OBGYN Review File (Final) References • Doctors’ slides and notes • Kaplan notes • 435 teamwork • meded video Done by • Allulu Alsulayhim • Ebtisam Almutairi • Haifa Alwael • Jawaher Abanumy • Laila Mathkour • Nada Aldakheel • Rawan AlQahtani

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
OBGYNReviewFile(Final)
References
• Doctors’slidesandnotes• Kaplannotes• 435teamwork• mededvideo
Doneby• AlluluAlsulayhim• EbtisamAlmutairi• HaifaAlwael• JawaherAbanumy• LailaMathkour• NadaAldakheel• RawanAlQahtani
Anatomyoffemalepelvic
FemaleExternalGenitalia(vulva)Bartholinglands• liesoneachsideofthevagina,intheposteriorlowerthird1/3oftheintroitus.• Secretemucus–alkaline• Bartholincyst:whentheorificeoftheBartholinductbecomesobstructed.Management
:isconservativeunlesspressuresymptomsoccurduetosize.• Bartholinabscess:itmayoccurduetoinfection(mostlycausedbyE.coliandanaerobic
Bacteroidesspecies,andseldomduetogonococcus).Management:OutpatienttreatmentisI&DwithplacementofaWordcatheterunderlocalanesthesia
InternalreproductiveOrgansVagina• Invaginaonlyknowtheepitheliumandacidity.• Thecoveringepitheliumofvaginaisnon-keratinizedsquamousepithelium,it'stough
whichleadtotheacidity• Thevaginaisacidic.IthaslowPH=4.5,soit'sverydifficulttogetbacterialinfections.Supportsofcervixanduterus• Cardinalligaments:ifthisligamentisaffectedthenitwillleadtouterineprolapse• Pubocervicalligaments• UterosacralligamentsEpisiotomyIndications:• fetalweightgreaterthan4kg• operativedelivery• shoulderdystocia• CrowningoffetalheadFetalCirculation• Theumbilicalvein,carryingoxygenatedbloodfromtheplacentatothefetalbodythroughthe
ductusvenosus,whichdirectlyenterstheinferiorvenacava• IVC→cristadividens→rightatrium→foramenovale→leftatrium→leftventricle→
ascendingaorta→brain,heartandupperlimbs• SVC+IVC→rightventricle→ductusarteriosus→descendingaorta→visceraandlowerlimbs• Ductusarteriosus:shuntsmildlyoxygenatedbloodfrompulmonaryarterytodescendingaorta• Ductusvenosus:shuntshighlyoxygenatedbloodfromumbilicalveintotheIVC,sothisstructure
carriesoxygentofetalorgans)
EmbryologyoftheFemaleGenitalOrgan• Gonads:Thegonadsdevelopfromthemesotheliumonthegenitalridge• Uterus&FallopianTubes:FusionofthetwoPMNducts(mullerianducts)• Vagina:Theupper2/3ofthevaginaformedbymulleriantubercle.Thelower1/3formedby
urogenitalsinus
CongenitalMalformationsoftheFemaleGenitalTract• 45XOembryotheovariesdevelopbutundergoatresia→streakovaries• MullerianAgenesis:Failureofmullerianductdevelopment→absenceoftheuppervagina,
cervixanduterus.ovariesarepresentbecauseovariesdon’tdevelopfromMullerianducts)IntersexualityCongenitalAdrenalHyperplasia(CAH):Deficienciesofvariousenzymesrequiredforcortisol&aldosteronebiosynthesis(21-hydroxylase).femalemaypresentatbirthwithambiguousgenitalia.Youwillfind17-α-hydroxyprogesterone↑.Tx:Cortisol.
Physiologyofmenstrualcycle
MenstrualcycleoccurswiththematurationoftheHypothalamicpituitaryovarianaxis.Thehormonesproducedincludegonadotropin-releasinghormone(GnRH)fromthehypothalamus,whichstimulatesfollicle-stimulatinghormone(FSH)andluteinizinghormone(LH)fromtheanteriorpituitary,whichstimulatesestrogenandprogesteronefromtheovarianfollicle.
• Ovary:functional&morphologicchangesresultinginfollicularmaturation,ovulationandcorpusluteumformation.
• Endometrium:functionalandmorphologicchanges,eithertoprepareitforconceptionorsheddingofthemenstrualendometrium.
• FSH:stimulatesthegrowthofgranulosacellsandinducesthearomataseenzymethatconvertsandrogenstoestrogens.
• LH:stimulatestheproductionofandrogensbythethecacells,whichthengetconvertedtoestrogensinthegranulosacellsbythearomataseenzyme.TheLHsurge,stimulatessynthesisofprostaglandinstoenhancefollicleruptureandovulation.LHincreasesinthepre-ovulatoryperiod.
Phasesofmenstrualcycle
Menstrualphase Duetostrongvasoconstrictionandproteolyticactivity,functionalstratumofendometrialtissuediesandisdischargedduringmenstrualbleeding
Follicularphase Duetotheriseoffolliclestimulatinghormone(FSH)duringthefirstdaysofthecycle,severalovarianfolliclesarestimulated
Ovulation Mostimportantevent:LHsurgesurge=suddenincrease.LHincreasesinthepreovulatorystage
Lutealphase HighlevelsofEstrogenandProgesteronesuppressproductionofFSHandLHthatthecorpusluteumneedstomaintainitself.
Physiologicalchangesinpregnancyhematologicalchanges:
• pregnancyishypercoagulablestate,soMoreriskforDVTsandPEs.• MinimalnormalHblevelforpregnantwomenis10g/dl.• physiologicalsystolicmurmurdevelopwhichdisappearsafterdelivery(Ejectionsystolic
murmur),whilearrhythmiasarepathological!• Peripheralresistancedecreases.Renalchanges:Dilationoftheureters,kidneypelvis&calyces.Endocrinechanges:• Prolactinlevel ↑untilthe30thweekofpregnancythenmore slowly toterm.
so,sometimesthepregnantladymaytellyouthatherbreastissecretingmilkandthatiscompletelynormal.
• enlargementofthyroidglandcausedbylowplasmaiodinelevels.• Thereisincreaseinweightofapproximately12.5kgatterm.
Gestationaldiabetesmellitus
• Gestationaldiabetesiscarbohydrateintolerancethatoccursinpregnancyafterthe24thweek
• PrevioushistoryofGDMisariskfactorforearlyscreeninginpatientswithmildcarbohydrateresistance.
• 2-h75gOGTTisthestandardofcaretestandwhat’scurrentlyusednowdaysforgestationaldiabetes.
• Afastingplasmaglucose>7.0mmol/L(126mg/dl)isdiagnosticofovertdiabetes.• ManagementbeforeconceptionindiabeticwomenincludecontrollingHbA1clevels• Iftheglycosylatedhemoglobiniselevated,orderafetalechocardiogramat22–24weeks
toassessforcongenitalheartdisease.EffectsofDMonpregnancy:Maternaleffects:• Thecesareansectionrateindiabeticpregnanciesapproaches50%becauseoffetal
macrosomia.• Injurytothebirthcanalsecondarytomacrosomia.Fetaleffects:• Hypoglycemiawhenbabyisexposedtohismom’shighbloodglucoselevels,he
produceslotsofinsulinsoassoonasthebaby’scirculationisdetachedfromhismotherhe’sexposedtohighinsulinanditcauseshypoglycemia.

• Hypocalcemiacausedbyfailuretoincreaseparathyroidhormonesynthesisafterbirth.• MostcommonfetalanomalieswithovertDMareNeuralTubeDefectsandcongenital
heartdisease.• Fetalsurveillanceformacrosomia
Anemiainpregnancy
• Serumirondecreases• TotalBindingIronCapacity(TBIC)increases• Instrictvegetarians,VitaminB12isalsodeficient.• ToconfirmIronDeficiencyAnemiayouneedtohave:decreasedIronandincreased
ferritin&transferrinlevels.• Anemiamanagement:Ifshe’slessthan30weekswegiveirontablets,butifmorethan
30weekswegiveironparenteraltherapyduringpregnancyPreconception,antepartum,intrapartumandpostpartumcare
Preconceptioncare• Womenshouldtakeadailymultivitamincontainingfolicacid(0.4mgperday)• womenwhohavehadaninfantwithaneuraltubedefect“highriskwomen”should
takevitaminsplus4mgoffolicaciddailybeforeconception.Highriskwomen:previousHxofNeuraltubedefectsorifsheisonanti-epilepticsorobese
• Rubella:ifthemotherIgG-vethensheshouldhavethevaccineandavoidpregnancyfor3months
Antepartumcare• Toxoplasmosis:ifthemotherIgG-vethensheshouldavoidpets,cookhermeatswell.
Babywillhavebrainclassification,ventriculomegalyandseizure• Syphilis:babywillhave:Sniffles(rhinitis),Sabershin,Saddlenose,Hutchinson'Steeth• Rubella:babywillhaveblueberrymuffin(petechiaeorpurpura),cataracts,congenital
heartdefect,hepatosplenomegalyanddeafness• Herpes:ifthemotherhasactiveherpesdeliverwithC/S.congenitalherpesare:IUGR,
pretermandblindness• Smokingincreasestheriskof:Miscarriage,placentalabruption,Growthretardation,
SuddenInfantDeathSyndrome,birthdefectandpretermdelivery.• Estimateddateofdelivery:Add7daystothefirstdayofLMP,subtract3months,add
oneyearIntrapartumcare
• Labor:progressivecervicaleffacementanddilationresultingfromregularpainfuluterinecontractions
• Falselabor“Braxton-Hickscontractions”:Painless,irregularcontractionswithoutcervicaldilatation&effacement.
• Station:isthefetalpresentingpartinrelationtoischialspine• Signsofplacentalseparation:afreshshowofblood,umbilicalcordlengthens,the
fundusoftheuterusrisesupandtheuterusbecomesfirmandglobular.Postpartumcare• ifthepatienthasperinealpainthemostimportantDDxis:1-hematoma:ifitissmall
thenleaveitandgiveanalgesia,ifitisbigandbleeding(youwillseevitalabnormalityandthesizeisbig)thendodrainage2-tightsuturethenletheruseheatlampandsitzbath
• RhoGAM:IfthemotherisRh(D)negative,andherbabyisRh(D)positive,sheshouldbeadministered300μgofRhoGAMIMwithin72hoursofdelivery.
AntenatalfetalassessmentIndicationforantepartumfetalsurveillance:• Maternal• Pregnancycomplication:(decreasedfetalmovements“mostcommonindication‘,IUGR)LatePregnancyAssessment:1-Fetalmovementcounting(kickchart):• Started~28winnormalpregnancy,~24winhighriskpregnancy.
o CARDIFFTECHNIQUE:10movementsin12hourso 2-SADOVSKYTECHNIQUE:4movements/hour
2-Contractionstresstest(CST):Atleast 2uterinecontractionsover20minutes.3)Nonstresstest(NST):• Thefirststepintheassessmentoffetalwell-beingistheNST.• Reactive:
o Atleasttwoaccelerationsfrombaselineof15bpmforatleast15secwithin20minuteso “<32weeks,≥10beats/min,lasting≥10s”
• Non-reactive:Noaccelerationfor40min>contractionstresstestorbiophysicalprofile4-Amnioticfluidindex(AFI)• Normalvalue:5-25cm• <5cm(urinarytrackanomalies,renalperfusion)• >24cm(GItrackanomalies,decreasedfetalswallowing)5)Biophysicalprofile(BPP):CombinesNSTwithUSS estimationAFV, fetalbreathing, bodymovementreflex/tone/extension-flexionmovement.6-DopplerVelocimetry:DopplerstudiesaremostlyvaluableforIUGRInterpretationofCTG:
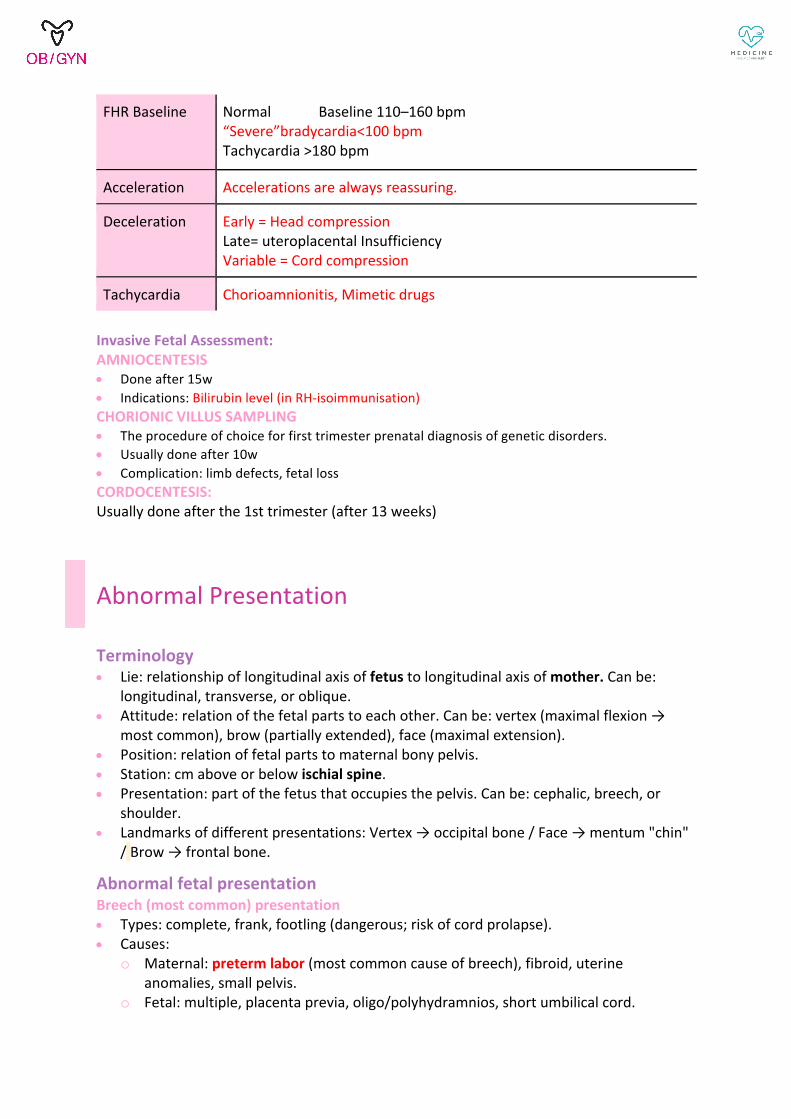
FHRBaseline Normal Baseline110–160bpm“Severe”bradycardia<100bpmTachycardia>180bpm
Acceleration Accelerationsarealwaysreassuring.
Deceleration Early=HeadcompressionLate=uteroplacentalInsufficiencyVariable=Cordcompression
Tachycardia Chorioamnionitis,Mimeticdrugs
InvasiveFetalAssessment:AMNIOCENTESIS• Doneafter15w• Indications:Bilirubinlevel(inRH-isoimmunisation)CHORIONICVILLUSSAMPLING• Theprocedureofchoiceforfirsttrimesterprenataldiagnosisofgeneticdisorders.• Usuallydoneafter10w• Complication:limbdefects,fetallossCORDOCENTESIS:Usuallydoneafterthe1sttrimester(after13weeks)
AbnormalPresentation
Terminology• Lie:relationshipoflongitudinalaxisoffetustolongitudinalaxisofmother.Canbe:
longitudinal,transverse,oroblique.• Attitude:relationofthefetalpartstoeachother.Canbe:vertex(maximalflexion→
mostcommon),brow(partiallyextended),face(maximalextension).• Position:relationoffetalpartstomaternalbonypelvis.• Station:cmaboveorbelowischialspine.• Presentation:partofthefetusthatoccupiesthepelvis.Canbe:cephalic,breech,or
shoulder.• Landmarksofdifferentpresentations:Vertex→occipitalbone/Face→mentum"chin"
/Brow→frontalbone.
AbnormalfetalpresentationBreech(mostcommon)presentation• Types:complete,frank,footling(dangerous;riskofcordprolapse).• Causes:
o Maternal:pretermlabor(mostcommoncauseofbreech),fibroid,uterineanomalies,smallpelvis.
o Fetal:multiple,placentaprevia,oligo/polyhydramnios,shortumbilicalcord.

• Management:o Before36weeks→waitforspontaneousturningofbaby.o After36weeks→shouldbeofferedoptions:
§ Vaginalbreechdelivery(VBD):lithotomyposition→afterbuttocksprotrudesfromvulvadoepisiotomy→deliverbodythenhead.
§ Externalcephalicversion(ECV):ü doneafter38weeks,ifmumrh-vegiveanti-D,ü Contraindications:contractedpelvis,scaruterusfromprevC/Sor
myomectomy,placentaprevia.ü Complications:membranerupture,uterinerupture,abruptio
placenta,cordprolapse.§ ElectiveC/S
Facepresentation• Causes:unknownpossiblyexcessivetoneofextensormusclesoffetalneck.• Diagnosis:duringlaborbypalpatingnose+mouth+eyesinvaginalexam• Management(modeofdelivery):
o Mento-anterior→vaginaldeliveryispossibleusingforceps.o Mento-posterior→caesarean.
Browpresentation• Diagnosis:duringlaborbypalpatinganteriorfontanelle+supra-orbitalridge+noseon
vaginalexam.• Management:deliverybycaesarean(b/cpresentingdiameteris13.5cm“mento-
vertical”whichisincompatiblewithvaginaldelivery).Shoulderpresentation• Causes:transverseorobliquelie,placentaprevia,highparity,pelvictumor,uterine
anomaly.• Management:
o Intactmembrane→ECVmaybeattemptedifnootherpathology.o Rupturedmembrane→deliverybyemergencycaesarean.
ThromboembolicDisease
• DupplexDoppler,x-rayvenogram&V/Qscanarethemaindiagnostictools.• Duringpregnancy,LMWHisthepreferredanticoagulantasitismoreeffectiveandsafer
thanstandardheparin.Oralanticoagulantiscontraindicated.(Ifsheisonwarfarinswitchtoheparin)
• Oralanticoagulantsshouldnotbegivenatanystageduringpregnancybuttheyaresafe&maybemoreconvenientafterdelivery.

Bleedinginearlypregnancy(abortion)
• Femalepresentswithvaginalbleedingin1sttrimester:o Ddx:spontaneousabortion,viableintrauterinepregnancy,ectopicpregnancy.o Assessment:
§ serialβHCG(if↑50%in48hours=viable)§ transvaginalUS(todeterminesiteofpregnancy)
Cervixopen Cervixclosed
Productspassed Incompleteabortion Completeabortion
ProductsNOTpassed Inevitableabortion Missedabortion
• Spontaneousabortionislossofpregnancybefore20weeksgestation.• Causes:
o 1sttrimester:chromosomalabnormalities→↑with↑maternalage.o 2ndtrimester:maternalsystemicdisease,antiphospholipidsyndrome,abnormal
placenta,anatomicreasons,cervicalincompetence(hxofcervicalconebiopsy).o Otherriskfactors:historyofabortion,smoking,uncontrolledDM.
• Types:o Threatenedabortion:bleeding+closedcervix+viableintrauterinepregnancy
(intactsac+normalfetalheart).o Inevitableabortion:bleeding+crampinglowerabdominalpain+cervicopen.o Missedabortion:vaginalbleeding+closedcervix+USshowslongfetalsacwithno
fetalheartactivity⇒needsevacuation(D&C)• Treatment:
o Conservative/expectantmanagement:watchandwait.o Medical:vaginalmisoprostol(usedtoinducelabor)o Surgical:D&Co REMEMBERtogiveRhoGAMtoRh-vewomen.
• Complications:hemorrhage,endometritis,septicabortion.• Furtherinvestigations:ifrecurrent2ndtrimesterabortions→Hysterosalpingogram.
Multiplepregnancies
Types:• Zygosity:
o Dizygotic“fraternal”:morethan2eggsfertilized.o Monozygotic“identical”:splittingofovumafterfertilization.
• Chorionicity:chorionic(#ofplacenta)vsamniotic(#ofsac)
o Dichorionic-diamniotic→divisionoccurs0-3days.o Monochorionic-diamniotic→divisionoccurs4-8days.o Monochorionic-monoamniotic→divisionoccurs6-12days.o Conjoined/Siamesetwins→divisionafter12days.
Complications• Maternal:anemia,hyperemesisgravidarum,preeclampsia,GDM,hydramnios,C/S,
uterineatony&postpartumhemorrhage.• Fetal:congenitalabnormalities,IUGR,placentalabruption,cordentanglement(mono-
mono),malpresentation,prematurity,placentaprevia,cordprolapse.• TTTS(twin-to-twintransfusionsyndrome)inmonochorionic→imbalanceofbloodflow
b/wAVcommunicationsleadingto:o Onebaby“donor”=underperfused(hypovolemia,hypotension,oligohydramnios,
anemia,growthrestriction)o Otherbaby“recipient”=overperfused(hypervolemia,hypertension,
polyhydramnios,cardiomegaly,thrombosis,edema,ascites).
Management• EarlyUSisdiagnostic(showsnumberoffetuses).• TodeterminechorionicitydoearlyUS(lambdasign→di-ditwins).• Monitoringisimportant!Bothmother(BP,GDM)andbabies.• Management:
o Adequatenutritionformother=iron+folate+calcium.o ThemodeofdeliverydependsonGA,chorionicity,presentation,etc..o Mo-moarealwaysdeliveredpreterm(32-34W)duetoriskofcordentanglementby
C/S+betamethasone.o Di-mo(at34-37+6W)anddi-di(canreachupto38weeks)canbedeliveredeither:
§ Vaginallyifcephalic-cephalic(mostcommonpresentation)orcephalic-breech.§ C/Sifbreech-breechorbreech-cephalic.§ Notethatthefirstfetustobedelivereddeterminesthemodeofdelivery.
PreEclampsia/Eclampsia/GestationalHTN• Preeclampsia:Onsetofhighbloodpressure(>140/90)after20weeksgestationwith
proteinuria(+1dipstickor300mg/dl)orendorgandysfunctionorwithoutproteinuriawithpresenceof1ormoreofseverpreeclampsia
• Eclampsia:presenceofnew-onsetgrandmalseizuresinawomanwithpreeclampsia• chronichypertension:knownhypertensionbeforepregnancyordevelopmentofhypertension
before20weeks’gestation.• superimposedpreeclampsia:thosewomenwithchronichypertensionwhodevelopnewonset
proteinuria.• gestationalhypertension:hypertensionwithoutproteinuriaorothersignsoforgandysfunction
firstappearsafter20weeks’gestationorwithin48to72hoursofdeliveryandresolvesby12weekspostpartum.
• Severpreeclamisa:thrombocytopenia,DIC,elevatedtransaminasesorothersignsofhepaticinjury,CNSsymptoms,anelevatedserumcreatininelevel,pulmonaryedema
Management

• PreeclampsiaGestationalage37ormore→delivery• severepreeclampsiaoreclampsiawhosediseasepresentsatorbeyond34weeks’gestation→
delivery• Severepreeclampsiapresentingatlessthan34weeks’gestation
o seizureprophylaxis:magnesiumsulfateIV,IMo controlofhypertension(Arterialbloodpressure≥160mmHgsystolicor≥110mmHg
diastolicmustbetreatedimmediately)§ Hydralazine:thebest§ LabetalolHydrochloride:Avoidifevidenceofasthmaoracuteheartfailure.§ Nifedipine.
• Eclampsia:Treatmentforseizureismagnesiumsulfate&deliveryofbaby.• Chronichypertension
o Methyldopaisthesafestantihypertensivemedicationinpregnancy.o calciumchannelblockers.o labetalol
Posttermpregnancy
• Definition:pregnancyreachingorextendingbeyond42weeksofestimatedgestationalage.
• Mostcommoncause:incorrectestimationofgestationalage.• Complications:
o Maternal:vaginaltrauma,caesareansection(andsubsequentcomplications:infection,bleeding,thromboembolicevents,visceralinjury),postpartumhemorrhage.
o Fetal:§ Macrosomia:>4.5kg→↑riskofC/S,shoulderdystocia.§ Postmaturitysyndrome:duetoinfarctionofplacenta→decreasefetal
subcutaneousfat+drywrinklyskin+longfingernails.§ Meconiumaspirationsyndrome:leadingtochemicalpneumonitis,mechanical
obstruction.§ Oligohydramnios:babyprioritizesbloodtobrain&thusdecreaseurine
production.§ Intrauterinefetaldemise(UFD)increasesafter41weeks.
• Intervention:o Firstwemustaccuratelymeasuregestationalage.o Membranesweeping→releaseprostaglandinsthatincreasechanceof
spontaneouslabor.o Fetalsurveillanceshouldbeginat41weeks“expectantmanagement”o Inductionoflaborshouldoccurbetween41&42weeks.
InductionOfLabor(IOL)

• Risks:Abnormalfetalheartratepatterns,Deliveryofpreterminfantduetoincorrectestimation
ofGA,Meconiumfetalaspiration• Indications:Post-termpregnancy,IUGR,Non-reassuringfetalsurveillance,Maternalmedical
conditions(DM,renaldisease,HPT,gestationalHPT),Fetaldeath.• Contraindications:Previousmyomectomy,Fetaltransverselie,Placentaprevia,VasapreviaMethodsofIOL• Ifthecervixisstillunfavorable:cervicalripeningwithprostaglandinE1orE2• Consideramniotomy+oxytocinonlyifthecervixispartiallydilatedandcompletelyeffaced,and
thefetalheadiswellapplied
IUFDManagement
Watchfulexpectancy
• About80%ofpatientsexperiencethespontaneousonsetoflaborwithin2to3weeksoffetaldemise.
• Rarecomplicationsincludeintrauterineinfectionandmaternalcoagulopathy
Inductionoflabor(IOL)
• Indications:emotional,thoseinriskofchorioamnionitis,IUFD>5weeksFromweek12-28• VaginalsuppositoriesofprostaglandinE2(dinoprostone)
o contraindicatedinpatientswithprioruterineincisions,patientswithhistoryofasthmaoractivepulmonarydisease
• Misoprostol
• After28weeks• ifthecervixisfavorable:Misoprostolfollowedbyoxytocin
OperativeDeliveries• Instrumentsusedinoperativevaginaldelivery:ForcepsandVacuum(ventouseextractor)• Thevacuumextractoriscontraindicatedinpretermdelivery
Indicationsofoperativedelivery• Maternalo Prolongedorarrested2ndstagelaborepicallyinMaternalcardiacdiseaseo Poormaternalefforto Patientswithretinaldetachmentorpostopforsimilarocularconditions.
• Fetalo Fetaldistresso Prematurity(useForcepsonly)o Certainmalpositionse.g.occipitoposterior
PrerequisiteforforcepsandventouseCervixhastobefullydilated+Membranesruptured+Headhastobeengaged(0station)+Headpositionknown+Vertex(cephalic)presentation.ComplicationsofInstrumentalDelivery

Genitaltractlacerations(Cervix,vagina),maternalHemorrhage,FacialPalsytothefetus
PuerperalsepsisCommonpostpartuminfections
Riskfactors Causes Clinicalfinding Management
Urinarytractinfection
Foleycatheterorvaginalprocedure
Normalbowelflora
• Highfever• Costovertebral
flanktenderness• Positiveurinalysis
Nitrofurantoin&cephalosporins
Woundinfection Emergencycesareansectionafterprolongedruptureofmembraneandprolongedlabor
StreptococcusStaphylococcus
Persistentspikingfeverdespiteantibiotics.
Cephalosporin
Mastitisorbreastabscess
Breastfeedingwomen S.aureus • Feverofvariabledegree
• localized,unilateralbreasttenderness.
7-10daysofDicloxacillin
Endometritis • Cesareansection• ProlongedROM• Prolonginternal
fetalmonitoring
polymicrobialinfections
gentamicin&clindamycin
RhesusIsoimmunizationRequirements1. Mothermustbeantigennegative2. Babymustbeantigenpositive.(Sofatheris+).3. AdequatefetalRBCsmustcrossoverintothematernalcirculation4. AntibodiesassociatedwithHemolyticdiseaseofthenewborn(Erythroblastosisfetalis)5. Asignificanttiterofmaternalantibodiesmustbepresenttocrossoverthefetus(>1:8)DetectingFetomaternal/TransplacentalHemorrhageKleihauer-Betketest:ThiscanassesswhethermorethanonevialofRhoGAMneedstobegivenwhenlargevolumesoffetal–maternalbleedmayoccur(e.g.,abruptioplacentae).

TechniquestoEvaluateFetalRhStatus• MCAdoppler(mostvaluabletodetectfetalanemia)• Amnioticfluidspectrophotometry(besttoestimatefetalbilirubinconcentration)• Percutaneousumbilicalbloodsampling(PUBS)→wecanmeasurefetalHb,Hct,bloodgases,pH,
andbilirubinlevels.ManagementPlan/Approach• Fetalriskispresent(haveallrequirements)butnosevereanemia:1stpregnancygiveRho-GAM,
not1stpregnancyjustwaitandwatch• Atypicalantibodytiter(1:8):managementisconservative.RepeatthetiterMonthly(2to4
weeks)aslongasitremains<1:8.• Severeanemia(PUBSshowsfetalhematocrittobe≤25%orMCAflowiselevated):Intrauterine
transfusion(freshORh-)• Timingofdelivery:• Deliveryisperformedifgestationalageis>34week.• Ifdeliveryisexpectedtooccurbefore34weeks’gestationbetamethasoneshouldbegivenat
least48hoursbeforedeliver• Rho-GAM• AspreventioninpregnantwomanwhenthereissignificantriskoffetalRBCspassingintoher
circulation• Uncomplicatedpregnancy(ifsheisRh-andtiteris<1:8):300μgofRhoGAMprophylactically.• Within72hof(deliveryofanRh(D)-positiveinfant,chorionicvillussampling(CVS),orD&C)→
300mcgofRhoGAM• AllpregnantwomenwhoareRhD-veandAntiD-veandexperience→(spontaneousorinduced
abortion,ectopicpregnancy,significantvaginalbleeding,abdominaltrauma,orexternalcephalicversion)shouldreceive50to100μgbefore12weekofgestationand300μgafter12week.
• “partial”molarpregnancy.
PROM• Prematureruptureofthemembranes(PROM):Prematureruptureofmembranesbeforethe
onsetoflabor• pretermPROM(PPROM):Pretermprematureruptureofmembranesoccurringbefore37weeks
estimatedgestationalageDiagnosis• onphysicalexam:Asterilespeculumexamination(poolingtest)+Anultrasoundshouldbe
performedtoassessfetalpositionaswellastoassesstheamountofamnioticfluid• confirmation:Nitrazinepaperwhichwillturnblue+Ferning• Chorioamnionitisisdiagnosedclinicallywithallthefollowingcriterianeeded:Maternalfeverand
uterinetenderness,purulentfluidfromcervicalosandmaternalleukocytosisandmaternaltachycardia.
Management• Ifthepatientisterm>37weeks:Ifthepatientdoesnotgointospontaneouslaboron
herownthenlaborinductionshouldbeperformedwithoxytocin.• from34to36weeksandsixdays:Aninductionoflaborhasstartedforthesepatients
onceruptureofmembranesisconfirmed.Ifthefetusisbreachthenacesareansectionwillhavetobeperformed.SomanagementexactlysameastermPROM.

• between24weeksand33and6days:inpatient+Corticosteroids+Tocolytics+Antibiotics.Deliverywillbeinducedbetween32and34weeks
• PROMoccurslessthan(<23wofGA):Eitherinducelaborormanagepatientwithbedrestathome.
• Chorioamnionitis:delivery
Pretermlabor• Deliverybetween24-37wksofEGAthatincludeuterinecontractions+cervicaldilation(atleast
2cm)orchangeinserialexamination(indilationoreffacement).• Evaluations:Vaginalexamination→cervicallength,dilation,station,presentation.Swap/Culture
forpresenceofGroupBstrep.• Diagnosis:TrueUterinecontractions→4/20min.(Poorindicatorofpretermlabor).Cervical
changes→80%effacementor2cmdilation.(Goodindicator)Management• Hydrationandbedrest• Antibiotic• Ifapatientdoesn’trespondtohydrationandbedrest,giveTocolytictherapy.• Betamethasoneif<34w.• DeliveryinPretermlaborisusuallyvaginally(normallyorusingoutletforceps),exceptforverylow-birthfetuses(↓1500g)wherecesareandeliveryisbetter,asin28wks.breechpresentation.
• HxofpretermlabororHxofshortcervix:Progesterone• Ifpatientis24-34weeksEGA:Corticosteroids:Mostimportanttoreducetheratesfor
Respiratorydistresssyndrome,Intracranialhemorrhage,Necrotizingenterocolitis,anddeath.
Bleedinginearlypregnancy(Ectopic)
• Definition:implantationofembryooutsidetheuterinecavity(mostcommonlyfallopiantube,specificallydistalampulla).
• Riskfactors:PID(x3),historyofectopic,historyoftubalsurgery,historyofchlamydiainfection,smoking,idiopathic,IUCD.
• Presentation:amenorrhea+unilaterallowerabdominalpain+vaginalbleeding.• Investigation:serialβHCG(noorpoorincreaseinlevels)+vaginalUS(absenceof
intrauterinepregnancy).• Management:
o Medical→methotrexate.§ Absolute#:hemodynamicinstability,liver/kidneydisease,lungdisease,breast
feeding,notcomplyingw/followupβHCGtesting.§ Relative#:fetalcardiacactivity,largeectopic>3.5cm,highβHCG>5000mIU.
o Surgical:§ laparoscopy(better)orlaparotomy(reservedforruptured)

§ salpingostomy(onlyremovingectopicpregnancy/mayrecur)orsalpingectomy(removalofentiretube/betterifothertubeisnormal).
3rdtrimesterbleeding• Placentalabruption(painfulvaginalbleeding)“mostcommon”
o Riskfactors:trauma,cocaine,HTN,multiplegestations,prevhxofabruption.o Diagnosebyclinicalexamination.
• Placentaprevia(painlessvaginalbleeding)o DiagnosebyUS(digitalcervicalexamis#).o Riskfactors:prev.C/S.historyofmyomectomy,multiparous,advancedage,
smoking,multiplegestations.o Management:modeofdeliveryisC/S.o Complications:bleedingorextensionofplacentaltissue(accreta,increta,
percreta)mayrequirecaesareanhysterectomy.o Vasaprevia(fetalbloodloss→canleadtoantepartumhemorrhage+fetal
death)• Note:Kleihauer-betketestcandetermineifbabyormotherisbleedingbydetecting
fetalerythrocytesinmaternalblood.
IntrauterineGrowthRestriction(IUGR)IUGR:estimatedfetalweight(EFW)<5−10%ileforgestationalage.Orbirthweight<2,500gramTypes:1-SymmetricIUGR:• Headandabdomenbothsmall• Etiology:Fetal(decreasedgrowthpotential)• causes:aneuploidy(T21,T18,T13);infection(TORCH/alsocouldbemalaria.),structural
anomalies• Workup:detailedsonogram,karyotype,andscreenforfetalinfections2-AsymmetricIUGR:• Headnormal,abdomensmall• Etiology:Maternal+Placental• Placental:primaryplacentaldisease),infarction,abruption,TTTS,velamentouscordinsertion.• Maternal:hypertension,smallvesseldisease(SLE,ChronicDM1),malnutrition,tobacco,alcohol,
streetdrugs,antiphospholipidsyndrome,Infections,Teratogenexposure.• Workup:Monitoringiswithserialsonograms,non-stresstest,AFI,biophysicalprofile,and
umbilicalarteryDopplersDiagnosis:

• Screeningtoollow-riskwomenistheassessmentofuterinesizebyfundalheightmeasurement.• Ultrasonographyisthegoldstandardtoassessfetalweight• Doppler(umbilical,uterinearteryS/Dratio,MCA).• Absent/reversedend-diastolicflowpredictsworseprenataloutcomesanditsusuallyan
indicatorfordelivery.Antepartumcare:• Fetalmonitoring->normal.DOUltrasonography->• normalgrowth=noclinicalintervention.• abnormalstronglysuggestsIUGR->deliveryisindicatedatgestationalagesof34weeks.• assessPulmonarymaturitybyamniocentesis,butIfsevereoligohydramnios->deliveryshould
bestronglyconsideredwithoutassessmentoflungmaturity.• .ambiguous(equivocalforIUGR->bedrest(w/kickcounting),fetalsurveillance,andserialU/S
measurementsat3-weeklyintervals.Afterbirth:• Examine:toruleoutcongenitalanomalies,chronicinfections.• Monitor:(hypoglycemia,hypothermia,Respiratorydistresssyndrome)Macrosomia:• >90−95%ileforgestationalage.Or(EFW)4000-4500grams• management:Electivecesarean(ifEFW>4,500gindiabeticmotheror>5,000ginnondiabetic
mother).
PostpartumHemorrhage
• vaginaldeliverybloodloss≥500mLorcesareansectionbloodloss≥1,000mLClassifications:• Primary:99%happensonlyinthefirst24hofdelivery.Secondary:After24h.
Signs Management
Uterineatony Enlargedfloppy,softuteruslikeadough
Uterinemassage,Oxytocin,ergot,Carboprost.OrSurgeryiftheabovedidn'twork>B-lynchsuture,uterinearteryligationofInternaliliac,embolization.
Lacerations Usingvaginaldeliveryinstrumentswiththepresenceofacontracteduterus.
Suturing&repair
Retainedplacenta Missingplacentalcotyledons Uterine curettage. Ormanualremoval

DIC bleedingfromIV/venipuncturesites
Correctionofcoagulopathy
Uterineinversion Beefy-appearing,andfailuretopalpatetheuterusabdominally
elevatingthevaginalfornicesandliftingtheuterusbackandoxytocin.
Preventionofuterineatonybyactivemanagementofthirdstageoflabor:fundalmassage,gentlecordtraction,IV/IMoxytocin.
PubertyDisorderCentralprecociouspuberty(CPP)• CPPisphysiologicallynormalpubertaldevelopmentthatoccuratanearlyage.• Causes:Idiopathic,CNStumors,CNSdysfunction• Investigations:IncreasedLH:LH/FSHratio>1→PubertalgonadotropinresponseCPP.GnRH
stimulationtest:highLH>FSH• Tx:ThetreatmentofchoiceisAGnRHAnaloguePeripheralprecociouspuberty/PseudoPP(PPP).• GnRHindependentDuetoinappropriatesexhormonesecretionorexposuretoexogenoussex
steroids.• Causes:Abnormalsecretionofgonadotropins,Functioningovariantumorsorcyst,Congenital
adrenalhyperplasia• Investigations:DecreasesLH:LH/FSHratio<1→Prepubertalgonadotropinsecretion(PPP).
GnRHstimulationtest:FSH>LH• Tx:Treatthecause.
AmenorrheaPrimaryamenorrhea• ifBreastspresent,uteruspresentmostcommolyitisimperforatehymen• ifBreastspresent,uterusabsent.DifferentialdiagnosisisMüllerianagenesisorcomplete
androgeninsensitivity• ifbreastisabcentanduterusispresent:oneofDDxisTurner’ssyndrome(45x0)→gonadal
dysgenesisSecondaryamenorrhea• Asherman’ssyndrome:SecondaryamenorrheafollowingdestructionoftheendometriumBy
overzealouscurettage• Prematuremenopause:Ovarianfailure• Hyperprolactinemia:duetopituitaryadenomaseenonMRI.Tx:Bromocriptine• Sheehan’ssyndrome:Necrosisofant.pituitaryduetoseverepostpartumhemorrhage,Bcof
panpituitarismtheprolactinmaynotsecreted→unabletobreastfeedInvestigationofsecondaryamenorrhea
• PregnancyTest.Thefirststepinmanagementofsecondaryamenorrheaistoobtainaqualitativeβ-hCGtesttoruleoutpregnancy.
• ProgesteroneChallengeTest(PCT):+vemeansanovulation(e.g.PCOS)• Estrogen–ProgesteroneChallengeTest(EPCT)
o ElevatedFSHsuggestsovarianfailure(e.g.prematuremenopause)o LowFSHsuggestshypothalamic–pituitaryinsufficiency(e.g.pituitarytumors)o –veEPCTmeansabnormalflow(e.g.Ashermansyndrome)
PelvicInflammatoryDiseases(PID)• Ascendingmicroorganismsfromvagina&endocervixtoendometrium,tubes,contiguous
structures.N.Gonorrhoeae N.Gonorrhoeae
Gram–vediplococcus Intracellularorganism Producemildformofsalpingitis.
Rapidgrowth SlowgrowthRapidandintenseinflammatory
response Insidiousonset
• Signs&symptoms:Abdominalpain,AbnormalDischarge,Fever• Management:ceftriaxone+doxycycline±metronidazoleandtreatthepartner(Reinfectioncan
occurifmalepartnerisuntreated)
PolycysticOvarianSyndrome(PCOS)• Characterizedbyovulatorydysfunctionandhyperandrogenism.• asetofsymptomsduetoelevatedAndrogensinwomen.Biochemicalchanges:1. Raisedandrogenproduction.”testosterone”2. Peripheralinsulinresistanceandhyperinsulinemia3. Proposedmechanismforanovulationandelevatedandrogenlevelisduetoincreaselevelof
luteinizinghormone.Signsandsymptoms:• Menstrualdysfunction• Anovulation• Signsofhyperandrogenism(Hirsutism,acne,hairfall).• infertility.• ObesityInvestigation:LH,FSHlevels&ultrasounds&Endometrialbiopsy(malignancy)criteriaofdiagnosing:• Afterexcludingotherdiseases,wehavetofind2criteriafromthe3whichis: • anovulatorycycle(changeinmenstrualpattern).

• Hyperandrogenism(hirsutism,acne,Acanthosisnigricans,hairloss)orbiochemical• USshowspolycystic.Management:1. Lifestylemodificationisthefirstlineoftreatment2. Medicalmanagement:
o Menstrualirregularity:First-linemedicaltherapyisoralcontraceptiveo Anovulation:Clomiphenecitrateorletrozoleo Hypoglycemicagent:Metformino Topicalhairremoval:eflornithineo Topicalacneagent:benzoylperoxide,tretinointopicalcream
3. Surgicalmanagement:aimtorestoreovulation• Laparoscopically:(ectrocutare/Laserdrilling./Multiplebiopsy)
ContraceptionLongactingreversiblecontraceptionProgesteroneIUDSideeffect:lightermenstrualcycleoramenorrhea.CopperIUD:Sideeffectsincludeheavierandcrampierperiods.Implants:Sideeffectsincludeirregularbleedingspottingforthedurationofinsertion.• TheonlycontraindicationstoallIUDusearepelvicinfection,canceroftheuterus,ordistortion
orinappropriatesizeoftheuterinecavity.SterilizationMaleSterilization:• whetherrightorleftvasdeferensisligatedtopreventspermfromenteringtherestofthe
seminalfluid.• Semenanalysisiscollected4-3monthswith20ejaculatesFemaleSterilization• TubeLigationorHysteroscopytubeocclusion• Consoffemalesterilization:Ectopicpregnancy• Prosoffemalesterilization:Decreaselifetimeriskofovariancancer,Protectionfrompelvic
inflammatorydiseases.Estrogen-progesteronecontraceptives• Minipills(progesterone-onlypills)onlyworkefficientlywithregularandfrequentbreastfeeding.• increasestheriskofDVT• Contraindications:
o Migrainewithaurao Historyofbloodclotso Personalhistoryofbreastcancero Personalhistoryofliverdiseaseo Forwomenover35thelistalsoinclude:Smoking,HTNormigraine.
DepoProverainjectionsSideeffectsincludeAmenorrheaandanaverageof10poundsweightgain.Barriersfemaleandmalecondomsareprotectedagainstsexualtransmittedinfections.

EmergencyContraception• twopills0.75mgoflevonorgestrelwithin72hoursoftheintercourse.• ulipristalacetate30mganditcanbeusedupto120hoursaftertheintercourse.
Endometriosis
• Definition:Benignconditioninwhichendometrialglandsandstromaarepresent
outsidetheuterinecavityandwalls.• Occurrence:womenwithchronicpelvicpainhaveendometriosis.• Sitesofoccurrence:ovaries,Pelvicperitoneum→Posteriorcul-de-sac,Roundligament,
fallopiantube.• Symptoms:Dysmenorrhea+Dyspareunia+Dyschezia• Signs:
o fixednon-Mobileuterus.Secondarytoadhesions.o ovarianendometriosis(chocolatecyst)tenderbutnotpalpable.o uterosacralnodularity(classicsign).
• Diagnosis:2outof4o endometrialstromao endometrialglando endometrialepitheliumo hemosiderin-ladenmacrophages.
Management:• Medicaltherapy:EtherPregnancyIfWantedOrPseudopregnancyPseudomenopause.• Surgicaltherapy:Largeendometriomas(>3cm)areusuallyamenableonlytosurgical
resection.• Followup:itisNotmalignantbutassociatedwithhigherriskofovariancarcinomaby
mechanismwhichisnotclear.
Lowergenitaltractinfections
Vulvarvaginitis
Bacterialvaginosis(mostcommon)• Polymicrobialinfection→imbalanceofnormalaerobic&anaerobicorganisms.• Riskfactors:postmenopausalwomen.• Symptoms:thinwhitedischarge,fishyodor.• Diagnosis:wetmount(cluecellsw/stippledborder),pH>4.5,whifftest.• Treatment:metronidazole1stline(oralorvaginal),orclindamycin(vaginal).Vulvovaginalcandidiasis• Organism:candidaalbicans→mostcommon.• Riskfactors:DM,obesity,pregnancy,antibiotics,C/S,OCP,tightclothes.• Symptoms:thickwhitecheesydischarge,itching,dyspareunia.
• Diagnosis:wetmount(pseudohyphae,yeast),pH<4.5,+veyeastculture.• Treatment:fluconazole(antifungalsingledose),orvaginalmiconazole.Trichomoniasis• Organism:trichomonasvaginalis→facilitatestransmissionofHIV• Riskfactors:swimmingpools,hottubs,STDs.Associatedw/PID,endometritis.• Symptoms:yellowprofusefrothydischarge,malodorous,strawberrycervix.• Diagnosis:wetmount(flagellatedmotileorg.),pH>4.5,testforotherSTDs.• Management:metronidazole(1stline)+treatpartner.
DysmenorrheaPrimarydysmenorrhea
• Thesymptomstypicallybeginseveralhourspriortotheonsetofmenstruationandcontinuefor1to3days.
• SymptomsappeartobecausedbyexcessproductionofendometrialprostaglandinF2αresultingfromthespiralarteriolarconstrictionandnecrosisthatfollowprogesteronewithdrawalasthecorpusluteuminvolutes
• Treatment:NSAIDsarefirst-line.OralcontraceptivessecondlineSecondarydysmenorrheaCauses4. Endometriosis 5. Adhesions 6. PelvicInflammatoryInfection7. Adenomyosis 8. Leiomyomata 9. Polyps10. Cervicalstenosis 11. Tumors(benignor
malignant)orcysts
ManagementTreattheunderlyingcause
Menopause• Menopauseisdefinedas12monthsofamenorrhea,associatedwithelevationof(FSH,LH)• AtthetimeofmenopauseFSHconcentrations>30mIU/mlSignandSymptoms• Amenorrhea:Themostcommonsymptomissecondaryamenorrhea• Hotflushes:predictableprofusesweatingandsensationofheat• Increasedriskofosteoporosis
o WegiveCa2++vitaminD,encouragethemtodoweight–bearingexercise,stopsmokingandalcohol.WecouldgiveHRTorbisphosphonates(alendronate,risedronate)orSERM(raloxifene)
Management

SystemicHormonetherapy(HRT):Itisthemosteffectivetreatmentforhotflushes.Ifshehasauteruswegiveestrogen+progesterone(toprotectherfromendometrialcancer).Ifshehasnouteruswegiveestrogenonly.
PelvicFloorDisorders• Cystocele:Herniationorbulgingoftheanteriorvaginalwallandoverlyingbladderbaseintothe
vaginallumen.Triad:1-Postmenopausalwoman2-Anteriorvaginalwallprotrusion3-Urinaryincontinence
• Rectocele:Herniationorbulgingoftheposteriorvaginalwallandunderlyingrectumintothevaginallumen.Triad:1-Postmenopausalwoman2-Posteriorvaginalwallprotrusion3-Digitallyassistedremovalofstool
• Enterocele:HerniationofthepouchofDouglascontainingsmallbowelintothevaginallumen• Symptoms:Vaginalpressureorheaviness,Vaginalorperinealpainordiscomfort• Riskfactors:Onevaginaldeliveryormore,Pelvicsurgery,increasedintra-abdominalpressurePelvicOrganProlapseQuantificationexamination• Stage0:Noprolapse,thecervixorvaginalcuffisatthetopofthevagina.• StageI:Theleadingpartoftheprolapseismorethan1cmabovethehymen• StageII:Theleadingpartoftheprolapseislessthanorequalto1cmaboveorbelow
thehymen• StageIII:Theleadingedgeismorethan1cmbeyondthehymen,butlessthanor
equaltothetotalvaginallength• StageIV(Procidentia):CompleteeversionManagementKegelexercises+PessariesIncontinence
Stress
incontinence
Hypertonic(urge)
incontinence
Hypotonic(neurogenic)incontinence
Irritablebladder Fistula
Cause
MuliparityIncreaseabdominalpressure
Detrusormuscleoveractivity
AbsentDetrusormusclecontractionduetoneurologicalcause(MS,DM,trauma)
Inflammationcomingfromstone,UTIorcancer
Previousradiationorsurgeryonthepelvic.IBD(crohn)
Presentation
Urinelosswithincreasedintra-abdominalpressure
UrgencyNocturnalLeakofurine
Lossofurineintermittentlyinsmallamountsandpelvicfullness.
Frequency,urgency,dysuria
Contiousleakwithnormalfunction
Diagnosis
YoumayfindcystoceleQ-tiptest+veUrineanalysis–ve
PhysicalexaminationnormalUrineanalysis–ve
Physicalexamination:distendedbladder
Physicalexaminationisnormal
Youwillseethefistulaonphysicalexamination

Cystometry-ve
Cystometry:involuntarydetrusorcontractions
Urineanalysis–veCytometry:markedlyincreasedresidualvolume
Urineanalysis:WBCs,RBCsCytometry:normal
Treatment
KeagelPessariesSurgery(Tension-FreeVaginalTapeormmK)
Anticholinergicmedications:oxybutyninandtolterodine
Intermittentself-catheterization.Cholinergicmedications+α-adrenergicblocker
Treattheunderlysingcause
Surgery(fistuloectomy)
Infertility
FibroidTypesoffibroids• Intramuralisthemostcommontype&usuallyasymptomatic.• Subserosal,canbedescribedasnon-tenderfirmmass.Itssymptomsdependontheir
location(pressuresymptoms).
Infirtility
Testthemale(erection,flagellated,count)
Maleproblem
1- erectiledysfunction:council+PDE5Inhibitors2- countingandmotility:doartificialinseminationA- IUI(intrauterineinsemination)B- IVF(invirtofertilization)
Femaleproblem
Roleoutovulationproblem
Anovulation
Prolactinomaorthyroidproblem
PCOS
Normal
Check for↓ovarianreserve
Normal ↓ovarianreserve
AnatomyviaHSG
Normal Anatomyproblem
Diagnosticlaproscopy
Unexplaned Endometriosis
+ve -ve
+ve -ve
↑prolactinorTSH SignsofPCOS
Antimullerial hormoneFollicular countDay3FSH/estrdiol
+ve-ve
-ve +ve
-ve +ve
Treatmedically Giveclomiphene
NotreatmentL
Surgicalrepairorartificialinsemination
Doscop laserablation
Doartificialinsemination
Howtocheckforovulation?Basaltemperature
UrineLHDay22progesterone

• Submucosal,distorttheuterinecavity.Mostcommonpresentasmenorrhagiaormetrorrhagia.
• Othertypes,pedunculated¶sitic.Degenerationsoffibroids:• Reddegeneration,inpregnantwomen.extreme,acutepain,andnarcotics.Shouldbe
managedbyanalgesiainpregnant.Myomectomydoneafterpregnancy.• Calcificdegeneration,it'spotentialtobecomesarcoma.• Othersdegenerationslike,Hyaline,fatty,cystic,necrosis.DxofFibroidsHx&PE,US(abdominal&transvaginalUStoexcludeendometrialhyperplasia),CT&MRI.Hysteroscopy(forsubmucosalfibroids).Biopsy.Management.• Observationmostly.• Medicationsifsherefusedsurgery.Deprovera,GnRHanalogous,Danazol• Surgery,Myomectomy.Ifpatientwishestomaintainfertility.Hysterectomy,Ifpatient
hascompletedherchildbearing;definitivetherapyisanabdominalorvaginalhysterectomy.
• Embolizationifshewantstopreservetheuterus.
Abnormaluterinebleeding• menstrualflowoutsideofnormalregularity,frequency,volumeorduration.common
andcanrangefromcompleteabsenceofbleeding(amenorrhea)tolife-threateninghemorrhage.
EtiologyPALMCOEINacronymforAUBdifferentials.structural(PALM,mostcommoninperiandpost-menopausalwomen):• Polyp.• Adenomyosis.identifyinganenlarged,symmetric,tenderuterus.• Leiomyoma.• Malignancy.functional(COEIN,mostcommoninreproductivewomen):• Coagulopathy:mostcommoninadolescentwomenwhopresentswithheavybleeding.• OvulatoryDysfunction:PCOS(mostcommoncauseofovulatorydysfunction),STD.• Endometrialprocess:usuallyaffectedbyestrogen.• Iatrogenic.• Notyetclassified.EvaluationofAUB• Hx&PE.• Iftheperiodisirregular:ovulatorydysfunction.• Ifthereisbleedingbetweentheperiods:structuralcause• Heavyperiods:coagulopathy• Labs:Thyroid,CBC,Anemia,coagulopathy.
• EMBinhighriskwomen,likeDM,Obesity.• US.
ONCOLOGYREVISION(DonebyRawanALQahtani)
1. Cervical neoplasms:
• Howtoscreenforcervicalcancerandwhen?1. ByPapsmear:westartscreenthepatientattheageof>21yearsold,every3years.Until65yearsoldwhichis
theupperlimitbecausetheincidenceisnotsignificant.2. HPVtest:Itistheotherwayforscreening.westartscreenthepatientattheageof>30yearsold,every5years.
Why>30,Because80-90%ofthemwillbepositiveforHPVinfectioninpatients20-30yearsoldandtheywillclearitspontaneouslybytheirimmunesystems.Only10-20%theywillhavepersistentinfectionwhichwillprogressandchangetheirDNAandleadtotumorgrowth.ForthosewhohavepersistentHPVpositivewehavetodocolposcopytovisualizethecervix,ifwecannotseeanythingwewilltakerandombiopsytodetectanypremalignantlesion.
• HowHPVcausecarcinogenictransformation?Afterenteringourbody,ittargetsthecervicalcellsandstarttochangeDNAespeciallytwotumorsuppressorgenewhicharep53andretinoblastoma.SoViralproteincalledE6suppressesp53,whileE7suppressretinoblastomagene. Thesetwogeneswereimportantascheckpointwhichpreventandcorrectanyabnormalchangeincells.Soinhibitionoftumorsuppressorgenewillleadtocarcinogenesischanges.Thisprocesstakesfrom10-15yearstoyearstoprogressintocancerandneedlesstimeinimmunocompromisedpatients.
• HPVVaccine:o 99.9%ofcervicalcancerisHPVpositive,sothisistheonlycancerwhichweknowthecauseofitanditis
preventablebyHPVVaccine.o TherearedifferentoncogenestrainsofHPV,suchas16&18&31&33&45&52&58whichcause95%of
cervicalcancer.While6&11arebenignstrainwhichcausewarts.o Nowthelatestvaccine(Gardasil)covers9strainwhichare(16,18,31,33,45,52,58).o Someofstudiesshows93%decreasedtheincidenceofcervicalcancerwiththosewhohadhighgradelesion.
Whichmeanyouprevent93%ofpeoplewithhighgradelesiontoprogresstocancer.o Patientswhoare+veoralreadyshowdysplasiacanstillreceiveHPVvaccine,asitcanprotectthemfromother
strainsofHPV.o Insomecountrytheyvaccinatedbothfemaleandmale.
• Whataretheexpectedresultsfrompapsmear?o Normal(Iwillrepeatitevery3year)o Cancer:(Squamouscellcarcinoma(70%)orAdenocarcinoma(20%)whichismoreaggressiveandcomefromthe
canal)o precancerousabnormality(DYSPLESIA),
§ Highgrade(HSL).§ Lowgrade(ASCUS&LSL){ASCUS=Atypicalsquamouscellofundeterminedsignificant,thisisthemost
commonabnormalityinpapsmear,andtheonlyindicationforHPVtestwithbestadvantageandcosteffectivewaytoscreenthepeoplewithASCUSbyusingHPVtestsoanypatientwithASCUSitisworthtoscreenthemwithHPV}.ü Ifitwaspositive,wegotocolposcopy.ü Ifitwasnegative,wegotonormalscreeningevery3years.
• What wewilldonextincaseofabnormalfindinginpapsmear?

WewillgoforcolposcopytovisualizethecervixIfshowsalesionyoucantakeintralesionalbiopsy.Ifnot,takearandombiopsy.
o IftheywerenegativeorlowgradesuchasCIN1,reassurethepatientandfollowherafter6months.o IftheywereCIN2orCIN3,wehavetodosomethingadditionaleitherconebiopsyorLEEP.Lookingformargins,if
theyare-vesothepatientistreatedwhichmeanIalreadyhavetakenthelesionsononeedforfurthertherapy,ifthemarginswerepositivewehavetodoanotherconebiopsyandcouncilherabouthysterectomyifshecompletedherfamily.
o Ifthebiopsyshowscancer,whichisdefinedasinvasionofbasementmembrane.Inprecancerouslesionordysplasia,itmayinvolvethewholethickness,butitneverneverinvadesthebasementmembrane.Onceitstartsinvadethebasementmembraneitisnowinvasivecervicalcancer.
• Whatisthemostcommonhistopathologicalcervicalcancer?Squamouscellcarcinoma(70%)orAdenocarcinoma(25%)lymphoma,sarcomaandmetastasis(5%).
• StagingofCervicalcancer:o Inanycancer,weneedtostagesowecandeterminethemanagement.o Cervicalcancerisclinicallystagingwhichmeanbysimpletoolssuchas(CT,MRI,physicalexamination,histories,
colposcopy,proctoscopyandcystoscopy)wecanstageit.Unlikeothergyncancerwhichsurgicallystagingwhichmeanweneedtodosurgerytostageit.Evenifthesurgeryrevealpositivefindingsuchaslymphnodeorinvasiveofrectumwewillnotchangeourclinicalstagingorupgradeit.Butforsurethemanagementwillbechangeaccordingtothefinding.
o Themostcommongynecologicalcancerindevelopingcountryiscervical,becausethelowsocioeconomicstatus.o ThemostcommongynecologicalcancerindevelopedcountryisEndometrial,becausetheirlifestyleandobesity.o ThemostcommongynecologicalcancerinSaudiArabiacountryisOvarian
- Done by Luluh Alzeghayer,435 <3
Forexample,aladywasdiagnosedwithinvasivesquamouscellcarcinomaofcervix.shewascomplainingoflowerlimbswellingduetolymphedemaorsciaticpainandfootdrop,orwithinvestigationshehadhydronephrosis,wecandiagnoseherclinicallyasstage3B.Somepatientmaydieduetorenalfailurenotfromcervicalcanceritself
o Anotherexample,aladywasdiagnosedwithinvasivesquamouscellcarcinomaofcervix. HerPelvicexamination
revealedthickeningoftherightparametriumbutnotouttothelateralSidewall.wecandiagnoseherclinicallyasstage2B.
o Anotherexample,aladywasdiagnosedwithinvasivesquamouscellcarcinomaofcervix.shewascomplainingofpassingstoolthroughvaginalopening.wecandiagnoseherclinicallyasstage4A.
o Incaseof1A1isdependofageandparity,ifsheisayoungladywhoisplanningtohavekids,wegotoconebiopsywithnegativemargins,ifsheiselderlywomenwhocompletedherfamilywegotosimplehysterectomy.
o Thesamefromstage1A2-2A2,wewillgoforradicalhysterectomyifsheiselderlywomen,andinyoungwomenwithlowparitywegofortrachelectomywhichisasurgicalprocedureusedtotreateligiblewomenwithearlystagecervicalcancerbyremovingonlythecervix,uppervaginaandparametrium.
o 4Bitisapalliativecarewhichcouldbecomfortcarewithanalgesicandantiemeticor

o couldbechemotherbyorsurgerytodecreasetheaccelerateofdiseaseandexpandthelifealittlebit.Forexample,wecandopalliativehysterectomyforthosewhocomplainofvaginalbleedingbutthatwillnotcurethepatient.
o Itisgoodforthepatientifshepresentswithearlystagesowecureher,becauseunlikeothergynecologicalcanceruninsecondstagewecannotdoasurgeryandwegoforchemoradiation.IncervicalcancertheMainpresentingcomplaintispostcoitalbleeding
o Theindicationforchemoradiationincervicalcancer(positivemargins,positivelymphnode,positiveparametria.Iftheyarenegativepatientdoesnotneedradiationandthefollowupaftersurgeryitisenough.
o Thefollowup,thefirsttwoyearsevery3months,thenextthreeyearsevery6months.
2. Ovarian neoplasms:
o Done by Luluh Alzeghayer,435 <3
• Epitheliumovariantumor:
o Debulking(cytoreduction)=TAH-BSO+LNremoval+omentectomy+anyvisibledisease.o TheypresentwithNonspecificsymptoms:abdominaldistension,ascites,intestinalobstruction,paraneoplastic
syndromee.g.weightloss.o themostcommonstageatthepresentationinpatientwithovariantumor?Stage3:peritonealmetastasis.o Whatarethemarkersforovariantumor?
• Whataretheriskfactorsforovariantumor?o Nulliparity,becausewitheveryovulationthereistraumaandinjurytoepithelialline.o Anythinginterferewithovulationisprotectivesuchasmultiparity,pregnancy,hysterectomyandOCP.o Familialhistorywhichassociatedwithovariantumors:
§ BRCA1&2.RiskofbreastCAinbothis60-80%.RiskofovarianCAinBRCA1=40%,BRCA2:20%§ Lynchsyndrome(cancerofcolon60-80%,ovaries5-10%,endometrium40%,bladder,ureter,biliary,brain)
• Thesurvivalrateinovariancancerdependsonoutcomeofdebulking.• Afterthedebulkingwefollowupthepatientintheclinicwithtumormarkers.• Theomentumisacommonsiteforrecurrence.• Itiscontraindicatedtotakethebiopsyfromtheovarybecauseyouwillspreadthetumorandupstagethedisease.• Themanagementforbothtypes(seriousandmucinous)isthesame,exceptthatinmucinoustypewedo
appendicectomytoremovetheappendixasapartofsurgery,becausemostofmucinouscancerarearisefromGIoriginuntilprovenotherwise.
• WehavetodoCTscanforchest,abdominalandpelvicforallpatient.

NON-Epitheliumovariantumor• Whatisthemostcommongermcelltumor?itusedtobedysgerminomabutnowitisimmatureteratoma.• theyaretotaloppositeinprognosis,dysgerminomaiscurablewithgoodprognosewhileimmatureteratomaisonof
theworsttumorwhichaffectyoungwhichcausedeathandverybadprognose.• schillerduvalbodiesisspecialhistopathologicalfindinginyolksactumor. • Whatisthemostcommonsexcordtumor?Granulosecelltumor,itstumormarkerisinhibin.• Call-ExnerbodiesisspecialhistopathologicalfindinginGranulosecelltumor.• Whatisspecialaboutgranulosacelltumor?
1. 1-ItisEstrogensecretingtumor,sothepatientwillpresenteitherwithvaginalbleedingorbreasttendernesswhicharesignofexcessiveestrogen,besidehighinhibinlevel.
2. 2-Alsowehavetodoendometriumbiopsybecauseshehasariskfordevelopingendometriumcancer.3. 3-inaddition,thefollowupwillbeforlife,becausetheriskofrecurrenceishighevenafter35years.
• IfthepatientpresentwithhirsutismwewillthinkaboutSertoliLeydigcelltumorwhichistestosteronesecreting,anditisatypeofsexcordtumor.
Metastaticovariancancer:
Krukenbergtumors:whichmeanmetastatictumorscomefromsomewhereelsetotheovary.themostcommonismetastaticfromthestomach.Inallcasesarestage4,andthemanagementdependontheorigin.
Borderlinetumors(non-invasivebutcanmetastasized):• Itliesbetweenbenignandmalignantandfeaturefromboth.Soitdoesnotinvadelikebenignlesionbutatthesame
timeitmetastasizeslikemalignant.• Goodprognosis(80-90%).Butmayrecuraslow-grademalignanttumor.• Theydon’trespondtochemonorradiation,thegoldstandardissurgicalresection.
3. Endometrium neoplasms:
Done by Luluh Alzeghayer,435 <3
• 90%ofpatientspresentearly(stage1)duetoAUB(abnormaluterinebleeding).• MostcommoncauseofAUBinpostmenopausalwomenisgenitalatrophy.• PerformendometrialbiopsyforanypatientwithAUBwhoseage>40especiallypostmenopausal.• ThosewithstrongriskfactorssuchasobesityandPCOSorfamilyhistoryeveniftheyareyoungerthan40wewill
endometrialbiopsy.• Anyyoungwomenwhodiagnosedwithcoloncancershouldbescreenedforothergynecologicalcancer.
Theresultsofbiopsy• ItcouldbeNormal,Cancerorprecancerousabnormality(Hyperplasia)• Riskofprogressionofhyperplasia(premalignant)tomalignancy:• Simplehyperplasiawithoutatypia:1%withatypia(x10):10%• Complexhyperplasiawithoutatypia:3%withatypia(x10):30%• WehavetodoCTCAP(chest,abdominal,pelvic),ifthebiopsyshowscancer.

Done by Luluh Alzeghayer,435 <3
• Brachytherapyisaformofradiotherapytothetoppartofvaginawhichisthemostcommonsiteforrecurrence.• Stage2isunique,itinvolvesthecervix,andwemayfindalesionduringexamination.Wemanageitlikecervicalcancer
bytwoways,eitherbyradicalhysterectomywithremovalofparametrium.Orexternalbeamradiationfollowedbysimplehysterectomy.
• intheendometriumeitherchemoorradiationnotbothtogether,unlikecervicalcancerwhichstartwithchemotosensitizethetissuethenradiation.
Patientwithbenignchangeswanttopreservefertility:• Benignchangescanbetreatedbyprophylactichysterectomyorhighdoseprogesterone.• Highdoseprogesteronefortreatingapatientwithlowgradeendometroidendometrialcancer(80%
responsetotreatment)• Conditions:lowparityandwishtopreservefertility,grade1endometroidendometrialcancer,no
myometrialinvasion,LN<1cmonMRI(MRIisusedinsteadofsurgicalbiopsy).• Followupin3months,ifbiopsyis-ve,refertoIVF.ifstill+ve,doublethedoseofprogesteroneandrepeat
thebiopsyin3months.Ifsheisstill+ve,repeatMRI,ifstillshowingnolymphadenopathyandnomyometrialinvasion,continuemedicaltreatmentfor3moremonths.Afterthese9monthsfromdiagnosis),ifstill+ve,medicaltherapyfailed,andpatienthastoundergocompletesurgicalstaging.
4. GTD & GTN neoplasms:
Gestationaltrophoblasticdisease(GTD):DonebyLuluhAlzeghayer,435<3
• MostcommonPresentation:Largeuterus,vaginalbleeding,hyperemesisgravidarum,thyrotoxicosis(becausebHCGhasthesamealphasubunitofTSH).
• Diagnosis:Quantitativeb-HCG:extremelyhighbHCGlevels.• CanbeseeninUS:
o snowstormappearance(COMPLETEMOLE)

o hydropicvilli,thecaluteinovariancysts(noneedtotreatthem,theyregressafterresolutionofGTD)o partoffetusorgestationalsaccanbeseen(INCOMPLETEMOLE),itissimilartomissedabortionwhere
theycanfindpartoffetusafterabortion.• HowthePatientshouldbefollowed?andwhy?
weeklywithb-HCGuntil3consecutive-veresultsthenmonthlyfor6months.BecausetherecurrenceandthereisarisktochangeintoGTN.
• Whichtype,weneedtogiveAnti-DifthemotherisO-?Incompletemolar,becausethereisfetus.• Duringthefollowup,wegivethemOCPtoavoidconfusionregardingthesourceofhighb-HCG
GestationaltrophoblasticNeoplasia(GTN):• itistheonlyneoplasiawetreatitwithoutanybiopsyorhistopathogytodiagnose.• Wedonottakeabiopsybecausethediagnoseisclearwithcontext• HowcanIknow,itischangingtoGTN?
o b-HCGisnotdroppingasexpected,plateauingorrebounding,oro Ifstill+veafter6monthsfromthetimeofevacuation,oro Ifhistopathologyaftertheevacuationofmolarpregnancycame+veforchoriocarcinomaorInvasivemole.
• Whatarethetypes?1. Invasivemole(intheuterusbutstarttoinvade)2. Choriocarcinoma(itcanbemetastasizedtobrain,liver,andmostcommonlylung)3. Bothrespondstochemo95%withanexcellentprognosis.4. Placentalsitetrophoblastictumours(PSTTs):Highb-HCG+highHPLinpost-partumwomen=Placental
sitetrophoblasticuntilprovenotherwise. • Aftermiscarriageornormalpregnancy orterm(notaftermolar).• b-HCGishigh(usuallyinfewthousands),butnotashighasmolar• Humanplacentallactogen(HPL)iselevated.• US:highlyvascularlesion.• Biopsy(D&C),sometimes-ve(difficultdiagnosis)• Locallyinvasive,doesn’tmetastasize.Resistanttochemoandradiotherapy.• Rx.:hysterectomyorwedgeresectiontopreservefertilityiflowornoparity. • b-HCG,CXR,CTBRAIN,ABDOMEN,USSPELVISAREUSEDTODEFINETHESCOREANDTHESTAGE.• Youdon’thavetoknowthedetailofscore,justknowthecutpointis7,itisdivededintotwogroupslowrisk
andhighrisk.• ThegoodthingaboutGTNischemoandradiosensetive,butnevergiveradiobecauseyouwilldestroyboth
ovaryandendometrium.
Done by Luluh Alzeghayer,435 <3
Related Documents











