TO INTEGRATE -- OR HOW?A Decision Model for Practices
Charles Cooper, PhD Director of Professional Affairs
North Carolina Psychological Association
APA State Leadership Conference March 10, 2013
THE EXPECTED ENVIRONMENT:
2

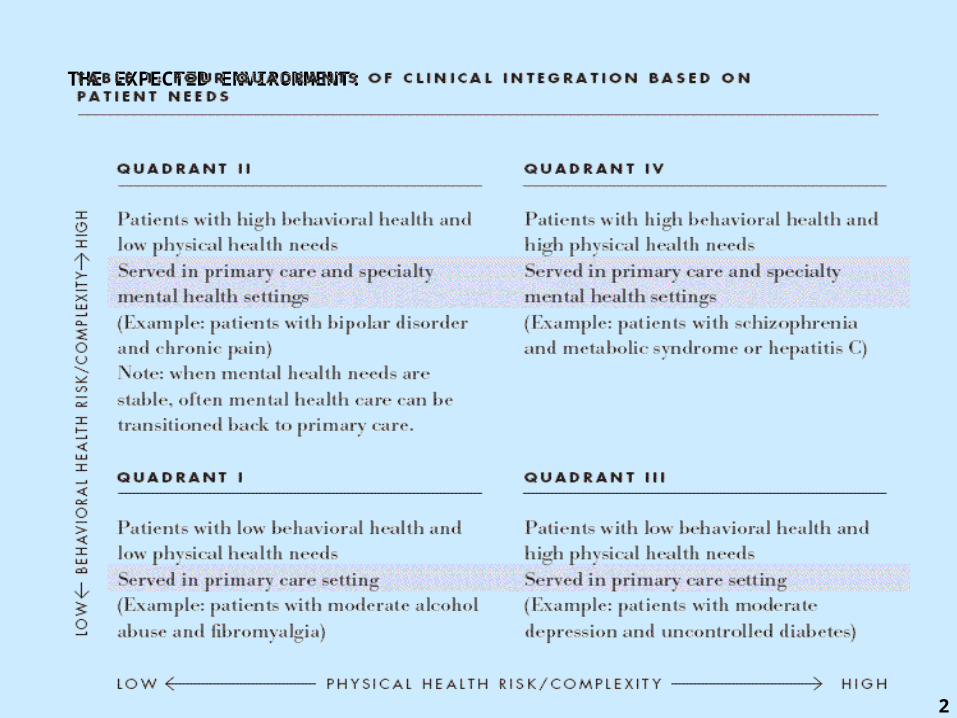
THE EXPECTED ENVIRONMENT
Low Physical Health Risk/Complexity
High Physical Health Risk/Complexity
High Behavioral Health Risk/Complexity
QUADRANT II
Clients served in primary care and specialty mental health settings
For treatment of: bipolar disorder, chronic pain
Note: with MH stable, care can be transitioned to PCP
QUADRANT IV
Clients served in primary care and specialty mental health settings
For treatment of: schizophrenia, metabolic syndrome or hepatitis C
Low Behavioral Health Risk/Complexity
QUADRANT I
Clients served in primary care setting
For treatment of: moderate alcohol abuse, fibromyalgia
QUADRANT III
Clients served in primary care setting
For treatment of: moderate depression, uncontrolled diabetes
THE MAUER MODEL
3

Integrated Care – The Individual Model
A Two-Dimension Model for Decision Making
I. Top Margin: Level of Integration occurs along a spectrum, from No Integration to Full Integration.
II. Side Margin: Actions would be based on the clinician's inclination towards integration and where the clinician is in his or her career.
4

The Individual Decision Model Level of Integration
Clinician Practice Qualities
No Integration
Maintain current practice format while keeping
watchful eye on developments
Ultra light IntegrationGreatly improve communication with targeted primary care
referral sources
Light Integration
Offering contracted services
to primary care, medical homes,
or ACOs
Moderate Integration“Co-Location”
maintaining part or all of a
practice within a primary care
setting
Full IntegrationAssuming an
employed position within an integrated setting
Early Career inclined toward integration
Early Career disinclined toward integration
Mid Career Inclined toward integration
Mid Career disinclined toward integration
Late Career inclined toward integration
Late Career disinclined toward integration
5
Level of Integration
Clinician Practice Qualities
No Integration
Ultra light Integration
Light Integration
Moderate Integration
Full Integration
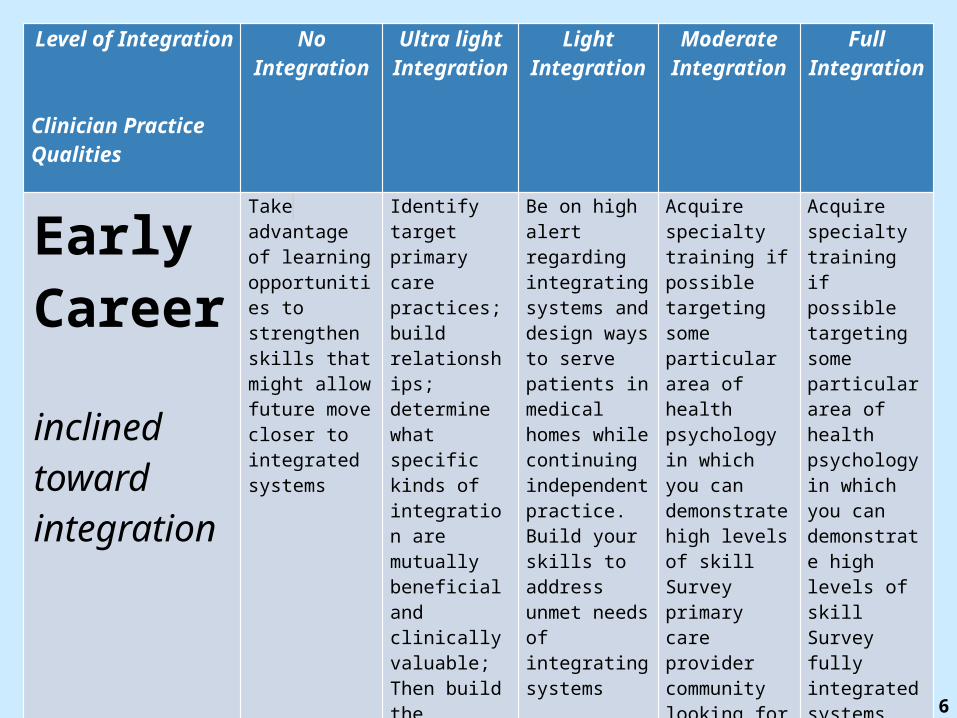
Early Career
inclined toward integration
Take advantage of learning opportunities to strengthen skills that might allow future move closer to integrated systems
Identify target primary care practices; build relationships; determine what specific kinds of integration are mutually beneficial and clinically valuable; Then build the collaboration
Be on high alert regarding integrating systems and design ways to serve patients in medical homes while continuing independent practice. Build your skills to address unmet needs of integrating systems
Acquire specialty training if possible targeting some particular area of health psychology in which you can demonstrate high levels of skillSurvey primary care provider community looking for co-location possibilities
Acquire specialty training if possible targeting some particular area of health psychology in which you can demonstrate high levels of skillSurvey fully integrated systems and their needs for behavioral health
6

Level of Integration
Clinician Practice Qualities
No Integration
Ultra light Integration
Light Integration
Moderate Integration
Full Integration
Early Career
disinclined toward integration
Develop a niche that will likely grow regardless of integration. Be prepared to change strategy should local system developments require it.
Identify one or more niches that hold promise for creating practice distinction. Build on that niche and be aware of how it could be affected by integration in the larger health system
Take advantage of medical homes and integrated systems and their organized care management. Seize marketing opportunities with care managers for niche offerings and specialized services not offered in the “home”
Take advantage of rapidly growing awareness of unmet behavioral needs of primary care patients. Seize marketing opportunities by offering niche services especially tailored to those unmet needs.
Take advantage of integrated systems and their organized care management. Seize opportunities with care coordinators for marketing your niche offerings and specialized services not offered in the “home”
7

Level of Integration
Clinician Practice Qualities
No Integration
Ultra light Integration
Light Integration
Moderate Integration
Full Integration
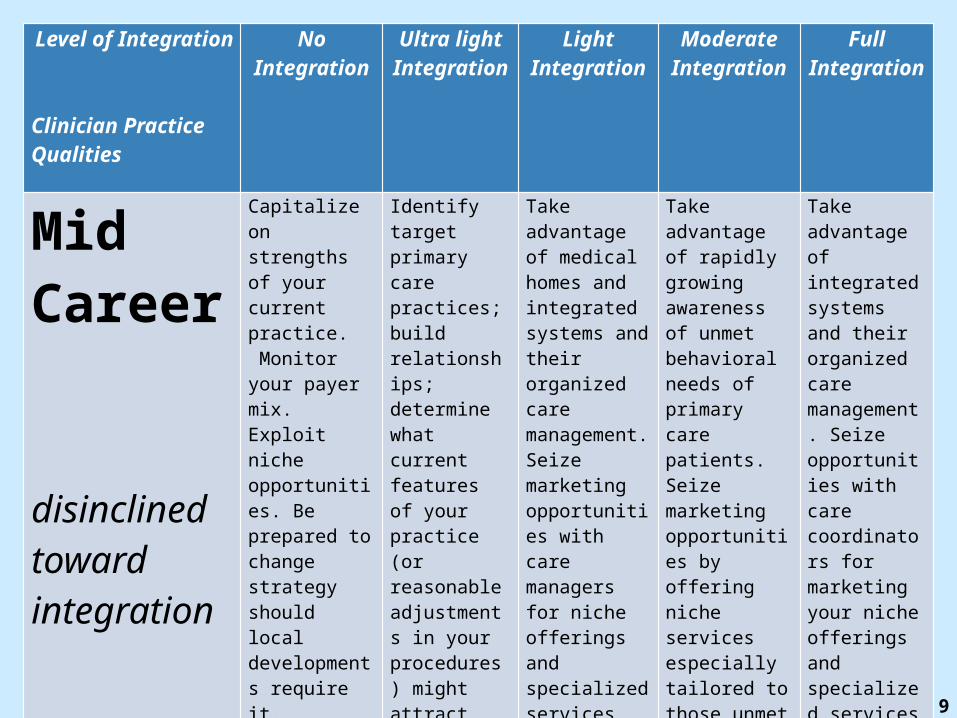
Mid Career
inclined toward integration
Capitalize on strengths of your current practice. Be prepared to change strategy should local developments require it.
Identify target primary care practices; build relationships; determine what specific kinds of integration are mutually beneficial and clinically valuable; Then build the collaboration
Take advantage of your practice reputation in the community. Watch for compatible primary care or “medical home” organizations – particularly ones with likely unmet needs for behavioral services for which they may need to refer out.
Take advantage of your practice reputation in the community. Survey primary care provider community looking for compatible co-location possibilities. Build relationships and explore how to put a “toe in the water”
Capitalize and build on skills and interests that may be sought by fully integrated systems. Acquire additional training in areas that may be in demand within those systems. Get to know the developing integrated systems and their needs. Build relationships.
8
Level of Integration
Clinician Practice Qualities
No Integration
Ultra light Integration
Light Integration
Moderate Integration
Full Integration
Mid Career
disinclined toward integration
Capitalize on strengths of your current practice. Monitor your payer mix. Exploit niche opportunities. Be prepared to change strategy should local developments require it.
Identify target primary care practices; build relationships; determine what current features of your practice (or reasonable adjustments in your procedures) might attract referrals; Then build the collaboration.
Take advantage of medical homes and integrated systems and their organized care management. Seize marketing opportunities with care managers for niche offerings and specialized services not offered in the “home”
Take advantage of rapidly growing awareness of unmet behavioral needs of primary care patients. Seize marketing opportunities by offering niche services especially tailored to those unmet needs.
Take advantage of integrated systems and their organized care management. Seize opportunities with care coordinators for marketing your niche offerings and specialized services not offered in the “home”
9

Level of Integration
Clinician Practice Qualities
No Integration
Ultra light Integration
Light Integration
Moderate Integration
Full Integration
LateCareer
inclined toward integration
Take advantage of reputation, “health orientation” and relationships. If necessary, adjust practice to respond to new referral patterns that may emerge with some large integrating systems
Identify target one or more primary care practices; Take advantage of reputation, “health orientation” and relationships to strengthen collaboration, communications, and coordination of care with mutual patients
Take advantage of your practice reputation in the community. Watch for compatible primary care or “medical home” organizations – particularly ones with likely unmet needs for behavioral services for which they may need to refer out.
If feasible, consider locating practice very near primary care setting or find other ways to reduce barriers to easy, “warm” referrals. Regular consultation / contact with primary care providers can approximate co-location
If skills, interests, financial rewards and other compatibilities make practice “inside” a fully integrated setting desirable, explore part of full time affiliation with such a setting. Assess your readiness to accept significant work culture change.
10

Level of Integration
Clinician Practice Qualities
No Integration
Ultra light Integration
Light Integration
Moderate Integration
Full Integration
LateCareer
disinclined toward integration
Maintain awareness of changes that may occur and diversify referral and payer mixes. Enhance niche aspects of practice.
Maintain awareness of changes that may occur and diversify referral and payer mixes. Enhance niche aspects of practice. Be open to making reasonable adjustments to foster referrals from primary care providers
Maintain awareness. Do an occasional assessment of yourself and of the developments in integrating health systems to ascertain if it is worth building relationships with, marketing to, and collaborating with primary health providers. See if what you already do can “sell” to them.
Watch with interest.
Watch with interest.
11
Integrated Care – The Practice Model
A Two-Dimension Model for Decision Making
I. Top Margin – Level of Integration: occurs along a spectrum, from No Integration to Full Integration.
II. Side Margin – Economic/Business Factors: strategic choices and actions would be based factors of “supply” and “demand” and an analysis of strengths, weaknesses, opportunites and threats, (SWOT).
12

Level of Integration
Business Conditions for Decision Making
No Integration
Ultra light Integration
Light Integration
Moderate Integration
Full Integration
Demand
•High and clear demand•Murky, ambiguous or unclear demand•Nil, low or mismatched demand
Supply
•Excellent•Uncertain, or Underdeveloped•Inadequate
Additional Factors
•SWOT•Wildcards
13
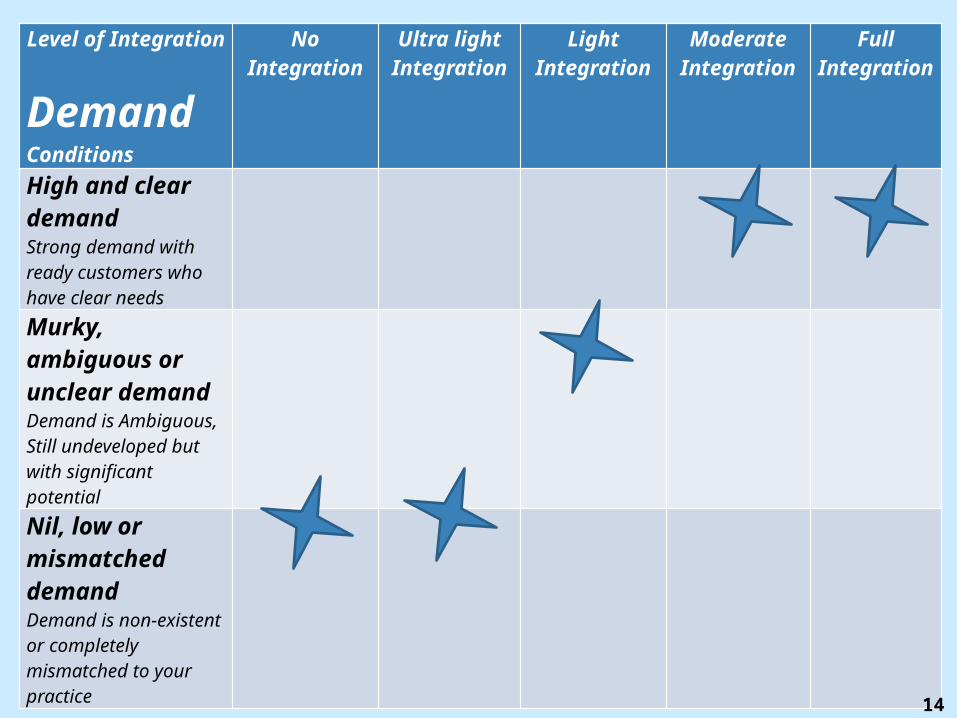
Level of Integration
Demand Conditions
No Integration
Ultra light Integration
Light Integration
Moderate Integration
Full Integration
High and clear demandStrong demand with ready customers who have clear needsMurky, ambiguous or unclear demandDemand is Ambiguous, Still undeveloped but with significant potentialNil, low or mismatched demandDemand is non-existent or completely mismatched to your practice
14

Integrated Care TablePractice Decision Model
None Collaboration FullIntegration Spectrum
Demand: High and Clear
Build relationships, Explore needs, Match resources to need, Make concrete proposals, Work out logistics, potential roles and workflow, Develop contracts, Coordinate and/or educate
Murky, Ambiguous, or Unclear Demand
Establish early communications with potential collaborators; Explore mutual interests; Engage in “Integration Education”; Conduct needs assessments
Low, Nil, or Completely Mismatched Demand
Engage the primary care community; Find ways to start communications; Work on joint projects; Participate in basic education in “Integration Awareness Building”
15
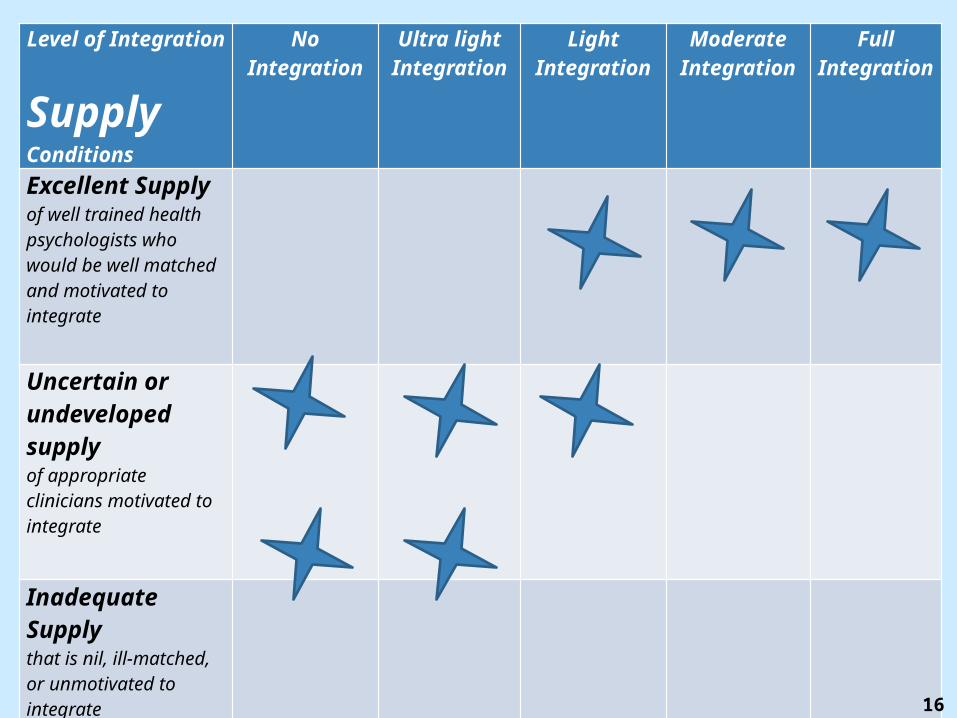
Level of Integration
Supply Conditions
No Integration
Ultra light Integration
Light Integration
Moderate Integration
Full Integration
Excellent Supplyof well trained health psychologists who would be well matched and motivated to integrate
Uncertain or undeveloped supply of appropriate clinicians motivated to integrate
Inadequate Supply that is nil, ill-matched, or unmotivated to integrate
16
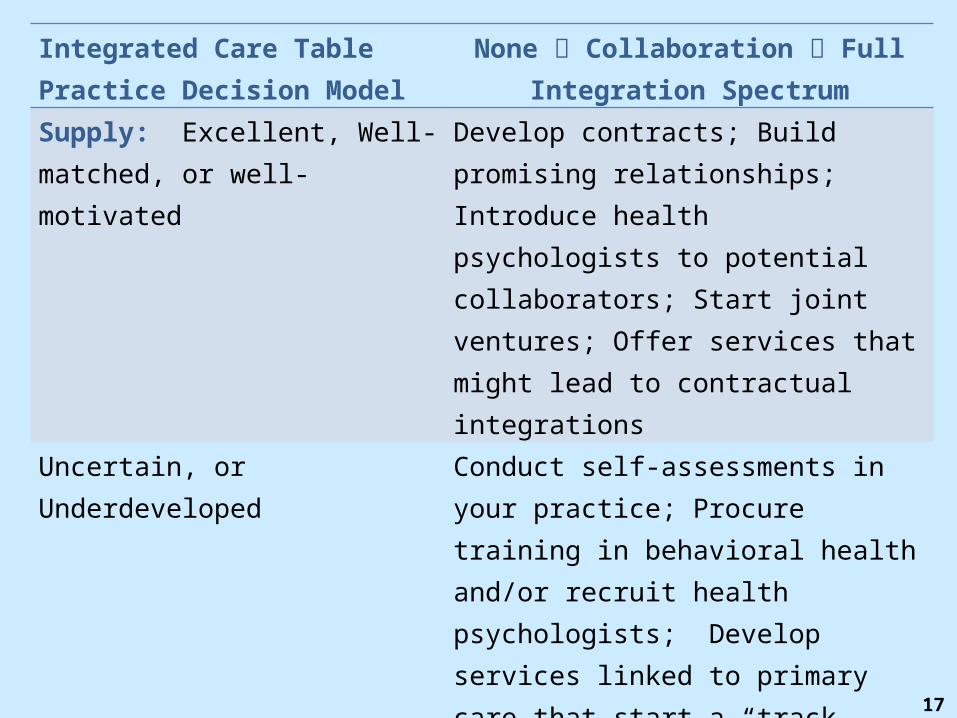
Integrated Care TablePractice Decision Model
None Collaboration FullIntegration Spectrum
Supply: Excellent, Well-matched, or well-motivated
Develop contracts; Build promising relationships; Introduce health psychologists to potential collaborators; Start joint ventures; Offer services that might lead to contractual integrations
Uncertain, or Underdeveloped Conduct self-assessments in your practice; Procure training in behavioral health and/or recruit health psychologists; Develop services linked to primary care that start a “track record” for your practice in integrated care
Nil, completely Unmotivated, or ill-matched
Look for hidden talent within the practice; Augment skills, retrain, or recruit behavioral health specialists
17

LEVEL OF INTEGRATION
ADDITIONAL FACTORS
No Integration
Maintain current practice format while keeping
watchful eye on developments
Ultra light IntegrationGreatly improve communication with targeted primary care
referral sources
Light Integration
Offering contracted services
to primary care, medical homes, or
ACOs
Moderate Integration“Co-Location”
maintaining part or all of a practice within a primary
care setting
Full IntegrationAssuming an
employed position within an
integrated setting
STRENGTHSE.g., Management Capabilities are strong; reputation good and relationships excellent
WEAKNESSESE.g., Risk Tolerance is low; technology and IT is underdeveloped
OPPORTUNITIESE.g., To establish a strong referral network with primary care
THREATSE.g., Gradual loss of referrals as medical homes pick treat internally WILDCARDS Timing (Especially bad or good)Internal and external cultures
18
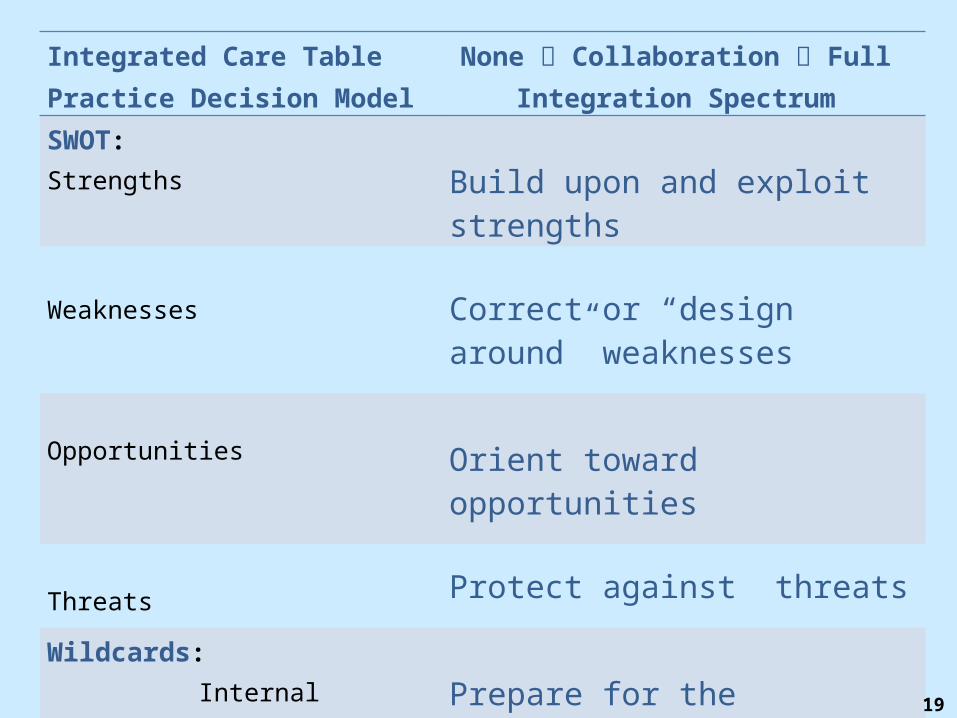
Integrated Care TablePractice Decision Model
None Collaboration Full Integration Spectrum
SWOT: Strengths Build upon and exploit strengths
Weaknesses Correct or “design around” weaknesses
Opportunities Orient toward opportunities
Threats Protect against threats
Wildcards: Internal Culture Time Considerations Competition
Prepare for the unexpected!!!
19

A Case Study in North Carolina
A Case Study – The Demand Side
• The Business Environmento The Research Triangle Area of NC (3 major cities)o Large University-Based Health Systemso Large Independent Practice Association (IPA)o History of care integration in primary care settings (Medicaid)o Interest in care integration by commercial carrier (Private Sector)
21
A Case Study – The Supply Side
• HRC Behavioral Health & Psychiatry, PAChapel Hill and Raleigh, NC
22
A Case Study – Early Days
• Founded 1967
• 25 to 30 clinicians in two cities
• Multidisciplinary approach
• EAP Experience / Contract Experience
• General reputation in community
• Two experienced health psychologists
• High motivation to integrate (co-locate +)
23
A Case Study – The Supply Side
• The Practice Group• Long history in the community
• Multi-specialty group practice o Psychologists ………………………………………………………..14
Health Psychologists ………………………………………….2o Psychiatrists …………………………………………………………. .6
Mid-level providers (Physician’s Assistants)…………………. .2o Social Workers………………………………………………………....2o Licensed Professional Counselor (substance abuse specialist)….1
• Total ……………………..…………………………….27
24

The HRC Integration Story: Phase I
• Pre-Integration Days
o Referral Promotion: Internal discussion and monitoring the local landscape to promote referrals
o Relationship Building: with a nearby primary/urgent care practice, “The Family Doctor”
o My Job as Director of Professional Affairs >> SLC attendance >> awareness of need to develop practice as business
25
The HRC Integration Story: Phase II
• Early Integration• Conversations with medical director of biggest
commercial carrier in area Discovered carrier’s strong interest in integration
• Invited conversations with nearby urgent care practice, “The Family Doctor” o How could we be more responsive? o How can we communicate most effectively? o How could we be better “integrated”?
• Discovery of a “Go Between”o Lawyer with interest in integrated care, provider
group contracting, and compliance with referral and kick-back issues under federal and state law
26
The HRC Integration Story: Phase III
• Integration Matureso HRC contracts with Family Doctor practice to be their
behavioral resource for “Medical Home” statuso The “go-between” Steve Shaber (Poyner & Spruill Raleigh)
identifies prospective primary care practice o HRC identifies a clinician from our group who wants to co-
locate. o Discussions begin with Family Medical Associates of Raleigh
(Key IPA)o Contracting begins re: space, support services, coordination
of health records, money flows, etc.o Consultant/representative sent to the commercial carrier
27
The HRC Integration Story: Phase IV
• Current Challenges: o Entering primary care cultureo Clarifying expectationso Refining contracts
Rent Services
o Fixing logistics, documentation, and information flows
o Dealing with insurance incompatibilities (panels and managed care problems)
o Dealing with payer + CPT code constrictions Eg, Health and Behavior Code 96150 – limit to 3
28

The HRC Integration Story: Phase IV
• Current Challenges, cont’d: o Dealing with time demands for unpaid services
Hallway consults Uninsured patients and network incompatibility
o How to demonstrate value to primary care patientso Implementation Science Initiativeo How to reconfigure the “mother practice” to accommodate co-location
Less need for space in original psychology practice Challenges to cohesion and connection to original group
29
Q&A
• What are the implications for other kinds of practices?
• What are implications for independent practice?
• How can our state, provincial, and territorial associations help practitioners?
• How can APA help?
30
Resources• Collins, C et.al. Evolving Models of Behavioral Health Integration in
Primary Care, Milbank Memorial Fund, May 2010. http://www.milbank.org/reports/10430EvolvingCare/EvolvingCare.pdf
• Community Care of North Carolina (CCNC). https://www.communitycarenc.org/population-management/behavioral-health-page/
• Mauer, B. 2006. Behavioral Health/Primary Care Integration: The Four Quadrant Model and Evidence-Based Practices. Rockville, MD: National Council for Community Behavioral Healthcare.
• Mechanic, David. Seizing Opportunities Under The Affordable Care Act For Transforming The Mental And Behavioral Health System. Health Affairs, 31, no.2 (2012): 376-382
• Trend Watch; Bringing Behavioral Health into the Care Continuum: Opportunities to Improve Quality, Costs and Outcomes. American Hospital Association. January 2012
• Multiple articles on integrated care at APA’s Practice Central http://www.apapracticecentral.org/ (Search terms: “Integrated Care”)
31