THYROID HORMONES AND METABOLISM
Dr (Mrs.)Geeta KurhadeB. Sc., M.B.B.S., D.G.O., M.D.Senior Lecturer,Physiology Unit, Department of Basic Sciences,EWMSC,Mt.Hope




Symptoms: Weight loss , ↑ appetite , frequent bowel movements
Exophthalmos (Protruding eyes),Goiter ( possible) Nervousness , Tremors , Restlessness.
Tachycardia, irregular heart beat and palpitations
Heat intolerance ,↑ sweating , Fatigue , Muscle weakness
Double vision , Eye irritation .
Breast enlargement in men (possible) , Menstrual irregularities in women

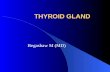
Adult woman with the characteristic puffiness that often accompanies hypothyroidism. Puffiness & hair texture improved after treatment with desiccated thyroid.



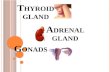
Enlargement of the thyroid gland and its extension in retrosternal space.

Introduction :

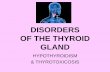
A scintiscan generated using a radioactive isotope

Thyroid gland: A. Structure, Synthesis, Storage, Release, transport of
hormone.
B. Regulation of thyroid hormone- Roles of TRH, TSH, stress & cold.
C. Physiological Effects.
D. Dysfunction.

Located immediately below the larynx on each side of & anterior to trachea.
largest -15-20 grams in adults.
Two thyroid hormones: triiodothyronine (T3) tetraiodothyronine (T4) or thyroxine.
Complete lack –BMR ↓ to 40-50%. Excess secretion-BMR ↑to 60-100%

Intro contd...

Thyroid gland in situ:

1) Thyroid follicle 2) Colloid 3) Simple cuboidal epithelium 4) Parafollicular cells (C cells)

Features of thyroid gland1) Thyroid follicle - Circular structure-filled with
pink colloid
2) Colloid - composed of the protein-thyroglobulin-secreted by cuboidal epithelial cells
(3) Parafollicular cells produce calcitonin.

Secretions of thyroid gland:
1) Thyroxine T4
2) Tri iodothyronine T3
3) Reverse Tri iodothyronine RT3
T3 is also formed in peripheral tissues by de- iodination of T4
T3 is more active than T4 & RT3 is inactive

Active Vs. Inactive Follicles:
ACTIVE FOLLICLES PASSIVE FOLLICLES
Small follicles Scalloped colloid edges Cuboidal/columnar cells Reabsorption lacunae Surrounded by fenestrated
capillaries Microvilli projecting in colloid
& canaliculi extend Prominent ER Secretory droplets of
thyroglobulin present.
Inactive and Large follicles Colloid abundant Flat cells



Ingested Iodine and its fate Normal minimal daily intake for normal thyroid
function- 150 μg in adults. Normal dietary Iodine 500 μg / l. 120 μg enters thyroid, 40 μg in ECF+ 80 μg in
T3,T4 - metabolised in liver & other tissues . (Of 80 μg enterohepatic circulation- 20 μg is
excreted in stools & 60 μg/l enters ECF) . 480 μg/l excreted in urine.
Iodised salt contains 1 part sodium iodide to every 100,000 parts of Sodium chloride.

Thyroglobulin: Synthesised in thyroid cells & secreted into
colloid by exocytosis.
T3 &T4 synthesised in the colloid by iodination & condensation of tyrosine molecule which are bound in peptide linkage in Thyroglobulin.
Hormone remains bound to thyroglobulin until secreted, then thyroglobulin ingested back in thyroid cells.

In the cells peptide bonds hydrolysed –T3 & T4 discharged into capillaries.
Three functions of thyroid cells:1. Trapping & transport of Iodine. 2. Synthesis of thyroglobulin & its secretion
into colloid (also in blood 6 ng/ml).3. Removing thyroid hormone from
thyroglobulin & secreting it into circulation.


Synthesis of thyroid hormoneA) Dietary iodine (stomach) (I2)→Iodide (I-) circulates in blood
[0.3 μg /dl.]B) Follicular cells active trap I- → Na+- I- symport (linked to
Na+-K+-pump ) - electrochemical gradient forms → through the apical membrane → into the follicular colloid → oxidized by thyroid peroxidase to I2 at the colloid surface of the apical membrane.
C) The rough ER synthesizes thyroglobulin- build up by a long peptide chain with tyrosine units & a carbohydrate unit completed by the Golgi apparatus.
D) Iodide-free thyroglobulin released by exocytosis at the apical membrane .

E) In the cell, oxidized iodide + tyrosine units (L-tyrosine) at one or two positions→ hormone precursors MIT & DIT.
MIT + DIT → tri-iodothyronine (3,5,3`-T3)
DIT + DIT (oxidative condensation) → tetra-iodothyronine (T4) or thyroxine.
Small amounts of the inactive reverse T3 (3,3`,5`- T3)
is also synthesized.

Levels of various components : MIT= 23% (Not secreted by gland)
DIT=33% (not secreted by gland)
T4=35% ( secreted 80 μg, blood level 8 μg /dl )
T3=7% (4 μg, blood level .15 μg/ dl )
RT3=traces ( 2 μg)

Transport of T4 & T3 to tissues: On entering the blood > 99% of T4 & T4 T3 combines
immediately with several plasma proteins synthesized in liver.
Mainly:
Thyroxine-binding globulin (TBG also k/as Transthyrenin
Thyroxine binding prealbumin and albumin (TBA)

Because of high affinity the hormones are released to cells slowly.
Half the T4 in blood is released in 6 days (high affinity) and half the T3 in one day (low affinity).
In the target cells T4 and T3 again combine with intracellular proteins and stored to be used slowly over a period.

Control of thyroid gland activity : The hypothalamic-pituitary-thyroid axis controls the
thyroid gland function and growth by negative feedback control.
The T3 and T4 concentrations in the blood are recorded by pituitary and hypothalamic receptors.
There is only a minimal nocturnal increase in TSH secretion and T4 release.

Mechanism of action of thyroid hormone
Most of T4 is converted into T3 ↓ Binds to thyroid hormone receptors located at
thyroid hormone response element at DNA ↓ Forms hetrodimer with retinoid X receptor
(RXR) ↓

Receptor activated → initiates transcription → different types of mRNA formed → RNA translation on ribosomes → different types of proteins formed.
Thus T3 stimulates cellular metabolism and ↑ over all metabolic rate.

Metabolism contd..... T4 prohormone - biological half-life of 7 days
- deiodinised by monodeiodinase to the more potent T3 - just before it is used in the cells.
T3 - eliminated quickly due to lowest degree of protein binding- (half-life 24 hours)
T3 - final active hormone- present in a very low concentration (10-9 mol per l).

PHYSIOLOGICAL FUNCTIONS OF THYROID HORMONE

Physiological function:
i) Acts as catalyst-activates energy producing respiratory process in the cell.
ii) Synthesis of important proteins (the Na+-K+-pump, respiratory enzymes, erythropoietin, b-adrenergic receptors, sex hormones, growth factors etc).
iii) Absorption of carbohydrates in the intestine and the gut excretion of cholesterol
iv) Modulation of reproductive function.

Physiological Functions of Thyroid hormone
1) Important cellular constituents stimulated by T3:
Mitochondria↑ number and activity- ↑ rate of ATP formation.
The Na+-K+-pump – ↑active transport of ions Myosin ATPase → ↑ heat production ↑
temperature → ↑ BMR Acts on many enzyme systems and proteins for
growth ,maturation including CNS development.

2) Effect on growth-in growing children : Essential for growth & metamorphosis
Hypothyroid → ↓ rate of growth.
Fetal life → ↓hormone → ↓ growth & maturation of brain and physical growth
Without specific thyroid therapy within days or weeks after birth
CRETINISM.


Hyperthyroidism:
↑ growth.
Excessive skeletal growth with fast fusion of epiphyses.

3) Stimulates the carbohydrate metabolism: i) Rapid uptake of glucose by cells ii) Enhanced glycolysis iii) Enhanced gluconeogenesis
iv) ↑ rate of absorption from GIT v) ↑ insulin secretion. vi) ↑ Hepatic glucose output & peripheral glucose
utilization.
vii) ↓ sugar tolerance.

Stimulates the fat metabolism:
i) Lipid are mobilized rapidly from the fat tissue- ↓ fat stores .
ii) ↑ free fatty acid concentration in plasma.
iii) Accelerates the oxidation of free fatty acids.
iv) Accelerates hepatic metabolism of fatty acids, cholesterol and triglycerides.

Effect on protein metabolism:
↑ turnover- Hyper metabolism
In physiological concentrations - thyroid hormones stimulate the synthesis as well as the degradation of proteins “ ANABOLIC ACTION”
In supra physiological doses - protein “CATABOLIC ACTION” predominates.
HENCE In hyperthyroidism skeletal muscle protein stores suffer depletion.

Protein metabolism contd.. ↑ skeletal muscle amino acid release → ↑ plasma
concentration of glucoplastic amino acids HENCE ↑ substrate supply to ↑ hepatic gluconeogenesis.
↑ Thyroid hormone → cardiac hypertrophy The stimulatory effect BECAUSE ↑ protein synthesis
at a pre translational level - reflected by a generalized ↑ in total cellular RNA.
Serum total protein concentration is slightly ↓ or even unchanged in hyperthyroidism.

Effect on plasma and liver fat cells : ↑ thyroid hormone ↓ cholesterol BECAUSE ↑ cholesterol secretion in bile which is excreted in
feces.
↓ phospholipids & triglycerides in plasma ↑ the free fatty acids.
↓ thyroid hormone causes reverse effects with hypercholesteremia → atherosclerosis.

Increased requirement for vitamins:
BECAUSE ↑in quantities of various body enzymes - vitamins being essential parts of various enzymes & coenzymes.
HENCE Relative vitamin deficiency can occur in
hyperthyroidism. Hypothyroidism-carotenimia- (hepatic
conversion of carotene- Vit A needs Thr)

Explain myxedema and puffiness of face in hypothyroidism Skin normally contains a variety of proteins
combined with polysccharides, hyluronic acid and chondroitin sulfuric acid.
In hypothyroidism these complex accumulate & promote water retention- puffiness of face.
When treated with thyroid hormone-proteins are metabolized & diuresis continues untill myxedema clears.

Calcium & Phosphorous metabolism:
Removes Ca & P from bones.
↑ loss of Ca & P in excretion.
Leads to osteoporosis.

Effect on sexual function: To men- Hypothyroidism -loss of libido, erectile
problems,gynecomastia,abnormal sperm morphlogy
Thyrotoxicosis- ↑- impotence, abnormal sperm motility

To women- changes in Serum levels of Sex Hormone Binding Globulin (SHBG)
• ↓ thyroid hormone –hypomenorrhoes menorrhagia/polymenorrhoea /amenorrhoea & ↓libido.Infertility because midcycle ovulatory peak of LH is blunted /absent- no ovulation.
• ↑ thyroid hormone- amenorrhoea /oligomenorrhea
• Overt hypothyroidism- spontaneous abortion,premature delivery

Effect on CVS : ↑ blood flow , cardiac rate and output as well as
ventilation. The high BMR ↑ the core & shell temperature →
the peripheral vessels dilate → ↑ COP (60% rise a. ↑ blood volume due to ↑ Na+ & H2O retention b.↑ direct action of Thr on cardiomyocytes ) → A circulatory shock develops -high output failure.( rise in COP insufficient to match the vasodilatation)
↑ HR – direct effect on excitability of heart. Pulse pressure ↑, circulatory time shortens.

Effect on RS: ↑ respiration because ↑ rate of metabolism.
↑ oxygen utilization.
↑ CO2 formation.
Hence increased rate and depth of respiration

GIT:
↑ GIT motility.
↑ appetite & food intake.
↑ rates of secretion of digestive juices.

Kidneys: ↑ N2 excretion.
↑ Creatinine excretion.

Excitatory effects on CNS:
Essential for normal sensory & emotional activity
Extreme nervousness.
Psychoneurotic tendencies.
Anxiety complexes.
Extreme worry.
Paranoia

CNS, ANS, PNS & voluntary muscles:
In hyperthyroidism- nervousness, irritability, fine muscular tremors.
Catabolism of muscles - wasting weakness, myasthenia.
ANS – sweating , hyperactivity of GIT, vasomotor instability.

Effect on sleep:
Exhausting effect on musculature - hence tiredness - but excitable effect on brain-hence difficult to sleep.
Hypothyroidism - somnolence (sleep > 12 hours)

Effect on other glands : ↑Thyroid hormone - ↑ rate of secretion of other glands
(it also ↑ needs of other tissues to those hormones.)
i) ↑ Thyroid hormone - ↑ glucose metabolism- ↑ need insulin.
ii) ↑ metabolic activities related to bone formation- ↑ need of PTH
iii) ↑ rate of inactivation of glucocorticoids in liver -Feed back ↑ in ACTH production by anterior pituitary.

Midline swellings of neck due to thyroid abnormalities a) Solitary thyroid nodule or uninodular goiter b) Fluid filled (simple cysts), or partly solid and partly fluid, (complex cysts). c) Thyroid nodules cystic nodules.

Signs and symptoms
Hyperthyroidism Hypothyroidism
Thermal Heat intolerant, fever (rare) warm, vasodilated peripheries, raised BMR
cold intolerant, hypothermia, lowered basal metabolic rate
Body weight Decreased Increased
GIT Increased appetite but sometimes anorectic, diarrhoea, vomiting
Decreased appetite, constipation, large tongue
Cardio respiratory Breathlessness, tachycardia, atrial fibrillation, palpitations, systolic hypertension (high output with low peripheral resistance, angina, heart failure.
bradycardia, pericardial effusion, oedema, hypertension (low output with high peripheral resistance), heart failure, hypercholesterolemia
Mental and behavioural Hyperkinesis, tremor, irritability, restlessness, psychosis
Tiredness, poor memory, dementia, slow reflexes, depression, psychosis
Bones and muscles Proximal myopathy, wasting Arthralgia (joint pain), myalgia (muscle pain)
Hair and skin Pretibial myxedema * (NOT the same as ordinary myxedema) in Graves disease
Thin dry unmanageable hair, coarse dry skin, myxedema (Mucopolysccharides under skin.
Eyes and ears Exophthalmos, lid lag Puffy eyes, deafness
Reproductive Amenorrhea/ oligomenorrhea, loss of libido, gynecomastia
Menorrhagia / oligomenorrhea, loss of libido
Thyroid Diffuse goitre, high flow bruit Goitre, deep voice

Treatment of hypothyroidism T3 - liothyronine sodium [Cytomel]) is available much
shorter-acting hence dosage are multiple times a day. T4 (levothyroxine sodium [Levoxyl, Synthroid]) is the
preferred treatment because it is more stable form & requires once a day dosing. Synthetic T4 is steadily converted to T3 naturally in blood stream and this conversion is appropriately regulated by the body tissues
The average dose of T4 replacement in adults is approximately 1.6 micrograms per kilogram per day. This translates into approximately 100 to 150 micrograms per day.

Thyroid hormone overload for prolonged period: Hyperthyroidism will suffer from
muscle atrophia, bone destruction & hunger damage, due to increased catabolism of cellular proteins and fat.
Eventually hypothyroidism may
develop due to suppression.

Diagnosis??

Some interesting terms: Pseudogoiter
Goiter
Modigliani Syndrome
Performing the Pemberton’s test
Hypothyroidism- Hashimoto's disease
Graves disease( Auto-immune thyroid disease)

Hyperthyroidism : causes
Graves' Disease
Functioning adenoma ("hot nodule") & toxic multinodular goiter (TMNG)
Excessive intake of thyroid hormones
Abnormal secretion of TSH
Thyroiditis (inflammation of the thyroid gland)
Excessive iodine intake

Basic causes of hypothyroidism:
A) Due to diseases of thyroid gland.
B) Secondary to pituitary failure (pituitary hypothyroidism) ↑ TSH in response to test dose of TRH.
C) Hypothalamic failure (Hypothalamic hypothyroidism.
B & C will respond to a test dose of TSH.

Hypothyroidism : Hashimoto's thyroiditis. Lymphocytic thyroiditis (which may occur
after hyperthyroidism). Thyroid destruction (from radioactive
iodine or surgery) Pituitary or hypothalamic disease Medications Severe iodine deficiency

Condition TSH Free T4 Free T3 Other investigations
Graves' Disease
reduced++ usually raised (not if isolated T3 thyrotoxicosis)
usually raised
Thyroid scan - diffuse isotope uptakeThyroid peroxidase antibodies (suggestive) and TSH-receptor antiboides (more specific indicator)
Toxic adenoma "hot nodule"
Reduced raised or normal
raised or normal
hyroid scan - functioning nodule with suppression of other tissue
Toxic multi-nodular goitre
Reduced raised or normal
raised or normal
thyroid scan - enlarged gland with multiple active nodules
Thyroiditis Reduced variably increased
variably increased
thyroid scan - low radioiodine uptakethyroglobulin level - ↑↑↑ESR - often raised
Factitious thyroxine-induced hyperthyroidism
Reduced raised raised or normal
thyroid scan - low radioiodine uptakethyroglobulin levels -absent
Pregnancy normal raised total T4, normal FT4
raised total T3, normal FT3
positive pregnancy test

Free Thyroxine index (FTI) The T-Uptake is an assessment of unsaturated thyroid binding proteins in serum. The
free thyroxine index is an estimate of the amount of circulating free thyroxine.
The free thyroxine index (FTI), is a normalized measurement that remains relatively constant in healthy individuals and compensates for abnormal levels of binding proteins.
Hyperthyroidism causes increased FTI and hypothyroidism causes decreased values. When serum contains high levels of T3 and T4 as in hyperthyroidism, fewer unoccupied binding sites are available. Conversely, in hypothyroidism, more binding sites are available.
TU results are changed by drugs or physical conditions that alter the patient's thyroxine-binding globulin levels, or drugs that compete with endogenous T4 and triiodothyronine (T3) for protein-binding sites.
The T-Uptake (TU) values used are interpreted in conjunction with total thyroxine (T4) measurements. The free thyroxine index is calculated as:
-FTI=(T4 concentration) x (% TU)/100