1
ABNORMAL PSYCHOLOGY CASE STUDY
Abnormal Psychology Case Study
By Gavin
Crimina
l Jus
tice

2
Abstract
This paper will investigate possible cause (s) (causal) and contributions to schizophrenia. This paper will focus on the Genetic/Neurological contributions to schizophrenia and the latest medical treatments for schizophrenia based on these contributions. This paper will address the environmental impact/aspects of the disorder; schizophrenia. At this time, there is no cure only treatment for schizophrenia. Treatment approaches will be proffered and considered for effectiveness in treating this disorder. In our modern era Kraepelin, first described this condition and he called it dementia praecox. Much more is known comparatively speaking since Emil Kraepelin’s first comprehensive description of the condition now known as or called, Schizophrenia. Historical writings and records allude to this disorder as far back as the Pharaoh’s of Egypt era. Although there is no known cure at this time for schizophrenia, there are treatments that can assist the patient in ameliorated living. Among the newer treatments, psychotherapy and psychoeducation show promising results. Presenting patient Shonda will be assessed in this paper and a regimen of treatment extended specifically for her.
Crimina
l Jus
tice

3
Abnormal Psychology: Case Study 6
Introduction:
Schizophrenia is a disorder that can be assigned to the Axis 1 Classification according to
DSM-IV-TR. Schizophrenia is a “devastating psychotic disorder that may involve characteristic
disturbances in thinking (delusion), perception (hallucinations), speech, emotions, and behavior”
(Barlow & Durand, p. 471). The cause of schizophrenia is not known at this time…exactly, but
researchers believe that genetics and environment contribute to the development of this
disease—mental disorder. The case study selected for this paper is Abnormal Psychology
Continuous Schizophrenia: Paranoid Type. The subject, Shonda, for this case study, meets the
criteria for this diagnosis. Shonda hears voices, her speech pattern is disjointed and difficult to
follow, has delusions and hallucinations of being under surveillance by the FBI, CIA; she has
significant impairment in her ability to work. The subject has connection genetically to a relative
that was placed in a mental health care facility. Shonda was raised without emotional attachment
by both parents. Shonda has a brother but has little contact with her sibling. Shonda is currently
taking antipsychotic medication, haloperidol (Haldol).
This paper will address the following. The Genetic/Neurological contributions to
schizophrenia and medical treatments, the environmental impact/aspects cause (s) (causal)
contributions of/to the disorder; schizophrenia, diet contributions, and treatment approaches such
as medical, psychosocial, and others. “Despite much research, environmental influences that
can be said to cause a schizophrenic illness remain elusive” (Leask, pg.323). Psychosocial
treatments for Shonda’s schizophrenia will be examined, and a specific regimen will be proposed
for the patient/subject, Shonda.
Crimina
l Jus
tice

4
I. Introduction of the Disorder
Description & Historical Background
Much is known comparatively speaking since Emil Kraepelin circa 1856-1926 CE. Peter
Williamson, Mind, Brain, and Schizophrenia introduces Kraepelin with these facts and
observations:
“The first comprehensive description of the condition was provided by Emil
Kraepelin, who described a condition he called dementia praecox, around the end of the
nineteenth century (circa 1887). These patients were differentiated from those with
manic-depressive insanity and paranoia by virtue of the fact that most of them never
recovered. His description of these patients (Kraepelin, 1919) is remarkable, even when
viewed after a century has passed.
Kraepelin observed that "patients perceive in general what goes on around them
often much better than one would expect from their behavior" but they "do not take any
notice of what they may perceive quite well, nor do they try to understand it; they do not
follow what happens in their surroundings even though it may happen to be of great
importance for them." Patients were found to be emotionally dull with a loss of interest
and singular indifference toward others. They had "no real joy in life," "no human
feelings"; to them "nothing matters," "everything is the same," and they feel "no grief and
no joy" (Williamson, p. 4).
However, symptoms of this disorder were recorded in ancient times. And the actual word
schizophrenia is only less than a hundred years old. Eugen Bleuler, Kraepelin’s contemporary,
introduced the word schizophrenia in 1908. Schizophrenia is derived from the Greek words for
split (skhizein) and mind (phren) meaning split-mind (Barlow & Durand, p. 472). The disease
Crimina
l Jus
tice

5
itself was known in Ancient times. In his paper Notes on the History of Schizophrenia
Theocharis Chr. Kyziridis posits that the disorder now known as schizophrenia was known in the
ancient past with/by comparative symptoms. These symptoms can be compared to the modern
diagnosis starting with Kraepelin’s dementia praecox condition description. The disorder can be
traced back to written documents in Pharaonic Egypt and also to the second millennium before
Common Era (BCE). Details appeared in the Book of Hearts which was part of the Eber
papyrus. The Hindus description dates back to 1400 BCE. The Chinese text called The Yellow
Emperor’s Classic, describes similar symptoms and was written 1000 BCE. Comparative
symptoms were known in ancient times according to manuscripts written and transitioned
through time.
“One of the problems with investigating disorders such as schizophrenia is that the
tools available in the past to evaluate subtle, small changes in the brain have been rather
crude. Thus most of the work done in the past century to investigate brain structural
abnormalities in schizophrenia was based on methods that were crude, prone to error, and it
therefore did not further our knowledge and understanding of brain abnormalities in
schizophrenia… Through the knowledge of history can we understand the roots of
schizophrenia and its historical evolution. Both of them are extremely helpful for the
understanding of the disease itself” (Id p. 46-47).
Disorder Classification
Schizophrenia is a disorder that can be assigned to the Axis 1 Cluster A (Odd or
Eccentric) Classification according to DSM-IV-TR. The assigned DSM-IV-TR code is 295.30.
“DSM categorizes personality disorders into three clusters, A, B, and C. Cluster A is
Crimina
l Jus
tice

6
characterized by odd or eccentric behavior and includes paranoid, schizoid, and schizotypal
personalities. This cluster tends to be the most treatment refractory and is probably the most
likely to have underlying biogenetic factors” (Magnavita, p. 7). In Durand and Barlow’s
Essentials of Abnormal Psychology they list Schizophrenia into four sub categories as follows.
(p. 479-80)
1. Paranoid Type
2. Disorganized Type
3. Catatonic Type
4. Residual Type
The schizophrenia disorder criterion is listed with these features: (Id p. 475)
• Delusions
• Hallucinations
• Disorganized speech
• Grossly disorganized or catatonic behavior
• Negative symptoms such as affective flattening alogia
• Social and occupational dysfunction
• Neglected self-care
• Persistence for at least 6 months
Paranoid schizophrenia presents with prominence of delusions, vivid auditory
hallucinations, and delusions of persecution, this is accompanied by delusions of being watched
or being followed by the FBI, CIA and or; always seeing the same person on the street (Kring,
Davison, Neale, & Johnson, p. 358).
Crimina
l Jus
tice

7
Studies on Schizophrenia Disorder
Studies on schizophrenia disorders include family, twin, adoption, and molecular which
includes Shotguns and Lasers. Family studies are/were used to indicate the risk of schizophrenia
within the family. Abnormal Psychology 10 Edition Ann M. Kring, Gerald C. Davison, John M.
Neale, Sheri L. Johnson posits (p. 360) that the results of family studies support the notion that a
predisposition for schizophrenia can be transmitted genetically. In Schizophrenia Revealed
Michael Foster Green says (p. 53) that schizophrenia does indeed run in families however, not
with a certainty for any one person but with a rate higher than would be expected. Family
studies show 8 percent of siblings and 5 percent of parents of a schizophrenic individual will
have schizophrenia compared to about 1 percent of the general populace.
Twin studies bring forth the comparisons between two types of twins, identical,
monozygotic (MZ) and fraternal, dizygotic (DZ). The percentages are higher for MZ twins
because they share 100 percent of their genes (Green, p. 55) whereas DZ share 50 percent of
their genes, the same as any sibling. Kring et al chart them (pg. 360) at risk for schizophrenia
from people with the disorder at 12.08 percent for DZ twins and 44.3 percent for MZ twins.
Green however, says “There are many twin studies in schizophrenia: the concordance rates vary
somewhat, but the rates for MZ twins are always higher than for DZ twins (p. 55). Green further
states that the percentages are 48 percent for MZ twins and 17 percent for DZ twins according to
a study by Irving Grottesman (1991). The nearly three-fold increase between the two can only
be explained genetically.
Adoption studies according to Green (p. 58) are probably the best way to separate and
examine genetic and environmental factors. The study of children, whose mother had
schizophrenia but were raised from infancy by adoptive parents without schizophrenia, provides
Crimina
l Jus
tice

8
clearer confirmations of genetics role in schizophrenia (Kring et al, p. 361). Studies were done
in Nordic countries such as Finland, Denmark, Sweden and Norway that keeps/kept superb
national records for adoption and psychiatric hospitalizations, and this system of record keeping
made is easy to locate individuals with mental illnesses for research purposes. Green says;
“studies have shown that adoptees born to mothers with schizophrenia have higher rates of
schizophrenia themselves, even though they are not raised with their biological mothers” (p. 58).
“The risk for other disorders, such as schizoaffective, schozophreniform, and schizotypal
personality disorder, was also greater among the adoptees with a biological parent with
schizophrenia than among the control adoptees” (Kring et al, 361). Therefore based on adoption
research, the genetic linkage can be determined and or established.
Molecular studies are focused on what constitutes the genetic predisposition, as it appears
that the predisposition for schizophrenia is not transmitted by a single gene (Kring et al,). Green
says that it is technically incorrect to look for a “gene” because a schizophrenia-relevant gene
has many alleles (p. 60) (in genetics, either of a pair (or series) of alternative forms of a gene that
can occupy the same locus on a particular chromosome and that control the same character)
(WordWeb Pro, V5.52) researchers are looking for a particular version of a gene (an allele) that
contributes to risk for the disorder.
Linkage studies such as the “shotgun” approach look at the entire genome to look for links
between a certain region of a chromosome and the disorder. This type of research looks for a
“marker” that indicate a specific location on a chromosome.
“These studies collect DNA from a family that has several members with
schizophrenia, as well as many members who are not ill. Scientists compare the marker
alleles in the affected members to the unaffected members. Demonstrating that the affected
Crimina
l Jus
tice

9
members have the same marker allele and the non-ill members no not, shows genetic
linkage for the disease” (Green, p. 61).
In contrast, association studies (Laser) have a narrow laser like focus. These types of
studies begin with a certain gene in mind, one that is relevant to the disorder. And the focus is
associated to the disorder by looking at what scientists posit could be attributed to some kind of
abnormality in a substance found possibly secreting from the schizophrenic individual.
However, Green posits (p. 63) that “if we target a single substance that is important for
schizophrenia, we will not be looking for a single gene. For years the substances of greatest
interest for schizophrenia have been neurotransmitters, the chemical messengers in the brain.”
However, this research may not yield the desired results. Other neurotransmitter systems are
being actively investigated such as serotonin, GABA, acetylcholine, and glutamate.
Case Comparison
The original case (Case Study 6: Shonda: Continuous Schizophrenia: Paranoid Type)
diagnosis aligns with the DSM-IV-TR criteria for paranoid schizophrenia. Shonda has a long
history of mental illness and was somewhat functional as an employee of a local community
mental health center doing light cleaning and other chores. Shonda does not show up for work,
her caseworker becomes worried, and goes to Shonda’s home to pay her a visit. The caseworker
discovers that Shonda is exhibiting serious complications from her disorder. Shonda’s condition
has worsened and the caseworker is concerned and determines that Shonda might need a
medication adjustment and arranges for her to be checked into the clinic for assessment. Shonda
will undergo assessment on her condition and medications to see if any changes are necessary.
This case study ties in with the background of the disorder, however, what has been learned
Crimina
l Jus
tice

10
through this case study can and does supersede standard conventional treatments based on earlier
studies and diagnosis of schizophrenia. Scientific studies have increased the understanding of
schizophrenia and newer treatments are proffered and should be seriously considered.
Shonda’s current intervention regimen is probably an atypical schizophrenic treatment
regimen perhaps even archaic by today’s improved treatment programs found in progressive
mental disorder health care facilities. Shonda is being treated according to the case study with
intervention by medicine/medication only as it appears. Her drug of selection by the attending
Doctors is haloperidol (Haldol). Shonda has been taking the medication for years, and she has
taken other antipsychotic medicines previously. The problem with this regimen is that Shonda is
not showing any improvement and her treatment resides in either a change in medication (s) or
an increase/decrease in medication dosage. Although functional, (limited) Shonda is not
receiving other treatments that could or would assist her in improving her mental state and
functionality. Shonda should be included into the following treatment regimens.
Aside from drugs, there are several treatments that show progress and promise. Among
these treatments is a therapy known as psychosocial treatment. Mayo Clinic; Psychosocial
treatments; has the following recommendations. This treatment can be utilized once the
psychosis recedes. After psychosis recession a program like this can be integrated into Shonda’s
daily regimen. Psychosocial treatments focus on social training skills, family therapy, vocational
rehabilitation and obtaining gainful employment. Because Shonda has been already working
and has her own home, she would be a good candidate for psychosocial therapy.
Once Shonda’s delusions and auditory hallucinations are reduced, implementation of
psychoeducation and normalization treatments could be established. Shonda, using
psychoeducation and normalization techniques, will learn how to divert attention away from
Crimina
l Jus
tice

11
hearing the voices. Shonda will be encouraged to watch TV, listen to music, make
conversations, read, and perhaps play a video game. With the correct medical and therapeutic
regimen, Shonda’s mental and physical state would improve.
II. Biological Aspects of this Disorder
Genetic/Neurological Contributions to Schizophrenia:
Roles of Neurotransmitters
What neurotransmitter(s) have been linked to this disorder and how do they influence
behavior? See Appendix A for pictorial example of neurotransmitters.
Doctors in the fields of Psychology and Psychiatry have long said that the etiology of
schizophrenia was not completely known. According to an article by Sherrie Thomas, The
Etiology of Schizophrenia the dysfunction of several neurotransmitter systems such as,
dopamine, serotonin (5-hydroxytryptamine, 5-HT), and glutamate are thought to play a part in
schizophrenia. While Durand and Barlow state that one of the major theories, although
controversial, involves dopamine as the cause of schizophrenia (p.488). Williamson lists some
of the neurotransmitters involved in schizophrenia dopamine, glutamate, and serotonin (p. 15).
There seems to be a consensus that dopamine and serotonin play a major part in schizophrenia.
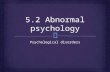
What are neurotransmitters? (See Figure 4.4) for a neurotransmitter transfer depiction.)
Neurotransmitters are “chemicals that cross the synaptic cleft between nerve cells to
transmit impulses from one neuron to the next. Their relative excess or deficiency is involved in
several psychological disorders” (Barlow & Durand, p. 45).
“Neurotransmitters exist in a delicate balance with one another. If the levels of
one neurotransmitter become too low, the balance can shift and other neurotransmitter
Crimina
l Jus
tice

12
levels can become too high. Neurotransmitter-related disorders occur when the current
levels of neurotransmitters are unable to properly relay the electrical signal from one
nerve cell (neuron) to the next. A neurotransmitter imbalance can result from the levels
being either too high or too low” (nhnatural, p. 1).
If for instance the dopamine levels were in excess the resultant could be one of the major factors
in schizophrenia. According to Peter Williamson in his book Mind, Brain, and Schizophrenia (p.
45) the original dopamine theory of schizophrenia was that hyperactivity of dopamine
transmission was responsible for the symptoms of schizophrenia. If there is an excess or
depletion of neurotransmitters, the imbalances could cause disorders that influence behavior
patterns.
Genetic Research and Contributions
What is known about the genetic contributions to this disorder—what does the research
suggest?
Barlow and Durand Essentials of Abnormal Psychology posit (p. 485) that there is no
other area of abnormal psychology that so clearly illustrates the intriguing mystery of genetic
influences on behavior as it does on schizophrenia. They further crystallize that they can safely
say in generalization “Genes are responsible for making some individuals vulnerable to
schizophrenia” (Id, p. 485). Peter Williamson Mind, Brain, and Schizophrenia (p. 9) says it is
known for some time that there is a strong genetic basis to schizophrenia. First-degree relatives
increase the risk 10-fold whereas identical twins increase the risk to 50-fold in comparison to the
general population. However, because of the 50% concordance in twins suggests that there are
other contributing factors such as brain development and obstetric complications. The risk of
Crimina
l Jus
tice

13
developing schizophrenia ranges from 1 percent in the general population to 50% in
Monozygotic twins according to Barlow and Duran (p. 485).
Sherine Thomas in her article The Etiology of Schizophrenia says because there is not a
100% concordance rate among monozygotic twins (MZ) and people can apparently carry the
genotype for schizophrenia without ever developing the disease, therefore there is probably no
single dominant gene for schizophrenia (p. 2). And Williamson also makes a similar assessment
wherein he says
”However, the marked heterogeneity of findings in schizophrenia indicates that
no single gene is likely to be the smoking gun…As time goes on, it is likely that a
number of genes will be weakly linked to schizophrenia. Some of these may convey
vulnerability stress. Others may result in the brain neurodevelopment anomalies…While
characterization of the genes involved in schizophrenia will no doubt be helpful, it is
likely that schizophrenia is best understood at a different level: the level of neuronal
circuits” (Williamson, p. 183).
While genes may be a contributing factor, chemical imbalances in the neurotransmitters could be
determinate. This coupled with “triggers” such as stress, could be the catalyst or main
psychological trigger that can cause episodic schizophrenia or complete DSM-IV Axis 2 criteria
for diagnosed schizophrenia.
Brain Abnormalities
Are brain abnormalities indicated in this disorder? Is so, what influence do they have on
this disorder?
Crimina
l Jus
tice

14
“It is believed that there is something different about the workings of the brain in
people with schizophrenia. It is only since the introduction of positron emission
tomography (PET scans), computer axial tomography (CT scans) and magnetic resonance
imaging (MRI), that the structure and function of the brain has been examined in detail.
A number of brain-imaging and post-mortem studies have shown that abnormal brain
morphology and physiology appear to be involved in the development of schizophrenia”
(Thomas, p.3).
This clearly indicates that brain abnormalities are existent in patients with schizophrenia.
However, to what levels can be determined with some applied testing assessment procedures.
Brain matter volume and loss can be found in the brains of schizophrenics as the following
attests:
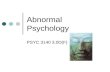
“Significant Loss of Brain Gray Matter: Individuals with schizophrenia, including those
who have never been treated, have a reduced volume of gray matter in the brain,
especially in the temporal and frontal lobes. Recently neuroscientists have detected gray
matter loss of up to 25% (in some areas). The damage started in the parietal, or outer,
regions of the brain but spread to the rest of the brain over a five year period. Patients
with the worst brain tissue loss also had the worst symptoms, which included
hallucinations, delusions, bizarre and psychotic thoughts, hearing voices, and depression”
(schizophrenia.com). (See Figure 4.1 Image Source)
There is good evidences with the added capabilities of the introduction of the positron
emission tomography (PET scans), the computer axial tomography (CT scans), plus the magnetic
resonance imaging (MRI) techniques, that brain abnormalities can now be seen via this
Crimina
l Jus
tice

15
technology. This visual aid into the size and functioning of the brain can assist in diagnosis and
treatment for mental disorders such as schizophrenia. Also, the chemical actions and reactions
can be viewed. This assists in understanding the neurotransmissions taking place in the brain.
Will this be encouraging or discouraging? Does brain imaging provide an important tool in brain
abnormality assessment? Yes, as the following describes.
“One could say that the findings from the neuropsychological studies are both
encouraging and discouraging. Discouraging because no finding differentiates all
patients from controls, and what findings there are do not seem to be specific to
schizophrenia. However, a few themes are starting to emerge from the data that are
encouraging. First, there are abnormalities in a number of brain regions-the frontal,
temporal, and basal ganglia regions being more common than others. Secondly, many of
the abnormalities found are related to known functions of these areas-executive function,
verbal fluency, memory, and encoding, among others. Finally, none of these regions
could account for these abnormalities in isolation. They are linked in functional neuronal
circuits that appear to be damaged in some way. But what and where is the damage?
Clearly, neuropsychological tests do not allow us to look into the brain, but brain imaging
techniques do” (Williamson, p. 73-74).
III. Environmental Aspects of this Disorder
Environment Influences on Schizophrenia
Nature of Influences
Crimina
l Jus
tice

16
Substance Abuse and Misuse
“The possible effects of season and geography of birth, urbanization, immigration,
substance misuse, prenatal influenza, famine and other stresses,” (Id) can possibly contribute to
this disorder. Schizophrenia however, is usually diagnosed using a “diagnostic system defined
by behavioral syndromes and not by knowledge of etiology and pathophysiological mechanisms.
Psychiatry remains the only branch of medicine where there is a lack of useful laboratory tests to
confirm the diagnosis” (Csernansky, p. 89). Can diagnosis of Schizophrenia become
complicated because of conditions associated with drug-induced disorders? Many drugs present
symptoms that could lead the clinician to misdiagnose this disorder by masking. Drug abuse and
dependence present psychotic symptoms such as hallucinations, delusions, and thought disorder
(Id. p. 90). Can drugs, alcohol, stimulants, hallucinogenic drugs such as Phencyclidine (PCP),
lysergic acid diethylamide (LSD), and assorted Opioids present the same symptoms as
schizophrenia? (See Appendix A Table 1) Substance use or abuse can be an environmental
influence that indicates or duplicates Schizophrenia. Therefore it is imperative that during
diagnosis that the clinician does not misdiagnose because of the physiological effects of these
agents. Schizophrenia symptoms can parallel and be masked by the abuse and misuse of certain
drugs and alcohol. The clinician must conduct a multi-panel drug screen test to eliminate drugs
and or alcohol as the causal agency. However, drug abuse and misuse can be a contributing
factor. “Because chronic psychoses in the context of substance abuse may begin at an earlier
age than in the onset of schizophrenia in the absence of substance abuse, some authorities have
suggested that substance abuse precipitates the illness in the genetically predisposed”
(Csernansky, p. 65).
Crimina
l Jus
tice

17
Primary Influences
The Nuclear Environment
According to Brown and Barlow a great deal of research has examined the aspects of the
person’s social and family influences on emergence or course of the symptoms of schizophrenia.
(p.238) Stuart J. Leask Environmental Influences in Schizophrenia: the Known and the Unknown
posits that one’s genes are the ultimate environmental influence because they affect both internal
and external environment profoundly—by defining the organism. (p. 327). Michael Foster
Green, Schizophrenia Revealed (p. 53) says that:
“Schizophrenia does indeed run in families, not with certainty for any one person but
with a rate higher than would be expected. Family studies show that about 8 percent of
siblings and 5 percent of parents of a schizophrenic individual will have schizophrenia,
compared to roughly 1 percent in the general population…Children of schizophrenic
individuals have about a 12 percent chance of developing schizophrenia” (p. 54).
Family studies have consistently shown that schizophrenia runs in families. In Schizophrenia:
Cognitive Theory, Research, and Therapy (Beck, Rector, Stolar, & Grant) the genetic connection
is considered highly likely to be inherited.
“Eighty years of behavior genetics research in the form of twin, family, and
adoption studies indicate that schizophrenia is highly heritable. Family studies have
consistently shown that schizophrenia runs in families and that the degree of genetic
sharing with the affected member predicts the likelihood of developing
schizophrenia…There is now considerable evidence implicating environmental factors in
the etiology of schizophrenia. Mary Cannon and colleagues, for example, have conducted
a quantitative review that identified three groupings of obstetric complication associated
Crimina
l Jus
tice

18
with schizophrenia: complications occurring during pregnancy (e.g., bleeding, diabetes),
complications occurring at the time of delivery (emergency cesarean delivery, asphyxia),
and abnormal fetal growth and development (e.g., low birth weight). The risk of
schizophrenia associated with obstetric complications is double that without such
complications, a small effect that is comparable in magnitude to the risk associated with
variation in particular genes (Gilmore & Murray)” (Beck et al, p. 12-13).
The connection genetically and environmentally can be established in the early stages of
pregnancy. Jonathan Picker, Ph.D. says in his article The Role of Genetic and Environmental
Factors in the Development of Schizophrenia that risk for schizophrenia appears to begin as early
as the first trimester in pregnancy.
” Other prenatal factors are also implicated in the second and third trimesters.
These include maternal rubella and respiratory infections, low socioeconomic class,
maternal deprivation resulting from war or famine, urban birth, obstetric complications,
and birth in late winter/early spring (Dohrenwend et al., 1992; Lewis and Murray, 1987;
Marcelis et al., 1999; Susser et al., 1996; Torrey et al., 1997). A direct observation of
genetic and environmental factors interacting in the perinatal period was demonstrated
when it was shown that fetal hypoxia, an environmental insult, was associated with
decreased grey matter and increased cerebrospinal fluid (CSF) in patients with
schizophrenia and their relatives but not in genetically low-risk individuals (Cannon et
al., 1993)” (Picker, Ph.D.).
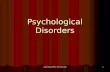
The genetic connection can be seen graphically (See Appendix B) in Barlow and
Durand (p. 485) specifically in identical twins, this is their findings:
Crimina
l Jus
tice

19
“Gottesman (1991) summarized the data from about 40 studies of schizophrenia,
as shown in Figure 12.3. The most striking feature of this graph is its orderly
demonstration that the risk of having schizophrenia varies according to how many genes
an individual shares with someone who has the disorder. For example, you have the
greatest chance (approximately 48%) of having schizophrenia if it has affected your
identical (monozygotic) twin, a person who shares 100% of your genetic information.
Your risk drops to about 17% with a fraternal (dizygotic) twin, who shares about 50% of
your genetic information. And having any relative with schizophrenia makes you more
likely to have the disorder than someone in the general population without such a relative
(about 1%). Because family studies can't separate genetic influence from the impact of
the environment, we use twin and adoption studies to help us evaluate the role of shared
experiences in the cause of schizophrenia” (Barlow and Durand, p. 485)
Michael Foster Green says in his book Schizophrenia Revealed, that schizophrenia is
undoubtedly a genetic disorder and the estimated inheritability rates range from 74 percent to as
high as 90 percent. And, the most important factors for the development of schizophrenia are
transmitted through the genetics (p. 51-52). Subsequently, the genetic link is known and
understood by researchers to be a major contributor to schizophrenia.
Interactions with Biological Influences
Place of Birth: Urbanization:
The risk increases in comparative environments such as rural and urban areas.
“Researchers have found a positive correlation between rural birth, and living conditions and
Crimina
l Jus
tice

20
lower rates of schizophrenia. In fact, a number of studies have demonstrated that psychotic
illness is more prevalent in urban settings than in rural areas. Why this potential connection
exists is unclear, but higher rate in urban areas may be due to environmental toxins, the social
context that people live in, and viruses or influenza, including prenatal infections. Where you are
born and brought up is a larger contributing factor to risk than genetic predisposition”
( Schizophrenia.com). If one looks at the predilection that is found—more in urban areas than
rural areas—for disease susceptibility and mental psychosis based on environmental causes, one
can correlate schizophrenia to diet and environment that is evident genetically (biologically)
imposed on each succeeding generation. People who live in an environment replete with toxins,
inadequate diet, and a constant bombardment of social diseases, such as flu strains et al, coupled
with pregnancy weaknesses because of biological and environmental pressures, it stands to
reason that the resultant would be offspring that are biologically/genetically damaged. The
biological effects are and can be enhanced by the environmental influences, and both are
contributory towards this disorder if one is predisposed to schizophrenia genetically. What
treatments are existent or forthwith for schizophrenia? Can proper diet assist the schizophrenic
patient? Can improper diet prove to be detrimental to schizophrenia?
Diet
Bad or incorrect diet can be detrimental to the schizophrenic patient. In Shonda’s case,
her diet requirements will enter the regimen when she achieves the ability to learn correct
choices and how to incorporate these correct choices into her daily therapeutic program. It is
Crimina
l Jus
tice

21
recommended that Shonda be assigned a Dietician to assist her with correct food and vitamin
choice selections. Some problems that schizophrenics incur can, and does, include diabetes and
blood sugar complications. Sugar problems exacerbated with drug and stimulant excesses, can
cause complications in the schizophrenic.
Blood sugar problems are exacerbated by excessive stimulant, drug use, (Leask, p. 325)
and diet.
“It is well known that diet affects a person's physical health and can lead to
conditions such as diabetes and coronary heart disease. But can your diet affect your
mental health as well? An article in the British Journal of Psychiatry suggests that it does.
The most consistent correlation found in this study, was that increased consumption of
refined sugar results in an overall worse outcome for schizophrenia, as measured by both
the number of days spent in the hospital and poor social functioning”
(schizophrenia.com).
Excessive intake of sugar, refined carbohydrates, caffeine, alcohol and cigarettes, (Leask, p.
325,) as well as stimulant drugs, (such as amphetamines and cocaine) (nimh.nih.gov) all affect
one’s ability to keep their blood sugar level balanced. Antipsychotic medication may also
complicate blood sugar level control. The incidence of blood sugar problems and diabetes is
much higher in those with schizophrenia. Excessive smoking is also linked to an increased risk.
Your daily intake of sugar, refined carbohydrates, nicotine, caffeine, and stimulant drugs
should be regulated by a psychiatrist and a dietician. “Previous studies have shown that insulin
resistance and diabetes as well as heart disease occur with greater frequency in people with
schizophrenia. Insulin resistance is increased by regularly high intake of sugar and saturated fats”
(Id). Also pay particular attention to the following: (foodforthebrain.org)
Crimina
l Jus
tice

22
• Essential fat imbalances (Need to use Omega 3 & 6 oils)
• Excessive oxidant intake and not enough antioxidants (Ester C is useful here as an
antioxidant)
• Food allergies (Avoid red food dyes)
Diet and substance usage must be considered in the patient’s diagnosis. And for the long
term prognosis, a dietary regimen should be prescribed according to mental and physical
condition, and overall patient system demand. This should be correlated with the results of the
lab panels of the patient.
IV. Treatment Approaches
Medical Treatments:
Medical Approaches to Treatment
What types of medical approaches (ECT, prescription medications, psychosurgery) are
used in treating this disorder?
Treatment (s) begins with initial work-ups, (medscape.com) to rule out any conditions
that may mimic schizophrenia, identify any comorbid conditions, and establish a baseline for
monitoring the treatment course and response to treatment. Medical examinations begin with
thorough physical and mental examinations. “The physical exam should include a thorough
neurologic exam, plus urine and serum screening for alcohol, other drugs that may be abused,
and level of antipsychotic medications if currently prescribed. In addition, such basic lab tests as
CBC; serum electrolytes; glucose, liver, renal, and thyroid function; and HIV and syphilis
testing” (medscape.com). The possible medical approaches to treatment include the following.
Crimina
l Jus
tice

23
Several medical treatment therapies exist, including the somewhat faded
electroconvulsive therapy (ECT), that may be used when someone does not respond to
medication, Barlow and Durand (pg. 243). Used early in the 20th century, and subsequently
abused as a therapy, the treatment has since evolved into a safe and reasonably effective
treatment for severe cases that do not respond to medications, found useful in cases of severe
depression. The usual first course of treatment is described as:
“While prescription of an antipsychotic medication for schizophrenia is the first
step of treatment and for the resolution of an acute episode of psychosis, it is increasingly
recognized that comprehensive care requires the integration of adjunctive therapies and
attention to long-term treatment goals, including relapse prevention and psychosocial
rehabilitation. In the absence of a cure for schizophrenia, clinicians can optimize
outcomes by combining pharmacotherapy with a treatment approach that incorporates
symptom monitoring, assessment of treatment adherence and medication side effects,
management of medical and psychiatric comorbidities, and nonpharmacologic therapies
directed at functional rehabilitation and improved quality of life” (Mahgerefteh, Pierre, &
Wirshing, pg. 1).
Medications such as antipsychotic are listed in Barlow and Durand (p. 429) Barlow and Durand
(p. 496) et al. See Appendix C for a table that describes many of these medications. Taken from
(uspharmacist.com).
Barlow and Durand considered the treatment of schizophrenia with antipsychotic
medications a real breakthrough in the 1950s with the advent of drugs called neuroleptics,
(meaning “taking hold of the nerves”) and these drugs provided the first real help and hope for
Crimina
l Jus
tice

24
patients diagnosed with schizophrenia. (p.495) However they go on to say that these drugs are
effective with some and not with others (Id). There are also intrusive therapies such as
psychosurgery (aka frontal lobotomy) that can be considered as a treatment for schizophrenia.
Although considered by many to be a barbaric procedure the operation is still used in some
societies such as Kenya (Barlow & Durand, p. 495).
“Psychosurgery has a very checkered past in psychiatry. Frontal lobotomies
introduced in the United States by Walter Freeman in 1936 were proposed as a way of
isolating the diseased frontal lobe from the rest of the brain. Unfortunately, they lead to
emotional flatness, euphoria, and a lack of judgment. With the introduction of better
treatments such as chlorpromazine, psychosurgery has been all but abandoned… Of
particular interest is the use of chronic electrical stimulation of the sub-thalamic nucleus
in medical refractory Parkinson disease, a treatment that has been associated with lasting
benefits in many patients (Krause et al, & Romito et al.). The precise mechanism of
effectiveness is not known, but it is likely that the stimulation leads to diminished
inhibitory outflow of the internal segment of the globus pallidus onto the motor thalamus,
resulting in improvement in the motor symptoms of the disease. Is it possible that deep
brain stimulation could be offered to refractory schizophrenic patients? Many of these
patients face a lifetime in seclusion. I would not doubt that many would choose to take
the risks of surgery if one were available. Unfortunately, no procedures are available, but
it is likely only a matter of time before one is developed” (Williamson, p. 179-80).
Psychosurgery probably should be considered as a last resort treatment option. Other treatments
such as medications and psychotherapy should be considered first.
Crimina
l Jus
tice

25
Medical Benefits of Medications
What are the effects these medications have on the brain chemistry or neurotransmitter
activity?
"Given the relative safety of most antipsychotic medications," the APA Guideline
recommends that the psychiatrist "begin treatment with an appropriate medication, even in states
where involuntary use of medication must be approved by a court, and perform the necessary
evaluations as they become possible" (medscape.com). Mayo Clinic in the article Schizophrenia
by Mayo Clinic Staff explains the medical concept of antipsychotics used to control
schizophrenia.
“Antipsychotic medications are the most commonly prescribed to treat
schizophrenia. They're thought to control symptoms by affecting the brain
neurotransmitters dopamine and serotonin. A person's willingness to cooperate with
treatment may affect medication choice. Someone who is uncooperative may need to be
given injections instead of taking a pill. Someone who is agitated may need to be calmed
initially with benzodiazapine such as lorazepam (Ativan), which may be combined with
an antipsychotic” (mayoclinic.com, p. 7).
The drugs used to control schizophrenia can effectively block and regulate the production or
non-production of dopamine, serotonin, GABA, and norepinephrine all thought to contribute to
schizophrenia as neurotransmitters.
Contraindications
What, if any, side effects are associated with the medical treatments?
Crimina
l Jus
tice

26
The article Schizophrenia, (nimh.nih.gov) says that some of the antagonists to
schizophrenia can be found in drugs such as cocaine, marijuana, and amphetamines. These
drugs may worsen the existing condition. Schizophrenia nimh.nih.gov also says:
“Addiction to nicotine is the most common form of substance abuse in people
with schizophrenia. They are addicted to nicotine at three times the rate of the general
population (75 to 90 percent vs. 25 to 30 percent).
The relationship between smoking and schizophrenia is complex. People with
schizophrenia seem to be driven to smoke, and researchers are exploring whether there is
a biological basis for this need. In addition to its known health hazards, several studies
have found that smoking may make antipsychotic drugs less effective.
Quitting smoking may be very difficult for people with schizophrenia because
nicotine withdrawal may cause their psychotic symptoms to get worse for a while.
Quitting strategies that include nicotine replacement methods may be easier for patients
to handle. Doctors who treat people with schizophrenia should watch their patients'
response to antipsychotic medication carefully if the patient decides to start or stop
smoking” (nimh.nih.gov, p. 3).
Side effects include the following:
“The most common side effects associated with conventional antipsychotics are
sedation, anticholinergic and antiadrenergic effects, and neurological side effects. Nearly
all patients experience sedation early in treatment with conventional antipsychotics, but
the symptom can often be managed by lowering the dose, consolidating divided doses
into a once-a-day bedtime dose, or prescribing a less sedating antipsychotic. Between
10% and 50% of patients taking conventional antipsychotics develop anticholinergic or
Crimina
l Jus
tice

27
antiadrenergic side effects. In some cases, patients have mild and tolerable side effects
such as transient dry mouth, blurred vision, or constipation. More serious anticholinergic
side effects can include central anticholinergic toxicity leading to impaired cognition,
delirium, and hallucination” (medscape.com, p. 2)
Promising Treatments
Which of these medical treatments are most successful according to research that has
been conducted?
Aside from drugs, there are several treatments that show progress and promise. Among
these treatments is a therapy known as psychosocial treatment. Mayo Clinic Psychosocial
treatments; has the following recommendations. This treatment is utilized once the psychosis
recedes then a program like this can be integrated into the patient’s daily regimen. Psychosocial
treatments focus on social training skills, family therapy, vocational rehabilitation and obtaining
gainful employment. And this therapy includes teaching the patient how to cope with the stress
related problems, and how to collectively manage their illness. Williamson offers the following
under the chapter subtitle: Is There Any Reason to Be Hopeful: (p. 180)
“Over the last 50 years, the only option in the treatment of schizophrenia has been
drugs that block D2 receptors. As models of schizophrenia have developed, some other
possibilities have started to emerge. The early attempts to find drugs that decrease
dopamine subcortically and 'without decreasing dopamine cortically have been
disappointing, but there are now some other approaches targeting glutamate, GABA, and
other neurotransmitters. Of these, drugs that affect the glycine receptor and lamotrigine
look promising, but many more are in development (Miyamoto et al,). One of the
Crimina
l Jus
tice

28
limitations of the glutamatergic drugs is that ionotropic receptors are ubiquitous in the
brain. Metabotropic receptors may be more regionally specific but we do not as yet know
if they have any antipsychotic properties.
Probably the most hopeful sign in treatment is that we are now starting to think
about ways of preventing deterioration in patients, not just providing acute treatment of
their symptoms. Many of the drugs already available such as lamotrigine have the
potential to prevent deterioration by virtue of their neuroprotective properties. However,
long-term studies are required to demonstrate these benefits. This research is not
something that the drug companies are eager to do, but it is essential if we hope to change
the course of this disorder” (Williamson, p. 180).
Psychosocial Treatments of Schizophrenia
Common Treatments
“Psychosocial rehabilitation for persons with schizophrenia refers to programs
and treatment interventions that are intended to provide knowledge and teach skills and
behaviors for "living in the world," This includes work and social skills, education about
the disease, medications, symptom management, and relapse prevention. The notion that
patients with schizophrenia can significantly improve their level of functioning is crucial
to the paradigm of recovery, A longitudinal study comparing patients who participated In
a "meds, maintenance, and stabilization" program vs. a bio-psycho-social rehabilitation
Crimina
l Jus
tice

29
program after being discharged from a state hospital in the late 1950s showed that, 30
years later, those who had been in the rehabilitation program had far fewer symptoms of
schizophrenia, had a greater percentage in the workforce, and had better community
adjustment” (Csernansky, p. 184-85).
With this in mind, it will benefit the patient, in this case Shonda, to participate in
psychosocial therapeutic programs as necessary. The schizophrenic patient will need several
psychosocial skill sets to basically survive with their disease in a real world setting. Also, the
caretakers whether they are immediate family, or others, also need training on how to facilitate
that care for their loved one or patient. Schizophrenia is not an easy disease to comprehend or
treat without specific skills. The following list the major psychosocial treatment programs as
listed in Mayo Clinic. (mayoclinic.com).
1. Social skills training.
This focuses on improving communication and social interactions.
2. Vocational training and rehabilitation with supported employment.
This usually focuses on helping people with schizophrenia to find and then keep jobs.
3. Family interventions.
The education of the family in how to support the individual afflicted with schizophrenia.
4. Individual therapy.
This will instruct the person with schizophrenia how to cope with their illness and how to
recognize signs of relapse.
Most Effective Schizophrenia Treatments
Crimina
l Jus
tice

30
The most effective of these psychosocial treatments can be realized in the rehabilitation
sector of this treatment regimen. Schizophrenia patients must learn how to function within
society while learning how to cope with their disease. Social skills such as shopping at a store,
initiating conversations in general, making friends, finding and then keeping a job are all
necessary for the schizophrenic patient if they are going to function outside of a medical care
facility. Coupled with their medicines, the patient must learn how to adapt to social settings
while living with their disorder. They must learn self-help skills such as personal hygiene,
money management, and proper nutrition. The most effective treatments as previously
mentioned by Csernansky were those who followed a “rehabilitation program after being
discharged from a state hospital in the late 1950s showed that, 30 years later, those who had been
in the rehabilitation program had far fewer symptoms of schizophrenia, had a greater percentage
in the workforce, and had better community adjustment.” The rehabilitation program (s) with the
medication applications can be effective in schizophrenia management.
Treatment Plan for Shonda
Continuous Schizophrenia: Paranoid Type
Shonda’s case indicates the necessity of an antipsychotic medication regimen. Shonda
will continue to take the neuroleptic haloperidol (Haldol) because of her increase in auditory
hallucinations and other conditions that she exhibits. Shonda will be reassessed by the
psychiatric team, in accordance with her treatment plan, to see if she will continue to take this
medication or if there is enough improvement to be prescribed another medication or reduce the
dosage that will allow Shonda more functionality. Shonda will be placed into a psychosocial
Crimina
l Jus
tice

31
management program that will allow her to once again return to the work force. Shonda as of
late has been unable to function at her job. Once the delusions and auditory hallucinations are
reduced using psychoeducation and normalization treatments, Shonda should be susceptive to
further psychosocial treatments.
“Psychoeducation and Normalization As discussed broadly by Kingdon and
Turkington (1991), patients vary in the degree to which they want an explanation for the
occurrence of their voices. Some patients explain the voices as a function of having
schizophrenia. As part of the early psychoeducation process, patients are socialized to the
stress-vulnerability view of psychosis and hallucinatory activity, in particular. As such,
explanations to enhance understanding of the role of vulnerability factors can draw on a
number of critical biological (e.g., genetics) psychological (e.g., developmental
experiences), and social (e.g., isolation and marginalization) variables that make sense to
the patient in terms of comprehension and experience…The provision of
psychoeducation with a "normalizing" rationale also initiates the accumulation of
evidence to fuel alternative explanations of the voices, which will be the key component
of their successful treatment” (Beck, Rector, Stolar, & Grant, p. 243-45)
The patient Shonda, using psychoeducation and normalization techniques, will learn how
to divert attention away from hearing the voices. Shonda will be encouraged to watch TV, listen
to music, make conversations, read, and perhaps play a video game. Shonda will be encouraged
to engage in effortful activities such as playing sports, working out at a health spa, going for a
walk or jog. These activities can become diversions to voices and act as a suppression or
suppressors. Many cases of voice noise acceleration occur during anxious arousal moments, so
Crimina
l Jus
tice

32
Shonda will be encouraged through therapy to utilize relaxation methods, and meditation
techniques.
With the modern treatment medications and therapies, Shonda’s prognosis is positive.
Shonda has already functioned at a job in the past and has had her own apartment. Shonda will
be encouraged to be retrained as needed because of her relapse and once again she will occupy
her own apartment and have a job. Because Shonda’s schizophrenia is complicated with
paranoia, the therapist must gain her trust. With the right therapy and therapist team, Shonda
should show improvement if the sessions are coupled with good communications, positive
reinforcement, a warm working relationship between Shonda and the therapy team. Because of
her paranoid suspicions, Shonda will need reassurance that everyone on the therapy team is on
her side.
V. Conclusion
Evidence abounds that connects schizophrenia to families predisposed genetically to this
disorder. The family inheritance rate varies, but is significantly higher than the general
populace. Environmental contributions such as drug and alcohol use (and abuse) are also
contributing factors. The geography of birth, urbanization, and influenzas transferred to the fetus
can impact the predisposed recipient also. This seems to affect those living in an urban setting
more so when compared to those who live in rural areas. The lack of prenatal care, diet, famine
and stresses all complicate and are participatory in generating weaknesses in the predisposed for
the schizophrenic disorder. However, the genes are the ultimate environmental influence
Crimina
l Jus
tice

33
because they affect both the internal and external environment profoundly. Nonetheless, current
treatment plans are having an effect on schizophrenia and this can be seen in positive
advancements. Many psychological models are available for treatment regimens.
Psychological Models
Psychological models that can be applied to treatment and understanding of this
disorder—schizophrenia are found in psychodynamic, behavioral, humanistic, cognitive and
biological models. Which psychological model (s) affords the best treatment and control
regimens for the paranoid schizophrenic patient? The Psychodynamic approach and treatment
with its origin in the psychoanalysis of Dr. Sigmund Freud, is still practiced by psychotherapists
in larger cities (Barlow & Durand, p. 23), the insurance companies have reduced the therapy
sessions to around 25 per year, most courses of therapy only last fewer than 10 sessions (Kring,
Davison, Neale, & Johnson, p. 45-46). This treatment is based on the three parts as defined by
Freud, The Id, Ego, and Superego. Freud believed that people are “stuck” in any one of these
stages and have not progressed beyond that particular stage. Would this therapy prove beneficial
to the schizophrenia disorder? As a therapy that involves talking and listening, it could be useful
in conjunction with medication during initial case presentation and discovery of patient’s
background, otherwise as a standalone therapy, no!
Behavioral models are based on operant conditioning by Pavlov, Watson, and B.F.
Skinner. Could this model and treatment prove beneficial?
“Everything from preparing a meal and managing finances to communicating with a
psychiatrist about medication side effects requires psychosocial skills that many patients
are lacking. Some patients had the skills before they became ill, others never really had
Crimina
l Jus
tice

34
them. How does one train patients in the use of such skills? If you are a behaviorist, you
would use behavioral principals such as reinforcing desired behaviors and ignoring non-
desired behaviors” Green, p. 138).
The response solicited and used in operant conditioning behaviorism was a reward based system.
To reinforce the desired behavior patients were rewarded for correct actions and responses. “In
social skills training, a particular group of skills is selected; these could include skills necessary
for managing symptoms, for community re-entry, or for starting and maintaining conversations.
The trainers use a range of techniques, including teaching, demonstrating the desired behavior,
coaching the patient during role-plays of desired behavior, giving strong verbal encouragement,
and assigning homework” (Id, p. 139). Would this therapeutic approach be one that would assist
and improve the patient with schizophrenia? Yes it would!
Humanistic approaches offer an approach that seeks the good and potential of every
individual. The Humanistic Theory posits:
“Jung and Adler broke sharply with Freud. Their Fundamental disagreement concerned
the very nature of humanity. Freud portrayed life as a battleground where we are
continually in danger of being overwhelmed by our darkest forces. Jung and Adler, by
contrast, emphasized the positive, optimistic side of human nature. Jung talked about
setting goals, looking toward the future, and realizing one's fullest potential… The
underlying assumption is that all of us could reach our highest potential, in all areas of
functioning, if only we had the freedom to grow. Inevitably, a variety of conditions may
block our actualization. Because every person is basically good and whole, most blocks
originate outside the individual” (Barlow & Durand, p. 24).
Crimina
l Jus
tice

35
Can this positive approach find usefulness in schizophrenia therapy? Yes because, the
patient already has problems with their disorder that separates them from the general population
and they usually have problems with confidence (self) and self-assurance. Making the patient
see their potential, orienting them to something that accentuates the positive, followed by giving
them the training and freedom to grow and improve is essential for their overall wellbeing.
Other possible models are cognitive and biological. Cognitive behavior therapy for
schizophrenia uses a psychotherapeutic approach to treat the symptoms of schizophrenia. The
cognitive approach has the patient alter their beliefs, views, and assumptions and to shift their
views about their symptoms (Green p. 136). This treatment model compliments other models of
treatment.
“Although medications are crucial in the management of schizophrenia, many
people with the disorder are not compliant with taking the medications, and even if they
are compliant, over 50% of people with schizophrenia will continue to have distressing
symptoms. Thus, complementary and additional treatments are needed. Cognitive and
behavioral interventions have demonstrated effectiveness with depression, panic, eating
disorders, OCD, insomnia, phobias, and other disorders. Cognitive Therapy has also been
shown to be very effective in helping patients with schizophrenia manage their
symptoms. Outcome studies suggest that patients who receive CT have fewer and less
intense hallucinations and delusions, and recover their functioning to a greater extent than
patients who do not receive Cognitive Therapy” (McFarr, p. 2).
This treatment regimen shows effectiveness in schizophrenia management by patients using this
therapy model.
Crimina
l Jus
tice

36
Model (s) of Choice for Shonda
The model (s) of choice for Shonda would be found in the behavioral, humanistic, and
cognitive models. Because Shonda needs to continue her medications she will also need to learn
or relearn some behavioral concepts. And Shonda needs positive reinforcement, so humanistic
treatment would also be conducive to her treatment regimen. For Shonda, one model exclusively
would not achieve the best results. Therefore a composite of therapy models would produce the
best results. Cognitive therapy would prove beneficial to Shonda. She would learn how to
ameliorate her condition, be able to foresee a relapse before it comes. And before she becomes
incapable of doing her job or taking care of herself again, Shonda will have the knowledge and
experience to handle this problem, whereas in the past, she did not. She would learn how to
better control her symptoms pre-relapse and recognize any signs of emergent onset. The
biological model would be inappropriate for Shonda as she has had little contact with her sibling
and her parents were aloof from her during upbringing. Her history already reveals a biological
connection to this disorder.
Schizophrenia’s Future
“Genetically, schizophrenia is a complex disease whose pathogenesis is likely governed
by a number of different risk factors. While substantial efforts have been made to identify
the underlying susceptibility alleles over the past 2 decades, they have been of only
limited success. Each year, the field is enriched with nearly 150 additional genetic
association studies, each of which either proposes or refutes the existence of certain
schizophrenia genes. To facilitate the evaluation and interpretation of these findings, we
have recently created a database for genetic association studies in schizophrenia
Crimina
l Jus
tice

37
(‘‘SzGene’’; available at http://www.szgene.org). Currently, these meta-analyses
highlight not only over 20 different potential schizophrenia genes, many of which
represent the ‘‘usual suspects’’ (e.g. various dopamine receptors and neuregulin 1), but
also several that were never meta-analyzed previously… Eventually, only the concerted
efforts of genetics, genomics, proteomics and clinical disciplines will give rise to new
diagnostic and therapeutic targets that, hopefully in the not too distant future, will benefit
the millions of patients afflicted with this debilitating disorder.” (Bertram, p. 806 & 811).
The future for people with schizophrenia continues to improve. Research studies are
advancing. Medical advancements will continue to produce medications that will help control
the symptoms of schizophrenia. Although there is no cure, treatments that work well are and will
continue to be available. The science of neurotransmitter function is advancing every year. At
the onset of understanding this disorder, there was little that could be done. Now however,
treatment regimens are replete and patients are receiving adequate treatment for their disorder
with medications and therapies. Today many people with schizophrenia are improving enough
to lead independent, comfortable lives. They are able to work and live in their own homes
whereas, in times past they would likely end up in a mental care facility for the rest of their lives.
Shonda’s Future
Shona’s future is optimistically bright but contingent on her treatment regimen and
response to this program. With the newer models and modalities of treatment programs
available today, Shonda can function very well in society. However, her assessment should
determine employment options accordingly. She should be advanced slowly and encouraged to
learn more and do more on the job and for herself as well. If Shonda utilizes the
Crimina
l Jus
tice

38
psychoeducation and normalization treatments, she can really improve because these therapies
will offer an alternative to her symptoms and a distraction that she will find to be positive and
enjoyable. Based on what has been covered and discovered in this project, Shonda has a bright
future ahead of her.
Final Thoughts
Evidence abounds that connects schizophrenia to families predisposed genetically to this
disorder. The family inheritance rate varies, but is significantly higher than the general
populace. Environmental contributions such as drug and alcohol use (and abuse) are also
contributing factors. The geography of birth, urbanization, and influenzas transferred to the fetus
can impact the predisposed recipient also. This seems to affect those living in an urban setting
more so when compared to those who live in rural areas. The lack of prenatal care, correct diet,
famine and stresses all complicate and are participatory in generating weaknesses in the
predisposed for the schizophrenic disorder. However, the genes are the ultimate environmental
influence because they affect both the internal and external environment profoundly.
Nonetheless, current treatment plans are having an effect on schizophrenia and this can be seen
in positive advancements in the current treatment regimens of schizophrenia.
Crimina
l Jus
tice

39
References
APA guideline for treating adults with schizophrenia: Treatment strategy in the acute phase.
http://www.medscape.com/viewarticle/431253_3
Barlow, David H. & Durand, V. Mark Abnormal psychology an integrative approach (2nd ed.,
Vol. 1). Belmont, CA, USA : Wadsworth/Thomson Learning
Barlow, David H. & Durand, V. Mark Abnormal psychology: Media edition (2nd ed., Vol. 1).
Belmont, CA, USA : Wadsworth/Thomson Learning
Barlow, David H., Durand, V. Mark, Essentials of abnormal psychology. Centage Learning:
Mason, OH
Beck, A.T., Rector, Neal A., Stolar, Neal M., Grant, Paul M. Schizophrenia:
Cognitivetheory, research and therapy. New York, NY: Guilford Press
Bertram, Lars, Genetic research in schizophrenia: New tools and future perspectives
http://schizophreniabulletin.oxfordjournals.org/cgi/content/abstract/sbn079
Csernansky, John G., (1st ed.) Schizophrenia: A new guide for clinicians. NY: Marcel
Dekker, Inc.
Country and Rural life (vs. city living) before age 15 is associated with lower rates of
schizophrenia http://www.schizophrenia.com/prevention/country.html
Diet may affect outcome of schizophrenia
http://www.schizophrenia.com/sznews/archives/002546.html
Durham, Jennifer., PharmD, Eon, Stacy., Schizophrenia: A review of pharmacologic and
nonpharmacologic treatments. http://www.uspharmacist.com/content/c/16526/
Green, Michael F., Ph.D., Schizophrenia revealed: From neurons to social interactions. New
York, NY: W. W. Norton & Company, Inc.
Crimina
l Jus
tice

40
Kring, Ann M., Davison, Gerald C., Neale, John M., & Johnson, Sheri L., Abnormal psychology
(10th ed.) Danvers, MA: Wiley & Sons.
Leask, Stuart J., Environmental influences in schizophrenia: The known and the unknown
http://apt.rcpsych.org/cgi/reprint/10/5/323.pdf
McFarr, Lynn Marcinko, PhD. Schizophrenia and cognitive therapy
http://www.academyofct.org/Library/InfoManage/Guide.asp?FolderID=1097&SessionID
Magnavita, Jeffrey J., Etiology, theory, psychopathology, and assessment
http://media.wiley.com/product_data/excerpt/62/04712011/0471201162.pdf
Mahgerefteh, Shirly., Pierre, Joseph M., MD, and Wirshing, Donna A., MD Treatment
challenges in schizophrenia: A multifaceted approach to relapse prevention.
http://www.psychiatrictimes.com/display/article/10168/49456?verify=0#
Neurotransmitters: Testing/Treating
http://www.nhnatural.com/services/neurotransmitterbalance.html
Picker, Jonathan, Ph.D. The role of genetic and environmental factors in the development of
schizophrenia.
http://www.psychiatrictimes.com/display/article/10168/52516?pageNumber=3
Schizophrenia: Food for the brainhttp://www.foodforthebrain.org/content.asp?id_Content=1638
Schizophrenia by Mayo Clinic staff http://mayoclinic.com/health/schizophrenia/DS00196
Schizophrenia is a disorder of the brain (as is Bipolar Disorder / Manic Depressive)
http://www.schizophrenia.com/disease.htm
Schizophrenia: National Institute of Mental Health
http://www.nimh.nih.gov/health/publications/schizophrenia/
Thomas, Sherine., The etiology of schizophrenia
Crimina
l Jus
tice

41
Williamson, Peter, Mind, brain, and schizophrenia. New York, NY: Oxford University Press
Web Pro 5.52 World Net Database. Princeton University. Installed Software Program
Crimina
l Jus
tice

42
Appendix A
Figure 4.4 This computer graphic of a synapse shows the release of neurotransmitters (pink
spheres at lower center) by vesicles inside the synaptic knob (upper center). The
neurotransmitters will cross the gap and bond to the receptors of the adjacent cell, which is how
information is transmitted along the nervous system. © Alfred Pasieka/Photo Researchers, Inc.
Crimina
l Jus
tice

43
Figure 4.1 The Image Source is: Laboratory of Neuro Imaging, UCLA, Derived from
high-resolution magnetic resonance images (MRI scans), the above images were created after
repeatedly scanning 12 schizophrenia subjects over five years, and comparing them with
matched 12 healthy controls, scanned at the same ages and intervals. Severe loss of gray matter
is indicated by red and pink colors, while stable regions are in blue. STG denotes the superior
temporal gyrus, and DLPFC denotes the dorsolateral prefrontal cortex. Note: This study was of
Childhood onset schizophrenia which occurs in 1 of every 40,000 people and is frequently a
significantly more aggressive form of schizophrenia (than later onset schizophrenia which
afflicts approximately 1 of every 100 people) (schizophrenia.com).
Crimina
l Jus
tice

44
Appendix A-Table 1 Prescription Drugs Reported to Cause Various Psychotic Symptoms
Paranoia and delusions
Acyclovir
Amphetamines
Anabolic steroids
Cephalosporins
Cimetidine
Corticosteroids
Hallucinations
Anticholinergic drugs
Baclofen (on discontinuation)
Calcium-channel blockers
Cimetidine
Dopamine agonists
Ethambutol
Crimina
l Jus
tice

45
Cycloserine
Dopamine agonists
Ethosuximide
Methylphenidate
Theophylline
Other unspecified psychotic symptoms
Aminoglycosides
Beta-blockers
Bumetanide
Cyclobenzaprine
Gancyclovir
Hydralazine
Lidocaine
5-Flucytosine
Indomethacin
Isoniazid
Phenytoin
Vincristine
Procaine penicillin
Sympathomimetics
Tocainide
Trimethoprim
Vinblastine
Zidovudine (AZT)
Crimina
l Jus
tice

46
Appendix B
Crimina
l Jus
tice