




1
Value Analysis Brief: Operative Fixation for Flail Chest
DJ11092B

2DJ11092B
Abstract
• Background: Flail chest is a life-threatening injury typically treated with supportive ventilation and analgesia. Some evidence now suggests rib fixation can improve patient outcomes. The purposeof this brief is to summarize the clinical and economic value ofoperative fixation for treatment of flail chest based on currentevidence.
• Methods: Informed by comparative, peer-reviewed literature published after 1990 on clinical and economic outcomes after operative fixation of flail chest or rib fracture. Both MEDLINE and EMBASE databases were queried.
• Results: Seven manuscripts compared rib fixation vs. non-operative management of rib fractures. Analysis of the data showed patients treated with rib fixation were 60% less likely to die, 70% less likely to get infection/pneumonia, on average received 6 fewer days of ventilation, and on average were in the ICU for 8 fewer days compared to non-operative management. Assessment of hospital economic data also demonstrated favorable results for rib fixation over non-operative management.
• Abstract
• Introduction and Methods
• Burden of Flail Chest
• Role of Fixation in the Care Pathway
• Results
• Mortality
• Infection/Pneumonia
• Ventilator Dependence
• Total ICU days
• Economics
• About MatrixRIB
• Limitations
Limitations: Though data were pooled via meta analysis to increase statistical power, most included studies were small. Furthermore, only two of the seven comparative studies were prospective in design. Retrospective comparative studies, particularly those with non-concurrent controls, are subject to risk and indication biases. All comparative outcomes were short-term in nature.

3DJ11092B
Introduction and Methods
• This value analysis brief summarizes the clinical and economic value of operative fixation for treatment of flail chest.
• The contents of this value analysis brief were informed by:
– Comparative, peer-reviewed literature published after 1990 on clinical and economic outcomes after operative fixation of flail chest or rib fracture. Both MEDLINE and EMBASE databases were queried.
• Where possible, data from multiple studies were pooled using random effects meta analysis.
• Abstract
• Introduction and Methods
• Burden of Flail Chest
• Role of Fixation in the Care Pathway
• Results
• Mortality
• Infection/Pneumonia
• Ventilator Dependence
• Total ICU days
• Economics
• About MatrixRIB
• Limitations
4DJ11092B
Flail chest is associated with significant mortality and morbidity.
• Commonly defined as unilateral fractures of at least 3 consecutive ribs, each with 2 or more fractures.1
– The flail segment moves paradoxically (outward with expiration and inward with inspiration), contributing to respiratory compromise.
• Occurs in 5-13% of patients with chest wall trauma, most commonly resulting from motor vehicle accidents2
• Mortality between 10 – 20%3
• Abstract
• Introduction and Methods
• Burden of Flail Chest
• Role of Fixation in the Care Pathway
• Results
• Mortality
• Infection/Pneumonia
• Ventilator Dependence
• Total ICU days
• Economics
• About MatrixRIB
• Limitations
1. Helzel I, Long W, Fitzpatrick D, Madey S, Bottlang M. Evaluation of intramedullary rib splints for less-invasive stabilisation of rib fractures. Injury [Internet]. 2009 Oct;40(10):1104–10.
2. Wanek S, Mayberry JC. Blunt thoracic trauma: flail chest, pulmonary contusion, and blast injury. Critical Care Clinics [Internet]. 2004 Jan 29];20(1):71–81.
3. Simon B, Ebert J, Bokhari F, Capella J, Emhoff T, Hayward T, et al. Management of pulmonary contusion and flail chest: an Eastern Association for the Surgery of Trauma practice management guideline. The journal of trauma and acute care surgery [Internet]. 2012 Nov ;73(5 Suppl 4):S351–61.
5DJ11092B
Flail chest is associated with significant mortality and morbidity (cont.)
• Patients with flail chest commonly have multiple, non-thoracic injuries, including traumatic brain injury.1
• Respiratory compromise in patients with flail chest frequently warrants mechanical ventilation (MV), particularly in the presence of concomitant pulmonary contusion.1
• Impaired pulmonary function and/or prolonged mechanical ventilation can increase risk for potentially fatal complications, including
– pneumonia,
– sepsis, and
– atelectasis.2
• Abstract
• Introduction and Methods
• Burden of Flail Chest
• Role of Fixation in the Care Pathway
• Results
• Mortality
• Infection/Pneumonia
• Ventilator Dependence
• Total ICU days
• Economics
• About MatrixRIB
• Limitations
1. Wanek 20042. Shackford SR. Analytic Review: Blunt Chest Trauma: The Intensivist’s Perspective. Journal of Intensive Care Medicine
[Internet]. 1986 May 1; (3):125–36

6DJ11092B
Patients with flail chest are reported to suffer from long-term pain and disability.
• The following have been observed after long-term follow up of patients with flail chest:
– persistent chest wall pain1,2,
– chest wall deformity2,
– dyspnea on exertion1, and
– prolonged disability.1
• Abstract
• Introduction and Methods
• Burden of Flail Chest
• Role of Fixation in the Care Pathway
• Results
• Mortality
• Infection/Pneumonia
• Ventilator Dependence
• Total ICU days
• Economics
• About MatrixRIB
• Limitations
1. Landercasper J, Cogbill T, Lindesmith L. Long-term Disability after flail chest injury. Journal of Trauma. 1984;24(5):410–4.2. Simon 2012

7DJ11092B
The clinical burden of flail chest is associated with significant economic impact.
• In the US, patients with flail chest are in the hospital an average of 15 days, predominantly in the intensive care setting.1
– Costs per incremental ICU day without MV = $3,9022
– Costs per incremental ICU day with MV = $4,9452
• More than 30% of patients require additional care in post-acute settings.1
• Indirect, societal costs result from inability to work or reduced workplace productivity.
• Abstract
• Introduction and Methods
• Burden of Flail Chest
• Role of Fixation in the Care Pathway
• Results
• Mortality
• Infection/Pneumonia
• Ventilator Dependence
• Total ICU days
• Economics
• About MatrixRIB
• Limitations
1. Healthcare Cost and Utilization Project. 2010. Hospital discharges with International Classification of Diseases, Clinical Modification, 9th Revision (ICD-9-CM) for flail chest (807.4) as a primary diagnosis.
2. Dasta JF, McLaughlin TP, Mody SH, Piech CT. Daily cost of an intensive care unit day: The contribution of mechanical ventilation*. Critical Care Medicine [Internet]. 2005 Jun;33(6):1266–71. NOTE: updated from $US 2005 to $US 2013 using a 1.28 inflation multiplier from the Medical Care Component of the CPI-U. NOTE: Data from table 7 for 3+ days, trauma patients.
8DJ11092B
Surgical fixation has been adopted for a selectsubset of patients with flail chest.
• According to guidelines from the Eastern Association for the Surgery of Trauma (EAST):1
• The UK’s National Institute for Health and Clinical Excellence (NICE) has concluded the following:2
• Abstract
• Introduction and Methods
• Burden of Flail Chest
• Role of Fixation in
the Care Pathway
• Results
• Mortality
• Infection/Pneumonia
• Ventilator Dependence
• Total ICU days
• Economics
• About MatrixRIB
• Limitations
1. Simon 20122. National Institute for Health and Clinical Excellence IPG 361 www.nice.org.uk/guidance/IPG361
“Surgical fixation may be considered in cases of severe flail chest failing to wean from the ventilator or when thoracotomy is required for other reasons.”
“Current evidence on insertion of metal rib reinforcements to stabilise a flail chest wall is limited in quantity but consistently shows efficacy. In addition, there are no major safety concerns in the context of patients who have had severe trauma with impaired pulmonary function.”
9DJ11092B
Surgical fixation has been adopted for a selectsubset of patients with flail chest (cont.)
• Lafferty and colleagues offer additional considerations for operative fixation of flail chest, including:1
– Failure to wean from ventilator;
– Paradoxical movement visualized during weaning;
– The extent of pulmonary contusion; and
– No substantial brain injury.
• Abstract
• Introduction and Methods
• Burden of Flail Chest
• Role of Fixation in
the Care Pathway
• Results
• Mortality
• Infection/Pneumonia
• Ventilator Dependence
• Total ICU days
• Economics
• About MatrixRIB
• Limitations
1. Lafferty PM, Anavian J, Will RE, Cole P a. Operative treatment of chest wall injuries: indications, technique, and outcomes. The Journal of bone and joint surgery. American volume [Internet]. 2011 Jan 5;93(1):97–110.

10DJ11092B
Two prospective and five retrospective studies
compared outcomes between fixation and nonoperative management of flail chest.
• Abstract
• Introduction and Methods
• Burden of Flail Chest
• Role of Fixation in the Care Pathway
• Results
• Mortality
• Infection/Pneumonia
• Ventilator Dependence
• Total ICU days
• Economics
• About MatrixRIB
• Limitations
Author (year)Study design
CountrySample
SizeFixation Method
Ahmed (1995)1 Retrospective UAE 64 K-wires
Balci (2004)2 Retrospective Turkey 64 Suture and traction
Granetzny (2005)3Prospective, randomized
Germany 40 K-wires or steel wire
Nirula (2006)4 Retrospective USA 60 Adkin struts
Solberg (2009)5 Retrospective USA 16 Titanium plates
Tanaka (2002)6Prospective, randomized
Japan 37 Judet struts
Voggenreiter (1998)7
Retrospective Germany 42Rib clamp or pelvic reconstruction plate
Comparative Studies, Fixation Versus Nonoperative Management of Flail Chest
1. Ahmed Z, Z Mohyuddin,“Management of Flail Chest Injury: Internal Fixation versus Endotrachial Intubation and Ventilation”, J Thoracic and Cardiovascular Surgery, 1995;1676–1680.
2. Balci AE, Eren S, Cakir O, Eren MN. Open fixation in flail chest: review of 64 patients. Asian Cardiovasc Thorac Ann 2004;12:11e15.3. Granetzny A, Abd El-Aal M, Emam E, Shalaby A, Boseila A. Surgical versus conservative treatment of flail chest. Evaluation of the pulmonary status. Interactive
cardiovascular and thoracic surgery [Internet]. 2005 Dec;4(6):583–7.4. Nirula R, Allen B, Layman R, Falimirski ME, Somberg. Rib fracture stabilization in patients sustaining blunt chest injury. Am Surg 2006; 72:307–309.5. Solberg BD, Moon CN, Nissim A a, Wilson MT, Margulies DR. Treatment of chest wall implosion injuries without thoracotomy: technique and clinical outcomes.
The Journal of trauma [Internet]. 2009 Jul;67(1):8–13.6. Tanaka H, Yukioka T, Yamaguti Y, Shimizu S, Goto H, Matsuda H, et al. Surgical stabilization of internal pneumatic stabilization? A prospective randomized
study of management of severe flail chest patients. The Journal of trauma [Internet]. 2002 Apr;52(4):727–327. Voggenreiter G, Neudeck F, Aufmkolk M, Obertacke U, Schmit-Neuerburg KP. Operative chest wall stabilization in flail chest—outcomes of patients with or
without pulmonary contusion. J Am Coll Surg 1998;187:130–48.

11DJ11092B
Study or Subgroup
Ahmed 1995
Balci 2004
Granetzny 2005
Voggenreiter 1998
Total (95% CI)
Total events
Heterogeneity: Tau² = 0.00; Chi² = 0.68, df = 3 (P = 0.88); I² = 0%
Test for overall effect: Z = 2.68 (P = 0.007)
Events
2
3
2
3
10
Total
26
27
20
20
93
Events
11
10
3
8
32
Total
38
37
20
22
117
Weight
21.8%
31.0%
15.6%
31.6%
100.0%
M-H, Random, 95% CI
0.27 [0.06, 1.10]
0.41 [0.12, 1.35]
0.67 [0.12, 3.57]
0.41 [0.13, 1.34]
0.40 [0.21, 0.78]
Fixation No Fixation Risk Ratio Risk Ratio
M-H, Random, 95% CI
0.05 0.2 1 5 20Favours fixation Favours no fixation
Patients who received operative fixation for flail chest
were approximately 60% less likely to die from sustained injuries than patients treated nonoperatively.
• Abstract
• Introduction and Methods
• Burden of Flail Chest
• Role of Fixation in the Care Pathway
• Results
• Mortality
• Infection/Pneumonia
• Ventilator Dependence
• Total ICU days
• Economics
• About MatrixRIB
• Limitations
Meta analysis of Relative Risk of Death, Fixation versus No fixation for Flail Chest

12DJ11092B
• Abstract
• Introduction and Methods
• Burden of Flail Chest
• Role of Fixation in the Care Pathway
• Results
• Mortality
• Infection/Pneumonia
• Ventilator Dependence
• Total ICU days
• Economics
• About MatrixRIB
• Limitations
Meta analysis, Relative Risk of Chest Infection/Pneumonia Risk, Fixation versus No fixation for Flail Chest
Chest infection or pneumonia were approximately 70% less likely to occur among patients who received
operative fixation.
Study or Subgroup
Ahmed 1995
Balci 2004
Granetzny 2005
Solberg 2009
Tanaka 2002
Voggenreiter 1998
Total (95% CI)
Total events
Heterogeneity: Tau² = 0.00; Chi² = 3.78, df = 5 (P = 0.58); I² = 0%
Test for overall effect: Z = 4.81 (P < 0.00001)
Events
4
0
2
0
4
4
14
Total
26
27
20
9
18
20
120
Events
19
8
10
3
17
7
64
Total
38
37
20
7
19
22
143
Weight
27.1%
3.1%
12.9%
3.1%
32.1%
21.7%
100.0%
M-H, Random, 95% CI
0.31 [0.12, 0.80]
0.08 [0.00, 1.33]
0.20 [0.05, 0.80]
0.11 [0.01, 1.91]
0.25 [0.10, 0.60]
0.63 [0.22, 1.83]
0.29 [0.18, 0.48]
Fixation No Fixation Risk Ratio Risk Ratio
M-H, Random, 95% CI
0.01 0.1 1 10 100Favours fixation Favours no fixation
13DJ11092B
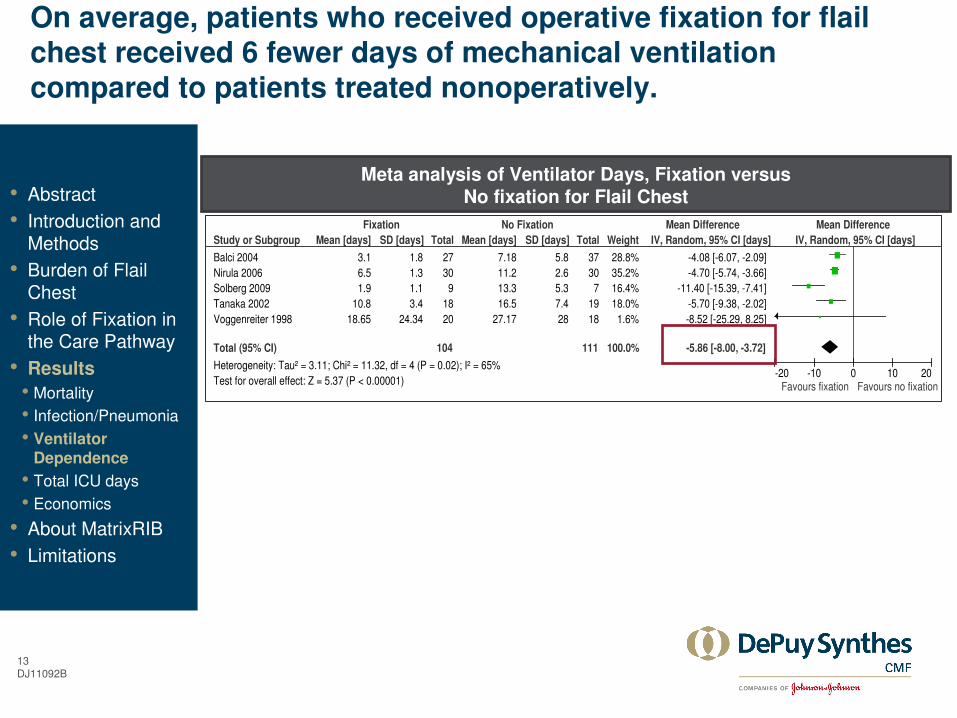
Study or Subgroup
Balci 2004
Nirula 2006
Solberg 2009
Tanaka 2002
Voggenreiter 1998
Total (95% CI)
Heterogeneity: Tau² = 3.11; Chi² = 11.32, df = 4 (P = 0.02); I² = 65%
Test for overall effect: Z = 5.37 (P < 0.00001)
Mean [days]
3.1
6.5
1.9
10.8
18.65
SD [days]
1.8
1.3
1.1
3.4
24.34
Total
27
30
9
18
20
104
Mean [days]
7.18
11.2
13.3
16.5
27.17
SD [days]
5.8
2.6
5.3
7.4
28
Total
37
30
7
19
18
111
Weight
28.8%
35.2%
16.4%
18.0%
1.6%
100.0%
IV, Random, 95% CI [days]
-4.08 [-6.07, -2.09]
-4.70 [-5.74, -3.66]
-11.40 [-15.39, -7.41]
-5.70 [-9.38, -2.02]
-8.52 [-25.29, 8.25]
-5.86 [-8.00, -3.72]
Fixation No Fixation Mean Difference Mean Difference
IV, Random, 95% CI [days]
-20 -10 0 10 20Favours fixation Favours no fixation
On average, patients who received operative fixation for flail chest received 6 fewer days of mechanical ventilation
compared to patients treated nonoperatively.
• Abstract
• Introduction and Methods
• Burden of Flail Chest
• Role of Fixation in the Care Pathway
• Results
• Mortality
• Infection/Pneumonia
• Ventilator Dependence
• Total ICU days
• Economics
• About MatrixRIB
• Limitations
Meta analysis of Ventilator Days, Fixation versus No fixation for Flail Chest

14DJ11092B
On average, patients who received operative fixation
for flail chest were in the ICU for 8 fewer days than those who received nonoperative care.
• Abstract
• Introduction and Methods
• Burden of Flail Chest
• Role of Fixation in the Care Pathway
• Results
• Mortality
• Infection/Pneumonia
• Ventilator Dependence
• Total ICU days
• Economics
• About MatrixRIB
• Limitations
Meta analysis of ICU Days, Fixation versus No fixation for Flail Chest
Study or Subgroup
Nirula 2006
Solberg 2009
Tanaka 2002
Total (95% CI)
Heterogeneity: Tau² = 43.44; Chi² = 11.93, df = 2 (P = 0.003); I² = 83%
Test for overall effect: Z = 1.93 (P = 0.05)
Mean [days]
12.1
5.4
16.5
SD [days]
2.7
1.5
7.4
Total
30
9
18
57
Mean [days]
14.1
21
26.8
SD [days]
2.7
13.6
13.2
Total
30
7
19
56
Weight
41.4%
25.9%
32.7%
100.0%
IV, Random, 95% CI [days]
-2.00 [-3.37, -0.63]
-15.60 [-25.72, -5.48]
-10.30 [-17.15, -3.45]
-8.24 [-16.60, 0.12]
Fixation No Fixation Mean Difference Mean Difference
IV, Random, 95% CI [days]
-20 -10 0 10 20Favours fixation Favours no fixation

15DJ11092B
Two studies from the meta analysis, as well as one publication on the cost of ICU days, permitted estimation of the potential economic impact of fixation for flail chest on US hospitals.
• Abstract
• Introduction and Methods
• Burden of Flail Chest
• Role of Fixation in the Care Pathway
• Results
• Mortality
• Infection/Pneumonia
• Ventilator Dependence
• Total ICU days
• Economics
• About MatrixRIB
• Limitations
• Mean days in the ICU (with and without mechanical ventilation) were calculated for patients with and without fixation from Nirula (2006) and Solberg (2009).
• Using an inflation factor from the Medical Care Component of the Consumer Price Index for Urban Consumers (CPI-U), $US 2013 costs for ICU days were estimated from Dasta (2005): $3,902/day without mechanical ventilation and $4,945 with mechanical ventilation.
• Implant costs for patients undergoing fixation were estimated from manufacturer list prices1, as well as a recent study on operative fixation of flail chest.2
• Estimated operating room costs ($25/minute x 171 minutes) were derived per-minute charges in the operating room updated to $2013 using the Medical Care Component of the CPI-U3, as well as on mean operating room time for rib fixation.2
1. DePuy Synthes data on file. 2. Bottlang M, Long WB, Phelan D, Fielder D, Madey SM. Surgical stabilization of flail chest injuries with MatrixRIB implants: A prospective
observational study. Injury [Internet]. Elsevier Ltd; 2013 Mar;44(2):232–8.3. OR costs estimated to be $25 per minute: derived from operating room charges of $62/minute updated to $US 2013 using the Medical
Care Component of CPI-U and converted to costs using national average cost-to-charge ratio of .30, informed by the following data sources: Shippert RD. A study of time-dependent operating room fees and how to save $100,000 by using time-saving products. American Journal of Cosmetic Surgery 2005; 22 (25-34) and Dalton K, Freeman S, Bragg A. Refining cost to charge ratios for calculating APC and MS-DRG relative payment weights. RTI International. CMS Contract No. HHSM-500-2005-0029I. July 2008.
Author (year)
Mean ICU days,
without MV
Mean ICU days,
with MVSample Size
FixationNo
fixationFixation
No fixation
Fixation No fixation
Nirula (2006) 5.6 2.9 6.5 11.2 30 30
Solberg (2009) 3.5 7.7 1.9 13.3 9 7
Mean days,
weighted average5.1 3.8 5.4 11.6 39 37

16DJ11092B
Operative fixation may reduce hospital costs for management for flail chest by approximately 17% due to reductions in ICU and mechanical ventilation days.
• Abstract
• Introduction and Methods
• Burden of Flail Chest
• Role of Fixation in the Care Pathway
• Results
• Mortality
• Infection/Pneumonia
• Ventilator Dependence
• Total ICU days
• Economics
• About MatrixRIB
• Limitations
*Weighted mean days in ICU with mechanical ventilation (MV) from Nirula (2006) and Solberg (2009) = 5.4 with fixation vs.11.6 without fixation; weighted mean days in ICU without MV = 5.1 days with fixation vs. 3.8 days without fixation. ICU and MV Costs derived from Dasta (2005) and updated to $US 2013 using the Medical Care Component of the Consumer Price Index. ICU costs without MV = $3,902 and with MV = $4,945. Implant costs and mean OR time of 171 minutes based on 2013 list prices of MatrixRIB and utilization data from Bottlang M, Long WB, Phelan D, Fielder D, Madey SM. Surgical stabilization of flail chest injuries with MatrixRIB implants: A prospective observational study. Injury [Internet]. Elsevier Ltd; 2013 Mar;44(2):232–8.
OR costs estimated to be $25 per minute: derived from operating room charges of $62/minute updated to $US 2013 using the Medical Care Component of CPI-U and converted to costs using national average cost-to-charge ratio of .30, informed by the following data sources: Shippert RD. A study of time-dependent operating room fees and how to save $100,000 by using time-saving products. American Journal of Cosmetic Surgery 2005; 22 (25-34) and Dalton K, Freeman S, Bragg A. Refining cost to charge ratios for calculating APC and MS-DRG relative payment weights. RTI International. CMS Contract No. HHSM-500-2005-0029I. July 2008.
Potential Perioperative Cost Differences for US Hospitals, Fixation vs. No Fixation*
NOTE: Costs and hospital length of stay vary by individual hospitals. As such, the above results may not be applicable to your institution.

17DJ11092B
From payer and societal perspectives, operative fixation may be cost-effective relative to nonoperative management of flail chest.
• Abstract
• Introduction and Methods
• Burden of Flail Chest
• Role of Fixation in the Care Pathway
• Results
• Mortality
• Infection/Pneumonia
• Ventilator Dependence
• Total ICU days
• Economics
• About MatrixRIB
• Limitations
• An economic model showed operative fixation for flail chest to be less costly and offer quality-of-life benefits relative to nonoperative management:1
– US Medicare costs were predicted to be ($17,162 vs. $22,537, for operative and nonoperative management of flail chest, respectively).
– Operative fixation also offered quality-of-life benefits relative to nonoperative management.
• Tanaka et al. (2002) also reported lower medical costs for Japanese public health insurance for patients who received operative fixation relative to those who received nonoperative management ($13,455 vs. $23,423, p < 0.05).2
1. Bhatnagar A, Mayberry J, Nirula R. Rib fracture fixation for flail chest: what is the benefit? Journal of the American College of Surgeons [Internet]. Elsevier Inc.; 2012 Aug:201–5.
2. Tanaka 2002.
NOTE: Costs and hospital length of stay vary across individual hospitals, payers, and countries. As such, the above results may not be locally applicable.
18DJ11092B
MatrixRIB System
• Abstract
• Introduction and Methods
• Burden of Flail Chest
• Role of Fixation in the Care Pathway
• Results
• Mortality
• Infection/Pneumonia
• Ventilator Dependence
• Total ICU days
• Economics
• About MatrixRIB
• Limitations
19DJ11092B
The MatrixRIB Fixation System was designed to
provide stable fixation of normal and osteoporotic ribs.
• Abstract
• Introduction and Methods
• Burden of Flail Chest
• Role of Fixation in the Care Pathway
• Results
• Mortality
• Infection/Pneumonia
• Ventilator Dependence
• Total ICU days
• Economics
• About MatrixRIB
• Limitations
• Pre-contoured titanium alloy locking low-profile 1.5mm plates with 2.9mm locking screws
– Plates precontoured to fit average rib shape, which minimizes intraoperative bending
– Plate stiffness similar to cadaveric osteoporotic rib*, allows for flexibility of the rib cage
– Plates long enough to fixate multiple and comminuted/oblique fractures
– Anterior plating technique minimizes disruption of intercostal soft tissues
• Intramedullary splints enable minimally invasive approach
• Specialized instrumentation
NOTE: The MatrixRIB System was not the fixation device used in any of the previously referenced clinical studies. Please refer to the MatrixRIB technique guide and package insert for full indications, contraindications, instructions for use, warnings and/or precautions.
*Data on file in DePuySynthes test report MT08-481. Mechanical test results are not
necessarily indicative of clinical performance.
20DJ11092B
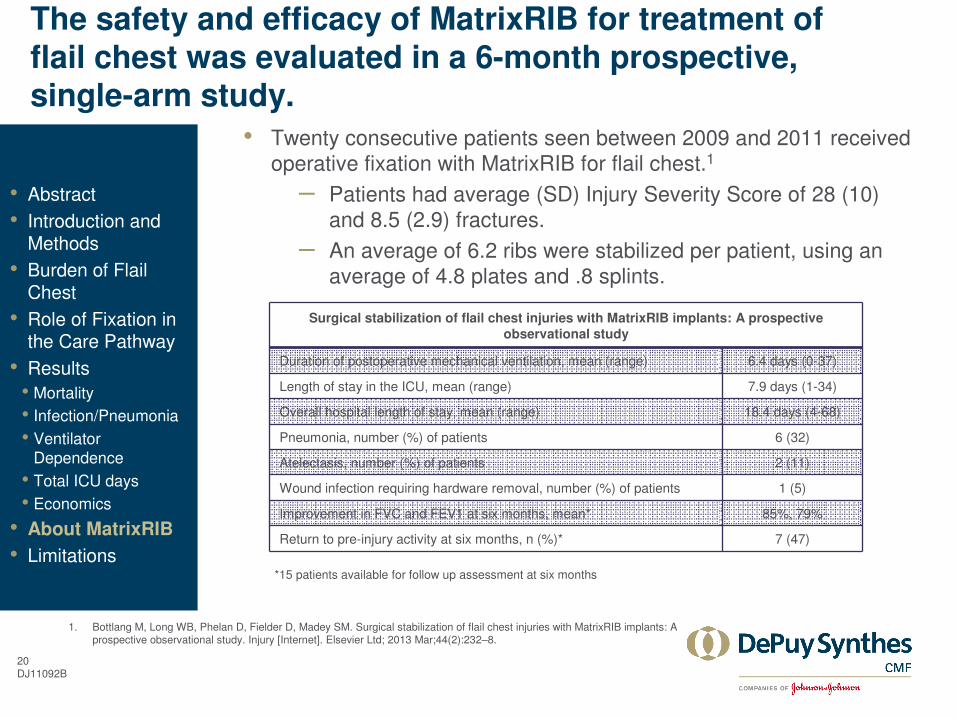
The safety and efficacy of MatrixRIB for treatment of
flail chest was evaluated in a 6-month prospective, single-arm study.
• Abstract
• Introduction and Methods
• Burden of Flail Chest
• Role of Fixation in the Care Pathway
• Results
• Mortality
• Infection/Pneumonia
• Ventilator Dependence
• Total ICU days
• Economics
• About MatrixRIB
• Limitations
• Twenty consecutive patients seen between 2009 and 2011 received operative fixation with MatrixRIB for flail chest.1
– Patients had average (SD) Injury Severity Score of 28 (10) and 8.5 (2.9) fractures.
– An average of 6.2 ribs were stabilized per patient, using an average of 4.8 plates and .8 splints.
Surgical stabilization of flail chest injuries with MatrixRIB implants: A prospective
observational study
Duration of postoperative mechanical ventilation, mean (range) 6.4 days (0-37)
Length of stay in the ICU, mean (range) 7.9 days (1-34)
Overall hospital length of stay, mean (range) 18.4 days (4-68)
Pneumonia, number (%) of patients 6 (32)
Atelectasis, number (%) of patients 2 (11)
Wound infection requiring hardware removal, number (%) of patients 1 (5)
Improvement in FVC and FEV1 at six months, mean* 85%, 79%
Return to pre-injury activity at six months, n (%)* 7 (47)
*15 patients available for follow up assessment at six months
1. Bottlang M, Long WB, Phelan D, Fielder D, Madey SM. Surgical stabilization of flail chest injuries with MatrixRIB implants: A prospective observational study. Injury [Internet]. Elsevier Ltd; 2013 Mar;44(2):232–8.

21DJ11092B
Limitations of the evaluated studies
• Though data were pooled via meta analysis to increase statistical power, most included studies were small.
• Only two of the 7 comparative studies were prospective in design.
– Retrospective comparative studies, particularly those with non-concurrent controls, are subject to risk and indication biases.
• Neither patients nor assessors were blinded in any of the studies, introducing several forms of bias.
• All comparative outcomes were short-term in nature.
• Abstract
• Introduction and Methods
• Burden of Flail Chest
• Role of Fixation in the Care Pathway
• Results
• Mortality
• Infection/Pneumonia
• Ventilator Dependence
• Total ICU days
• Economics
• About MatrixRIB
• Limitations

22





























