TREATMENT OF DISTAL FEMUR FRACTURES DANIEL ZINAR , MD LOS ANGELES COUNTY HARBOR UCLA MEDICAL CENTER CHIEF ORTHOPEDIC TRAUMA PROFESSOR OF CLINICAL ORTHOPEDIC SURGERY UCLA MEDICAL SCHOOL

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
TREATMENT OF DISTAL FEMUR
FRACTURES
DANIEL ZINAR , MD
LOS ANGELES COUNTY HARBOR UCLA MEDICAL CENTER
CHIEF ORTHOPEDIC TRAUMA
PROFESSOR OF CLINICAL ORTHOPEDIC SURGERY UCLA MEDICAL SCHOOL
DISCLOSURES
•Nothing to disclose
•No royalties
•No industry affiliation
DISTAL FEMUR FRACTURES
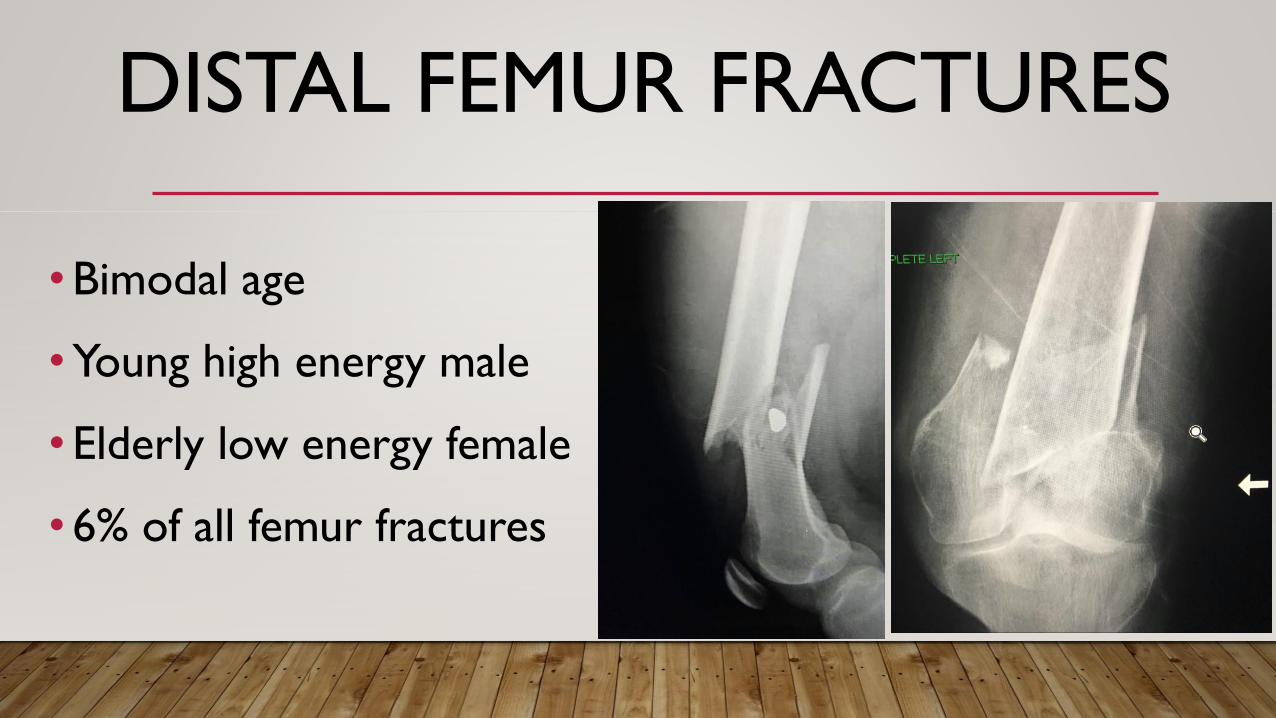
•Bimodal age
•Young high energy male
•Elderly low energy female
•6% of all femur fractures
DIFFICULT FRACTURES
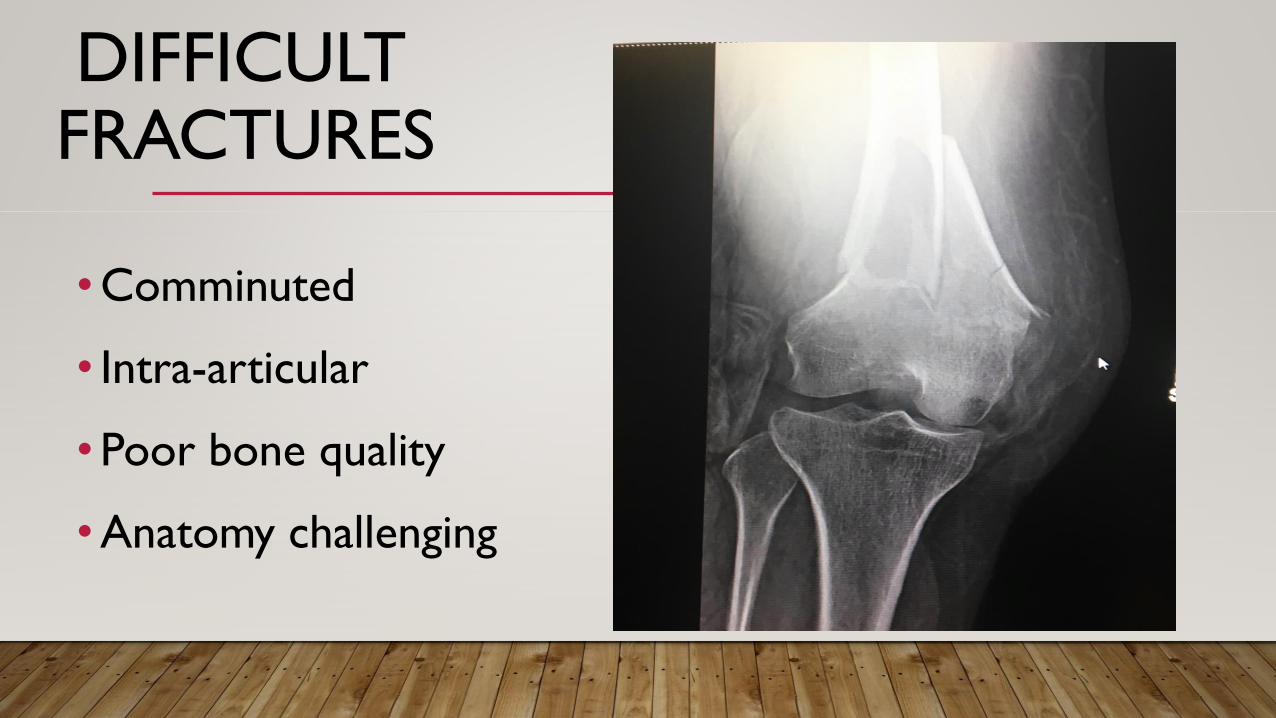
•Comminuted
• Intra-articular
•Poor bone quality
•Anatomy challenging
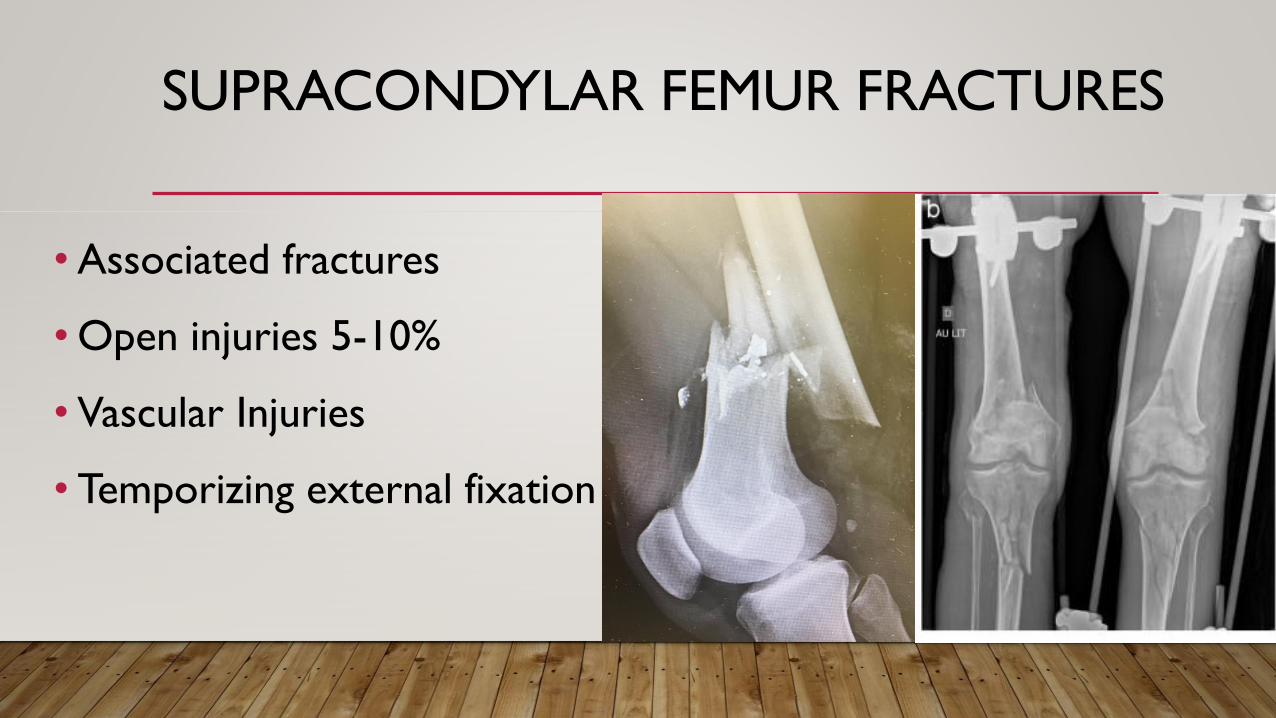
SUPRACONDYLAR FEMUR FRACTURES
•Associated fractures
•Open injuries 5-10%
• Vascular Injuries
• Temporizing external fixation
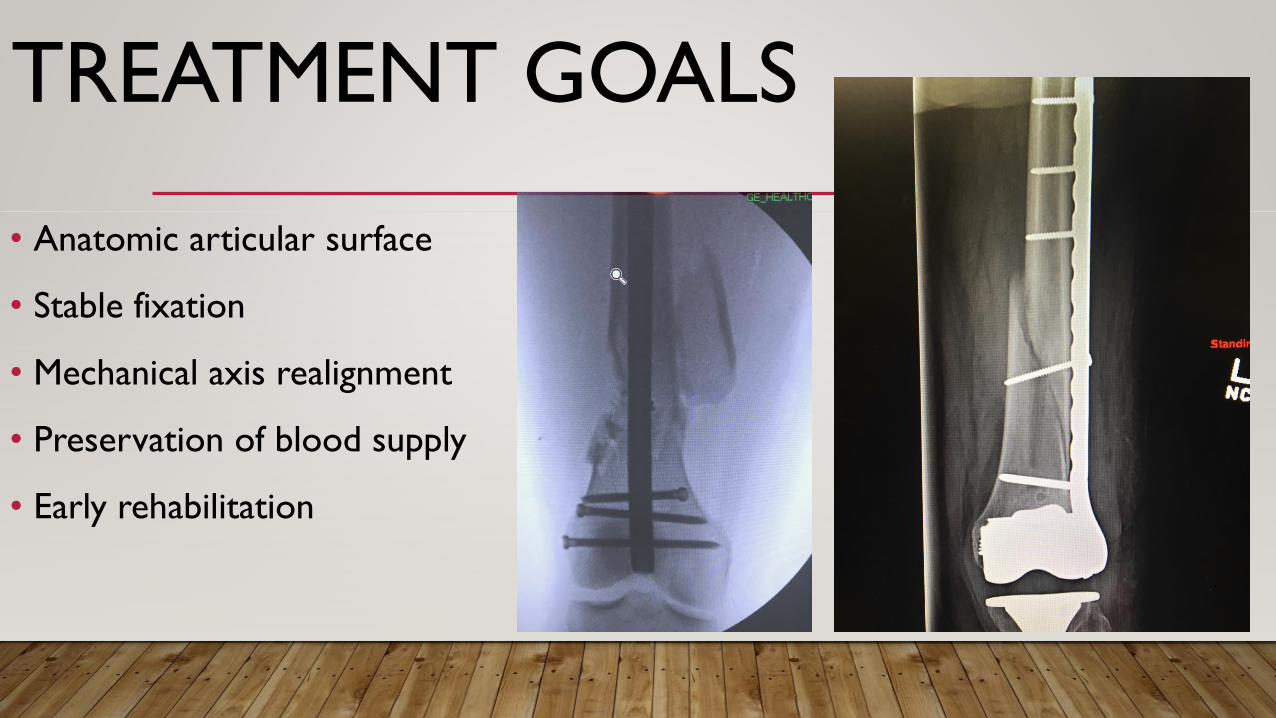
TREATMENT GOALS
• Anatomic articular surface
• Stable fixation
• Mechanical axis realignment
• Preservation of blood supply
• Early rehabilitation
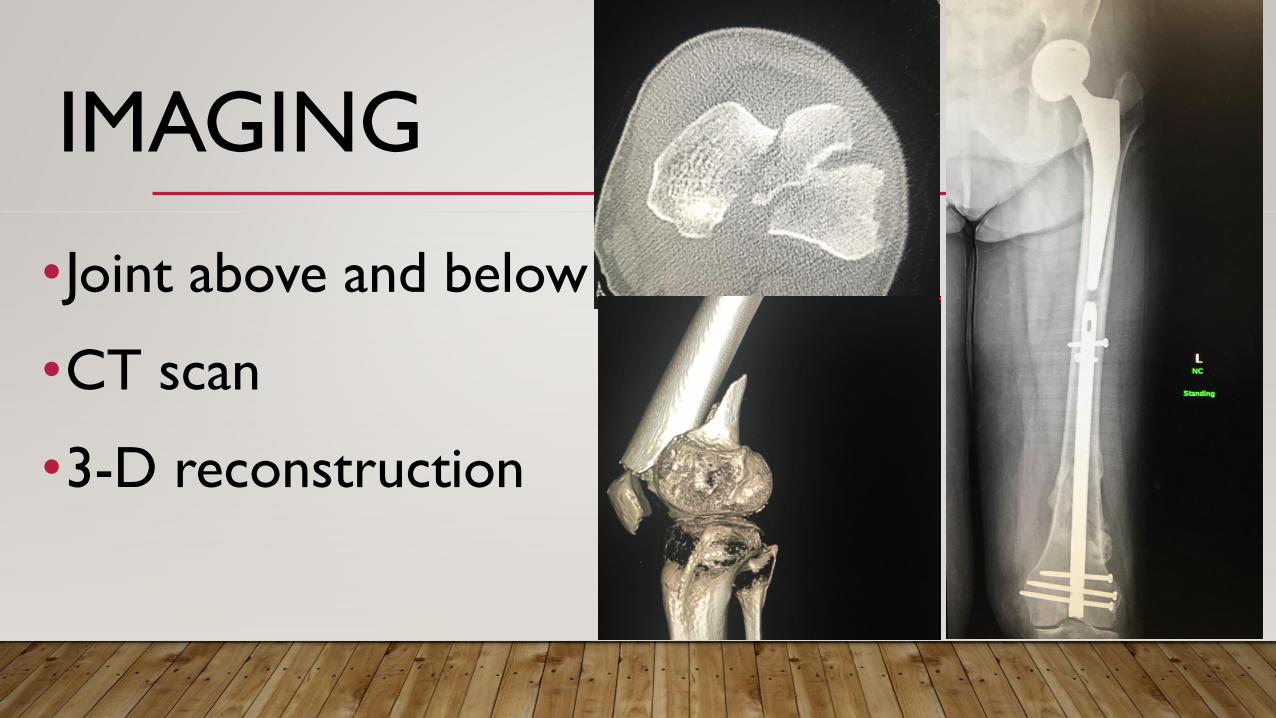
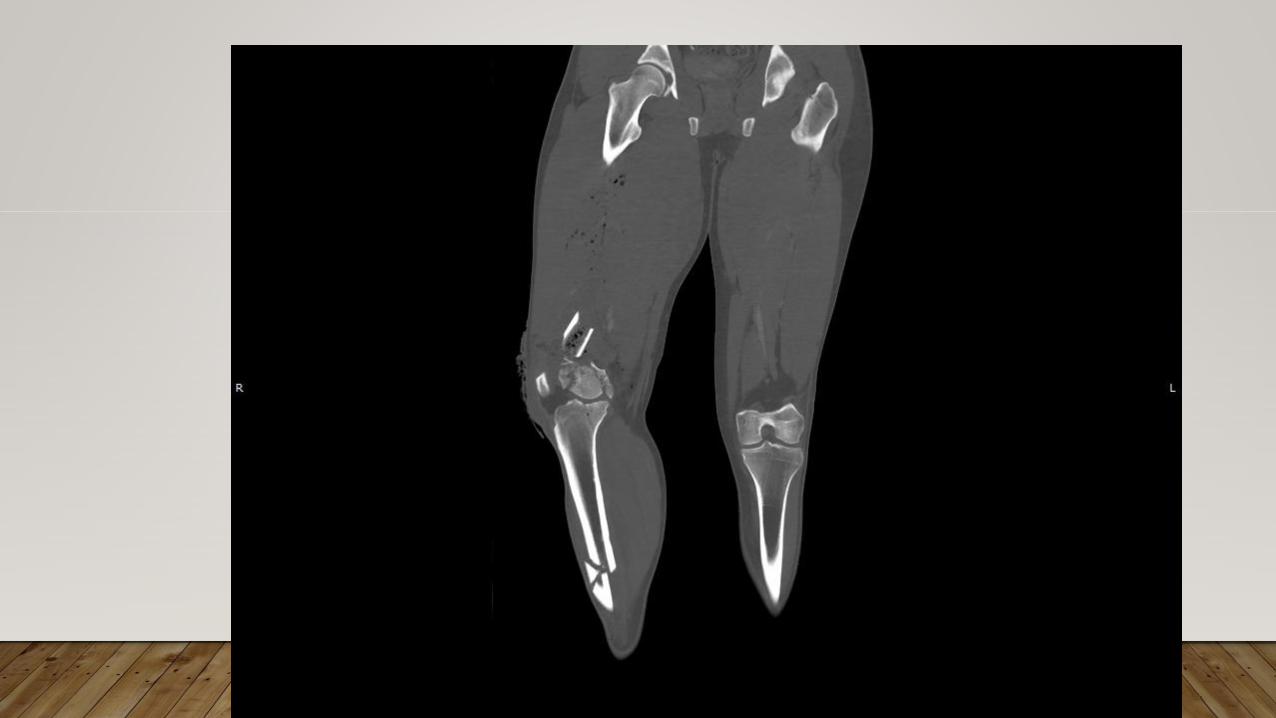
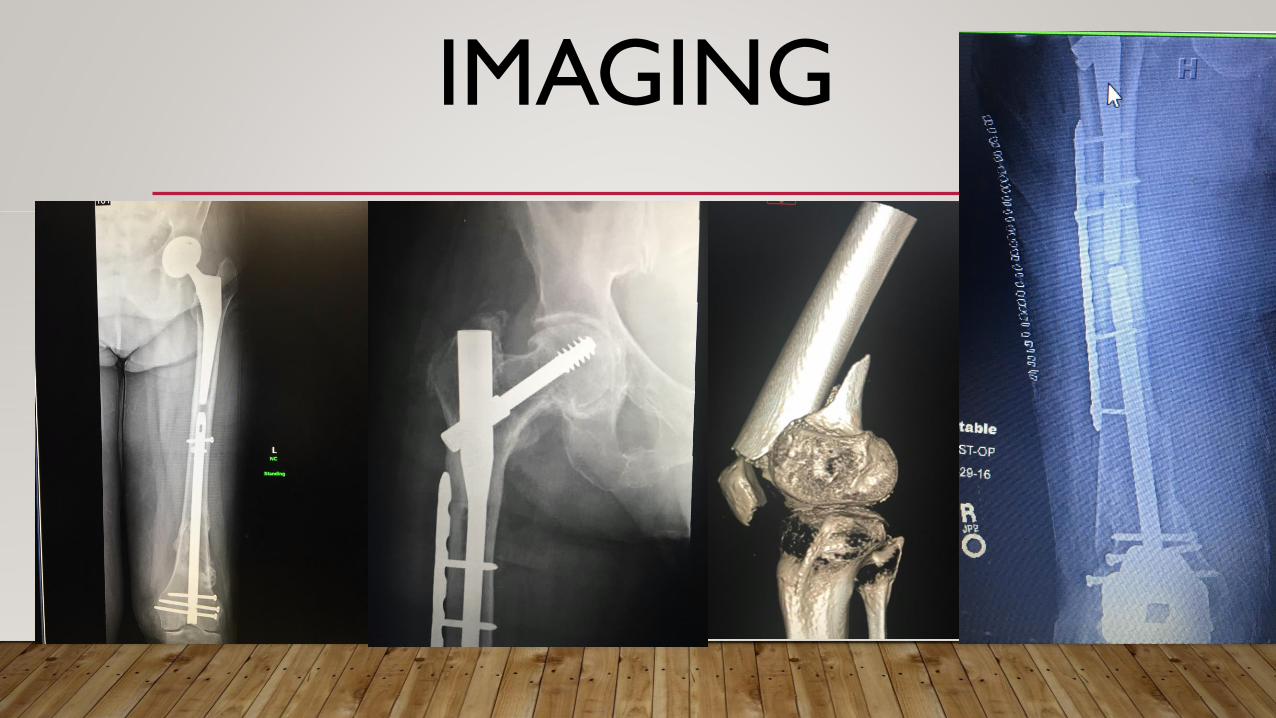
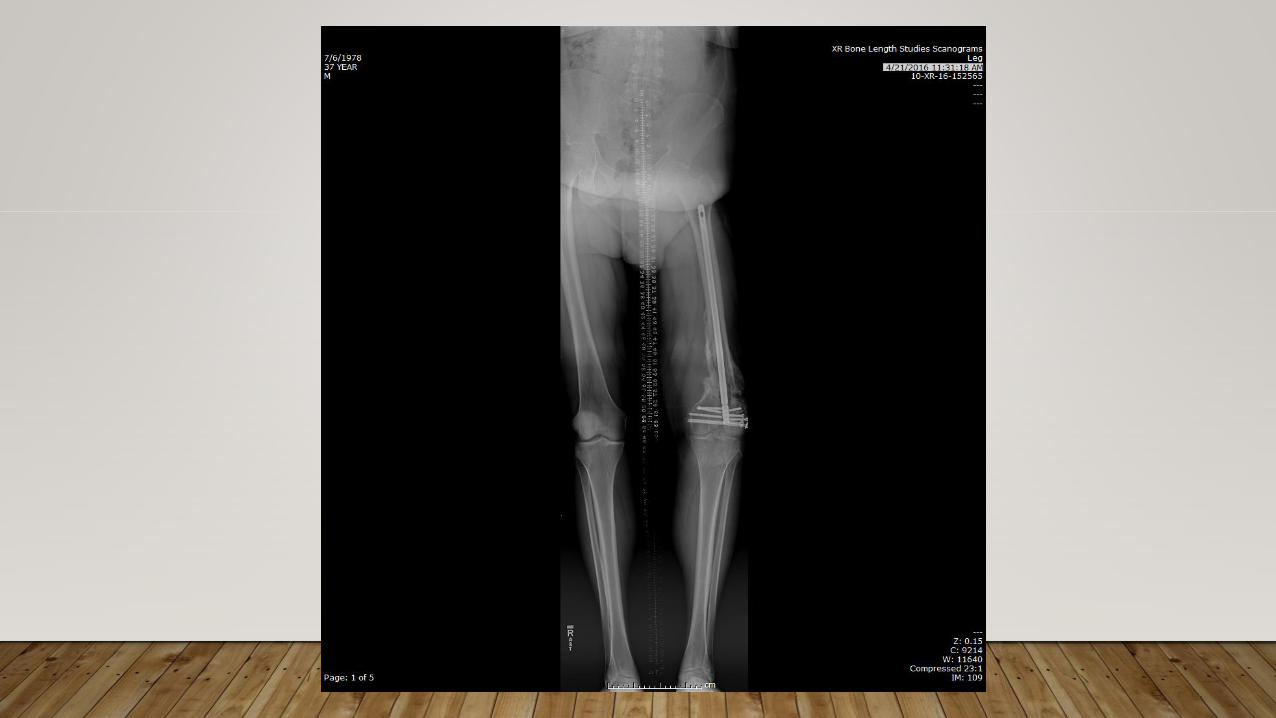
IMAGING
•Joint above and below
•CT scan
•3-D reconstruction
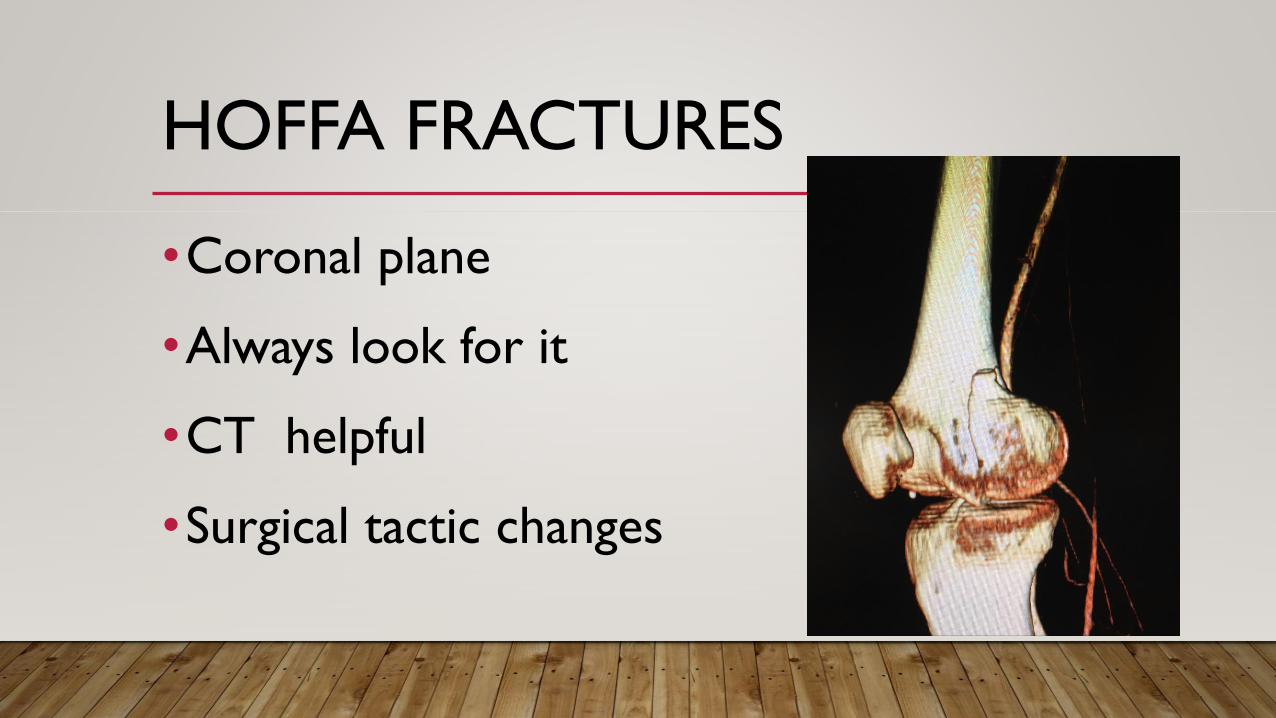
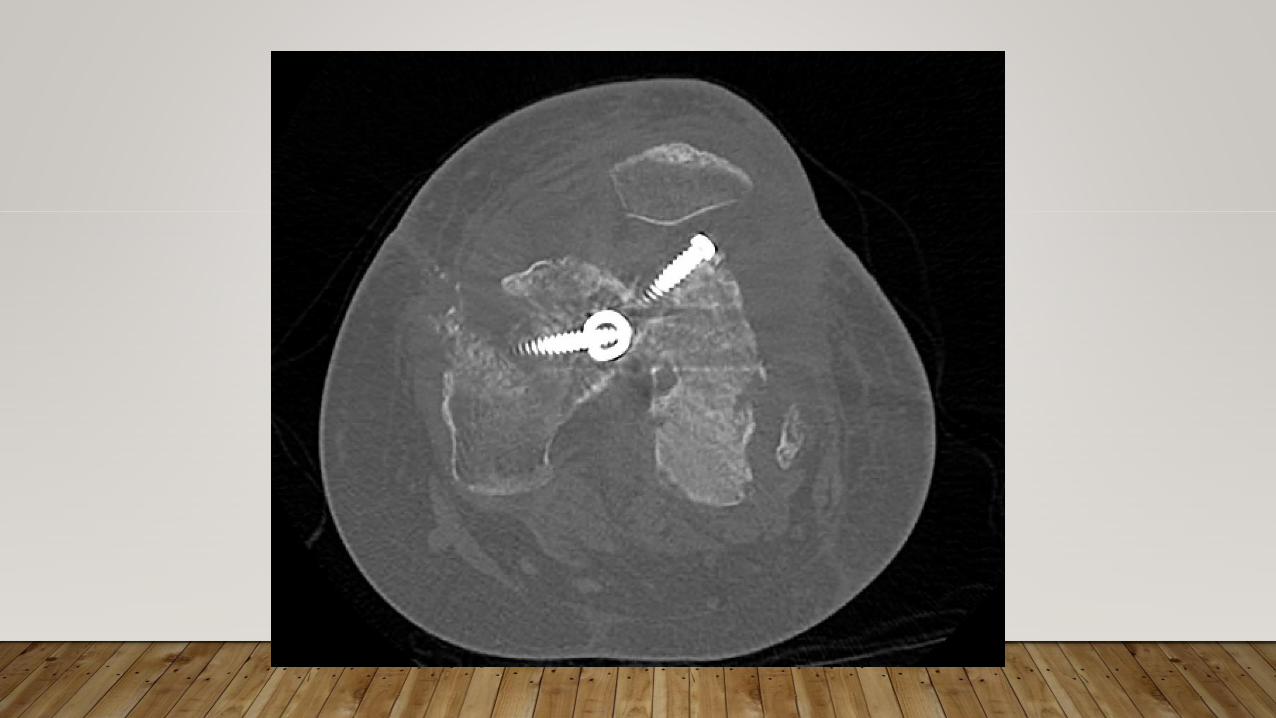
HOFFA FRACTURES
•Coronal plane
•Always look for it
•CT helpful
•Surgical tactic changes
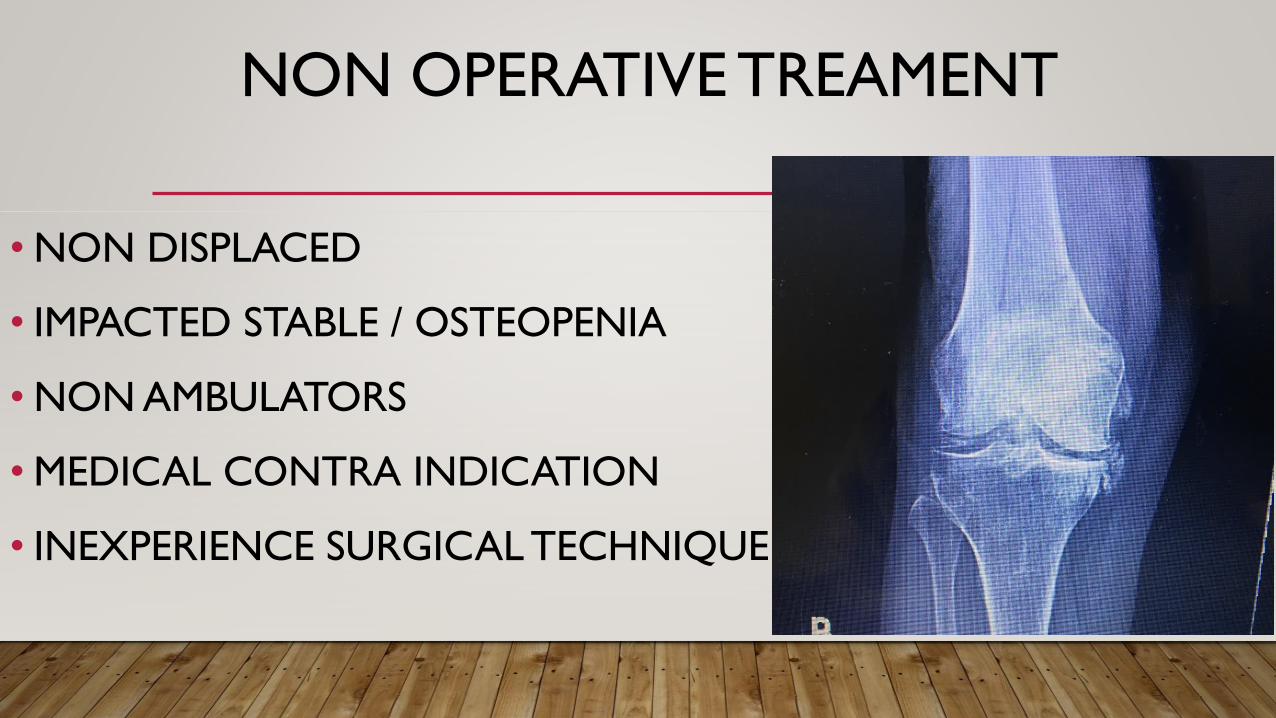
NON OPERATIVE TREAMENT
• NON DISPLACED
• IMPACTED STABLE / OSTEOPENIA
• NON AMBULATORS
• MEDICAL CONTRA INDICATION
• INEXPERIENCE SURGICAL TECHNIQUE
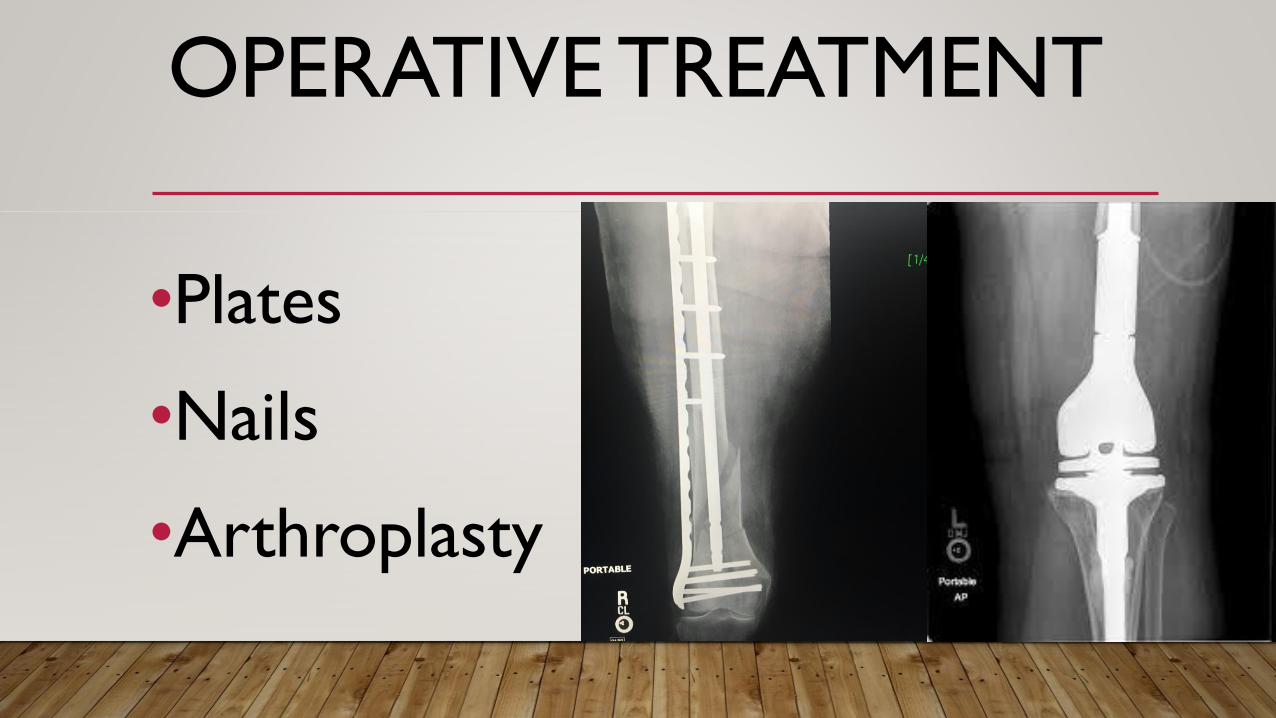
OPERATIVE TREATMENT
•Plates
•Nails
•Arthroplasty
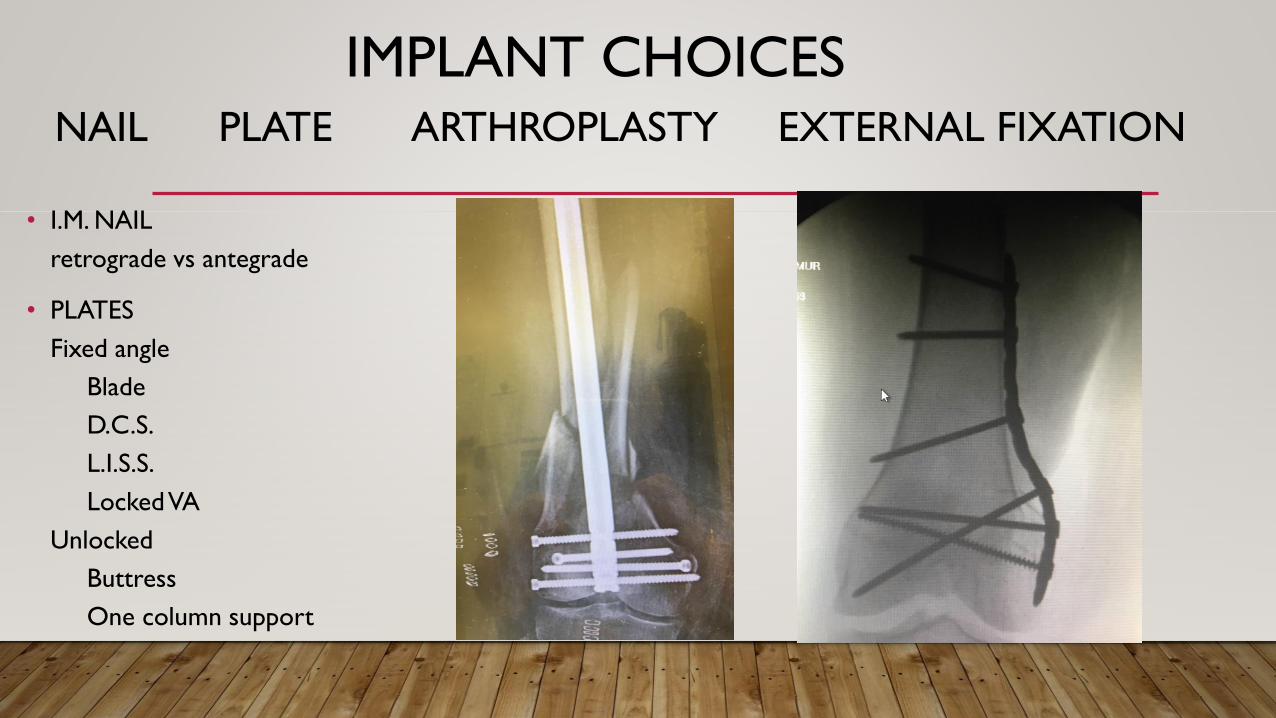
IMPLANT CHOICESNAIL PLATE ARTHROPLASTY EXTERNAL FIXATION
• I.M. NAIL
retrograde vs antegrade
• PLATES
Fixed angle
Blade
D.C.S.
L.I.S.S.
Locked VA
Unlocked
Buttress
One column support
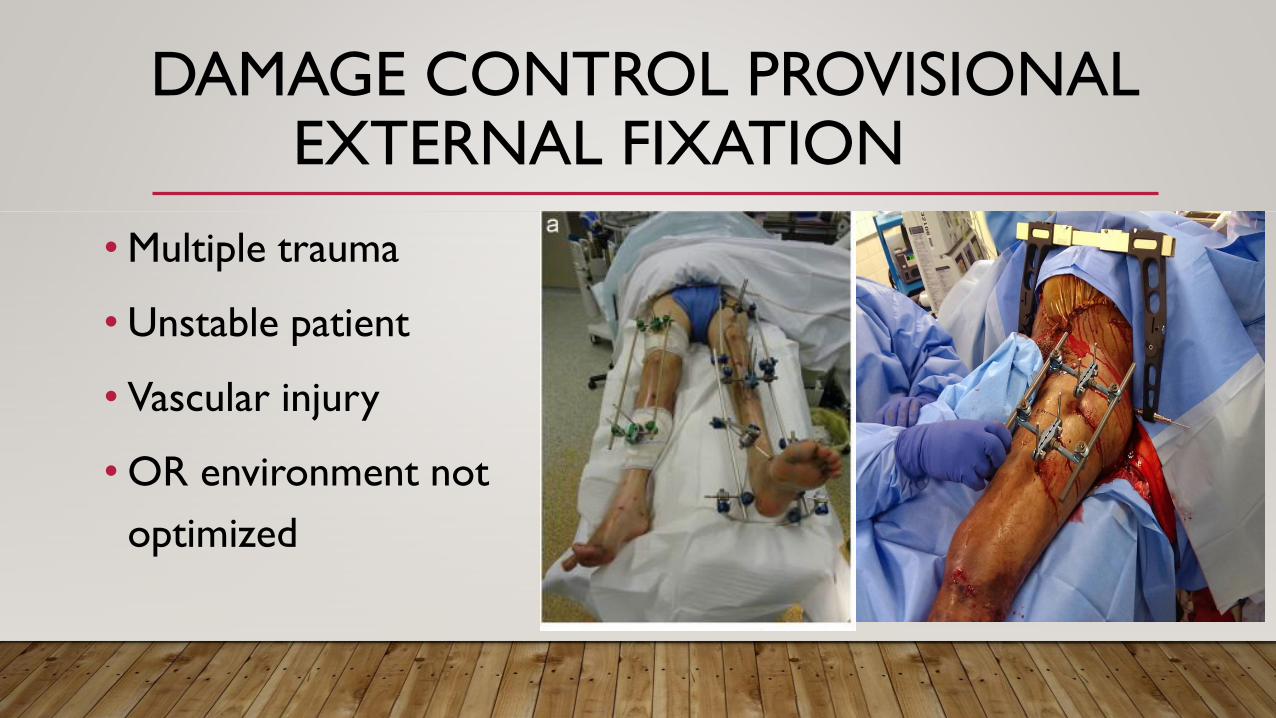
DAMAGE CONTROL PROVISIONALEXTERNAL FIXATION
• Multiple trauma
• Unstable patient
• Vascular injury
• OR environment not
optimized
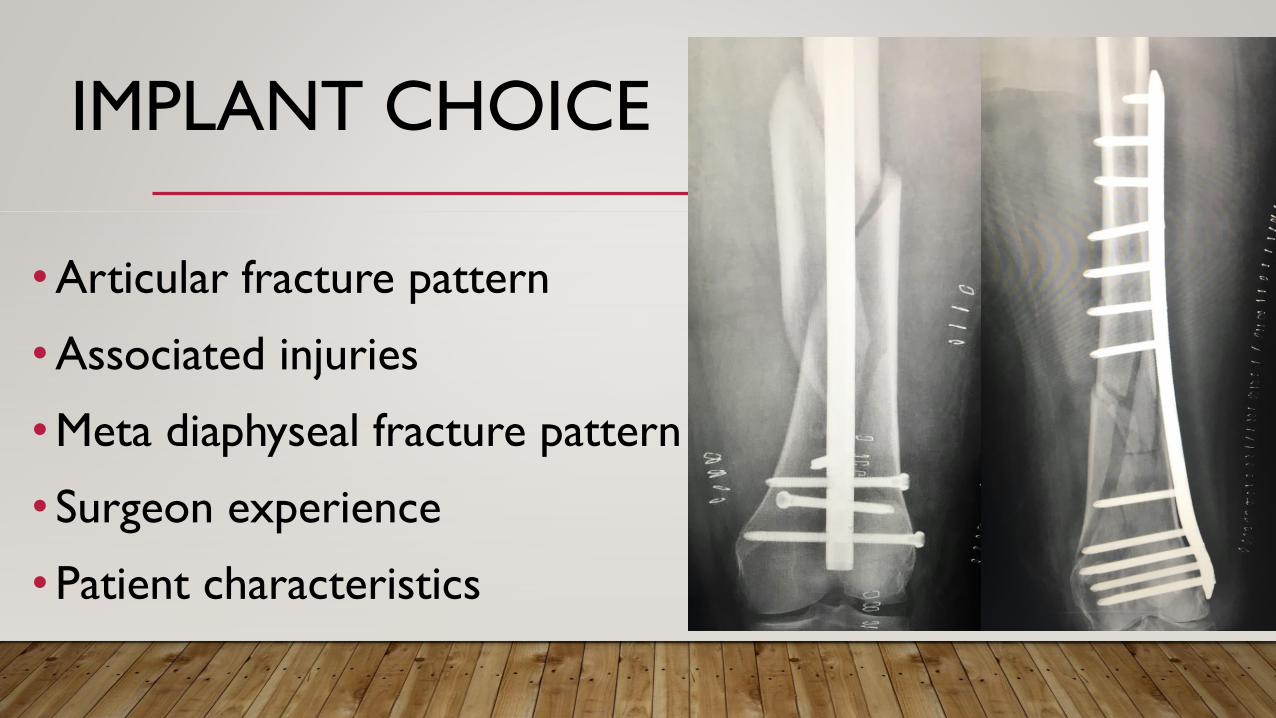
IMPLANT CHOICE
•Articular fracture pattern
•Associated injuries
•Meta diaphyseal fracture pattern
• Surgeon experience
•Patient characteristics
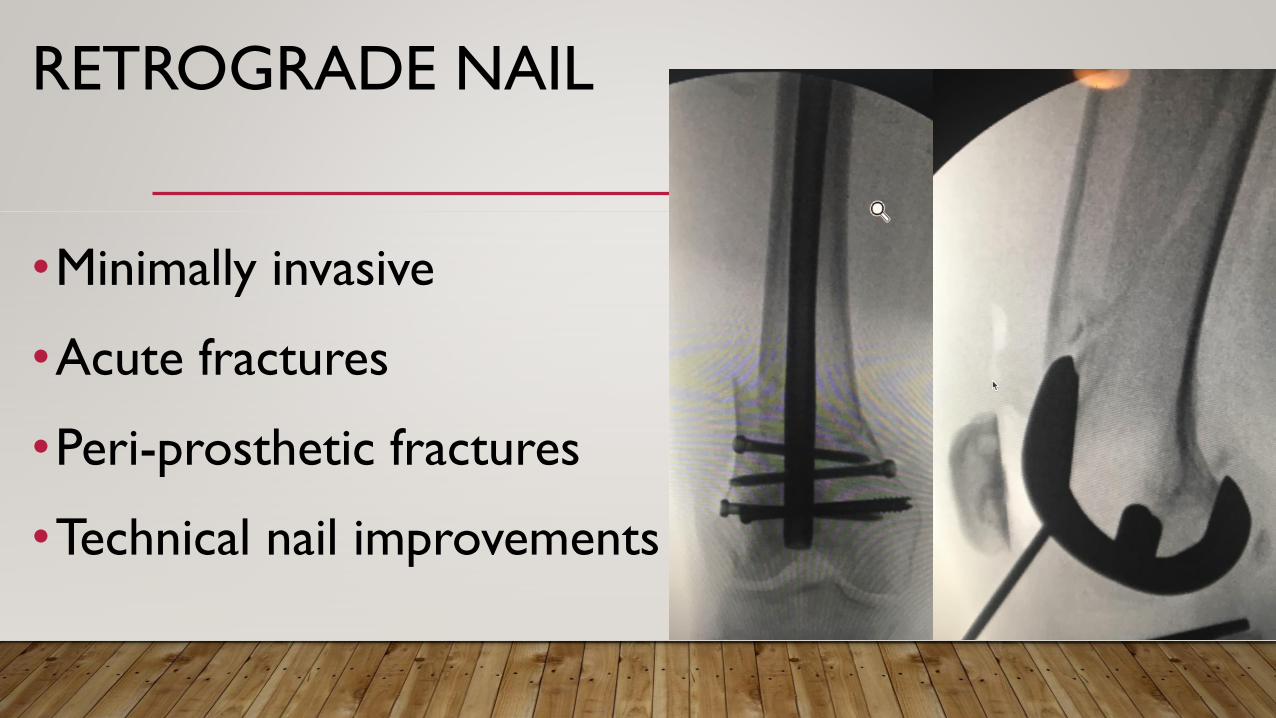
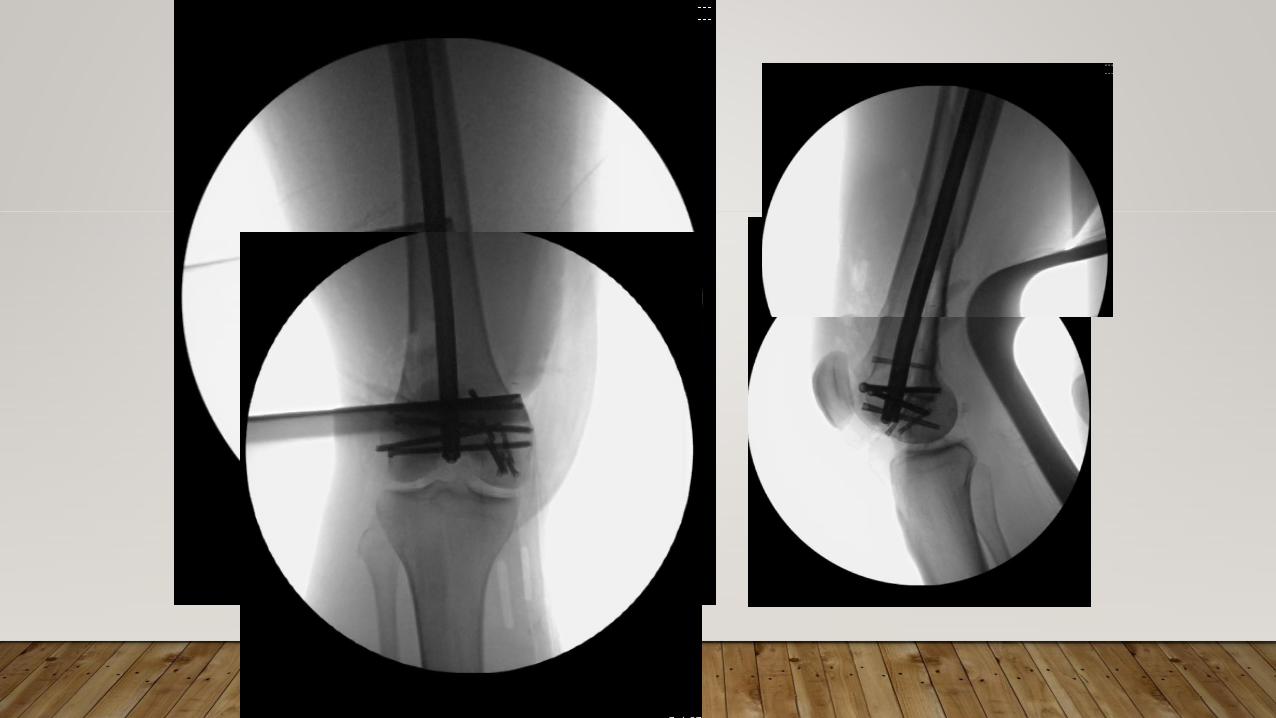
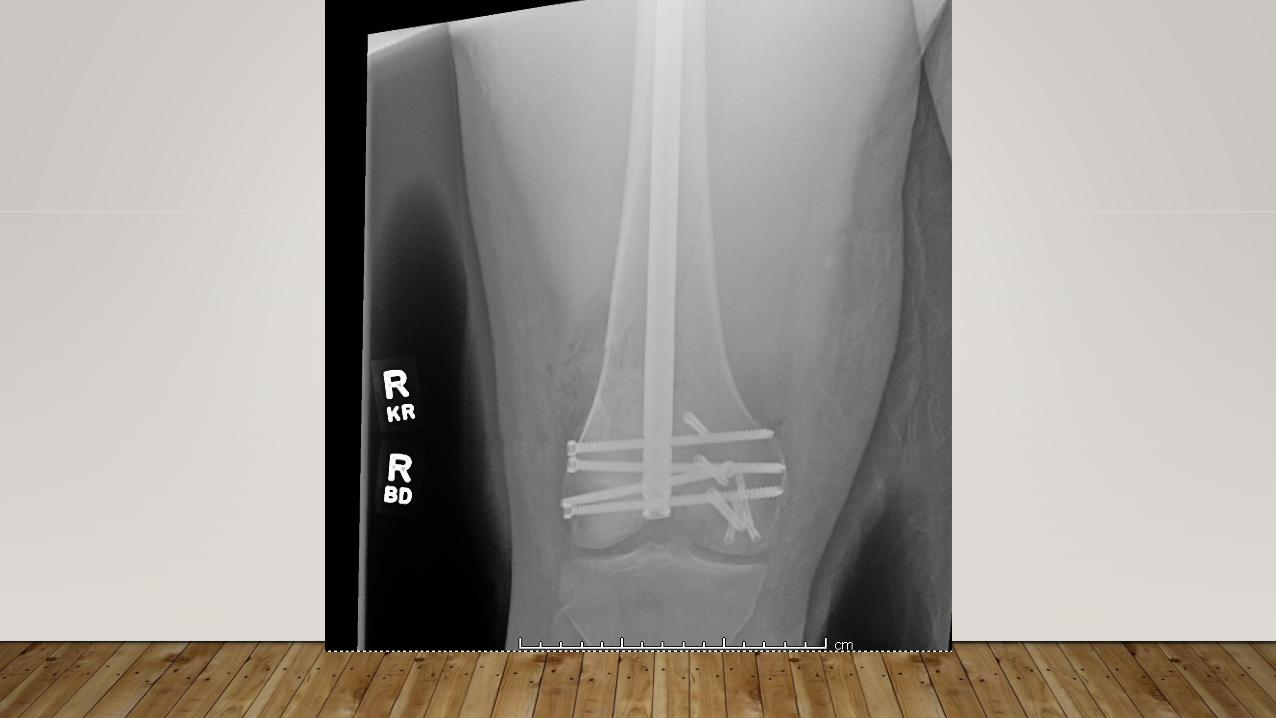
RETROGRADE NAIL
•Minimally invasive
•Acute fractures
•Peri-prosthetic fractures
•Technical nail improvements
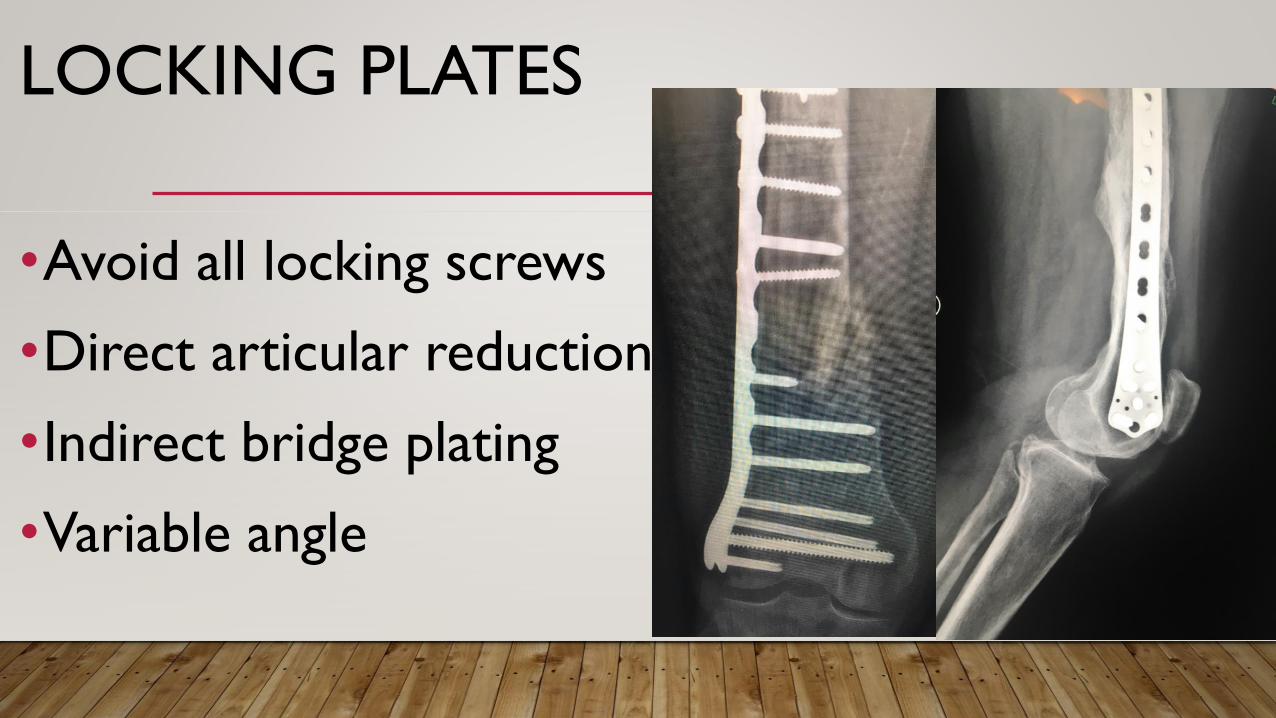
LOCKING PLATES
•Avoid all locking screws
•Direct articular reduction
•Indirect bridge plating
•Variable angle

92 year old
female
W.D.
Trip and
fall

4 months
post op
no new trauma
W.D.
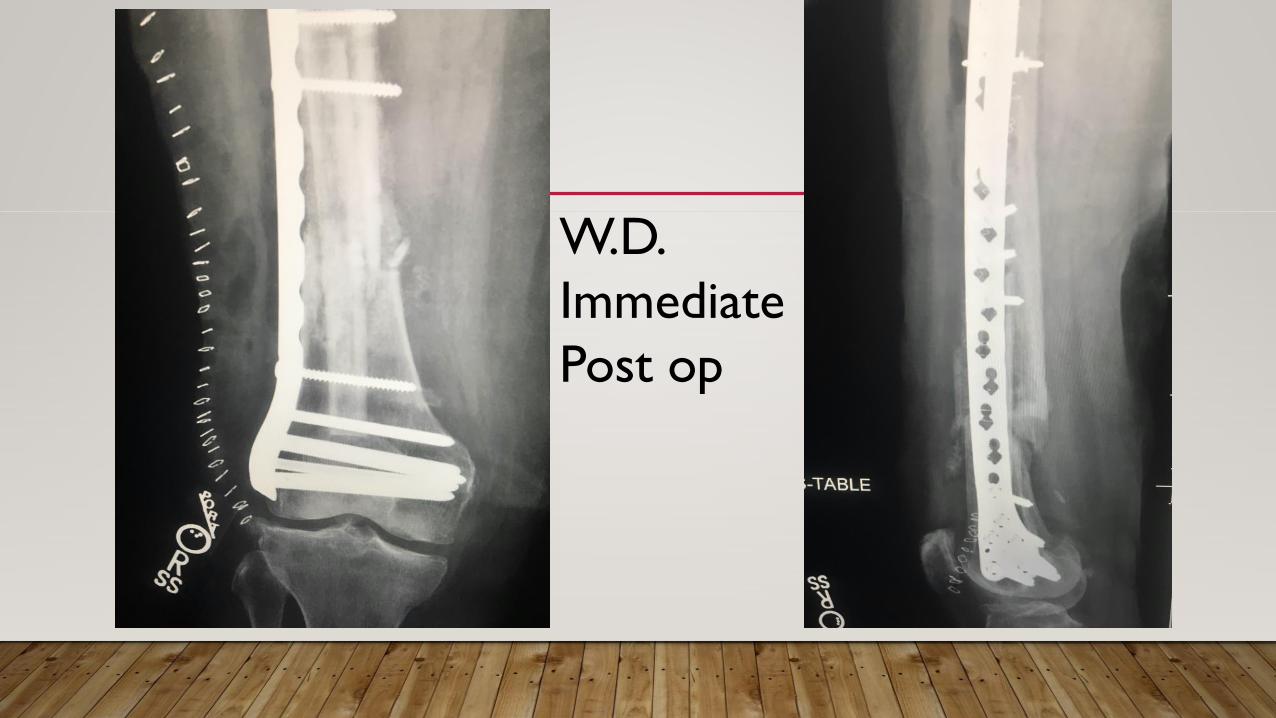
W.D.
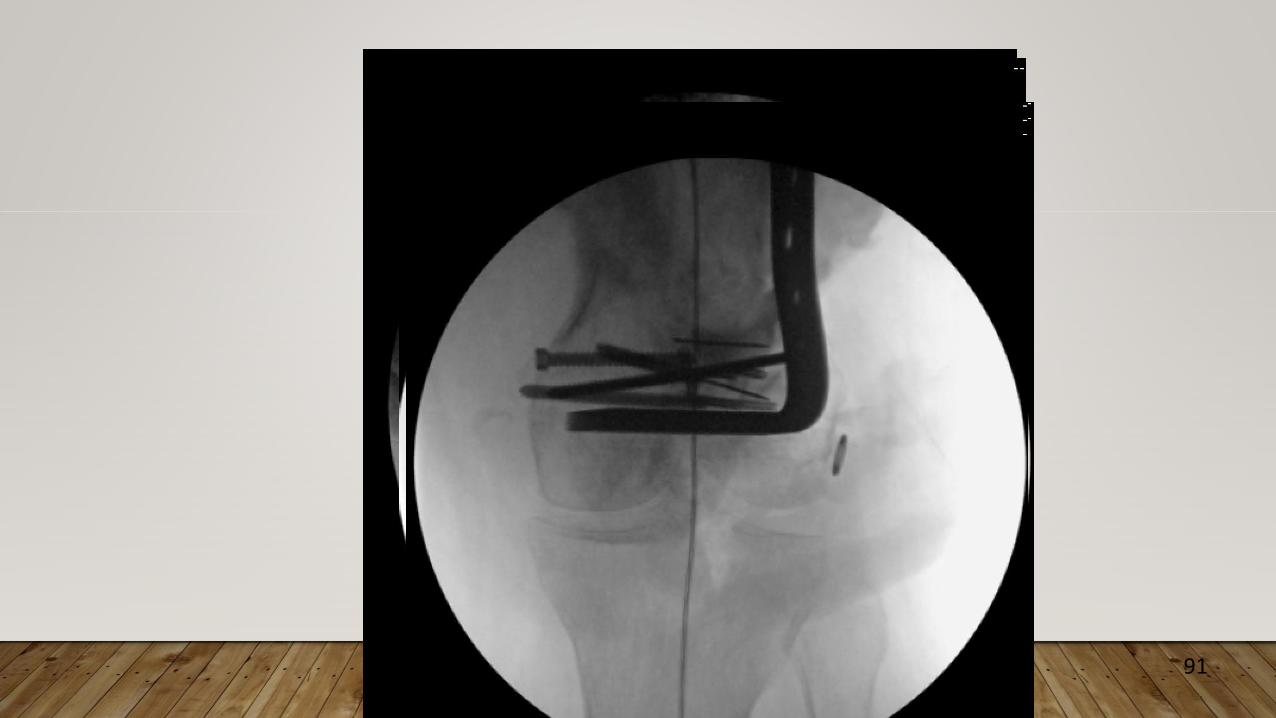
Immediate
Post op
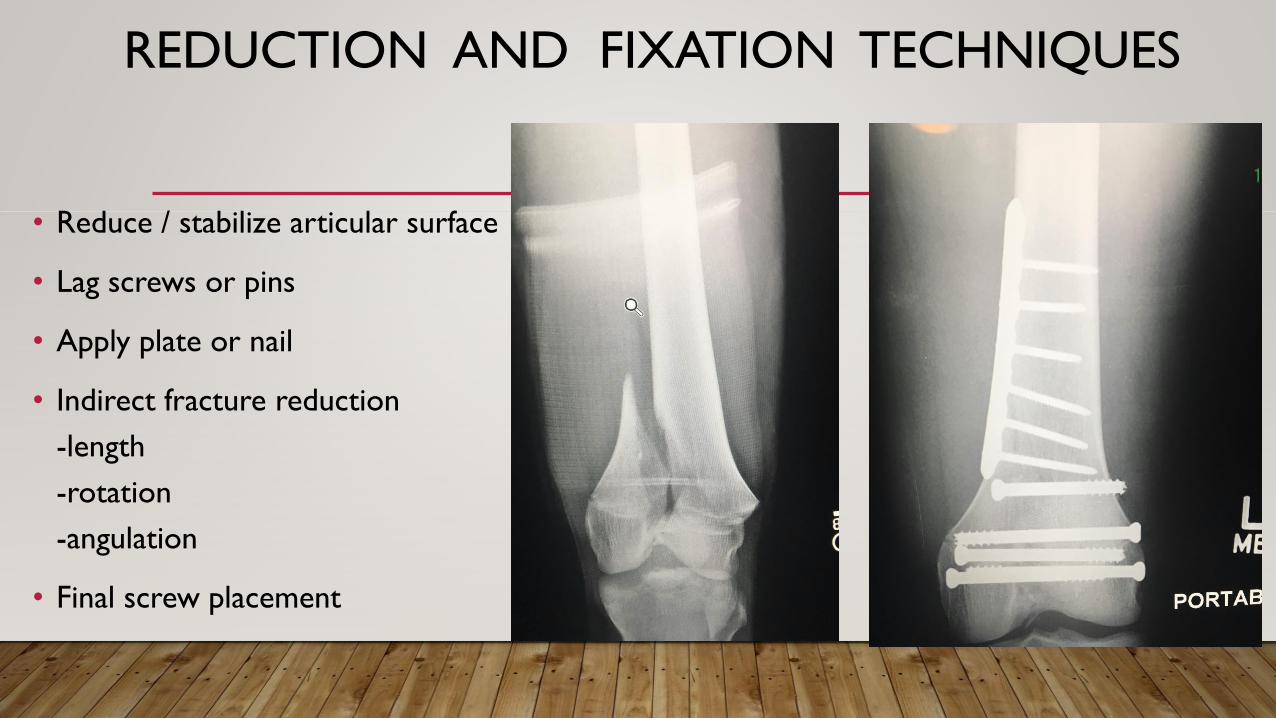
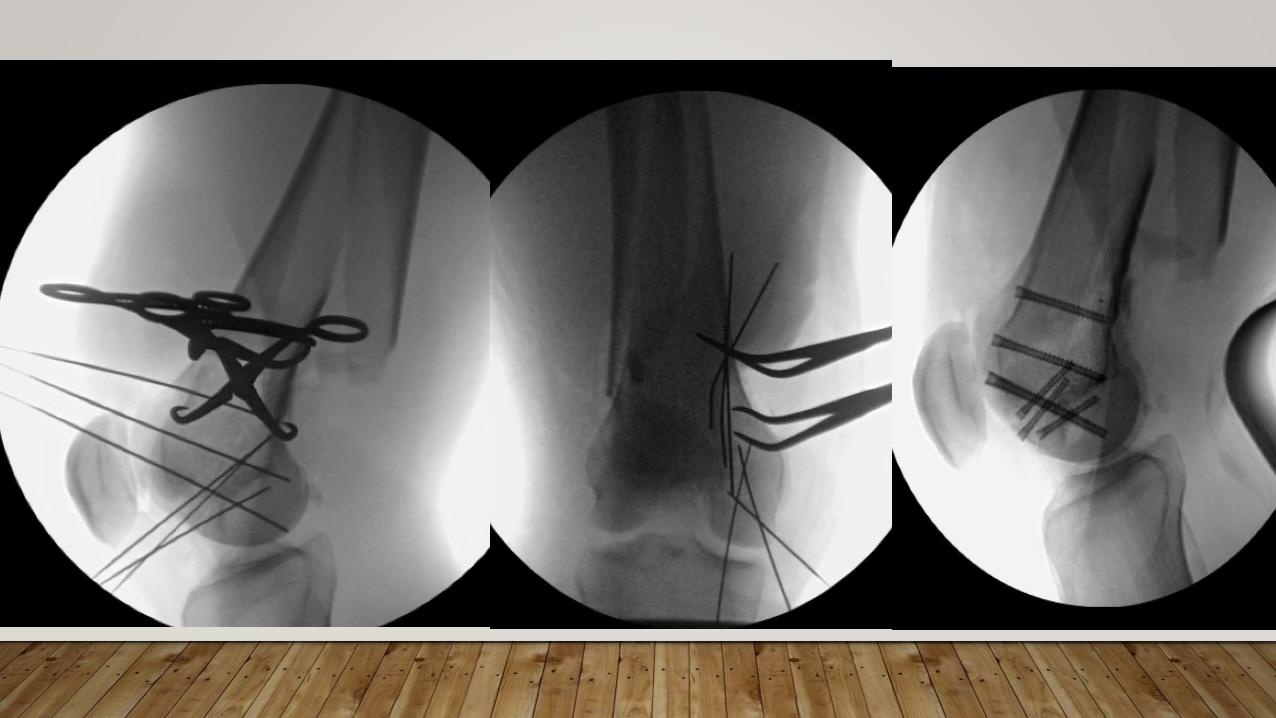
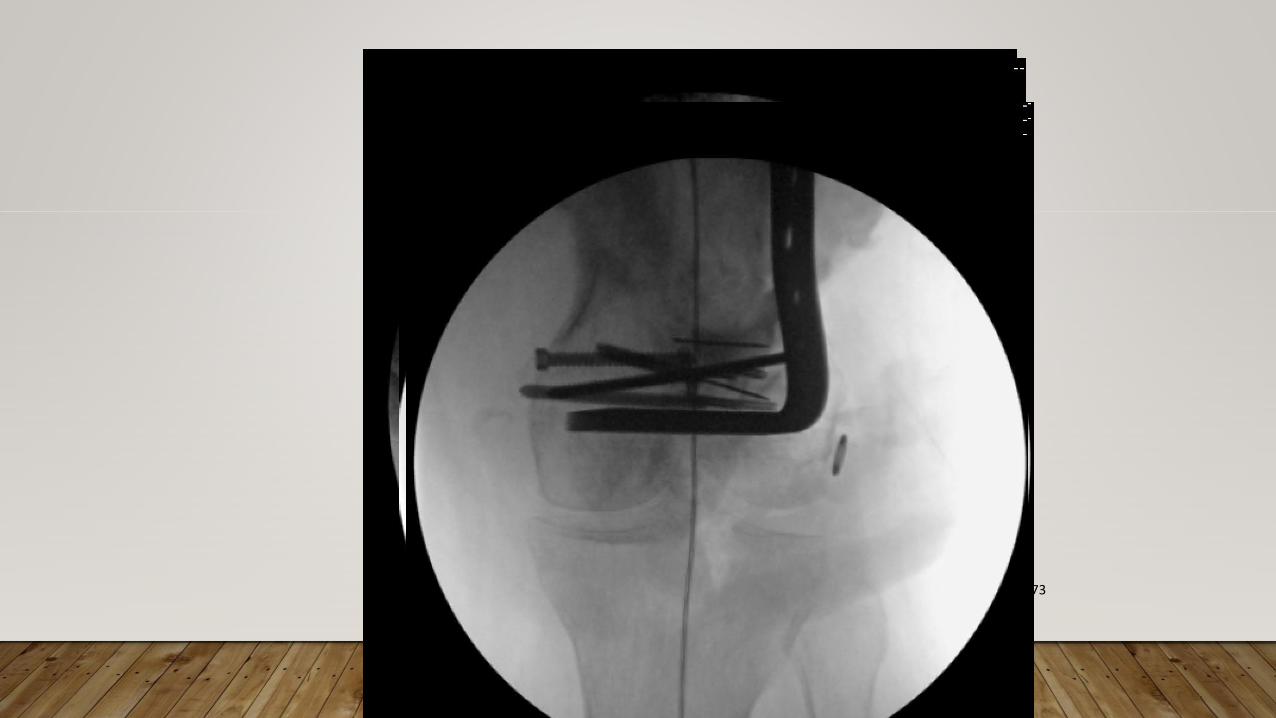
REDUCTION AND FIXATION TECHNIQUES
• Reduce / stabilize articular surface
• Lag screws or pins
• Apply plate or nail
• Indirect fracture reduction
-length
-rotation
-angulation
• Final screw placement
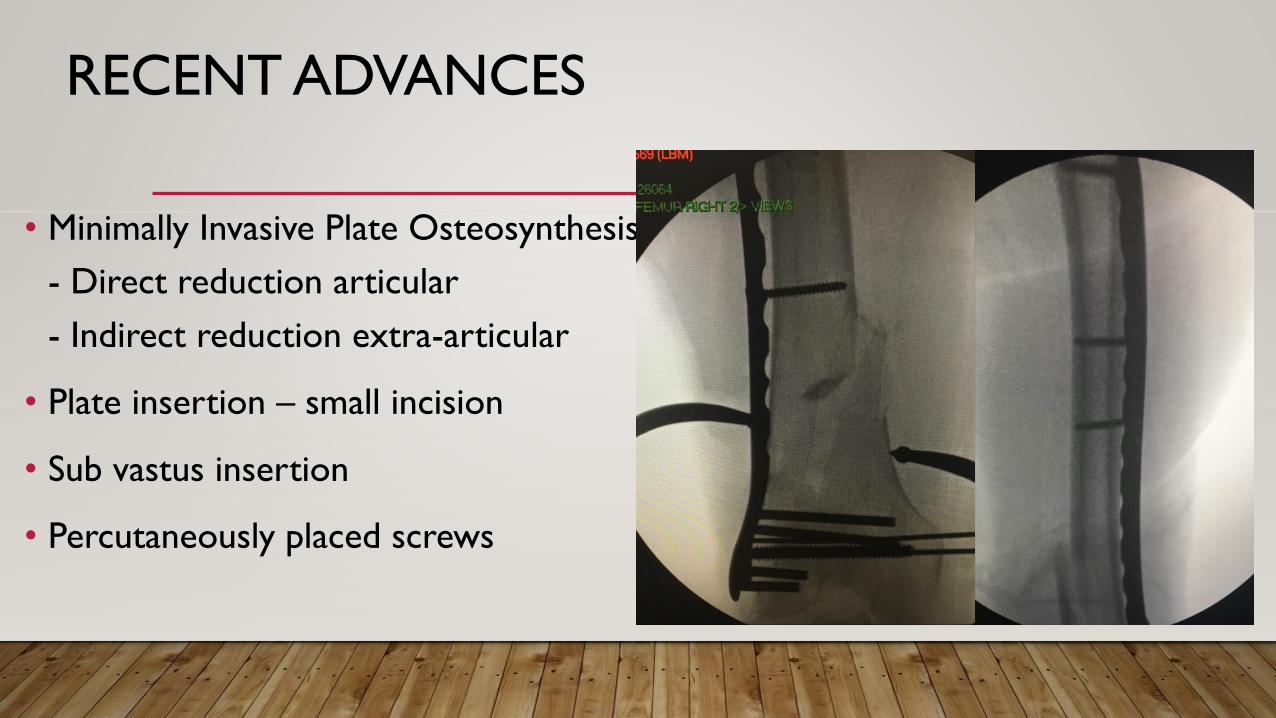
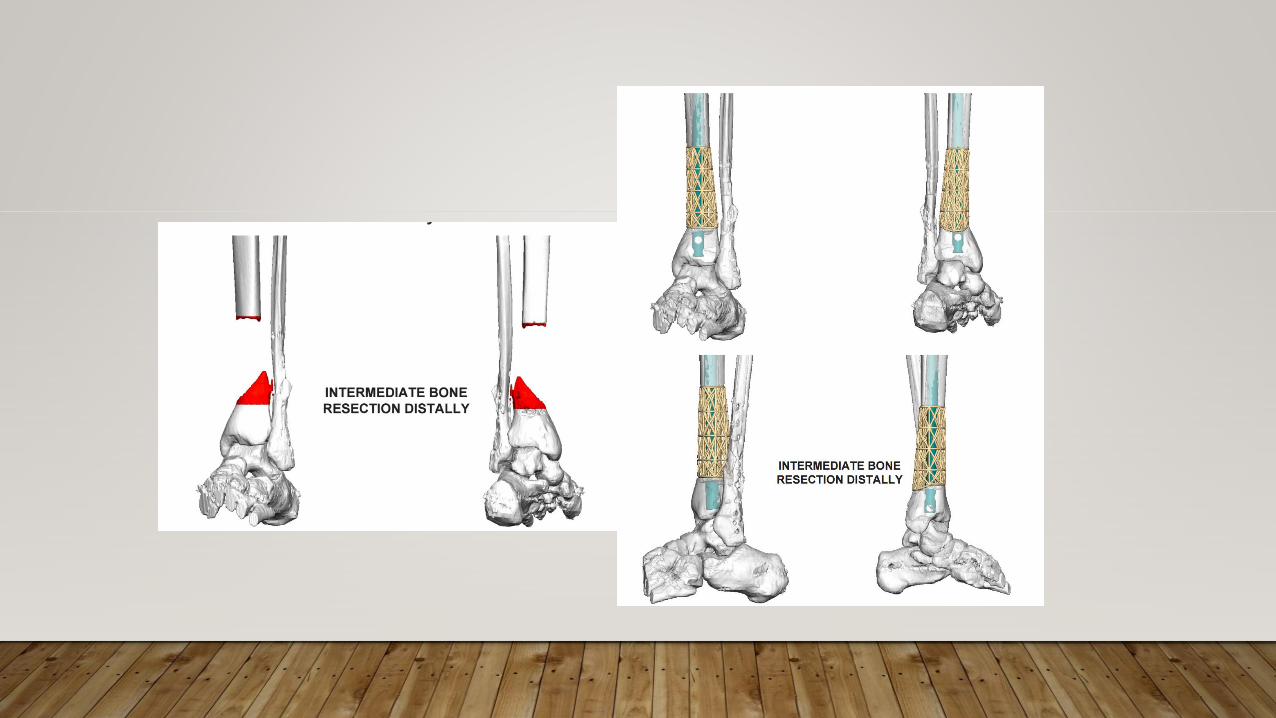
RECENT ADVANCES
• Minimally Invasive Plate Osteosynthesis
- Direct reduction articular
- Indirect reduction extra-articular
• Plate insertion – small incision
• Sub vastus insertion
• Percutaneously placed screws
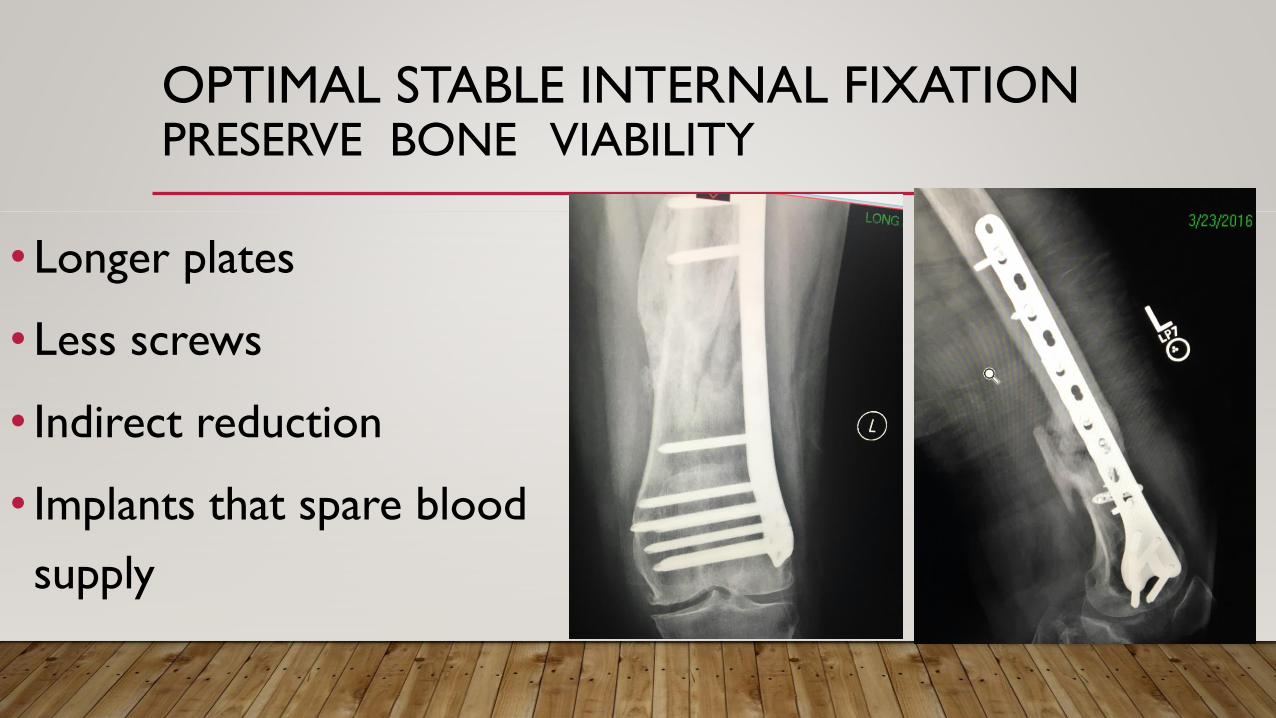
OPTIMAL STABLE INTERNAL FIXATIONPRESERVE BONE VIABILITY
• Longer plates
• Less screws
• Indirect reduction
• Implants that spare blood
supply
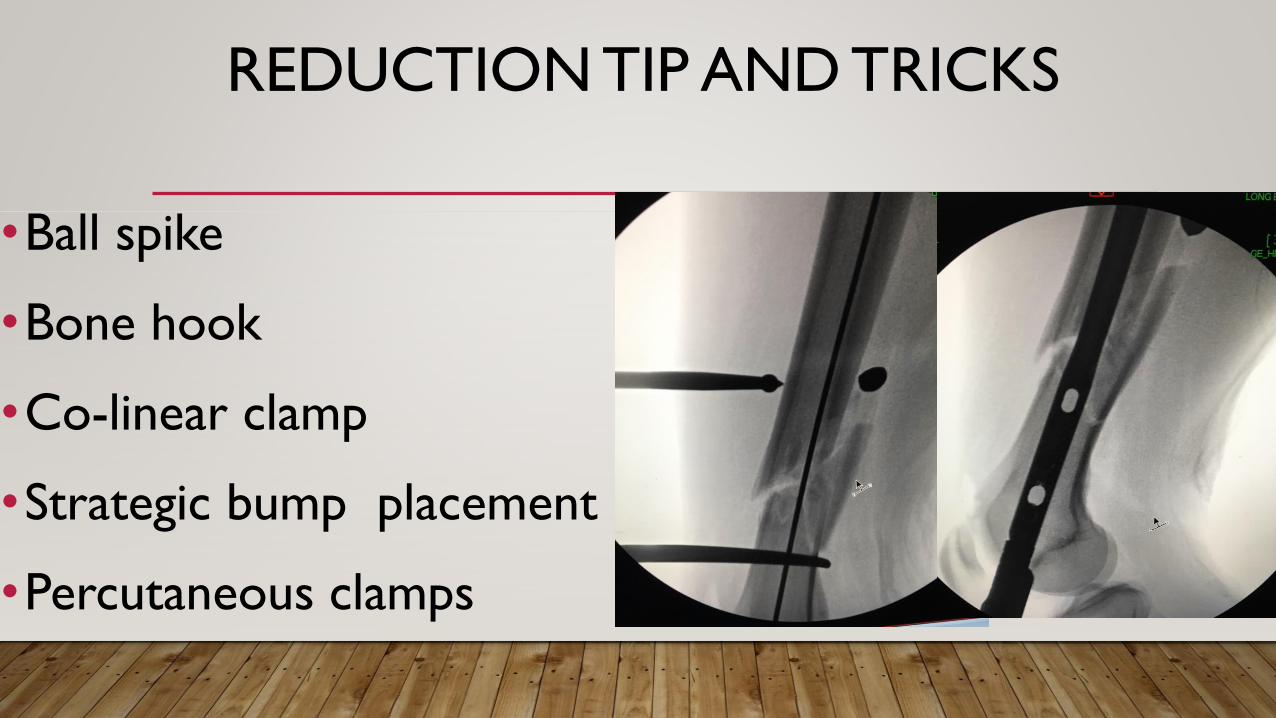
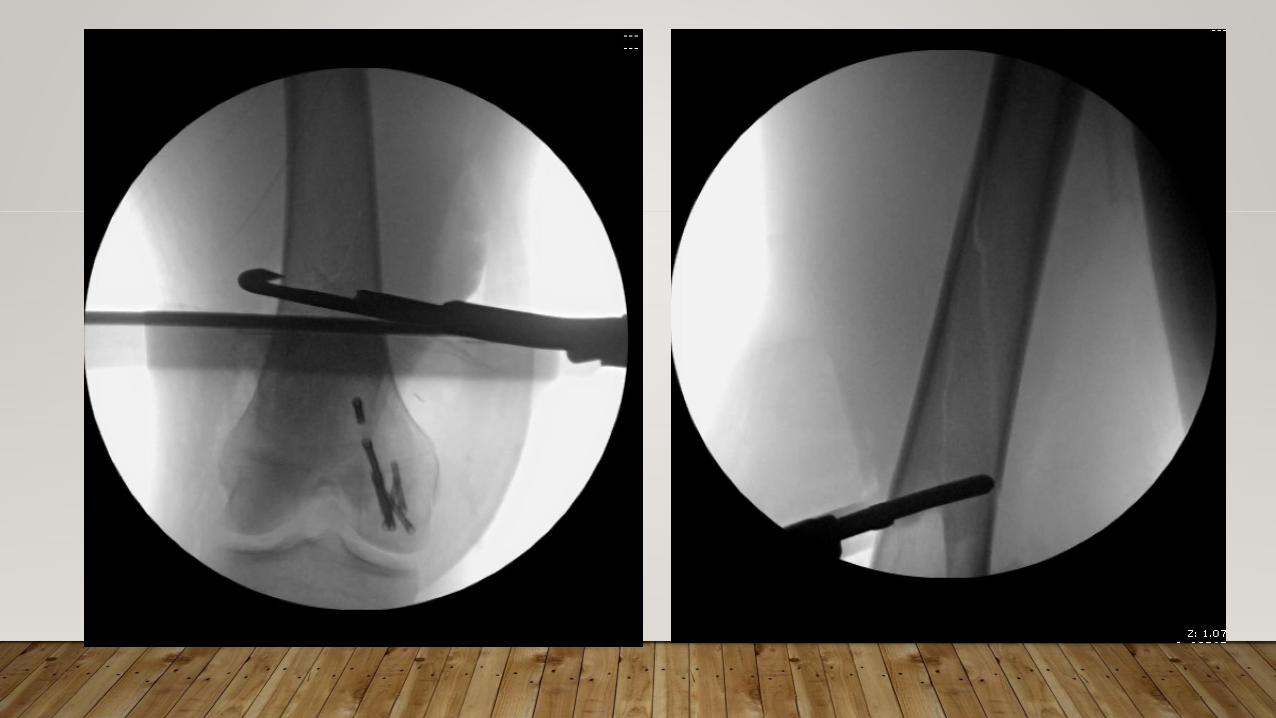
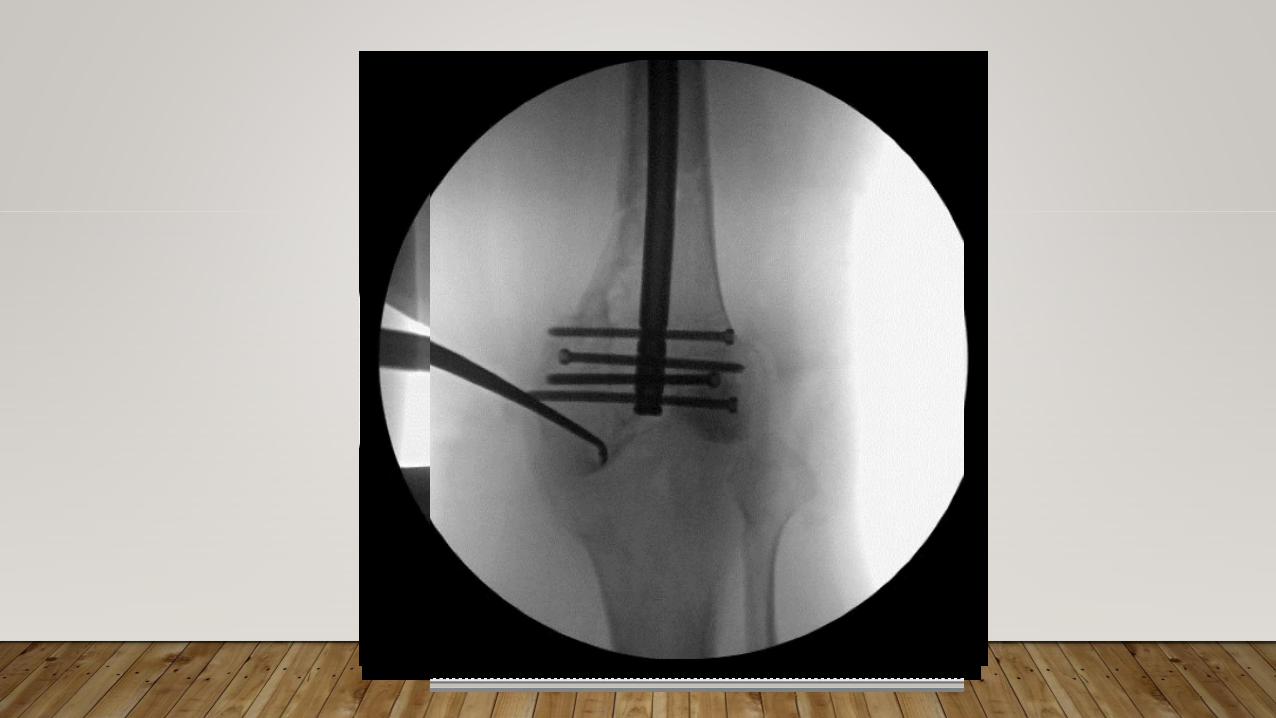
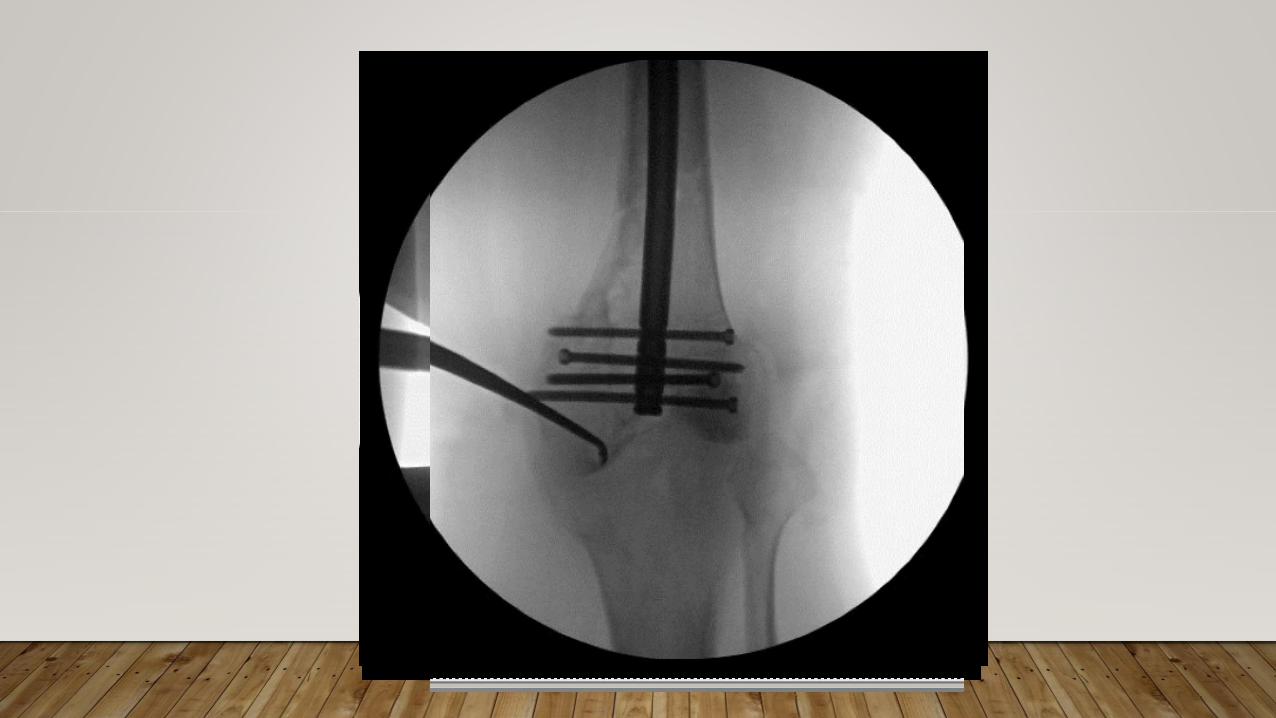
REDUCTION TIP AND TRICKS
•Ball spike
•Bone hook
•Co-linear clamp
•Strategic bump placement
•Percutaneous clamps
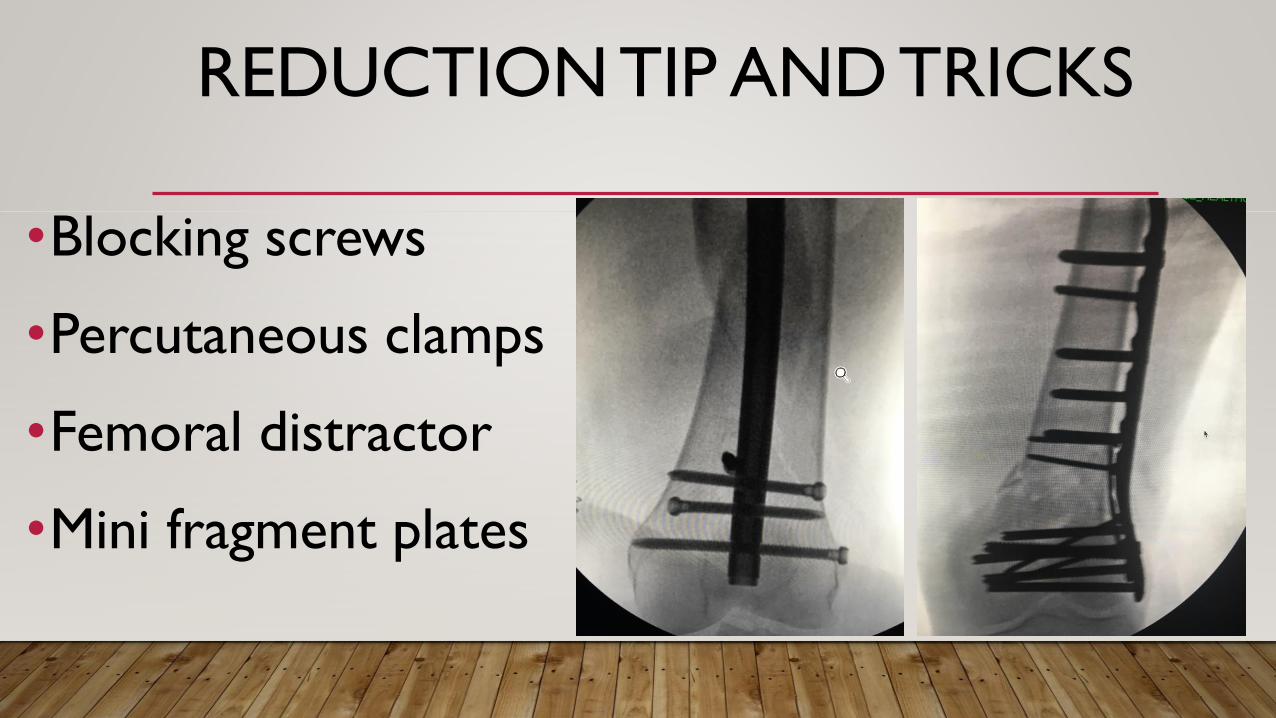
REDUCTION TIP AND TRICKS
•Blocking screws
•Percutaneous clamps
•Femoral distractor
•Mini fragment plates
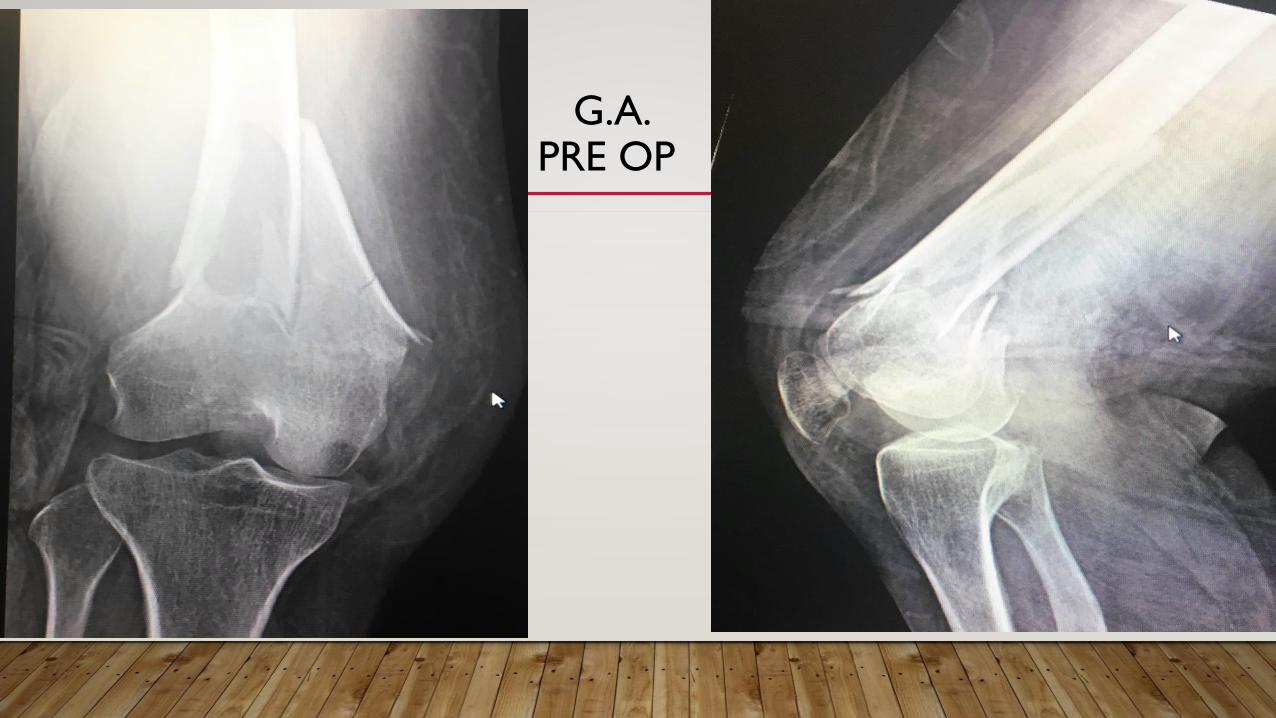
G.A.PRE OP

G.A. POST OP
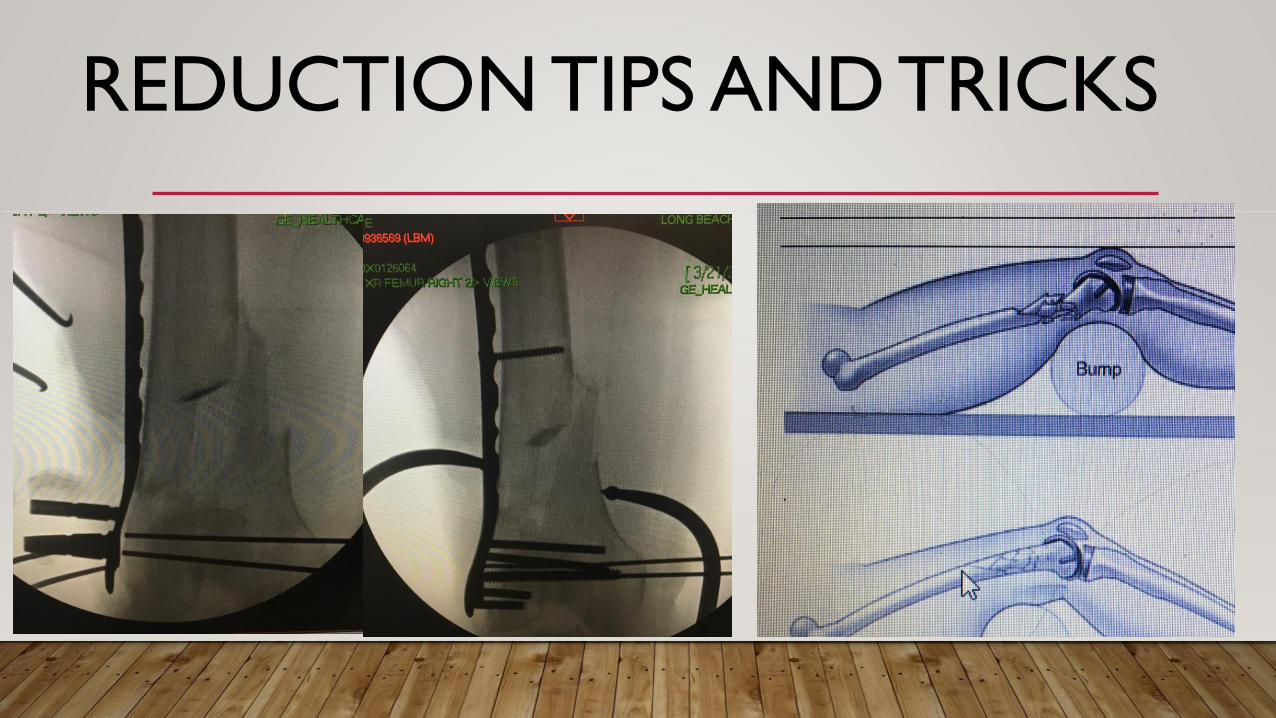
REDUCTION TIPS AND TRICKS
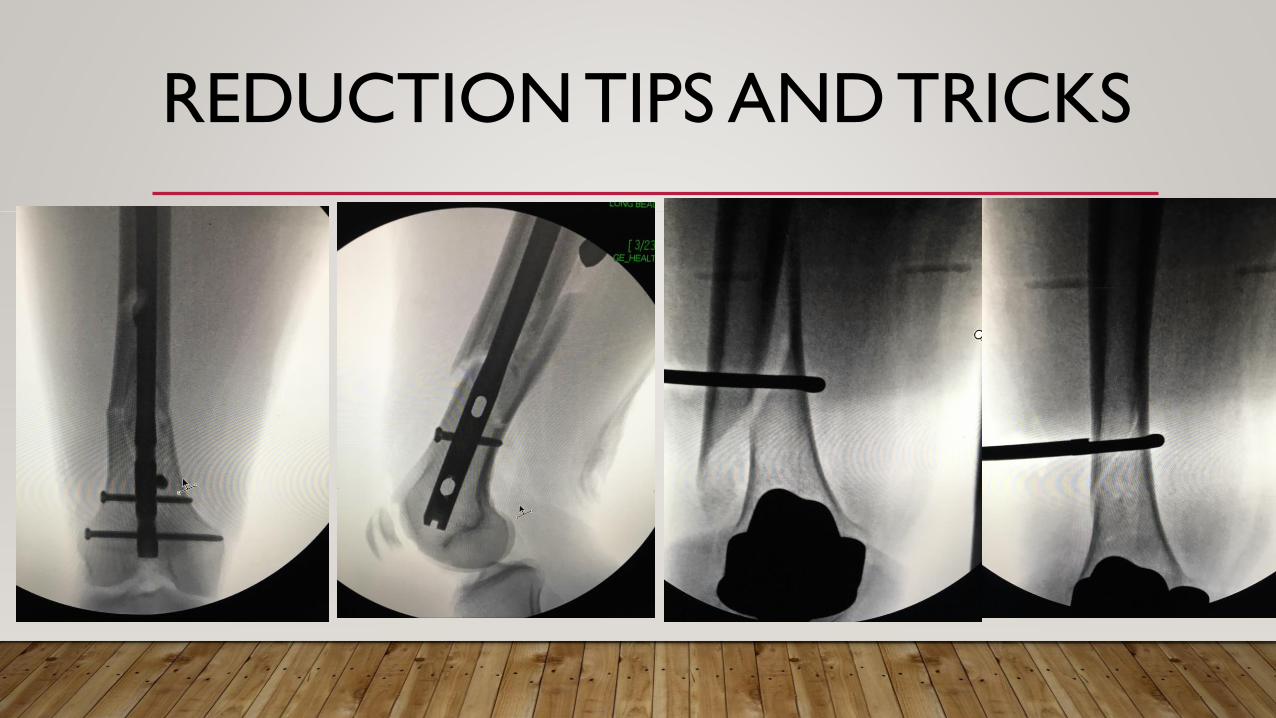
REDUCTION TIPS AND TRICKS
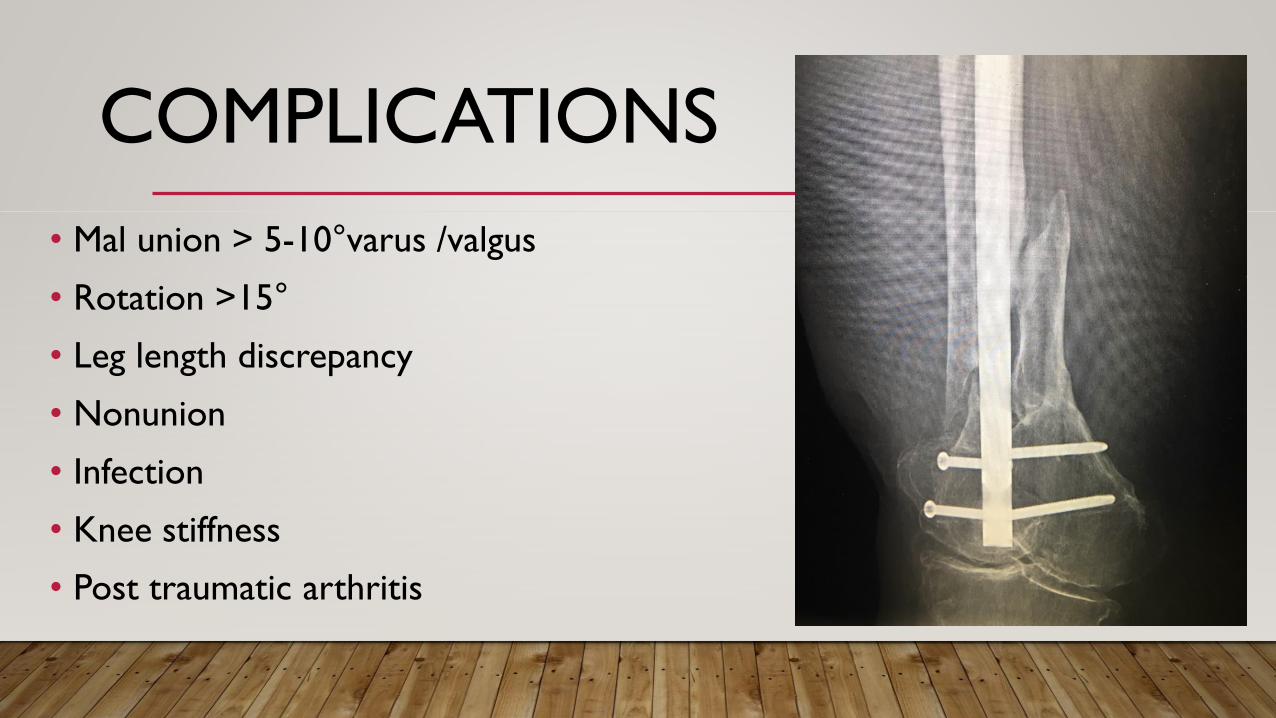
COMPLICATIONS
• Mal union > 5-10°varus /valgus
• Rotation >15°
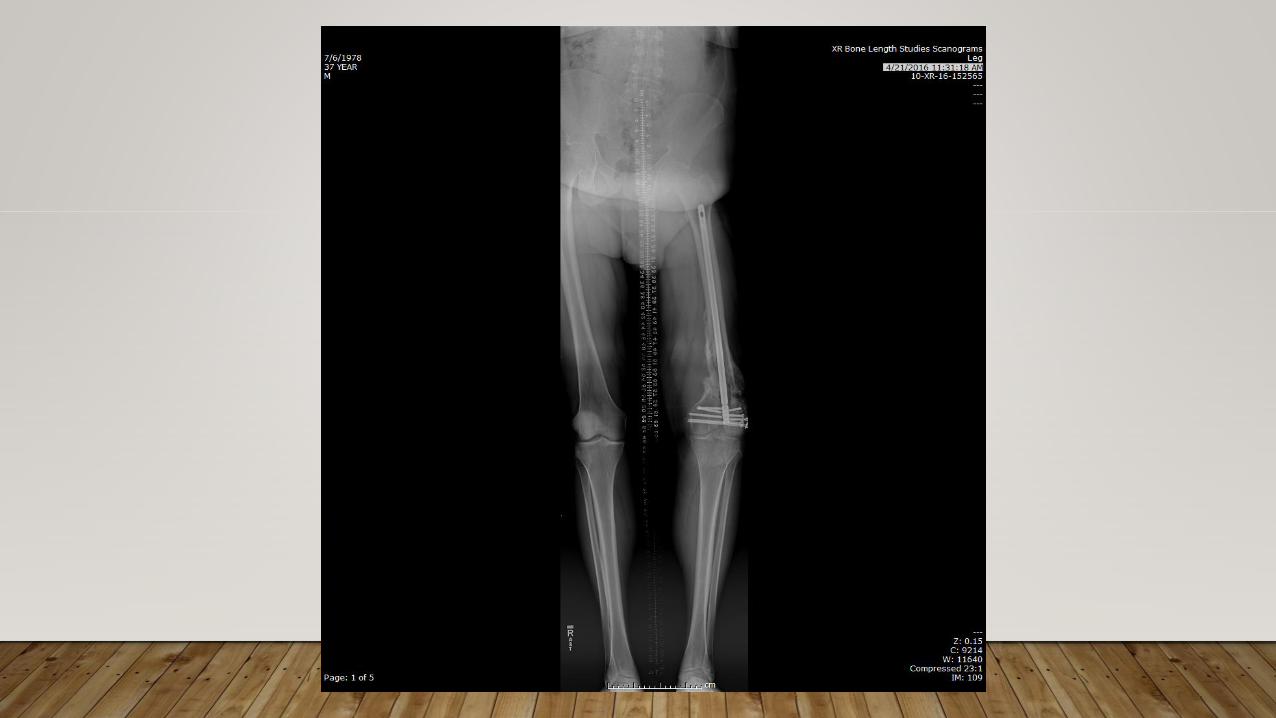
• Leg length discrepancy
• Nonunion
• Infection
• Knee stiffness
• Post traumatic arthritis
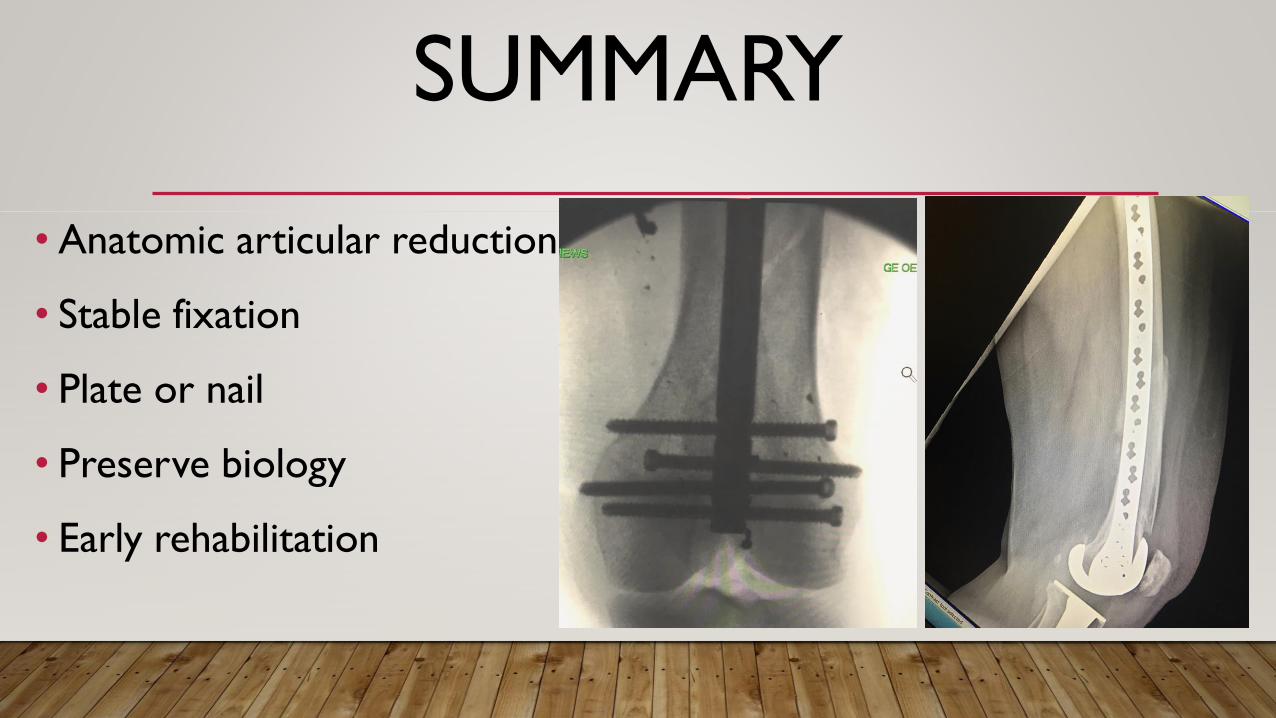
SUMMARY
• Anatomic articular reduction
• Stable fixation
• Plate or nail
• Preserve biology
• Early rehabilitation
THANK YOU
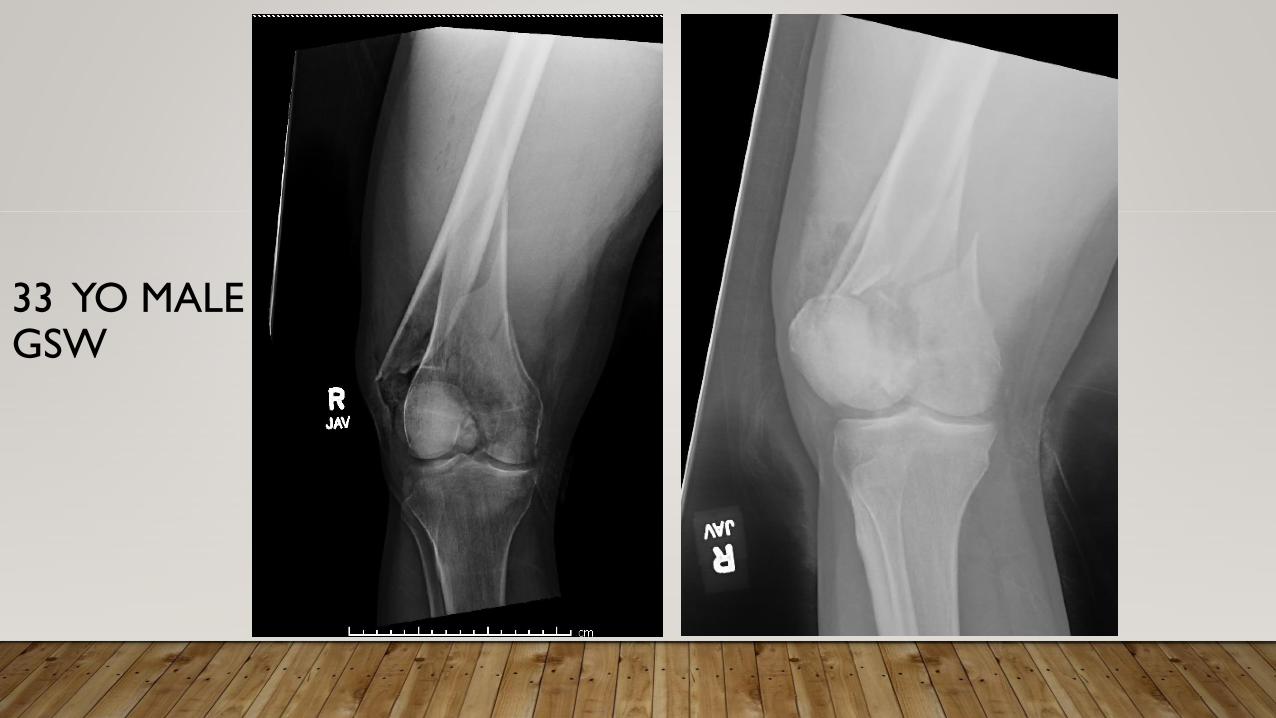
33 YO MALE GSW
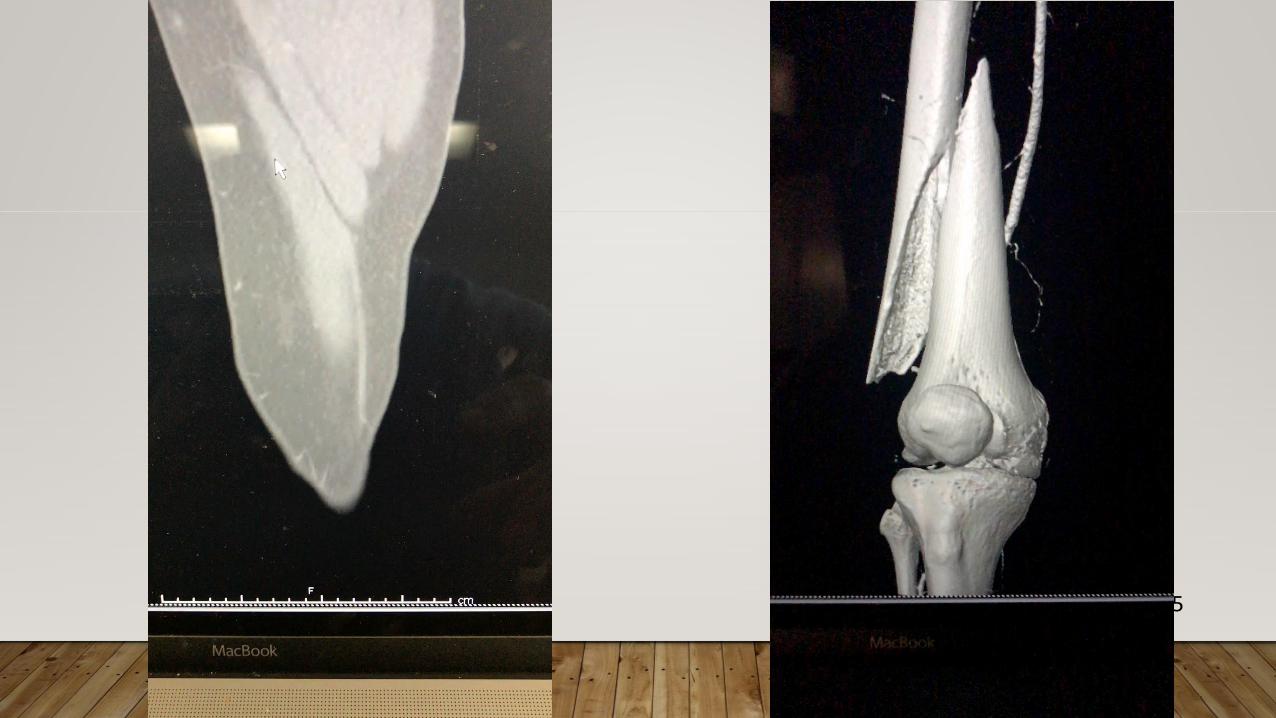
35

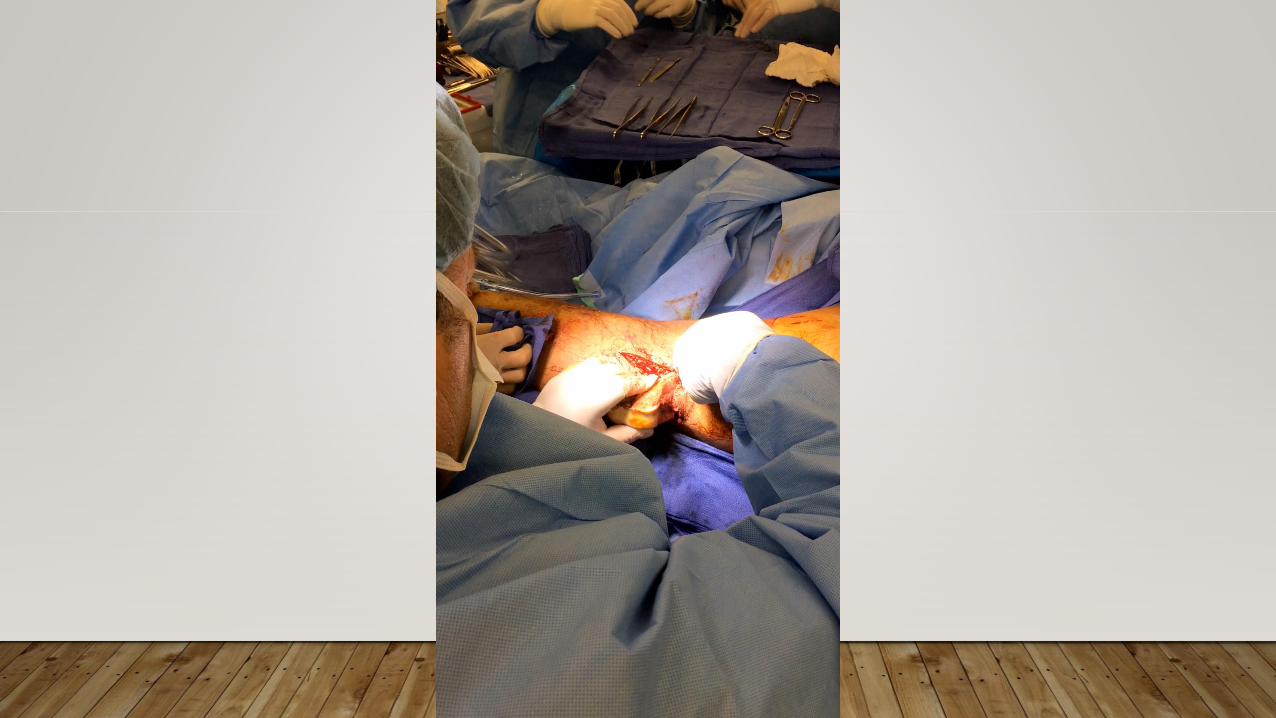
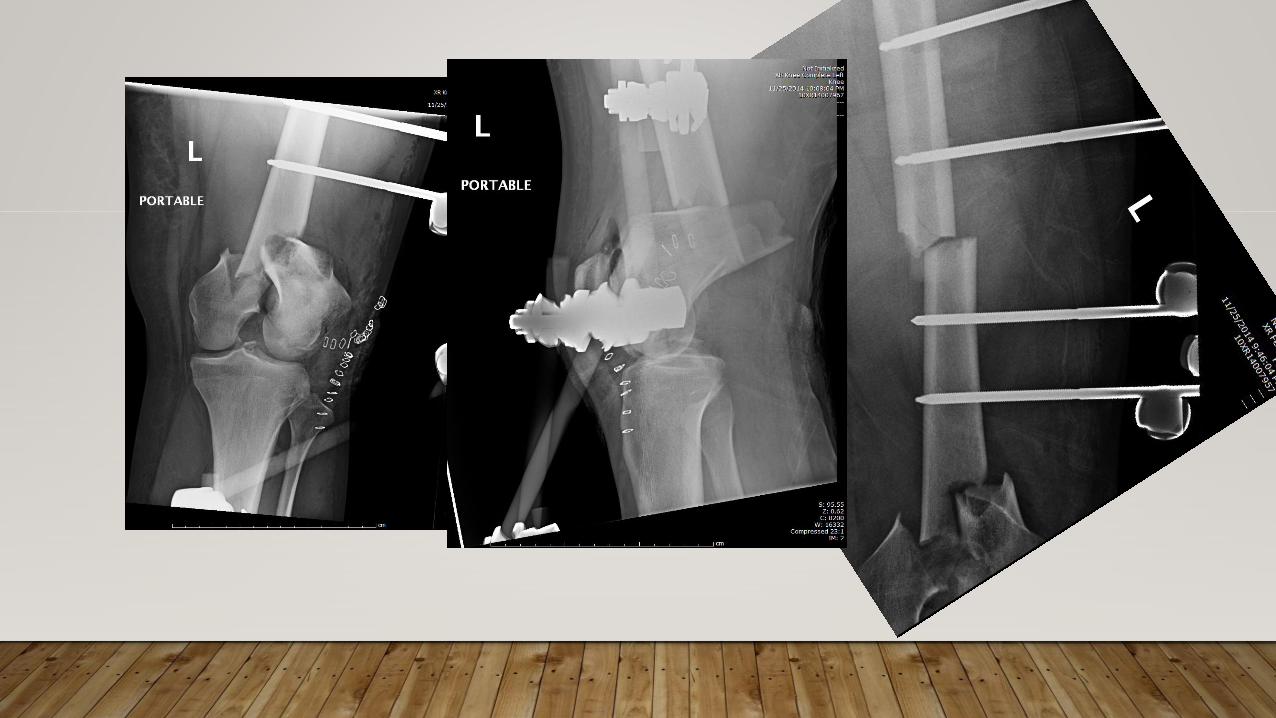
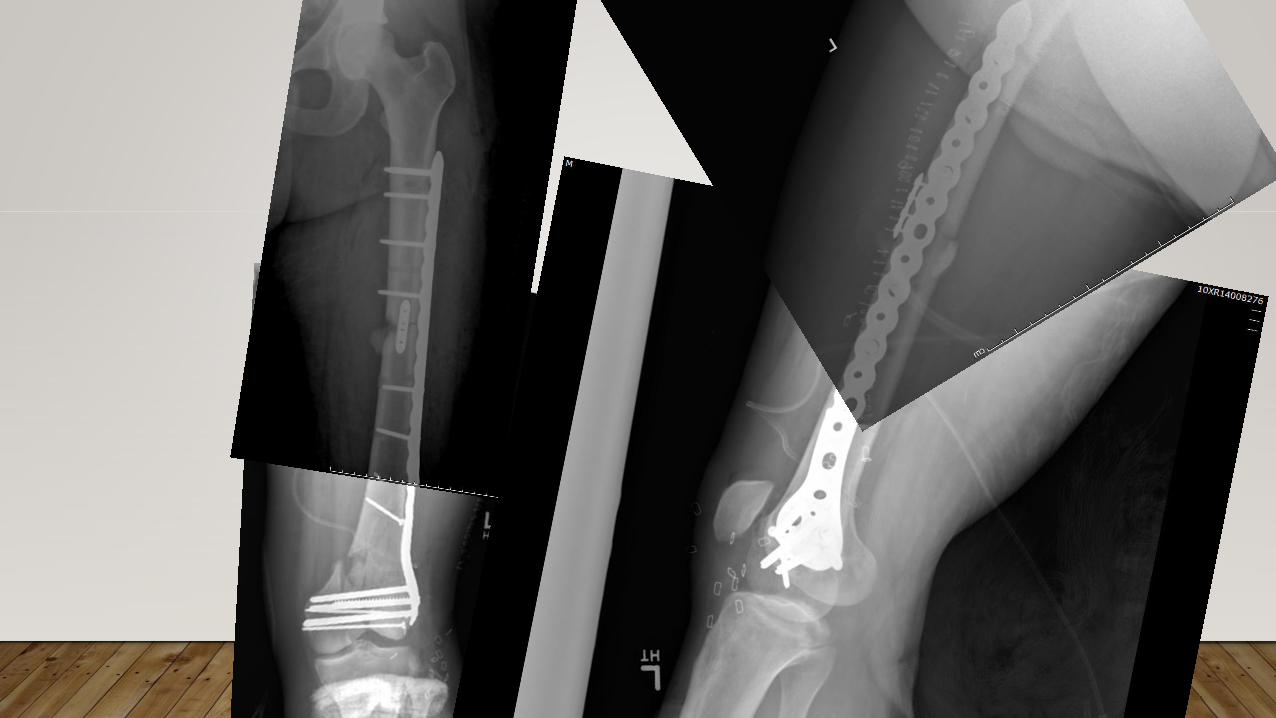
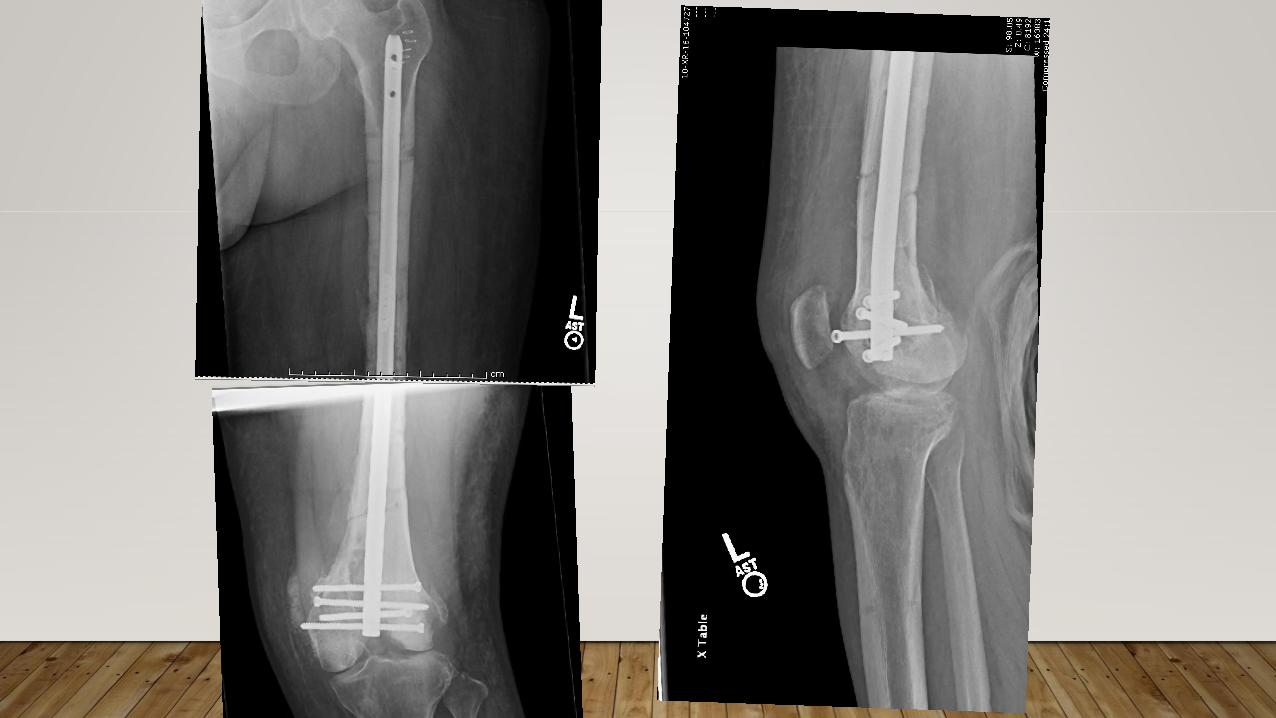
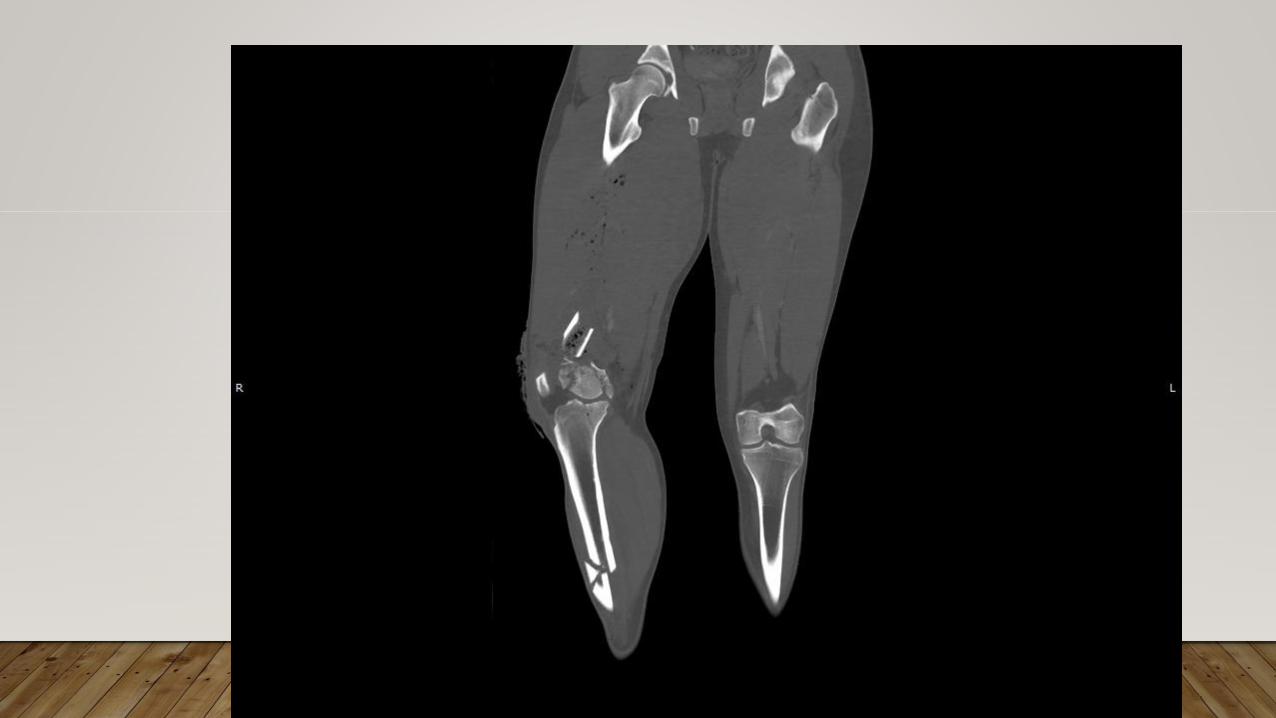
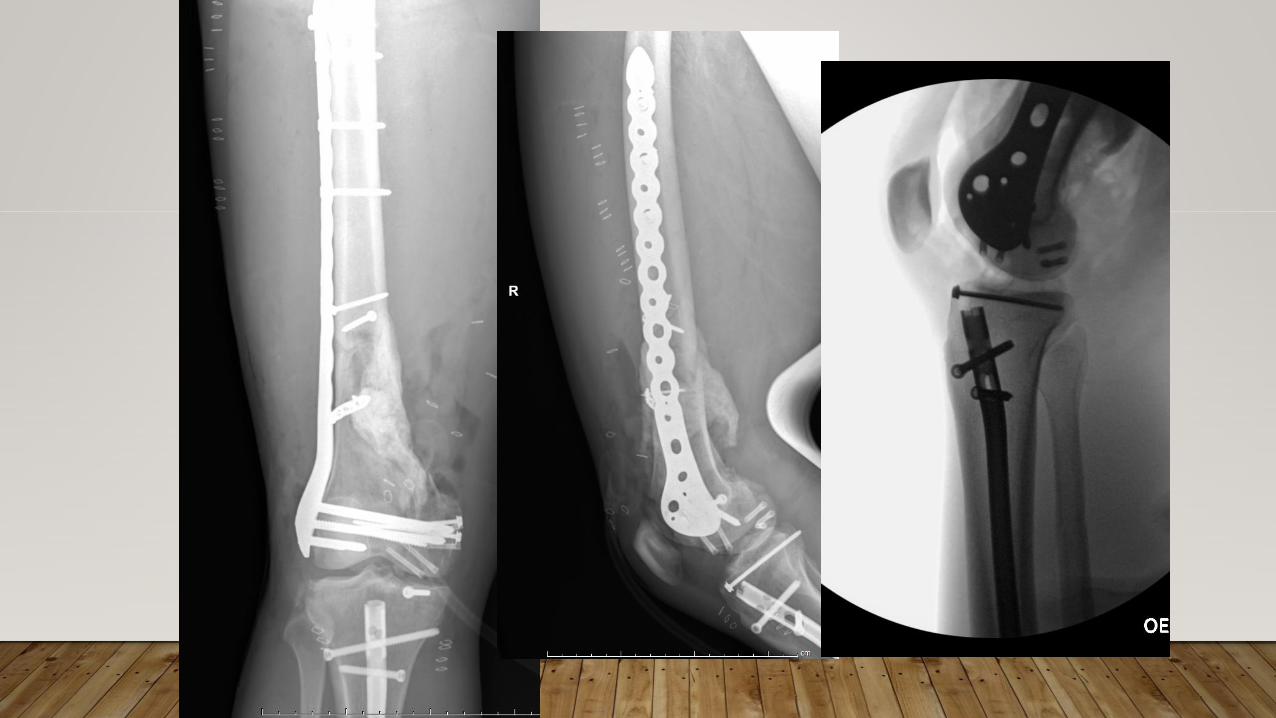
CASE 2
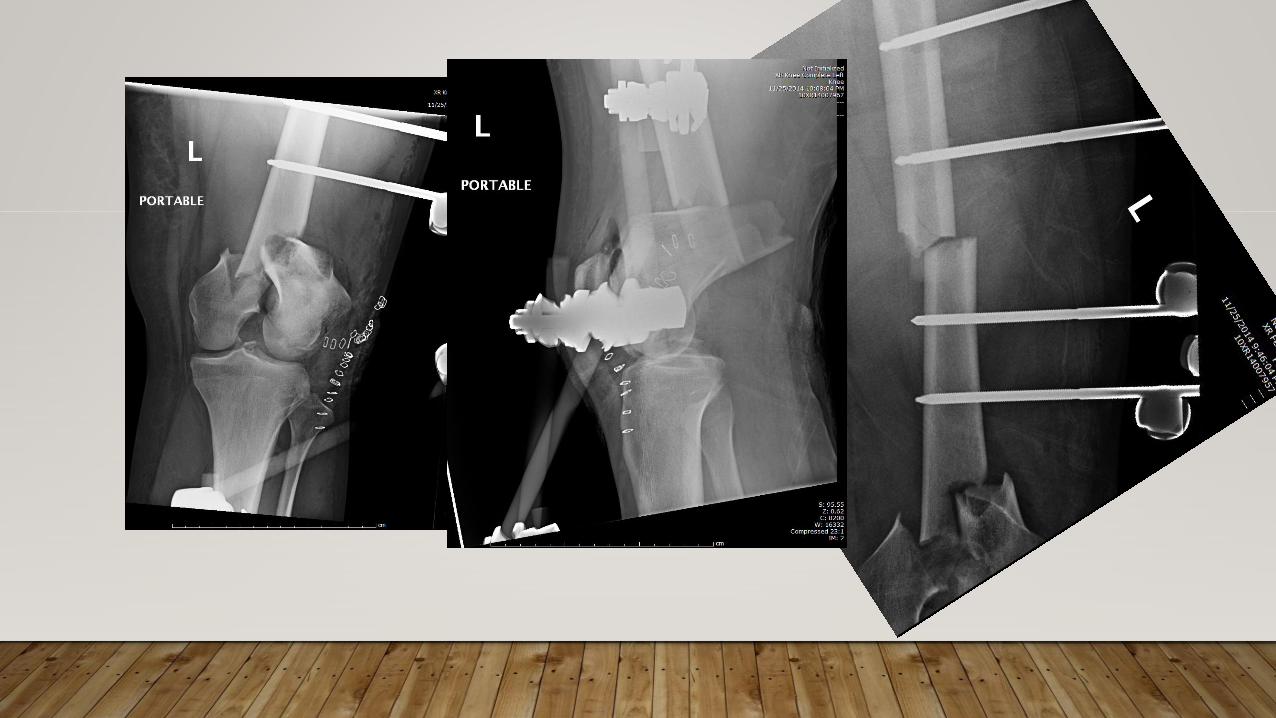
• 23M MCA at 60 MPH
• Open knee injury
• Small subarachnoid hemorrhage
• Hemodynamically stable
• Neurovascular intact



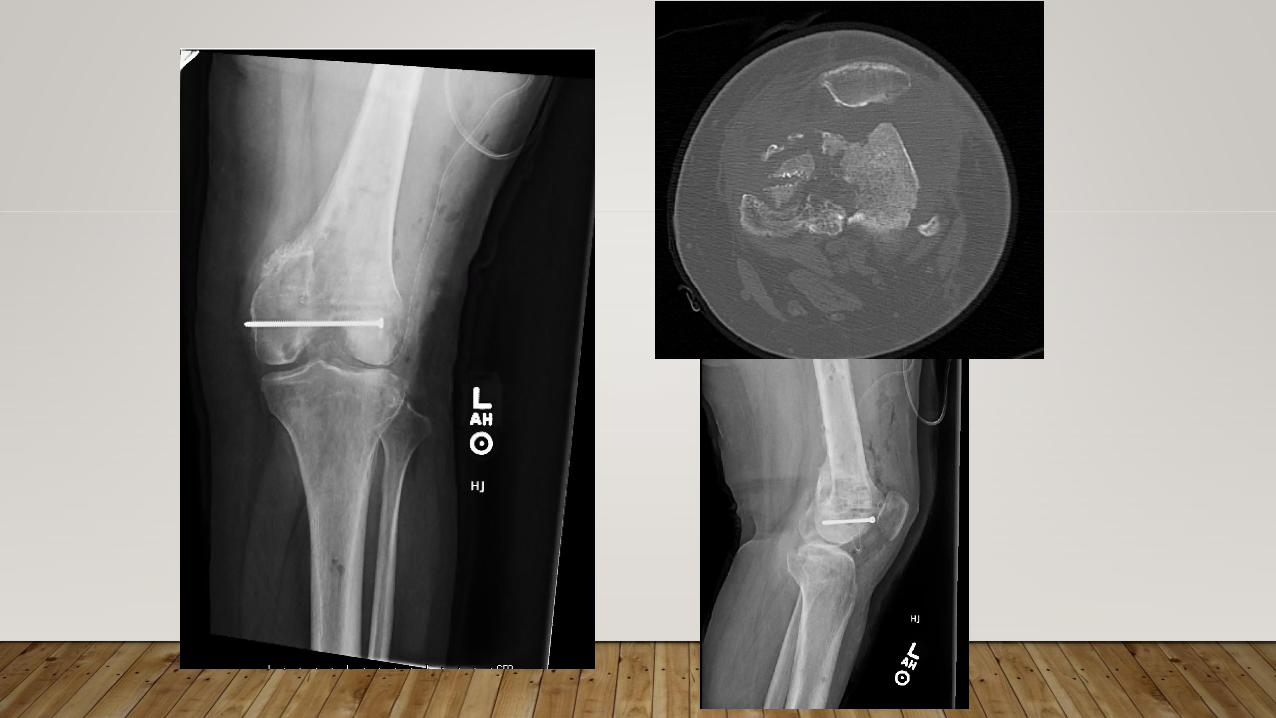
5 months
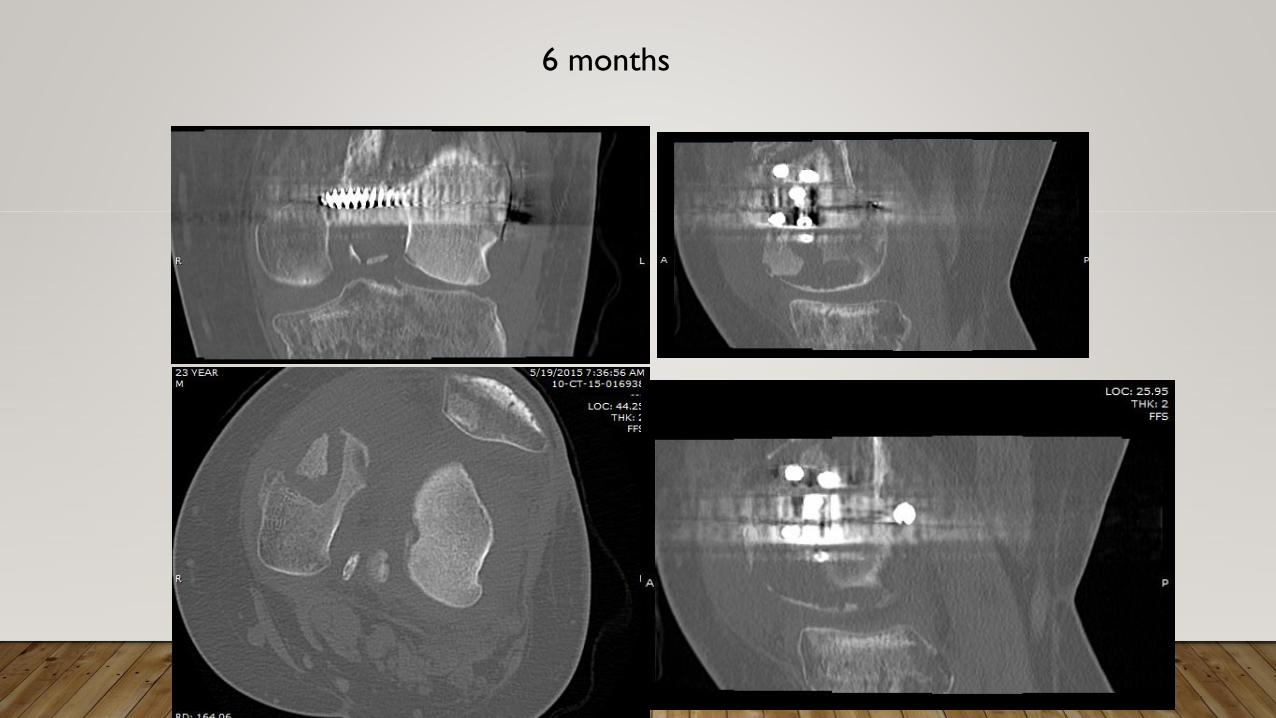
6 months


PUSSES OUT!


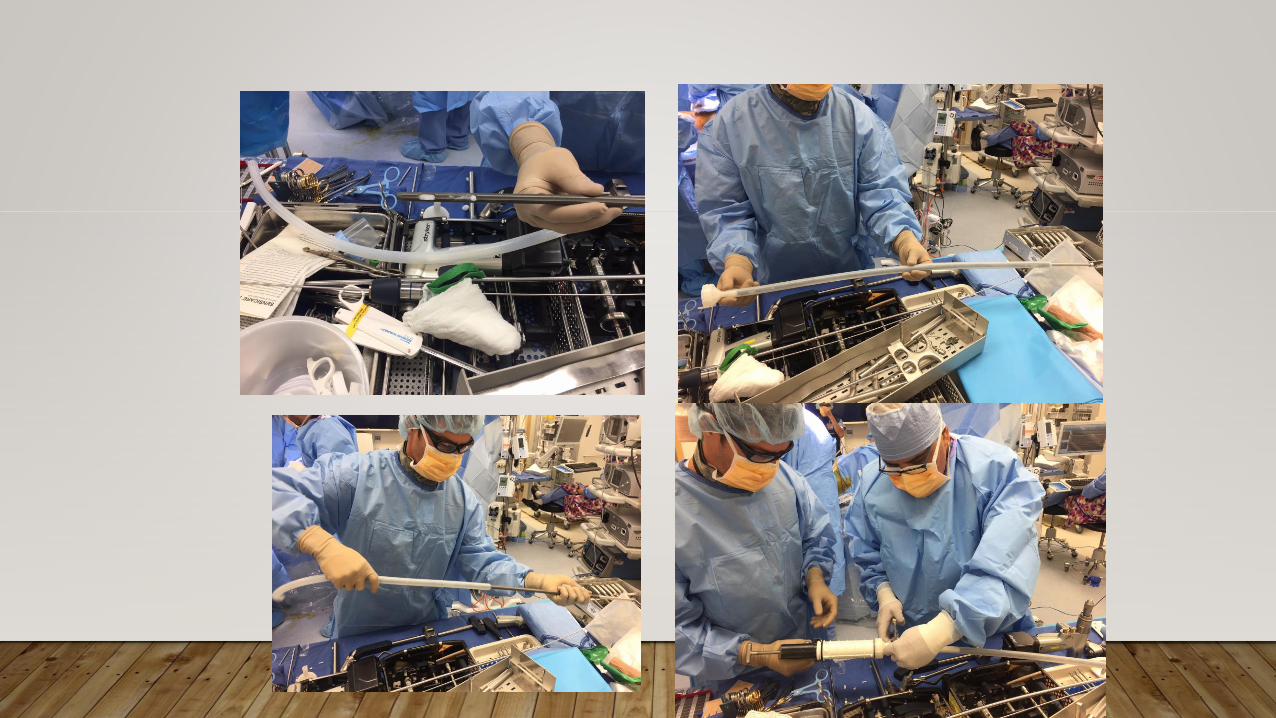
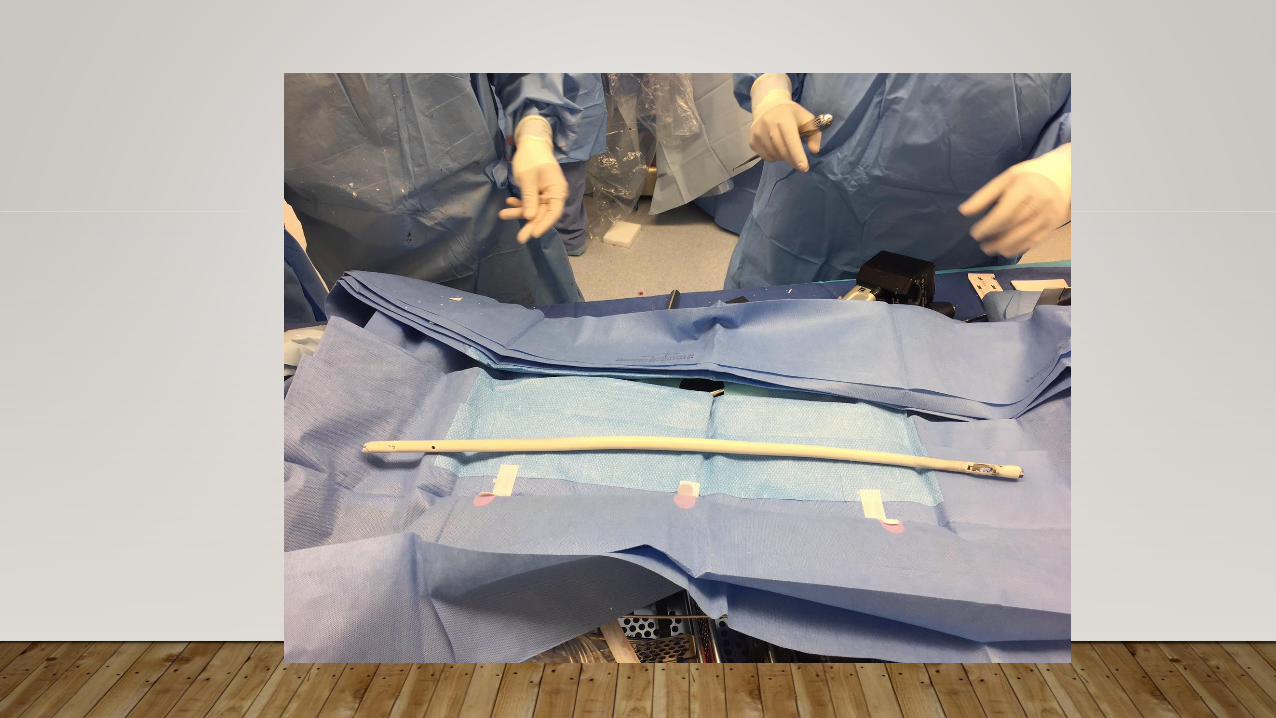
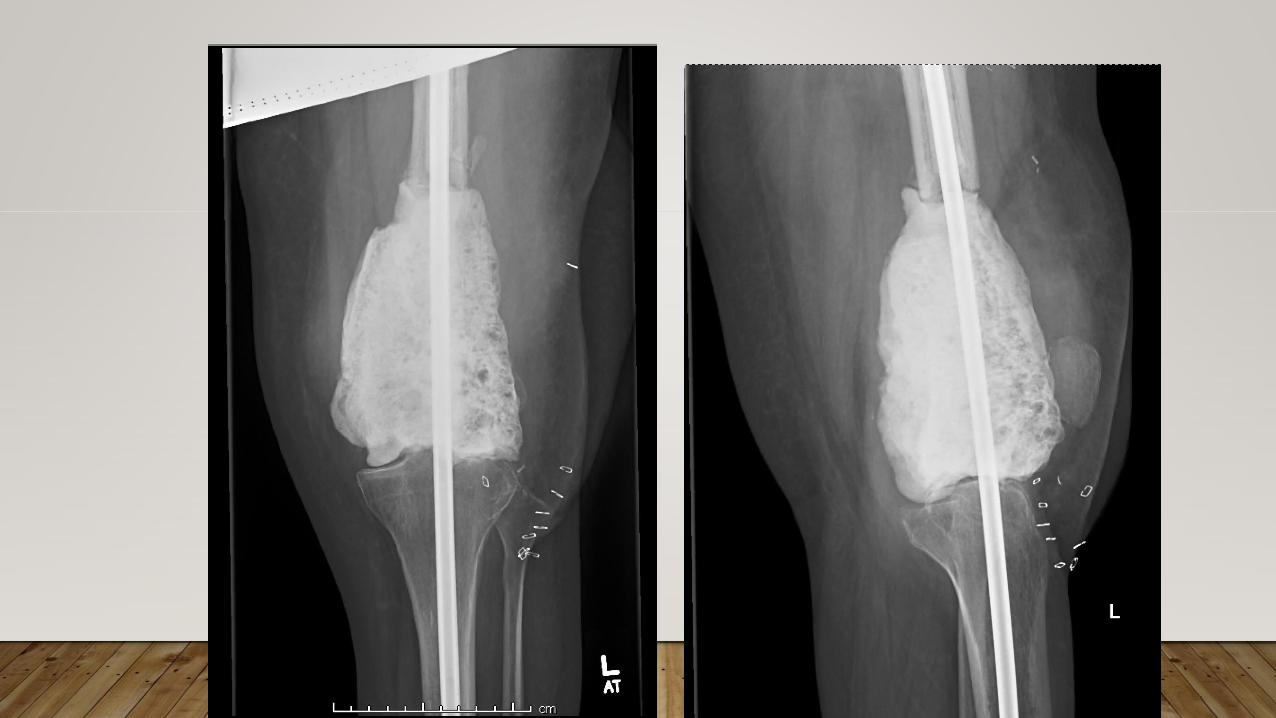
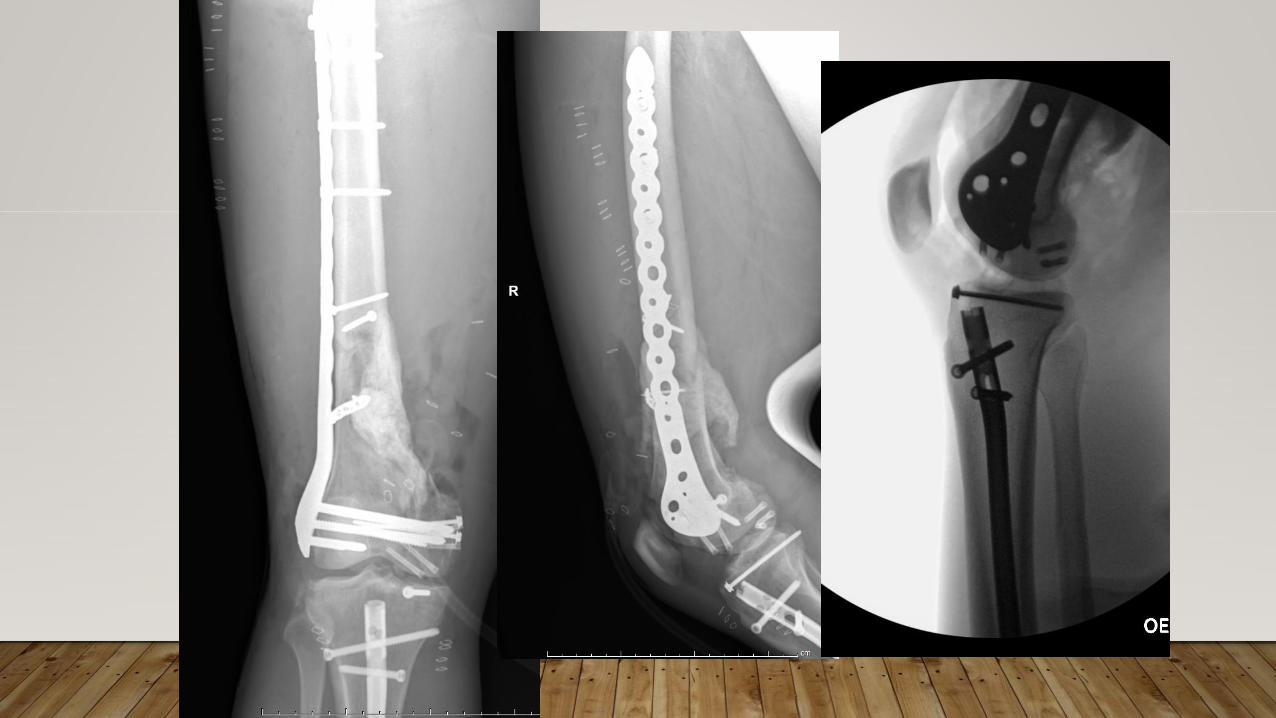
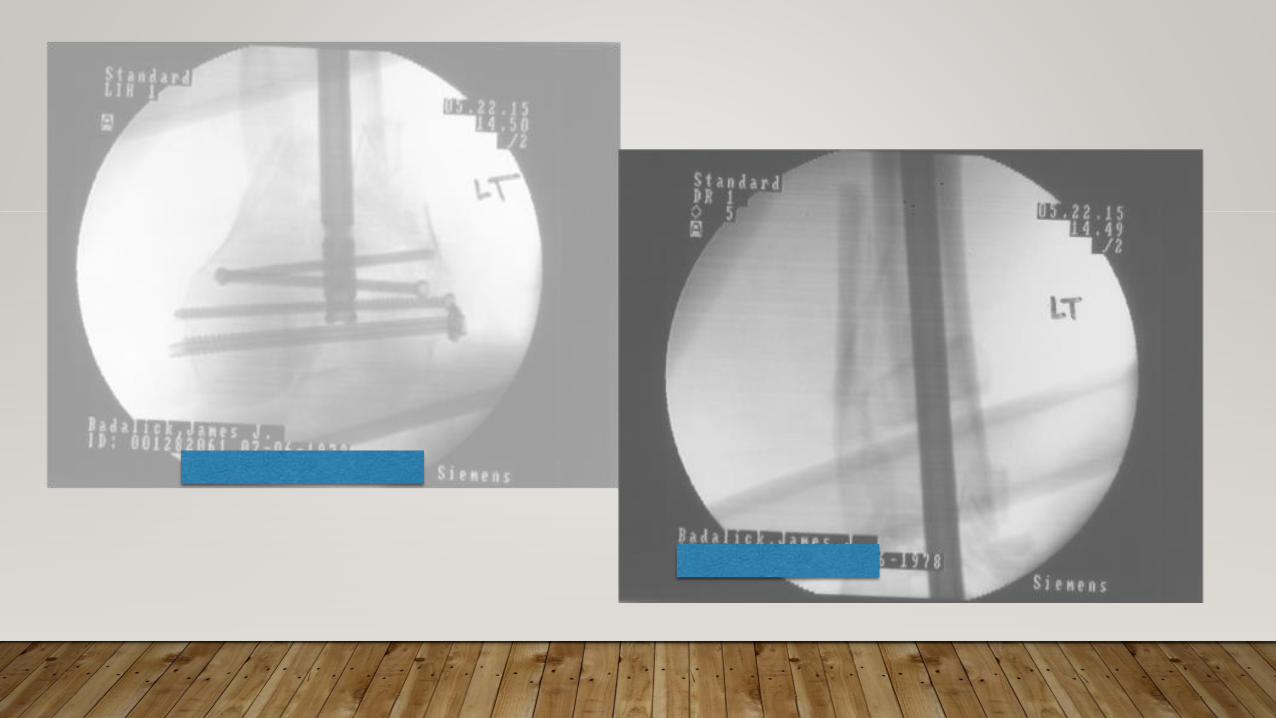
CASE 3
• 20M high speed MCA
• Multiple open fractures RLE
• Rib fractures/pulmonary contusion
• Stable
• Neurovascular exam intact

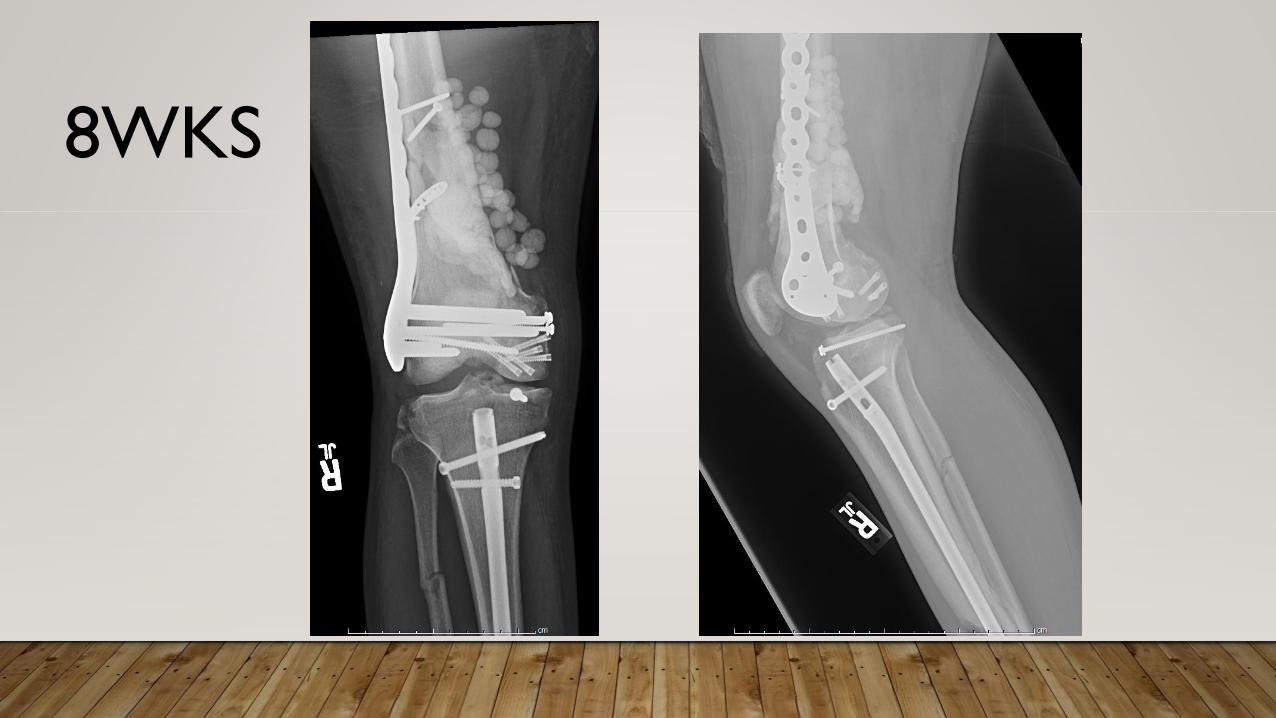
8WKS
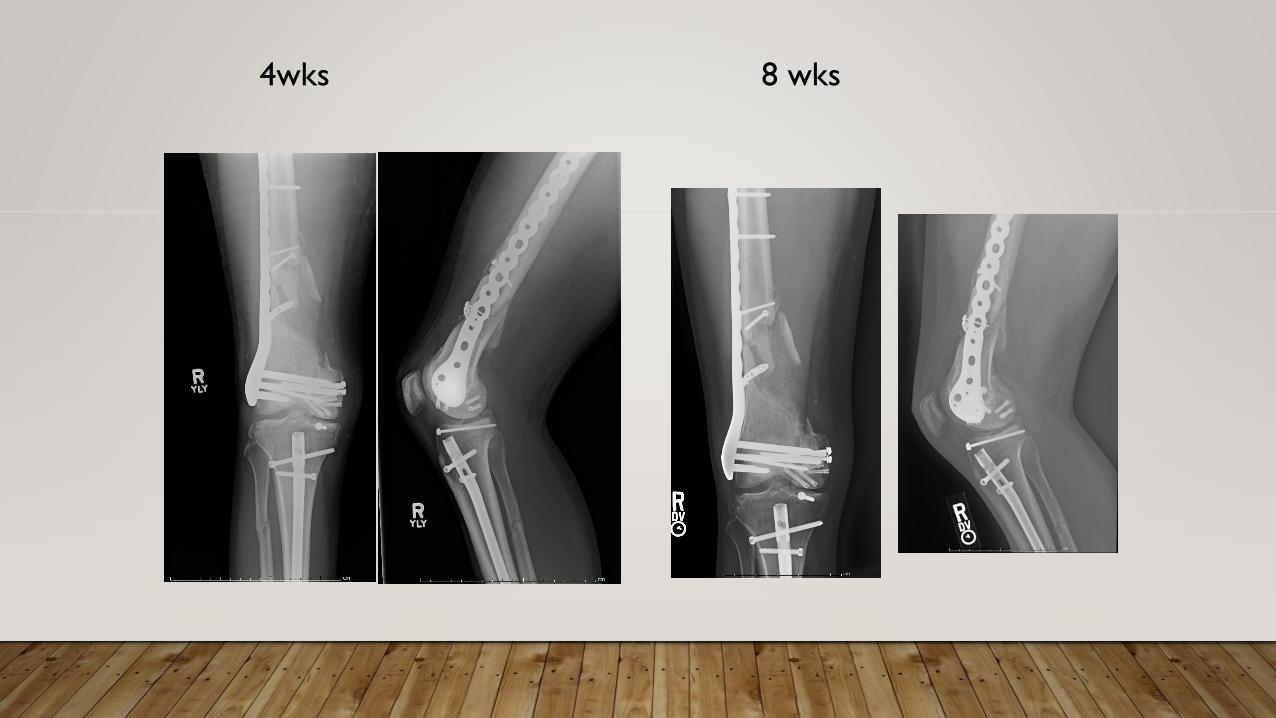
8 wks4wks

3.5 months

6 weeks

8 weeks

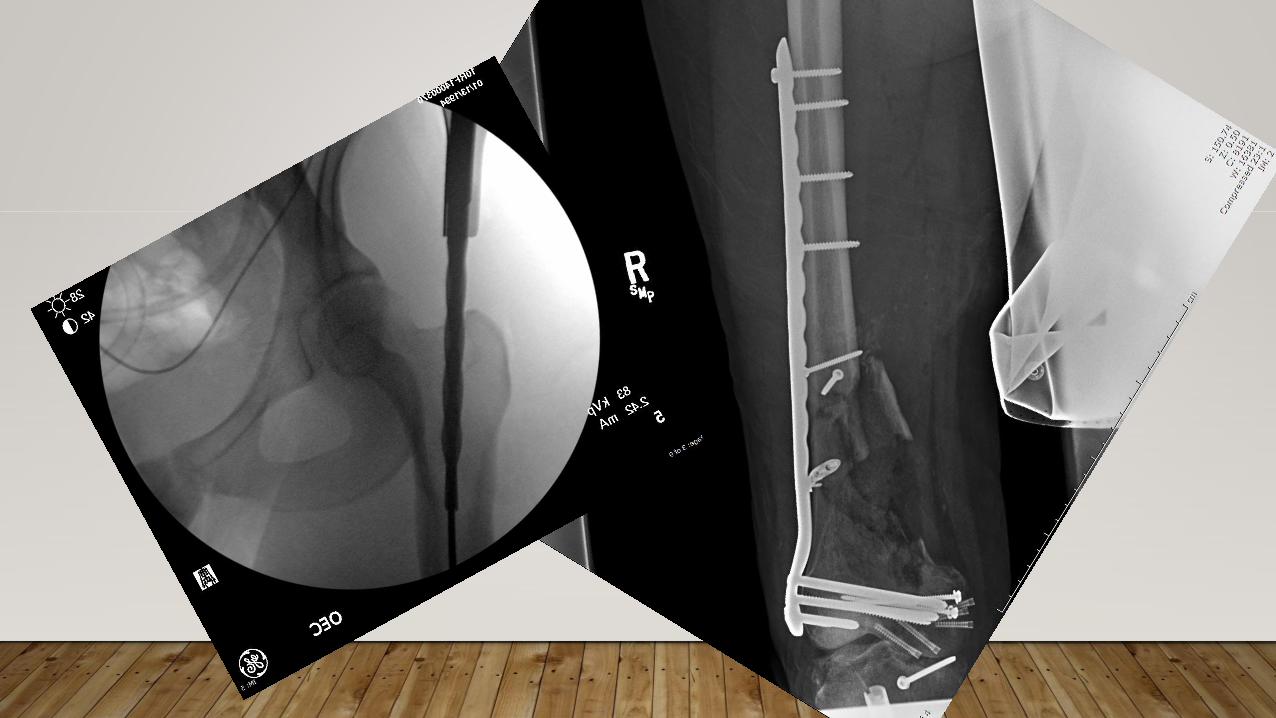
4 MONTHS AFTER NAIL
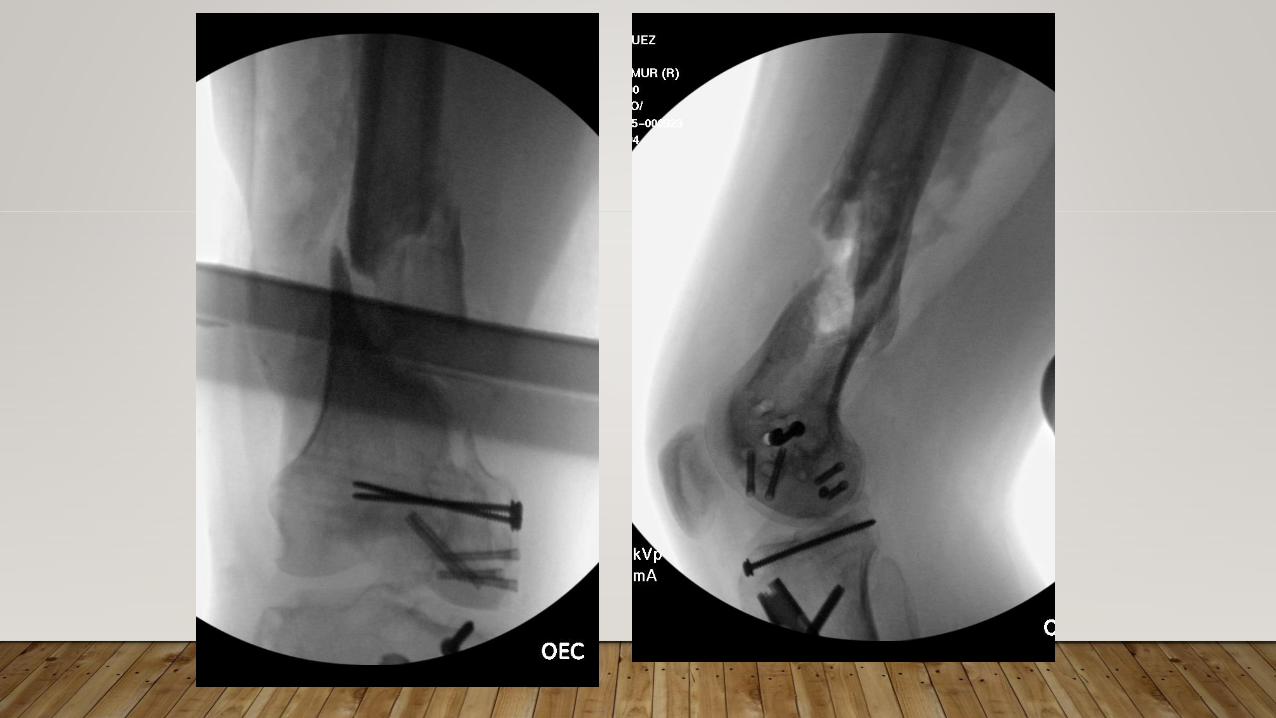
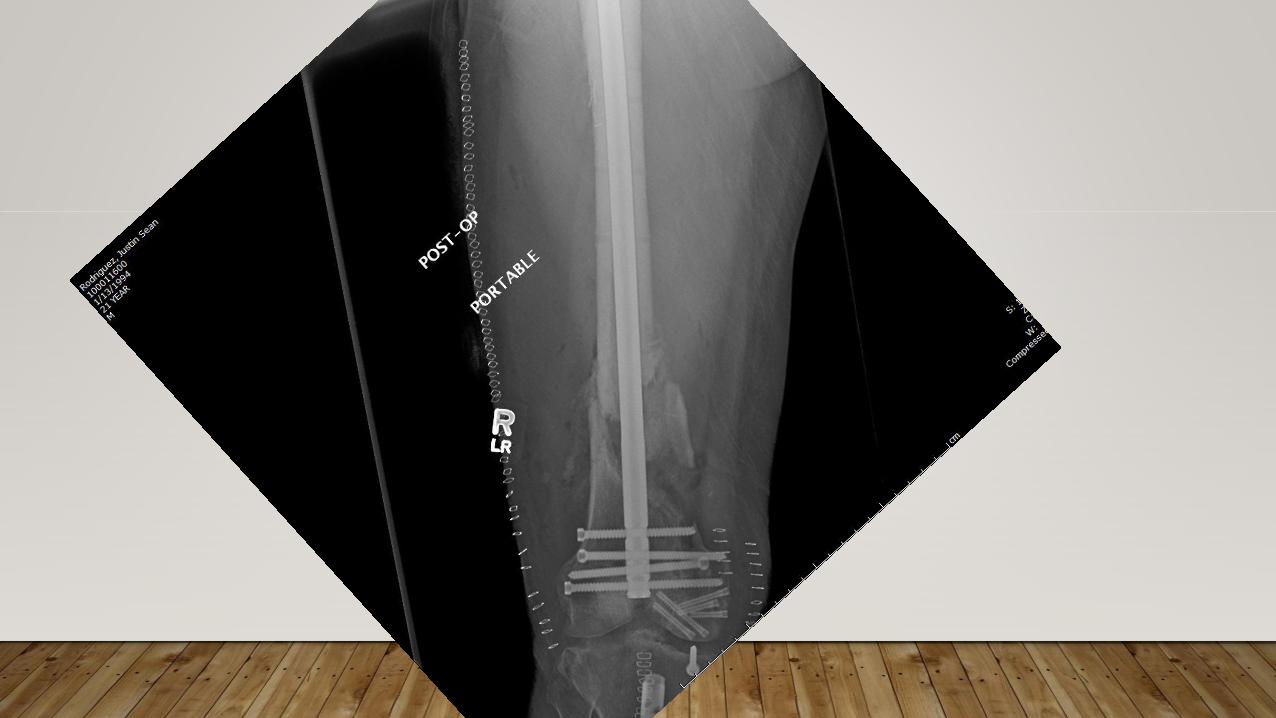
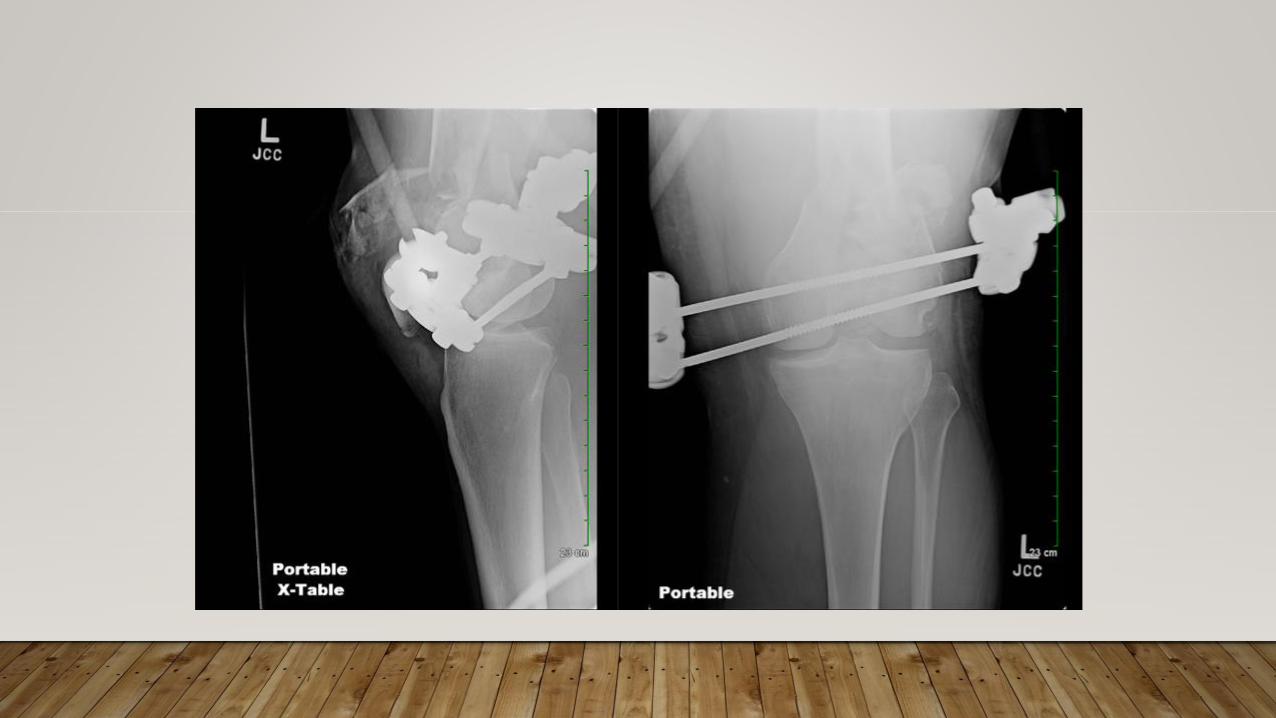
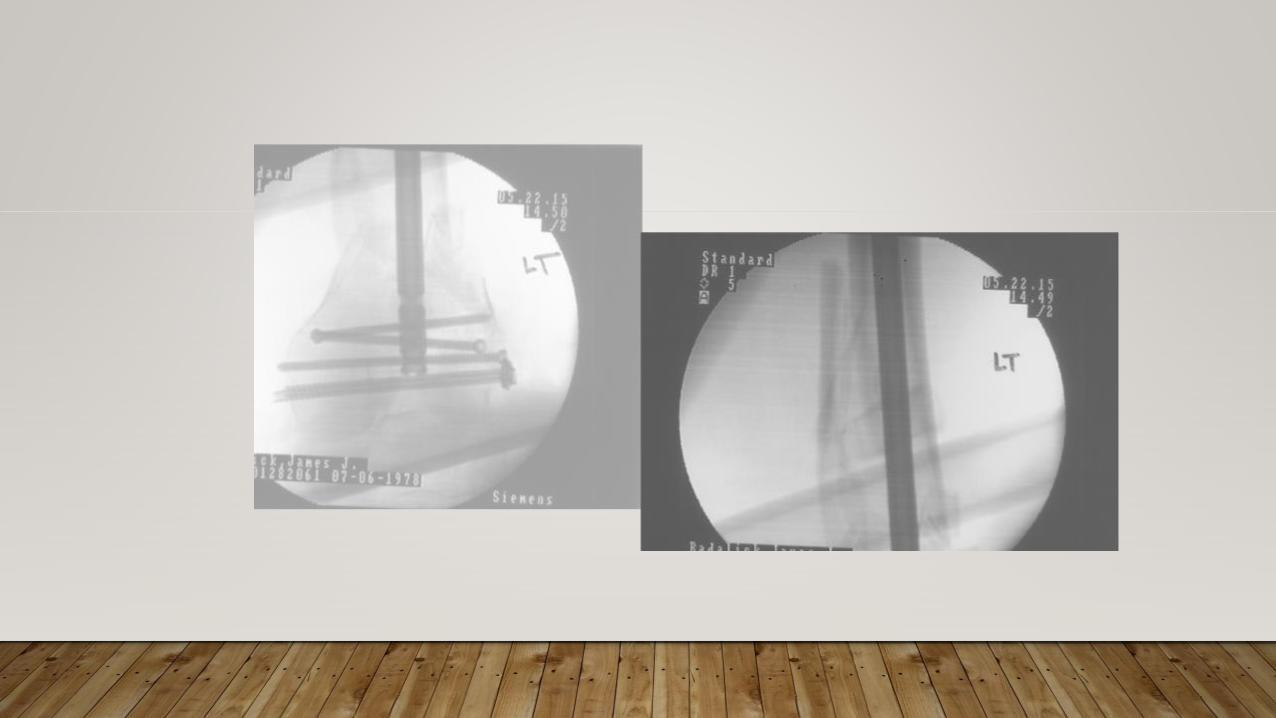
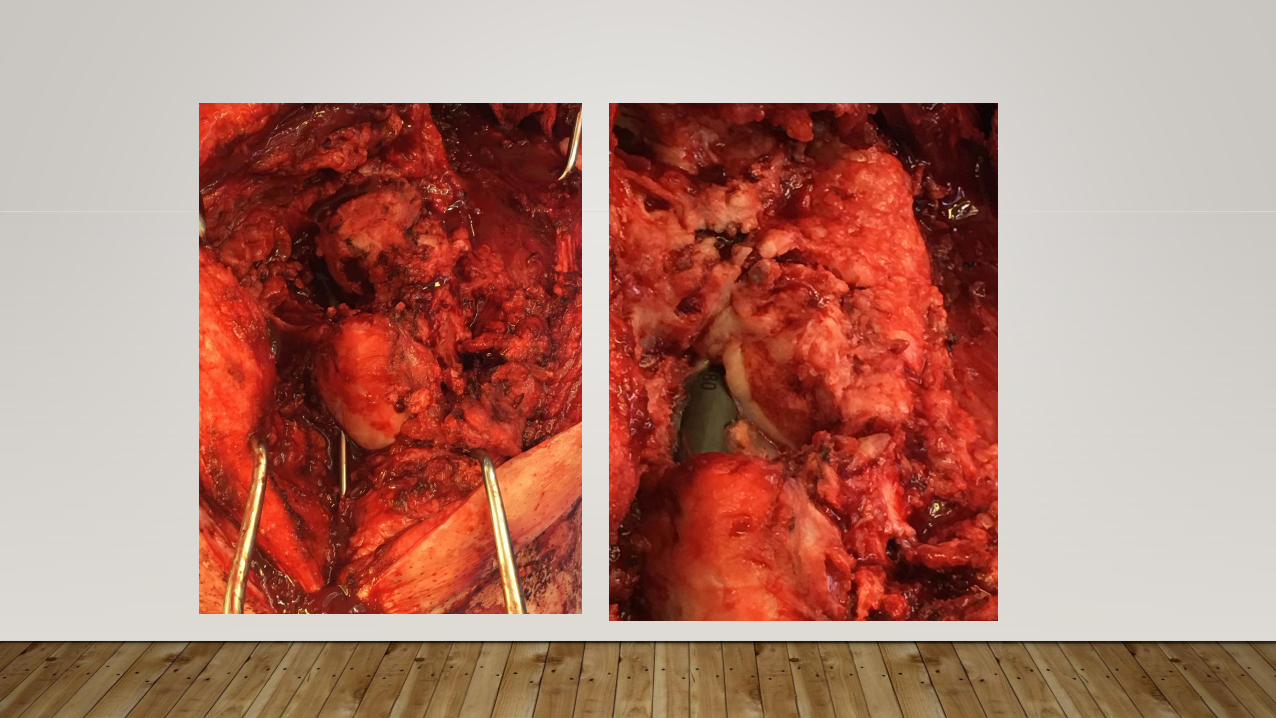
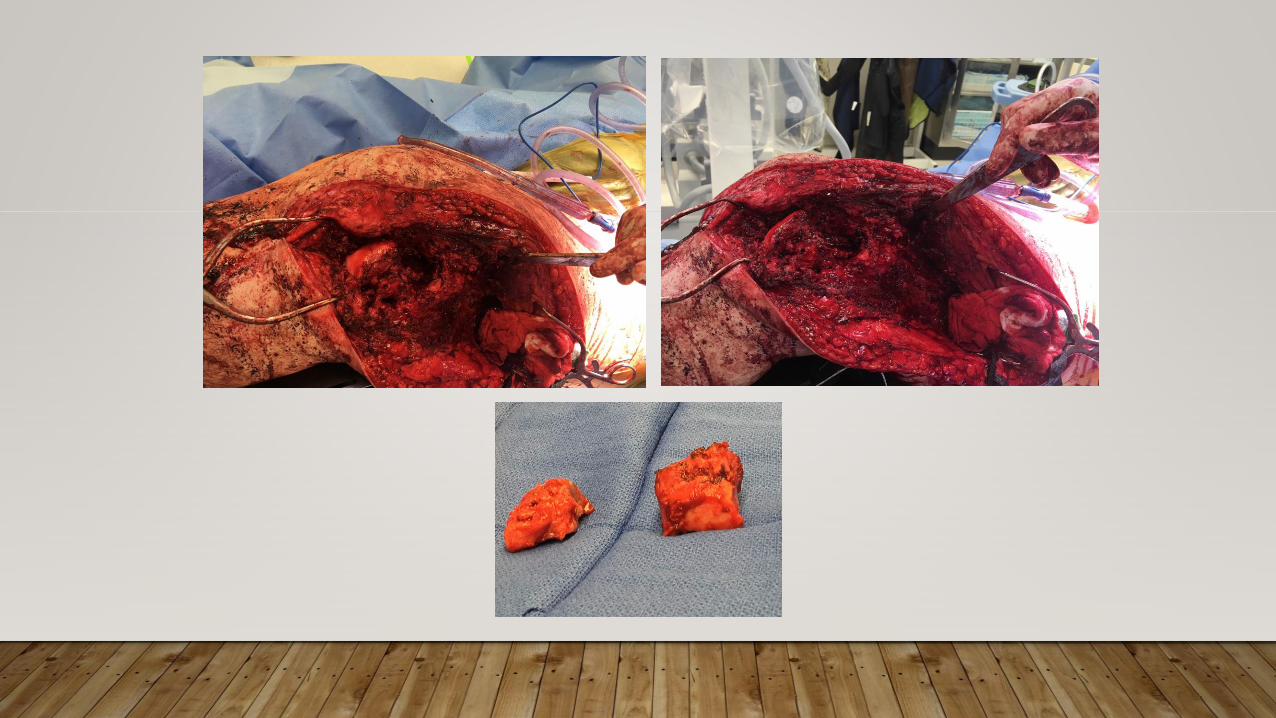
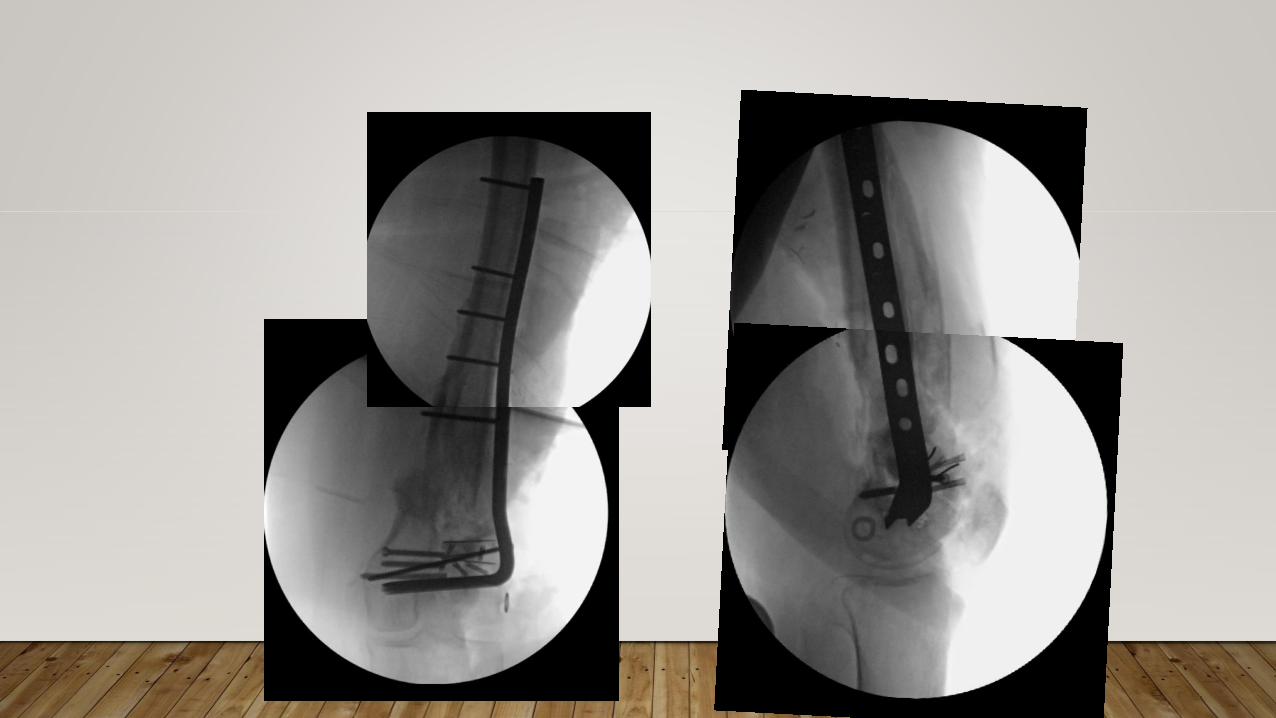
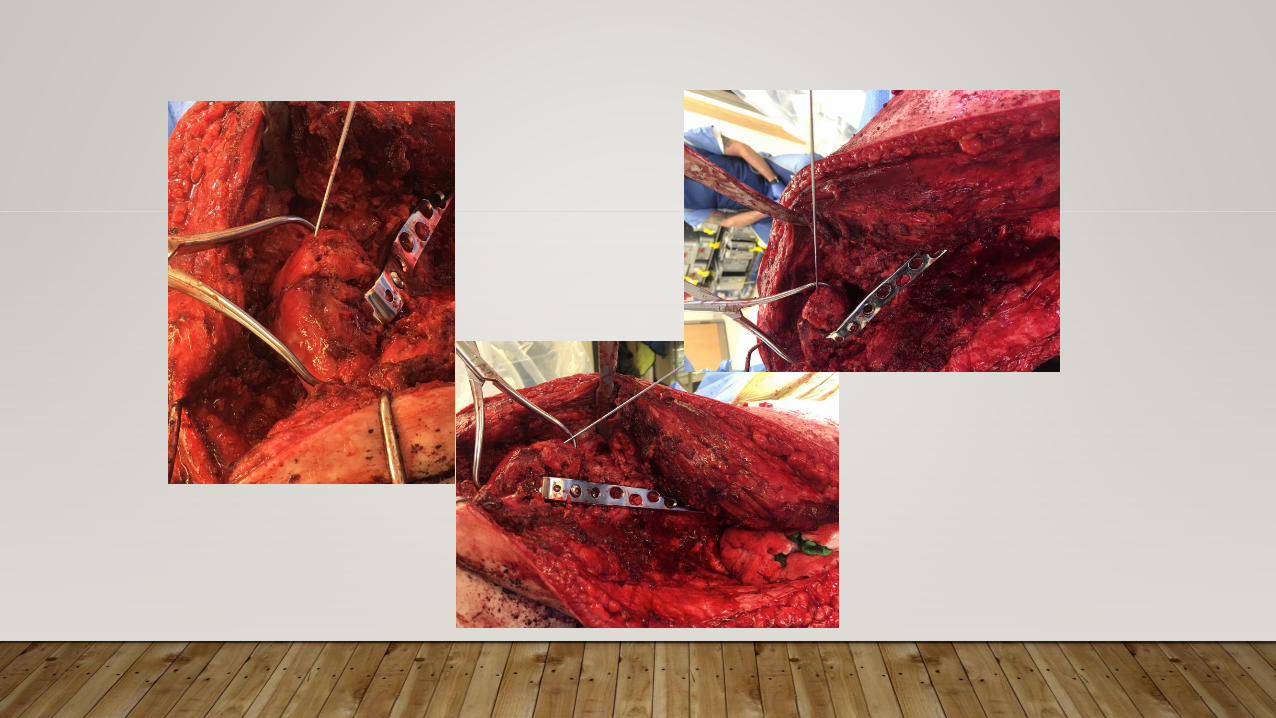
CASE 4
•36 yo Male
•Open Left distal Femur Fracture



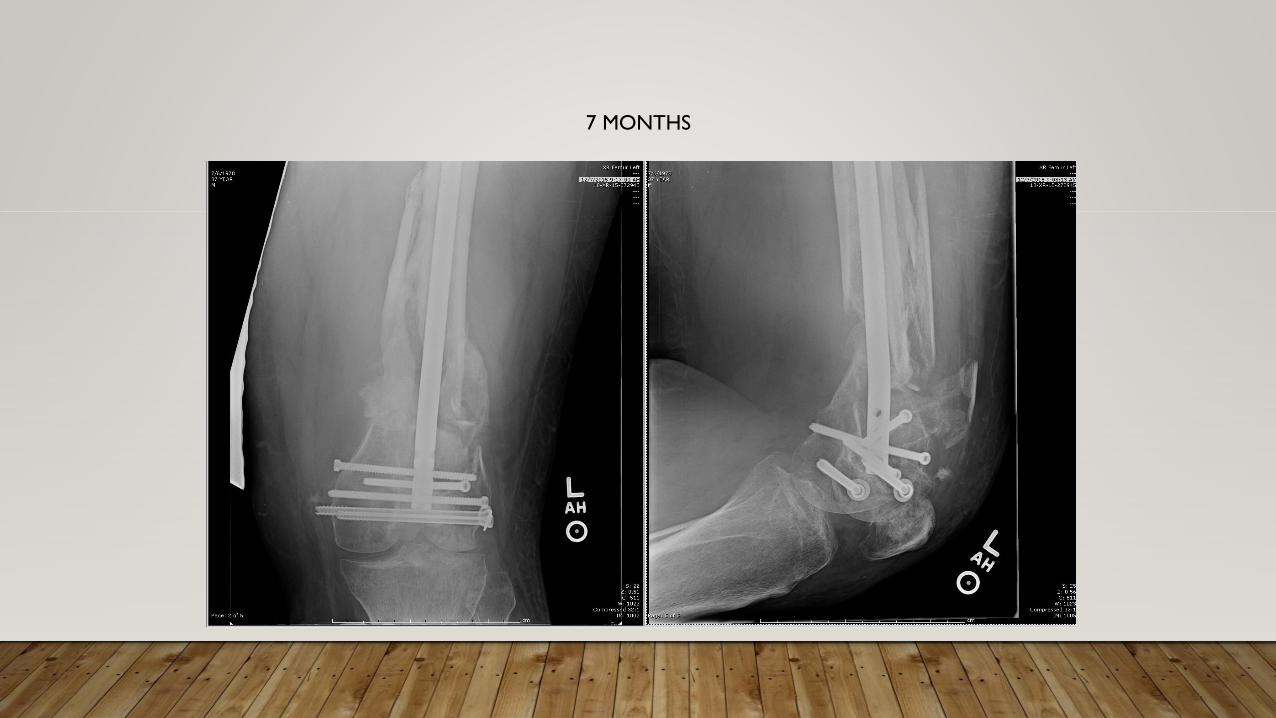
7 MONTHS

83

10 MONTHS

85

86

90
91
92

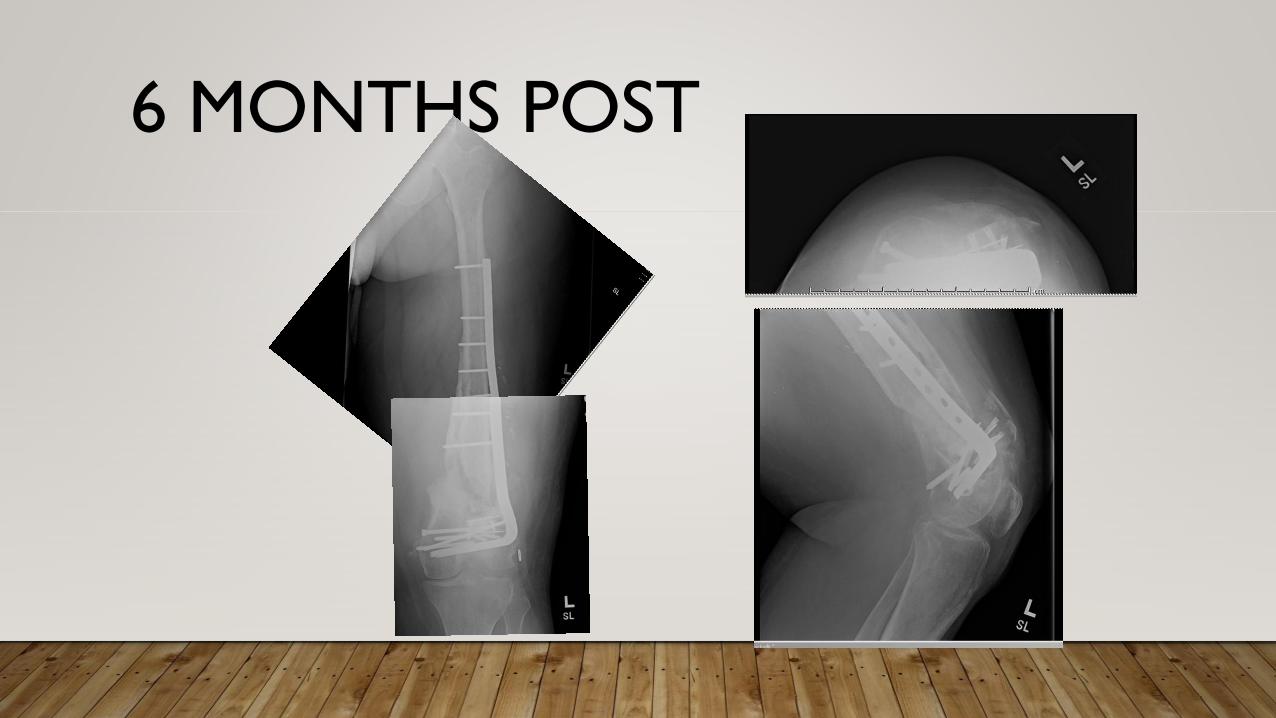
6 MONTHS POST
DISCLOSURES
•Nothing to disclose
•No royalties
•No industry affiliation
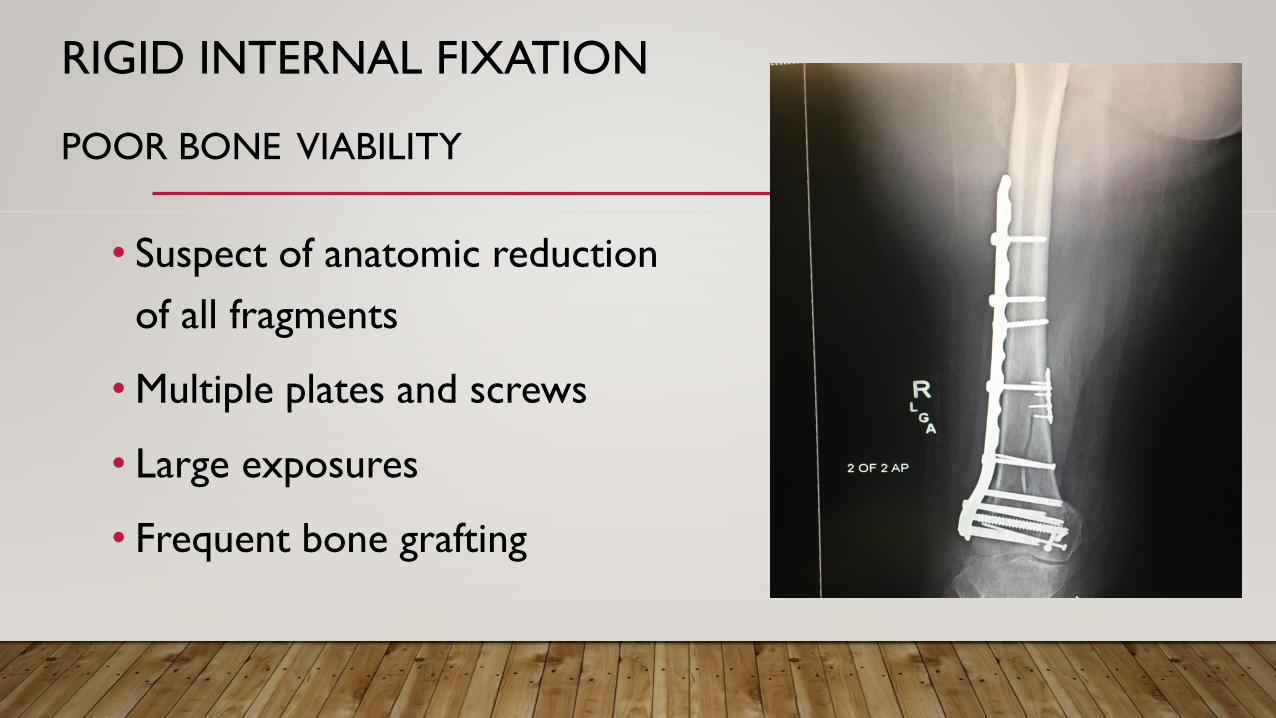
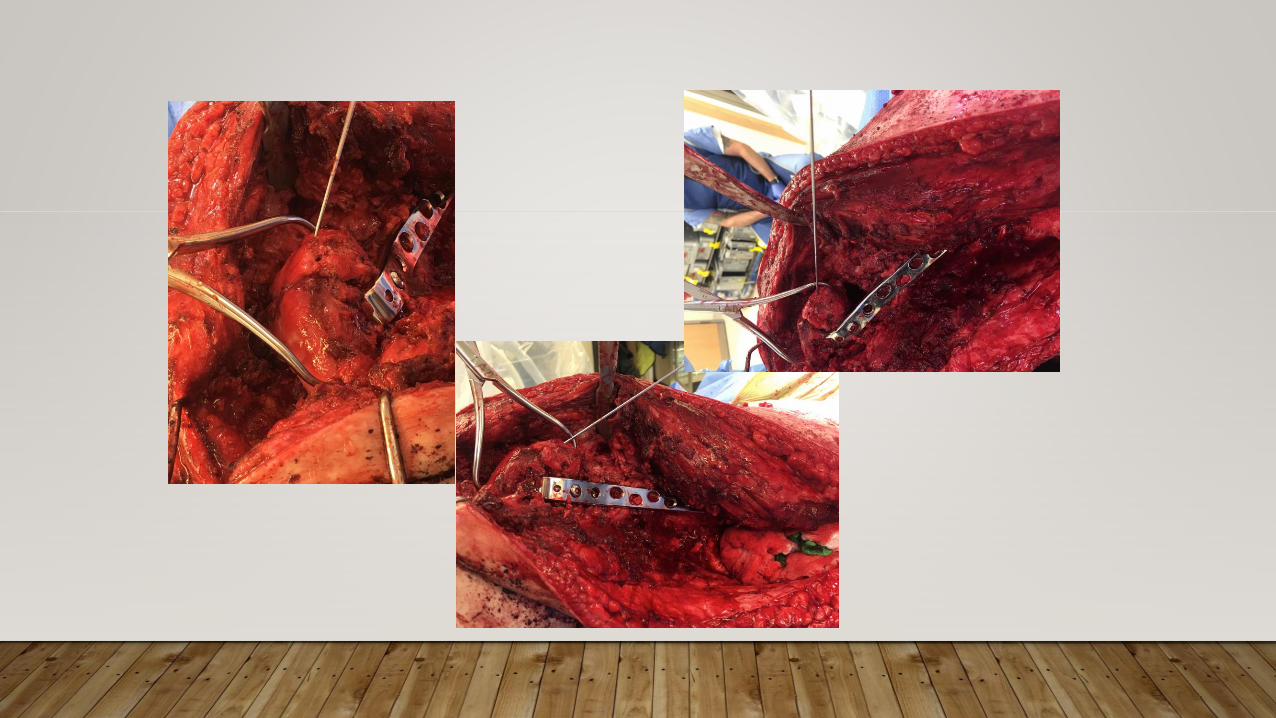
RIGID INTERNAL FIXATION
POOR BONE VIABILITY
• Suspect of anatomic reduction
of all fragments
• Multiple plates and screws
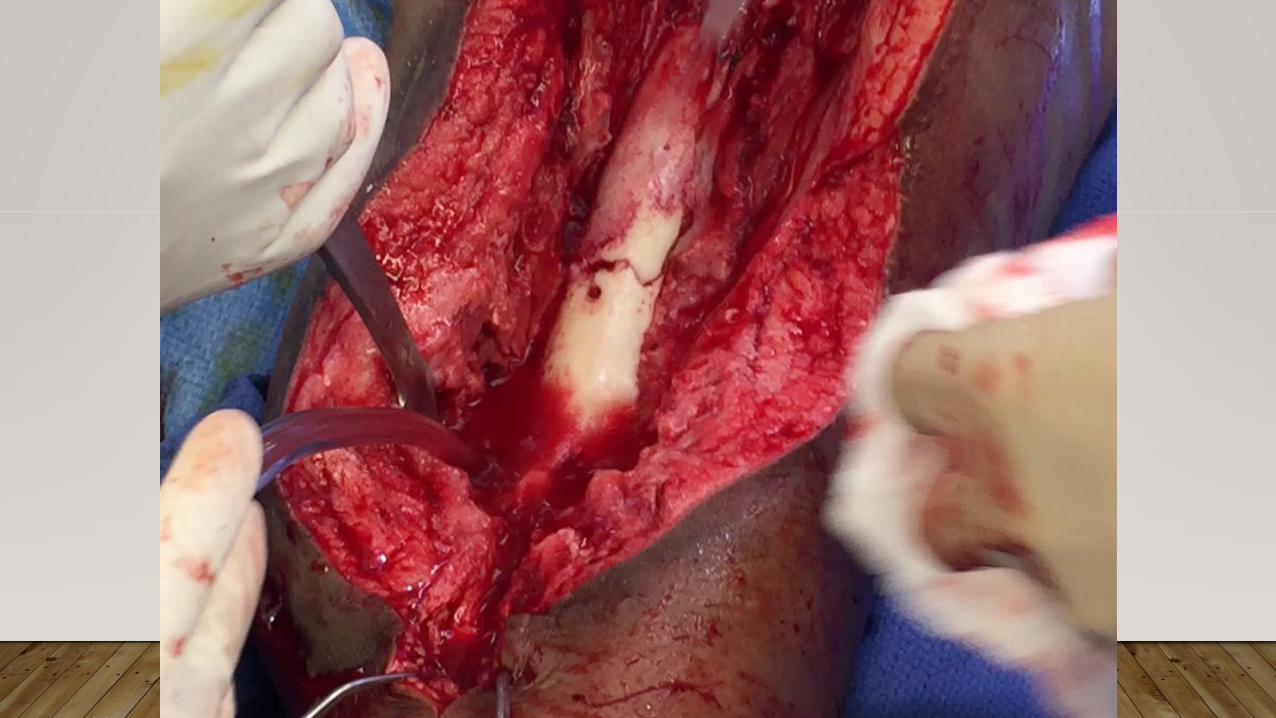
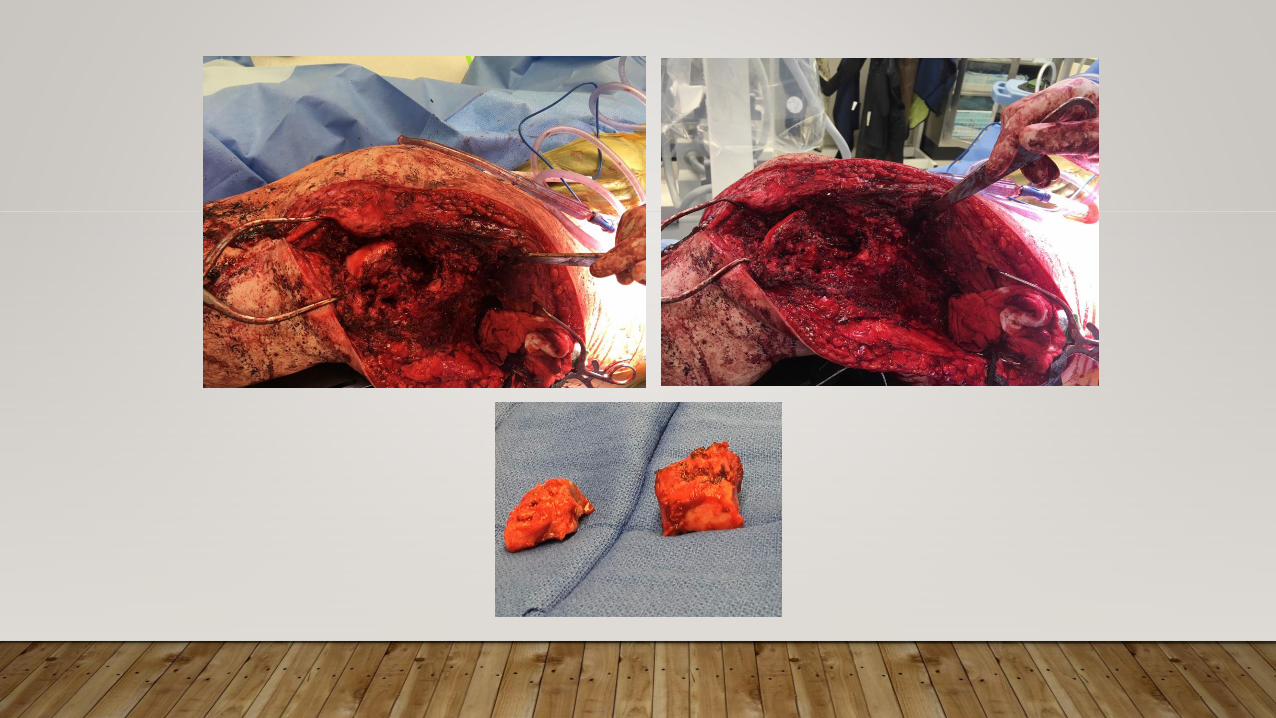
• Large exposures
• Frequent bone grafting
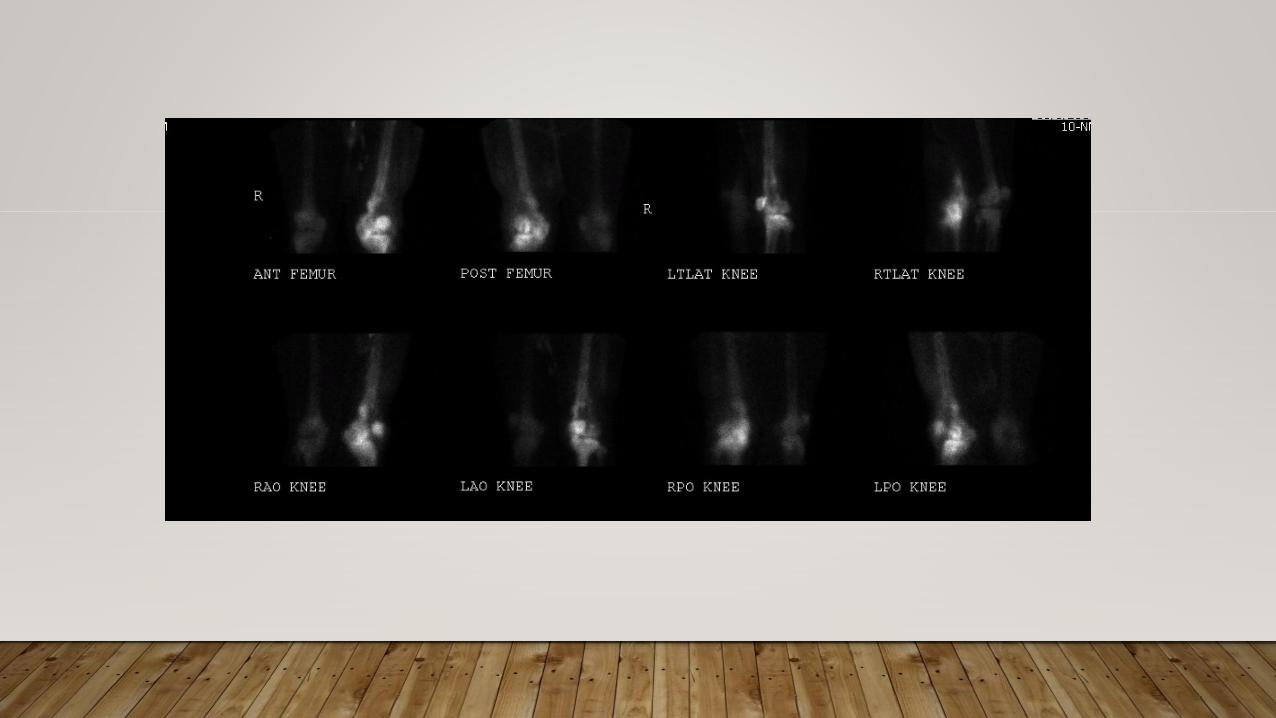
IMAGING
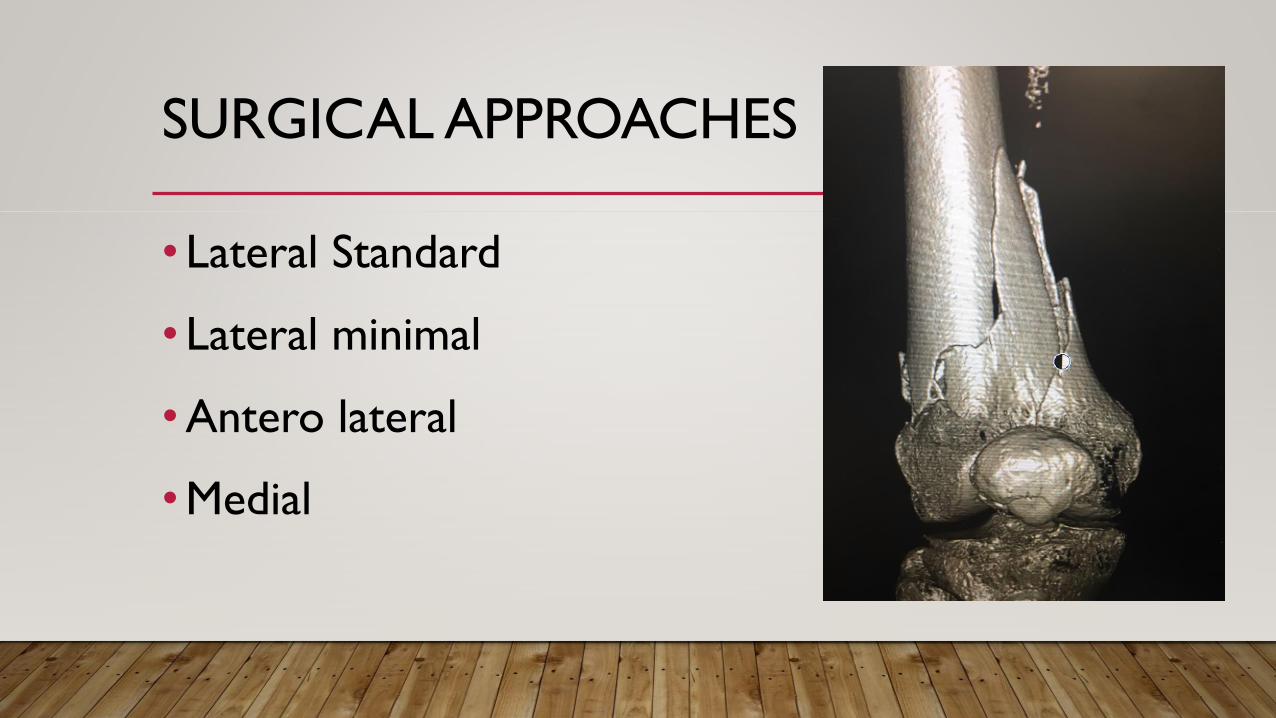
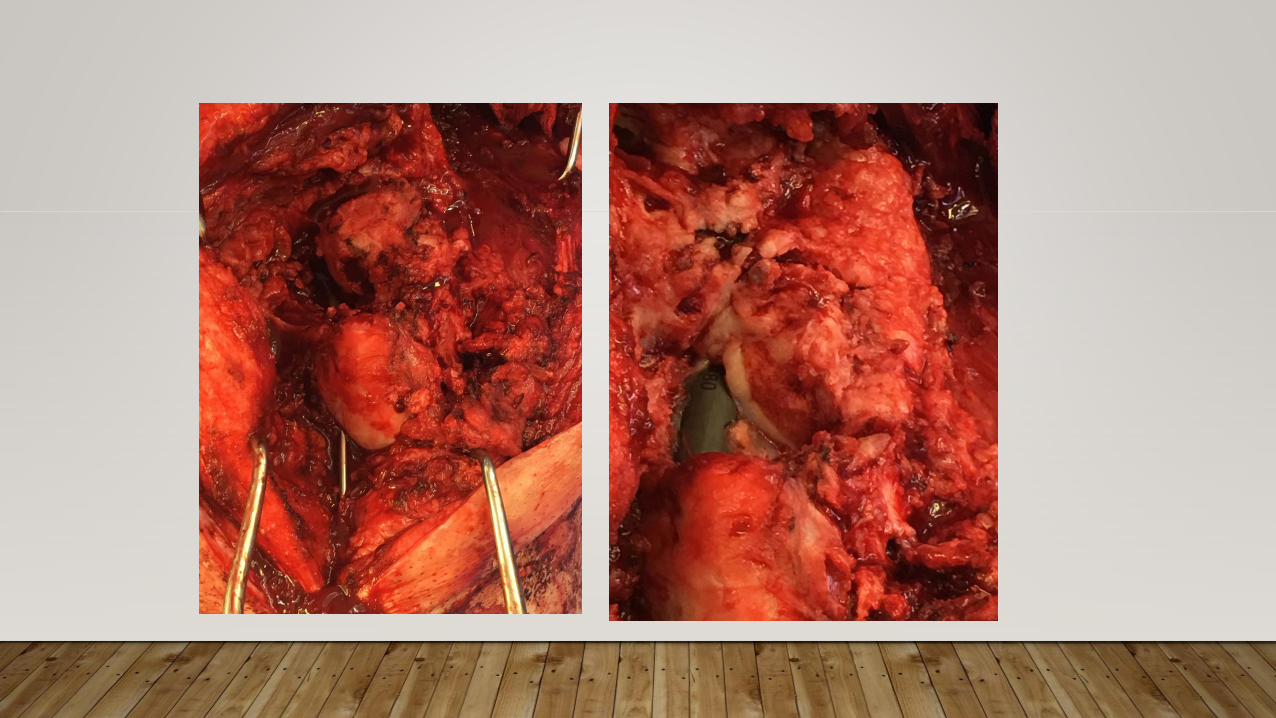
SURGICAL APPROACHES
• Lateral Standard
• Lateral minimal
•Antero lateral
•Medial
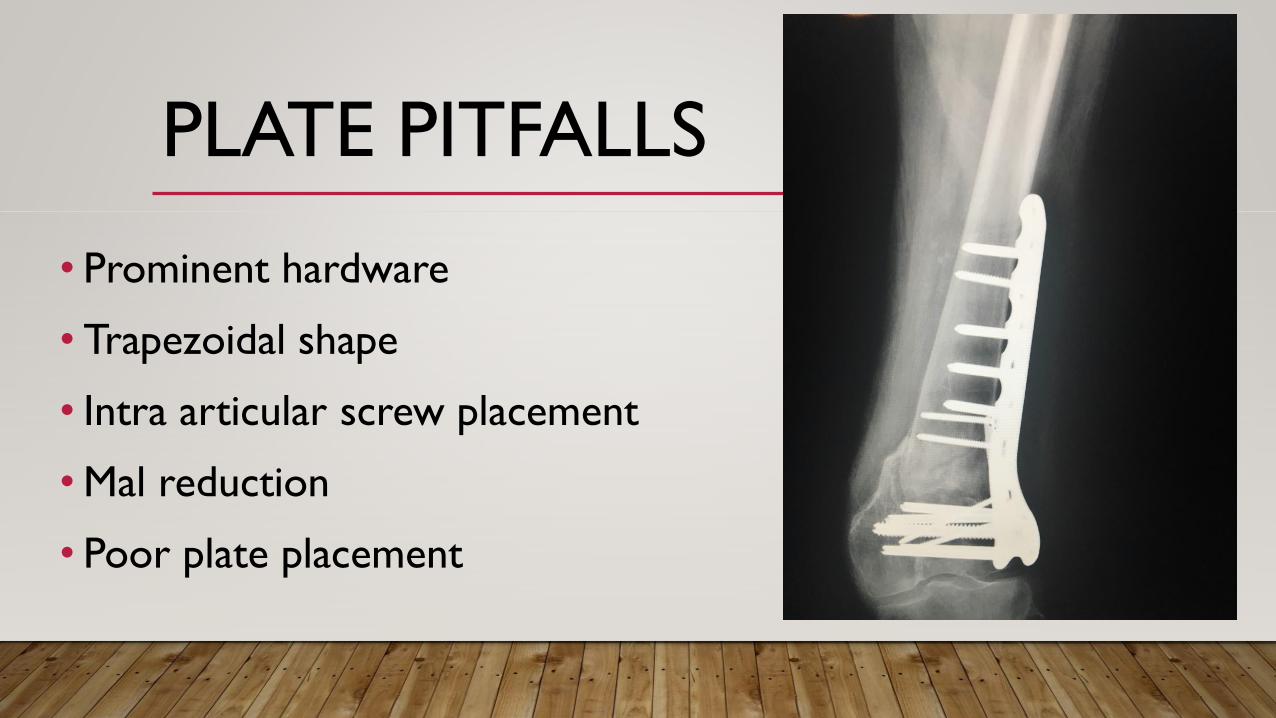
PLATE PITFALLS
• Prominent hardware
• Trapezoidal shape
• Intra articular screw placement
•Mal reduction
• Poor plate placement
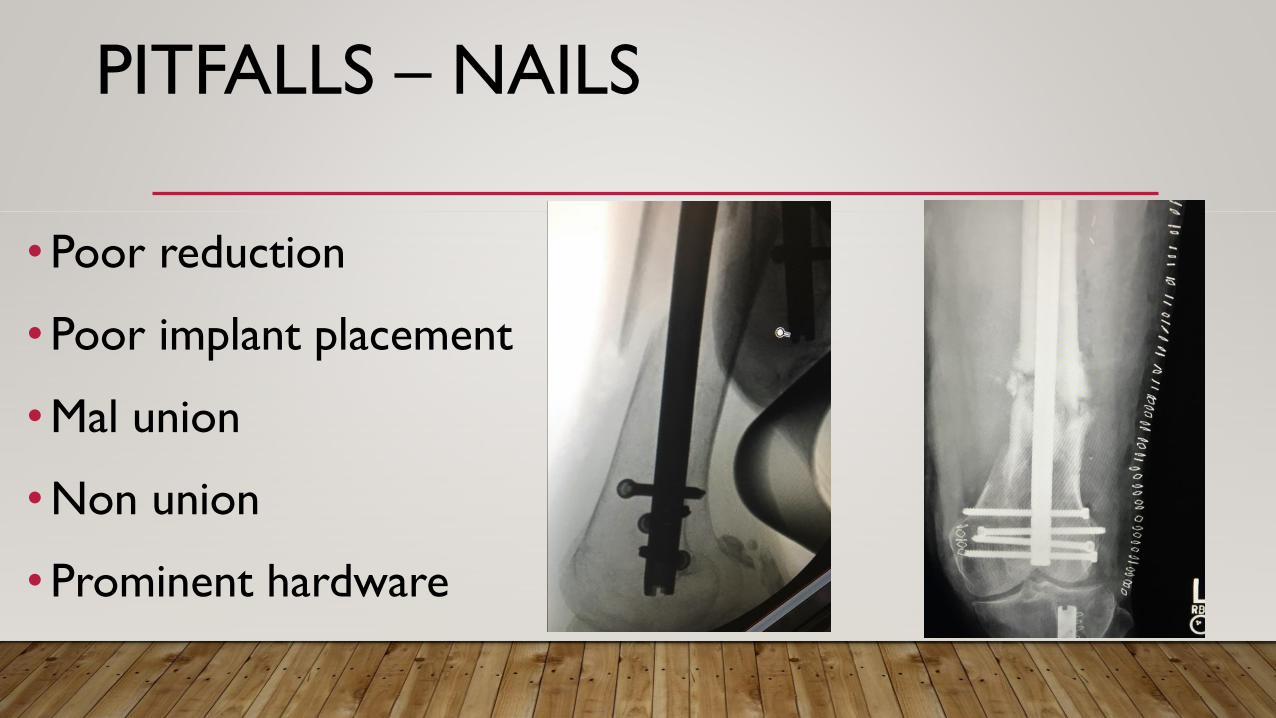
PITFALLS – NAILS
•Poor reduction
•Poor implant placement
•Mal union
•Non union
•Prominent hardware
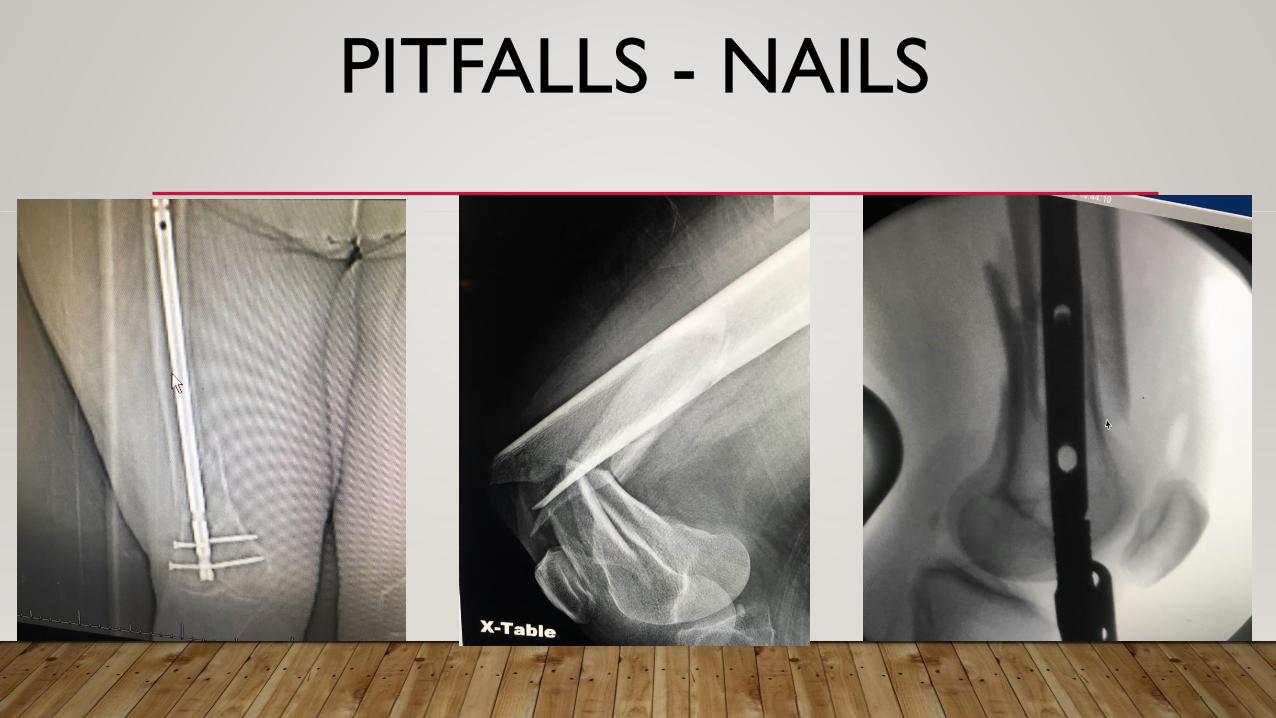
PITFALLS - NAILS
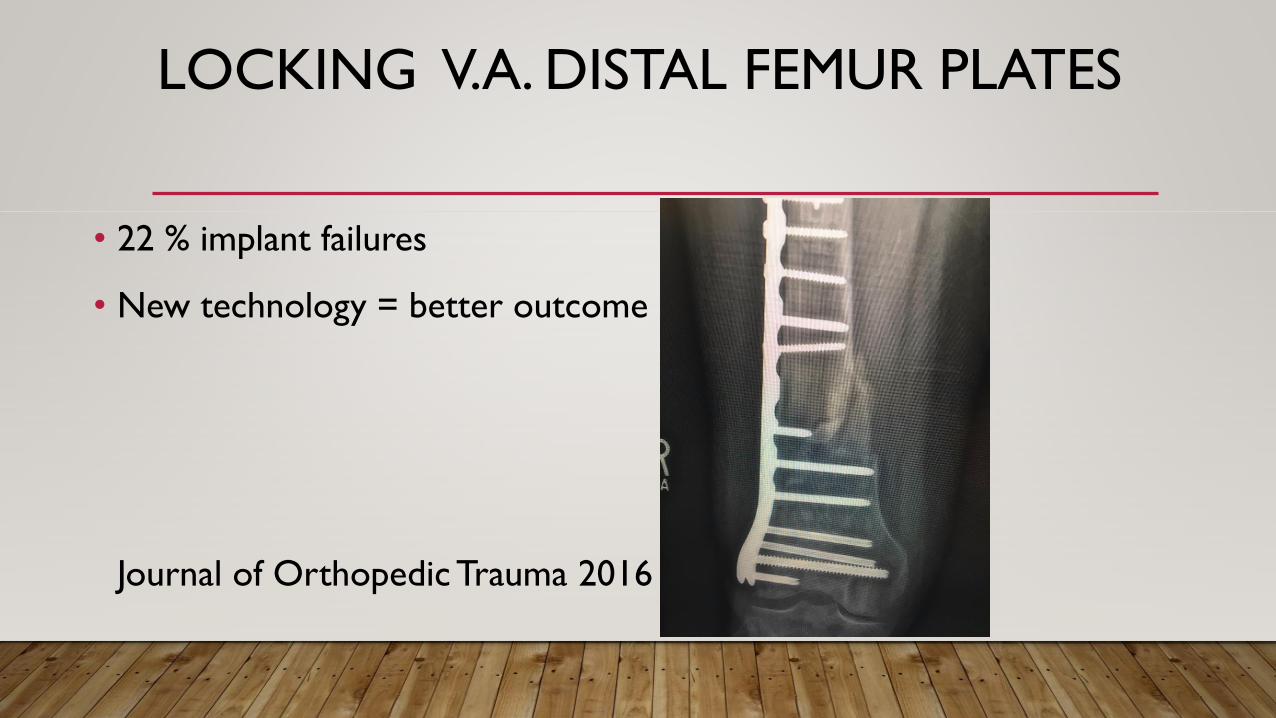
LOCKING V.A. DISTAL FEMUR PLATES
• 22 % implant failures
• New technology = better outcome
Journal of Orthopedic Trauma 2016
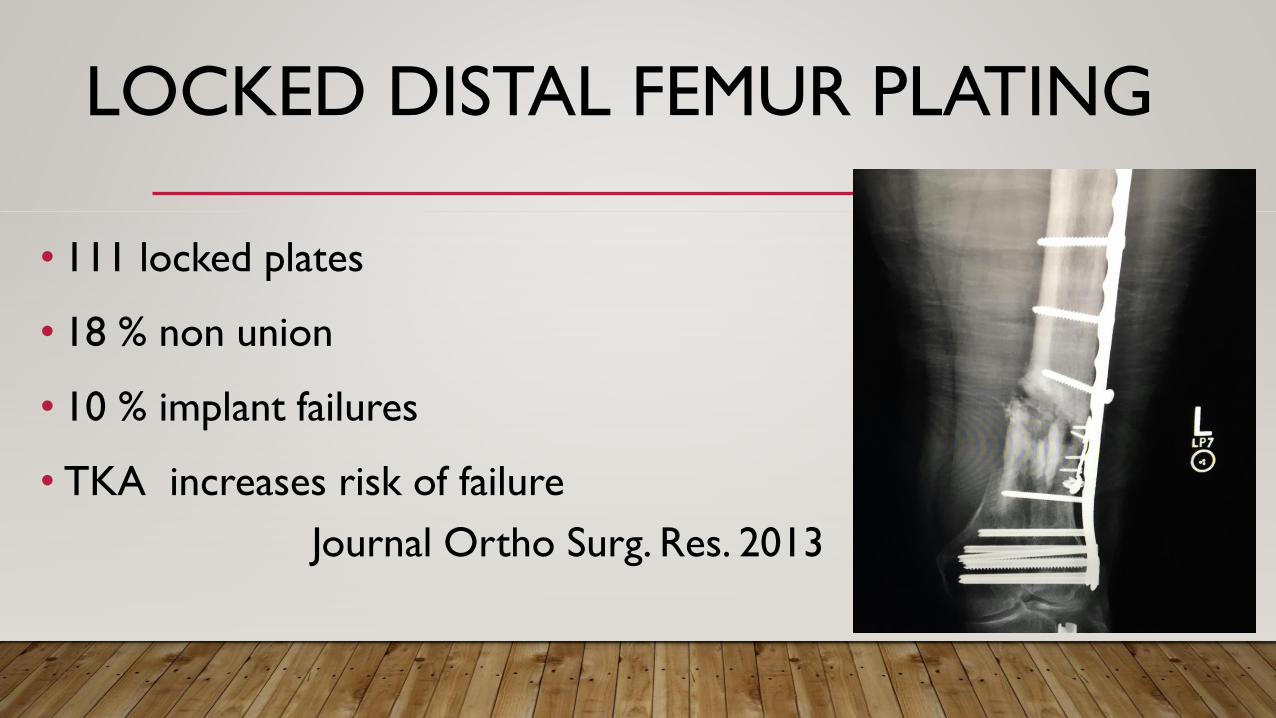
LOCKED DISTAL FEMUR PLATING
• 111 locked plates
• 18 % non union
• 10 % implant failures
• TKA increases risk of failure
Journal Ortho Surg. Res. 2013
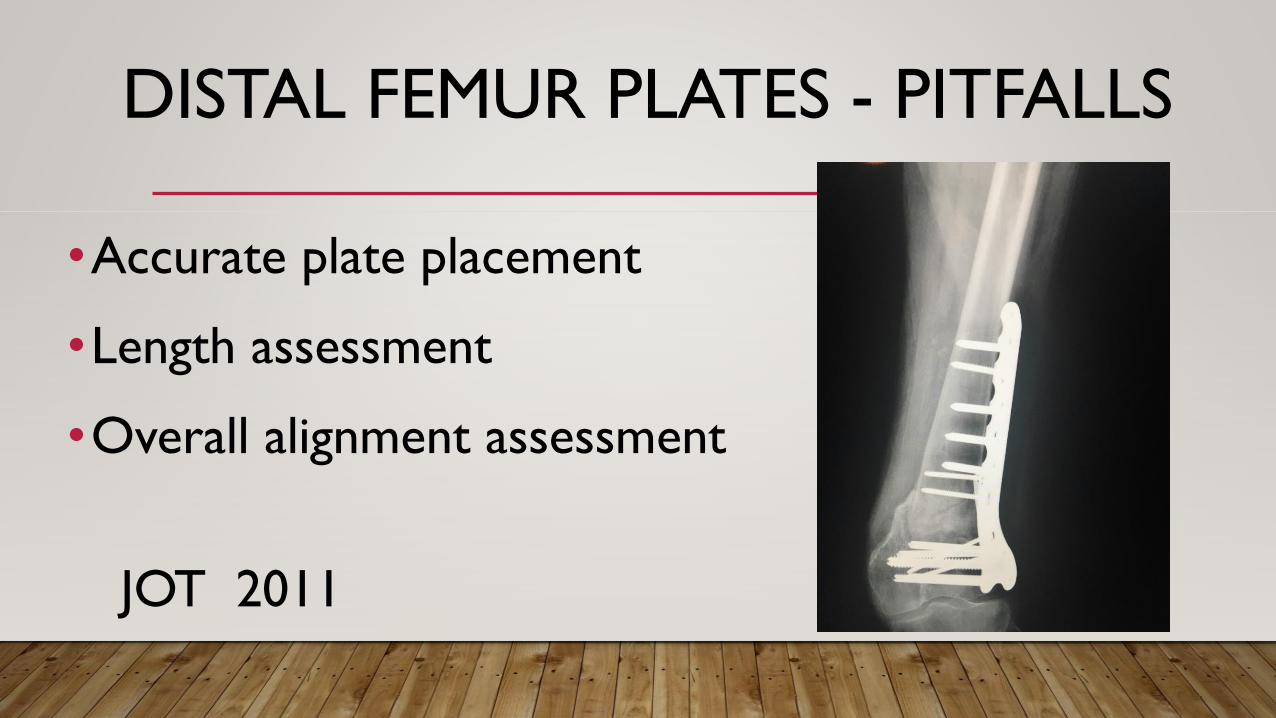
DISTAL FEMUR PLATES - PITFALLS
•Accurate plate placement
•Length assessment
•Overall alignment assessment
JOT 2011
AO/OTA CLASSIFICATION
• 33 distal femur
• A EXTRA-ARTICULAR
• B INTRA-ARTICULAR
UNICONDYLAR (HOFFA)
(coronal split)
• C INTRA-ARTICULAR
BICONDYLAR
DISTAL FEMUR GEOMETRY
• Knee joint perpendicular to floor
• Mechanical axis
• Center of hip, knee, ankle
• Anatomic axis femur 81° to articular
surface
FRACTURE DEFORMITY
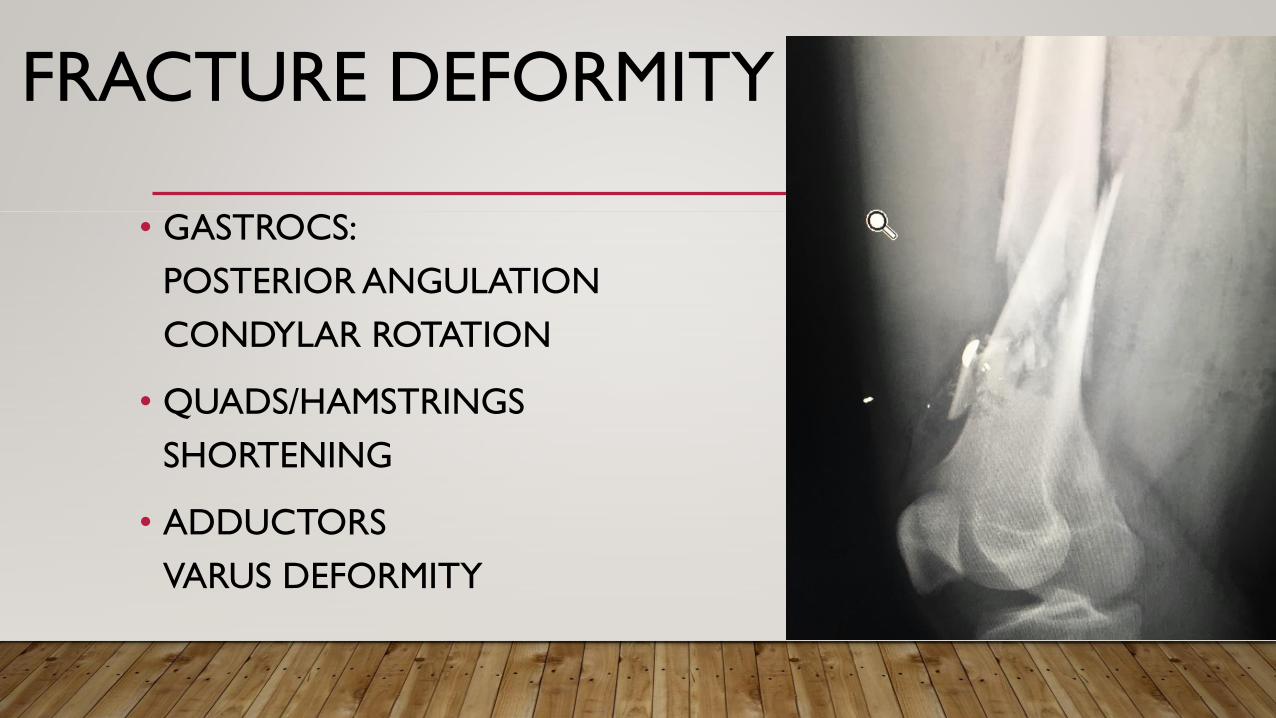
• GASTROCS:
POSTERIOR ANGULATION
CONDYLAR ROTATION
• QUADS/HAMSTRINGS
SHORTENING
• ADDUCTORS
VARUS DEFORMITY
SURGICAL ANATOMY
• Femoral shaft
• Anterior ½ of condyles
• Plates co-linear
• Anterior ½ of condyles
• Proper alignment
DISTAL FEMUR ANATOMY
•Trapezoidal shape
•Condyles wider
posteriorly
•Slope to PF joint
SURGICAL ANATOMY
• ANTERIOR FEMUR SLOPE
• AVOID PENETRATION MEDIAL
CORTEX
• 8-10 MM SHORTER OF PROJECTED
IMAGE
• SCREWS OR BLADE
FIXED ANGLE DEVICESBLADE DCS LOCKED PLATES
• Blade or Lag screw
• Parallel to articular surface
• Avoid intercondylar groove
• Avoid intercondylar notch
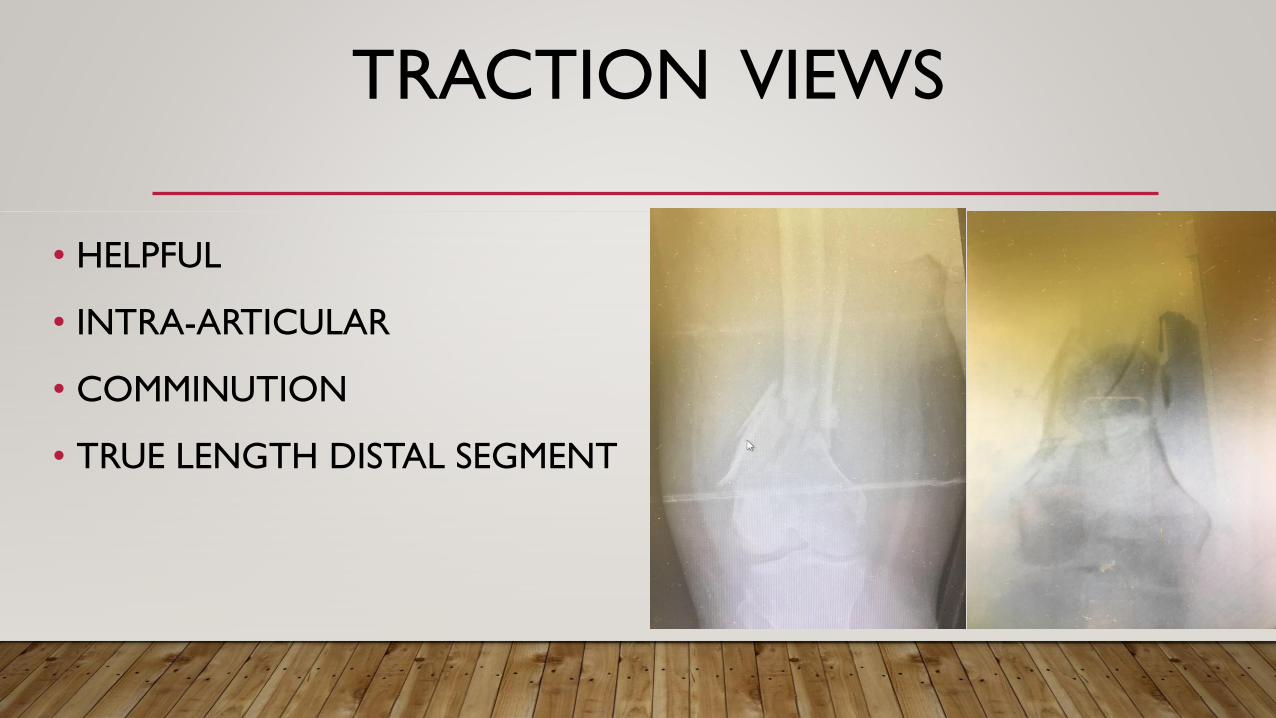
TRACTION VIEWS
• HELPFUL
• INTRA-ARTICULAR
• COMMINUTION
• TRUE LENGTH DISTAL SEGMENT
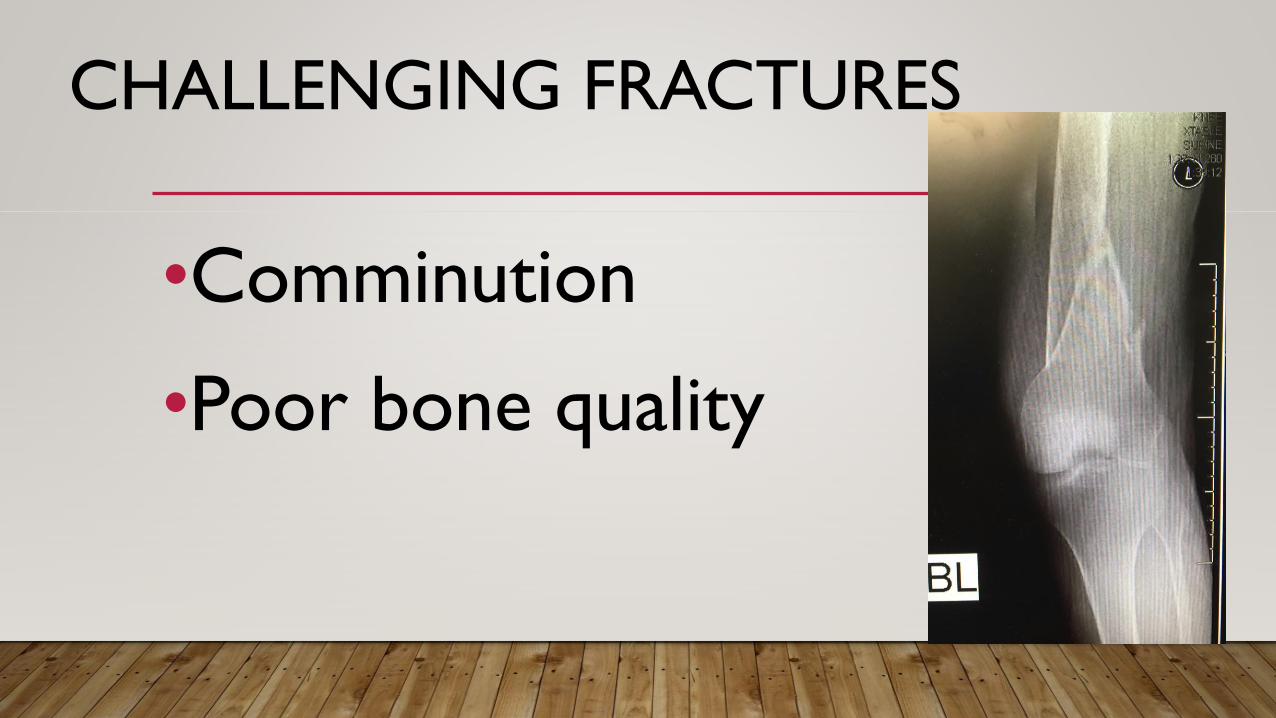
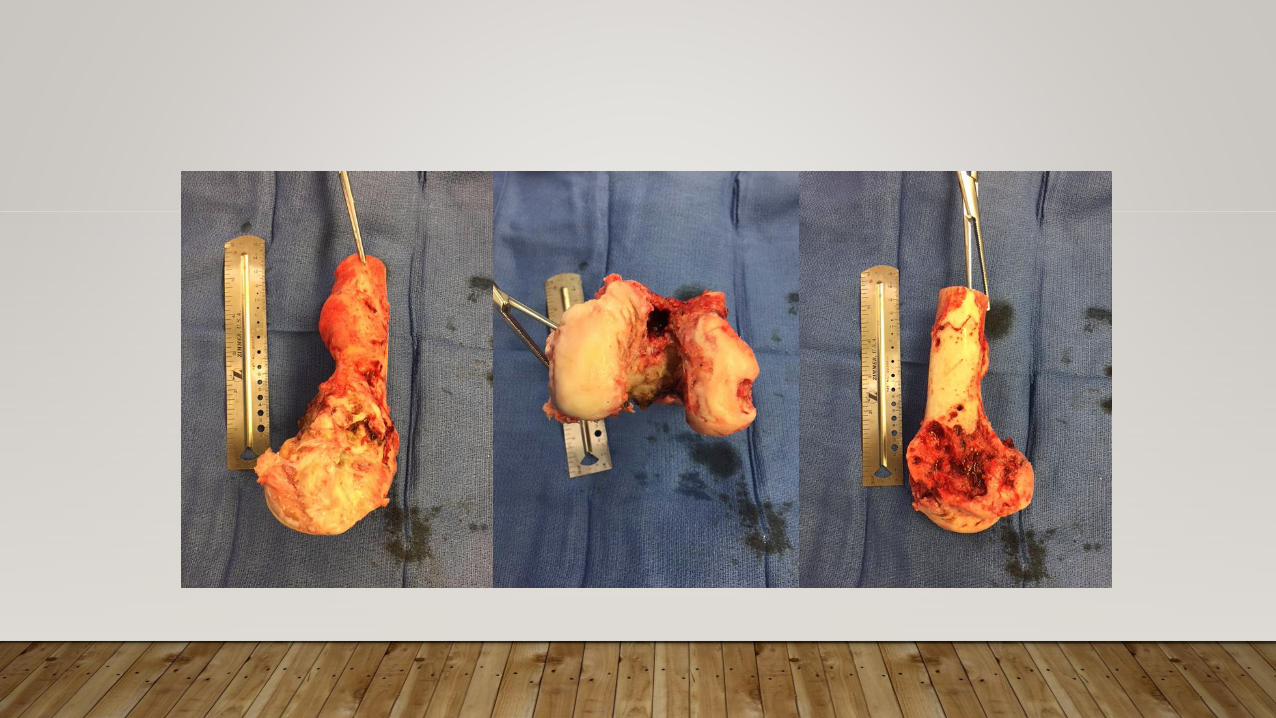
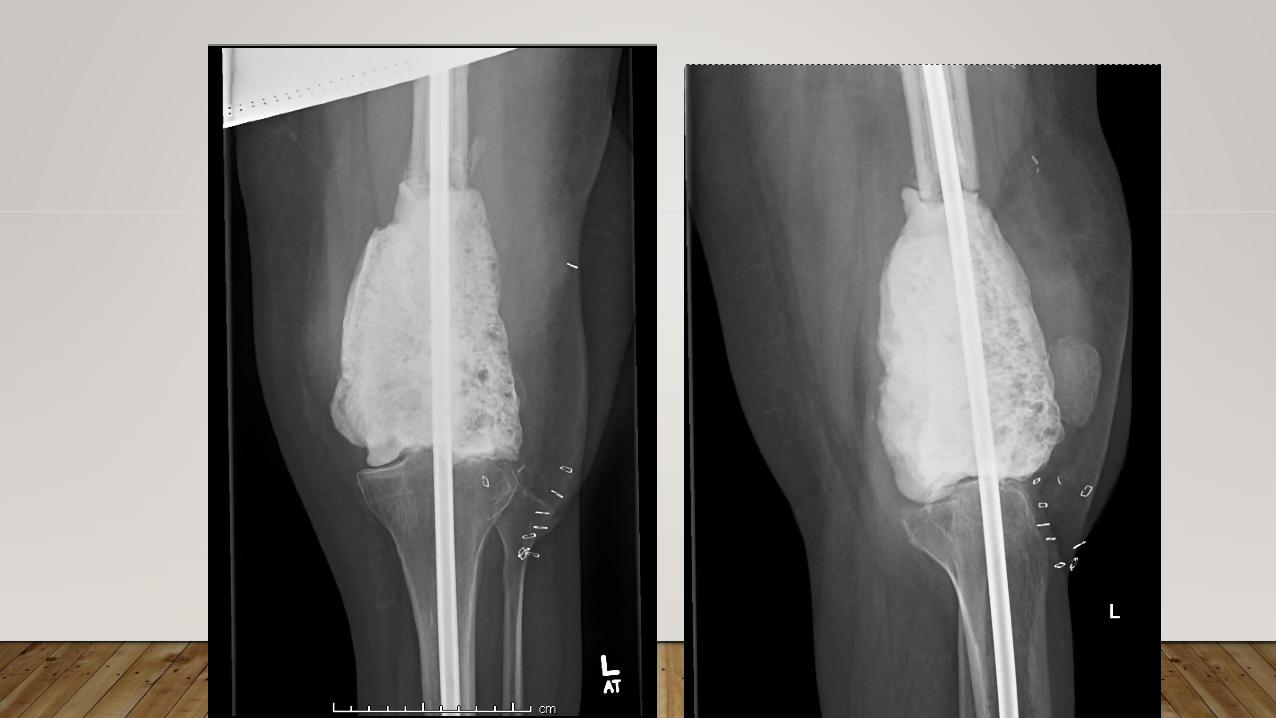
CHALLENGING FRACTURES
•Comminution
•Poor bone quality
CASE 1
• 23M MCA at 60 MPH
• Open knee injury
• Small subarachnoid hemorrhage
• Hemodynamically stable
• Neurovascular intact




5 months
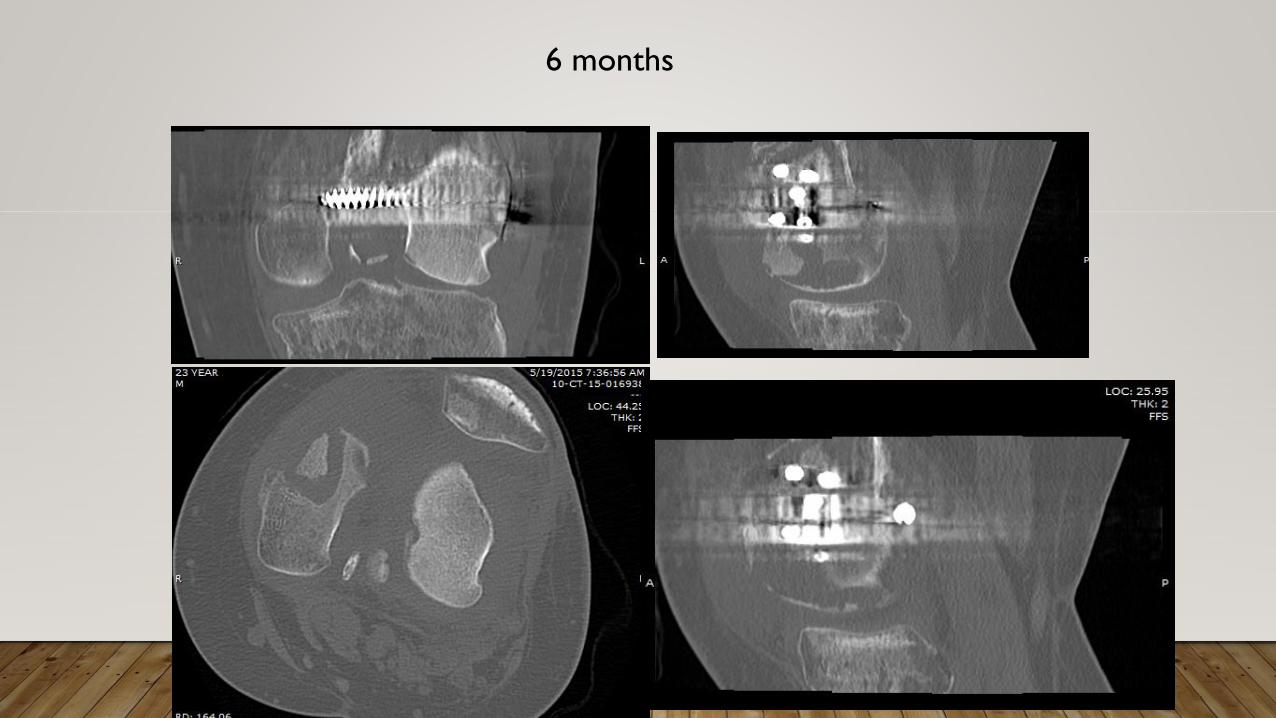
6 months
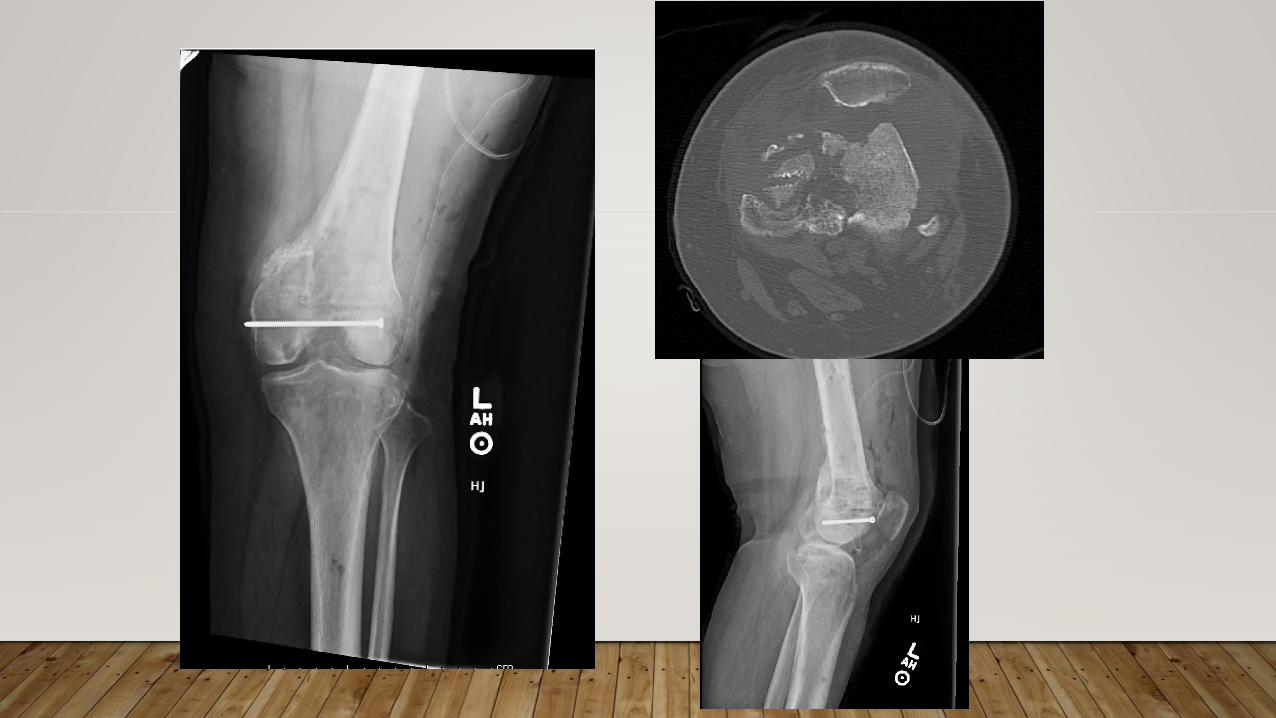

PUSSES OUT!





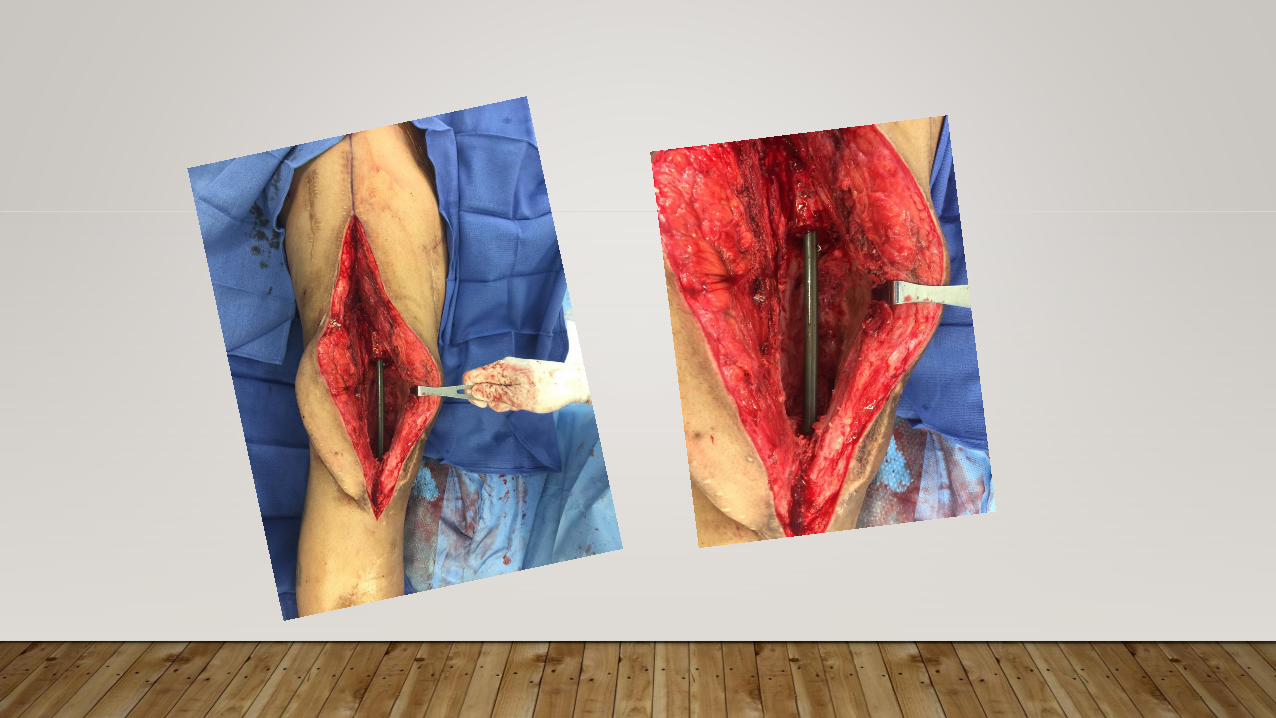
CASE 2
• 20M high speed MCA
• Multiple open fractures RLE
• Rib fractures/pulmonary contusion
• Stable
• Neurovascular exam intact

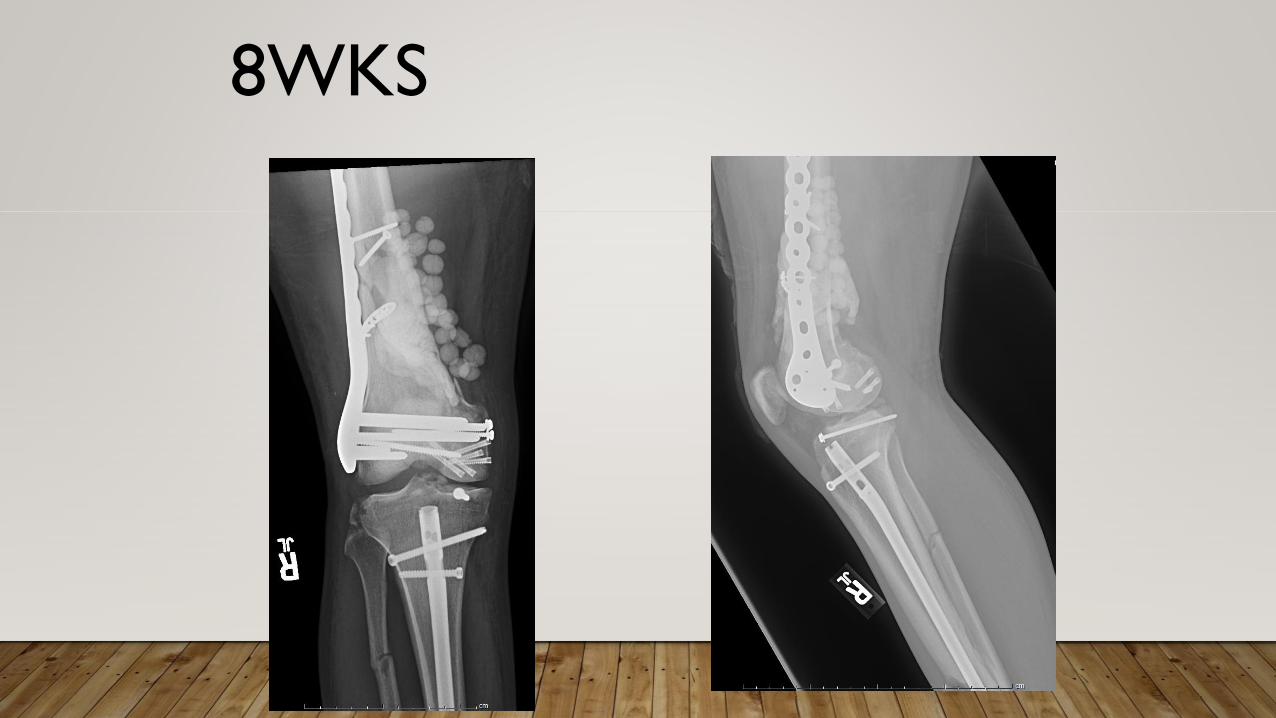
8WKS
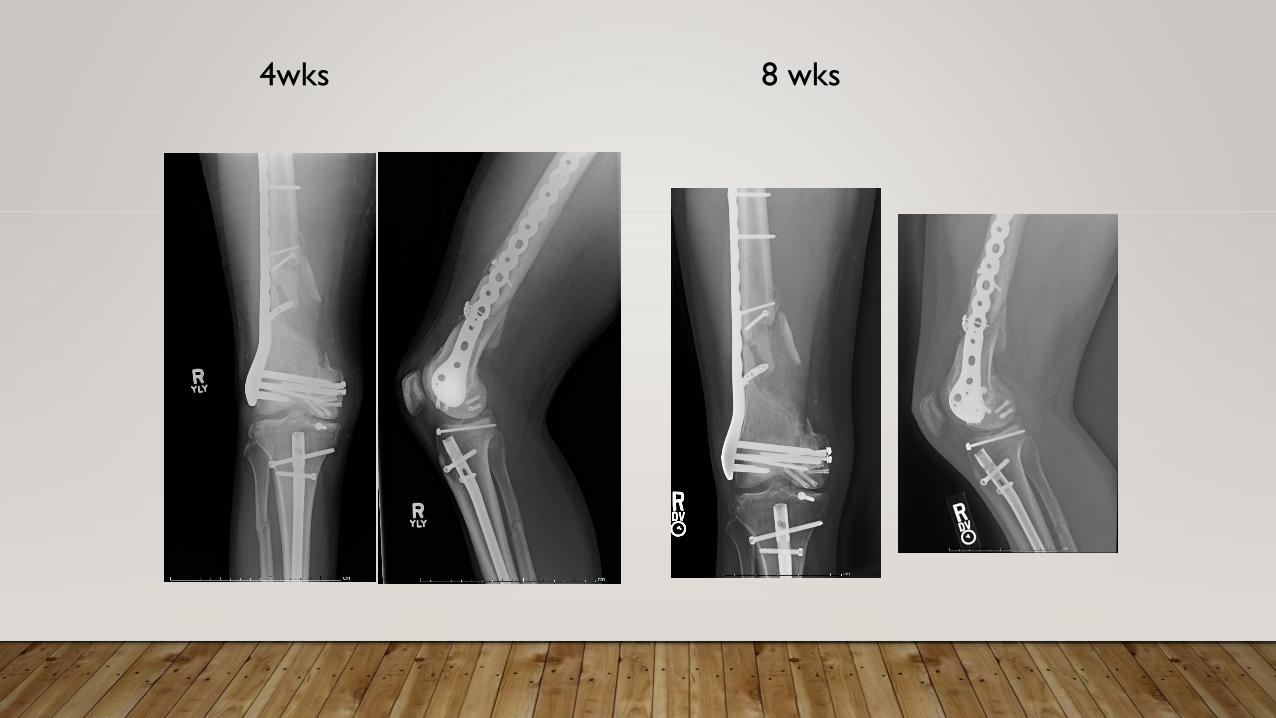
8 wks4wks

3.5 months



6 weeks

8 weeks

4 MONTHS AFTER NAIL
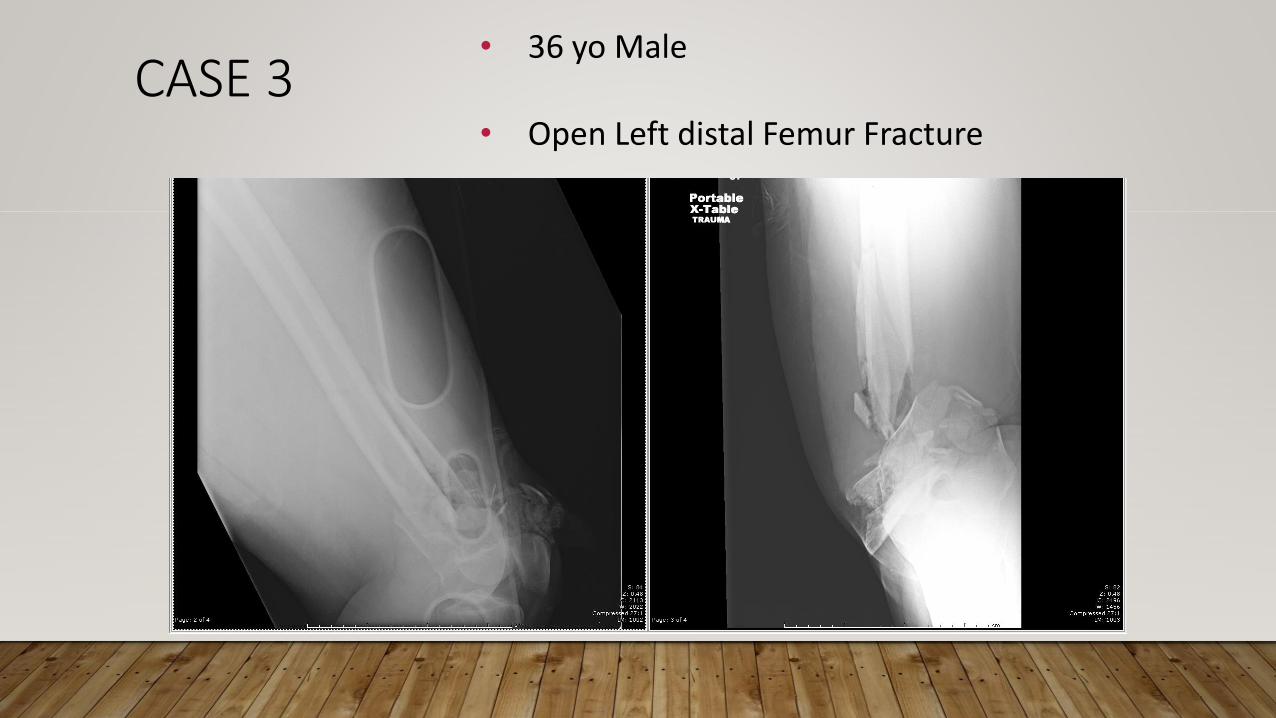
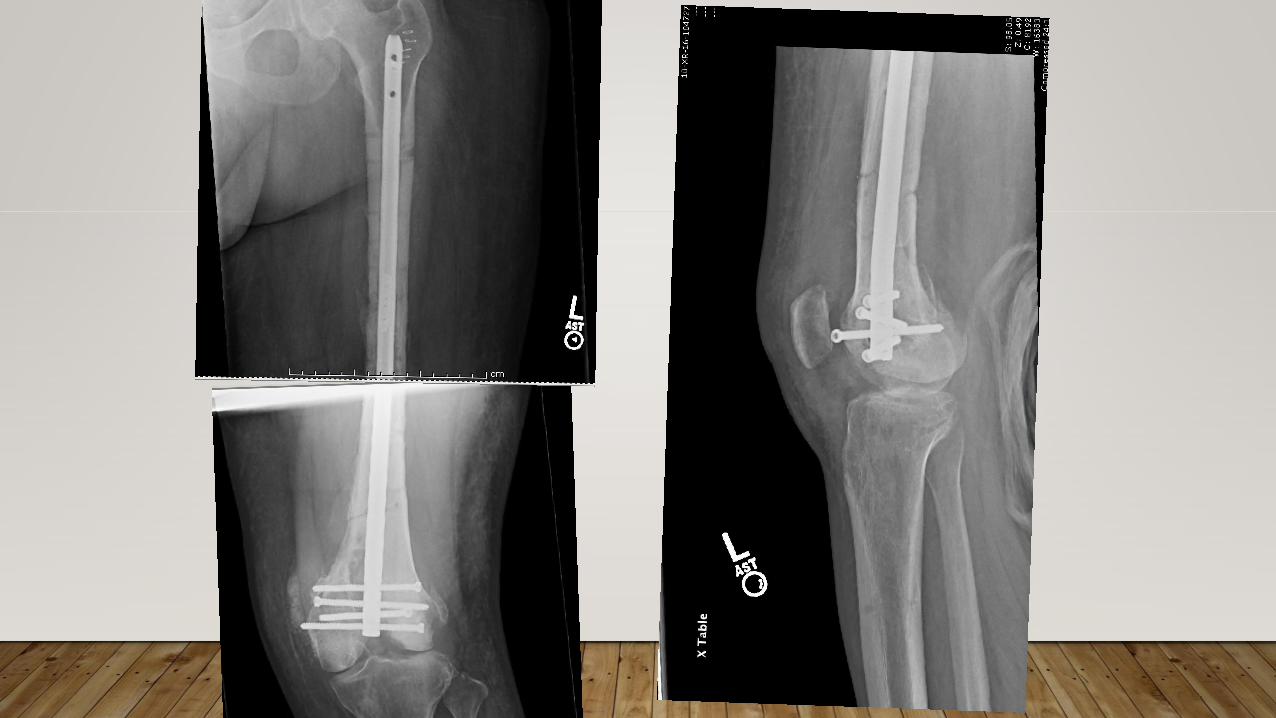
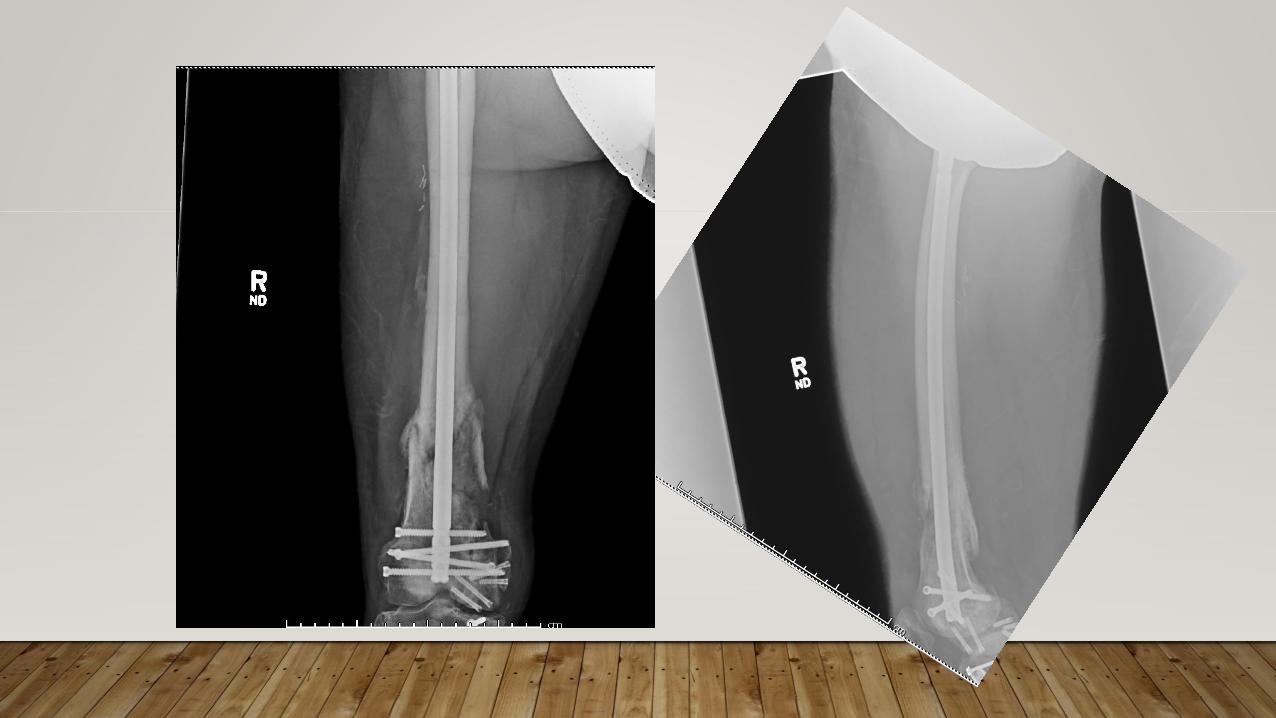
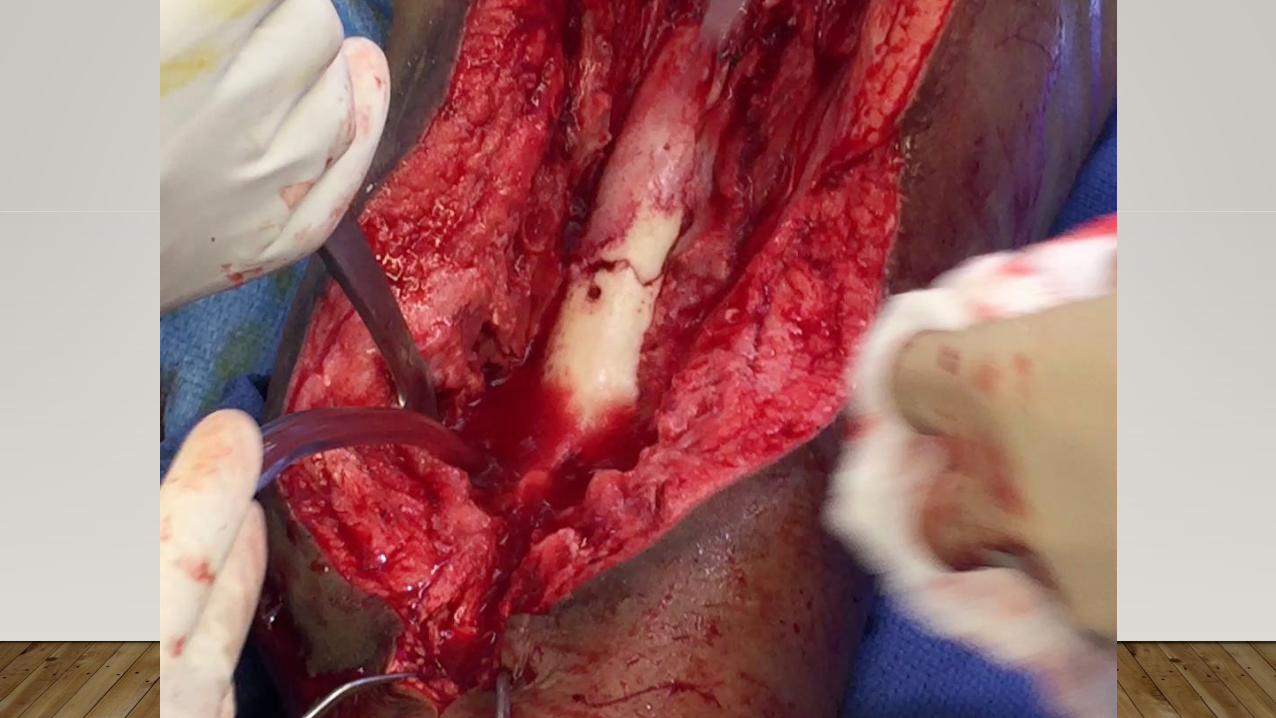
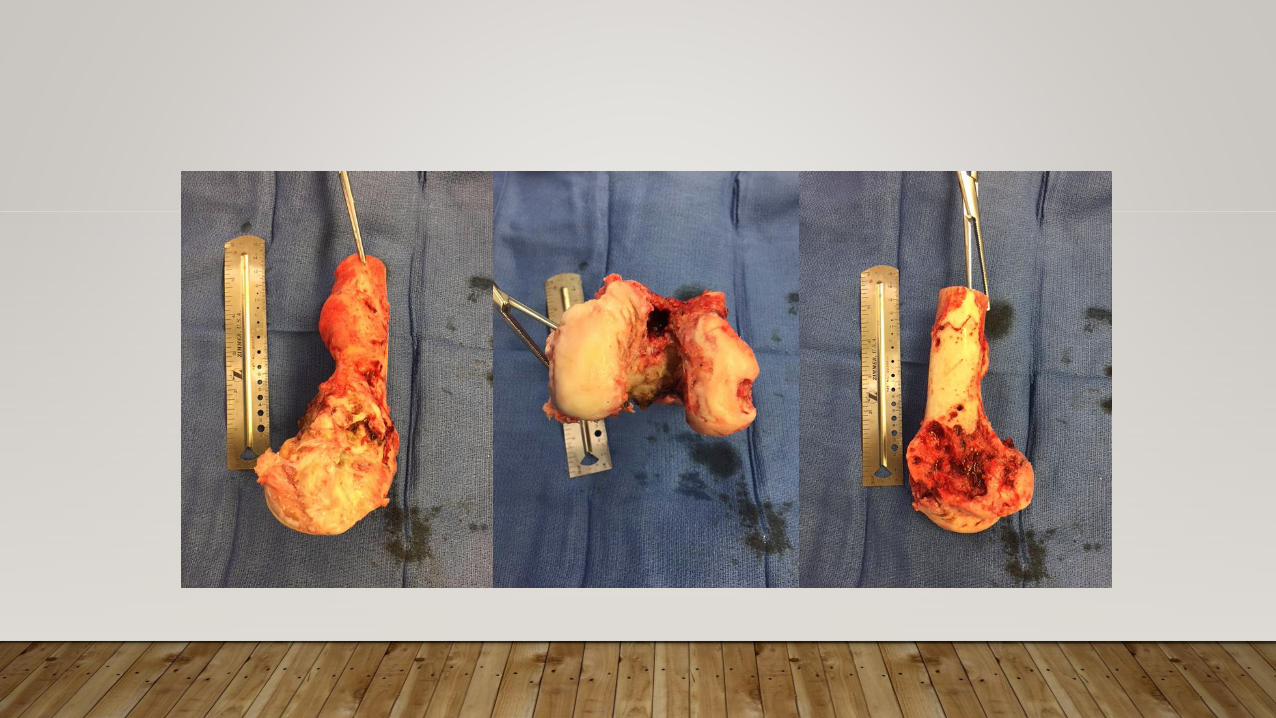
CASE 3• 36 yo Male
• Open Left distal Femur Fracture



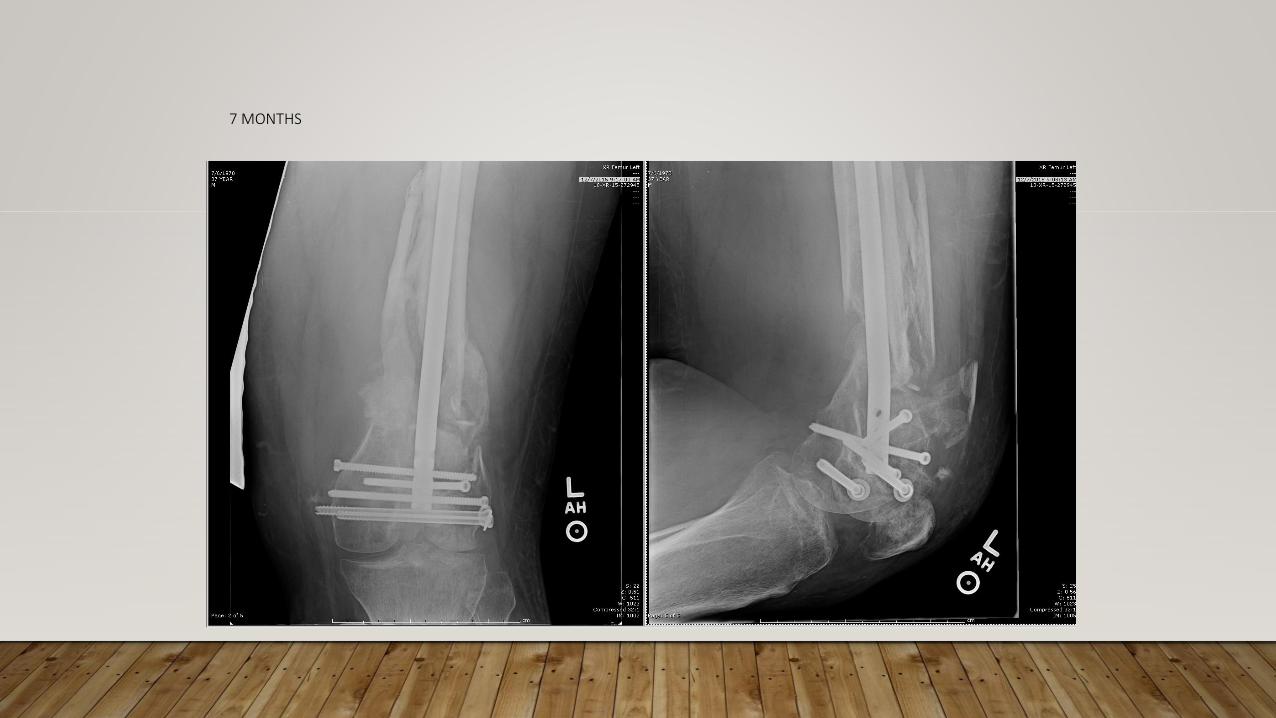
7 MONTHS

165

10 MONTHS

167
168

172
173
174

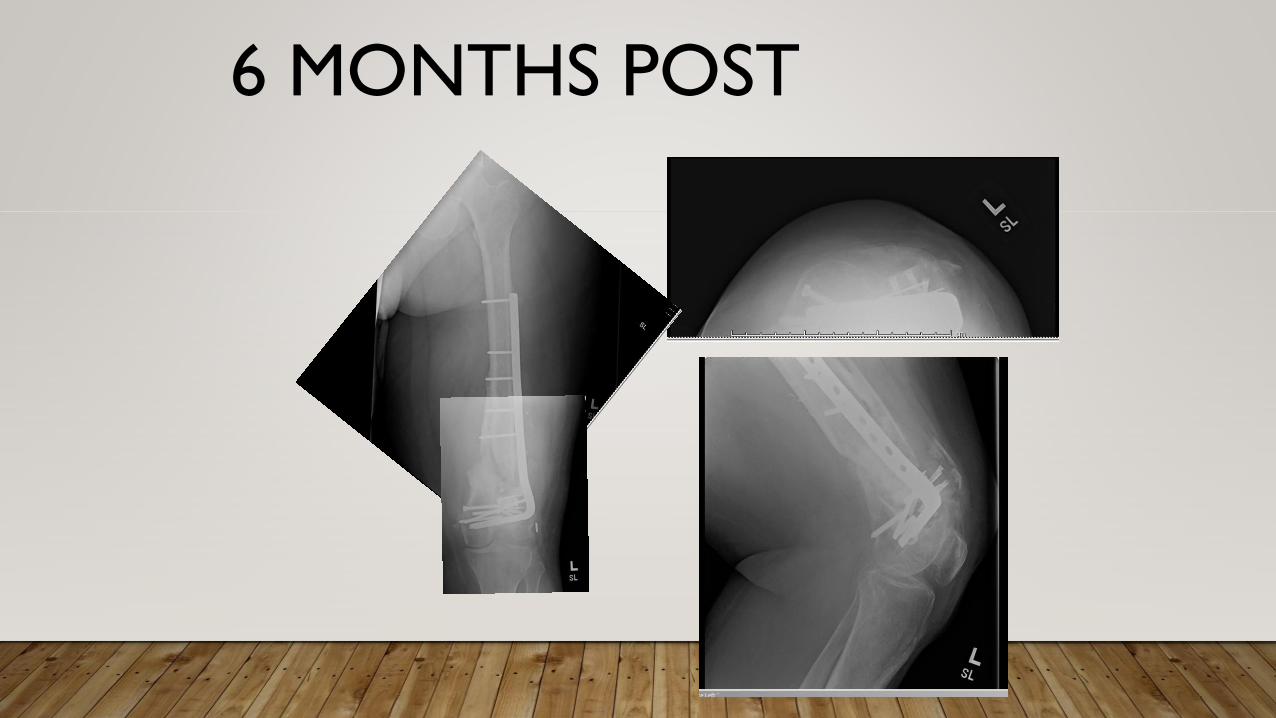
6 MONTHS POST

1 YEAR
Related Documents











