



Pediatric Distal Radial Pediatric Distal Radial FracturesFractures
Andrew Grabowski1/21/00GCOH

TorusTorus
Bulges secondary to a longitudinally compressive force
Only involves one cortex
TorusTorus
May present with only minimal swelling or hematoma
Treatment consists of a cast or splint from 2-4 weeks
Mostly for protection and comfort

TorusTorus
GreenstickGreenstick
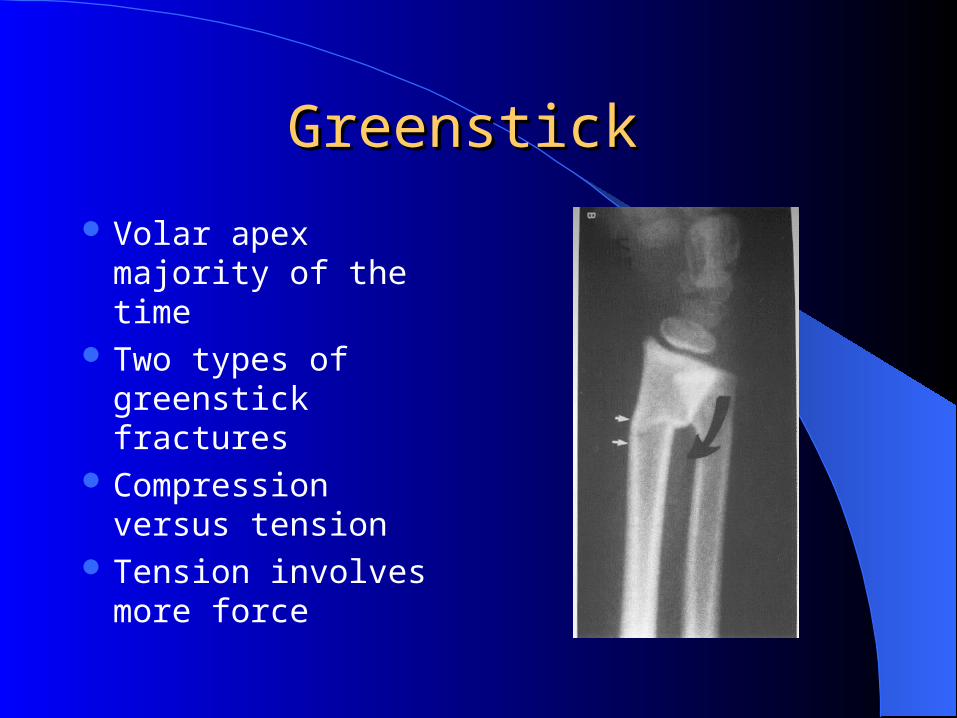
Volar apex majority of the time
Two types of greenstick fractures
Compression versus tension
Tension involves more force
GreenstickGreenstick
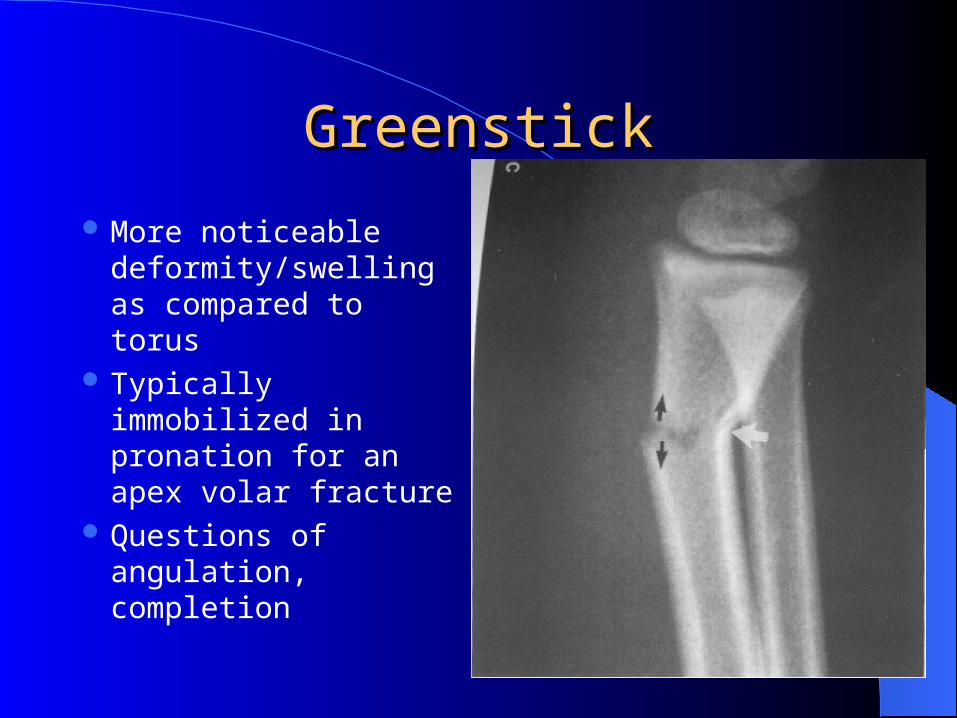
More noticeable deformity/swelling as compared to torus
Typically immobilized in pronation for an apex volar fracture
Questions of angulation, completion
BayonetBayonet
Complete loss of end-to-end appositionBoth the dorsal and volar cortexes failed,
resulting in a disruption of both corticesMost bayonet fractures are dorsal
BayonetBayonet
Obvious deformity fracture compared to torus and greenstick
Classic “silver-fork” deformity
Questions of acceptable angulation

BayonetBayonet






























