Second Floor, Parkway One Parkway Business Centre Princess Road Manchester M14 7LU A vision of an integrated Mind-Body Service Version 4.2.0 Author: M E Y Capek March 2016 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Second Floor, Parkway OneParkway Business Centre
Princess RoadManchester
M14 7LU
A vision of an integratedMind-Body Service
Version 4.2.0
Author: M E Y Capek
March 2016
1

SUMMARY
The topic of Medically Unexplained Symptoms (MUS) or its currently more preferred term Bodily Distress Syndrome (BDS), hereafter to be referred to as MUS/BDS, is one that is coming very much to the fore.It incorporates the known functional disorders such as irritable bowel syndrome, chronic fatigue syndrome, non-epileptic seizures andmany others; and the somatoform disorders in which there are physical symptoms due to emotional distress. Because of the broad range of conditions that come under the aegis of MUS/BDS and the multiple associations between these ailments, they can be best thought of as one condition. They all can vary in severity. Left unmanaged there are heavy costs incurred on the patient, on servicesand on society as a whole.
Therapies are available if the patient can reach them. But up until now only a very few services have seriously tried to tackle the problem that MUS/BDS presents. More often than not what service thatis available is very fragmented and often only deals with a single aspect of the whole syndrome. Patients with MUS/BDS have been low priority for both physical and mental health planners. For the benefit of the patients who have one of these conditions and the public purse, it is strongly argued that this must change.
In summary, to meet this challenge, what is proposed is a 4-step stepped-care approach. Along side this will be a programme of education to enable clinicians to meet their clinical and thereafterthe financial saving objectives. The configuration described followsa stepped care delivery model approach. These 4-steps are:
1. Management by GP and secondary sector physical health centres.2. Management by self-help services3. Management by services at a level compatible with IAPT4. Management by a new specialised unit.
Steps 1, 2 and 3 can easily be met, and by and large will be in-keeping with current service provision. Step 4 will require a new dedicated specialist MUS/BDS service and is where nearly all the investment will be needed. This would manage the individuals with the most complex cases including those patients who are frequent attenders to the acute trusts. The creation of a best practice high
2

end MUS/BDS service, would see liaison psychiatry and inter-personaltherapies at its heart, but supplemented with other specialists and specific therapists creating a truly experienced multi-disciplinary team.
This document is deliberately comprehensive. There is much clinical information contained within. It is there, not only to guide those who have to make the decisions about these matters, but also to givebest practice guidelines for all clinicians who will meet these conditions.
It sets out to inform and improve attitudes. Because MUS/BDS is verymuch at that focus where physical health and mental well being meet,it starts by advocating a genuine holistic and needs-led approach. It then moves on to provide a way of thinking about symptoms in general that may help manage these conditions much better in the future. By normalising symptoms into a process of mind-body communication that has positive intent, it is hoped that clinicians will have a much more constructive regard towards these patients andtheir problems. In particular, leaving symptoms ‘unexplained’ is unhelpful.
In order to lead by example, in writing this document, when talking about the topic, care has been taken to be mindful of the reader, particularly one who has one of the conditions comprising BDS, and not to overuse the terms ‘mental’ or ‘psychological’.
There is a detailed literature review. It contains the latest up to date thinking on the topic. Included are sub-sections describing in more detail the extent of the problem and considerations regarding therapies and service development. Whereas the previous section deals with attitudes, this deals with knowledge.
The final section is a vision of an outline best practice model. In particular the nature and working ethos of a high end MUS/BDS service is very tightly defined. The evidence base for estimating the financial savings and the processes for their delivery are described.
This document should not be seen as the final word but as the starting point.
3

4

CONTENTSCONCEPTS AND ATTITUDES 6
The Holistic Approach 6Improving well-being is based on needs led decision making
9
Further consultation approaches 12Integration 14Symptoms-What are they and how to describe them 14Making a positive diagnosis 15Mind-Body modelling 17
THE EVIDENCE BASE 22Terminology 22Prevalence 23Healthcare costs 25Therapies for BDS 26Costs/benefits of therapy 27Barriers to overcome 27Service provision 28Managing the Individual Patient 30
ASSESSMENT 30TREATMENT 31
Training 32Considerations for service development 33
A VISION OF PROVIDING A COMPREHENSIVE SERVICE 35A stepped care model 35The role of the GP 36
TRAINING 37The Role of the Physical Health Specialist 37The role of Self Help and High Intensity Well-being Services
38
A specialist BDS service 38PREAMBLE 38TITLE 38ETHOS OF SERVICE 39MANAGEMENT CONSIDERATIONS 40WHO IT IS FOR 42STAFFING 42REFERRALS 43WHAT IT WILL DO 43LINKS WITH OTHER SERVICES 44
5

MONITORING 44TEACHING AND RESEARCH 44MANAGING THE COST OF AN MUS/BDS SERVICE 44SERVICE DEVELOPMENT 46MANAGING THE PROCESS 47
REFERENCES 49
VERSION HISTORY 53
APPENDICES 53
Appendix 1: Inventory of Healthy Emotional Skills 53
Appendix 2. Figure 5 in list form 55
Appendix 3: The Definition of Bodily Distress Syndrome 56
Appendix 4: A poster displayed at the RCGP Conference 2013 presenting the use of hypnotherapy in a general practice setting.
57
LIST OF FIGURES, AND TABLES
Figures
Figure 1 Two patient life lines 8Figure 2 Conceptualising Mind-Body integration 1
3Figure 3 Beck’s Cognitive Model 1
7Figure 4 A Biodynamic Approach to Symptom Causation 1
8Figure 5 A Mind Map of the Functional Conditions Arising from
Psychological Distress19
Figure 6 A Diagrammatic Description of the Different Terms in Use
22
Figure 7 The GP’s Management Algorithm for a Medically Unexplained Symptom
36
Figure 8 Description of a Specialist Step 4 BDS Service 41
6

Tables
Table 1 The Psychiatric History 7Table 2 4 different clinical scenarios 1
1Table 3 Examples of Low physical, low psychological
consultations12
Table 4 Making a positive diagnosis of a functional disorder 16
Table 5 Possible Psychological Precursors to Non-Organic Symptoms
20
Table 6 Doctors’ Perceptions of the principle issues patientspresent
38
Table 7 A Stepped Care Approach 35
7
CONCEPTS AND ATTITUDES
Much of what is written in this section is relevant to the whole of mental health practice. It is provided to be able to place the management of MUS/BDS within the context of both physical and psychological health.
The Holistic approach
Bodily Distress Syndrome (BDS) which subsequently will be defined and used as the term to denote what is currently being referred to as the psychosomatic disorders or medically unexplained symptoms (MUS) are amongst the hardest to manage. In the more severe forms the patient’s condition, becomes pervasive into every aspect of his or her life. It naturally follows that managing these patients well,must involve a holistic approach. It is a term that is widely used but in reality, what is it? How does one recognise holistic practice?
Practicing holistically implies taking every distinct facet of that person in such a way to be able to consider the individual as a whole unique person. Therefore, if an important facet from the person’s whole life is missing, it is no longer practicing holistically. It is therefore necessary to describe each facet that together can be deemed to be holistic practice.
Psychiatric history taking aims to be thorough. This is presented inTable 1. Necessary information to be able to make a diagnosis and formulate the patient’s difficulties in a manner that is able to guide therapy is obtained. The mental health history ignores neitherthe patient’s physical health, nor the social context of the patient.
Such an approach works well but it has its limitations. Psychiatric diagnosis is not an accurate science. (Nielssen et al, 2010). When an individual reaches the state that he or she needs to seek help, that person more often than not is well removed from their more usual condition of functional well-being. Thus the assessing clinician will be gaining a very distorted picture of the person’s life as a whole based on the current presentation.
8
The term coined to denote an holistic approach is “a bio-psycho-social model”. However for some people even this excludes a major facet. To some holistic can also imply mind, body and spirit.
Transpersonal Psychotherapy (TP) takes a view of the whole person well beyond current psychology and psychiatric practice. It is not for everyone because there are attitudes that are derived more from religion and spirituality than psychology. Furthermore, it means different things to different people and there has not been a satisfactory definition to quote describing what it actually is. Poulton (2015) probably gives the best and most understandable description.
The relevance to developing a service for mind-body syndromes is that TP has paradigms of thinking that would enhance the delivery ofthat service. TP concerns higher state consciousness beyond the physical. It deals with a person’s purpose, meaning and role in life. When patients have debilitating physical symptoms with or without obvious medical cause, with or without psychological distress, the question “Why me?” is not just a declaration of anguish, it is one that is demanding an answer.
TP encompasses the notion that at the core of the individual is an essence that has many skills, talents and attributes. We are born with the potential and it is the opportunity that allows these to flourish. Given the right circumstances humans are constantly striving to satisfy their full potential.
Basic information Name Age marital status Current occupation Route of referral Current legal status (detained under
Mental Health Act?).
Presenting complaints
History of presenting complaints
Past psychiatric and medical history Previous psychiatric diagnoses Chronological list of episodes of
Employment Chronological list of jobs
o Which job did they hold for thelongest period?
o Which job did they enjoy most? If the patient has had a series of
jobs—why did they leave each? Account for periods of unemployment
in the patient's history Is the type of job undertaken
consistent with the patient's level of educational attainment?
Relationships Sexual orientation. Chronological account of major
9

psychiatric inpatient, day hospital, and outpatient care
Current medical conditions Chronological list of episodes of
medical or surgical illness Episodes of symptoms for which no
treatment was sought Any illnesses treated by GP
Drug history List names and doses of current
medicationo have they been taking it?
Previous psychiatric drug treatments. History of adverse reactions or drug
allergy. Any non-prescribed or alternative
medications taken.
Family history Draw a family tree detailing names,
ages, relationship, and illnesses of first- and second-degree relatives.
Are there any familial illnesses?o Include bipolar and psychotic
disorders
Childhood Were there problems during their
pregnancy or delivery? Did they reach development milestones
normally? Was their childhood happy? In what sort of family were they
raised?
Education Which primary and secondary schools
did they attend?o If more than one of each, why
was this? Did they attend mainstream or
specialist schools? Did they enjoy school—if not, why? At what age did they leave school and
with what qualifications? Type of further education and
qualifications attained.o If they left higher education
before completing the course—why was this?
relationships.o Reasons for relationship
breakdown. Are they currently in a relationship? Do they have any children from the
current or previous relationships?o Who do the children live with?o What relationship does the
patient have with them?
Forensic Have they been charged or convicted
of any offences?o What sentence did they receive?
Do they have outstanding charges or convictions at the moment?
Social background information Current occupation. Are they working
at the moment?o If not, how long have they been
off work and why? Current family/relationship
situation. Alcohol and illicit drug use Main recreational activities.
Premorbid personality How would they describe themselves
before they became ill? How would others have described them?
(Not included, but normally to be expected would be the person’s religious, ethnic, linguistic and cultural background. This would include an anticipated understandingof the person’s premorbid belief system.)
Table 1. The psychiatric history: Adapted from Semple & Smythe (Eds) The Oxford
10

handbook of Psychiatry (2013)
The balance of attributes is different from person to person. Identification of the attributes can help inform the healing process. These attributes not only include the innate skills but thepatient’s natural coping strategies, e.g. when stressed does the patient tend to respond to that stress by doing something about it (behavioural), thinking excessively about it (cognitive), emoting (emotional), internalising it (suppressing it) or somatising it. Somatisation therefore is in itself not a bad thing. Understand the mind-body connection and the somatisation can inform the person about the stress. Finding those basic characteristics may require enquiring back to childhood. Depending on circumstances it may need to involve asking the living relatives
Psychological Well-being is a life long paradigm. TP tries to help the person conceptualise the whole life; past, present and future. TP has the attitude that all life experiences, even the traumatic and painful ones, are of merit and can be used positively.
Figure 1 conceptualises the whole life of 2 patients and the role oftherapists and others.
11

Figure 1. Two patient lifelines. Horizontal axis is time and vertical is emotional and functional well-being. The upper case is simpler with a single intervention restoring the patient. In the lower more complex case, there are several antecedents before the major functional collapse. Recovery is staged and more protracted Often it is incomplete.
So in summary, taking a holistic view implies addressing the person’s physical, psychological social and spiritual welfare. It implies taking a whole life view by understanding the present in thecontext of the innate characteristics, the past and the hoped for future.
Improving well-being is based on needs led decision making
Patient’s life line
Birth Death
Contact with GP/Therapist helping the patient find their own way back onto their line of full potential
Patient’s life line
Birth
Death
Contact with GP/Therapist helping the patient onto the start of their recovery.
Different therapeutic interventions, positive life events and wise life choices helping the patient back onto their line of full potential.
12

At a recent conference for mental health clinical leads, Jaqui Dyer (2015), Vice Chair of the Mental Health Task Force working to promote the 5 year Forward View for Mental Health in England reported that emerging from the 20,000 responses they had received were 4 key themes and priorities.
Attitudes and experiences-hope and dignity and respect and care Prevention and empowerment
o Balance of power and resources is too centric Access, including reducing variability Integrated care and support particularly across the board and
between Physical and Mental Health.
It could be argued that these themes, all patient-centric, could be achieved by deriving clinical decisions based on need and not diagnosis.
Currently much of mental health therapy follows a ‘medical model’ approach. The medical model works on the basis that the person is well and healthy until such time that symptoms appears as a sign of the onset of a particular defined psychiatric condition. The diagnosis then informs the best therapeutic approach to take and remedy the patient from the particular malady.
While there is much to commend this approach including the evidence base of many patients recovering from psychiatric and psychological conditions there are drawbacks. Making a psychiatric diagnosis is not an accurate science with discrepancies existing between psychiatric experts (Nielssen et al, 2010).
Furthermore it has been suggested that this approach may inadvertently be promoting mental health stigma. (Flanagan et al, 2009). The paper is worth a read and the title is pointed. The participants were community mental health practitioners, at a large,state-run community mental health center treating non-psychotic patients. The conclusion was “…stigma in mental health settings may come from at least two sources: practitioners’ emphasis on symptoms,deficits, and problems but also a culture in which practitioners feel pressured to make diagnoses and “treat the chart” rather than the person. Interventions targeting stigma therefore need to addresssystemic and cultural issues as well as practitioner beliefs and attitudes if they are to be effective.” While it is a study based in
13

the United States, the conclusion is probably transferable to components of mental health Services in the UK.
With psychiatrists tending to take the lead in running mental healthservices and psychiatrists being trained in the medical model methodology this systematic approach is pervasive. It is very easy for both client and therapist to ask, “what went wrong?” and, “what needs to be done to put it right?” This works well up to a point. Mental health well-being generally and mind-body syndromes specifically may have many antecedents which are not recognised. People have the ability to function, and function well, even though there may be factors that will subsequently lead to the person’s emotional system breaking down. The developing alcoholic who is lacking the insight to the psychological damage is a case in point.
There are many situations where the medical model is less effective than desired. Drewek(2015) in the IAPT Progress Report with its verylargely based CBT modeling approach notes that patients being referred for common psychological problems the recovery rate is usually between 40-50%. At 55.2% the recovery rates for MUS are the highest of all the conditions treated, but is still barely more thanhalf. The approach taken is that of assess the patient, diagnose or give a problem descriptor and treat according to current best practice guidelines.
So why do half the patients not recover? Excluding the therapist andthe client-therapist relationship reasons, experience on the ground suggests the following are possible patient related explanations:
The patient has other needs such as other health, financial, housing or social that for the patient take priority, and therefore cannot engage on a psychological therapy.
The condition is too engrained or is being stimulated by a deeper imprint or trauma that needs to be resolved.
CBT imparts a skill. Once the skill is learnt and the patient applying it, there is no further improvement available by this technique alone.
The IAPT progress report provides another interesting statistic. Only up to 60% of patients have been given a diagnosis or problem descriptor, implying that this is not always readily available. And yet these are people who are in mental health services.
14

Understanding an individual by taking a whole life approach, particularly when many aspects of that life are beyond the immediaterecall of memory may be difficult, but so too sometimes is making a diagnosis. Fortunately to help those with psychological symptoms, the latter is often not essential.
A humanistic psychologist whose writings have much informed transpersonal psychotherapy was Abraham Maslow. He is best known forhis eponymous hierarchy of social needs (Maslow, 1943 and 1954). These needs are at the heart of human well-being. His original concept was derived with 5 social needs. In order these were physiologic, safety, belonging and love, self esteem and self-actualisation. He later added ‘cognitive’ and ‘aesthetic’ needs between self-esteem and self-actualisation; and ‘transcendence’ became the new highest level need.
The underlying principle is that a person must address the lowest level of need that is not satisfied before moving onto the next. It is not the rigorous following of the hierarchy that is being advocated, although it can give guidance. It is the principle that the most pragmatic approach to helping patients with MUS/BDS or otherpsychologically based conditions is one that is not diagnosis led butneeds led.
A needs led approach is in part based on the assumption that we are all born with an in-built desire to heal. Implied is not only that therapy can be patient led, but it can be trusted and therefore the role of any therapist is to act as the patient’s guide to self-healing.
It is acknowledged that there will be times when the patient’s mental state, be it psychotic, organic or more simply just highly disturbed, and the desire to heal cannot assert itself. Under these circumstances responsible relatives and social/mental health services can work together determining what the person’s primary needs are. Achieving mental health stability may be that priority need.
Furthermore, following a needs-led approach is not incompatible withthe medical model. In managing MUS/BDS it is necessary to understandthe patient’s individual physiology. Physical and psychiatric
15

diagnoses where these are readily available and sit comfortably withthe patient, physicians, and mental health workers alike should be made. This will help form the understanding of the physical health context of the patient’s psychological state.
Later in this paper, it will be seen that in managing patients with suspected MUS/BDS, the first step is to exclude or ascertain the nature of any physical illness, ensuring that the physiology is in astate of equilibrium.
Furthermore, mental health services are not averse to following needs when necessary. They are very good at understanding and managing the issues of safety that surround the patient, regardless of the patient’s diagnosis.
But if there is another more fundamental reason for following a needs-led service it is this. The relationship between any two people is able to pass the test of time when they each are able to support the other in times of need. The person who has unmet needs can have these fulfilled by the other. A successful therapeutic alliance should be no different. It is based on the mutual understanding of the patient’s difficulties. The patient will sense these through identifying his own unmet needs and the successful therapist will be able to address and resolve these needs. If the therapist, medical or otherwise, is too intent on making a diagnosisand treating a condition, it is little surprise that the patient whose need will remain unmet will fall out with the service providers, particularly as the latter are supposed to be the expertsin addressing psychological distress. From an inter-personal perspective addressing needs is natural.
It could be a challenge to many within mental health services, and to doctors particularly, to trust and adopt a different modality of thinking, but the rewards for all could be great.
Further consultation approaches
PsychologicalLow High
16

Physical
High
PhysicalDetermining “What is the problem, and what is the solution?”
PsychosomaticAs for Physical Health andAs for Mental Health and
Helping the patient make the connection between the physical symptoms and the psychological aetiology?
Low
Health PromotionEnsuring the patient meets certain objectivecriteria known to be associated with good health.
Mental HealthDetermining what needs to be undertaken for the patient to put their life back on track, through the understanding of prior events and future aspirations?
Table 2. 4 different clinical scenarios It is suggested that each has its ownmodality of thinking.
There are several different ways to classify the consultation types in clinical practice; e.g. acute or chronic condition, new problem or review. These and the nature of the condition presenting will affect the approach that the clinician is taking with the patient. In managing patients with MUS/BDS it may be of help first to understand another concept of classifying consultations. The clinical scenarios that doctors face may be categorised broadly according to 4 types (Table 2)
The Physical Health Problem, High Physical-Low Psychological, is managed best by the classical medical model with its problem solvingapproach, as described above. The Mental Health Problem, Low Physical-High Psychological, as is argued above, is best managed by a holistic needs-led approach taking into account the person’s
17

attributes, life events to date and hopes and aspirations for the future.
Presenting problems that are Low Physical-Low Psychological are deemed to be Health Promotion. There is no clinical problem to be solved and there are no life issues causing emotional distress. The cognitions of the clinician when faced with a healthpromotion scenario are to measure certain aspects of the patient’s well-being against known healthy parametersand advise accordingly. Examples of this are in Table 3.
Health checks Well person’s health
check Family planning Delay of menstruation 8-week baby check Ante-natal clinic Pre-anaesthetic
health checkTable 3. Some examples of Low physical, Low Psychological consultations.
Physical health promotion with its known healthy physiological and life style parameters is well established. Not so with PsychologicalHealth Promotion. While practitioners may have a sense of whether psychological health exists in a patient or not, there does not appear to be any accepted definition of mental health or the equivalent health promotion parameters that can be used to gauge patients psychological well-being. An attempt at doing this is placed in Appendix 1.
It is the somatoform and functional disorders that give rise to the Psychosomatic scenarios that are High Physical-High Psychological. The clinical approach needs to be in part as for the Physical scenarios, i.e. problem solving, part as in the Mental Health problems of needs led and in addition if possible the re-attributionof the physical ailment to the relevant psychological antecedent.
The degree of the Physical and Psychological inter-connection is on a spectrum. They may be separate as in for example the diabetic patient who is also depressed. They may be fully integrated as in the functional disorders such as Chronic Fatigue Syndrome and Irritable bowel syndrome. They may be somewhere between the two whenthe symptoms are out of proportion to the severity of the underlyingphysical condition
Integration18

Look at Figure 2. The upper part gives a diagrammatic depiction of how physical health and mental health services have been classicallyarranged. They are separate but they try to take similar approaches.Even the research into therapies is similar. Take a clinical condition and trial 2 or more therapeutic approaches to see which has the most favourable outcomes.
The lower part is trying to state that mental health and physical health are conceptually different. They are best thought of not as 2parallel concepts, but as 2 different dimensions of the one mind-body construct. They are very much interconnected. Mind and body cannot be separated. However, services and the clinicians who deliver these services may need to approach a clinical scenario along one dimension but be fully aware that the other dimension exists and it too needs to be promoted.
19

Figure 2. Conceptualising Mind-Body integration. The upper diagram depicts classical thinking and arrangement of services. Physical and Mental health are two separate entities not meeting. The lower diagram depicts the way in which physical and mental health care should be considered; two concepts, different dimensions but integrated into one whole.
If mental health is operating on a different ‘dimension’ to physicalhealth, then may be mental health research needs to develop and promote techniques improving the meaningfulness of mental health research outcomes.
The psychosomatic conditions are where the mental and the physical meet. When they become chronic and severe, neither the physical nor the psychological components are improving. It is as though there isa ‘knot’ preventing resolution. This is just one reason that makes the patients with these conditions the most challenging.
Symptoms-What are they and how to describe them.
We are brought up to think of symptoms as an indicator of being somesort of malfunction of the body. After all, the young child with a fever and any combination of a cough, diarrhoea or vomiting, will befeeling unwell. The child being unwell, feels unwell, becomes clingy. The parents, either with or without the help of a doctor,
20

explain that what the child is feeling are symptoms of whatever condition the child has. Several illnesses later, the message is repeated and symptoms equate with illness. The child growing up is able to discern the difference between those feelings that are responses to every day events, such as hunger, tiredness, anger, etc. and those that reflect illness.
Society reflects this attitude.
Years and many events later, the adult now develops symptoms attendsa doctor, who finds nothing physically wrong. But the symptoms persist as they often do in this situation. It doesn’t take a great deal of logic either by the person or others around to say, “If there is no physical problem, there must be a mental or psychological problem.” This notion is not necessarily correct and could be harmful.
May be what we call ‘symptoms’ needs to be thought of in a differentway?
Williamson (2008) has suggested that the symptoms may have positive psychological intent by being a psychological mechanism to produce physical and/or emotional homeostasis and equilibrium. When we look at mind-body modelling in due course there is merit in this notion. The implication is that symptoms are constructive features of mind-body interaction, ‘if only we know how to interpret them’. We can give some examples. The epigastric pain after food warns us not to eat for a few hours, may be not to drink as well, and may be watch what we eat in the future. To the pregnant woman near term, who develops tightening associated with increasing severity and frequency of abdominal; the pains may be great but the message is clear: “I am going into labour, I need blankets, hot water and a fewpeople around me who I trust to help and support me.” Knowing that migraine is a condition that can arise when stress is alleviated, the throbbing pulsatile headache on a Friday night all associated with visual disturbances can inform us that we have just finished a stressful week.
Taking these and many other examples into consideration, it is therefore proposed that we have this simply put definition:
21

A symptom is an awareness of mind-body communication.
Note the direction of communication is not specified. In itself there is no implication of illness. Feelings, in an emotional sense,are similar to this proposed definition of symptoms except feelings reflect the emotional or intuitive aspects of the mind alone. What is not stated in this definition is the message to be conveyed. Likecommunication in any language, it needs to be learnt and understood.
Such a notion is perfectly compatible with attribution re-modelling described later. By always having a positive regard to what the bodyis relating, it should be much less stigmatising. The reasons for such a definition will become clearer when describing the ethos of the proposed service.
Making a positive diagnosis
When the patient is presenting with symptoms and features that are related to MUS/BDS the consultations may follow a typical pattern. The same is followed regardless of whether it is within general practice or in secondary care out patients. The only difference being that in the latter the patient will have symptoms longer, and will already have been seen by the GP.
The patient will sit down and describe the symptoms. The doctor willexamine and will send for some investigations. These are returned with normal findings. At the review consultation, the consultation may close with one of the following alternatives coming from the doctor:
1. “There is nothing wrong with you.”2. “There is nothing physically wrong with you”3. “We have done all the tests and I have found nothing wrong with
you. “4. “I don’t know what is wrong with you.”5. “I could find nothing wrong with you within my specialty.6. “All the tests we did were normal and from this I conclude you
have… ( and insert the relevant functional disorder).
None of these statements are satisfactory. The first is at odds withthe patient’s experience. They are not malingering. The patient is likely to become angry or angrier at the suggestion, and depending
22

on the symptoms may re-present worse the next time. The second may be a clinically more accurate statement but the patient may well take the attitude, “if the doctor does not believe it to be physical, he must think it is all in my head”. The third is better but still leaves the patient ‘hanging’ with unexplained symptoms. Italso begs the question, that there must be some more tests that can be done. The fourth while honest makes the doctor sound unnecessarily incompetent and takes the patient no further forward. The fifth is similar to the fourth without making the doctor sound inept. The doctor is technically accurate and showing a degree of probity by not trying to practice outside his training and remit.
The last is the least bad. It is making the diagnosis by exclusion of other diagnoses. This may be the way for the diagnosis of certainconditions but even for these the explanation to the patient needs to be better by being based on actual positive findings that guide the physician to making the diagnosis. This would not be done for organic illness, e.g., “I know you have cancer because we have demonstrated that the tests for all other conditions proved to be normal.” Such an approach is unacceptable for organic illness, therefore so to should it be unacceptable for BDS conditions.
The start of any medical consultation is based on the history and examination and looking for patterns that point towards particular physical conditions. Clearly the first priority is to ensure that there is no serious physical condition, and that any ‘red flag’ symptoms are not present. But in the same way that there are clinical patterns that point to organic illness, there are patterns that can be looked for that will swing the differential diagnosis infavour of the ultimate diagnosis being MUS/BDS/a functional disorder. See Table 4. which is based on Burton 2013 and < http://www.neurosymptoms.org/ >.
MUS here is a particularly poor term, because even if there is no organic cause we should be trying to provide the patient with the best explanations we can. They need not be complicated.
Some common features regarding functional symptoms in general The more symptoms the more likely that MUS/BDS is existing The symptom is more bizarre, e.g. only under certain specific
circumstances, or exhibits a contradictory pattern.23

Symptoms that emerge when relaxing or resting. Symptoms worse when tired towards the end of the day. Symptoms tend to be worse when focussing on the symptom and easier when the
mind is engaged elsewhere. Symptoms tend to have more descriptive, may be metaphoric language. These
can act as verbal cues to explore the psychological nature of the symptoms. Symptoms that do not follow a neurological basis.
o Shooting pains going up or down the back, particularly on one side.o Shooting pains going across the midline.o Paraesthesia and/or numbness in all 10 fingerso Paraesthesia (as distinct from pain) down one arm
Specific Symptoms Palpitations are less likely to be organic if short-lived (less than 5
minutes); heart rate less than 100; occur while falling a sleep; and described as a pounding sensation or as the occasional extra or missed beat.
Chest pain aggravated by palpation; or chest pain aggravated by inspiration, when there is nothing to imply the pain is pleuritic in nature; or the pain can be localised with finger tip accuracy are all reassuring that the pain is external to the thoracic contents.
Breathlessness due to hyperventilation may be ascertained by observing obvious low shallow breathing, trying to inhale more air than exhale, features of a respiratory alkalosis, such as paraesthesia, carpo-pedal spasm and improvement with re-breathing through a paper bag.
Acid dyspepsia, with or without additional pathology, such as ulceration, or being H. pylori positive is likely to have a large psycho-somatic component.
Other known stress related conditions such as IBS, asthma, migraine should have the psychological component acknowledged
Pelvic pain in which the patient appears to walk normally is more likely tobe functional.
Chronic fatigue syndrome has the characteristic post-exertional fatigue andmyalgia for the next few days.
Muscle spasm, be it due to injury or psychological stress may have a local tender point that can be reassuring.
Functional weakness often has the characteristic of the patient dragging the externally rotated leg behind the ‘good one’. A positive Hoover’s sign is confirmatory. This is best carried out in the sitting position by first demonstrating relative ‘weakness’ of hip extension by comparing that passively elevating the ‘weak’ leg against resistance which is minimal is carried out easily. Then ask the patient to elevate the good leg against the resistance of a hand pressing down, whilst elevating the ‘weak’ leg. The ‘weak’ leg suddenly becomes strong again as the patient’s focus is awayfrom the weakness and the ‘weak’ leg is augmenting the instructions.
Dissociative or non-epileptic blackouts are best observed and do not have the typical tonic-clonic seizure look. Clues favouring a functional condition include falling down and lying still for 30 seconds; closed mouthand eyes with resistance to opening the eyes; side to side head and body movements as distinct from flexion/extension movements; and weeping or crying after a ‘seizure’.
In dissociative dizziness, the language used is “like being there, but not there”, or “disconnected”. These are phrases implying dissociation.
A functional tremor may be ascertained by the ‘Entrainment test’. With the
24

patient outstretching his hands in tremor, the examiner rhythmically pinches his own thumb and forefinger, and asks the patient to copy with onehand while the examiner observes the other. In a functional tremor, the tremor speeds up and slows down in the other hand according to the speed ofthe examiner’s pinching.
Functional blindness is ascertained when there is a narrow field of vision viewing distant objects, but much wider when close in.
Night sweats (except in a peri-menopausal woman) and blushing are more likely not to have an organic cause
Unhelpful features A history of anxiety and depression. While there is a significant overlap
between MUS/BDS and anxiety/depression, the latter is just as likely in thepresence of organic illness, e.g., the patient is worried over what they may have.
Symptoms occurring or disappearing at sleep.Table 4. Some clinical features that may help in making a positive diagnosis of afunctional disorder.
Negative findings are helpful to guide the diagnosis away from serious organic illness but it is the shared understanding, based onpositive features that will be used as the start of any resolution of the symptoms. Depending on circumstances, anything based on nervous over-activity causing muscle tension or spasm, sympathetic and parasympathetic imbalance, vascular over-reactivity, hormones that are out of phase, or over-stretching the immune system due to being run down would be appropriate. It is the combination of negative findings for serious pathology; positive findings for a functional disorder, where they exist; and a satisfactory physiological explanation of the symptoms that will help the patientcomes to terms that the symptoms are not organic. The patient understanding does not need to be psychologically based where this is not warranted.
Mind-Body modelling
Models of explaining the mind-body connection are being mentioned here, as it is believed it will aid the understanding of further sections.
The programme of psycho-education must include the clinicians, the non-clinical leaders who help design services and then the patients.The modelling should be neither over-detailed, nor complex. But it should be sufficient to explain the important concepts to aid patient understanding. It should be compatible with clinical
25
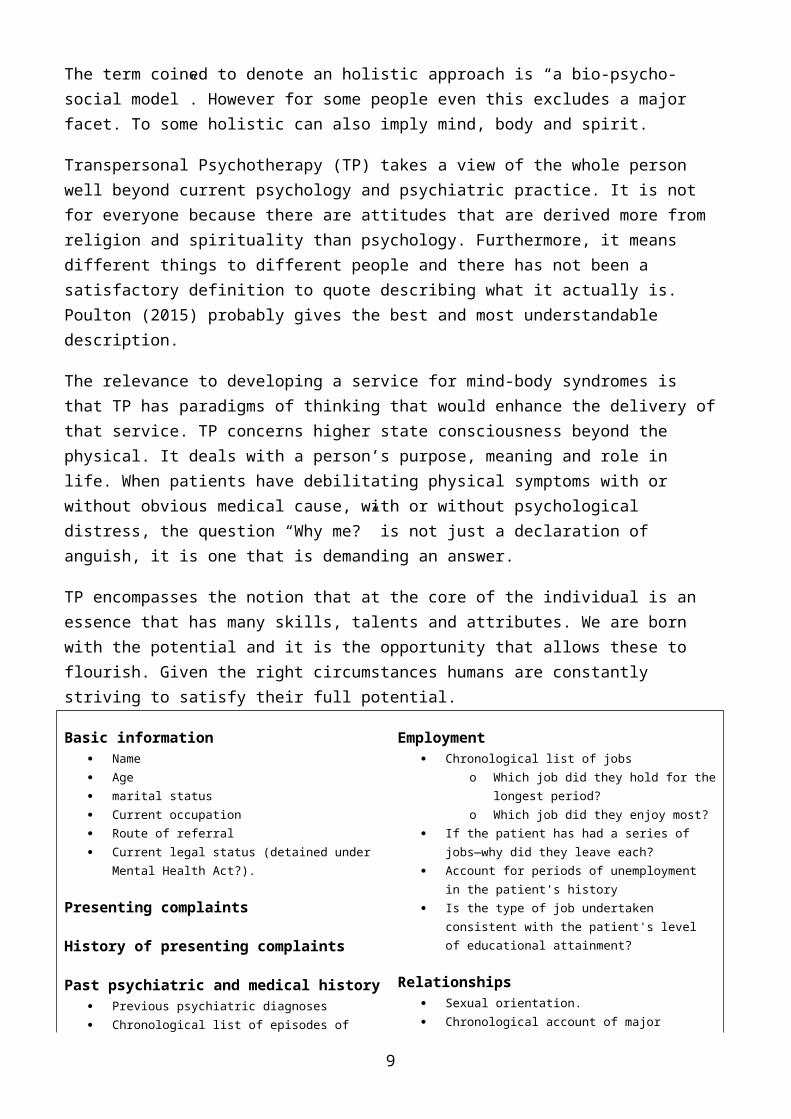
observation. Figures 3 and 4 represent two simple models. The first is Beck’s cognitive model. The second is a more biodynamic approach and specifically drawn up for this paper.
Figure 3. Beck’s Cognitive Model. There is a 5-way bidirectional interaction. This is genuinely bio-psychosocial.
Beck’s cognitive model can be thought of in layers. First is the psychological Cognitive-Behavioural-Emotional (CBE) triangle, which is the basis of CBT. The next layer includes the somatic. When they exist this is where is situated the physical component to symptoms. There is a normal healthy psychosomatic interaction, which when there is over-activity in the one, is reflected by over-activity in the other. And finally is the social setting. It acknowledges how those around us can affect not only how we think or feel, but also our physical well-being. Likewise, if we are poorly, it has consequences on those around. It is a truly 5-way bidirectional bio-psychosocial interaction.
The standard model for illness behaviour self regulation comes from Leventhal et al (1992). The Common Sense model of self regulation describes a cerebral and behavioural homeostatic process in which there is continuing cognitive and emotional representation, practical and emotional coping and on-going appraisal of outcomes. The Bio-dynamic model depicted in Figure 4 has elements of Leventhal’s model but is much simpler to explain. From the patient’s
Social
Environment
Behavioural
Emotional
Somatic
Cognitive
26

perspective it is attractive because it is symmetrical, implying that the physical and mental component are given equal prominence.
Figure 4. A Biodynamic Approach to symptom causation. The mind-body cycle may continue to give rise to symptoms, long after either the mental distress or the physical challenge has abated.
Figure 4 provides a means to explain causation. Essentially ‘Mind’ and ‘Body’ are inter-related. The mental distress and physical challenge are stressors. These respectively produce the reactions ofphysiological responses and cognitive processing. The conscious mindmay only be partly aware of the latter. The reactions may be protracted or incompletely resolved. By the time the patient presents the stressors may have long gone. This is inevitably true for PTSD. Irritable Bowel Syndrome (IBS) may have a prior infective cause. (Camilleri, 2005) The person may not be aware of the originalstressors, but a ‘memory’ of the mind-body pattern persists and the symptoms remain.
Figure 4 is also compatible with another very useful concept. In aiding management it some times helps to consider the 3 ‘P’s of Predisposing, Precipitating and Perpetuating factors. The Physical Challenge and the Mental Distress are equivalent to the
27

Precipitating factors. The individual’s milieu, past and present would determine the Predisposing and Perpetuating factors respectively.
The next level for patients to understand may be the mechanisms by which the cognitive processing results as bodily symptoms. There arethe physical and the psychological explanations. Capek (2012) has summarised how the psychosomatic disorders may be physically mediated. (Figure 5 and Appendix 2) Essentially it may be through the nervous, the cardiovascular, the endocrine or immune systems. Alimentary manifestations may be mediated by the parasympathetic component of the nervous system. For many of the conditions their functional pathogenesis may be multifactorial.
Figure 5. A Mind Map of the Functional Conditions Arising from Psychological Distress. For explanation see main text.
28

Pain is often mediated through muscle tension. As an example, for atypical chest pain, a very simple physical examination that does not even require a doctor is to press the site of the pain. It is very reassuring to find the tender spot. The pain being external is not cardiac, respiratory or oesophageal.
Ewin & Aimer (2006) described the cognitive expressions, which are the psychological precursors that may be behind the bodily manifestations. (Table 5). Looking at the brief examples, it is clear how important it is for all doctors, but particularly GPs, to have the necessary consultation skills. It is partly the recognitionof the psychological cues when they emerge, and partly the asking ofthe right questions to bring out the answers without falsely leadingthe patient.
Once the GPs or others recognise these cognitive expressions it is necessary to show skill and tact to ensure it is not just the doctorwho makes the connection but also the patient. This is usually achieved not by making a statement but by asking the right questions. For example in the case of proven non-cardiac chest pain in a patient whose parent died of a heart attack at the same stage of life, the question may be, “Now that we know that the pain is notfrom your heart, what do you think underlies this pain?” Note the use of the word ‘underlies’ with its implication of subliminal activity. Making a statement has the potential for the patient to block the idea. Asking the right question forces the patient to think in order to hopefully give the right answer.
Cognitive expression Body or Organ language: where the mind uses the body to convey a
messageo As in “It feels as though I have been stabbed in the back” or
“My blood is boiling”. Imprint: another person saying the wrong thing at the wrong time.
o As in “It will leave you with pain for the rest of your life” Guilt or self-punishment
o Recognised by “If only I had done…” or “It is out of characterfor me to…”
Identification: When some one close has had similaro Recognised by “My relative/best friend had these symptoms and
died of…” Trauma
o Recognised by what was happening at the time of onset of the 29

symptom Conflict: for example when having to make a choice but cannot.
o The choice may be between ‘what would like to do’ and ‘what would want to do.’
Hysteria or gaino Not only for compensation but may also be to promote the care
and support from others.Table 5. Possible Psychological Precursors to Non-Organic Symptoms. (based
on Ewin & Aimer, 2006)
These and other examples presented elsewhere to denote the level of skill that clinicians will require.
On the next page is a case history of a teenager who had a functional somatic disorder characterised by heavy periods. There isno magic. It demonstrates what is possible to achieve with a modicumof skill and knowledge.
From patient to patient symptoms arising from reasons other than organic pathology may vary in quantity, severity and longevity. As may already be clear they touch many aspects of the health service. Different professionals, clinical and non-clinical, will require a level of understanding relevant to their role. But regardless of thecontext, the dichotomy between physical health and mental health is not helpful and we need to be thinking in terms of mind and body being fully integrated with each other.
30

CASE HISTORY
Natalie
Natalie was 23 years old when she presented herself to her new GP. There were 2 matters striking from this first consultation. She camewith her mother. Most 23 year olds would be independent, so there was an impression of fragility about her. Second was her request forthe progesterone only contraceptive pill. Not unusual by itself but for the last 8years Natalie had been having very heavy, painful and frequent menstrual bleeds that the combined pill was not able to regularise. The unanswered questions were ‘What is going on here? Why does an otherwise healthy 23-year-old develop such severe primary polymenorrhagia?’ Natalie was aware of the GP’s concerns.
It was the 5th consultation that she first came without her mother. Her last period was essentially normal. It became possible to go deeper.
GP: How many marks out of ten would you give the first 15 years of your life?Natalie: 8.
So no obvious abuse there
GP: What was the worst thing to have happened to you in those first 15 years?
Natalie: I was involved in an accident. The driver had been advised not to drive. He could not see. He thought I was a dog. I hit the bonnet of the car and then the windscreen. I can remember being on the floor and the next thing was waking up in hospital several days later. I was told that my mother had to be chased out of the ambulance as the ambulance drivers were working on me.
GP: Have you ever talked about it?
Natalie: Only in the court.
GP: What was happening to your periods at the time
Natalie: I was on my second period.
31
Notes: It helps knowing how life events can give rise to symptoms, in this case the trauma of the near death experience. It also helps to ask the right questions. Having a positive regard to symptoms, inthis case it is not a problem but a matter to be understood, almost certainly helped her to resolve the issue. The initial positive interest by the GP was probably a factor to help her start the healing process herself. There are 2 not incompatible explanations. The first was that her sub-conscious mind was trying to communicate the presence of a problem, not the periods, but the emotional trauma. The second is that given she was on a period at the time, her neuropsychology associated the emotional trauma and the menses. Shewas referred for CBT to deal with any further emotional aspects of the trauma
32
THE EVIDENCE BASE
Terminology
This section, unless otherwise stated is based upon Henningsen et al(2011a)
It is well known that there is a group of conditions that have physical symptoms with no obvious physical pathology to explain the symptoms and/or the conditions have a psychogenic origin. Over the years the terms used to describe the collection have included psychosomatic medicine, somatoform disorders, functional disorders, functional somatic syndrome, complex somatic symptom disorder and medically unexplained (physical) symptoms. The current favoured termproposed (citing Fink, 2007) is Bodily Distress Syndrome (BDS). There are nuance differences between the terms, though over the years they have at times been used interchangeably used. They all imply the close relationship that exists between mind and body.
BDS, which is the term to be used here, has a clear diagnostic definition based on the number of symptoms presenting. It is well established that the more bodily symptoms the person has, the more likely there will be psychological distress. (Mayou & Farmer, 2002) The term BDS carries no implication of the condition being unidirectional in its aetiology. Indeed between the bodily symptoms and the emotional distress the original aetiology may be in either direction and may be cyclical with the one aggravating the other as a vicious circle.
For clinical purposes, and for the purposes here, a good working concept to be employed is that patients with BDS have physical and emotional distress regardless of whether that emotional distress is either felt by the patient or manifested as an otherwise recognised psychological disorder. That is, the patient with BDS may have physical distress with or without overt psychological distress. The working definition of BDS is in Appendix 3. Figure 6 summarises.
33

Figure 6. A Diagrammatic Description of the Different Terms in Use.
BDS needs to be considered to be distinct from three other common clinical scenarios. They are first the patients with recognised psychological illness, who have an increased susceptibility for organic disease whether it is already established or not. Second arethe patients with recognised organic illness(es) who develop a separate recognised psychological syndrome as a consequence of theirphysical illness. Third are patients with a recognised organic illness who develop secondarily worsening of the symptoms of that physical illness due to psychological reasons. The way the definition of BDS is constructed appears in the main to exclude these three alternative scenarios.
Usage of the terms here will in the main follow that suggested by Creed et al (2011a). MUS is the term to denote all medically unexplained symptoms. It is all encompassing regardless of numbers, severity or chronicity. Somatisation disorders relates to the more severe and chronic end of the spectrum. Functional somatic disordersrelate to specific clinic syndromes, such as IBS, CFS, and Fibromyalgia etc. BDS broadly incorporates somatisation disorders and the specific functional disorders.
Prevalence
MUS
BDS
Somatoform
Disorders
Functional
Somatic Disorder
s
34

This section, unless otherwise stated is based upon Creed et al (2011a). Secondary referencing has in the main been omitted.
Anecdotally, doctors, be they primary care physicians, secondary care physicians or secondary care psychiatrists recognise BDS as a significant clinical issue drawing heavily on financial and human resources without appearing to be helping patients. The scale of theproblem has been assessed.
Citing Cherry et al, (2005), in the USA, a study ranked the diagnostic groups according to the frequency of visits to the doctor. ‘Symptoms, Signs; ill defined conditions, came in 5th with 6.3%% behind conditions of the Respiratory, Nervous, Circulatory andMusculoskeletal systems.
Citing Nimnuan et al (2001), in the UK, the figures for the estimated prevalence of MUPS in 2 London Hospitals over the period 1995-1997 were:
• Chest 59%• Cardiology 56%• Gastroenterology 60%• Rheumatology 58%• Neurology 55%• Dental 49%• Gynaecology 57%
Other studies (year in brackets) appear to reflect similar results. General Medical (1993) 52% Gastro-, neuro & Cardiology
(1996)35%
Gastro-, neuro & Cardiology(2004)
39%
General Medical (2004) 53% Neurology (2001) 30% Neurology (2000) 30% Neurology (2009) 30% General Medical (2009) 50%
The same authors summarised a number of surveys looking at the impact on primary care. The figures below give the incidence of the presenting complaint being ‘medically unexplained’.
35

• Primary care patients presenting with illness (1991) 7-12.6%• Booked consultations (1997) 19%• Primary Care attenders (2004) 23.6%• Sweden (2004) 16%• International, Primary Care attenders with 5+ Medically
Unexplained Symptoms (2001) 15.4%• South Asian primary care population in the UK (2000) 33%
The South Asian population in the UK study reflects common observation that the cultural effect of this population is to minimise mental illness and to somatise psychological distress.
Bridges & Goldberg (1985) estimated that MUPS accounted for 20% of new consultations in primary care.
The prevalence may be based upon surveys of symptoms or on surveys of conditions. The outcomes depend on the definitions of who is to be included and age cohort under study. Definitions also change withtime. Based on a PHQ-15 score greater than or equal to 15 a typical figure is 10%. European surveys of somatoform disorders are in the range 2.1-24.6%. A typical figure is 14%
Lieb et al (2002) studied adolescents ages 14-24 over a 3 and a halfyear period. Their findings were a reported incidence of 25.7% and prevalence of 48%. Their high prevalence in part appears to be due their inclusion criteria. While the symptom count may have varied over time, the presence of a somatoform disorder remained stable.
Creed et al (2011a) pointed out that it is only the persistent MUS leading to distress and/or impairment that are diagnosed as having asomatoform disorder. They conclude that Somatoform disorders occur in 6% of the population, 16% of primary care attenders and up to 33%of patients in secondary care clinics. This definition excludes the functional disorders
The presence of MUPS is associated with other mental health conditions. There is a correlation between borderline personality disorder and the presentation of somatic complaints. (Sansone et al 2008). In psychiatric out patients those who scored above the cut off for BPD had at least twice the number of self-reported symptoms.
36

Burton (2003) reviewed the overlap between MUS and other psychiatricdisorders. In this review, for a variety of reasons, it is difficultto have equivalence between the surveys he reviewed. 2 papers quotedgave figures for both a psychiatric disorder in patients with MUS and then MUS in a psychiatric disorder. The percentages respectivelywere 66-69% and 32-55%. Bridges and Goldberg (Unknown) reckon that 57% of patients with psychiatric disorder fulfilled the criteria forsomatisation.
(IAPT, 2008). State that 70% of those with MUPS have anxiety and depression. They have 50% more consultations, 50% greater healthcare costs and 33% more hospitalisations than those without. It is estimated MUPS makes up 5-10% of in patient care, and there isevidence they are at risk of unnecessary investigations and surgery creating iatrogenic illness. Anecdotally, there are individual patients to whom when looked at retrospectively, this appears true. (Author’s note)
It is not just the morbidity but also possibly an increased mortality. MacFarlane et al, 2001 found for those patients with chronic regional pain or chronic widespread pain there were respectively 21% and 31% increase in deaths, mainly from cancers.
In summary it is a huge problem. Its recognition up until now may reflect the heterogeneity of the condition, and being recognised by too few individuals as being the one broad syndrome that it is.
Healthcare costs
This section, unless otherwise stated is also based upon Creed et al(2011a).
It is believed that potentially there is massive potential for savings to be made to the public purse. Bermingham (2010) studied the financial year 2008-2009. Patients with MUS were 50% and 33% more likely to attend primary or secondary care respectively. Overall the expenditure on patients with medically unexplained symptoms by the health service was estimated at £3.2 billion, that is 10% of the NHS budget for that year. The cost caused by loss of quality of life and days off work was estimated at around £14 billion.
37

A study in the Netherlands (citing Meerding et al, 1998) ranked the diagnostic groups according to their expense and ‘Symptoms, Signs; ill defined conditions, came in 5th at 4.8% behind, Mental Handicap/Downs syndrome, Musculoskeletal, Dementia and other mental disorders.In UK out patients “Signs, Symptoms and ill-defined conditions” was the 4th most expensive category in primary care. After adjustment forchronic illness, psychiatric illness, illness behaviour, health anxiety and demography, the number of somatic symptoms is an independent predictor of consultation frequency.
Specifically Irritable Bowel Syndrome (IBS) in 2006 had an estimatedcost to the UK NHS of £224.11Million. For Chronic Fatigue Syndrome (CFS) the direct healthcare costs was estimated in 2003 at £808/patient. The societal costs of £14,060/patient are due to time lost to work and on the carers.
In the USA the cost of health claims for Fibromyalgia patients was double than for the non-fibromyalgia patients, even though the claims were for numerous other illnesses, rather than the fibromyalgia itself. Another study compared fibromyalgia patients with rheumatoid arthritic patients. They had a similar level of disability, similar costs on claims but twice the additional co-morbidity with other conditions.
A survey in Norway described three independent factors to healthcarecosts, which were age, number of organic illnesses and the number ofbodily symptoms. Like the costs of fibromyalgia, implied is that a large proportion of the costs are due to the associated co-morbid conditions.
The overall impression gained from both the literature and working in the health service is that condition of BDS is being largely ignored. It is noteworthy that while Public Health England gathers much data, including much around mental health disorders, there is nothing specifically on the conditions that comprise BDS. The most closely related entry is on recording admissions to hospital for headaches or migraine. (http://fingertips 2015) The problem appears large. Because of the massive costs, there is high potential for making savings and yet no individual branch of medicine, nor commissioning organisation appears to have taken on the challenge of
38

radically improving the health of these patients that appear to lie between primary care, secondary physical care and mental health care.
Therapies for BDS
This section, unless otherwise stated is based upon Creed et al (2011b).
For the somatoform conditions several therapies have been tried. There is overlap between them but they include the use of anti-depressants, behavioural therapy, Cognitive Behavioural Therapy (CBT), Psychodynamic inter-personal therapy (PIT) and reattribution re-modelling. The last is usually through training GPs to integrate into the consultation a conversation with the patient on how emotional distress, may lead to the symptoms.
The UK-MUST trial (Morriss et al, 2007), which was typical of trialslooking into reattribution, gave GPs 6hrs of training. This led to changes in doctor-patient communication and a more positive attitudeby the doctors, but there was no improvement in terms of the consumption of medical resources, subjective health, sickness absence or symptoms. Furthermore the difficulty in recruiting GPs into this and similar trials was noted
IAPT (2014) clearly recommends the use of CBT as an evidence based treatment.
Citing Kroenke (2007), a review of therapies and CBT had favourable outcomes.
However a study in Sri Lanka (citing Escobar, 2007) demonstrated a high response to a control group with structured care negating the potentially positive outcome. Creed et al point out that by comparing any therapy with usual care or a waiting list control it is easy to demonstrate an improvement. Provide structured care, other therapies also achieve results. They point out the evidence for the first consultation and that it is important to understand the patient’s views of the medically unexplained symptoms compared with the importance of performing investigations.
39

Specific therapeutic approaches will be needed for the different conditions. For example, Chronic Fatigue Syndrome (CFS) therapy willinclude Graded Exercise Therapy (GET)
Creed et al (2003) not only demonstrated the clinical effectiveness of PIT in severe irritable bowel syndrome (IBS) but after the initial outlay to provide the therapy, it was cost effective. Aftera year of follow up the estimated average savings per patient was $687.
NICE and the British Society of Gastroenterology recommend the use of hypnosis in severe IBS.
Peter Whorwell and his team have demonstrated the further benefits of hypnosis in non cardiac, non-dyspeptic chest pain. (Miller et al,2007; Miller & Whorwell, 2009). Accepted to be efficacious in IBS and other functional alimentary disorders, it is therefore not unreasonable to conclude that hypnosis would be effective for most if not all of the BDS conditions. Flammer & Alladin (2007) undertooka meta-analysis for psychosomatic disorders. They concluded that they had demonstrated hypnotherapy to be highly effective in their treatment. They added “that hypnotherapy could be made more effective by including components addressing emotional and underlying factors rather than just focusing on symptoms.” Capek’s own personal audit (see appendix 4) clearly demonstrated overwhelming improvement for many individual patients with a multitude of different psychosomatic and psychological conditions when there is already a well established doctor-patient relationshipand patients were either doctor or patient selected for hypnosis.
For the overall picture it is not that therapies are not available to help these patients. They are, but they are too thinly spread andit is not always possible to match the right patient to the right therapist.
Costs/benefits of therapy
There is a little research studying the cost-benefits of therapy aimed at MUS/BDS. What there is, even within the constraints of clinical trials, does appear to be beneficial.
40

Psycho-dynamic Interpersonal Therapy (PIT), a therapeutic approach used in MUS/BDS has been shown to be cost effective in high utilisers of psychiatric services (Guthrie et al, 1999). In IBS, Creed et al (2003) demonstrated significantly lower healthcare costs. The saving in the Creed study was noted to come from a reduction in the number of gastroenterology out patient visits. Thisstudy also had an additional interesting observation that psychotherapy appeared to have an influence helping to bring patients off welfare benefits whereas the anti-depressant Paroxetinehad the opposite effect.
Parsonage et al (2014) evaluated a new Primary Care Psychotherapy Consultation Service (PCPCS) in The City and Hackney. This service was targeted at patients who because of their complexity fall through gaps in existing service provision, or may be frequent usersof health services, be it in the primary or secondary care settings.While the service was not specifically aimed at patients with MUS/BDS the type of patient they incurred and those with MUS/BDS have similarities. Their estimation is that this service reduced thecosts of NHS service use by £463 per patient in the 22 months following the start of treatment. This represents a quarter off, from what it had been. Of these savings, 66% is accounted for by fewer A&E and outpatient attendances and inpatient stays. Two-thirdsof the savings occurred in the year following therapy. It is estimated that treatment by the PCPCS has a cost per QALY (quality-adjusted life-year) of around £10,900 indicating that the service isgood value for money.
What the Parsonage (2014) and Guthrie (1999) studies suggest is thatintroduce a service where there is an unmet need, there are savings to be made elsewhere that are greater than the cost of the service itself. While one cannot conclude that such an inference applies universally, given that MUS/BDS, particularly at the severe complex end, is known to be a heavy drain on healthcare resources and has a lot of associated morbidity; it is not unreasonable to assume that when managed well the potential savings from the excess healthcare costs will be materialised. The Creed (2003) paper has demonstrated that saving for one form of psychotherapy for one of the functional conditions.
41

Barriers to overcome
Unless otherwise stated this section refers to Henningsen et al (2011b). Secondary referencing has in the main been omitted.
The different terminology between specialties, primary and secondarycare and between countries is highly fragmenting. Different terms emanating from different sources can mean different therapeutic approaches when in reality it is the same condition trying to be treated. The same condition can also be coded in several ways, depending on the source. Regardless, ideally terms need to be acceptable to patients, while at the same time accurately reflect the nature of the condition.
In many countries social policy encourages the fragmentation. Not only is service organisation fully separated into physical health providers and mental health providers with no communication between,but so too is service planning. Payments for services may be item ofservice based for investigations and treatments leaving good communication skills and promoting rehabilitation unrewarded. Work place and insurance companies pay out more for physical illness diagnoses.
General practice may be seen as the place where managing physical and psychological illness meets and can therefore be promoted to manage BDS. While this may be true for the lower end of the spectrum, the evidence suggests that primary care alone cannot cope.Indeed these patients give rise to many in the ‘heart sink’ group. The dynamics of the consultation are such that often doctors and patients do not see ‘eye to eye’ to the dissatisfaction of both. Thedoctor correctly recognises the emotional nature of the symptoms; but the patient erroneously working on the premise that a physical symptom reflects an underlying physical condition wants more tests which the doctor is trying to avoid so as not to reinforce the underlying psychological aetiology.
A number of papers are noted studying consultation dynamics further.There appear to be many factors working together to that focuses theconsultation away from the psychological and onto the physical. Early in the condition’s natural history patients do have thoughts that may be the symptoms are psychologically based. But they do not
42

necessarily offer the suggestion to the doctor. This may be because of their own attitude to psychological illness; or concern about thedoctor’s attitude; or concern that by offering a psychological cause, the doctor will inadequately search for a possible physical condition. Patients with BDS give cues that they seek more emotionalsupport than with symptoms due to disease. These cues are often missed and doctors may not feel comfortable exploring psychological issues.
Salmon et al (2007) the consultation dynamic is described. Patients present with symptoms. Doctors dismiss both the physical and the psychosocial nature of these symptoms. Patients return with increased intensity and number of symptoms. Therefore the doctor implements disease focussed strategies.
The suggestion is to change the somatising behaviour of the doctors.
Service provision
This section, unless otherwise stated is based upon Fink et al (2011b).
A survey of family physicians in Denmark (Fink & Rosendal, 2008) compared Family Physician satisfaction when managing certain conditions. The outcome was 95.3% satisfaction for Physical Disease dropping to 56.7% and 53.6% respectively for mental disorder with orwithout somatic symptoms and MUS. Fink et al (2011) note studies in secondary care out-patients in which typically less than 10% with MUS receive specific treatment with anti-depressants or psychological therapies. They also comment upon the European Consultation Liaison Psychiatry Workgroup study collecting data on 34,500 patients in acute wards of 33 general hospitals across Europe. (citing de Jonge et al, 2001) A prevalence of 14% somatoformdisorder was recorded but only 61(0.002%) patients were referred to a liaison psychiatrist.
Where there is provision and it is very patchy, services are arranged along 3 models. The first is that patients are seen in specialist secondary care clinics such as IBS in gastroenterology and headaches in neurology, etc. with or without liaison psychiatricsupport. Psychiatrists see somatoform and related diagnoses, leaving
43

the bulk of MUS in primary care. This may be the most common model, but it is the most poorly coordinated for patient care. Referral back to the primary care physician with the non-diagnosis of ‘no (insert specialty of choice) disease found ’ This model is good for those patients with a single specific condition, where there are patient support groups for that condition and there is a specific interest of the specialist seeing for that condition.
The second model is where set up there are disease specific clinics such as an IBS service or headache clinics. These may or may not be multi-disciplinary. Primary and secondary care physicians may both refer into these clinics. Psychiatry continues to look after the somatoform disorders. In reality the presence of these clinics is very variable both within and between countries. For example while UK and the Netherlands may have CFS clinics, they are missing in Germany and the Nordic countries. What clinics occur where, tend to be in response to the local political pressure at the time. The drawback of these clinics is that they fail to take a holistic approach to BDS, particularly for the patient with multiple syndromes. Thus not only does it sanction the fragmenting specialty dominated view, but also it becomes wasteful to have patients attendseveral clinics, one for each different syndrome.
The third model is a specialist BDS service in which primary care physicians, secondary care physicians and psychiatrists may all refer into. This would be multi-disciplinary. There may need to be separate programmes for certain specific syndromes. The risk to sucha service is whether it would be able to deal with the large numbers, thus it may only cater for the most severe end, e.g. somatoform disorders and multiple functional disorders. But the advantages would be a pooled skill resource with therapies, e.g. CBT, antidepressants, physical activation beneficial regardless of the diagnosis. It would become easier to meet the prioritised patient’s needs.
The German model is described in detail. Traditionally, in Germany, Psychiatry and psychotherapy have been in opposition to each other with the latter being more closely associated with internal medicineand psychosomatic medicine. Thus there is a long tradition linking psychosomatic medicine with the bio-psychosocial model of classical
44

internal medicine. There are 3 levels of care. The first is basic care. Since 1994 there has been an educational standard in the subject for all doctors and a curriculum of study of 80 hours, of which at least half must be completed during the specialty training.‘More than 60,000 of the 360,000 German GPs have completed courses in psychosomatic basic care. Once the training is completed there are financial incentives to have longer consultations with these patients. There is a model of care, The Extended Reattribution Model(TERM) that sets out the consultation steps to take a patient through.
Level 2 is a collaborative model for physicians and general psychotherapists, both psychodynamic and CBT, working together. Level 3 is for specialised psychosomatic/psychotherapeutic services for those who have the condition severely. The treatments are fully funded by health insurance companies. Levels 2 and 3 suffer from theproblems of being too highly associated with mental health and the associated stigma. For level 3 there is an in-patient option that combines somatic diagnostics with physical and psychological therapies that are more acceptable. Patients have to apply to the insurance company for in-patient treatment, and thus only the most long standing will succeed.
The German approach is the model recommended.
If one is trying to establish a single co-ordinated service it is sensible to use a single over-riding term, such as BDS to describe the various syndromes. The service needs to have psychological/psychiatric and medical/surgical input. The latter is to manage concurrent and/or remedial medical problems. Rehabilitation will be a strong focus so therapists skilled in this,social medicine and physical training will be essential.
Because of the high prevalence and wide spectrum of severity. The model should be stepped-care. To prevent chronicity GPs and other doctors should be trained in the condition to manage appropriately the mild to moderate cases leaving the more severe to the specialistservice.
The location of the specialist service should be within general hospitals to have access to the investigation and treatment services
45

they can provide. It also pulls it away from psychiatric service location with the high risk of stigma and non-attendance. The service should be available to all patients who need it. In particular the service should avoid having specific conditions to qualify for inclusion. Research and Teaching should be available.
Managing the Individual Patient
This section, unless otherwise stated is based upon Creed et al (2011c).
ASSESSMENT
Patient assessment is to determine the following: Presence or otherwise of BDS The nature of BDS, i.e. specific functional syndrome and/or
somatoform disorder Severity of the BDS Any co-existing physical illness Any co-existing psychiatric disorders. Illness behaviour, particularly in the more severe forms.
Patients may be viewed on a spectrum. At one end are the least complex cases, low risk, patients readily willing to talk about psycho-social factors and the conditions are of shorter duration. Atthe other end are the cases that are highly complex, with co-morbid issues, most disabling, poor relationships with doctors, possible litigation and/or disability issues and poor outcome. In the middle are patients with some co-morbidity, which if it can be addressed can prevent a potentially poor outcome to become a favourable one.
The Commissioning Unit of London (2010 describes 2 examples of best practice in which patients are assessed by 3 specialists from different disciplines. At the Functional Neurology Clinic at King’s College Hospital, a psychiatrist, a neurologist and a relevant allied healthcare worker, such as a SALT or a neuro-physiotherapist,all see the patient. At Guy’s and St Thomas’ Foundation Trust the approach for chronic pelvic pain in which consultants in gynaecology, anaesthetics and clinical psychology, each see and thendiscuss the same patient. The patients find it helpful to gain an insight from 3 different perspectives.
46

Assessment may be undertaken over more than one interview and may include relevant investigation. If necessary, to exclude possible but unlikely physical illness, they should be done with informing the patient of the anticipated normal result.
Psychometric testing may be helpful. The 2 most useful measures are the PHQ-15(citing Kroenke et al, 2002) and Whiteley Index of Health Anxiety(citing Welch et al 2009). For the patient who has had multiple physical investigations, all with a negative result, it maybe the psychometric test that will have the first positive outcome.
For the more complex patient, the attitude of the patient towards healthcare professionals, specifically and generally needs to be explored with the patient.
Ultimately there should be a tangible explanation for the symptoms. A balance needs to be made between describing what the patient has and giving unhelpful labels. A thorough and supportive assessment initself has been shown to have some therapeutic benefits. (Fink, 2007)
Finally, the assessment period itself may be used for motivating patients. This may be achieved by:
Covering both physical and psychological nature of the complaints
Including the patient’s understanding regarding cause and seriousness
The health professional being supportive Giving an explanation of the symptoms is given in a tangible
way that promotes self-management.
TREATMENT
With mild to moderate cases the aim will be to restore full functioning and minimise the symptom. In the severe cases, it may beonly to restore the function and well-being.
4 important tasks are proposed for clinicians to do to assist management. This is within the capability of all doctors, regardlessof training.
Explain how symptoms may develop in the absence of underlying physical illness.
47

Specific measures the patient can take to alleviate symptoms Discuss the role of self-medication, some of which may be
helpful and others clearly not. Consider giving patients written literature.
A stepped care approach is suggested. The broad outlines are: Step 1: Keep management within primary care.
o Reassure regarding there being no organic illness with an explanation to how the psychological factors may perpetuate
o Provide symptomatic reliefo Encourage a healthy lifestyle including exercise and
dietary change as necessaryo Consider an anti-depressant if requiredo If required guide away from illness patterns of behaviouro If required encourage reframing within a bio-psychosocial
modelo If necessary arrange regular reviews to prevent symptom
exacerbation as the trigger for making an appointment. Step 2: Refer to secondary care
o Refer to a mental health specialisto May need to refer to a physician if there are new symptoms
or worsening of existing symptoms suggesting concomitant organic illness.
Step 3: Refer to a multi-disciplinary team
The Commissioning support for London(2010) presented a stepped care model for its management, not dissimilar to the IAPT model for common psychological ailments. This was followed up by an implementation report in 2011. This document provides a good description on a model of care to be provided by GPs. One of the essential first steps was to simply Reed Code the relevant patients with ‘16H-unexplained symptoms continue’ Other Reed codes are available but they are too psychiatrically loaded to be acceptable to patients.
Specialist treatments include CBT and Psychodynamic Interpersonal Therapy (PIT). The first challenges and tries to break the vicious circles between the symptoms themselves and the associated thoughts,behaviours and feeling. PIT attempts to address assumed unresolved
48

underlying emotional factors that may have been predisposing, precipitating or perpetuating reasons for the symptoms.
Both therapies encourage the patient to take responsibility for their own well-being, indeed they both require the active participation of the patient, Symptom diaries can help in this respect, though by highlighting the symptoms, they can make the patient worse initially.
‘Activation’, the process by which patients undertake more activity,is seen as an important component in the management. This may for example be in the form of GET for CFS.
Because therapies aim to alter the behavioural response to symptoms,part of the management strategy to be included is the doctor’s response to the reassurance-seeking patient. The GP can challenge the patient to come up with more plausible explanations. By not responding as previously, hopefully the patient’s behaviour will be extinguished as it would for other anxiety disorders.
Therapies for severe BDS may trigger or exacerbate depression or anxiety.
In using brief PIT, it is suggested to use a ‘farewell letter’. Thus, the farewell letter aims to highlight that ‘therapy’ is not simply a course of treatment but a life attitude change to be continued long after the sessions have been completed. The farewell letter states, the starting position, describes the progress made thus reinforcing it, and encourages future steps the patient may wish to take.
Pharmacological agents may be used for symptomatic relief. In general terms they help in the short term. Anti-depressants help notonly for the concomitant mood disorder but also as an analgesic, to reduce somatic symptoms and to aid commencing exercise. There is little information on their long-term use. Its role needs to be discussed with the patient, so as to be agreed and not misconstrued.
Training
This section, unless otherwise stated is based upon Fink et al (2011c).
49

Various models have been tried, primarily to train GPs. One prominently proposed is that of the Danish model, TERM that stands for The Extended Reattribution and Management Model (citing Fink et al, 2002). The training is comprehensive. There is a 2 day residential course followed by three 2 hour evening meetings at one or two week intervals and a booster meeting after 3 months. There isa focus on consultation skills with quality history taking and empathic feedback to the patient. Thenceforth it is possible to re-negotiate a new model of understanding. In the light of the patient’s perceptions and health beliefs. Management depends on severity. The training involves a lot of doctor/patient role-playingand videoing of doctor/actor role-playing.
After training half the GPs and not the other half, the main outcomes were as follows:
The GPs who took part felt more confident, comfortable and satisfied than those who had not.
The GPs discussed more psychosocial issues with the patients after their training.
Patients were significantly more satisfied with the consultation from a trained GP.
Patients with somatoform disorders had less physical disabilityat 2 years. Patients with MUS, according to the GP showed no significant improvement.
For those with somatoform disorders there was less in the intervention group but this was not statistically significant at the 5% level.
The German system allowed for psychosomatic training to take the TERM model and develop it further. There are 3 stages to the re-modelling process. The first is simply to challenge the patient’s current beliefs. What do you feel caused the symptoms? What do they indicate? For some patients that is all that may be tried. The second level is to develop an alternative disease model. The third level is to take the original response based around physical symptoms and replace it with confronting the psychosocial situationsthat previously were avoided.
There is a general need for up-skilling any health professional who comes in contact with such patients. For specialist physicians the
50
full programme as described above is unrealistic. A more modest goalmay be to promote the development of the skill to recognise MUS/BDS and have the initial conversation with the patient. Training would need to be tailored, e.g. without training, non-medical professionals may find it difficult to have the authority to state to the patient that there is no organic disease behind the patient’ssymptoms.
Training can be done to several degrees. A comprehensive curriculum would include:
Knowledge about the conditions. Diagnostics Bio-psychosocial thinking Needs led thinking Consultation skills Pharmacological considerations Psycho education and basic supportive care Attribution re-modelling Therapeutic training.
Not every practitioner will require all components.
Unlike other countries, the German model has specialists specifically trained in psychosomatics. The training is longer and exceeds that for general psychotherapy or psychiatry. It also ensures that covered are both psychoanalytic and behavioural models of therapy.
The German model, while possibly ideal is largely unattainable in this country. But there does need to be an emphasis. The training needs to start by giving the subject higher priority in medical schools and then on the GP and specialist training courses. It no longer seems right that specialist training does not train how to best manage the high numbers coming through the clinics with a condition that is not part of the specialty. (Author’s opinion)
Considerations for service development
This section, unless otherwise stated is based upon Creed et al (2011d).
51
It is important to use whatever language or phrase is appropriate for the patient. The service should be ‘need’ led, i.e. be able to deal with the needs of the local population and individual patients.Sometimes that need may be relatively simple like having the multiple somatic symptoms being recognised as a BDS condition. The ‘need’ should be couched in terms people without medical knowledge should understand. In the UK GPs being at the forefront for commissioning services is helpful. Patients and self-help organisations should also be involved.
Service development should have clear aims and objectives that are both achievable and measurable. Healthcare planners focus on priorities. The local understanding of how healthcare priorities aredetermined is essential to improving services for BDS. But services for BDS are not seen as high priority by either physical health or psychiatric health services.
Service planners and those promoting them need to be realistic. There will be start up costs, particularly regarding training and due to administrative changes. Savings will be delayed until the service is up and running. By having a specialist BDS service the largest savings from the Healthcare budget will come not by preventing the first inappropriate referral, but the second. The largest savings will be the societal costs, estimated to be £13 billion annually (Bermingham et al 2010). Being outside the healthcare budget, this is not so appealing to the healthcare decision makers.
Consideration needs to be given to piloting, implementation and rollout. Service development will need to be based upon what is already on the ground and the interests of the local trendsetters.
Whatever model is decided, the role of GPs is essential, as is a specialist multi-disciplinary team. They will not be able to see everyone. GPs will need to be further skilled and clinically supported by the specialist service. The training of medical specialists to recognise the BDS conditions, advise patients of anticipated negative results and initiate the conversation around symptoms, should be part of the package. Helpful literature on patient symptoms will need to be written.
52

A systems approach to MUS in Plymouth was described. Their experience gives rise to some key learning points. They had a stakeholder event in which 27 practitioners from 8 professional groups attended. Despite this, having agreement with so many partiesmade it difficult.
Managing co-morbid and anxiety was accepted but there was no agreement that the local IAPT service should provide the CBT component for patients with MUS. There was a concern whether those patients who saw their symptoms as being physical would accept an overtly framed mental health service. Consultants in secondary carewould find a ‘psychological toolkit’ useful, as this was not coveredin their training. Patient information leaflets to support consultations were written. The patient representatives insisted that the term ‘medically unexplained symptoms’ was removed. Risk management and missing organic diagnoses were concerns. There were problems with the referral template into secondary care that did notallow for the possibility of MUS without labelling it a disease. It was a challenge to engage GPs who had little interest in the topic.
Service development in Plymouth is moving on. It is acknowledged there are:
Close professional relationships and co-location of the staff Clearly identified leaders who ‘champion’ the service Gradual development of the service Use of case managers who work in under close supervision of
experienced psychiatrists. A triage system to identify and work with the complex cases Mental health staff prepared to fit in with the medical
setting.
A VISION OF PROVIDING A COMPREHENSIVE SERVICE
A stepped care model
Medically unexplained Symptoms (MUS) and Bodily Distress Syndrome (BDS) covers a broad spectrum of conditions and severity. They all need to be catered for. The condition lends itself well for stepped care arrangements. The Commissioning Support Unit for London (2012) proposes a 3-stepped model. Here is presented a 4-step model.
A stepped care approach (Table 7) should not prevent patient entry to a higher level if required. The advantage is that when working
53

well, patients can be stepped up with each step building on the previous. Thus if required, this hopefully may make a successful outcome at step 4 easier.
Who is providing Nature and focus of the interventionStep 1
GPs. Specialists who
meet these patients in their clinics
Prevention of deterioration Reassure no harm will come Psycho-education-including bio-
psychosocial reframing Provide written literature Provide symptomatic relief Consider anti-depressants as
appropriate Break the reassurance seeking
behaviours, if necessary by regular appointments.
Step 2
Self-help services
Psycho-education providing mind-bodyconcepts allowing patients to formulate their own framework for personal self understanding.
Low-intensity psychological and psychosocial interventions as required.
Provide insight and support to dealing with potential perpetuating factors.
cCBT ‘Activation’
Step 3
Higher well-being services that includes psychological training (IAPT-equivalent)
Time limited CBT Time limited PIT GPwSI supported to be able to
reassess on-going symptoms, deteriorating or new symptoms.
Step 4
A proposed new specialist service for BDS
To manage by an MDT approach, the most complex and entrenched cases.
To manage those cases where the symptoms from physical illness are out of proportion to the severity ofthe condition.
Eclectic mix of therapies availableTable 7. A Stepped Care Approach.
54

The stepped care model is only a guideline. There is clearly overlapbetween the nature of the service provided and who provides that service. For example the latter will depend on the training, experience and comfort of the provider. As a further example breaking the reassurance seeking behaviour by the GP and giving regular appointments may be as part of the plan for patients being seen in step 4. And as a final example psychosocial support while indicated in this stepped care for Steps 2 and 4 should not be excluded from Steps 1 and 3.
The role of the GP
The GP has been described as the ‘gatekeeper’ to the NHS and never more important has this role been. It is the GP who determines whether a particular patient will be managed down a physical route, a psychological one, or kept in primary care. Patients present with symptoms all the time. It is the constant triaging of these symptomsthat GPs do. There is a natural desire not to miss a serious physical condition, but in so doing avoidance of iatrogenically creating the somatoform patient must now be given greater priority. There are many aspects of GP training that can assist in safely achieving this balance. These include the focus on consultation skills, by exploring the patient’s ideas, concerns and expectations over symptoms; managing uncertainty and safety netting. Figure 7 presents an algorithm for the first time management of patient’s symptoms is proposed.
55

Figure 7. The GP’s Management Algorithm for the first presentation of a symptom the GP anticipates will be medically unexplained. The words used and their predictive value are to try and help resolution before chronicity sets in.
For the symptoms that have developed a degree of chronicity but still without a physical cause a different approach may be needed. The patient may not be able to discard a physical aetiology, but mayaccept there is a psychological component or can be helped by psychological methods even if it is a physical condition.
Patient presents with symptoms, unlikely to be
physically significant.
Advise the specialist, “I would be grateful if you would reasonably exclude serious
pathology. I will then be able to manage the patient’s symptoms.”
Advise patient, “The concerns you raise would not give rise to the symptoms you describe. I think we
can safely wait but is there anything you feel you would like
me to do?”Advise patient, “We can deal with whatever the results show, but I anticipate they will all
come back clear.”
Advise patient, “I agree. If it persists or something new emerges please come back, but
I am anticipating your symptoms will settle.”
Do not fall out with the patient.
Acknowledge, explore and meet
patient’s concerns about symptoms as
appropriate.
Patient acknowledges the likelihood of the symptoms being psychologically
based.
Advise patient, “I anticipate the specialist will not find any
serious pathology. If that is so we can then work out how to best
help these symptoms.”
Yes
No
Manage within the consultation
Refer patient for investigation
Refer patient for second opinion
56

TRAINING
Because of the large disparity between general practitioner recognition of MUS and its prevalence, all GPs will need to be up skilled. Medical student and GP specialist training are good places to start and can help. With medico-political will a training programme for all GPs is perfectly feasible as Clinical Commissioning Groups (CCGs) are able to make attendance at courses compulsory. It just then needs to make the courses interesting and relevant.
Material that could and possibly should be included is: Enhancing general mental health skills and knowledge Enhancing knowledge and understanding of MUS/BDS Enhancing easiness with emotional talk Re-attribution training of MUS
There is much overlap between all of these. Enhancing the general mental health skills is important not only in its own right. There is co-morbidity, which needs to be managed. Some patients are emotionally worse before they become better. Psychodynamically the patients may be somatising as a means not to be aware of the emotional underpinning. Doctors need to feel comfortable managing the underlying emotion.
The Role of the Physical Health Specialist
The specialist needs to be very clear about his own management pathways. And when further investigation becomes clinically meaningless. The same cues that patients give to GPs could easily be given to consultants. Once the specialist has determined the patient’s complaints occur outside his usual remit the challenge is to send the patient back without the patient leaving thinking it hasbeen a waste of time. Explanations can remain simple. For example, “I have seen the back of your nose and throat, and your vocal cords and I am satisfied everything is as it should be.” Phrases from patients such as, “I was hoping you would find something wrong, because then I would know what I am dealing with.” can be very telling. The specialist would do well to highlight this back to the GP to encourage the GP to explore further.
57
A number of the conditions in Figure 5, page 20 have had surgical treatments to them. While surgeons may see their prime skills are with their hands they too need to be aware of BDS. Treating BDS by irremediable surgery is just adding to the patient’s problems. But on the other hand, for the surgeon to do nothing can be difficult. The younger woman with urinary incontinence or retention with no obvious pathology does not present with easy options. Arguments by patients can be persuasive, such as that for a hysterectomy by a patient with polymenorrhagia: “I was abused as a child, I don’t wantchildren because I would end up abusing them and I don’t want that.”
Screening for BDS may well need to be an early intervention. Many consultants have specialist nurses. It may be these nurses who will be best able to have the conversation with the patients and be trained for such.
Leaflets will help. But before they can be issued, these need to be acceptable to the specialist issuing and the relevant patient group.
The role of Self Help and High Intensity Well-being services
The current self-help service for common psychological problems provides easily accessible information and baseline advice for patients with these problems. There is no reason why with suitable training this role could not be expanded to include advice on MUS.
With a small group of patients, 16 in the treatment arm, Burton et al (2012) showed that a GP with a special interest in MUS could makea difference. His study compared standard care and 4 sessions with the GPwSI lasting in turn 60, 20, 20 and 20 minutes over standard care alone. The approach was not intended to be therapeutic or to demonstrate other benefits, but to show the acceptability for patients to have a discussion on their symptoms. This model would betransferable but it would need proper evaluation.
The concern for non-medical staff of advising patients on symptom management but with genuine organic illness can be allayed. Current behaviour patterns are for GPs to consider and reasonably exclude organic illness first, and referral for symptom relief comes very much later. The second level of safety, will be on any mental health
58

triaging process in place. Anything obviously missed can be and willbe sent back for further examination. Finally as the number of sessions with trained personal at self-help is small, the patient will very quickly be returned. If the patient is attending still believing they have an undiagnosed organic condition, they are probably not suitable for Step 2.
The High Intensity Well-being Service is a suggested title to avoid the use of a term too psychologically loaded. It is equivalent to the current step 3 IAPT level of service. The current training curriculum (IAPT, 2011) covers health anxiety but none of MUS in itsown right, the functional somatic disorders nor the somatoform disorders. The staff are likely to require training in these areas.
GPwSI and/or Liaison Psychiatrist support and supervision are essential. Training in appropriate symptomatic management for these doctors is likely to be beneficial and ought to be given.
A specialist BDS service
PREAMBLE
In the description there are many variables and many unknowns. On occasions the description appears to describe alternatives or to be promoting a specific structure or outcome. These are mentioned for discussion and not necessarily as a current preferred position.
TITLE
What such a service is called is as fundamental as what it does. Criteria for a good title need to satisfy the following conditions
Acceptable to patients:o To those who do not accept the psychological nature of
their symptomso To those of ethnic background that shuns mental health
disordero In particular, it must not be stigmatisingo It does not disaffirm genuine physical illness
Acceptable and useable to potential staff who would be able to refer easily to it
59
Conveys to those who are likely to refer to the service what itdoes
Affirms the multi-disciplinary nature of the service Encourages the connection between mind and body, and by
corollary discourages dualistic thinking Portrays its ethos (optionally has an easy acronym)
The Oldham and Leeds units both have the terms ‘psychological medicine’. But this is a term also used to denote psychiatry, as in the DPM, Diploma in Psychological Medicine. Before such a service iscommissioned consulting widely on its name may well be time and money well invested.
A possible title is to call the Step 4 specialist service a Centre for Advanced Holistic Medicine. Thus in Manchester the unit would becalled Manchester CAHM (sounding like ‘Manchester Calm’, though if preferred Centre for Advanced hoListic Medicine would have the same effect.)
ETHOS OF SERVICE
The ethos of any service conveys the attitudes to be upheld. It is now accepted practice that all patients should be treated equally and a service should be open to all regardless of age, race, etc. This list contains the additional elements specific to a BDS service. The list should not be seen as being exhaustive but those matters listed are its basis:
1) Excellence
This may be stating the obvious, but it needs particular emphasis. Such a service as is described here will be a pioneer site for the country. How it functions and its outcomes will be closely observed by those elsewhere. Getting it right first time will mean that the model may be successfully repeated elsewhere. Failings will hold back its dissemination.
2) Successful management outcome is based on a healthy doctor-patient (Client-carer) and service user-service relationships.
60

This is also stating the obvious but again needs emphasising. This group of patients having been notoriously hungry on resources are a significant source of ‘heart sink’ patients. Indeed the patient’s history may have several failed therapeutic relationships behind it.These patients entering the service will have nowhere else to go. Therefore it is important that the relationship the patient has withthe service and the staff is constantly promoted and not allowed to drop.
3) Service providers are aware that every word said may be remembered and may be inadvertently harmful as well as being intentionally beneficial. Thus every word said by a therapist should have a therapeutic intention.
Another truism. There is a fine balance between a specialist giving a patient the honest assessment and allowing patients to come to their own conclusions. Therapists should not rush to suppositions and assumptions, which through initial over-zealous investigation may have been in part the reason the BDS has developed. Ideally patient and therapist should come up with a formulation that the patient is very comfortable with.
4) Symptoms are not problems but messages reflecting mind-body communication. They are signals to alert the mind that there may be a matter to be addressed.
It is more than semantics. It is also about changing attitudes. Reframing the concept of what a symptom is allows a more helpful attitude towards them can be developed. Taking the idea of Williamson (2008) that symptoms always have positive intent, this istrue for the crushing central chest pain, the haemoptysis and the back pain with problems of micturition. In all of these the mind has alerted us to a physical health matter that needs attention. In the absence of physical illness, symptoms can also alert us to psychological distress. These may be simple such as the lethargy evoked at the thought of going into a stressful work environment. Orthey may become complex and develop into a BDS syndrome. The symptoms may still be the mind sending a signal to alert the person.That neither patient nor therapist can interpret the message from the signal does not negate the mind’s intention. What it does do is to change the attitude. It does ask what happened that the mind is
61

now sending me a signal and what is the message? Instead of stagnating the patient’s mind with the symptom(s), it is asking a question to which the patient at some time may come up with an answer and hence move forward.
5) The patient is, as far as possible, to be fully understood. That is not only the physical symptoms in the context of other physical illness and the patient’s current situation, but also inthe context of the patient’s life ‘from cradle to the grave’.
This is anything but obvious and for many practitioners may involve a paradigm shift. This is about generating an attitude that not onlyviews the patient in the present with the BDS symptoms but also in the setting of the patient’s unfinished life story. It is about understanding the development of the condition from a time long before the symptoms started, in the context of the patient’s hopes and aspirations and how these can or cannot be met in the future. Itis acknowledging that for the duration that the patient is under themanagement of the service, this is merely a point in time in the context of the longevity of the patient’s life. Such an attitude is aimed at the staff to not only think about the patient in the present with the symptoms but also his past in the sense of where hecame from and his future to where he is going.
This and the previous item should enable staff to develop a much deeper understanding than simply seeing a symptom as a problem or a condition but an aspect of the person to guide the therapist and thepatient through therapeutic choices.
6) The patient determines the end point, i.e. whether the aim is forthe alleviation of the symptoms to be full, partial or simply accepted and managed psychosocially.
This is aimed at empowering the patient. It allows the highly motivated patient to achieve complete resolution without suggesting that less will be achieved. It also allows help for those whose circumstances do not permit the deep-rooted psychological work.
MANAGEMENT CONSIDERATIONS
There is likely to be much debate on this matter. The service will need to be autonomously managed to ensure its function is not
62

undermined. Whether this should be as a service independent of otherlocal providers or as a subsidiary unit of one of them remains to beseen. The latter approach will have benefits with administration and with part time clinicians who may have another role. The drawback that would need to be met is the image of the parent Trust.For example Pennine Care has a name with an image likely to be acceptable. Within it, the most relevant Department of PsychologicalMedicine, which possibly has too much of a mental connotation for many. A third option may be that an existing Trust takes on the initial responsibility of its management with a view to its subsequent independence.
Another issue is how should the new BDS service relate to existing specialist services. There could be resistance. It is important not to dilute the expertise by fragmenting the remit, therefore the recommendation here is to include current functional disorders service within the scope of a specialised BDS service. Thus a local service where there is a unit with specialist expertise, such as forCFS, IBS, fibromyalgia, chronic pain or headache could reasonably beincluded.
63
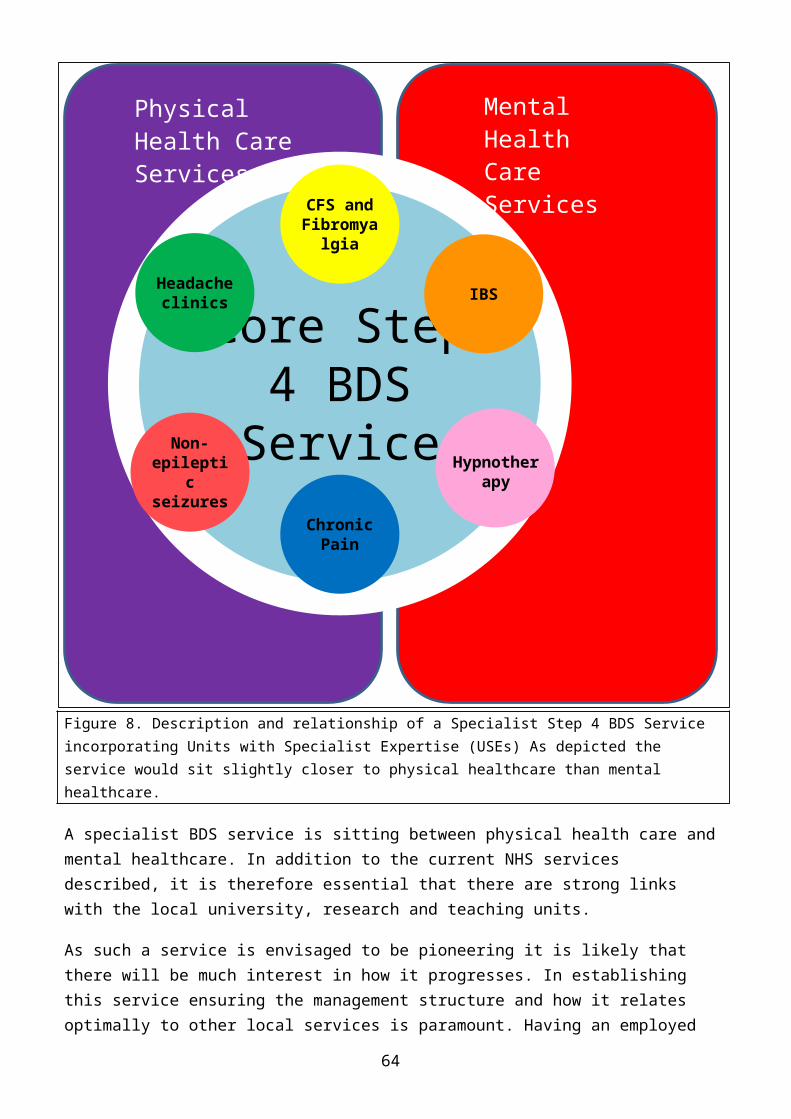
Figure 8. Description and relationship of a Specialist Step 4 BDS Service incorporating Units with Specialist Expertise (USEs) As depicted the service would sit slightly closer to physical healthcare than mental healthcare.
A specialist BDS service is sitting between physical health care andmental healthcare. In addition to the current NHS services described, it is therefore essential that there are strong links with the local university, research and teaching units.
As such a service is envisaged to be pioneering it is likely that there will be much interest in how it progresses. In establishing this service ensuring the management structure and how it relates optimally to other local services is paramount. Having an employed
Core Step 4 BDS
Service
CFS and Fibromya
lgia
IBS
Hypnotherapy
Chronic Pain
Non-epilepti
c seizures
Headache clinics
Physical Health Care Services
Mental Health Care Services
64

researcher in residence to provide the link between the clinical andmanagerial expertise, advice on good practice and for reporting the outcomes of service changes is recommended.
WHO IT IS FOR
This service is for patients registered with the defined GPs.
The service is an adult service for ages 16 onwards. There will be no upper age limit though referrers may need to justify further how the service will benefit patients aged beyond 65.
The service in the main should be for the moderate to severe end of the BDS spectrum. There should be no distinction in access between those patients who have a recognised specific somatic condition or amore generalised somatoform disorder. The service must be ready to see proportionately more with less severe BDS but whose psychological insight is constrained.
Patients with BDS who also have a confirmed physical illness will not be excluded. Indeed these may be the most complex and most needypatients. Another high priority group for the service would be thosepatients who have physical illness but the symptoms are out of proportion to the severity of the condition. It is these patients that provide the highest challenge and by breaking the ‘revolving door’ cycle may provide the savings to fund the service. The serviceshould manage those patients who would fulfil diagnostic criteria for a personality disorder and where physical symptoms are a significant part of the condition. The service should not take on the role of post-illness rehabilitation as in cardiac or pulmonary rehabilitation. But it may see these patients if after such a programme difficulties remain.
Patients should be sufficiently cognitively aware to allow discussion on the nature of their own symptoms.
STAFFING
The Centre will be staffed by a multidisciplinary team, with the following elements:
• Medical
65
o Liaison psychiatry doctorso Anaesthetisto GPwSIo General physiciano General and/or orthopaedic surgeon
• Therapeutico Clinical psychologistso CBT therapistso Psycho-dynamic Inter-personal therapistso RMNso Physiotherapists with MH Trainingo MH Occupational therapistso MH Social Workers
• Allied professionso Physiotherapyo Dieteticso Pharmacist
• Administrative support.
There will be training grades in addition.
While the therapeutic staff, may have a particular model of training, they are expected to possess and use eclectic skills. All therapists will have regular 1-to-1 peer supervision.
The medical staff is all likely to be part time and the therapeutic staff may have full time posts available. The exact proportions may vary from time to time according to need.
There will be regular meetings with all the team members attending. These are anticipated to be weekly or fortnightly according to the duration and the agenda. The team meetings will allow cross skillingso that all team members will benefit from the experience of the fellow members.
REFERRALS
Referrals may be made by any GP.
It is essential that prior to the referral that the GP has reasonably excluded genuine physical illness. This will be differentfor the different presentations but the referrer should be able to
66

state why conditions potentially on the differential diagnosis list do not apply. For example, for a symptom of chronic lethargy a FBC, U+Es, LFTs, Fasting blood Glucose, TFTs, Vitamin B12, Folic Acid andFerritin would be seen to exclude associated physical diagnosis.
The liaison psychiatrists may assess patients on the wards for the consultant medical, surgical and psychiatric colleagues. Where it isappropriate for there to be on-going care following such an assessment the service must confirm with the GPs that they are agreeable.
GPs should make any information requested by the service available. Secondary sector providers should be expected to do the same.
WHAT IT WILL DO
By taking a thorough overview of the patients referred, the aim is to significantly improve the health and quality of life of those patients who have significant impairment in function due to their physical symptoms. There will be a bio-psychosocial (holistic) approach to assessing and treating the full range of patients’ problems. It will be needs and patient preference led, but drawing upon the best evidence available. Thus social matters that may be perpetuating the condition will be attended to first.
Patients requiring this service will already have seen many healthcare professionals. As a successful outcome is based upon a healthy client-carer relationship the nature of previous such relationships the patient has had will be explored. If necessary andin a non-accusatory manner, the risks of potential future breakdown with the service and how this may be prevented will be discussed.
On initial assessment the patient can expect to see at least 2 and may be 3 different team members each from a different discipline. These will be selected based on the information made available in the referral letter. If possible, and if all the necessary information is at the team’s disposal, on the day, the patient but advised by the team will prepare and agree a therapeutic strategy, otherwise it will take place when ready.
Part of the assessment will include as far as possible a biophysicalexplanation for the manifestation of each symptom.
67

The patient will move from assessment to the therapeutic program. This may include seeing one of the therapists for up to 20 sessions.This should not be viewed as an absolute limit if substantial progress has been made and further sessions beyond the 20 can be reasonably anticipated to yield further gains.
The service is patient-centred and needs-led. Therapy will be eclectic. Thus while therapists will need to understand and be familiar in the use of a wide variety of therapeutic models, the therapists at times may need to move freely between the models. Thuswhile the mainstay of therapy may be a CBT or PIT approach, the therapist may wish to combine this with, for example, hypnotherapy. For example Assen Alladin is a cognitive hypnotherapist. He combinesmindfulness and cognitive work in the patient’s hypnotic trance state with results that are superior than for CBT alone. (Alladin, 2009). Such an approach would be imaginative but at the same time provide evidence based care.
The service should establish the practice of closing cases with a ‘farewell letter’
LINKS WITH OTHER SERVICES
This will be as appropriate. In the course of the assessment or review conditions of a genuine physical nature may arise or be suspected. This will need to be managed accordingly and it may be that therapy may have to be interrupted or postponed. While the therapeutic side is intended to be self-sufficient, there may need to be specific skills, such as psychosexual counselling to be brought in.
The service should have links to support the medical and surgical clinics. This would be to provide advice and be available for secondopinions
MONITORING
Appropriate pre-, mid- and post- therapy psychometric measuring willtake place. Regular audits will be undertaken.
TEACHING AND RESEARCH
68

The unit will be encouraged to take part in both, teaching and clinical research. Training for this important subject needs to start with medical students. It would be hoped that a space can be found within the medical education curriculum. A strong case could be made to have posts at foundation and specialist training levels.
MANAGING THE COST OF AN MUS/BDS SERVICE
Up until now the financial aspects of such a service has not been included. This is to be corrected.
Bermingham’s (2010) analysis is that overall, including social care costs; MUS/BDS was costing the national exchequer £14 billion of which £3.2 billion (10% of the whole healthcare budget) was direct healthcare costs. A comprehensive specialist MUS/BDS/Liaison psychiatry unit as described by the South West SCN and that may be staffed as described above on page xx is estimated to cost £4.5 million.
Any service has a cost to it. By focussing clinically on the real issues, and reducing long-term morbidity there are savings to be made elsewhere. The challenge is to make the savings while managing the expenses of lead in costs. In practice how may the financial considerations be managed?
Each area will need to look at its local services and needs but for Steps 1, 2 and 3 as described above, managing MUS/BDS can usually beincorporated into the current structures and teams. Additional costsshould be minimal if any, and will relate only to training and education. The CCGs and the hospital directorates should already have educational processes in place that can be tapped into, thus any costs can be absorbed within current arrangements.
Step 4 is the high end dedicated service. Savings are anticipated but it is difficult to make predictions to their level.
The estimated cost of an MUS/BDS service for a 500-bed district general hospital is £4.5 million.
Parsonage et al (2012) has attempted to make the calculations for a liaison psychiatry service that aims to manage both the psychological co-morbidity that occurs in the secondary sector and
69
MUS/BDS. The best estimates for the whole of the NHS are £4.2 billion and £1.8 billion respectively giving a total of £6 billion. As a guideline figure, the estimated reduction in health care costs per patient, by introducing psychological interventions for patientswith physical conditions being treated in acute hospitals and similar settings is on average about 20%. (Chiles et al, 1999). Thisfigure is a little less but in keeping with that estimated from the City and Hackney PCPCS study. (Parsonage et al, 2014)
For planning purposes, it is better to be cautious. This seems like a good basis to make the calculations. Savings on this scale translate to potential cost reductions of around £1.2 billion a year(20% of £6 billion) at the national level, or £5 million a year for a typical 500-bed general hospital, based on an investment of £5 million annually. Estimated 20% savings, implies invest £5 million, and there is a potential £5 million of which £1 million will materialise.
The reasons for only a percentage of the potential savings materialising can be found in Chiles’ study. (1999) In his meta-analysis of various treatments, all patients in the studies’ cohortswere identified. The estimate of £5 million implies that all hospital co-morbidity and all MUS/BDS is uncovered, managed and resolved. There is a big difference between a research project that is able to account for every patient in the study and all the patients going through all departments in a large DGH. The latter isidealistic but clearly unrealistic, particularly for the present andnear future. Much of the psychological distress is hidden. As explained above much of the distress will have an inadvertent iatrogenic component to it. Even a comprehensive multi-disciplinary liaison psychiatry/MUS/BDS service could not possibly hope to successfully address that level of psychopathology.
It is not the introduction of an MUS/BDS service alone that will result in the savings but the totality of care that will also need to come from other services. The savings can be expected to arise bythe following processes:
A needs-led service will be more efficient as patients will be more readily satisfied thus generally reducing clinician carer contact.
70

A programme of psycho-education to patients regarding mind-bodyintegration, that will supplement the work of the practitionersin steps 1, 2 and 3 thus reducing the pressure on step 4 or preparing the patient for a step 4 referral instead of an acuteTrust referral.
A reduction of first referrals to acute Trusts for conditions due to an increased ability by general practitioners to confidently recognise MUS/BDS.
A reduction in iatrogenic MUS/BDS by clinicians being more aware of the power of their own words and avoiding phrase usagethat may be misinterpreted by and harmful to patients.
Specialists in acute Trusts once trained to recognise MUS/BDS within their own specialty can have the initial conversation regarding its management, thus reducing future secondary care provision. This could be delegated to specialist nurses.
Within acute Trusts, improving recovery rates from physical illhealth by not only recognising overt clinical psychological syndromes that can have adverse outcomes but also by being moreaware and sensitive to the patients’ actual experiences.
A reduction of second and further referrals to the acute Trustsby referring to the specialist MUS/BDS service and correctly managing the clinical issues.
Essentially clinicians, both in the primary and secondary care will have the improved skill at preventing and recognizing MUS/BDS; and when it is not a matter that they themselves can deal with, there will be the availability of services that will prevent the patient with the undiagnosed physical symptom being repeatedly referred backfor further inappropriate clinical tests.
Making substantial in-roads into potential savings by the means described can only be achieved with a comprehensive training and motivational programme for all staff to deliver, thus supporting anyproposed new comprehensive service. This training is as important asthe service itself.
Health planners and commissioners may choose to be more adventurous.Given the current economic climate it is the area in which if the potential savings can be materialised there will be a genuine win-win-win. The win for the patients is improved physical and mental
71

health. The win for the staff is more job satisfaction, and finally there is a win for the finances and the wider society.
SERVICE DEVELOPMENT
Liaison Psychiatry has a remit beyond MUS/BDS bio-psychopathology. Furthermore alone, it would not address the whole of this unmet needthat exists. But there is sufficient overlap that services of liaison psychiatry and MUS/BDS may be considered together.
The financing of the service will need to be creative. Any anticipated savings will only manifest 12-24 months after the initial service investment. These would then help finance the next step and so on. There will need to be not only piloting of the service but also monitoring of the parallel physical health services. There is a risk that a new service will tap into previously unmet need. While this is of merit in itself and there may be societal savings, the potential savings of healthcare costs will be reduced. Monitoring social care costs will be necessary. Measuring the societal savings will be harder but also essential.
In determining the approach for service development there are several matters to consider. They are:
Who will be the service provider? Will it be primarily a trust providing acute services, mental health services or one newly developed to fulfil this role?
Piloting the service: How will this be done? The top end service needs to be sufficiently large for it to be truly acting as an MDT.
Where is the correct balance between having a well-defined long-term end point vision and working incrementally towards it; and basing each developmental step on the experience of theprevious, improving and modifying as progress is being made.
Funding strategy: How will the initial outlay be funded? Will it have to come from existing service or to be pump primed?
Estate: simply put where will the service have its clinical andadministrative bases?
Recruitment: Are there sufficient numbers of trained staff withthe skills to be employed into a specialist MUS/BDS service?
72
The development of the service has to be comprehensive. A global strategy needs to be thought through and must be in place to take into account the various levels of complexity, the structures that will provide the service, the training that will be necessary to support the processes that will create the efficiencies and the monitoring of the financial and service outcomes.
MANAGING THE PROCESS
Each area will need to consider how it best brings the service to fruition. It is probably for the local CCG to be at the front and co-ordinate and drive the necessary changes. While this may be seen as being a mental health initiative, if only because ultimately it will largely be the appropriately trained mental health practitioners to deliver the benefits, the financial savings will come from the physical healthcare budgets.
For the CCGs to be setting up a steering group may be the best avenue to make the changes. Set up a task and finish consultation group to plan and promote the next stages. The steering group is to consist of:
Influential people including GP, psychiatric and medical input. allied professions, e.g. psychologists, OTs, physiotherapists,
etc. Senior Healthcare planners and administrators, including
finance directors who can make things happen. Senior representatives of the CCG, physical healthcare
providers and mental healthcare providers. Representatives of units that may be incorporated into the
larger service. This may include single condition functional disorder clinics, pain clinics, etc.
Researcher
As appropriate the steering group may arrange for wider consultation, the obtaining of local data or site visits to comparable units to learn off their experience. The steering group, through the relevant finance directors and the researcher will undertake the necessary cost-benefit analyses. Assessments are to bemade for:
Training costs.
73

The potential savings to be made through less demand on physical health care services.
A guestimate when the return of savings will be made on investment.
Estimates for the societal savings.
It will be the steering group that will put together the detailed outline service specification as a proposal for discussion and consider how the notion is to be ‘sold’ to the relevant interested parties. Depending on the service model to be delivered it may be the steering group to arrange any bids for tender.
And finally it will be the steering group that will monitor the rollout. This will include not only the top end service but the necessary programme of psycho-education to GPs, hospital specialistsand relevant others. The roll out is likely to be phased starting with a pilot and ensuring that the expansion is built on the observed experience.
Ultimately the success of the project will be determined by ensuringthat at all levels the best possible people are involved
74

REFERENCES
Alladin, A. (2009) Evidence-based cognitive hypnotherapy for depression, Contemporary Hypnosis, 26, pp. 245–262.
Bermingham, S.L., Cohen, A., Hague J. & Parsonage M. (2010) The costof somatisation among the working-age population in England for the year 2008–2009, Mental Health in Family Medicine, 7, pp. 71–84.
Bridges, K.W. & Goldberg, D.P. (1985) Somatic Presentations of DSM-III Psychiatric Disorders in Primary Care, Journal of Psychosomatic Research, 29 pp. 563-9.
Bridges, K.W. & Goldberg, D.P. (Unknown) Somatic presentation of depressive illness in primary care, [Online]. Available at: europepmc.org/articles/pmc2573691/pdf/rcgpoccpaper00076-0016.pdf (Accessed: 26 April 2015).
Burton, C. (2003) Beyond somatisation: a review of the understandingand treatment of medically unexplained physical symptoms (MUPS), British Journal of General Practice, 53, pp. 233-241.
Burton, C. (2013) ABC of Medically Unexplained Symptoms, Chichester,BMJ Books, Wiley-Blackwell.
Burton, C., Weller, D., Marsden, W., Worth, A. & Sharpe M. (2012) A primary care symptoms clinic for patients with medically unexplainedsymptoms: Pilot Randomised Trial, [Online]. Available at: http://bmjopen.bmj.com/content/2/1/e000513.full (Accessed: 26 April 2015).
Camilleri (2005), Etiology and pathophysiology of Irritable Bowel Syndrome and chronic constipation, Advanced studies in Medicine, 5(10B), pp. S955-S964.
Capek, M.E.Y. (2012) ‘Medically Unexplained Symptoms’, in Brann, L. Owens, J. & Williamson, A. (eds.) The Handbook of Contemporary Clinical Hypnosis, Chichester: Wiley, pp. 229-245.
Chiles, J., Lambert, M. & Hatch, A. (1999) The impact of psychological interventions on medical cost offset: a meta-analytic review. Clinical Psychology: Science and Practice, 3 (2), 204-220.
Commissioning Support for London (2010) Medically Unexplained Symptoms (MUS), A Whole Systems Approach, Version 1.5.
Commissioning Support for London (2012) Medically Unexplained Symptoms (MUS), Project Implementation Report.
75

Creed, F., Barsky, A. & Leiknes, K.A. (2011a) ‘Epidemiology: Prevalence, causes and consequences’ in Creed F., Henningsen P., & Fink P. (eds.) Medically Unexplained Symptoms, Somatisation and Bodily Distress: developing better clinical services, Cambridge, Cambridge University Press, pp.1-42.
Creed, F., Kroenke, K., Henningsen, P., Gudi, A. & White P. (2011b) ‘Evidence-based treatment’ in Creed F., Henningsen P., & Fink P. (eds.) Medically Unexplained Symptoms, Somatisation and Bodily Distress: developing better clinical services, Cambridge, Cambridge University Press, pp. 69-96.
Creed, F., van der Felitz-Cornelis, C., Guthrie E., Henningsen, P., Reif, W., Schroder, A. & White P. (2011c) ‘Identification, assessment and treatment of individual patients’ in Creed F., Henningsen P., & Fink P. (eds.) Medically Unexplained Symptoms, Somatisation and Bodily Distress: developing better clinical services, Cambridge, Cambridge University Press, pp. 175-216.
Creed, F., Fernandes, L., Guthrie, E., Palmer, S., Ratcliffe, J., Read, N., Rigby, C., Thompson, D. & Tomenson B. North of England IBSResearch Group. (2003). The cost-effectiveness of psychotherapy and paroxetine for severe irritable bowel syndrome. Gastroenterology, 124(2):303-17.
Creed, F., Henningsen, P., & Byng, R. (2011d) ‘Achieving optimal treatment organization in different countries: suggestions for service development applicable across different healthcare systems’ in Creed F., Henningsen P., & Fink P. (eds.) Medically Unexplained Symptoms, Somatisation and Bodily Distress: developing better clinical services, Cambridge, Cambridge University Press, pp. 236-252.
Ewin, D. & Eimer, B. (2006) Ideomotor signals for rapid hypnoanalysis: a how-to manual, Springfield Illinois, Charles C. Thomas Publishers.
‘Fingertips’ (2015) http://fingertips.phe.org.uk/profile-group/mental-health/profile/ neurology/data#gid/1938132725/pat/46/ati/19/page/0/par/E39000003/are/E38000158 (Accessed: 26 April 2015)
Fink P., Burton C., De Bie J., Sollner W. & Fritzche K. P. (2011a) ‘Current state of management and organization of care’ in Creed F., Henningsen P., & Fink P. (eds.) Medically Unexplained Symptoms, Somatisation and Bodily Distress: developing better clinical services, Cambridge, Cambridge University Press, pp. 97-123.
Fink P., Sollner W., Fritzche, K. P. & Larisch, A. (2011b) ‘Training’ in Creed F., Henningsen P., & Fink P. (eds.) Medically
76
Unexplained Symptoms, Somatisation and Bodily Distress: developing better clinical services, Cambridge, Cambridge University Press, pp. 217-235.
Fink, P. & Rosendal, M. (2008) Unmet Need for Care for the Somatising and Mentally Ill Patients in Primary Care. 55th Annual Meeting of the Academy of Psychosomatic Medicine, poster and oral presentation Abstracts; 2008:44. [Online]. Available at www.apm.org/ann-mtg/2008/APM-proceedings-2008.pdf. (Accessed: 16 April 2015)
*Flammer, E. & Alladin A., (2007) The efficacy of hypnotherapy in the treatment of psychosomatic disorders: meta-analytical evidence, International Journal of Clinical and Experimental Hypnosis, 55(3), pp. 251-274.
Guthrie, E., Moorey, J., Margison, F., Barker, H., Palmer, S., McGrath, G., Tomenson, B. & Creed, F. (1999). Cost-effectiveness of Brief Psychodynamic-Interpersonal Therapy in High Utilizers of Psychiatric Services. Archives of General Psychiatry, 56; 519-526.
Henningsen, P., Fink, P., Haustner-Wiehle, C. & Reif, W. (2011a) ‘Terminology, classification and concepts’ in Creed F., Henningsen P., & Fink P. (eds.) Medically Unexplained Symptoms, Somatisation and Bodily Distress: developing better clinical services, Cambridge, Cambridge University Press, pp. 43-68.
Henningsen, P., Fazekas, C. & Sharpe, M. (2011b) ‘Barriers to improving treatment’ in Creed F., Henningsen P., & Fink P. (eds.) Medically Unexplained Symptoms, Somatisation and Bodily Distress: developing better clinical services, Cambridge, Cambridge University Press, pp. 124-131.
IAPT (October 2008) Medically Unexplained symptoms positive practiceguide.
IAPT (March 2011) National Curriculum for High Intensity Cognitive Behavioural Therapy Courses (Second Edition, Updated And Revised)
IAPT (July 2014) Medically unexplained symptoms positive: practice guide.
Leventhal H., Diefenbach M., Leventhal E.A. (1992), Illness cognition: Using common sense to understand treatment adherence and affect cognition interactions, Cognitive Therapy and Research 16, pp. 143–163.
Lieb, R., Zimmermann P., Friis, R.H., Höfler, M., Tholen, S., Wittchen, H. (2002) The natural course of DSM-IV somatoform disorders and syndromes among adolescents and young adults: a
77

prospective-longitudinal community study, European Psychiatry, 17, pp. 321–31
Mayou, R. & Farmer, A. (2002) Functional somatic symptoms and syndromes, British Medical Journal, 325, pp. 265-268.
Macfarlane, G.J., McBeth, J., & Silman, A.J. (2001) Widespread body pain and mortality: prospective population based study; British Medical Journal, 323, pp. 1–5
Miller, V. & Whorwell, P.J. (2009) Hypnotherapy for functional gastrointestinal disorders: A review, International Journal of Clinical and Experimental Hypnosis 57(3) pp. 279-292
Miller V., Jones H, & and P. J. Whorwell, P.J. (2007). Hypnotherapy for non-cardiac chest pain: long-term follow-up, Gut, 56, p. 1643.
Morriss, R., Dowrick, C., Salmon, P., Peters, S., Dunn, G., Rogers, A., Lewis, B., Charles-Jones, H., Hogg, J., Clifford, R., Rigby, C. & Gask L. (2007) Cluster randomised controlled trial of training practices in reattribution for medically unexplained symptoms. British Journal of Psychiatry, 191, pp. 536-42.
Nielssen, O., Elliott, G. & Large, M., (2010), The Reliability of Evidence About Psychiatric Diagnosis After Serious Crime: Part I. Agreement Between Experts, Journal of American Academy of PsychiatryLaw 38:516–23.
Nimnuan, C., Hotopf, M. & Wessley, S. (2001) Medically unexplained symptoms: an epidemiological study in seven specialties, Journal of Psychosomatic Research, 51, pp. 361-7
‘Neurosymptoms’, Anonymous (2015), Functional and Dissociative Neurological Symptoms: a Patient’s Guide (2015), http://www.neurosymptoms.org/, (Accessed online 5th September 2015)
Parsonage, M. Hard, E. Rock, B. (2014) Managing patients with complex needs. Evaluation of the City and Hackney Primary Care Psychotherapy Consultation Service. Centre for Mental Health.
Parsonage, M., Fossey, M. & Tutty, C., (2012) Liaison psychiatry in the modern NHS, Centre for Mental Health.
Poulton, C. (2015), “What is Transpersonal Counseling?” http://www.growingawareness.com.au/what-is-transpersonal-counselling, (Accessed 12th July 2015)
78
Salmon, P., Wissow, L., Carrol, J., Ring, A., Humphris G.M., Davies,J.C. & Dowrick F. (2007) Doctor’s responses to patients with medically unexplained symptoms who seek emotional support: criticismor confrontation?, General Hospital Psychiatry, 294, pp. 454-60.
Sansone, R.A., Nighat, A.T., Buckner, V.R., and Wiederman, M.W. (2008) The Relationship Between Borderline Personality Symptomatology and Somatic Preoccupation Among Internal Medicine Outpatients, Primary Care Companion Journal of Clinical Psychiatry, 10(4), pp. 286–290.
Semple, D. & Smyth, R. (Eds) (2013), Oxford Handbook of Psychiatry (3 ed.), Chapter 2 Psychiatric Assessment, Oxford University Press, Oxford. (Accessed online 12 th July 2015)
Williamson, A., (2008) Brief Psychological Interventions in Practice, Chichester, West Sussex, John Wiley & Sons Ltd.
79

VERSION HISTORY
This document has developed over time. It is likely to go through further incarnations. For this reason each document has been given aversion number, (Vx.y.z.). The version increment will reflect the level of change made. A version history is included. This document is v4.1.0
Version Submission Date
V4.2 To the Strategic Clinical Network Liaison Psychiatry Group
2nd April 2016
v4.1 23rd March 2016
v4 Submitted to Researchgate. Generic, non-locality based.
v3.4 Minor amendments of below
v3.2 Submitted for 3 CCGs internal discussions-draft.
8th September 2015
v3.1 Submitted for 3 CCGs internal discussions-draft.
24th August 2015
v3.0 Submitted for 3 CCGs internal discussions-draft.
3rd June 2015
v2 Submission to the Mental Health 5 year Task force
17th May 2015
v1 Submission to the mental health clinical leadership course
27th April 2015
80

APPENDICES
Appendix 1: Inventory of Healthy Emotional Skills
Some points This is a list of skills that a well balanced and rounded individual
will possess Not every one will have all the skills and different individuals
will possess a different mix Emotional distress will occur when the skills are exhausted beyond
their ability available When the patient’s presentation is complex and appears to have no
obvious avenue forward, the therapist may consider which skills a patient is lacking and which are being over used.
The skills listed can act as a checklist Once the primary skills lacking have been elucidated the best
therapeutic option can be considered Which can include the therapeutic approach to develop those skills
General Skills
To integrate the many facets of self into a common whole Implies utilising the Emotional, Cognitive, Intellectual
and Behavioural aspects of the mind in such a manner that they are all complementary to each other and working to thecommon good of self and others
Includes being able to resolve internal conflict and contradiction
To manage the stresses we face so as to allow emotional development without exceeding what cannot be satisfactorily handledTo be able to look after the physical health of the personTo utilise resources from within and avoid over-dependence on others.To develop and maintain positive self-esteem, self worth and self loveTo understand self, including knowing one’s own natural talents and limitsTo be able recognise the difference between reality and fantasyTo be able to dissipate all unnecessary suppressed emotionsTo be able to enhance psychological and physiological well-beingthrough techniques such as mindfulness, relaxation, meditation and self-hypnosis.To develop and utilise positive role models and positive imprinted mental imagesTo be able to forgive self and others when requiredTo develop and utilise a moral framework
81

To develop and utilise a concept of what feeling good, normal and healthy are like
Sensory Awarenesses and Emotions
To feel the full range of human emotion Love Anger Anxiety/Worry/Fear Guilt Sadness/Loss Hurt/Offence Disgust
To accurately assess the intensity of the skills.To feel more than 1 of these emotions simultaneously.To sense/perceive from within what one feels about oneselfTo perceive the non-verbal/sub-liminal cues and signalling from someone elseTo empathise with another, that is, literally to feel that person’s emotion as though “in that person’s shoes”To suppress emotions until such time they can be managed by othermeansTo have the mental flexibility to use each of the sensory skills as required
Behavioural responses
To have multiple means of expressing emotionTo have multiple skills of using emotions to affect changeTo be able to effectively communicate, verbally and non-verballyTo have the ability to be assertiveWhen feeling multiple emotions that responses are appropriate.To process lossesTo derive emotional benefit through cryingTo act contrary to feelings and inclinations when the situation demands
Includes the ability to say, "No" to others Includes the ability to control impulses and delay
gratificationTo have the flexibility of mind to use and move between each of the behavioural skills as required
Cognitions and Attitudes
To be able to use thought and logic to challenge feelingsTo develop and maintain an accurate sense of reality about the
82
present Includes being able to recognise when the emotional system
is creating a distortion of reality.To develop and maintain optimism about the future-i.e. to have hopeTo take responsibility for one’s own actions, including those emanating from the sub-conscious
Includes understanding that we alone have such responsibility and therefore ultimately no one can make us do what we don’t want
Includes learning from one's own mistakesTo develop and maintain the knowledge and understanding regarding positive mental health promotion
Includes appreciating general emotional processes and how this may apply to oneself
Includes appreciating the consequences of one’s own actionson self and others
Includes appreciating that the more we understand about others, the less angry we will be.
Includes appreciating that good people, including self and others, can act inappropriately due to errors of judgement arising from imbalances in the emotional system
To develop and maintain healthy attributions Includes giving feelings/emotions the correct explanation
for their existence Implies that the good things that happen are our successes Implies that when bad things happen to know the difference
between that which we can do to prevent in the future and that which is beyond our influence
To have ambitious but attainable goals and to know what is required to achieve theseTo give priority to what we perceive with our own senses over what others tell us.To give priority to looking after our own needs but not at the expense of undermining the well-being or needs of the next personTo develop the attitude of respecting the needs of others but not by undermining our own needs.
83
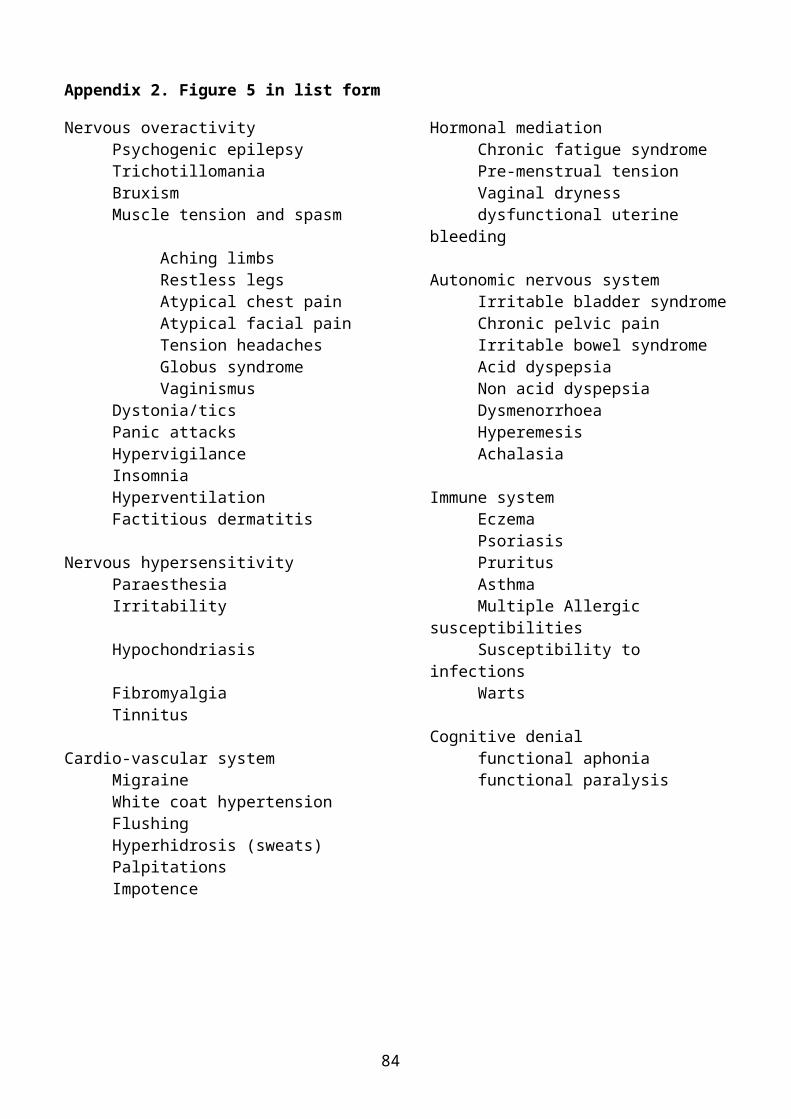
Appendix 2. Figure 5 in list form
Nervous overactivity Hormonal mediationPsychogenic epilepsy Chronic fatigue syndromeTrichotillomania Pre-menstrual tensionBruxism Vaginal drynessMuscle tension and spasm dysfunctional uterine
bleedingAching limbsRestless legs Autonomic nervous systemAtypical chest pain Irritable bladder syndromeAtypical facial pain Chronic pelvic painTension headaches Irritable bowel syndromeGlobus syndrome Acid dyspepsiaVaginismus Non acid dyspepsia
Dystonia/tics DysmenorrhoeaPanic attacks HyperemesisHypervigilance AchalasiaInsomniaHyperventilation Immune systemFactitious dermatitis Eczema
PsoriasisNervous hypersensitivity Pruritus
Paraesthesia AsthmaIrritability Multiple Allergic
susceptibilitiesHypochondriasis Susceptibility to
infectionsFibromyalgia WartsTinnitus
Cognitive denialCardio-vascular system functional aphonia
Migraine functional paralysisWhite coat hypertensionFlushingHyperhidrosis (sweats)PalpitationsImpotence
84

Appendix 3: The Definition of Bodily Distress Syndrome
≥3 cardiopulmonary/autonomic arousal symptomso palpitations/heart poundingo Precordial discomforto Breathlessness without exertiono Hyperventilationo Hot or cold sweatso Trembling or shakingo Dry moutho Churning in stomach/butterflieso Flushing or blushing
≥3 gastrointestinal arousal symptomso abdominal painso frequent loose bowel movementso feeling bloated/full of gas/distended regurgitationso constipationo diarrhoeao nauseao vomitingo burning sensation in chest or epigastrium
≥3 musculoskeletal tension symptomso pains in arms or legso muscular aches or painso pains in the jointso feelings of paresis or localised weaknesso back acheo pain moving from one place to anothero unpleasant numbness or tingling sensations
≥3 general symptomso concentration difficultieso impairment of memoryo excessive fatigueo headacheo dizziness
≥4 symptoms from one of the above groups. 1-3 of the above categories fulfilled for moderate or single
organ system BDS 4-5 of the above categories fulfilled for severe or multi-organ
system BDS
85

Appendix 4: A poster displayed at the RCGP Conference 2013 presenting the use of hypnotherapy in a general practice setting.
86

87
Related Documents











