

Types of Fetal Alcohol Spectrum disorder
Fetal Alcohol Syndrome (FAS)Alcohol-Related Neurodevelopmental Disorder (ARND)Alcohol-Related Birth Defects (ARBD)

Fetal Alcohol Syndrome (FAS):
FAS represents the severe end of the FASD . Fetal death is the most extreme outcome from drinking alcohol during pregnancy. People with FAS might have abnormal facial features, growth problems, and central nervous system (CNS) problems. People with FAS can have problems with learning, memory, attention span, communication, vision, or hearing. They may have one or more of these problems. This is one of the number one causes for mental retardation.
Alcohol-Related Neurodevelopmental Disorder (ARND):
People with ARND might have intellectual disabilities and problems with behavior and learning. They might do poorly in school and have difficulties with math, memory, attention, judgment, and poor impulse control.
Alcohol-Related Birth Defects (ARBD):
People with ARBD might have problems with the heart, kidneys, or bones or with hearing. They might have a mix of these.

PATHOPHYSIOLOGYAlcohol crosses the placenta and rapidly reaches the fetusFetus liver does not have significant alcoholdehydrogenase(ADH), ALDH and other antioxidants like glutathion Also amniotic acts as reservoir for alcohol, prolonging fetal exposure. Acetaldehyde( metabolite of ethanol) disrupt cellular differentiation and growth, disrupting DNA and protein synthesis and inhibits cell migration.Acetaldehyde and ethanol modify metabolism of carbohydrate, protein and fatsThey both also decrease the transfer of amino acids, glucose, folic acid, zinc and other nutrients across the placenta barrier which affects fetal growth.

Alcohol in a pregnant woman's bloodstream circulates to the fetus by crossing the placenta. There, the alcohol interferes with the ability of the fetus to receive sufficient oxygen and nourishment for normal cell development in the brain and other body organs.

Alcohol Exposure During the Pregnancy Trimesters
First: During the first trimester, alcohol interferes with the migration and organization of brain cells and the formation of the CNS.Second: Heavy drinking during the second trimester, particularly from the 10th to 20th week after conception, seems to cause more clinical features of FAS than at other times during pregnancy.Third: During the third trimester, the hippocampus is greatly affected, which leads to problems with encoding visual and auditory information (reading and math) and the inability to form or retain new memories.


Brain of Child with FAS
http://www.come-over.to/FAS/FASbrain.htm

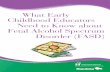
CELLS THAT SHOULD FORM MIDLINE STRUCTURES OF THE BRAIN AND FACE ARE
KILLED BY ALCOHOL
Developingbrain and
face
Heart
Mouse embryo (viewed from the front) at a stage corresponding
to a 22-23 day old human.
A close-up view of an alcohol-exposed mouse embryo shows cells killed by alcohol
that have taken up a dark blue stain.

EYE EYE
A C
B D
MOUTH MOUTH
NOSTRILSNOSTRILS
MIDLINE STRUCTURES OF THE FACE AND BRAIN ARE DEFICIENT INALCOHOL-EXPOSED MOUSE EMBRYOS AND IN INDIVIDUALS WITH FAS
THE FACE OF A CHILDWITH FULL-BLOWN FAS
HAS FEATURES THATCAN BE CAUSED BY DAMAGE TO MIDLINE
STUCTURES.
COMPARISON OF THE FACE (A) AND INTERIOR OF THE BRAIN (B) OF A NORMAL MOUSE EMBRYO AND ONE DAMAGED BY ALCOHOL (C&D) SHOWS THAT THE NOSTRILS
ARE ABNORMALY POSITIONED (C) AND THE BRAIN IS MISSING MIDLINE STRUCTURES (D).

SYMPTOMSGrowth RetardationFacial Features
Smooth philtrum Thin upper lip (thin vermilion) Small eyes Short upturned nose Flattened cheeks Small jaw ( maxillae or mandible)

Facial Features
NORMAL FEATURESABNORMAL FEATURES

Facial FeaturesNORMAL FEATURES
ABNORMAL FEATURES

SYMPTOMSCentral nervous system features
Microcephaly Mental retardation Hyperactivity Impaired language development Delayed development of gross motor skills like rolling
over, sitting up, crawling and walking Delayed in development of fine motor skills such as
grasping objects with the thumb and index fingers and transfer objects from one hand to the other.
Seizures

OTHER SIGNS Cardiac• Heart murmur; usually disappears by one year
of age• VSD• ASD Skeletal: Joint abnormalities, altered palmer
crease pattern, small distal phalanges and small fifth fingernail.
Renal: Horseshoe, aplastic, dysplastic or hypoplastic kidney.
Ocular: Strabismus, optic nerve hypoplasia Low birth weight

DIAGNOSIS The diagnostic criteria includes; Growth deficiency FAS facial features Central nervous system damage Prenatal alcohol exposure

Treatment Options:There's no cure or specific treatment for fetal alcohol syndrome. The physical defects and mental deficiencies typically persist for a lifetime. Heart abnormalities may require surgery. Learning problems may be helped by special services in school. Parents often benefit from counseling to help the family with a child's behavioral problem.

Examples of Successful Programs
Behavioral Regulation Training (BRT)
BRT teaches parents ways to modify the child’s environment to reduce excess stimulation, use appropriate social reinforcement, and communicate choices rather than commands.
Parent Child Interaction Therapy (PCIT)
Behavioral specialists conduct group sessions with parents to teach them appropriate and effective behaviors and interaction techniques
Parent-Assisted Social Skills Training
Children participate in didactic training sessions, behavior rehearsal, and coaching to reduce maladaptive behaviors and promote pro-social interaction skills

Parenting and TeachingTry differently, not harder!

Alcohol-relatedbirth defects
last a lifetime.
So Don’t drink while pregnant


ReferencesEmory University (n.d.). Maternal Substance Abuse and Child Development. Retrieved December 28, 2009 from http://www.psychiatry.emory.edu/ PROGRAMS/GADrug/fasqa.htm#doesGraefe, Sara. (2004). (Ed.). Living with FASD: A Guide For Parents. British Columbia: Special Needs Adoptive Parents. Groundwork Press. Retrieved December 23, 2009 from website: http://www.faslink.org/strategies_not_solutions.pdf
Kellerman, Teresa (2005). Symptoms of Fetal Alcohol Spectrum Disorders.Retrieved December 28, 2009 from http://www.come-over.to/FAS/faschar.htmKellerman, Teresa (2008). Prenatal Alcohol Exposure and the Brain. Retrieved December 28, 2009 from http://www.come-over.to/FAS/FASbrain.htm

References ContinuedKock, Gregory C. &Kupesky, Regina H. (2002). Parenting the Hurt Child: Helping Adoptive Families Heal and Grow. Pinon Press. Retrieved December 23, 2009 from website: http://www.faslink.org/strategies_not_solutions.pdf
Learning about FASD (2009). Retrieved December 31, 2009 from http://www.fasdoutreach.ca/elearning/learning-about-fasd
Look Who’s in Jail! (n.d.). Retrieved December 29, 2009 from http://www.come-over.to/FAS/jailbaby.htm
Mayo Clinic (2009). Fetal Alcohol Ayndrome. Retrieved December 28, 2009, from http://www.mayoclinic.com/health/fetal-alcohol-syndrome/DS00184/ DSECTION=symptoms.
National Institute on Alcohol Abuse and Alcoholism (n.d.). Module 10K Fetal
Alcohol Exposure. Retrieved January 2, 2010 from http://pubs.niaaa.nih.gov/publications/Social/Module10KFetaExposure
/Module10K.html
Related Documents