IJSS Case Reports & Reviews | August 2014 | Vol 1 | Issue 3 20 Gingival Enlargement: Revisited: A Case Series Atul Anand Bajoria 1 , M L Asha 2 , Medha Babshet 3 , Preeti Patil 3 , Piyush Sukhija 1 1 Post-graduate, Department of Oral Medicine and Radiology, Sri Hasanamba Dental College and Hospital, Hassan, Karnataka, India, 2 Professor and Head, Department of Oral Medicine and Radiology, Sri Hasanamba Dental College and Hospital, Hassan, Karnataka, India, 3 Assistant Professor, Department of Oral Medicine and Radiology, Sri Hasanamba Dental College and Hospital, Hassan, Karnataka, India Gingival enlargement can be hereditary or acquired. More than 20 prescription medications are associated with gingival overgrowth. A detailed review on the risk factors and pathogenesis from various peer reviewed journals has been discussed in this article. e aim was to discuss the role of drugs causing gingival enlargement, the hereditary gingival fibromatosis (HGF) and its possible pathogenesis. e following case series highlights four cases of gingival enlargement, one being a case of HGF and the other three being drug-induced gingival enlargement. Variable etiopathogenesis such as age, genetic predisposition, pharmacokinetic variables, tissue homeostasis, inflammation and growth factors have been associated with this disease. Inflammatory changes that occur within the gingival tissues appear to orchestrate the interaction between the “modified fibroblast” and the drug. Alternatively, these drugs influence directly the inflammatory response in the form of enlargement. is information is valuable for the clinician as it will have implication to treat the patient effectively. Keywords: Drug induced, Fibroblasts, Gingival overgrowth categories: Anticonvulsants, calcium channel blockers and immunosuppressant’s. 4 The following case series highlights four cases of gingival enlargement, one being a case of hereditary gingival fibromatosis (HGF) and the other three being drug-induced gingival enlargement. CASE REPORTS Case 1 A 22-year-old female patient came with a chief complaint of forwardly placed teeth in the upper front region. Patient gave a history of gingival enlargement since childhood. Family history revealed patient’s mother having similar gingival presentation. The medical history of the patient was not relevant. On examination, generalized enlargement of the interdental, marginal and aached gingiva was seen in both the arches, more pronounced on the buccal aspect. Surface was lobulated in the posterior aspect and the anterior aspect was smooth. Stippling was maintained. Gingiva was covering the cervical third of the anteriors, middle third of the canine and premolars and unto the occlusal aspect of the molars. Displacement was seen in the posterior teeth in both the arches. On palpation, the gingiva was firm in consistency, non-tender with pus discharge from the gingival sulcus of the lower posterior teeth. All complement of teeth was present except 18 and 28. There were root stumps in relation to 37, 38 and 48. Based on these clinical findings a provisional diagnosis of HGF was given and a differential diagnosis of inflammatory gingival enlargement was considered (Figures 1 and 2). INTRODUCTION Increase in size of gingiva is a common feature of gingival disease. This is clinically designated as gingival enlargement or gingival overgrowth. The terms overgrowth or enlargement are descriptive terms. Hyperplasia is a histologic term used to describe the increase in a number of cells. It should be distinguished from hypertrophy, which is an overgrowth due to increased size of the cells. Gingival enlargement is a gingival dimorphism associated with multiple factors. It is characterized by evident growth of the gingiva vertically toward the incisal edge of the clinical crown and horizontally toward the buccal-lingual area and is more prevalent in the buccal surfaces of the anterior teeth. 1 Various researchers have described multiple indices to evaluate gingival enlargement of which the Miranda and Brunet index had a better sensitivity in evaluating the gingival enlargement. 1 Classification of gingival enlargement is based on the degree of overgrowth as: Grade 0: No signs of gingival enlargement; Grade I: Enlargement confined to interdental papilla; Grade II: Enlargement involving papilla and marginal gingiva; and Grade III: Enlargement covering three-quarters or more of the crown. 2 Gingival enlargement can be hereditary or acquired. More than 20 prescription medications are associated with gingival overgrowth. 3 Drugs associated with gingival enlargement can be broadly divided into three Corresponding Author: Dr. Atul Anand Bajoria, Department of Oral Medicine and Radiology, Sri Hasanamba Dental College and Hospital, Hassan, Karnataka, India. Mobile: +91-9964837056. E-mail: [email protected] Case Report

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

IJSS Case Reports & Reviews | August 2014 | Vol 1 | Issue 320
Gingival Enlargement: Revisited: A Case Series
Atul Anand Bajoria1, M L Asha2, Medha Babshet3, Preeti Patil3, Piyush Sukhija1
1Post-graduate, Department of Oral Medicine and Radiology, Sri Hasanamba Dental College and Hospital, Hassan, Karnataka, India, 2Professor and Head, Department of Oral Medicine and Radiology, Sri Hasanamba Dental College and Hospital, Hassan, Karnataka, India, 3Assistant Professor, Department of Oral Medicine and Radiology, Sri Hasanamba Dental College and Hospital, Hassan, Karnataka, India
Gingival enlargement can be hereditary or acquired. More than 20 prescription medications are associated with gingival overgrowth. A detailed review on the risk factors and pathogenesis from various peer reviewed journals has been discussed in this article. The aim was to discuss the role of drugs causing gingival enlargement, the hereditary gingival fibromatosis (HGF) and its possible pathogenesis. The following case series highlights four cases of gingival enlargement, one being a case of HGF and the other three being drug-induced gingival enlargement. Variable etiopathogenesis such as age, genetic predisposition, pharmacokinetic variables, tissue homeostasis, inflammation and growth factors have been associated with this disease. Inflammatory changes that occur within the gingival tissues appear to orchestrate the interaction between the “modified fibroblast” and the drug. Alternatively, these drugs influence directly the inflammatory response in the form of enlargement. This information is valuable for the clinician as it will have implication to treat the patient effectively.
Keywords: Drug induced, Fibroblasts, Gingival overgrowth
categories: Anticonvulsants, calcium channel blockers and immunosuppressant’s.4
The following case series highlights four cases of gingival enlargement, one being a case of hereditary gingival fibromatosis (HGF) and the other three being drug-induced gingival enlargement.
CASE REPORTS
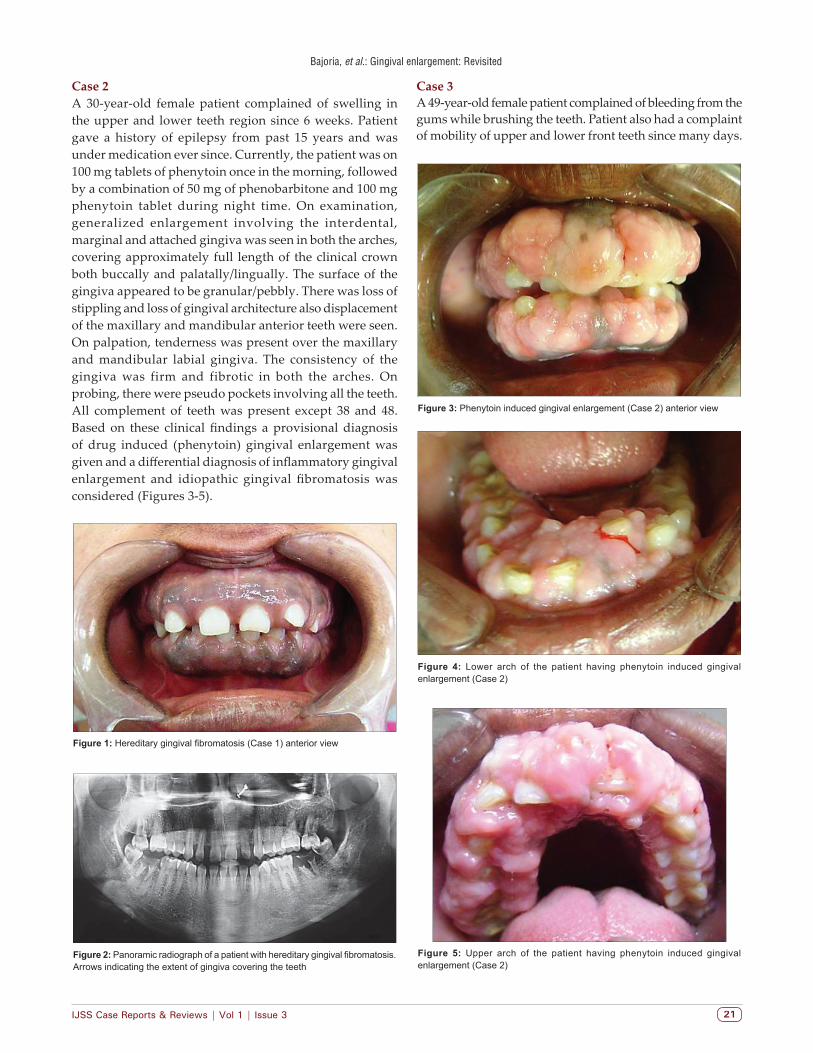
Case 1A 22-year-old female patient came with a chief complaint of forwardly placed teeth in the upper front region. Patient gave a history of gingival enlargement since childhood. Family history revealed patient’s mother having similar gingival presentation. The medical history of the patient was not relevant. On examination, generalized enlargement of the interdental, marginal and attached gingiva was seen in both the arches, more pronounced on the buccal aspect. Surface was lobulated in the posterior aspect and the anterior aspect was smooth. Stippling was maintained. Gingiva was covering the cervical third of the anteriors, middle third of the canine and premolars and unto the occlusal aspect of the molars. Displacement was seen in the posterior teeth in both the arches. On palpation, the gingiva was firm in consistency, non-tender with pus discharge from the gingival sulcus of the lower posterior teeth. All complement of teeth was present except 18 and 28. There were root stumps in relation to 37, 38 and 48. Based on these clinical findings a provisional diagnosis of HGF was given and a differential diagnosis of inflammatory gingival enlargement was considered (Figures 1 and 2).
INTRODUCTION
Increase in size of gingiva is a common feature of gingival disease. This is clinically designated as gingival enlargement or gingival overgrowth. The terms overgrowth or enlargement are descriptive terms. Hyperplasia is a histologic term used to describe the increase in a number of cells. It should be distinguished from hypertrophy, which is an overgrowth due to increased size of the cells. Gingival enlargement is a gingival dimorphism associated with multiple factors. It is characterized by evident growth of the gingiva vertically toward the incisal edge of the clinical crown and horizontally toward the buccal-lingual area and is more prevalent in the buccal surfaces of the anterior teeth.1
Various researchers have described multiple indices to evaluate gingival enlargement of which the Miranda and Brunet index had a better sensitivity in evaluating the gingival enlargement.1
Classification of gingival enlargement is based on the degree of overgrowth as: Grade 0: No signs of gingival enlargement; Grade I: Enlargement confined to interdental papilla; Grade II: Enlargement involving papilla and marginal gingiva; and Grade III: Enlargement covering three-quarters or more of the crown.2
Gingival enlargement can be hereditary or acquired. More than 20 prescription medications are associated with gingival overgrowth.3 Drugs associated with gingival enlargement can be broadly divided into three
Corresponding Author: Dr. Atul Anand Bajoria, Department of Oral Medicine and Radiology, Sri Hasanamba Dental College and Hospital, Hassan, Karnataka, India. Mobile: +91-9964837056. E-mail: [email protected]
Case Report
Bajoria, et al.: Gingival enlargement: Revisited
IJSS Case Reports & Reviews | Vol 1 | Issue 3 21
Case 3A 49-year-old female patient complained of bleeding from the gums while brushing the teeth. Patient also had a complaint of mobility of upper and lower front teeth since many days.
Case 2A 30-year-old female patient complained of swelling in the upper and lower teeth region since 6 weeks. Patient gave a history of epilepsy from past 15 years and was under medication ever since. Currently, the patient was on 100 mg tablets of phenytoin once in the morning, followed by a combination of 50 mg of phenobarbitone and 100 mg phenytoin tablet during night time. On examination, generalized enlargement involving the interdental, marginal and attached gingiva was seen in both the arches, covering approximately full length of the clinical crown both buccally and palatally/lingually. The surface of the gingiva appeared to be granular/pebbly. There was loss of stippling and loss of gingival architecture also displacement of the maxillary and mandibular anterior teeth were seen. On palpation, tenderness was present over the maxillary and mandibular labial gingiva. The consistency of the gingiva was firm and fibrotic in both the arches. On probing, there were pseudo pockets involving all the teeth. All complement of teeth was present except 38 and 48. Based on these clinical findings a provisional diagnosis of drug induced (phenytoin) gingival enlargement was given and a differential diagnosis of inflammatory gingival enlargement and idiopathic gingival fibromatosis was considered (Figures 3-5).
Figure 1: Hereditary gingival fibromatosis (Case 1) anterior view
Figure 2: Panoramic radiograph of a patient with hereditary gingival fibromatosis. Arrows indicating the extent of gingiva covering the teeth
Figure 5: Upper arch of the patient having phenytoin induced gingival enlargement (Case 2)
Figure 4: Lower arch of the patient having phenytoin induced gingival enlargement (Case 2)
Figure 3: Phenytoin induced gingival enlargement (Case 2) anterior view

Bajoria, et al.: Gingival enlargement: Revisited
IJSS Case Reports & Reviews| August 2014 | Vol 1 | Issue 322
She was a known hypertensive from past 10 years and under medication for the same (atenolol 50 mg and amlodipine 5 mg combination tablet in the morning). On examination generalized enlargement involving the interdental, marginal and attached gingival, covering approximately full length of the clinical crown both buccally and palatally/lingually in the posterior aspect of both the arches. Both the buccal and palatal/lingual gingiva was enlarged on the right side, whereas only the buccal gingiva was enlarged on the left side. Stippling was present. On palpation, tenderness was present over the maxillary and mandibular labial gingiva. The overall consistency of the gingiva was firm and fibrotic. There was pus discharge from the gingival sulcus in relation to 12, 38 and 45. Teeth present were 15, 14, 12, 24, 25, 26, 27, 38, 35, 34, 32, 42, 43, 44, 45 and 46 of which 12, 32 and 42 were Grade II mobile. Based on these clinical findings, a provisional diagnosis of drug induced (amlodipine) gingival enlargement was given and a differential diagnosis of inflammatory gingival enlargement and idiopathic gingival fibromatosis was considered (Figure 6).
Case 4A 45-year-old female patient came with a chief complaint of swelling in the right lower back tooth region from past 1 week. Patient was a known hypertensive from past 2 years and was under medication for the same (amlodipine 5 mg tablet once daily). Patient was also a known diabetic from past 2 years and taking metformin 1000 mg daily. On examination, generalized enlargement of the interdental and the marginal gingiva of both the arches were present, more pronounced in the lower arch having a pebbly surface. Stippling was present and the normal gingival architecture was lost in the lower arch. Midline diastema in relation to 11 and 21 was also seen with a high frenal attachment. On palpation, the gingiva was firm and fibrotic in consistency. Tenderness was present over the gingiva in relation to 46. Pus discharge from the gingival sulcus was observed in relation to 46, with Grade II mobility of 45 and 46. Apart from the upper canines, all complement of teeth was present with over retained deciduous canine bilaterally in the upper arch. Based on these clinical findings, a provisional diagnosis of drug induced (amlodipine) gingival enlargement was given and a differential diagnosis of inflammatory gingival enlargement and idiopathic gingival fibromatosis was considered (Figure 7).
DISCUSSION
HGF is a rare benign, asymptomatic, non-hemorrhagic and non-exudative proliferative lesion of the gingival tissue, which may manifest either as a nodular or symmetric form resulting in uniform enlargement of the gingiva. It may occur alone or as a part of syndrome, which include autosomal-dominant (Laband and Rutherford) or autosomal-recessive syndromes (Cross, Murray–Puretic–Dresher and Ramon).5
The mechanism behind drug-induced gingival hyperplasia involves inflammatory and non-inflammatory pathways (Figure 8).6-8
Kimball in 1939 reported the first case of phenytoin induced gingival enlargement.9
Phenytoin induced gingival hyperplasia has a higher prevalence rate of 50% when compared to cyclosporine and calcium channel blockers.10 Amlodipine is a third generation dihydropyridine calcium channel blocker used for the management of hypertension and angina.11
Phenytoin and amlodipine inhibit the intracellular calcium ion uptake which stimulates the gingival fibroblasts. However, only in those patients who are diagnosed with drug-induced gingival enlargement has fibroblasts with an abnormal susceptibility to the drug. The presence of this differential proportion of fibroblasts in these patients’ exhibits an abnormal fibrogenic response.12 Histologically
Figure 7: Amlodipine induced gingival enlargement (Case 4) anterior view
Figure 6: Amlodipine induced gingival enlargement (Case 3) anterior view
Bajoria, et al.: Gingival enlargement: Revisited
IJSS Case Reports & Reviews | Vol 1 | Issue 3 23
elevated expression of transforming growth factor beta (TGF-β) has been reported in lamina propria of phenytoin induced gingival hyperplasia.13
Phenytoin also up regulates B-chain of platelet derived growth factor - BB which acts as a mitogen and chemo-attractant for fibroblasts14-16 which increases the secretion of basic fibroblast growth factor leading to increased proliferation of gingival fibroblasts.13
Elevated levels of interleukin 1 beta and interleukin 6 have been reported in drug induced hyperplasia. They target the fibroblasts that trigger the proliferation of fibroblasts and exert the positive regulation on collagen and glycosaminoglycans synthesis.17
In cyclosporine, gingival enlargement reduced levels of matrix metalloproteinases one and three have been found, which leads to accumulation of extra cellular matrix (ECM) component.18
Elevated levels of TGF-β have been found in the gingival crevicular fluid (GCF) of patients diagnosed with cyclosporine-induced gingival enlargement, which increases the accumulation of ECM.19
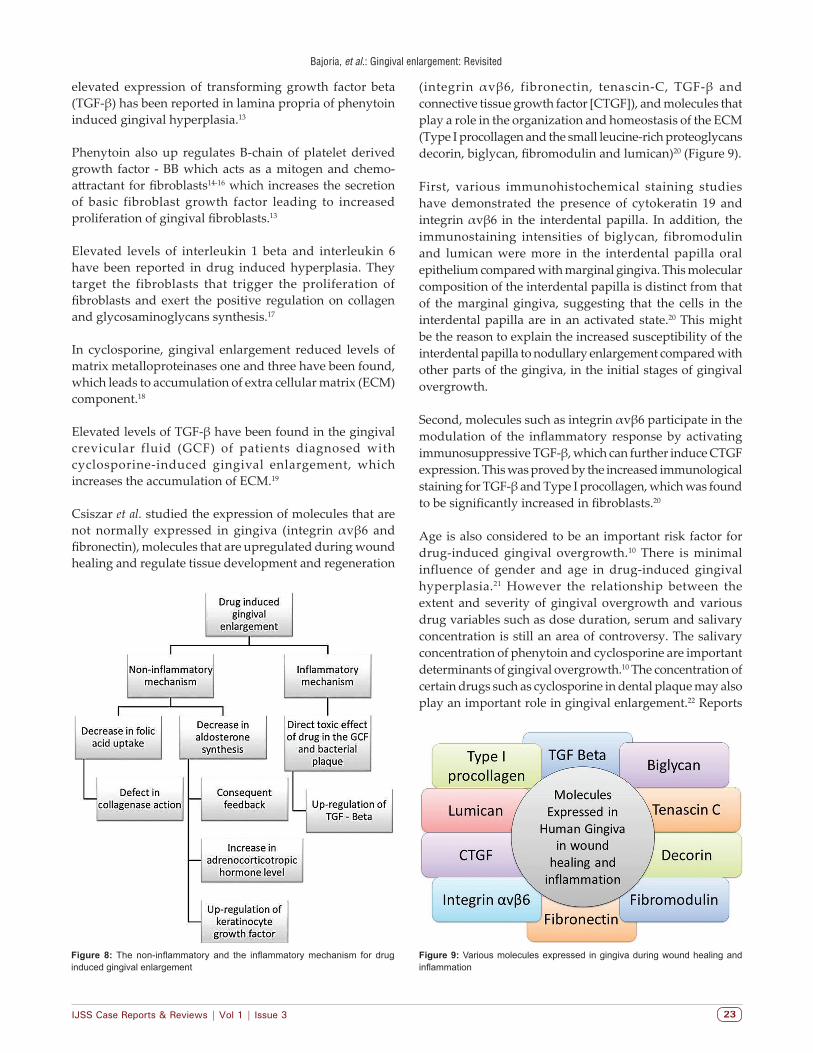
Csiszar et al. studied the expression of molecules that are not normally expressed in gingiva (integrin αvβ6 and fibronectin), molecules that are upregulated during wound healing and regulate tissue development and regeneration
(integrin αvβ6, fibronectin, tenascin-C, TGF-β and connective tissue growth factor [CTGF]), and molecules that play a role in the organization and homeostasis of the ECM (Type I procollagen and the small leucine-rich proteoglycans decorin, biglycan, fibromodulin and lumican)20 (Figure 9).
First, various immunohistochemical staining studies have demonstrated the presence of cytokeratin 19 and integrin αvβ6 in the interdental papilla. In addition, the immunostaining intensities of biglycan, fibromodulin and lumican were more in the interdental papilla oral epithelium compared with marginal gingiva. This molecular composition of the interdental papilla is distinct from that of the marginal gingiva, suggesting that the cells in the interdental papilla are in an activated state.20 This might be the reason to explain the increased susceptibility of the interdental papilla to nodullary enlargement compared with other parts of the gingiva, in the initial stages of gingival overgrowth.
Second, molecules such as integrin αvβ6 participate in the modulation of the inflammatory response by activating immunosuppressive TGF-β, which can further induce CTGF expression. This was proved by the increased immunological staining for TGF-β and Type I procollagen, which was found to be significantly increased in fibroblasts.20
Age is also considered to be an important risk factor for drug-induced gingival overgrowth.10 There is minimal influence of gender and age in drug-induced gingival hyperplasia.21 However the relationship between the extent and severity of gingival overgrowth and various drug variables such as dose duration, serum and salivary concentration is still an area of controversy. The salivary concentration of phenytoin and cyclosporine are important determinants of gingival overgrowth.10 The concentration of certain drugs such as cyclosporine in dental plaque may also play an important role in gingival enlargement.22 Reports
Figure 8: The non-inflammatory and the inflammatory mechanism for drug induced gingival enlargement
Figure 9: Various molecules expressed in gingiva during wound healing and inflammation

Bajoria, et al.: Gingival enlargement: Revisited
IJSS Case Reports & Reviews| August 2014 | Vol 1 | Issue 324
of high local concentration of amlodipine and phenytoin in the GCF of patients having gingival enlargement have been demonstrated,23,24 but it does not appear to be related to the extent of gingival overgrowth.25 An increased enlargement of the gingiva was observed in organ transplant patients receiving a combination of nifedipine and cyclosporine.26 Patients having high plaque score and gingival inflammation have a higher risk of developing drug-induced gingival enlargement than in patients having a good oral hygiene.27 The fibroblast heterogeneity till date remains the key factor for drug-induced gingival enlargement.10
There are mainly six risk factors responsible for drug-induced gingival overgrowth (Table 1).17
CONCLUSION
Gingival overgrowth is disfiguring, and can interfere in mastication and speech; hence a thorough understanding of the pathogenesis is essential. It is possible that the specific phenotype is inherent to the cells in the gingiva based on its anatomical location or that the cells are activated because of the presence of mild localized inflammation, even in clinically healthy tissue. Furthermore, the reason for the presence of a distinct cell phenotype in the interdental papilla oral epithelium and the function of the differentially expressed molecules are not clear.
Inflammatory changes that occur within the gingival tissues appear to orchestrate the interaction between the “modified fibroblast” and the drug. Alternatively, these drugs
influence directly the inflammatory response in the form of enlargement. This information is valuable for the clinician as it will have implication to treat the patient effectively. Newer molecular approaches are required to establish the pathogenesis of gingival overgrowth thus aiding in novel preventive and therapeutic modalities.
ACKNOWLEDGMENTS
We express our deep sense of gratitude and profound thanks to my respected teacher Dr. Asha ML, Professor and Head of the Department of Oral Medicine and Radiology, Sri Hasanamba Dental College and Hospital, Hassan for her constant encouragement, guidance and support in every aspect of this study. We are grateful to Dr. S Ravindra, Principal, Sri Hasanamba Dental College and Hospital, Hassan for providing us with all the college facilities to carry out this study successfully.
REFERENCES
1. Miranda J, Brunet L, Roset P, Farré M, Mendieta C. Reliability of two measurement indices for gingival enlargement. J Periodontal Res 2012;47:776-82.
2. Inglés E, Rossmann JA, Caffesse RG. New clinical index for drug-induced gingival overgrowth. Quintessence Int 1999;30:467-73.
3. Rees TD, Levine RA. Systematic drugs as a risk factor for periodontal disease initiation and progression. Compendium 1995;16:20, 22.
4. Dongari-Bagtzoglou A, Research, Science and Therapy Committee, American Academy of Periodontology. Drug-associated gingival enlargement. J Periodontol 2004;75:1424-31.
5. Bittencourt LP, Campos V, Moliterno LF, Ribeiro DP, Sampaio RK. Hereditary gingival fibromatosis: Review of the literature and a case report. Quintessence Int 2000;31:415-8.
6. Nyska A, Shemesh M, Tal H, Dayan D. Gingival hyperplasia induced by calcium channel blockers: Mode of action. Med Hypotheses 1994;43:115-8.
7. Marshall RI, Bartold PM. A clinical review of drug-induced gingival overgrowths. Aust Dent J 1999;44:219-32.
8. Lafzi A, Farahani RM, Shoja MA. Amlodipine-induced gingival hyperplasia. Med Oral Patol Oral Cir Bucal 2006;11:E480-2.
9. Pradhan S, Mishra P. Gingival enlargement in antihypertensive medication. JNMA J Nepal Med Assoc 2009;48:149-52.
10. Seymour RA, Ellis JS, Thomason JM. Risk factors for drug-induced gingival overgrowth. J Clin Periodontol 2000;27:217-23.
11. Joshi S, Bansal S. A rare case report of amlodipine-induced gingival enlargement and review of its pathogenesis. Case Rep Dent 2013;2013:138248.
12. Seymour RA. Calcium channel blockers and gingival overgrowth. Br Dent J 1991;170:376-9.
13. Saito K, Mori S, Iwakura M, Sakamoto S. Immunohistochemical localization of transforming growth factor beta, basic fibroblast growth factor and heparan sulphate glycosaminoglycan in gingival hyperplasia induced by nifedipine and phenytoin. J Periodontal Res 1996;31:545-55.
14. Iacopino AM, Doxey D, Cutler CW, Nares S, Stoever K, Fojt J, et al. Phenytoin and cyclosporine A specifically regulate macrophage phenotype and expression of platelet-derived growth factor and interleukin-1 in vitro and in vivo: Possible
Table 1: Multifactorial nature of drug induced gingival overgrowthFactors MechanismAge Children and adolescents unique fibroblast
phenotype increased androgen metabolismGenetic predisposition
Functional heterogeneity of fibroblasts
Pharmacokinetic variables
Threshold concentration of the drugConcentration of the drug in serum, saliva, gingival crevicular fluid and plaque
Drug induced alteration in gingival connective tissue homeostasis
Increased collagen productionIncrease in non‑sulfated glycosaminoglycans of the non‑collagenous matrixDecreased collagenase activityIncreased synthesis of TIMPs
Histopathology, ultrastructural factors and inflammatory change
Active protein synthesisReduced degenerative changesMononuclear and poly morphonuclear cell infiltrateIncreased prostaglandin E2
Drug induced action on growth factors
Increased expression of EGF and PDGF
TIMPs: Tissue inhibitors of metalloproteinases, EGF: Epidermal growth factor, PDGF: Platelet derived growth factor

Bajoria, et al.: Gingival enlargement: Revisited
IJSS Case Reports & Reviews | Vol 1 | Issue 3 25
molecular mechanism of drug-induced gingival hyperplasia. J Periodontol 1997;68:73-83.
15. Dill RE, Miller EK, Weil T, Lesley S, Farmer GR, Iacopino AM. Phenytoin increases gene expression for platelet-derived growth factor B chain in macrophages and monocytes. J Periodontol 1993;64:169-73.
16. Sporn MB, Roberts AB. Polypeptide Growth Factors and Their Receptors. New York: Springer-Verlag; 1991.
17. Seymour RA, Thomason JM, Ellis JS. The pathogenesis of drug-induced gingival overgrowth. J Clin Periodontol 1996;23:165-75.
18. Sonmez S, Cavdar C, Gunduz C, Nizam N, Biray C, Atila K, et al. Do MMP-1 levels of gingival fibroblasts have a role in the gingival overgrowth of cyclosporine-treated patients? Transplant Proc 2008;40:181-3.
19. Cotrim P, de Andrade CR, Martelli-Junior H, Graner E, Sauk JJ, Coletta RD. Expression of matrix metalloproteinases in cyclosporin-treated gingival fibroblasts is regulated by transforming growth factor (TGF)-beta1 autocrine stimulation. J Periodontol 2002;73:1313-22.
20. Csiszar A, Wiebe C, Larjava H, Häkkinen L. Distinctive molecular composition of human gingival interdental papilla. J Periodontol 2007;78:304-14.
21. Hassell TM. Epilepsy and the oral manifestations of phenytoin therapy. Monogr Oral Sci 1981;9:1-205.
22. Niimi A, Tohnai I, Kaneda T, Takeuchi M, Nagura H. Immunohistochemical analysis of effects of cyclosporin A on gingival epithelium. J Oral Pathol Med 1990;19:397-403.
23. Ellis JS, Seymour RA, Monkman SC, Idle JR. Gingival sequestration of nifedipine in nifedipine-induced gingival overgrowth. Lancet 1992;339:1382-3.
24. Seymour RA, Ellis JS, Thomason JM, Monkman S, Idle JR. Amlodipine-induced gingival overgrowth. J Clin Periodontol 1994;21:281-3.
25. McLaughlin WS, Ball DE, Seymour RA, Kamali F, White K. The pharmacokinetics of phenytoin in gingival crevicular fluid and plasma in relation to gingival overgrowth. J Clin Periodontol 1995;22:942-5.
26. Bökenkamp A, Bohnhorst B, Beier C, Albers N, Offner G, Brodehl J. Nifedipine aggravates cyclosporine A-induced gingival hyperplasia. Pediatr Nephrol 1994;8:181-5.
27. Seymour RA, Jacobs DJ. Cyclosporin and the gingival tissues. J Clin Periodontol 1992;19:1-11.
How to cite this article: Bajoria AA, Asha ML, Babshet M, Patil P, Sukhija P. Gingival enlargement: Revisited - A case series. IJSS Case Reports & Reviews 2014;1(3):20-25.
Source of Support: Nil, Conflict of Interest: None declared.
Related Documents











