A double-blind, randomized, controlled study of oral pirfenidone fortreatment of secondary progressive multiple sclerosis
Jonathan E Walker*,1, Shri N Giri2 and Solomon B Margolin2
1Board Certified Psychiatry and Neurology, 12870 Hillcrest, Suite #201, Dallas, TX 75230, USA; 2Marnac, Inc., 9400 N.Central Expressway, Suite #305, Dallas, TX 75231, USA
Currently, there are no approved treatments for secondary progressive multiple sclerosis (MS) that stabilize or reverse the neurologicaldisabilities associated with this disease. Oral pirfenidone was found to stabilize and overcome the disabilities in two published independentopen-label studies in secondary progressive MS. This led us to study pirfenidone in a phase II double-blind, randomized and controlled,clinical trial in patients with advanced secondary progressive MS for 12 months. Forty-three patients met the eligibility criteria approvedby the IRB and accepted by the FDA. Of these patients, 18 were randomly assigned to placebo and 25 patients to oral pirfenidone groups.All eligible patients were included in the statistical analysis of the data according to intention-to-treat principles. Some patients on oralpirfenidone manifested mild drug-related adverse effects, but it was well tolerated overall. By one month, pirfenidone significantly ( PB/
0.05) improved the Scripps Neurological Rating Scale (SNRS) scores, and scores remained significantly improved for 3, 6 and 12 monthswhen compared to the baseline SNRS scores. In contrast, the SNRS scores of patients on oral placebo were not significantly improved at1, 3, 6 or 12 months of the study, when compared with baseline scores. Oral pirfenidone significantly ( PB/0.04) reduced the incidence ofrelapses (27.8% on placebo versus 8.0% on pirfenidone). Furthermore, oral pirfenidone treatment was associated with a markedimprovement in bladder dysfunction (40.0% on pirfenidone versus 16.7% on placebo). Expanded Disability Status Scale scores and MRIlesion count were not significantly different in the placebo and pirfenidone groups. These findings indicate a significant effect of pirfenidoneon clinical disability and bladder function for secondary progressive MS patients. A major multicentre, double-blind, randomized,controlled trial is justified.Multiple Sclerosis (2005) 11, 149�/158
Key words: multiple sclerosis; pirfenidone; TNF-alpha; treatment
Introduction
Multiple sclerosis (MS) is a demyelinating disorder that
is characterized by neurological deficits attributable to
demyelinating lesions and progressive axonal loss in the
white matter. It is one of the most common central nervous
system disorders, with prevalence of 250 000�/350 000
persons in the USA.1 The clinical signs of MS may appear
at any age, although the onset of this neurological disorder
in childhood or after age 50 is rare. The incidence of MS in
females is twice that in males. Although the underlying
pathogenic mechanisms of MS are poorly understood,
environmental, genetic and immune factors have been
implicated.2�4
The immunological factors responsible for destruction
of the myelin sheath have been the focus of much
investigation. In this regard, there is a great deal of
evidence for the involvement of TNF-alpha in the demye-
lination and consequently in the progressive pathogenesis
of MS5�9 for a number of reasons. First, it has been
demonstrated in vitro that TNF-alpha is cytotoxic for
murine and rat oligodendrocytes, the myelin-producing
cells in the CNS,10 and there is a strong association
between TNF-alpha level in cerebrospinal fluid (CSF)
and disease progression in patients with MS.11 Secondly,
both TNF-alpha and interferon-gamma are able to induce
expression of intercellular adhesion molecule-1 (ICAM-1)
on human brain endothelial cells12 and on both oligoden-
drocytes and astrocytes in vitro.13 There is also evidence
that TNF-alpha is able to induce expression of vascular
cell adhesion molecule-1 (VCAM-1) on spinal cord en-
dothelium in animals suffering from experimental allergic
encephalomyelitis (an animal model of MS).14 Upregula-
tion of ICAM-1 and VCAM-1 on brain endothelium has
been demonstrated in MS plaques15 and is probably a
prerequisite for entry of inflammatory cells in the CNS
parenchyma. Increased levels of ICAM-1 and TNF-alpha
in serum and CSF of MS patients have been found to
correlate with disease activity.16 In addition, proinflam-
matory cytokines such as TNF-alpha, IL-1 and interferon-
gamma induce the synthesis of nitric oxide17,18 with broad
proinflammatory activity. There is a strong expression of
inducible nitric oxide synthase activity in macrophages in
regions of active demyelination in MS lesions.19
The evidence that TNF-alpha plays a pivotal role in the
pathogenesis of MS led us to investigate the effects of
pirfenidone, a known inhibitor of TNF-alpha synthesis
*Correspondence: Jonathan E Walker, 12870 Hillcrest,Suite #201, Dallas, TX 75230, USA.E-mail: [email protected] 14 April 2004; revised 23 September 2004;accepted 29 September 2004
Multiple Sclerosis 2005; 11: 149�/158www.multiplesclerosisjournal.com
# 2005 Edward Arnold (Publishers) Ltd 10.1191/1352458505ms1134oa

and its pharmacological and toxicological actions,20 �22 in
two independent open trials in secondary progressive MS
patients.23,24 Encouraged with the favourable outcome of
these two open trials, we tested in the present study the
efficacy of pirfenidone in a phase II double-blind, rando-
mized study in patients with advanced secondary pro-
gressive MS.
Methods
Study designThe protocol for a randomized double-blind controlled
study in advanced secondary progressive MS that was
approved by an institutional review board and accepted
by the FDA was followed in this trial study. Each patient
enrolled in the study signed an approved informed
consent form that was properly countersigned by a
qualified witness.Forty-three patients with severe secondary progressive
MS were initially enrolled in the study. Patients were
evaluated for neurological dysfunction and had brain MRI
scans just before being enrolled and subsequently at six
and 12 months.
Patient selection Forty-three patients with a diagnosis of
advanced secondary progressive MS25 were recruited for
this double-blind study from a single neurology practice.
The demographic and baseline clinical characteristics of
patients randomly assigned to placebo and pirfenidone
groups are shown in Table 1. Patients had relapsing and
remitting MS for varying lengths of time since the first
neurological diagnosis (Table 1). At baseline, none of the
patients were immunosuppressed as evaluated by total
WBC counts, WBC differential counts or lymphocyte
counts.The neurologist had closely followed all patients before
being admitted to the study and these patients had
experienced definite progressive worsening symptoms
for two years or longer. The enrolled patient population
was drawn from an ongoing neurology practice and this
setting reflected a traditional neurology specialty practice.
Inclusion criteria Included: 1) clinically definite or la-
boratory-supported advanced secondary MS, using the
Poser criteria;25 2) presence of secondary progressive
disease (patients must have worsened by at least one
EDSS unit in the last two years); 3) patients must not have
had an exacerbation during the 30 days prior to enrolment;
4) presence of progressive component of the disease for at
least two years; 5) presence of modified Expanded
Disability Status Scale (EDSS) scores between 5 and 8; 6)
agreement to use adequate contraception during the study
for fertile female patients; and 7) patients must be able to
understand and sign an informed consent form.
Exclusion Patients were excluded from the study based
on the following criteria: 1) unlikely to complete the
scheduled follow-up visits; 2) treated with immunosup-
pressive drugs within the past 90 days; 3) pregnancy or
breast feeding; 4) severe medical illness of any kind; and
4) inability to undergo an MRI scan.After completion of screening evaluations, 43 qualifying
patients were enrolled. The procedure for randomization
and blinding were as follows. Dr Walker’s assistant first
informed Marnac, Inc., the sponsor of the study, of a new
patient to be enrolled and randomized into the study. At
that time, the representative of the sponsor would assign
the next sequential patient number using a Random
Digital Table26 to the patient along with the patient’s
initials to drug A (pirfenidone arm) or drug B (placebo
arm) predetermined by the randomization table. The
medication starter package would then be labelled with
the number and patient’s initials according to the rando-
mization table and delivered only to Dr Walker who
acknowledged receiving the package by his signature on
an official form developed by the sponsor of the study.The effectiveness of the blinding was maintained by
strictly adhering to the following guidelines: 1) the bottles
containing the capsules were delivered only to Dr Walker,
and they were coded and could not be identified as to
whether they contained placebo or pirfenidone capsules;
2) the code was never in the possession of Dr Walker
and his staff as it was kept under security lock and key
at the Central Management Regulatory administration
office; 3) Dr Walker had no way of knowing who was
on placebo and who was on pirfenidone; 4) Dr Walker and
Table 1 Demographic and baseline clinical characteristics of the placebo versus pirfenidone groups
Baseline characteristics Placebo Pirfenidone
Female Male Female Male
Number of patients 14 4 18 7Age 49.29/1.79* 58.39/5.33** 45.99/2.49 52.39/4.40MS first symptoms (years ago) 13.39/3.74 16.89/6.76 11.79/1.78 13.49/2.40EDSS scores (unit) 6.119/0.19 6.39/0.48 6.149/0.14 6.439/0.34SNRS scores 66.99/3.6 70.59/4.17 62.49/2.67 54.19/4.52
Each value represents mean9/SEM.
*No significant difference (P �/0.05) between females in placebo and females in pirfenidone groups for any matching characteristics
(Student’s t -test).
**No significant difference (P �/0.05) between males in placebo and males in pirfenidone groups for any matching characteristics
(Student’s t -test).
Oral pirfenidone in secondary progressive multiple sclerosisJE Walker et al.
150
Multiple Sclerosis

a radiologist interpreted the MRIs independently; and5) Dr Walker did not know the name of the patients in theprocess of interpreting MRIs as the name of the patientswere blocked by opaque tape. The representative ofthe sponsor had access to the blinding code around theclock in case of an emergency for unblinding purposes.Dr Walker, the investigator of the study, and the patientsremained blinded throughout the entire period of the trial.These steps maintained the effectiveness of the blinding
procedure even though Dr Walker was responsible forevaluating the clinical status of the patients.
Schedule of observation The clinical visits for the historyand physical and neurological examinations of the pa-tients occurred at the baseline, and then at 1, 3, 6, 9 and 12months. The parameters for neurological evaluationsincluded: Scripps Neurological Rating Scale (SNRS)according to Sipe et al .27 and EDSS according to themodified criteria from Kurtzke.28 The MRI scan was doneat baseline, six and 12 months according to the procedure
described in our earlier papers.23,24 The numbers of newor enhancing lesions were determined by comparing MRIscans at six and 12 months with the baseline scans. Theradiologist and Dr Walker, the investigator of the study,were blinded to the group (placebo versus pirfenidone)and evaluated the MRIs independently.
Laboratory blood tests The blood tests including CBCand SMAC-20 (sodium, potassium, chloride, glucose,BUN, creatinine, calcium, phosphate, total protein, albu-min, bilirubin, AST, alkaline phosphatase) were per-
formed at baseline, six and 12 months after beginningtreatment.
Relapse A clinical relapse was defined as the appear-ance of new symptoms or worsening of an old existingsymptom, attributable to MS and accompanied by objec-tive worsening of neurological findings (SNRS). To bescored as a relapse, the alterations must have been severeas determined by an increase from baseline at least onepoint on two functional system scores or at least twopoints on one functional system score, and preceded by an
interval of disease stability or improvement. The worsen-ing must have lasted for at least 24 hours in the absence offever, and must have required short-term medicationswith oral prednisone.
Study medications The study medications were providedby Marnac, Inc., (Dallas, TX), the sponsor of the trial, ina form suitable for oral administration as follows:1) pirfenidone pure powder 400 mg without excipientswas encapsulated in a hard gel capsule; 2) placebocapsules containing inert white powder were also encap-
sulated in matching hard gel capsules. There were 50capsules in each dispensing bottle. The capsules contain-ing pirfenidone or placebo were prepared in compliancewith the FDA-approved Good Manufacturing Practices atthe Department of Veteran’s Affairs Cooperative StudiesProgram, School of Pharmacy, University of New MexicoHealth Sciences Center, Albuquerque, NM.
Dose regimen for administration Patients were initiallytitrated for each capsule preparation up to a maintenancedose over a period of 10�/14 days to assure adequatetolerance to oral drugs during the trial. During this period,each patient started with one capsule twice daily for twodays, increased to one capsule three times daily for twodays, four capsules daily for two days (one in the morning,one at noon and two in the evening), five capsules dailyfor two to four days (two capsules in the morning, onecapsule at noon, two capsules in the evening) followed upwith two capsules three times a day for a maximum of sixcapsules.
Patients were instructed to take capsules during mealsor with other food and swallow with a full glass of wateror other nonalcoholic beverage. An antacid, such as Tums,was given to counteract any gastric discomfort. A fewpatients dissolved the content of the capsule into a glass oforange juice and then swallowed. This measure was takento minimize the gastric discomfort of the capsules. Anydrowsiness was minimized with caffeine beverage, if itoccurred.
All patients had been off all disease-modifying therapy,including corticosteroids, for at least three months. Con-comitant medications known to induce skin rash wereavoided. The administration of any concomitant drugswas promptly recorded in the appropriate section of theCase Report Forms. All blinded coded pirfenidone andplacebo capsules were delivered only to Dr Jonathan E.Walker, the principal clinical investigator of the study, andhis signature was required to confirm all drug deliveries.
Endpoints and plan of treatment The enrolled patients atthe onset were studied in order to acquire the baselinedata for their documented degree of progression of thedisease and neurological status, CBC, differential, urineanalysis and an MRI of the brain. The neurologicalevaluation included: 1) vital signs (blood pressure, pulseand respiration rate); 2) classical neurological examina-tion; 3) SNRS score; and 4) EDSS score.
Evaluation and statistical considerations
The primary outcome This was based on inhibition of theprogression of disease as assessed by the SNRS scores atbaseline, one, three, six and 12 months. The secondaryoutcomes included: 1) incidence of relapse; 2) urinarybladder dysfunction; 3) EDSS scores; and 4) number ofnew and gadolinium-enhancing lesions on MRI brainscans at baseline, six and 12 months.
The safety profile This included pre-drug baseline his-tory and physical examinations followed by regularlyscheduled (baseline, six and 12 months) blood chemis-tries, blood cell counts and urine analyses.
The methods employed for testing the data for statisticalsignificance were approved by the IRB and accepted bythe FDA. All eligible patients who were enrolled in thetrial were included in the analysis of the data as mandatedby the intention-to-treat principles.29 The data for patientsin placebo and pirfenidone-treated groups are presented
Oral pirfenidone in secondary progressive multiple sclerosisJE Walker et al.
151
Multiple Sclerosis

as mean9/SEM. The SNRS scores at one, three, six and 12months for each group were compared with the baselinedata of the same group. Repeated Measures of ANOVAfollowed by Newman�/Keuls Multiple Comparison Testwas performed to analyse the statistical significance of theSNRS scores among the four groups of each arm of thestudy using SigmaStat for Windows Version 1, JandelScientific Corporation (San Rafel, CA). The differences inranks in the changed SNRS scores from the baseline dataof the individual patients between the pirfenidone andplacebo groups at one, three, six and 12 months were alsoanalysed for statistical significance using the Mann�/
Whitney Two-Sample Rank Test according to the proce-dure described by Zar.30 In addition, Student’s t -test andchi-square as appropriate were used for statistical analysisof data. A value of P B/0.05 was considered to be theminimum level for statistical significance.
Results
Reasons for drop outOut of the initial 43 patients with secondary progressiveMS who met the inclusion criteria, 18 were assigned atrandom to the placebo and 25 to the pirfenidone groups.The demographic and baseline clinical characteristicsof patients in placebo and pirfenidone groups are sum-marized in Table 1. There was no significant difference(P �/0.05) in any clinical parameter in females or malesbetween the placebo and pirfenidone groups. This pro-vides evidence that patients in placebo and pirfenidonegroups were well matched on all clinical parameters priorto starting treatment.
In the placebo group, seven patients dropped out of thestudy (39%), whereas in the pirfenidone group, ninepatients dropped out (36%). The time of drop out forpatients in the placebo group averaged 6.149/0.96 monthswith a range of one to nine months, whereas in thepirfenidone group, the average was 4.229/0.86 monthswith a range of one to eight months. There was nosignificant difference in the time of drop out betweenthe two groups. Seven patients dropped out only as aresult of continual marked progression of disease in theplacebo group. Other reasons for drop out in the placebogroup included supraventricular tachycardia (1), hepatitis(1) and colon surgery (1). In the pirfenidone group, thereasons for drop out (unrelated to drug therapy) includedcongestive heart failure (1), discontinuation of treatmentwithout notification (1), patient’s request to withdrawfrom the trial because of travelling distance (1), lack ofimprovement (1), generalized weakness (1) and progres-sion of disease in (1) patient. Three patients dropped outfrom the trial in the pirfenidone group due to drug-relatedadverse effects: nausea (1), weight loss and anorexia (1)and skin rash (1).
Laboratory testThe laboratory blood test results for electrolytes anddifferential white cell counts and urine analyses for both
groups were normal at baseline and at all subsequentintervals during the trial period.
Scripps Neurological Rating Scale
There was no statistically significant (P �/0.05) differencein mean SNRS score between the placebo and pirfenidonegroups when patients were initially assigned at random totheir respective arms of the study (Table 1). The improve-ment in the SNRS scores of all enrolled patients in theplacebo and pirfenidone groups at one, three, six and 12months was compared with their respective mean baselineSNRS scores according to the intention-to-treat principles.
The mean SNRS scores at one, three, six and 12 monthswere not significantly different (P �/0.05) from the base-line score of the patients on placebo (Table 2). Thisprobably indicates a mild placebo effect on SNRS scoresfor these patients. However, the patients taking pirfeni-done had significant (P B/0.05) increases (RMANOVA) inthe mean SNRS scores at one, three, six and 12 months ascompared to the mean baseline score of this group (Table2). The increases in the SNRS score indicate the effective-ness of pirfenidone therapy in reducing neurologicaldysfunction of patients suffering from advanced second-ary progressive MS. This effect was noted from one monthonward.
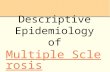
The changes in SNRS scores from the baseline scoresof individual patients in the pirfenidone and placebogroups at one month are summarized in Figure 1. Thechanged scores ranged from �/8 to �/22 units in patientson oral pirfenidone, whereas the changed scores inpatients on oral placebo ranged from �/5 to �/9 units.The Mann�/Whitney Two-Sample Rank Test revealedthat the rank in changed SNRS scores was significantly(P B/0.05) higher in patients on oral pirfenidone than thepatients on placebo.
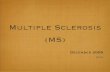
The changes in SNRS scores from the baseline scoresof individual patients in pirfenidone and placebo groupsat three months are summarized in Figure 2. The changedSNRS scores ranged from �/8 to �/29 units in patientson oral pirfenidone, whereas the changed scores inpatients on oral placebo ranged from �/9 to �/14 unitsat this time. The rank in changed SNRS scores wassignificantly (P B/0.05) higher in the patients on oralpirfenidone than the patients on oral placebo accordingto the Mann�/Whitney Two-Sample Rank Test.
Table 2 Scripps scores at baseline one, three, six and 12 months in
secondary progressive MS patients on oral placebo or pirfenidone
Months Placebo (n�/18),mean scores/units
Pirfenidone (n�/25),mean scores/units
Baseline 67.79/2.89 60.29/2.371 69.09/2.62 NS 65.59/2.30*3 71.69/3.07 NS 68.19/2.38*6 71.29/3.44 NS 69.19/2.80*
12 71.29/3.62 NS 68.39/2.75*
Each value represents mean9/SEM.
*Improvement in values is statistically significant (P B/0.05) from
baseline (RM ANOVA).
NS�/not significant.
Oral pirfenidone in secondary progressive multiple sclerosisJE Walker et al.
152
Multiple Sclerosis

The changes in SNRS scores from the baseline scoresof individual patients in pirfenidone and placebo groupsat six months are summarized in Figure 3. The changedSNRS scores in patients on oral pirfenidone ranged from�/13 to �/39 units, whereas the changed SNRS scores
in patients on oral placebo ranged from �/25 to �/19 units.The rank in changed SNRS scores was significantly(P B/0.05) higher in the patients on oral pirfenidone thanthe patients on oral placebo according to the Mann�/
Whitney Two-Sample Rank Test.The changes in SNRS scores from the baseline scores
of individual patients in pirfenidone and placebo groupsat 12 months are summarized in Figure 4. The changedSNRS scores in patients on oral pirfenidone ranged from�/13 to �/37 units, whereas the changed SNRS scoresin patients on oral placebo ranged from �/25 to �/19 units.The rank in changed SNRS scores was significantly(P B/0.05) higher in the patients on oral pirfenidonethan the patients on oral placebo according to theMann�/Whitney Two-Sample Rank Test.
RelapsesDuring the 12 months of the trial, 5/18 patients (27.8%)with advanced secondary progressive MS experiencedrelapses in the placebo group as compared to 2/25 patients(8.0%) in the pirfenidone group (Table 3). The relapseswere controlled by oral prednisone (100mg/daily) forseven days. The oral pirfenidone significantly (P B/0.04)suppressed the occurrence of relapses in the secondaryprogressive MS patients over the placebo.
Urinary bladder dysfunction
The effects of oral placebo or pirfenidone on urinarybladder dysfunction of patients with secondary progres-sive MS are summarized in Table 4. The bladder function
Pirfenidone1 Month
11
-8
0 03
11
3
13
6 4
22
0 0 1
-1
1012
4 3 3 50
12 10 9
-30
-20
-10
0
10
20
30
40
5 6 7 9 11 13 14 15 16 18 19 25 26 27 29 31 32 33 35 36 39 40 41 42 43
Patient Number
Ch
ang
es in
Scr
ipp
s S
core
Placebo1 Month
4
-4
0
-1
0 04
-3
0
7
-5 -4
4 2 38 9
0
-30
-20
-10
0
10
20
30
40
1 2 3 4 7 10 12 17 20 21 22 23 24 28 30 34 37 38
Patient Number
Ch
ang
es in
Scr
ipp
s S
core
s
Figure 1 Changes in SNRS scores from the baseline of the
individual patients on oral pirfenidone or placebo at one month.Rank in changed SNRS scores of patients in pirfenidone group
was significantly (PB/0.05) higher than patients on oral placebo
(Mann�/Whitney Two-Sample Rank Test).
Pirfenidone3 Month
11
-5-8
0 0
14
4
159
4
29
0
8
0
-1
21
127 7 7
1115
1216
9
-30
-20
-10
0
10
20
30
40
5 6 7 9 11 13 14 15 16 18 19 25 26 27 29 31 32 33 35 36 39 40 41 42 43
Patient Number
Ch
ang
es in
Scr
ipp
s S
core
Placebo3 Month
6 71
-9
60
8
-5
47
30
9
2 3
14 14
0
-30
-20
-10
0
10
20
30
40
1 2 3 4 7 10 12 17 20 21 22 23 24 28 30 34 37 38
Patient Number
Ch
ang
es in
Scr
ipp
s S
core
s
Figure 2 Changes in SNRS scores from the baseline of the
individual patients on oral pirfenidone or placebo at threemonths. Rank in changed SNRS scores of patients in pirfenidone
group was significantly (PB/0.05) higher than patients on oral
placebo (Mann�/Whitney Two-Sample Rank Test).
Pirfenidone6 Month
11
-3-8
0
9
16
2
17
94
39
0
13
-13-4
21
129
127 5
16
23
16
9
-30
-20
-10
0
10
20
30
40
5 6 7 9 11 13 14 15 16 18 19 25 26 27 29 31 32 33 35 36 39 40 41 42 43
Patient Number
Ch
ang
es in
Scr
ipp
s S
core
Placebo6 Month
6 8 8
-25
10
0
9
-5
6 71
-4
10
-2
3
12
19
0
-30
-20
-10
0
10
20
30
40
1 2 3 4 7 10 12 17 20 21 22 23 24 28 30 34 37 38
Patient Number
Ch
ang
es in
Scr
ipp
s S
core
s
Figure 3 Changes in SNRS scores from the baseline of the
individual patients on oral pirfenidone or placebo at six months.
Rank in changed SNRS scores of patients in pirfenidone group
was significantly (PB/0.05) higher than patients on oral placebo(Mann�/Whitney Two-Sample Rank Test).
Oral pirfenidone in secondary progressive multiple sclerosisJE Walker et al.
153
Multiple Sclerosis

in four (4/18) patients (22.2%) on placebo underwent
deterioration during the trial period. For example, two
patients who had normal bladder function at the baseline
developed a moderate degree of bladder dysfunction in
one month and remained that way for the duration of the
study, whereas a moderate degree of bladder dysfunction
in two patients at baseline progressed into severe dysfunc-
tion in six months and continued at that level for the
entire 12 months of the trial. In contrast, none of
the patients (0/25) on oral pirfenidone experienced any
further deterioration of bladder function from the base-
line. The absence of any further deterioration in urinary
bladder function in patients on oral pirfenidone was in
marked contrast to patients on placebo who developed
significant (P B/0.007) deterioration during the trial
period. The bladder function in patients on placebo was
improved in 16.7% patients (3/18) who had severe
dysfunction at the baseline in contrast to an improvementin 40% patients (10/25) in the pirfenidone group withinsix months followed by restoration of normal bladderfunction during the trial period. Thus, patients withsecondary progressive MS on oral pirfenidone showeda significant (P B/0.05) improvement in urinary bladderdysfunction as compared to the patients on placebo(Table 4).
EDSS scoresThe EDSS scores of patients suffering from secondaryprogressive MS on placebo or pirfenidone are summarizedin Table 5. Patients on placebo trended to deteriorate,while patients on pirfenidone appeared to stabilize. Thedifference was not statistically significant however.
MRI evaluationsThe MRI evaluations of secondary progressive MS patientson placebo and pirfenidone were carried out prior tostarting treatment (baseline) and at six and 12 months oftreatment. Total number of lesions present in the whitematter, periventricular and subcortical white matter werequantified using MRI scan. Also quantified were enhan-cing lesions in these areas. There were no statisticalsignificant differences in the number of lesions amongthe baseline, six and 12 months either in placebo orpirfenidone group as analysed by RMANOVA (data notshown). Similarly, there were no statistically significantdifferences in the baselines, six or 12 months betweenplacebo and pirfenidone groups when compared at thecorresponding times by unpaired Student’s t -test.
Pirfenidone12 Month
11
-3-8
0
9 9
2
17
94
37
0
12
-13 -4
21
12
0
15
5 6
16
23
129
-30
-20
-10
0
10
20
30
40
5 6 7 9 11 13 14 15 16 18 19 25 26 27 29 31 32 33 35 36 39 40 41 42 43
Patient Number
Cha
nges
in S
crip
ps
Sco
re
Placebo12 Month
69 11
-25
12
0
9
-5
8 71
-6
11
-8
3
12
19
0
-30
-20
-10
0
10
20
30
40
1 2 3 4 7 10 12 17 20 21 22 23 24 28 30 34 37 38
Patient Number
Cha
nge
s in
Scr
ipp
s S
core
s
Figure 4 Changes in SNRS scores from the baseline of the
individual patients on oral pirfenidone or placebo at 12 months.
Rank in changed SNRS scores of patients in pirfenidone group
was significantly (PB/0.05) higher than patients on oral placebo(Mann�/Whitney Two-Sample Rank Test).
Table 3 Incidence of relapse of secondary progressive MS
patients on oral placebo or pirfenidone during 12 months of
clinical trial
Treatment Number ofpatients
Numberexperiencedrelapse
% patientsexperiencedrelapse
Placebo 18 5 27.8Pirfenidone 25 2 8.0*
*Statistically significant lower relapse rate (P B/0.04) by oral
pirfenidone (chi-square test).
Table 4 Effects of oral placebo or pirfenidone on urinary bladder
dysfunction in secondary progressive MS patients
Category Placebo (n�/18) Pirfenidone (n�/25)
Deterioration 4/18*�/22.2% 0/25�/0%Improvement 3/18�/16.7% 10/25**�/40%No effect 11/18�/61.10% 15/25�/60%
*Statistically significant deterioration in bladder function
(P B/0.007) compared to pirfenidone by chi-square test.
**Statistically significant improvement in bladder function
(P B/0.05) over placebo by chi-square test.
Table 5 EDSS scores at baseline one, three, six and 12 months in
secondary progressive MS patients on placebo or pirfenidone
Months EDSS scores* (mean9/SEM)
Placebo (n�/18) Pirfenidone (n�/25)
Baseline 6.149/0.18 6.229/0.141 6.149/0.18 6.229/0.143 6.089/0.20 6.209/0.146 6.089/0.24 6.209/0.14
12 5.979/0.27 6.169/0.16
*There is no significant difference between baseline and any
evaluation time of either placebo or pirfenidone group, though
there was a trend to worsening in the placebo group, whereas the
pirfenidone group trended toward stabilization.
Oral pirfenidone in secondary progressive multiple sclerosisJE Walker et al.
154
Multiple Sclerosis

Discussion
MS is a chronic, autoimmune inflammatory disorder ofthe central nervous system, characterized by a spatial andtemporal dissemination of pathological processes thataffect primarily the white matter in the central nervoussystem and thereby cause both physical and psychologicaldisability. Although the aetiology of MS is not clearlyunderstood, there is abundant evidence of the involve-ment of TNF-alpha in the demyelination that is consid-ered to be a major component in the pathogenesis ofMS.5�9 There is also evidence suggesting the involvementof oxidative stress in the pathogenesis of this disease.31,32
Pirfenidone, 5-methyl-1-phenyl-2-(H) pyridone, is anorally administered small molecule. Its beneficial effectsfor treatment of patients with advanced secondary pro-gressive MS have been reported in two independent openlabel trials23,24 and in the phase II double-blind rando-mized trial reported in the present study. This was shownby finding that patients on oral pirfenidone had signifi-cantly improved SNRS scores at one, three, six and 12months as compared to the baseline score of this group.However, this was not found for patients on placebo astheir SNRS scores at one, three, six and 12 months wereinsignificantly increased from the baseline scores. More-over, the patients on oral pirfenidone had significantlyhigher rank in improved SNRS scores from their indivi-dual baseline scores than the patients on placebo at allcorresponding times as indicated by the Mann�/WhitneyTwo-Sample Rank Test.
The second line of evidence for beneficial effects ofpirfenidone in secondary progressive MS was reflected bythe fact that only one patient in this group dropped outfrom the trial in contrast to seven patients in the placebogroup who dropped out as a consequence of the progres-sive worsening of their disease. The third line of evidencewas provided by a dramatic improvement in urinarybladder function of several patients in the pirfenidonegroup. Patients with MS have frequent problems withurinary bladder dysfunction (urgency, frequency and urgeincontinence due to bladder overactivity and/or incom-plete emptying) and the same type of dysfunction is foundin 75% of patients.33 There was a lack (0.0%) of anyfurther deterioration in the bladder function and a markedimprovement in the bladder function in 40% patients onoral pirfenidone as compared to 16.7% improvement and22.2% deterioration in the bladder function in patients onoral placebo during the trial period. Fourth, a significantreduction occurred in the number of patients experiencingrelapses on oral pirfenidone. For instance, 27.8% patientswith secondary progressive MS experienced relapseswhile on oral placebo as compared to only 8.0% patientson oral pirfenidone during the trial period.
EDSS scores of secondary progressive MS patientstrended to stabilize on pirfenidone whereas this indextrended to deteriorate in patients on placebo from thebaseline at one, three, six and 12 months. However, thedifference was not significant between the two groups.There were no significant differences in total MRI lesionsbetween the pirfenidone and placebo groups when
compared either at the corresponding time intervals or at
any time of evaluation to the baseline of each arm of the
study. It is not uncommon to find a discrepancy between
the clinical observations and some indexes used to
monitor the progression of MS. For instance, a reduction
in relapses without significant differences in the EDSS
score or in the development of active MRI lesions has been
reported in a controlled study.34 Although MRI is fre-
quently applied for diagnostic purposes, T2-weighted
lesions lack histopathologic specificity and thus measures
of T2 lesion load correlate poorly with the degree of
clinical disability.35,36 In fact, the use of MRI as a surrogate
outcome measure was examined by an international group
of investigators with expertise in clinical aspect of MS and
experimental therapeutics. The group agreed that MRI
does not represent a validated surrogate in any clinical
form of MS and clinical trials using MRI as a primary
outcome measure may fail to fully identify the effects of
therapy on clinical measures.37,38
The axonal injury in response to an excess production
of TNF-alpha by activated oligodendrocytes, macrophages
and microglia occurs in the pathogenic process of MS5�9
as well as in other degenerative and inflammatory diseases
of the neurons.39,40 As an excess production of TNF-alpha
plays a pivotal role in the pathogenesis of MS, any
therapeutic strategies that target TNF-alpha may have
potentially therapeutic benefits for management of MS.
Previous studies to treat MS with TNF-alpha neutralizing
antibody and TNF-receptor-blocking agents may have
failed because of their relatively poor ability to decrease
TNF-alpha synthesis, weaker blockade of TNF-alpha
receptors and/or poor accessibility to the CNS.41,42
The beneficial effects of pirfenidone in secondary
progressive MS patients as reported in this double-blind,
randomized, controlled study may primarily be due to its
ability to minimize the demyelination by inhibiting the
production and/or action of TNF-alpha as demonstrated
by several investigators both in vitro and in vivo.20�22 It is
probable that pirfenidone not only inhibits the production
and action of TNF-alpha in peripheral organs but also in
the central nervous system as well, as it is uniformly
distributed in body water and crosses the blood�/brain
barrier easily.43 Based on the finding of the authors of the
current paper that pirfenidone markedly inhibited the
porcine myeloperoxidase (pMPO)-induced increased pro-
duction of TNF-alpha by astrocyte cells of human origin
(unpublished), it is conceivable that pirfenidone may also
reduce the TNF-alpha-induced pathological proliferation
of astrocytes and help re-establish normal astrocyte
support of neurons and neuronal transmission.2,22,44
Other TNF-alpha-based therapies for MS were proven to
be not efficacious because they were weak inhibitors of
TNF-alpha synthesis and TNF-alpha receptor blockers.
However, besides well documented anti-TNF-alpha ac-
tion, by strongly inhibiting TNF-alpha synthesis and
blocking TNF-alpha receptors, pirfenidone has other
pharmacological effects, which could provide added
beneficial effects against secondary progressive MS. These
include: a) ability of pirfenidone to scavenge reactive
oxygen species (ROS)45,46 responsible for the oxidative
Oral pirfenidone in secondary progressive multiple sclerosisJE Walker et al.
155
Multiple Sclerosis

stress implicated in the pathogenesis of MS;31,32 b) ability
of pirfenidone to block the production of other proin-
flammatory cytokines21,47 secreted by the dendritic cells
in patient with MS;48 c) ability of pirfenidone to attenuate
inflammation49 involved in the pathogenesis of MS;50 d)
ability of pirfenidone to block the production of inter-
cellular adhesion molecues51 implicated in the MS
disease activity;15,16 and ability of pirfenidone to block
the synthesis of nitric oxide47 implicated in pathogenesis
of MS.19
Transcriptional activation of specific inflammatory
cytokine genes such as IL-1alpha, IL-6, IL-8 and TNF-
alpha is mediated by NF-kB activation in various cell
types under a wide range of conditions.52 Binding sites for
the NF-kB family of transcription factors are found in the
promoter and enhancer regions of a multitude of genes
including cytokines, chemokines and growth factors that
are involved in the inflammatory response. It has been
shown that activation and translocation of NF-kB from
cytoplasm into nucleus where it binds to DNA occurred invitro53 and in vivo54 in response to elevated levels of ROS
prior to transcriptional activation of inflammatory cyto-
kine genes and their gene products including TNF-alpha
in these studies. As NF-kB is an oxidant-sensitive tran-
scription factor,55 it is not surprising that bleomycin56,57
(generator of ROS)-induced activation of this transcription
factor was blocked by pirfenidone,58 a known scavenger
of ROS.45,46 This resulted in downregulation of the
expression of the inflammatory cytokine genes including
TNF-alpha and IL-1 genes and subsequently the produc-
tion of TNF-alpha and IL-1 as demonstrated recently
in vivo.47 Thus the blockade of activation of NF-kB by
pirfenidone in the CNS may conceivably be one of the
mechanisms for the inhibitory effects of pirfenidone on
synthesis of proinflammatory cytokines, ICAM-1 and NO
and this would arrest the ongoing inflammation and
demyelination which play a major role in the pathogenesis
of secondary progressive MS.The FDA has approved four disease-modifying thera-
pies for patients with relapsing�/remitting MS: interferon
beta-1b,59 two interferon beta-1a products60 and glatiramer
acetate.61 These drugs reduce the rate of clinical relapses
and progression of the disease by modulating the immune
system. Although interferon beta-1b has been approved for
use in secondary progressive MS in Europe and Canada, in
two recently completed phase III trials, it was found that
treatment with interferon-1b did not slow the progression
of disability.62,63 It does not always slow the progression
of axonal injury in MS.64
The FDA has recently approved mitoxantrone, a cancer
chemotherapeutic agent, for intravenous treatment of
patients with secondary progressive MS.65 However,
17.8% of the patients on mitoxantrone therapy had a
significant decline in left ventricular ejection fraction,
an index of mitoxantrone-induced cardiac toxicity as
revealed in a recent clinical trial.66 In fact, it was
suggested by the authors of this paper that ‘more stringent
cardiac monitoring guidelines than current Food and Drug
Administration (FDA) recommendations be used to
avert potential cardiac complications in SPMS patients
on Mitoxantrone.’ Pirfenidone has much less toxicityand risk than mitoxantrone and is orally effective andaffordable.
Although the encouraging results of this double-blind,randomized controlled study are based on a relativelysmall number of patients (43) with advanced secondaryprogressive MS, it is similar to the study reported bySipe et al.67 in evaluating the effect of cladribine intreatment of a small number of patients (48) with chronicprogressive MS. The beneficial effects of pirfenidonein two independent open label studies in advancedsecondary progressive MS patients, along with thisdouble-blind study, provide convincing evidence for anoteworthy beneficial effect of pirfenidone for the treat-ment of patients with advanced secondary progressiveMS. A larger multicentre, double-blind, randomized,controlled study could substantiate this beneficial effectin treatment of this debilitating disease.
AcknowledgementsThe oral pirfenidone and placebo capsules were providedby Marnac, Inc., Dallas, Texas. In addition, Marnac, Inc.provided the financial support to conduct this clinicaltrial. Dr Nancy A Cox, M.D., Ph.D., Medical Director andMs Judy A Lexvold, Director of Regulatory Affairs ofMarnac, Inc., assisted in the design and monitoring of thestudy. The authors are thankful to Mr Robert H Lexvold,Executive Vice President of Marnac, Inc., for reviewingand Ms Marcy L Raykowski for typing the manuscript.
Disclosure
Dr Jonathan E Walker, M.D., the investigator of this study,has been a paid consultant of Marnac, Inc. for a number ofyears. He does not hold stock or other equity in thecompany.
References
1 Anderson DW, Ellenberg JH, Leventhal CM, Reingold SC,
Rodriguez M, Silberberg DH. Revised estimate of the preva-
lence of multiple sclerosis in the United States. Ann Neurol1992; 31: 333�/36.
2 Compston A. Genetic epidemiology of multiple sclerosis.
J Neurol Neurosurg Psychiatry 1997; 62: 553�/61.
3 Sadovnick AD, Ebers GC. Epidemiology of multiple sclerosis:
a critical over-view. Can J Neurol Sci 1993; 20: 17�/29.
4 Allen I, Brakin B. Pathogenesis of multiple sclerosis-the
immune diathesis and the role of viruses. J Neuropathol ExpNeurol 1993; 52: 95�/105.
5 Merril JE, Benveniste EN. Cytokines in inflammatory brain
lesions: helpful and harmful. Trends Neurosci 1996; 19:
331�/38.
6 Van Oosten BW, Barkhof F, Scholten PE, von Blomberg BM,
Ader HJ, Polman CH. Increased production of tumor necrosis
factor alpha and not of interferon-gamma preceding disease
activity in patients with multiple sclerosis. Arch Neurol 1998;
55: 793�/98.
Oral pirfenidone in secondary progressive multiple sclerosisJE Walker et al.
156
Multiple Sclerosis

7 Gayo A, Mozo L, Suarez A, Tunon A, Lahoz C, Gutierrez C.
Interferon beta-1b treatment modulates TNF-alpha and IFN-
gamma spontaneous gene expression in MS. Neurology 1999;
52: 1764�/70.
8 Hofman FM, Hinton DR, Johnson K, Merrill JE. Tumor necrosis
factor identified in multiple sclerosis brain. J Exp Med 1989;
170: 607�/12.
9 Akassoglou K, Bauer J, Kassiotis G, Lassman H, Kollias G,
Probert L. Transgenic model of TNF-induced demyelination.
Adv Exp Med Biol 1999; 468: 245�/59.
10 Robbins DS, Shirazi Y, Drysdale BE, Lieberman A, Shin HS,
Shin ML. Production of cytotoxic factor for oligodendrocytes
by stimulated astrocytes. J Immunol 1987; 139: 2593�/600.
11 Sharief MK, Hentges R. Association between tumor necrosis
factor-alpha and disease progression in patients with multiple
sclerosis. N Engl J Med 1991; 325: 467�/72.
12 Wong D, Dorovini-Zis K. Upregulation of intercellular adhe-
sion molecule-1 (ICAM-1) expression in primary cultures of
human brain microvessel endothelial cells by cytokines and
lipopolysaccharide. J Neuroimmunol 1992; 39: 11�/22.
13 Satoh JJ, Kastruoff LF, Kim SU. Cytokine-induced expression
of intercellular adhesion molecule-1 (ICAM-1) in cultured
human oligodendrocytes and astrocytes. J Neuropathol Exp
Neurol 1991; 50: 215�/26.
14 Barten DM, Ruddle NH. Vascular cell adhesion molecule-1
modulation by tumor necrosis factor in experimental allergic
encephalomyelitis. J Neuroimmunol 1994; 51: 123�/33.
15 Cannella B, Raine CS. The adhesion molecule and cytokine
profile of multiple sclerosis lesions. Ann Neurol 1995; 37:
424�/35.
16 Sharief MK, Noori MA, Ciardi M, Cirelli A, Thompson EJ.
Increased levels of circulating ICAM-1 in serum and cere-
brospinal fluid of patients with active multiple sclerosis.
Correlation with TNF-alpha and blood-brain barrier damage.
J Neuroimmunol 1993; 43: 15�/22.
17 Lowenstein CJ, Snyder SH. Nitric oxide, a novel biologic
messenger [Review]. Cell 1992; 70: 705�/707.
18 Choi DW. Nitric oxide; foe or friend to the injured brain?
[Comment]. [Review]. Proc Natl Acad Sci USA 1993; 90:
9741�/43. Comment on: Proc Natl Acad Sci USA 1993; 90:
9808�/12.
19 De Groot CJA, Ruuls SR, Theeuwes JWM, Dijkstra CD, Van
der Valk, P. Immunocytochemical characterization of the
expression of inducible and constitutive isoforms of nitric
oxide synthase in demyelinating multiple sclerosis lesions.
J Neuropathol Exp Neurol 1997; 56: 10�/20.
20 Cain WC, Stuart RW, Lefkowitz DL, Starnes JD, Margolin SB.
Inhibition of tumor necrosis factor and subsequent endotoxin
shock by pirfenidone. Int J Immunopharmacol 1998; 20:
685�/95.
21 Hale ML, Margolin SB, Krakauer T, Roy CJ, Stiles BG.
Pirfenidone blocks the in vitro and in vivo effects of
staphylococcal enterotoxin B. Infect Immunity 2002; 70:
2989�/94.
22 Nakazato H, Oku H, Yamane S, Tsuruta Y, Suzuki R. A novel
anti-fibrotic agent pirfenidone suppresses tumor necrosis
factor-alpha at the translational level. Eur J Pharmacol 2002;
446: 177�/85.
23 Walker JE, Margolin SB. Pirfenidone for chronic progressive
multiple sclerosis. Mult Scler 2001; 7: 305�/12.
24 Bowen JD, Maravilla K, Margolin SB. Open-label study of
pirfenidone in patients with progressive form of multiple
sclerosis. Mult Scler 2003; 9: 280�/83.
25 Poser CM, Paty DW, Scheinberg L, McDonald WI, Davis FA,
Ebers GC et al . New diagnostic criteria for multiple sclerosis:
guidelines for research protocol. Ann Neurol 1983; 13:
227�/31.
26 Goldstein A. Biostatistics: an introductory text . New York, NY:
Macmillan, 1964: 234.
27 Sipe JC, Knobler RL, Braheny SL, Rice GP, Panitch HS,
Oldstone MB. A neurologic rating scale (NRS) for use in
multiple sclerosis. Neurol 1984; 34: 1368�/72.
28 Kurtzke J. Rating neurological impairment in multiple sclero-
sis: an expanded disability status scale (EDSS). Neurology
1983; 33: 1444�/52.
29 Lang TA, Secic M. How to report statistics in medicine:
annotated guidelines for authors, editors, and reviewers.
Philadelphia, PA: ACP Medical Writing and Communication,
American College of Physicians, 1997: 18�/21.
30 Zar JH. Biostatistical analysis , fourth edition. Upper Saddle
River, NJ: Prentice-Hall, Inc., 1999: 146�/48.
31 Ruuls SR, Bauer J, Sontrop K, Huitinga I, ‘t Hart BA, Dijkstra
CD. Reactive oxygen species are involved in pathogenesis of
experimental allergic encephalomyelitis in Lewis rats. J
Neuroimmunol 1995; 56: 207�/17.
32 Toshniwal PK, Zarling EJ. Evidence for increased lipid
peroxidation in multiple sclerosis. Neurochem Res 1992; 17:
205�/207.
33 Das Gupta R, Fowler CJ. Bladder, bowel and sexual dysfunc-
tion in multiple sclerosis. Management strategies. Drugs 2003;
63: 153�/66.
34 Bastianello S, Pozzilli C, D’Andrea F, Millefiorini E, Trojano
M, Morino S et al . A controlled trial of mitoxantrone in
multiple sclerosis: serial MRI evaluation at one year. Can J
Neurol Sci 1994; 21: 266�/70.
35 Barkhof F. The clinico-radiological paradox in multiple
sclerosis revisited. Curr Opin Neurol 2002; 15: 239�/45; 9:
1�/14.
36 Raeke MK. Multiple sclerosis and magnetic resonance ima-
ging: Advancement in linking the pictures with the progres-
sion. Arch Neurol 2001; 58: 35�/36.
37 Miller DH, Grossman RI, Reingold SC, McFarland HF. The role
of magnetic resonance techniques in understanding and
managing multiple sclerosis. Brain 1998; 121: 3�/24.
38 McFarland HF, Barkhof F, Antel J, Miller DH. The role of MRI
as a surrogate outcome measure in multiple sclerosis. Mult
Scler 2002; 8: 40�/51.
39 Shamash S, Reichert F, Rotshenker S. The cytokine network of
Wallerian degeneration: tumor necrosis factor-a, and inter-
leukin-1b. J Neurol Sci 2002; 22: 3052�/60.
40 Smith ME, van der Maesen K, Somera FP. Macrophage and
microglial response to cytokines in vitro : phagocytic activity,
proteolytic enzyme release, and free radical production. J
Neurosci Res 1998; 54: 68�/78.
41 Myers LW, Ellison GW, Merrill JE, El Hajjar A, St Pierre B,
Hijazin M et al . Pentoxyfylline is not a promising treatment
for multiple sclerosis in progression phase. Neurology 1998;
51: 1483�/86.
42 The Lenercept Multiple Sclerosis group and the University of
British Columbia MS/MRI analysis group. TNF neutralization
in MS: results of a randomized, placebo-controlled multi-
center study. Neurology 1999: 53: 457�/65.
43 Giri SN, Wang Q, Xie Y, Largo J, Morin D, Margolin SB et al .
Pharmacokinetics and metabolism of a novel antifibrotic drug
pirfenidone, in mice following intravenous administration.
Biopharmaceut Drug Disp 2002; 23: 203�/11.
44 Beutler B, Bazzoni F. TNF, apoptosis and autoimmunity: a
common thread? Blood Cells Mol Dis 1998; 24: 216�/30.
45 Giri SN, Leonard S, Shi X, Margolin SB, Vallyathan V. Effects
of pirfenidone on the generation of reactive oxygen species in
vitro. J Environ Pathol Toxicol Oncol 1999; 18: 169�/77.
Oral pirfenidone in secondary progressive multiple sclerosisJE Walker et al.
157
Multiple Sclerosis

46 Misra HP, Rabideau C. Pirfenidone inhibits NADPH-depen-
dent microsomal lipid peroxidation and scavenges hydroxyl
radicals. Mol Cell Biochem 2000; 204: 119�/126.
47 Iyer SN, Du X, Norris C, Margolin SB, Giri SN. Effects of
pirfenidone on inflammatory and anti-inflammatory cyto-
kines, CD4 and CD8 T-cells and nitric oxide levels in the
bronchoalveolar lavage fluid in bleomycin mouse model of
pulmonary fibrosis. Am J Respir Crit Care Med 2003; 167: 621.
48 Huang YM, Xiao BG, Ozenci V, Kouwenhoven M, Teleshova
N, Fredrik-Link H. Multiple sclerosis is associated with high
levels of circulating dendritic cells secreting pro-inflammatory
cytokines. J Neuroimmunol 1999; 99: 82�/90.
49 Iyer SN, Hyde DM, Giri SN. Anti-inflammatory effects of
pirfenidone in the bleomycin�/hamster model of lung inflam-
mation. Inflammation 2000; 24: 477�/91.
50 Coles AJ, Wing MG, Molyneux P, Paolillo A, Davie CM,
Hale G et al . Monoclonal antibody treatment exposes three
mechanisms underlying the clinical course of multiple
sclerosis. Ann Neurol 1999; 46: 296�/304.
51 Kaneko M, Inoue H, Nakazawa R, Azuma N, Suzuki M,
Yamauchi S et al . Pirfenidone induces intercellular adhesion
molecule-1 (ICAM-1) down regulation on cultured human
synovial fibroblasts. Clin Exp Immunol 1998; 113: 72�/76.
52 Bauerle PA, Henkel T. Function and activation of NF-kappa B
in the immune system. Annu Rev Immunol 1994; 12: 141�/79.
53 Brennan P, O’Neil LAJ. Effects of oxidants and antioxidants on
nuclear factor kappa B activation in three different cell lines.
Biochim Biophys Acta 1995; 1260: 167�/75.
54 Gurujeyalakshmi G, Wang Y, Giri SN. Taurine and niacin
block lung injury and fibrosis by down-regulating bleomycin-
induced activation of transcription nuclear factor-kB in mice.
J Pharmacol Exp Ther 2000; 293: 82�/90.
55 Schreck R, Albermann K, Bauerle PA. Nuclear factor kappa B:
an oxidative stress-responsive transcription factor of eukar-
yotic cells (a review). Free Radic Res Commun 1992; 17: 221�/
37.
56 Caspary WJ, Lanzo DA, Niziak C. Effect of deoxyribonucleic
acid on the production of reduced oxygen by bleomycin and
iron. Biochemistry 1982; 21: 334�/38.
57 Beckman JS, Beckman TW, Chen J, Marshall PA, Freeman BA.
Apparent hydroxyl radical production by peroxynitrite: im-
plications for endothelial injury from nitric oxide and super-
oxide. Proc Natl Acad Sci USA 1990; 87: 1620�/24.
58 Iyer SN, Du X, Margolin SB, Giri SN. Profiling the effects
of pirfenidone on a variety of transcription factors and signal
transduction pathways in the bleomycin mouse model
of pulmonary fibrosis. Am J Respir Crit Care Med 2003; 167:
804.
59 The IFNB Multiple Sclerosis Study Group. Interferon-1b is
effective in relapsing�/remitting multiple sclerosis. 1. Clinical
results of a multicenter, randomized, double-blind, placebo,
controlled trial. Neurology 1993; 43: 655�/61.
60 Jacobs LD, Beck RW, Simon JH, Kinkel RP, Brownscheidle CM,
Murray TJ et al . Intramuscular interferon beta-1a for disease
progression in relapsing multiple sclerosis. The Multiple
Sclerosis Collaborative Research Group (MSCRG). Ann Neurol
1996; 39: 285�/94.
61 Comi G, Filippi M, Wolinsky JS. European/Canadian multi-
center, double-blind, randomized, placebo-controlled study of
the effects of glatiramer acetate on magnetic resonance
imaging-measured disease activity and burden in patients
with relapsing multiple sclerosis. Ann Neurol 2001; 49:
290�/97.
62 Paty D. Results of the 3-year, double-blind, placebo-controlled
study of interferon beta-1a (Rebif) in secondary progressive
MS. Presented at the Ninth Annual Meeting of the European
Neurological Society, Milan, Italy, June 5�/9, 1999.
63 Hugh R, SPECTRIMS Group. ‘Relapsing’ versus ‘nonrelapsing’
SPMS: different prognosis and response to interferon therapy
in the SPECTRUM study. Neurology 2000; 54: A233 abstract.
64 Parry A, Corckill R, Blamire AM, Palace J, Narayanan S,
Arnold D et al . Beta-interferon treatment does not always slow
the progression of axonal injury in multiple sclerosis. J Neurol
2003; 250: 171�/78.
65 Hartung HP, Gonsette R, Konig N, Kwiecinski H, Guseo A,
Morrissey SP et al . Mitoxantrone in progressive multiple
sclerosis: a placebo-controlled, double-blind, randomized,
multicenter trail. Lancet 2002; 360: 2018�/25.
66 Avasarala JR, Cross AH, Clifford DB, Singer BA, Siegel BA,
Abbey EE. Rapid onset mitoxantrone-induced cardiotoxicity
in secondary progressive multiple sclerosis. Mult Scler 2003;
9: 59�/62.
67 Sipe JC, Romine JS, Koziol JA, McMillan R, Zyroff J, Beutler E.
Cladribine in treatment of chronic progressive multiple
sclerosis. Lancet 1994; 344: 9�/13.
Oral pirfenidone in secondary progressive multiple sclerosisJE Walker et al.
158
Multiple Sclerosis