Acute Respiratory Distress Syndrome Dr. Rikin Hasnani Post Graduate Dept Of Pulmonary Medicine SVS Medical College Mahabubnagar Telangana State

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Acute Respiratory Distress Syndrome
Dr. Rikin HasnaniPost Graduate
Dept Of Pulmonary MedicineSVS Medical College
MahabubnagarTelangana State

• Introduction• Pathophysiology • Clinical features• Management

Introduction And Definition • In 1967, Ashbaugh et al. described a syndrome characterized by the acute
onset of dyspnea, severe hypoxemia, diffuse lung infiltrates, and decreased respiratory system compliance in the absence of evidence for congestive heart failure (CHF).• In 1988, Murray and others introduced the Lung Injury Score (LIS), an
assessment tool for ARDS.• The LIS incorporates four parameters that are graded on a scale of 0 to 4: (1)
ratio of PaO2 to FIO2(PaO2/FIO2); (2) total respiratory compliance;(3) level of PEEP; and (4) extent of radiographic infiltrates.• In 1994 American European Consensus Conference (AECC) defined ARDS
and ALI.

Consensus Definition of ARDS• The AECC defines ARDS as the acute onset of illness with bilateral
chest radiographic infiltrates consistent with pulmonary edema, poor systemic oxygenation, and absence of evidence for left atrial hypertension. • The syndrome was referred to as ALI when the ratio of PaO2 to FIO2
(PaO2/FIO2); was ≤300, and ARDS when the ratio was ≤200.• Limitations of this Definition.

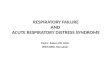
Berlin Definition - 2012
While the Berlin definition leaves the AECC definition of ARDS largely unchanged, the new definition addresses several specific ambiguities of the prior diagnostic criteria.

Epidemiology • Incidence 75 cases per lakh population• Mortality 26 to 58%• more people die annually with ARDS than from AIDS, asthma, and
breast cancer combined.• The most common causes of death among patients with ARDS arise
from the underlying insult or subsequent nosocomial pneumonia and sepsis. • Only rarely do patients die from progressive hypoxia and respiratory
failure.

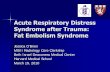
Cause of ARDS

Factors influencing risk of ARDS• Not all patients with an underlying cause (e.g., sepsis) of ARDS
develop the syndrome.• Clinical variables found to be associated with an increased risk of
ARDS include chronic alcohol abuse, hypoproteinemia, advanced age, increased severity, and extent of injury or illness as measured by injury severity score (ISS) or APACHE score, hypertransfusion of blood products, and cigarette smoking. • Diabetes mellitus and prehospitalization antiplatelet therapy appear
to decrease the risk of ARDS


Predicting ARDS-Lung injury prediction score (LIPS)• It is generated by sum of six predisposing factors and 9 risk modifiers.• six predisposing conditions are shock, aspiration, sepsis, pneumonia,
high-risk surgery, and high-risk trauma• nine risk modifiers alcohol abuse, obesity, hypoalbuminemia,
chemotherapy, need for oxygen, tachypnea, hypoxia, academia, and diabetes mellitus• The negative predictive value for a score <4 was 97%, while the
sensitivity and specificity for ARDS of a score >4 were 69% and 78%, respectively.

Pathophysiology • The essential factors that govern fluid exchange in the lungs are
expressed in the Starling equation for the microvascular barrier: Jv = LpS[(Pc – Pi) – σd(πc – πi)]The Starling equation predicts the development of two different kinds of pulmonary edema.Increased pressure pulmonary edemaIncreased permeability pulmonary edema


Stages of ARDS

Resolution of ARDS• Resolution of ARDS requires effective: • (1) reabsorption of alveolar edema, • (2) repair of the epithelial and endothelial barriers, and • (3) removal of inflammatory cells and exudates from the distal
airspaces.

Clinical Presentation• The development of ARDS usually follows a rapid course, occurring most
often within 12 to 72 hours of the predisposing event.• Dyspnea usually associated with agitation, anxiety.• As lung compliance decreases there is increased WOB, small tidal volume
and tachypnea.• The hallmark of ARDS is hypoxemia that is resistant to oxygen therapy
because of the large right-to left shunt.• Initially, patients may be able to compensate by hyperventilating, thereby
maintaining an acceptable PaO2 with an acute respiratory alkalosis.• Typically, patients deteriorate over several hours, requiring endotracheal
intubation and mechanical ventilation.

Differential Diagnosis of Acute Hypoxemic Respiratory Failure (AHRF)

Approach to clinical Diagnosis• Chest x ray

Lab investigations• Tropnin, BNP• LFT, RFT, hemogram• Bronchoscopy• Pancultures• Invasive hemodynamic monitoring is not recommended

Approach to Treatment• Treatment of respiratory system abnormalities• Diagnose and treat the precipitating cause of ARDS, if possible
• Maintain oxygenation, preferably using nontoxic FIO2 (<0.7), PEEP, or mechanical ventilation
• Prevent ventilator-induced lung injury (VILI) by using a low tidal volume ventilatory strategy with a limit (≤30 cm H2O) on static end-inspiratory airway pressure (plateau pressure)
• Keep pH in normal range without compromising goal to prevent VILI (but reverse a lifethreatening acidosis, even if it prevents meeting goal to prevent VILI)
• Enhance patient–ventilator synchrony and patient comfort by use of sedation, amnesia, opioid analgesia, and pharmacologic paralysis, if necessary
• Liberate or wean from mechanical ventilation when patient can breathe without assisted ventilation

• Treatment of nonrespiratory system abnormalities• Support or treat other organ system dysfunction or failure• General critical care (preventive and homeostatic measures)• Adequate early nutritional support

Treating inciting cause of ARDS

Maintaining Adequate oxygenation • High flow oxygen systems• Niv • Mechanical ventilation

Lung protective MV• In contrast to the typical diffuse-appearing
pattern noted on plain chest radiographs, the pattern of consolidation, atelectasis, and normal alveoli is actually heterogeneous.
• The key physiologic implication of these observations is that a ventilator-delivered tidal volume is preferentially distributed to the open alveoli, which represent only a small fraction of the entire lung, BABY LUNG


• The goals of lung-protective ventilation are to avoid injury due to overexpansion of alveoli during inspiration (so-called “volu-trauma”) and injury due to repetitive opening and closing of alveoli during inspiration and expiration (so-called “atelecta-trauma”). • The term “bio-trauma” encompasses the direct lung injury and the
concomitant release of inflammatory cytokines that produce remote cell death or organ injury.

Ventilator Strategy in ARDS1. Ventilator Setup and Adjustment2. Oxygenation Goal: PaO2 = 55–80 mm Hg or SpO2 = 88–95%3. Plateau Pressure (Pplat) goal:≤30 cm H2O4. pH Goal: 7.30–7.45

Ventilator Setup and Adjustment• 1. Calculate ideal body weight (IBW)a (also known as predicted body weight
[PBW])• 2. Use Assist/Control mode and set initial TV to 8 mL/kg IBW (if baseline TV
>8 mL/kg)• 3. Reduce TV by 1 mL/kg at intervals ≤2 h until TV = 6 mL/kg IBW• 4. Set initial rate to approximate baseline minute volume (but not >35 bpm)• 5. Adjust TV and RR to achieve pH and plateau pressure (Pplat) goals below.• 6. Set inspiratory flow rate above patient demand (usually >80 L/min);
adjust flow rate to achieve goal of I:E ratio of 1:1.0–1.3

Oxygenation Goal:• Goal is PaO2 = 55–80 mm Hg or SpO2 = 88–95%• 1. Use these incremental FIO2-PEEP combinations to achieve
oxygenation goal

Plateau Pressure (Pplat) goal:≤30 cm H2O• 1. Check Pplat (use 0.5-s inspiratory pause), SpO2, total RR, TV, and
ABG (if available) at least every 4 h and after each change in PEEP or TV.• 2. If Pplat >30 cm H2O, decrease TV by 1 mL/kg steps (minimum 4
mL/kg IBW)• 3. If Pplat <25 cm H2O and TV <6 mL/kg, increase TV by 1 mL/kg until
Pplat >25 cm H2O or TV = 6 mL/kg.• 4. If Pplat <20 cm H2O and breath stacking occurs, one may increase
TV in 1 mL/kg increments (to a maximum of 8 mL/kg)

pH Goal: 7.30–7.45• Acidosis management: pH <7.30• 1. If pH = 7.15–7.30, increase RR until pH >7.30 or PaCO2 <25 mm Hg
(maximum RR = 35); if RR = 35 and PaCO2 <25 mm Hg, may give NaHCO3• 2. If pH <7.15 and NaHCO3 considered or infused, TV may be
increased in 1 mL/kg steps until pH>7.15 (Pplat goal may be exceeded)

Rescue” or “Salvage” Interventions Used in Patients with ARDS and Severe Hypoxemia Resistant to Conventional Mechanical Ventilation and PEEP• Corticosteroids• Extracorporeal CO2 removal (ECCO2R)• Extracorporeal membrane oxygenation (ECMO)• High-frequency oscillatory ventilation (HFOV)• Inhaled nitric oxide (NO) or inhaled prostacyclin (epoprostenol/iloprost)• Pressure-controlled inverse ratio ventilation (PC-IRV)• Prone positioning• Recruitment maneuvers• Tracheal gas insufflation (TGI)

Corticosteroid

• The study revealed no differences in 60- or 180-day mortality rates. • Although parameters of respiratory function, including PaO2/FIO2; plateau
pressure; respiratory system compliance; and time to, and rate of, liberation from mechanical ventilation improved after corticosteroid administration; the corticosteroid treated group included more patients who returned to assisted ventilation. • Furthermore, no statistically significant differences between treated and
untreated groups in ICU or hospital days by 180 days were observed. • In addition, more adverse events related to weakness occurred in the
treated group than in those receiving placebo.• Finally, patients treated with corticosteroids after 14 days of persistent
ARDS had a significantly increased mortality. • Hence, the results of this study do not support the routine use of steroids
for late phase ARDS in general, and they argue against their use if ARDS has been present for 14 days or longer.

Extracorporeal Life Support• Extracorporeal Life Support (ECLS) is a therapy that utilizes an external
artificial membrane and a mechanical pump to provide gas exchange and systemic perfusion in patients with failure of lung and/or heart function. • The use of extracorporeal gas exchange, is based on the hypothesis
that more patients will survive if the lung is allowed to recover from its injury by “resting” using extracorporeal gas exchange temporarily.• Extracorporeal membrane oxygenation (ECMO) and extracorporeal
CO2 removal (ECCO2R) are types of ECLS.

Death or severe disability, the study’s primary outcome, occurred in 53% of the conventional arm versus 37% of those referred to the ECMO center. Among those referred to the ECMO center, 76% received ECMO. While the study demonstrated a statistically significant finding, the study design makes it impossible to distinguish the effects of the ECMO therapy from those of a specialized referral center.

High-frequency oscillatory ventilation (HFOV)• High-frequency oscillatory ventilation (HFOV) is a mode of ventilation
in which patients are supported with rapid pressure oscillations that generate very small tidal volumes. • Theoretically, HFOV may be regarded as the ultimate low-tidal volume
ventilator.• There is no significant mortality benefit over usual icu care. So not
recommended

Inhaled NO• Given via inhalation, NO selectively vasodilates pulmonary capillaries
and arterioles that serve ventilated alveoli, diverting blood flow to these alveoli and away from areas of shunt. • Lowering of the pulmonary vascular resistance, accompanied by
lowering of the pulmonary artery pressure, appears maximal at very low concentrations (0.1 ppm) in patients with ARDS.• Inhaled NO has been studied in several controlled clinical trials in
patients with ARDS.• While demonstrating improvements in oxygenation in some patients,
inhaled NO did not improve survival in any of the trials.

Tracheal Gas Insufflation• Tracheal gas insufflation (TGI) consists of delivering fresh gas through
a modified endotracheal tube at a point just above the carina. • The additional gas flow (i.e., flow provided in addition to the standard
tidal volumes delivered by the ventilator) tends to remove CO2-rich gas from the trachea and smaller airways.• Disadvantage with TGI - tracheal erosion, oxygen toxicity related to
an increased FIO2, and hemodynamic compromise or barotrauma due to TGI-induced auto-PEEP and a larger tidal volume than the ventilator is set to deliver• its routine use is not recommended.

PCV -IRV• PCV can limit maximal peak airway pressure as well as end-inspiratory
pressure and, hence, is favored by some clinicians. • However, the end-inspiratory pressure in PCV can be underestimated• TV delivered at set pressure is compliance dependent. Tv will increase
as ARDS improves.• Inverse ratio ventilation (IRV) with PCV is based upon an inspiratory
time (I) greater than expiratory time (E), that is, I:E >1 . • Lengthening the inspiratory time increases mean airway pressure
because more of the respiratory cycle is spent in inspiration, which may translate into improvements in oxygenation.

Prone Ventilation• About two-thirds of patients with ARDS improve their oxygenation
after being placed in a prone position.• Mechanisms that improves oxygenation• (1) increased functional residual capacity; • (2) change in regional diaphragmatic motion; • (3) perfusion redistribution; and • (4) improved clearance of secretions.


Problems with prone ventilation • Patients managed in the prone position need special attention to
prevent pressure necrosis of the nose, face, and ears. • Extra care is also needed to ensure security and patency of the
endotracheal tube.• Pressure on the eye may result in retinal ischemia, especially in
hypotensive patients. • There are incidence of cardiac arrhythmias or hemodynamic
instability when turned prone.


Recruitment maneuver • Lung recruitment maneuvers are defined as the application of CPAP aimed at
“recruiting” or opening totally or partially collapsed alveoli. • The alveoli are then kept inflated during expiration using an appropriately
high level of PEEP.• Methods of recruitment 1. 40cmH20 for 40-60 seconds2. 3 consecutive sighs/min with a plateau pressure of 45cmH2O3. 2 minutes of peak pressure of 50cmH2O and PEEP above upper inflection
point (obese/trauma patients may require >60-70cmH2O)4. long slow increase in inspiratory pressure up to 40 cmH2O (RAMP)5. stepped increase in pressure (e.g. Staircase Recruitment Manoeuvre)

Fluid therapy

• FACTT investigators developed a detailed fluid management protocol that, except for patients in shock (mean arterial pressure [MAP] less than 60 mm Hg or on vasopressors for hypotension), used four basic input variables (assessed every 1–4 hours) to determine the fluid management instructions:• (1) MAP; • (2) urine output; • (3) effectiveness of circulation; and • (4) intravascular pressure (central venous pressure [CVP] or PAOP


Other therapies • Neuromuscular blocking agent• Beta agonists• Macrolide • Statins

THANK YOU
Related Documents