Ethics and Policies Regarding “Medically Inappropriate Care” Felicia Cohn, PhD Bioethics Director Kaiser Permanete Orange County Clinical Professor University of California Irvine

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
EthicsandPoliciesRegarding“MedicallyInappropriateCare”
FeliciaCohn,PhDBioethicsDirector
KaiserPermanete OrangeCountyClinicalProfessor
UniversityofCaliforniaIrvine
Overview• Reviewthemeaningof“medicallyinappropriatecare”
• Assessaprocessforaddressingmedicallyinappropriatecare
• Considerpolicyneedsandimplicationsofmedicallyinappropriatecare.

“NaturalDeath”
“MedicallyInappropriateCare”Not medically indicated
Ineffective
Non-beneficial
Hopeless
Futile

SchneidermanLJ, JeckerNS, JonsenAR. Medicalfutility:itsmeaningandethicalimplications. AnnInternMed. 1990Jun15;112(12):949-54.• …weproposethatwhenphysiciansconclude(eitherthroughpersonalexperience,experiencessharedwithcolleagues,orconsiderationofpublishedempiricdata)thatinthelast100casesamedicaltreatmenthasbeenuseless
• Ifatreatmentmerelypreservespermanentunconsciousness orcannotenddependenceonintensivemedicalcare,thetreatmentshouldbeconsideredfutile.
• …treatprobabilityandutilityasindependentthresholds.…physiciansmustdistinguishbetweenaneffect,whichislimitedtosomepartofthepatient'sbody,andabenefit,whichappreciablyimprovesthepersonasawhole.Treatmentthatfailstoprovidethelatter,whetherornotitachievestheformer, is"futile".
• …physicianscanjudgeatreatmenttobefutileandareentitledtowithholdaprocedureonthisbasis.Inthesecases,physiciansshouldactinconcertwithotherhealthcareprofessionals,butneednotobtainconsentfrompatientsorfamilymembers.

TheElusive“F”Word
•QuantitativeFutility• Likelihoodthatinterventionwillbenefitpt isexceedinglypoor(reasonableprobabilityofsuccess).
•QualitativeFutility• Qualityofthebenefitaninterventionwillproduceisexceedinglypoor,i.e.resultwillbepoorqualityoflife.

TheFutilityofFutility

O!besomeothername:What’sinaname?thatwhichwecallaroseByanyothernamewouldsmellassweet;
ShakespeareRomeoandJuliet

Othernames…• CaliforniaMedicalAssociation:“Non-BeneficialTreatment”• “NBTgenerallynotindicatedforirreversiblemedicalconditionswhereimminentdeathisexpected.”
• “CMAModelPolicy:RespondingtoRequestsforNon-BeneficialTreatment.”July2011
• CriticalCareorganizations:“PotentiallyInappropriateTreatment”• Theterm“potentiallyinappropriate”shouldbeused,ratherthanfutile,todescribetreatmentsthathaveatleastsomechanceofaccomplishingtheeffectsoughtbythepatient,butcliniciansbelievethatcompetingethicalconsiderationsjustifynotprovidingthem.
• AnOfficialATS/AACN/ACCP/ESICM/SCCMPolicyStatement:RespondingtoRequestsforPotentiallyInappropriateTreatmentsinIntensiveCareUnits,June2015

Definitions/Descriptions• Anytreatmentaphysiciandeterminesintheexerciseoftheirprofessionaljudgmentwould:• Beineffective forproducingdesiredphysiologicaleffectthatthept/agentdesiresorexpects;or
• Producenoeffectsthatcanreasonablybeexpectedtobeexperiencedbypt asfurtheringtheirexpressedandmedicallyobtainablegoals;or
• Causeharmtothept significantlydisproportionatetothebenefit;
• Hasnorealisticchanceofreturningpt toalevelofhealththat permitssurvivaloutsideofacutecarehospital;or
• Wouldserveonlytomaintainpt’s lifeinapermanentlyunconsciousstate,unlessthereisevidencethatthepatientwouldvalueremainingaliveinthatstate.

CompetingEthicalObligations
Rel
atio
nshi
p &
Tr
ust
TreatmentRequestsMoralDistress• Differentinterpretationsofgoodsandharms.
• Perceivedbreakdownoffiduciaryrelationship.
• Decision-makingreducedtostrugglebetweenpatientautonomyvs.clinicianautonomy.
• Treatmentgoalsoftennotclarified.
• Subjectiveperceptionsofqualityofthislife.
• Noestablishedtransparentprocesstoresolvedisputes.
Helft PR,Siegler M,LantosJ.TheRiseandFalloftheFutilityMovement.NEJM343;2000;293-296

Fromdefinitiontoprocess

Whypolicy?InstitutionalPolicy Case-by-CaseBasis
Advantages -Clearguidelines.
-Decreasespotentialdiscrimination.
-Increasedconsistency.
-Moreflexibilityandroomforprofessionaljudgment.
-Lesscumbersomeprocess.
Disadvantages-Processmaybecumbersomeleadingtolackofutilization.
-Caseswillinevitablyfalloutsidethedefinitions.
-Inconsistencyandriskofdiscrimination.
-Lackofofficialadministrativesupport.
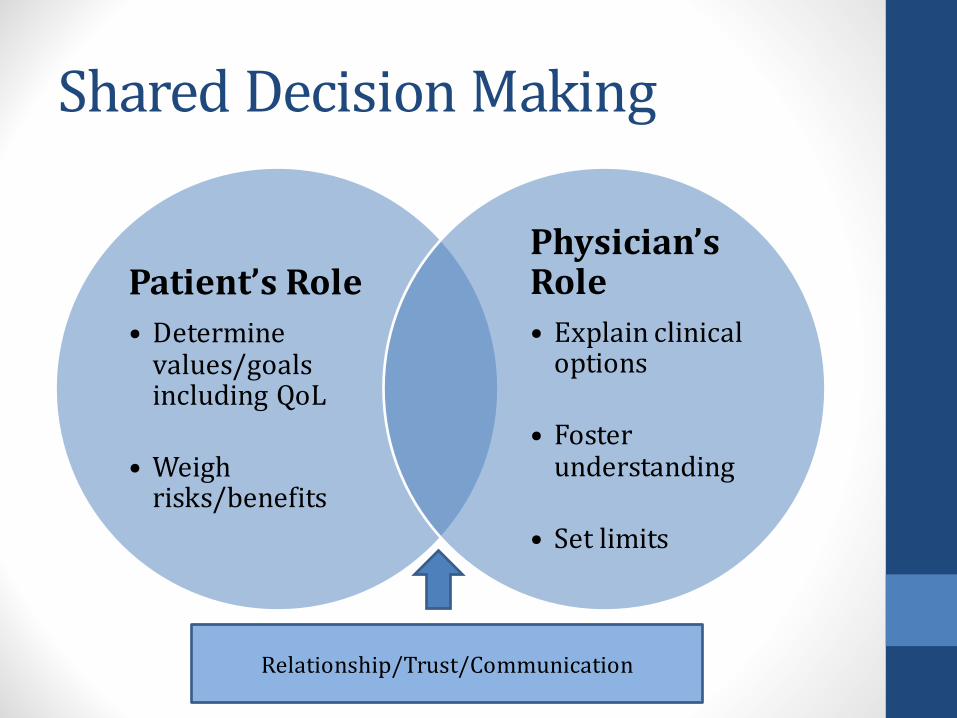
SharedDecisionMaking
Patient’sRole• Determinevalues/goalsincludingQoL
• Weighrisks/benefits
Physician’sRole• Explainclinicaloptions
• Fosterunderstanding
• Setlimits
Relationship/Trust/Communication

LegalSupportCaliforniaLaw• CaliforniaProbateCode4735:• “Ahealthcareprovider…..maydeclinetocomplywithanindividualhealthcareinstructionorhealthcaredecisionthatrequiresmedicallyineffectivehealthcare…”
• CaliforniaProbateCode4740:• “Ahealthcareprovider….acting ingoodfaithandinaccordancewithgenerallyacceptedhealthcarestandards…..isnotsubjecttocivilorcriminalliabilityforanyactionincompliancewiththisdivision,including,buttolimitedto,anyofthefollowingconduct:
• Decliningtocomplywithahealthcaredecisionofapersonbasedonabeliefthatthepersonlackedauthority.
• Decliningtocomplywithindividualhealthcare instruction…inaccordancewithSections4734to4736.”

PolicyDevelopment• BasedonCMAModelpolicyandCaliforniastatelaw• DevelopedbyRegionalBioethicsCommitteeover2yearperiod• Vettedbynumerousstakeholdergroups• Reviewedandapprovedbylegalandriskmanagement.• Reviewedandapprovedbyregionalleadership.• Reviewedandapprovedbyservicearealeadership• Annualreview
Steps• Enlistexpertconsultationfornegotiation/conflictresolution• Informpatient/surrogates• 2nd medicalopinion• Interdisciplinaryhospitalcommitteereview• Opportunitytotransferthepatienttoanalternateinstitution• Opportunitytopursueextramuralappeal• Decisionimplementation• Ongoingsupport

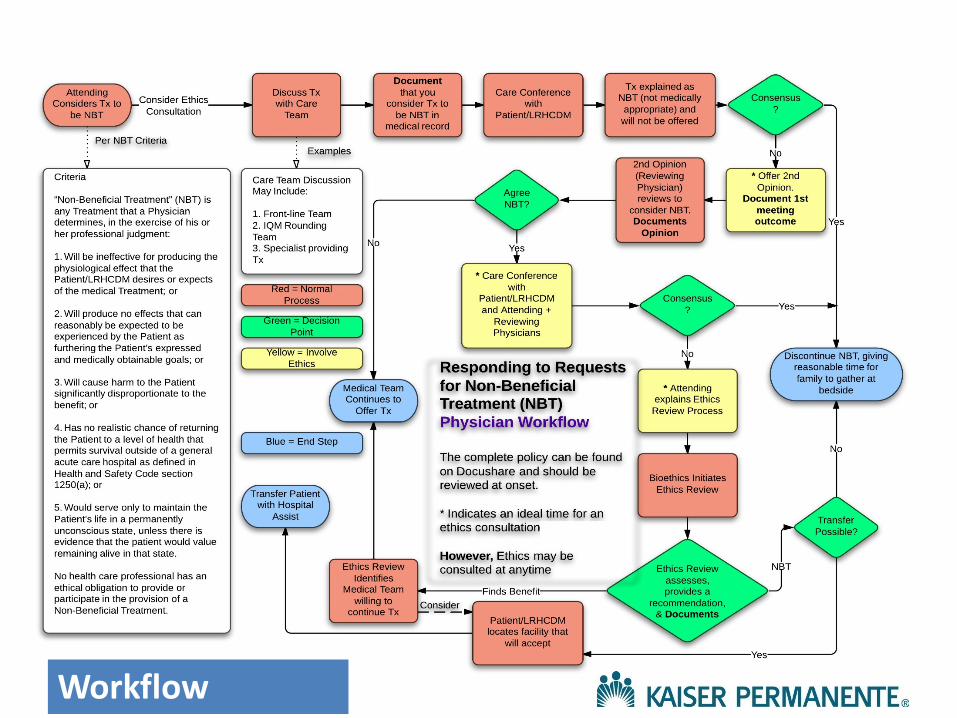
PolicyProcess• Step1:IdentifyNBT• Step2:CommunicationamongMedicalTeam• Step3:Communicationwithpatient/ decisionmakers• Step4:SecondOpinionbyReviewingPhysician• Step5:EthicsReview• SupportsInitiation/ContinuationofTreatment— transfertoanotherMD• SupportsForgoingTreatment—opportunityfortransfer,thantreatmentstops
20|©2011KaiserFoundation
HealthPlan,Inc.Forinternaluse
only.
November10,2016
Workflow

PuttingPoliciesIntoPractice

PolicyOutcomes• 1KPservicearea(SouthBay)• Retrospectiveevaluationofallbioethicsconsultations11/6/09(policyadoption)– 8/6/12.
• Case-specificdataforconflictinvolvingwithholdingorwithdrawingofnonbeneficial treatment.
• MainOutcomeMeasures:Conflictresolution• Results:• 146(39.4%)cases• 54(37.0%)ofthecases,resolutionoccurred.• 92(63.0%)NBTeventuallywithheldorwithdrawn.• 87(94.6%)wheretreatmentwaswithheldorwithdrawn,consensusreachedthroughpolicyprocess
• 5conflictsremained• CMNelson,BANazareth,Nonbeneficial TreatmentandConflictResolution:BuildingConsensus,PermJ2013Summer;17(3):23-27

5casesofpersistentconflictCasesofunilateralwithdrawal Patientpreferences
Afterethicscommitteecase
reviewTreatmentwithheld
orwithdrawn OutcomePostoutcomelitigation
1 Beneficialtreatmentperadvancedirective
Familythankful CPR,increaseddoseofvasopressors,antiarrhythmics
Comfortmeasuresinitiated;patientdiedinhospital
No
2 Unknown; familyneverdiscussedtreatmentpreferenceswithpatient
Familyaccepting CPR,stent,increaseddoseofvasopressors
Comfortmeasuresinitiated;patientdiedinhospital
No
3 Noadvancedirective;patientambivalentwithtreatmentpreferences,thenlostcapacity
Familyunaccepting CPR,dialysis,vasopressors,antiarrhythmics,tracheostomy,antibiotics
Comfortmeasuresinitiated;patientdiedinhospital
No
4 Familystatedthatpatientrequestedconservativetreatment;noadvancedirective
Familyunaccepting CPR,dialysis,feedingtube
Comfortmeasuresinitiated;patientdiedinsubacutecarefacilityposttransfer
No
5 Conservativetreatmentrequestedperadvancedirective
Familyunaccepting Nasogastrictubeandpercutaneousendoscopicgastrostomytube
Transferredtoanotherhospitalbyfamily;nofurthercontact
No

Societaldisconnect

Historically…

DoctorsDieDifferently“It’snotafrequenttopicofdiscussion,butdoctorsdie,too.Andtheydon’tdieliketherestofus.What’sunusualaboutthemisnothowmuchtreatmenttheygetcomparedtomostAmericans,buthowlittle.Forallthetimetheyspendfendingoffthedeathsofothers,theytendtobefairlyserenewhenfacedwithdeaththemselves.Theyknowexactlywhatisgoingtohappen,theyknowthechoices,andtheygenerallyhaveaccesstoanysortofmedicalcaretheycouldwant.Buttheygogently.
Ofcourse,doctorsdon’twanttodie;theywanttolive.Buttheyknowenoughaboutmodernmedicinetoknowitslimits.Andtheyknowenoughaboutdeathtoknowwhatallpeoplefearmost:dyinginpain,anddyingalone.They’vetalkedaboutthiswiththeirfamilies.Theywanttobesure,whenthetimecomes,thatnoheroicmeasureswillhappen—thattheywillneverexperience,duringtheirlastmomentsonearth,someonebreakingtheirribsinanattempttoresuscitatethemwithCPR(that’swhathappensifCPRisdoneright).”
DoctorsDieDifferently
“…victimsofalargersystemthatencouragesexcessivetreatment”
KenMurray,JournalofMedicine,August1,2013,https://www.ncnp.org/journal-of-medicine/1240-doctors-die-differently.html
CommunicationIsKey
“….partoftheir[physicians’]angstcomesnotsimplyfromthepressuretoprovideburdensometreatment,butalsofromaninabilitytofindtherightlanguageandconceptualframeworkfortalkingabouttheproblemwithpatientsandfamilies.”
SolomonMZ.Howphysicianstalkaboutfutility:makingwordsmeantoomanythings.JournalofLaw,Medicine,andEthics1993;21:231-237
BeyondCommunication…
• Family“threats”togotothemedia orattorney• Fairapplicationofpolicybasedonmedicalindications,whileremaining sensitivetoculturalandreligiousdifferences.• Institutionalsupportforapplicationinindividualcases.• Societalperspectives
Policyimplications• Physiciandutiesatthebedside• Respectforpatient/surrogateautonomy• Avoidharm(“overmasteredbydisease”)• Stewardresources
• Endsofmedicine• Recognitionoflimitsofmedicine• Limitsofautonomy
• SocietalObligations• Unsustainablecostsandmanpower• Opportunitycosts• Fairness:justdistributionofresources

CompetingEthicalObligationsandSocialContext
Rel
atio
nshi
p &
Tr
ust
PublicEngagement“Themedicalprofessionshouldleadpublicengagementeffortsandadvocateforpoliciesandlegislationaboutwhenlife-prolonging
technologiesshouldnotbeused.”
OFFICIALPOLICYSTATEMENT:AmericanThoracicSociety(ATS),approved10/15AmericanAssociationforCriticalCareNurses(AACN),12/14AmericanCollegeofChestPhysicians(ACCP),10/14EuropeanSocietyforIntensiveCareMedicine(ESICM),9/14SocietyofCriticalCareMedicine(SCCM),12/14

Individual,PhysicianorSociety?
And the winner is…



ResuscitativeServicesPolicyMedicallyInappropriateCPR
• AffirmspolicytoprovidemedicallyindicatedCPR,intheabsenceofaDNRorder.• IdentifiessituationsinwhichCPRisconsideredineffectiveandisnotmedicallyindicated:1. Terminallyillpatientwhoisimminentlydying2. Patientexperiencingirreversibleorganfailure
notexpectedtosurvivecurrenthospitalization3. Permanentlyunconsciouspatient
• DecisionthatCPRisnotmedicallyindicatedandwillnotbeofferedmustbedisclosedtopatient/agentanddocumentedinthemedicalrecord.

DNRandMIT/NBT
CPR
MIT/NBT
Related Documents











