GINGIVAL ENLARGEMENT

CONTENTS
• Introduction • Classification• Indices • Inflammatory Enlargement• Enlargements associated with systemic diseases • Neoplastic enlargement• Drug-induced enlargement• Idiopathic gingival enlargement • False enlargement• Conclusion• References

INTRODUCTION
Hypertrophic gingivitis
Gingival hyperplasia
Gingival enlargement
Gingival overgrowth

CLASSIFICATION
A] Based on etiologic factors and pathologic changes
I. Inflammatory Enlargement - Acute
- ChronicII. Drug-induced enlargement
III. Enlargements associated with systemic diseases
IV. Neoplastic enlargement (gingival tumors) Benign tumors Malignant tumorsV. False enlargement
ii) Systemic diseases causing gingival enlargement 1. Leukemia 2.Granulomatous diseases (Wegener's granulomatosis, sarcoidosis)
i) Conditioned enlargement 1. Pregnancy
2. Puberty 3. Vitamin C deficiency 4. Plasma cell gingivitis 5. Nonspecific conditioned enlargement

B] Based on location and distribution I. Localized
II. Generalized
III. Marginal
IV. Papillary
V. Diffuse
VI. Discrete

INDICES
Bokenkamp & Bohnhorst 1994
Grade 0 No signs of gingival enlargement
Grade 1 Enlargement confined to IDP
Grade 2 Enlargement involves IDP & marginal gingiva
Grade 3 Enlargement covers three quarters / more of
crown

Degree of gingival hyperplasia according to modified index by Angelopoulos & Goaz 1972
Grade Hyperplasia Size Tooth coverage
0 No Normal No
1 Minimal <2 mm Cervical 3rd or less
2 Moderate 2-4 mm Middle 3rd
3 Severe >4 mm More than 2/3rd

Gingival overgrowth index- Mc Gaw et al 1987
Grade 0 No overgrowth, feather edge gingival margin
Grade 1 Blunting of gingival margin
Grade 2 Moderate gingival overgrowth (one third crown
length)
Grade 3 Marked gingival overgrowth (more than one
thirds of crown)

Clinical index for drug induced gingival overgrowth Ingles et al 1999
Grade 0
Grade 1
Grade 2
Grade 3
Grade 4
1.No overgrowth
2. slight stippling, no/slight granular appearance
3. knife edge margin
4. no increase in the density or size
1. Early overgrowth slight increase in density
2.marked stippling and granular appearance
3.tip of the papillae is round
4.probing depth ≤ 3mm
1.Moderate overgrowth increase
in size of the papillae and rolled
gingival margins
2. The contour concave or straight
3. buccolingual dimension of upto
2mm
4. Probing ≤ 6mm
5. Papillae retractable
1. Marked overgrowth
encroachment on the clinical
crown
2. The contour convex
3. Buccolingual dimension
≥ 3 mm
4. The probing depth ≥ 6mm
5. Papillae retractable
1. Severe overgrowth, profound
thickening of gingiva
2. Large % of the clinical crown
is covered
3. Papillae - retractable
4. Probing depth ≥ 6mm
5.buccolingual dimension 3mm

1. INFLAMMATORY ENLARGEMENT
CHRONIC
ACUTE
INFLAMMATORY Gingival abscess
Periodontal abscess

a. Chronic inflammatory enlargement
Etiology
Plaque accumulation &
retention
Poor oral hygiene
Anatomic abnormalities
Improper restoration
Orthodontic appliances
Malocclusion

Clinical Features 1.
Slight ballooning of IDP & marginal gingiva
Life preserver shaped bulge
Smooth , edematous , bleed easily
Localised / generalised
Progress- slowly and painlessly
Pseudopockets

Discrete sessile or pedunculated tumor like mass
Interproximal / marginal or attached gingiva
Slow growing and painless
Clinical Features
1. 2.

Histopathology
1.Soft and friable
2.Firm and resilient

B. ACUTE INFLAMMATORY ENLARGEMENT
1. GINGIVAL ABSCESSEtiology Foreign substances
Clinical features Marginal gingiva or IDP Red swelling smooth shiny surface Fluctuant and pointed with
a surface orifice expresses purulent exudate

2. PERIODONTAL ABSCESSLateral abscess / parietal abscess
Depending on location - Gingival
- Periodontal (Acute / Chronic)- Pericoronal
Meng et al ’99Depending on number - Single - Multiple

Etiology
PERIODONTITIS RELATED
Extension of infection from PD pocket
Lateral extension of inflammation
Pocket with a tortuous course
Incomplete removal of calculus

Etiology NON PERIODONTITIS
RELATED
Impaction of foreign bodies
Endodontic perforation
Lateral cyst infection
Factors affecting morphology of root

Signs and symptoms
Acute abscess
- Mild to severe discomfort- Localized red, ovoid swelling- Periodontal pocket- Mobility- Tooth elevation in the socket- Tenderness to percussion or
biting- Suppuration - Elevated temperature- Regional lymphadenopathy
Chronic abscess
- No pain or dull pain- Localized inflammatory lesion- Slight tooth elevation- Intermittent exudation- Fistulous tract often associated with deep pocket- Usually without systemic involvement

ENLARGEMENTS ASSOCIATED WITH SYSTEMIC DISEASES
Two mechanisms
1. Magnification of an existing inflammation initiated by dental plaque
- conditioned enlargement
2. Manifestation of the systemic disease independently of the inflammatory status of the gingiva
- systemic disease causing enlargement

1. Conditioned enlargement
• Systemic condition exaggerates or distorts usual gingival response to plaque
• Bacterial plaque
Types 1. Hormonal – pregnancy , puberty2. Nutritional – vitamin C deficiency3. AllergicNon specific conditioned

1. Marginal and generalised enlargement2. Single or multiple tumor like masses
Hormonal changes - Progesterone and estrogen- Vascular permeability – edema , inflammatory response
Subgingival microbiota – P. intermedia
a. Enlargement in pregnancy

1. Marginal enlargement
- Generalised , more prominent
interdentally
- Bright red or magenta colour
- Friable , smooth & shiny
surface
- Bleeding – spontaneously or
on slight provocation
“ Pregnancy rhinitis”

2. Tumor like gingival enlargement“Pregnancy tumor”
- Discrete mushroomlike , flattened
spherical mass
- Dusky red or magenta , smooth
glistening surface
- Doesnot invade underlying bone
- Semifirm – soft , friable
- sessile or pedunculated
- Painless unless its size and shape foster
accumulation of debris

Angiogranuloma Thickened epilthelium
Newly formed, engorged capillaries
Fibrous stroma
Inflammatory infiltrate
Histopathology

Treatment
• Removal of plaque and calculus
• Tumor like gingival enlargement - surgical excision and
SRP
• Recurrence
• Spontaneous reduction – termination of pregnancy

• Male and female adoloscents
• Areas of plaque accumulation
• Facial surface
• Marginal and interdental
Histopathology
- Similar to Chronic
inflammation
Difference
b. Enlargement in puberty

c. Enlargement in vitamin C deficiency
Clinical features - Bluish red , soft , friable, boggy- smooth & shiny surface- Haemorrhage – spontaneous /
slight provocation- Surface necrosis with
pseudomembrane formation
• Classic description of scurvy• Acute deficiency – hemorrhage , collagen degeneration , edema • modify response to plaque

d. Plasma cell gingivitis
• Atypical gingivitis / plasma cell gingivostomatitis• Plasma cell granuloma – localised form• Allergic in origin
Clinical features

• Pyogenic granuloma
Clinical features • Discrete spherical , tumorlike mass , pedunculated ,
smooth surface• Bright red or purple , friable or firm• Painless• Hemorrhage
e. Nonspecific conditioned enlargement

2.Systemic Disease That Cause Gingival Enlargement
1. Leukemiamalignant neoplasia of WBC precursors - diffuse replacement of bone marrow – proliferating leukemic cells
- abnormal number and forms of immature WBCs- widespread infiltrates
Acute myeloid leukemia

Clinical features• Diffuse / marginal • Localised / generalised• Overextension of marginal
gingiva• Discrete tumorlike
interproximal mass• Bluish red , shiny surface• Firm • Hemorrhage

Leukemic infiltration
Leukemic cell infiltration of gingival corium
Gingival thickness
Gingival pockets
Plaque accumulation
Secondary inflammatory lesion

Histopathology - Connective tissue – dense mass of immature and
proliferating leukocytes , engorged capillaries , edema
- Epithelium – degree of leukocytic infiltration and edema

2. Granulomatous diseasea.Wegeners granulomatosis
- Acute granulomatous necrotising lesions of respiratory tract , nasal and oral defects
- Acute necrotising vasculitis
Clinical features-oral mucosal ulcerations -delayed healing-Papillary enlargement – reddish purple ,- bleeds easily-Strawberry gingiva

Etiology - Unknown - Immunologically mediated tissue injury
Histopathology

b. Sarcoidosis- Unknown etiology- Involve any organ
Clinical features

NEOPLASTIC ENLARGEMENT
1. Benign tumors of gingiva Epulis
a. Fibroma
i) Giant cell fibromaii) Peripheral ossifying fibroma

b. Papilloma- Proliferations of surface epithelium associated with HPV- HPV 6 & 11

c. Peripheral Giant Cell GranulomaPeripheral giant cell tumors
d.Central Giant Cell Granuloma- Arise within the jaw – central cavitation

e. Leukoplakia• WHO: White patch or plaque that does not rub off & cannot be diagnosed as any other disease
• Associated use of tobacco Other probable factors: Candida, HPV-16, HPV-18 &
Trauma

Gingival Cyst:Develop from odontogenic epithelium or traumatically implanted sulcular epithelium

2. Malignant tumors of gingiva
Squamous cell carcinoma:• 90% of all Oral cancer• 6th –most common cancer in males • 12th - females • Most common malignant tumor of gingiva

Malignant melanoma:
• Rare tumor hard palate, maxillary gingiva -older persons
• Darkly pigmented, rapid growth, early metastasis

Thankyou

GINGIVAL ENLARGEMENT

Contents • Introduction • Classification• Indices • Inflammatory Enlargement• Enlargements associated with systemic diseases • Neoplastic enlargement• Drug-induced enlargement• Idiopathic gingival enlargement • False enlargement• Conclusion• References

Drug induced gingival enlargement
• Side effect – non dental treatment• First case – Kimball 1939
Drugs associated with gingival overgrowth
Anticonvulsants
PhenytoinSodium valproatePhenobarbitone
Vigabatrin
Immunosuppressants
Cyclosporin
Calcium channel blockers
Dihydropyridines Nifedipine
Felopdipine Amlodipine
Phenylalkylamine Verapamil
Benzothiazepine Diltiazem

Prevalence of DIGO
• 50 % - phenytoin ( Angelopoulous & Goaz 1972)
• 30% - Cyclosporine • 10% - Nifedipine
(Seymour 1987 , Barclay 1992)
• In India, 57% of epileptic children - aged 8-13 years - phenytoin therapy
Prasad et al 2002

Risk factors for DIGO
Risk factors
Age
Sex
Drug variables
Concomitant medication
Genetic factors
Periodontal variables

•Early studies on phenytoin – teenagers , hospitalised or institutionalised•Two community based studies – 1. mean age 40.6 years –
Thomason 19922.Younger age – Casetta 1997 •Cyclosporin - children
(Daley 1994)•Calcium channel blockers – not applicable •Middle age and older
Circulating androgen + gingival fibroblasts
Testosterone – 5α dihydrotestosterone
PHT – enhances metabolism
Circulating androgen – adoloscents and teenagers
Age

•Phenytoin – no difference
Hassell 1981
•CsA- Male
•CCBs – male 3 times more
Sex Concomitant medication
•Nifedipine + cyclosporin –
increases prevalence but not the
severity
•Polypharmacy – PHT –
metabolised by P450
•other anticonvulants – induce
P450 isoenzyme

Drug variables
1. Drug dosage – poor predictor•Dose / pts body weight•PHT & CCB – therapeutic drug level 7-10 days•Cyclosporin – trough concentration•Area under plasma/ serum concentration time curve (AUC)
2. Type of preparation CsA – solution - 37 % - early onset – higher in saliva capsules – 43%
(Wondimu 1996)3. Salivary concentration PHT &CsA – salivary concentration positive correlation with OG
4. GCF – nifedipine

Genetic factors
Cytochrome P450 gene
polymorphism
HLA- DR1 – protection against
OG
HLA-DR2 – OG susceptible
Pernu 1994
Periodontal variables
Plaque scores & gingival inflammation – exacerbate OG

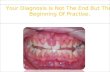
General features of DIGO
Painless beadlike enlargement of IDP
Marginal gingiva
Massive tissue fold
Plaque control difficult
Secondary inflammatory process
Combined enlargement

• Generalised
• Not in edentulous areas
• Chronic , slow
• Recurs
• Discontinuation of drug – spontaneous reduction

Histopathology

Anticonvulsants
• Epilepsy –
• First antiepileptic drug – phenytoin – DOC
• Merritt & Putman 1938
• 1st DIGO case
• Active metabolite – 5 parahydroxyphenyl – 5
phenylhydantoin
• Other hydantoins – ethotoin , mephenytoin
• Other anticonsulvant – succinimides , valproic acid

Anticonvulsant properties
1. Reduces excessive discharge2. Reduces spread of excitation Stabilising neuronal membraneNa – prevents influx K – blocks outward flow Ca – decreases calcium influx

• Clinical features
1. Esthetic disfigurement, 2. Malpositioning of teeth, 3. Interfere masticatory function, 4. Speech, 5. Oral hygiene

Theories of pathogenesis
1. Gingival fibroblasts1. High activity2. Low activity
Hasell 1983

2. Lack of collagen breakdown• FBS – inactive collagenase• mRNA collagenase levels are diminished• Gene expression of MMP-1, 2, and 3 was reduced by
phenytoin administration, • the TIMP-1 mRNA was markedly augmented
2005, Kato et al
• macrophages pretreated with phenytoin - lower production of MMPs
• intracellular pathway - related to a lower expression of α2β1-integrin

3. Non collagenous matrix
• Non collagenous matrix – 20% of dry weight
• Increased hexoamine , uronic acid
• Increased sulphated GAG
• Higher volume density of non collagenous protein
compared to collagenousDahllof et al 1984

4. Role of growth factors
• TGF-β - stimulating collagen biosynthesis
• latency-associated protein (LAP) - TGF-β inactive
• CTGF levels are increased
• Epithelial mesenchymal transition
• PDGF – PHT facilitated expression of PDGF B
– 6 times


5.Immunosuppression
sIgA - decreased
Repair process
Gingival overgrowth

6. PHT and Adrenal gland
Suppression of ACTH production
Suppression of adrenocortical function
Reduction of glucocorticoid synthesis
compensatory increase in the Somatotrophic hormone
Fibroblast proliferation

7. PHT and folic acid depletion
Decreases absorption of
folic acid
Blocks transport - intestinal epithelium
Enzyme folate reductase
Folic acid – DNA synthesis
Impaired maturation – sulcular epithelium
CT susceptible to inflammation

Cyclosporin induced gingival overgrowth
• Cyclosporin (CsA) - 1972 James Borel
• Organ transplantation , autoimmune disease
• Monotherapy - CsA• 2 drugs – CsA + cortisone / dihydropyridine• 3 drugs – CsA + cortisone + azathiprine
• Cyclosporin-induced gingival overgrowth – 1983 Rateitschak- Plu¨ss et
al

Cyclosporin and T cells
• a) Inhibits T cell helper function to accessory cells - interleukin 1
• b) Prevents the formation of receptors to interleukin I on the membrane of the T-cell.
• c) Renders T-cells unresponsive to - interleukin 2 .


Pathogenesis of Cs GO
Cyclosporin
Cytokines
Extracellular matrix
metabolism
Cell proliferationApoptosis
SynthesisDegradation -I/C pathway-E/C pathway

• More in labial aspect
• Soft, red or bluish-red, extremely fragile and bleed easily, more hyperemic than PIGO

Histopathology

Calcium channel blockers
• CCB’s introduced in 1980’s
• Used extensively in the management of CV disorders(HTN, angina, coronary artery spasm, cardiac arrythmia)
• NIFEDIPINE angina, mild to moderate HTN
• Relaxes smooth muscles and dilates the coronary arteries
• NIGO 1984 by Lederman et al

Pathogenesis: Nifedipine• Affects calcium metabolism similar to phenytoin• Role of TGF beta• Heparan GAG
Verapamil Subpopulation of fibroblast

• IDPmarginal attached
• Lobulated and nodular
• Anteriorly, facial surface
• Inflammation Combination enlargement


Idiopathic gingival enlargement
• Gingivomatosis , Elephantiasis, Idiopathic fibromatosis, Hereditary gingival hyperplasia , Congenital familial fibromatosis , Hereditary gingival fibromatosis
• rare oral disease • autosomal dominant
• hypertrichosis, mental retardation and epilepsy

• Nodular form• Symmetric form- most common type• During eruption of permanent teeth

• most common effects• diastemas, • Malpositioning of teeth • prolonged retention of primary teeth• cover the dental crowns • the alveolar bone is not affected (Bittencourt et al. 2000).


TGF 1
Increased proliferationHGF cells
Low levels of MMP 1, MMP 2
Myofibroblasts
High level of extracellular
matrix proteins (collagen)
TGF 1
Gingival overgrowth

False enlargement
a. Underlying osseous lesions• Commonly Tori, Exostosis
• Also seen in Paget’s disease, Fibrous dysplasia, Cherubism, Central giant cell granuloma, Ameloblastoma, Osteoma and Osteosarcoma

b. Underlying dental lesions• Various stages of eruption of primary dentition labial
gingiva• Developmental enlargement

Conclusion
Gingival enlargement are multifactorial and complex in nature , which may be in respone to various interaction between host and environment. GO considerably reduce the quality of life and may result in serios emotional and social problems due to esthetics and functionality hence the prevention and treatment based on the understanding the cause and underlying pathologic changes ,

References
• Newman MG , Takei HH , Klokkevold PR , Carranza FA . Carranza’s Clinical Periodontology, 10th edition
• Marshall R , Bartold M A clinical review of drug induced gingival overgrowth Australian dental journal 1999 ;44:4 219-232
• Seymour RA, Ellis JS, Thomason JM: Risk factors for drug-induced gingival overgrowth.J Clin Periodontol 2000; 27: 217–223.
• Seymour RA , Thomasan JM Pathogenesis of Drug Induced Gingival Overgrowth- J Clin Periodontol 1996;23:165-175
• Strawberry –like gingival tumor as first sign of Wegener’s Granulomatosis. J Periodontol 2008; 79: 1297-1303
• Seymour RA and Heasman PA: Drugs and the periodoniium. J Clin Periodontol 1988: 15: 1-16

• Jˆoice Dias Corrˆea et al Phenytoin-Induced Gingival Overgrowth: A Review of the Molecular, Immune, and Inflammatory Features ISRN Dentistry 2011,1-8
• Williamw . Hallmo&n J Effrey A. Rossmann The role of drugs in the pathogenesis of gingival overgrowth A collective review of current concepts Periodontology 2000, Vol. 21, 1999, 176-196
• Paulom. Camargo, Philip R.Melnick, Flavia Q. M. Pirih, Rodrigo Lagos & Henry H. Takei Treatment of drug-induced gingival enlargement: aesthetic and functional considerations Periodontology 2000, Vol. 27, 2001, 131–138
• Dustin Tedesco and Lukas Haragsim Cyclosporine: A Review Journal of Transplantation Volume 2012
• Bitu CC, Sobral LM, Kellermann MG, Martelli-Junior H, Zecchin KG, Graner E, Coletta RD. Heterogeneous presence of myofibroblasts in hereditary gingival fibromatosis. J Clin Periodontol 2006; 33: 393–400

Thankyou