


EthicsandPoliciesRegarding“MedicallyInappropriateCare”
FeliciaCohn,PhDBioethicsDirector
KaiserPermanete OrangeCountyClinicalProfessor
UniversityofCaliforniaIrvine
Overview• Reviewthemeaningof“medicallyinappropriatecare”
• Assessaprocessforaddressingmedicallyinappropriatecare
• Considerpolicyneedsandimplicationsofmedicallyinappropriatecare.

“NaturalDeath”
“MedicallyInappropriateCare”Not medically indicated
Ineffective
Non-beneficial
Hopeless
Futile

SchneidermanLJ, JeckerNS, JonsenAR. Medicalfutility:itsmeaningandethicalimplications. AnnInternMed. 1990Jun15;112(12):949-54.• …weproposethatwhenphysiciansconclude(eitherthroughpersonalexperience,experiencessharedwithcolleagues,orconsiderationofpublishedempiricdata)thatinthelast100casesamedicaltreatmenthasbeenuseless
• Ifatreatmentmerelypreservespermanentunconsciousness orcannotenddependenceonintensivemedicalcare,thetreatmentshouldbeconsideredfutile.
• …treatprobabilityandutilityasindependentthresholds.…physiciansmustdistinguishbetweenaneffect,whichislimitedtosomepartofthepatient'sbody,andabenefit,whichappreciablyimprovesthepersonasawhole.Treatmentthatfailstoprovidethelatter,whetherornotitachievestheformer, is"futile".
• …physicianscanjudgeatreatmenttobefutileandareentitledtowithholdaprocedureonthisbasis.Inthesecases,physiciansshouldactinconcertwithotherhealthcareprofessionals,butneednotobtainconsentfrompatientsorfamilymembers.

TheElusive“F”Word
•QuantitativeFutility• Likelihoodthatinterventionwillbenefitpt isexceedinglypoor(reasonableprobabilityofsuccess).
•QualitativeFutility• Qualityofthebenefitaninterventionwillproduceisexceedinglypoor,i.e.resultwillbepoorqualityoflife.

TheFutilityofFutility

O!besomeothername:What’sinaname?thatwhichwecallaroseByanyothernamewouldsmellassweet;
ShakespeareRomeoandJuliet

Othernames…• CaliforniaMedicalAssociation:“Non-BeneficialTreatment”• “NBTgenerallynotindicatedforirreversiblemedicalconditionswhereimminentdeathisexpected.”
• “CMAModelPolicy:RespondingtoRequestsforNon-BeneficialTreatment.”July2011
• CriticalCareorganizations:“PotentiallyInappropriateTreatment”• Theterm“potentiallyinappropriate”shouldbeused,ratherthanfutile,todescribetreatmentsthathaveatleastsomechanceofaccomplishingtheeffectsoughtbythepatient,butcliniciansbelievethatcompetingethicalconsiderationsjustifynotprovidingthem.
• AnOfficialATS/AACN/ACCP/ESICM/SCCMPolicyStatement:RespondingtoRequestsforPotentiallyInappropriateTreatmentsinIntensiveCareUnits,June2015

Definitions/Descriptions• Anytreatmentaphysiciandeterminesintheexerciseoftheirprofessionaljudgmentwould:• Beineffective forproducingdesiredphysiologicaleffectthatthept/agentdesiresorexpects;or
• Producenoeffectsthatcanreasonablybeexpectedtobeexperiencedbypt asfurtheringtheirexpressedandmedicallyobtainablegoals;or
• Causeharmtothept significantlydisproportionatetothebenefit;
• Hasnorealisticchanceofreturningpt toalevelofhealththat permitssurvivaloutsideofacutecarehospital;or
• Wouldserveonlytomaintainpt’s lifeinapermanentlyunconsciousstate,unlessthereisevidencethatthepatientwouldvalueremainingaliveinthatstate.

CompetingEthicalObligations
Rel
atio
nshi
p &
Tr
ust
TreatmentRequestsMoralDistress• Differentinterpretationsofgoodsandharms.
• Perceivedbreakdownoffiduciaryrelationship.
• Decision-makingreducedtostrugglebetweenpatientautonomyvs.clinicianautonomy.
• Treatmentgoalsoftennotclarified.
• Subjectiveperceptionsofqualityofthislife.
• Noestablishedtransparentprocesstoresolvedisputes.
Helft PR,Siegler M,LantosJ.TheRiseandFalloftheFutilityMovement.NEJM343;2000;293-296

Fromdefinitiontoprocess

Whypolicy?InstitutionalPolicy Case-by-CaseBasis
Advantages -Clearguidelines.
-Decreasespotentialdiscrimination.
-Increasedconsistency.
-Moreflexibilityandroomforprofessionaljudgment.
-Lesscumbersomeprocess.
Disadvantages-Processmaybecumbersomeleadingtolackofutilization.
-Caseswillinevitablyfalloutsidethedefinitions.
-Inconsistencyandriskofdiscrimination.
-Lackofofficialadministrativesupport.
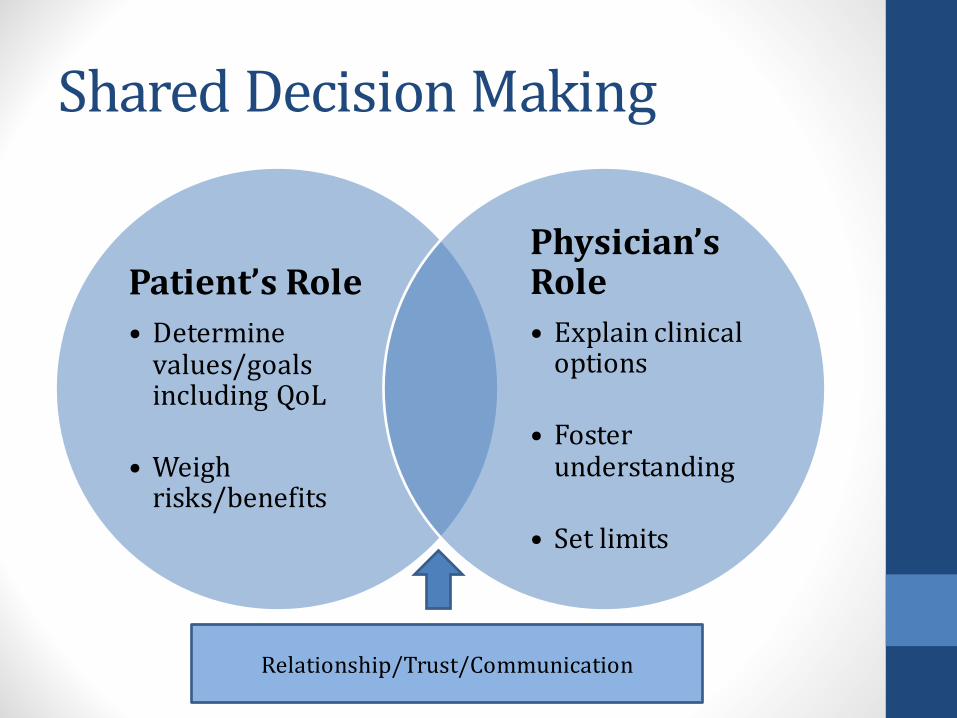
SharedDecisionMaking
Patient’sRole• Determinevalues/goalsincludingQoL
• Weighrisks/benefits
Physician’sRole• Explainclinicaloptions
• Fosterunderstanding
• Setlimits
Relationship/Trust/Communication

LegalSupportCaliforniaLaw• CaliforniaProbateCode4735:• “Ahealthcareprovider…..maydeclinetocomplywithanindividualhealthcareinstructionorhealthcaredecisionthatrequiresmedicallyineffectivehealthcare…”
• CaliforniaProbateCode4740:• “Ahealthcareprovider….acting ingoodfaithandinaccordancewithgenerallyacceptedhealthcarestandards…..isnotsubjecttocivilorcriminalliabilityforanyactionincompliancewiththisdivision,including,buttolimitedto,anyofthefollowingconduct:
• Decliningtocomplywithahealthcaredecisionofapersonbasedonabeliefthatthepersonlackedauthority.
• Decliningtocomplywithindividualhealthcare instruction…inaccordancewithSections4734to4736.”

PolicyDevelopment• BasedonCMAModelpolicyandCaliforniastatelaw• DevelopedbyRegionalBioethicsCommitteeover2yearperiod• Vettedbynumerousstakeholdergroups• Reviewedandapprovedbylegalandriskmanagement.• Reviewedandapprovedbyregionalleadership.• Reviewedandapprovedbyservicearealeadership• Annualreview
Steps• Enlistexpertconsultationfornegotiation/conflictresolution• Informpatient/surrogates• 2nd medicalopinion• Interdisciplinaryhospitalcommitteereview• Opportunitytotransferthepatienttoanalternateinstitution• Opportunitytopursueextramuralappeal• Decisionimplementation• Ongoingsupport

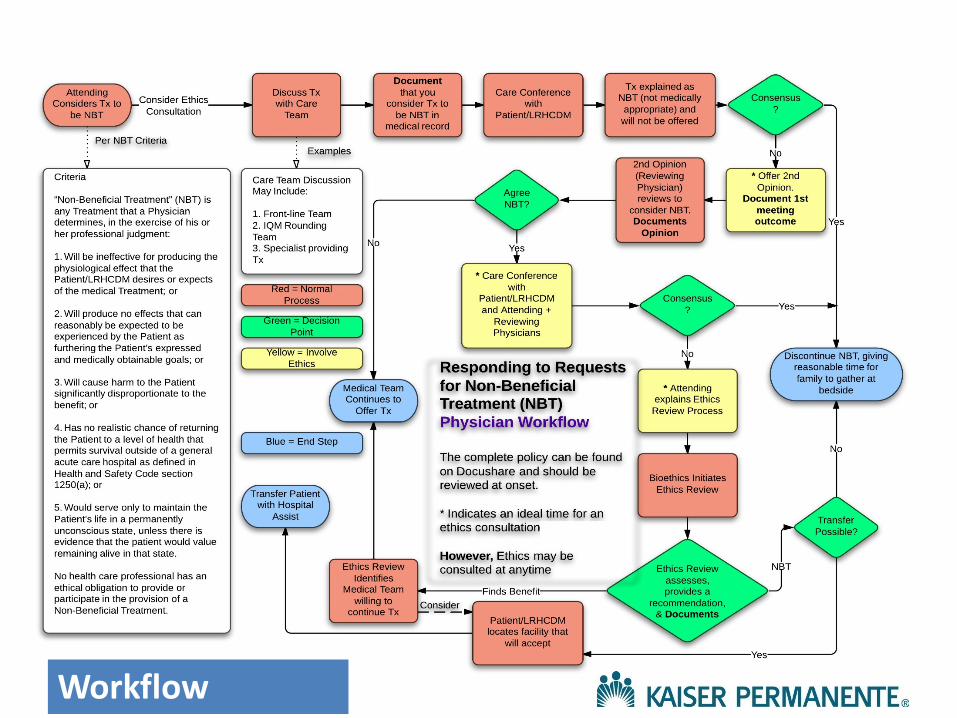
PolicyProcess• Step1:IdentifyNBT• Step2:CommunicationamongMedicalTeam• Step3:Communicationwithpatient/ decisionmakers• Step4:SecondOpinionbyReviewingPhysician• Step5:EthicsReview• SupportsInitiation/ContinuationofTreatment— transfertoanotherMD• SupportsForgoingTreatment—opportunityfortransfer,thantreatmentstops
20|©2011KaiserFoundation
HealthPlan,Inc.Forinternaluse
only.
November10,2016
Workflow

PuttingPoliciesIntoPractice

PolicyOutcomes• 1KPservicearea(SouthBay)• Retrospectiveevaluationofallbioethicsconsultations11/6/09(policyadoption)– 8/6/12.
• Case-specificdataforconflictinvolvingwithholdingorwithdrawingofnonbeneficial treatment.
• MainOutcomeMeasures:Conflictresolution• Results:• 146(39.4%)cases• 54(37.0%)ofthecases,resolutionoccurred.• 92(63.0%)NBTeventuallywithheldorwithdrawn.• 87(94.6%)wheretreatmentwaswithheldorwithdrawn,consensusreachedthroughpolicyprocess
• 5conflictsremained• CMNelson,BANazareth,Nonbeneficial TreatmentandConflictResolution:BuildingConsensus,PermJ2013Summer;17(3):23-27

5casesofpersistentconflictCasesofunilateralwithdrawal Patientpreferences
Afterethicscommitteecase
reviewTreatmentwithheld
orwithdrawn OutcomePostoutcomelitigation
1 Beneficialtreatmentperadvancedirective
Familythankful CPR,increaseddoseofvasopressors,antiarrhythmics
Comfortmeasuresinitiated;patientdiedinhospital
No
2 Unknown; familyneverdiscussedtreatmentpreferenceswithpatient
Familyaccepting CPR,stent,increaseddoseofvasopressors
Comfortmeasuresinitiated;patientdiedinhospital
No
3 Noadvancedirective;patientambivalentwithtreatmentpreferences,thenlostcapacity
Familyunaccepting CPR,dialysis,vasopressors,antiarrhythmics,tracheostomy,antibiotics
Comfortmeasuresinitiated;patientdiedinhospital
No
4 Familystatedthatpatientrequestedconservativetreatment;noadvancedirective
Familyunaccepting CPR,dialysis,feedingtube
Comfortmeasuresinitiated;patientdiedinsubacutecarefacilityposttransfer
No
5 Conservativetreatmentrequestedperadvancedirective
Familyunaccepting Nasogastrictubeandpercutaneousendoscopicgastrostomytube
Transferredtoanotherhospitalbyfamily;nofurthercontact
No

Societaldisconnect

Historically…

DoctorsDieDifferently“It’snotafrequenttopicofdiscussion,butdoctorsdie,too.Andtheydon’tdieliketherestofus.What’sunusualaboutthemisnothowmuchtreatmenttheygetcomparedtomostAmericans,buthowlittle.Forallthetimetheyspendfendingoffthedeathsofothers,theytendtobefairlyserenewhenfacedwithdeaththemselves.Theyknowexactlywhatisgoingtohappen,theyknowthechoices,andtheygenerallyhaveaccesstoanysortofmedicalcaretheycouldwant.Buttheygogently.
Ofcourse,doctorsdon’twanttodie;theywanttolive.Buttheyknowenoughaboutmodernmedicinetoknowitslimits.Andtheyknowenoughaboutdeathtoknowwhatallpeoplefearmost:dyinginpain,anddyingalone.They’vetalkedaboutthiswiththeirfamilies.Theywanttobesure,whenthetimecomes,thatnoheroicmeasureswillhappen—thattheywillneverexperience,duringtheirlastmomentsonearth,someonebreakingtheirribsinanattempttoresuscitatethemwithCPR(that’swhathappensifCPRisdoneright).”
DoctorsDieDifferently
“…victimsofalargersystemthatencouragesexcessivetreatment”
KenMurray,JournalofMedicine,August1,2013,https://www.ncnp.org/journal-of-medicine/1240-doctors-die-differently.html
CommunicationIsKey
“….partoftheir[physicians’]angstcomesnotsimplyfromthepressuretoprovideburdensometreatment,butalsofromaninabilitytofindtherightlanguageandconceptualframeworkfortalkingabouttheproblemwithpatientsandfamilies.”
SolomonMZ.Howphysicianstalkaboutfutility:makingwordsmeantoomanythings.JournalofLaw,Medicine,andEthics1993;21:231-237
BeyondCommunication…
• Family“threats”togotothemedia orattorney• Fairapplicationofpolicybasedonmedicalindications,whileremaining sensitivetoculturalandreligiousdifferences.• Institutionalsupportforapplicationinindividualcases.• Societalperspectives
Policyimplications• Physiciandutiesatthebedside• Respectforpatient/surrogateautonomy• Avoidharm(“overmasteredbydisease”)• Stewardresources
• Endsofmedicine• Recognitionoflimitsofmedicine• Limitsofautonomy
• SocietalObligations• Unsustainablecostsandmanpower• Opportunitycosts• Fairness:justdistributionofresources

CompetingEthicalObligationsandSocialContext
Rel
atio
nshi
p &
Tr
ust
PublicEngagement“Themedicalprofessionshouldleadpublicengagementeffortsandadvocateforpoliciesandlegislationaboutwhenlife-prolonging
technologiesshouldnotbeused.”
OFFICIALPOLICYSTATEMENT:AmericanThoracicSociety(ATS),approved10/15AmericanAssociationforCriticalCareNurses(AACN),12/14AmericanCollegeofChestPhysicians(ACCP),10/14EuropeanSocietyforIntensiveCareMedicine(ESICM),9/14SocietyofCriticalCareMedicine(SCCM),12/14

Individual,PhysicianorSociety?
And the winner is…


ResuscitativeServicesPolicyMedicallyInappropriateCPR
• AffirmspolicytoprovidemedicallyindicatedCPR,intheabsenceofaDNRorder.• IdentifiessituationsinwhichCPRisconsideredineffectiveandisnotmedicallyindicated:1. Terminallyillpatientwhoisimminentlydying2. Patientexperiencingirreversibleorganfailure
notexpectedtosurvivecurrenthospitalization3. Permanentlyunconsciouspatient
• DecisionthatCPRisnotmedicallyindicatedandwillnotbeofferedmustbedisclosedtopatient/agentanddocumentedinthemedicalrecord.

DNRandMIT/NBT
CPR
MIT/NBT































