SLE Discussion Topics
• The Path to Diagnosis
• Pathogenesis
• Impact on Patients: Mortality and Morbidity
• The Burden of Lupus
• Patient Support
2

The Path to Diagnosis

SLE Is an Autoimmune Disease That Primarily Affects Women of Childbearing Age
• SLE is a chronic, multisystem autoimmune disease characterized by:1
– Diverse clinical manifestations, which are the result of inflammation in affected organ systems2
– Being potentially life threatening when major organs are affected1
– Waxing and waning disease activity1
• SLE patient population:
‒ Nine out of 10 cases occur in women,3 with the majority diagnosed between 15 and 45 years of age4
‒ Tends to be more severe in men vs women5
‒ More common and severe among nonwhite populations6-9*
4
*Nonwhite populations include those of African, Asian, Australian Aboriginal, Hispanic, and Native American descent.
1. ACR Ad Hoc Committee on Systemic Lupus Erythematosus Guidelines. Arthritis Rheum. 1999;42:1785‐1796. 2. Wallace DJ, Hahn B, eds. Dubois' Lupus Erythmatosus. 7th ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2007. 3. D’Cruz DP, et al. Lancet. 2007;369:587‐596. 4. Cervera R, et al. Medicine. 1993;72:113-124. 5. Tan TC, et al. J Rheumatol. 2012;39:759-769. 6. Samanta A, et al. Ann Rheum Dis. 1991;50(7):490-492. 7. Boyer GS, et al. J Rheumatol. 1991;18:1477-1484. 8. Bossingham D. Lupus. 2003;12:327-331. 9. Fernandez M, et al. Arthritis Rheum. 2007;57(4):576-584.

A Range of Organ Systems May Be Involved
ACR Ad Hoc Committee on Systemic Lupus Erythematosus Guidelines. Arthritis Rheum. 1999;42:1785-1796.
Central Nervous System
Eyes and Mucous Membranes
Kidneys
GastrointestinalMusculoskeletal
Hematologic
Skin Heart and Lungs
5

1. ACR Ad Hoc Committee on Systemic Lupus Erythematosus Guidelines. Arthritis Rheum. 1999;42:1785-1796. 2. Heinlen LD, et al. Arthritis Rheum. 2007;56:2344-2351.
3. ACR Ad Hoc Committee on Neuropsychiatric Lupus Nomenclature. Arthritis Rheum. 1999;42:599-608.
• American College of Rheumatology (ACR) criteria were developed to classify patients diagnosed with SLE for research studies, not for clinical use1
– Four of 11 criteria must be met at any time in the patient’s history
• Additional symptoms indicating SLE may be evident upon presentation1
Symptoms Are Highly Varied
ACR SLE Classification Criteria1 Some Additional Clinical
Features of SLE
• Cutaneous– Malar rash– Discoid rash– Photosensitivity– Oral ulcers
• Musculoskeletal– Arthritis without deformed joints
• Cardiopulmonary– Pleuritis or pericarditis (inflammation of lining of the chest cavity
or heart)
• Renal– Proteinuria or cellular casts (excess protein or cells in urine)
• Neurologic– Seizures or psychosis
• Hematologic– Hemolytic anemia, leukopenia, lymphopenia, or thrombocytopenia
(decreased red blood cells, white blood cells, or platelets)
• Immunologic– Antibodies to native DNA, Smith antigen (Sm), or phospholipid– Antinuclear antibodies (ANA)
• Fatigue1,2
• Unexplained fever1
• Myositis2 (muscle weakness)
• Alopecia1,2 (hair loss)
• Raynaud phenomenon1,2
(pale or purple fingers and toes)
• Vasculitis1,2 (inflamed blood vessels)
• Nausea, vomiting1
• Peripheral neuropathy1
• Sicca complex2 (dry mouth or eyes)
• Headache2,3
• Psychiatric disorders (eg, depression, anxiety)3
6

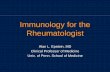
Similarity and Overlap Between SLE Manifestations and Multiple Other Conditions1,2
SLE Manifestation1 Other Condition
Lupus arthritisFibromyalgia with positive ANA;
rheumatoid arthritis3,4
Thrombocytopenia Idiopathic thrombocytopenic purpura5
Positive ANA Antiphospholipid antibody syndrome2,6
Serositis Undifferentiated connective tissue disease7,8
Malar rash Rosacea; polymorphous light eruptions9,10
1. ACR Ad Hoc Committee on Systemic Lupus Erythematosus Guidelines. Arthritis Rheum. 1999;42:1785-1796. 2. Cervera R, et al. Arthritis Rheum. 2002;46(4):1019-1027.
3. Calvo-Alen J, et al. Arthritis Rheum. 1995;38(10):1475-1484. 4. Levin RW, et al. Scand J Rheumatol. 1996;25(5):277-281. 5. John ML, Scharrer I. Hamostaseologie. 2012;32
Suppl 1:S86-S89. 6. Narain S, et al. Arch Intern Med. 2004;164:2435-2441. 7. Williams HJ, et al. J Rheumatol. 1999;26(4):816-825. 8. Bodolay E, et al. Clin Exp Rheumatol.
2003;21(3):313-320. 9. Black AA, et al. Lupus. 1992;1:229-237. 10. Pincus LB, et al. J Cutan Pathol. 2010;37:416-425.
Malar Rash Rosacea
Reproduced with permission courtesy of the National Rosacea Society
7
© 2013 American College of Rheumatology. Used with permission.

Variability in Symptoms at Presentation and Over Time Can Result in Difficulty in Diagnosis
• Accurate diagnosis may take several years1
• SLE may co-present with other autoimmune diseases2
• Patients with SLE may present with different symptoms at different times3
• No single test is sufficient to establish diagnosis4
–SLE should be suspected in patients with manifestations in ≥2 organ systems
1. Hopkinson ND, et al. Ann Rheum Dis. 1994;53(10):675-680. 2. McDonagh JE, Isenberg DA. Ann Rheum Dis 2000;59:230-232. 3. Heinlen LD, et al. Arthritis Rheum.
2007;56:2344-2351. 4. ACR Ad Hoc Committee on Systemic Lupus Erythematosus Guidelines. Arthritis Rheum. 1999;42:1785-1796. 5. Narain S, et al. Arch Intern Med.
2004;164:2435-2441.
In a study of 263 patients with presumptive SLE who were referred to an autoimmune disease center, 48% were ultimately diagnosed with a
different disorder5
8

9
Patient Case Study: Clinical Perspective*
Presentation
– Patient presented with edema of ankles, fatigue
– Patient reports joint pain, cold hands and feet, fever
– Joint pain follow-up visit. X-ray indicates no erosion or subluxation. Patient reports all symptoms resolved
– Rash on cheeks and nose
– Dermatologist report
– Patient presented with severe abdominal pain; reports occasional fever
– Gastroenterologist report
– Patient presented with severe Raynaud phenomenon
*Patient case study is for educational purposes only and represents hypothetical patient.
Denise G., 26-year-old African American female
Jun 11, 2010
Dec 20, 2010
Jan 20, 2011
Aug 22, 2011
Feb 1, 2012
Feb 7, 2012
Jul 16, 2012
Aug 15, 2011
Aug 9, 2012
– Apparent effect from recent flight; advised to sleep with legs elevated
– Flu test negative. Referred for x-ray of painful joints. Scheduled follow-up visit
– Patient advised to make an appointment if symptoms return
– Referred to dermatologist
– Diagnosed with rosacea
– Referred to gastroenterologist
– Symptoms resolved prior to visit without intervention, possible inflammatory bowel disease
– Referred to rheumatologist
Next Steps/Follow-UpDate
– Rheumatologist report – SLE diagnosis

9
Presentation
– Patient presented with edema of ankles, fatigue
– Patient reports joint pain, cold hands and feet, fever
– Joint pain follow-up visit. X-ray indicates no erosion or subluxation. Patient reports all symptoms resolved
– Rash on cheeks and nose
– Dermatologist report
– Patient presented with severe abdominal pain; reports occasional fever
– Gastroenterologist report
– Patient presented with severe Raynaud phenomenon
Denise G., 26-year-old African American female
Jun 11, 2010
Dec 20, 2010
Jan 20, 2011
Aug 22, 2011
Feb 1, 2012
Feb 7, 2012
Jul 16, 2012
Aug 15, 2011
Aug 9, 2012
– Apparent effect from recent flight; advised to sleep with legs elevated
– Flu test negative. Referred for x-ray of painful joints. Scheduled follow-up visit
– Patient advised to make an appointment if symptoms return
– Referred to dermatologist
– Diagnosed with rosacea
– Referred to gastroenterologist
– Symptoms resolved prior to visit without intervention, possible inflammatory bowel disease
– Referred to rheumatologist
Next Steps/Follow-UpDate
– Rheumatologist report – SLE diagnosisAug 9, 2012 – Rheumatologist report – SLE diagnosis
Jun 11, 2010
Patient Case Study: Clinical Perspective*
*Patient case study is for educational purposes only and represents hypothetical patient.

Denise G.: On the Path to Diagnosis
10
I felt so tired again today, even though yesterdayI was fine!
My fever keeps coming and going.
Why can’t any of the doctors figure out what’s wrong with me?
My friends are starting to think it’s all in my head, and sometimes I would wonder if they’re right…
Why is this happening to me?
Patient perspective is for educational purposes only
and represents hypothetical patient.
2/1/2010

Pathogenesis

• UV light
Environmental Triggers
Immune Dysregulation
Multiple Factors Result in Systemic Immune Dysregulation Leading to SLE*
SLE
Sex Hormone InteractionsFemale predominance
Mok CC, Lau CS. J Clin Pathol. 2003;56(7):481-490.
Multiple Genetic Polymorphisms
12
*Etiology is unknown, but factors presented here are thought to have major roles.

13
Immune Dysregulation Has Multiple Consequences
• Defective clearance mechanisms fail to remove cellular material exposed through normal apoptosis (cell death)1
• Failure of normal immune checkpoints leads to loss of self-tolerance2
–Abnormal immune cells treat the body’s own cellular components like foreign pathogens and produce autoantibodies1
1. Mok CC, et al. J Clin Pathol. 2003;56:481-490. 2. Tsokos GC. N Engl J Med. 2011;365:2110-2121.

14
Immune Dysregulation Has Multiple Consequences (cont)
• SLE is characterized by pathologic production of antibodies directed against self-antigens1
–Antinuclear antibodies are hallmark of disease
–Abnormal activation of B and T cells
• Autoantibodies form immune complexes with self-antigen that get deposited in tissue2,3
–Defective clearance mechanisms allow complexes to persist2,3
• Deposition of autoreactive B cells and immune complexes in tissues result in inflammation and can lead to organ damage2,3
• Damaged tissue stimulates additional immune response and inflammation, creating a vicious cycle of immune overactivity2-4
1. Muñoz LE, et al. Rheumatology (Oxford). 2005;44:1101-1107. 2. Mok CC, et al. J Clin Pathol. 2003;56:481-490. 3. Tsokos GC. N Engl J Med. 2011;365:2110-2121. 4. Crow MR. Arthritis Res Ther. 2009;11:245-256.

Numerous Factors Contribute to Underlying SLE
Pathogenesis and Subsequent Organ Damage1,2
Initiate Autoimmunity Immune Dysfunction Inflammation and
Organ/Tissue Damage
Genetic Susceptibility
(Immune-Related)
Stimuli(eg, Environmental,
Hormonal)
MusculoskeletalSystem
Brain
Heart
Lungs
Skin
Kidneys
Adaptive Immune System Activation
Immune Reactivity
Cytokines
Cytokines
Innate ImmuneSystem Activation
Autoantibodies
Cytokines
Autoimmune Amplification
1. Tsokos GC. N Engl J Med. 2011;365:2110-2121. 2. Mok CC, et al. J Clin Pathol. 2003;56:481-490. 3. Crow MR. Arthritis Res Ther. 2009;11:245-256. 15

Impact on Patients: Mortality and Morbidity

Bernatsky S, et al. Arthritis Rheum. 2006;54:2550-2557.
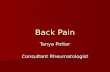
SLE Is a Chronic Disease With Higher Than Expected Mortality Rate
Collaboration of the Systemic Lupus International Collaborating Clinics (SLICC) and the Canadian Network for Improved Outcomes in Systemic Lupus (CaNIOS) investigator groups (US, Canada, England, Scotland, Iceland, Sweden, South Korea). Death data were prospectively collected or acquired through probabilistic linkage to vital statistics registries. Expected deaths in the general population were determined by multiplying person-years at risk in the cohort by the geographically appropriate age-, sex-, and calendar-year period-matched mortality rates. Risk of death was assessed as a standardized mortality ratio, calculated as the observed number of deaths divided by the number expected in the general population. Duration of disease at time of enrollment was <2 years for most patients, and 90% of patients were female.
General Population
Estimated Rate of Death Compared to the Age-Matched General Population
19.2xGreater Rate
8.0xGreater Rate
1.4xGreater
Rate
SLE Patient Age
(years)
3.7xGreater
Rate
≥6040-5925-3916-24
17
• Relative increase in mortality is highest in younger patients

• Compared to the general population,mortality rates were estimated to be1:– ~8x higher from
renal causes
– ~5x higher from infections
– ~2x higher from heart disease
• Organ damage is one of the most important correlates with mortality2
*Cause of death was acquired through probabilistic linkage to vital statistics registries. It is possible that the primary cause of death when identified as “lupus” was actually another
condition (eg, cardiovascular disease or infection), but the patient’s preexisting diagnosis of SLE may have led to this being listed as the cause of death.
1. Bernatsky S, et al. Arthritis Rheum. 2006;54:2550-2557. 2. Alarcon GS, et al. Arthritis Care Res. 2001(2);45:191-202.
23
109
53 2
Column1
Most Common Causes of Death1
(N=1255)*
Most Common Causes of Death in SLE Are Conditions Typically Associated With Aging1
Collaboration of the Systemic Lupus International Collaborating Clinics (SLICC) and the Canadian Network for Improved Outcomes in Systemic Lupus (CaNIOS) investigator groups (US, Canada, England, Scotland, Iceland, Sweden, South Korea). Mortality data were collected for 9547 patients followed 1958-2001 (76,948 person-years). A total of 1255 deaths occurred. Specific causes of death were not available from all cohorts. Duration of disease at time of enrollment was <2 years for most patients, and 90% of patients were female. Race/ethnicity was not reported for the entire cohort.
Pe
rce
nt
of
Ca
se
s
40
20
0 n=21n=34n=64n=114n=126n=291
18

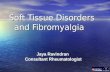
Percentage of Patients With Permanent Organ Damage
*The SDI (SLICC/ACR Damage Index) is a widely accepted scale that measures irreversible changes present for at least 6 months attributable to lupus, concomitant diseases,
or treatment in 12 organ systems.
Chambers SA, et al. Rheumatology (Oxford). 2009;48:673-675.
One-Third of SLE Patients Accrue Permanent Organ Damage Within 5 Years of Diagnosis
10%
33%
51% 55%65%
100%
0
20
40
60
80
100
1 Year (N=232)
5 Years (N=232)
10 Years (N=232)
15 Years (N=143)
20 Years (N=75)
25 Years (N=6)
Pe
rce
nt
of
Pa
tie
nts
Wit
h S
DI*
≥1
5 Years(N=232)
1 Year(N=232)
10 Years(N=232)
15 Years(N=143)
20 Years(N=75)
25 Years(N=6)
0.11 0.42 0.77 1.01 1.26 2.17Mean
Damage Score
Retrospective analysis of records for patients with ≥10 years of consistent follow-up presenting at the University College London Hospital SLE clinic. Year 0 represents time of diagnosis. Mean age at diagnosis was 31.2 years, 95% of patients were female, 72% were white, 14% were black, 10% were Asian (Indian), and 4% were “other.”
19

0
10
20
30
40
50
60
0 1 2 3 4 5
Percentage of Patients With Organ Damage Over 5 Years of Follow-Up
(N=298)
Disease Activity Over 5 Years of Follow-Up (N=298)
Patients Still Accrue Organ Damage Even With Low/Moderate Disease Activity
0
2
4
6
8
0 1 2 3 4 5
*The SLEDAI-2K (SLE Disease Activity Index 2000) is a validated measure of global SLE disease activity.†The SDI (SLICC/ACR Damage Index) is a validated measure of to assess damage in SLE.
Urowitz MB, et al. Arthritis Care Res. 2012;64:132-137.
Me
an
To
tal S
LE
DA
I-2
K*
Years in Registry
Pe
rce
nt
of
Pa
tie
nts
Wit
h S
DI†
>0
Years in Registry
Prospective analysis of patients in the SLICC cohort recruited within 15 months of diagnosis and followed annually for ≥5 years. Mean age at enrollment: 35.3 years; 87% female; 55% white, 12% black, 14% Asian, 16% Hispanic, 2% “other.” At enrollment, mean disease duration=5.5 months; mean SLEDAI-2K score=5.9.
20

Organ Damage May Be Subclinical inSLE Patients
– Higher in SLE patients vs controls2,3
• Prevalence of plaque in internal carotid artery is 3x higher
• Inadequate blood-vessel dilation (endothelial dysfunction), a sign of early plaque formation, is twice as common
1. Houssiau FA, et al. Br J Rheumatol. 1998;37(4):448-453. 2. Ahmad Y, et al. Rheumatology. 2007;46:983‐988. 3. El-Magadmi M, et al. Circulation. 2004;110:399-404.
Subclinical Cardiovascular Disease
Patients and Their Clinicians May Be Unaware As Organ Damage Accrues
– Osteonecrosis may be
asymptomatic in SLE
patients1
Bone Tissue Death
53% of Osteonecrotic Hips May Be Asymptomatic1
21

Cognitive Impairment*4Cardiovascular Disease1 Osteoporosis2 ESRD3
Organ Damage Can Result in Development of Chronic Diseases Usually Associated With Increased Age
22
ESRD =end-stage renal disease.
*Cognitive impairment involves dysfunction in the areas of complex attention, learning, memory, visual perception, and arithmetic. Impairment may involve specific domains or be global.
1. Esdaile JM, et al. Arthritis Rheum. 2001;44:2331-2337. 2. Ramsey-Goldman, et al. Arthritis Rheum. 1999;42(5):882-890. 3. Ward MM. Arch Intern Med. 1992;152(10):2082-2088.
4. Petri M, et al. J Rheumatol. 2008;35:1776–1781.

Esdaile JM, et al. Arthritis Rheum. 2001;44:2331-2337.
• Risks for coronary heart disease (CHD) and stroke are estimated to be significantly higher than in the general population
Cardiovascular Disease Can Be an Ongoing Issue for Patients With SLE
Cardiovascular Disease
Risk for GeneralPublic
7.5x risk of CHD compared to age-matched
controls
7.9x risk of stroke
compared to age-matched controls
23

Incidence of Myocardial Infarction (MI) in Young, Premenopausal Women Is High
Manzi S, et al. Am J Epidemiol. 1997;145:408-415.
Prospective analysis of the incidence of MI in 498 women with SLE. Cardiovascular incidence rates were compared to 2208 women of similar age participating in the Framingham Offspring Study, a prospective investigation of cardiovascular disease in the children of the 5209 men and women who participated in the original Framingham Heart Study. A comparison of MI rates was made over the same time period (1980-1993).
• Compared to the general population, rate of MI was higher in women with SLE overall
• Rate of MI is more than50 times greater for women with SLE aged 35-44
Incidence of MI in Women by Age
0
1
2
3
4
5
6
7
8
9
15-24 25-34 35-44 45-54 55-64
General Population
SLE PatientsIn
cid
en
ce
Rate
of
MI
p
er
10
00
Pe
rso
n-Y
ea
rs
(n=2208)
(n=498)
24

Ramsey-Goldman, et al. Arthritis Rheum. 1999;42(5):882-890.
Fracture Risk
Risk for GeneralPublic
Estimated 5x more likely to have bone fracture compared
to age-matched controls
18- to 24-year-olds are estimated to be 12x more
likely to have bone fracture
• Fracture risk is estimated to be significantly higher than in the general population
Osteoporosis Is a Major Concern for Patients With SLE
25

Nephritis* Impacts the Majority of Patients As SLE Progresses
Nephritis
Cumulative incidence of 54%1*†
54%
Present in 34% of adult patients at time of diagnosis1*
34%
26
• Prevalence is higher in African Americans and Hispanics than in
whites1; higher in men than in women2
• Renal damage is one of the most important predictors of mortality
for patients with SLE3
ESRD=end-stage renal disease
*Lupus nephritis defined as (1) renal biopsy demonstrating WHO, class II-V histopathology; and/or (2) proteinuria ≥0.5 g/24 h or 3+ proteinuria attributable to SLE; and/or (3) one of the
following features also attributable to SLE and present on 2 or more visits, done at least 6 months apart: proteinuria ≥2+, serum creatinine ≥1.4mg/dl, creatinine clearance
≤79ml/min, ≥10 red blood cells or white blood cells per high power field (HPF), ≥3 granular or cellular casts per HPF. Patients in whom other diseases (such as diabetes) might have
explained abnormal urinary findings were excluded.†Patients were followed for a mean of 5.5 years, and up to 8 years.
Renal damage ascertained using the SLICC Damage Index (SDI) at last visit.
1. Bastian HM, et al. Lupus. 2002;11:152-160. 2. Tan TC, et al. J Rheumatol. 2012;39(4):759-769. 3. Danila MI. Rheumatology. 2009;48:542-545.

• Involvement of cerebral microvasculature may result in
diverse central nervous system syndromes6
Neuropsychiatric Syndromes Affect From 37% to 80% of SLE Patients1-5*
Most Common Manifestations1
• Cognitive dysfunction7†
• Headache
• Depression
• Anxiety
Less Common Manifestations1
• Seizures
• Psychosis
• Movement disorders
*Definition of neuropsychiatric lupus included headache, per American College of Rheumatology criteria. Not all manifestations observed in SLE patients may be attributed to SLE. †Cognitive dysfunction included difficulties in attention, concentration, memory, and visual perception.
1. Brey RL, et al. Neurology. 2002;58:1214-1220. 2. Hanly JG, et al. J Rheumatol. 2004;31(11):2156-2162. 3. Sanna G, et al. J Rheumatol. 2003;30(5):985-992. 4. Mikdashi
J, Handwerger B. Rheumatology. 2004;43:1555-1560. 5. Hanly JG, et al. Ann Rheum Dis. 2010;69(3):529-535. 6. Brooks WM, et al. Arthritis Rheum. 2010;62(7):2055-2063.
7. Kajs-Wyllie M. J Neurosci Nurs. 2002;34(4):176-183. 27

Patient Case Study: Clinical Perspective*
– Patient presents with edema of ankles, hands, eye area; reports increased fatigue and need to urinate at night. Lab tests reveal proteinuria with hematuria and cellular casts
*Patient case study is for educational purposes only and represents hypothetical patient.
Cheryl M., 38-year-old white female
– Patient scheduled for renal biopsyApr 18, 2008
Mar 16, 2009
June 22, 2010
Nov 18, 2009
Apr 28, 2008
July 15, 2010
Sept 24, 2010
– Renal biopsy report
– Annual physical exam – Lab tests indicate hypertension, hyperlipidemia, and insulin resistance
– Painful frequent urination – Urinary tract infection confirmed
– Broken wrist from minor fall. Referred for DEXA scan
– Results reveal patient hasosteopenia
– Continued edema, fatigue, headaches. Urine is foamy
– Lab tests reveal proteinuria with hematuria, cellular casts, elevated serum creatinine. Renal biopsy indicates class V membranous lupus nephritis
– Follow-up appointment: persistent proteinuria with hematuria, cellular casts, elevated serum creatinine. Urine is brown. Patient reports numbness in extremities, frequent vomiting
– Diagnosed with end stage renal disease, placed on dialysis, added to kidney transplant list
38-year-old white female, diagnosed with SLE in 1998
Presentation Next Steps/Follow-UpDate
28
– Renal biopsy indicates class III focal lupus nephritis

– Patient presents with edema of ankles, hands, eye area; reports increased fatigue and need to urinate at night. Lab tests reveal proteinuria with hematuria and cellular casts
Cheryl M., 38-year-old white female
– Patient scheduled for renal biopsyApr 18, 2008
Mar 16, 2009
June 22, 2010
Nov 18, 2009
Apr 28, 2008
July 15, 2010
Sept 24, 2010
– Renal biopsy report
– Annual physical exam – Lab tests indicate hypertension, hyperlipidemia, and insulin resistance
– Painful frequent urination – Urinary tract infection confirmed
– Broken wrist from minor fall. Referred for DEXA scan
– Results reveal patient hasosteopenia
– Continued edema, fatigue, headaches. Urine is foamy
– Lab tests reveal proteinuria with hematuria, cellular casts, elevated serum creatinine. Renal biopsy indicates class V membranous lupus nephritis
– Follow-up appointment: persistent proteinuria with hematuria, cellular casts, elevated serum creatinine. Urine is brown. Patient reports numbness in extremities, frequent vomiting
– Diagnosed with end stage renal disease, placed on dialysis, added to kidney transplant list
38-year-old white female, diagnosed with SLE 1998
Presentation Next Steps/Follow-UpDate38-year-old white female, diagnosed with SLE in 1998
– Diagnosed with end-stage renal disease, placed on dialysis, added to kidney transplant list
28
Sept 24, 2010
– Renal biopsy indicates class III focal lupus nephritis
*Patient case study is for educational purposes only and represents hypothetical patient.
Patient Case Study: Clinical Perspective*

This is supposed
to be the prime of
my life, but some
mornings I wake
up feeling like I’m
80 years old. I feel
so weak since the
last renal biopsy,
Patient perspective is for educational purposes only and represents hypothetical patient.
and today I began
writing my will.
This is not where
I expected to be
at age 38!
29
7/29/2010
Cheryl M.: Facing End-Stage Renal Disease

The Burden of Lupus

• In a telephone survey of 829 patients with SLE:
‒ Nearly all patients (91%) had ≥1 valued life activity affected by SLE
‒ Almost half (49%) were unable to perform ≥1 valued life activity
Patients With SLE Have Impaired Function Affecting Multiple Aspects of Daily Life
Katz P, et al. Arthritis Rheum. 2008;59:465-473.
42% 44%50%
58% 61%73% 74%
83%
0
20
40
60
80
100
Pe
rce
nt
of
Pa
tie
nts
Some of the Valued Life Activities Affected by SLE (N=829)
Prospective phone interview study of patients participating in the University of California at San Francisco Lupus Outcomes Studies. Valued life activity (VLA) disability was assessed using a scale rating the difficulty of performing 21 activities. Changes in VLA disability were assessed for 1 year from baseline. Affected VLAs were those with any level of difficulty or inability to perform. Mean age at baseline was 47.2 years, mean duration of SLE was 12.7 years, 91% were women, and 70% were white.
31

SLE Can Make the Demands of Everyday Life More Challenging
• Multiple symptoms can make simple tasks seem impossible
– Fatigue
– Skin manifestations
– Joint stiffness
– Pain
– Depression
– Cognitive dysfunction
National Institute of Arthritis and Musculoskeletal and Skin Diseases, National Institutes of Health. Lupus: A patient care guide for nurses and other health
professionals.3rd ed. 2006. http://www.niams.nih.gov/Health_Info/Lupus/Lupus_Guide/chapter_1.asp#chp1_tre. Accessed May 8, 2013. 32

Fatigue Is One of the Most Prevalent Clinical Manifestations of SLE
88.7 85.5 82.6
0
10
20
30
40
50
60
70
80
90
100
Caucasian African American Hispanic
Zonana-Nacach A, et al. Lupus. 2000;9:101-109.
Pre
va
len
ce
of
Fa
tig
ue
(%
)
Prevalence of Fatigue Across Ethnic
Groups (N=223)
LUMINA=LUpus in MInorities: NAture Versus Nurture.
A subanalysis of 223 patients participating in LUMINA, a prospective, multiethnic study of the outcome of SLE patients diagnosed ≤5 years prior to study entry, conducted jointly by the University of Alabama at Birmingham, the University of Texas-Houston Health Science Center, and the University of Texas Medical Branch at Galveston.
• Fatigue is prevalent across caucasians, African Americans, and Hispanics
• Severity may be related to psychosocial factors and/or disease activity
33
(n=71) (n=83) (n=69)

Skin Manifestations and Photosensitivity Limit Activities of Daily Life
• Cutaneous lupus with photosensitivity is associated with significant impairments related to symptoms, emotions, daily functioning, and overall quality of life1
– Photosensitivity was self-reported in 68% of patients with cutaneous lupus1
– Disease activity may be triggered by fluorescent lights as well as sunlight2
– May cause patients to avoid outdoor activities1,3
1. Foering K, et al. J Am Acad Dermatol. 2012;66(2):220-228. 2. Rihner M, McGrath H Jr. Arthritis Rheum. 1992;35:949-952. 3. Wysenbeek AJ, et al. Ann Rheum Dis.
1989;48(6):461-463. 34

Survey: Work Loss Is a Common Consequence of SLE
Results from the National Burden of Lupus Survey, conducted by Gfk Roper Public Affairs and Communications from July through September 2011. Survey was designed to evaluate the daily and long-term impact of lupus on health, family relationships, career, and quality of life, and to identify potential gaps in communication. Includes feedback from 957 people in the lupus community (502 people with SLE [75% female], 204 supporters, 251 rheumatologists who treat SLE). Funded and developed by GlaxoSmithKline.
*To some extent.
Gfk Custom Research North America. National Burden of Disease Survey. 2011.
Only 31% of patients reported being employed
full time
63% quit work and/or retired earlier than
planned
67% reported reducing the
number of hours worked
83% said that having to leave their job was devastating*
84% said that not working
makes them feel inadequate*
35

SLE Increases Pregnancy Risks
• SLE increases several risks to mother and child1,2
• Risk of neonatal death is 7x greater than for the general population; risk of fetal death is 5x greater2
• Yet the majority of women with SLE can have successful pregnancies1
– Conceiving when lupus has been in remission ≥6 months significantly reduces risks3
– Pregnancy loss has dropped from 43% (1960-1965) to 17% (2000-2003)4
1. Clowse MEB, et al. Am J Obstet Gynecol. 2008;199(2):127.e1-127.e6. 2. Yasmeen S, et al. J Matern Fetal Med. 2001 Apr;10(2):91-96. 3. Kwok LW, et al. Lupus. 2011;20:829-
836. 4. Clark CA. J Rheumatol. 2005;32(9):1709-1712. 36
Maternal Risks Fetal Risks
Preeclampsia1 Intrauterine growth restriction1
Thrombosis1 Preterm delivery2
Maternal mortality1 Neonatal/fetal death2

Pregnancy Risks May Lead Some Women to
Avoid Having Children
• Concerns include1
– Maternal/fetal risks
– Medication teratogenicity
– Fear of genetic transmission of
lupus to children*
– Inability to care for child due to
disability or premature death
*SLE has a complex pattern of inheritance, involving multiple susceptibility genes. Both genetic and environmental factors play a role in the development of SLE, and transmission
cannot be predicted. Patient concerns about genetic transfer may be exaggerated.1,2
1. Clowse ME, et al. Arthritis Care Res. 2012;64:668-674. 2. Kelly JA, et al. Genes Immun. 2002;3(Suppl 1):S71-S85.
The majority of women with SLE
(>60%) have fewer biologic children than desired before
diagnosis, primarily by choice1
37

• 80% reported that lupus negatively impacted their ability to fulfill various family roles2
– Mother/father
– Husband/wife
– “Breadwinner”
• 88% reported that poor mental health impaired their ability to participate in activities they found enjoyable2
*To some extent.1. Boomsma MM, et al. Arthritis Rheum. 2002;47:196-201. 2. Hassett AL, et al. Arthritis Care Res (Hoboken). 2012;64(9):1341-1348. 3. Gfk Custom Research North America. National Burden of Disease Survey. 2011.
SLE Impacts Psychosocial Well-Being and Interpersonal Relationships1
Depression is common and some patients are suicidal1
68%88%
68% said lupus affects virtually
every relationship they have3*
88% reported mental health and well-being of their entire family was affected by lupus2
38

Survey: Invisible Symptoms Create a Disconnect Between Patients and Those Around Them
Results from the National Burden of Lupus Survey, conducted by Gfk Roper Public Affairs and Communications from July through September 2011. Survey was designed to evaluate the daily and long-term impact of lupus on health, family relationships, career, and quality of life, and to identify potential gaps in communication. Includes feedback from 957 people in the lupus community (502 people with SLE [75% female], 204 supporters, 251 rheumatologists who treat SLE). Funded and developed by GlaxoSmithKline.
87% of patients say they
downplay symptoms to
avoid upsetting their families*
87%DownplaySymptoms
75% of patients say their family and
friends think they can do more than
they actually can*; think they can
improve their condition by eating
better or exercising more (80%)*;
and believe they can identify with
living with lupus (67%)*
MostFeel
Misunderstood
ManyFeel
Unsupported
Only 52% of patients say their family and friends are
“very supportive”; 78% of supporters describe
themselves as “very supportive”
39*To some extent.
Gfk Custom Research North America. National Burden of Disease Survey. 2011.

Denise G.: Living With SLE
40
My coworkers don’t understand how it feels to be this tired. They resent that I’m less productive.
I stopped making plans with friends because I never
know what tomorrow will bring. They take it personally. They don’t realize how real my symptoms are.
I’m starting to feel so alone.
Patient perspective is for educational purposes only
and represents hypothetical patient.
11/14/2012

Patient Support

Survey: Communication Gaps Exist Between Patients and Caregivers
Results from the National Burden of Lupus Survey, conducted by Gfk Roper Public Affairs and Communications from July through September 2011. Survey was designed to evaluate the daily and long-term impact of lupus on health, family relationships, career, and quality of life, and to identify potential gaps in communication. Includes feedback from 957 people in the lupus community (502 people with SLE [75% female], 204 supporters, 251 rheumatologists who treat SLE). Funded and developed by GlaxoSmithKline.
42
52% of patients with lupus report they
minimize their symptoms when they talk to their
physicians*
72% of physicians are unaware that patients
tend to under-report
their symptoms*
*To some extent.
Gfk Custom Research North America. National Burden of Disease Survey. 2011.

87% of patients wish there were more resources available to them*
43
Survey: Patients May Feel Less Supported Than Their Doctors Realize
Results from the National Burden of Lupus Survey, conducted by Gfk Roper Public Affairs and Communications from July through September 2011. Survey was designed to evaluate the daily and long-term impact of lupus on health, family relationships, career, and quality of life, and to identify potential gaps in communication. Includes feedback from 957 people in the lupus community (502 people with SLE [75% female], 204 supporters, 251 rheumatologists who treat SLE). Funded and developed by GlaxoSmithKline.
54% of doctors
are frustrated by the limited
resources available to
educate their patients*
*To some extent.
Gfk Custom Research North America. National Burden of Disease Survey. 2011.

Patient Counseling May Improve Quality of Life for Those With SLE1
• Unpredictable nature of SLE had the greatest impact on emotional distress and quality of life2*
– Frequency of flare was associated with depression and anxiety3
• Increased education and perception of control over the illness were associated with reduced depression and anxiety regarding SLE challenges3
• Environmental triggers, such as exposure to ultraviolet light, may be modified to limit onset and severity of flares4
1. Karlson EW, et al. Arthritis Rheum. 2004;50(6):1832-1841. 2. Gfk Custom Research North America. National Burden of Disease Survey. 2011. 3. Beckerman NL, et al. J Multidiscip Healthc. 2011;4:63-72. 4. National Institute of Arthritis and Musculoskeletal and Skin Diseases, National Institutes of Health. Lupus: A patient care guide for nurses and other health professionals. 3rd ed. 2006. http://www.niams.nih.gov/Health_Info/Lupus/Lupus_Guide/chapter_1.asp#chp1_tre. Accessed May 8, 2013. 44
*To some extent.

Patient Interactions Are Opportunities to Provide Support
• Foster open communication1
– Ask how patients are coping1
• Changes in physical appearance
• Limitations on daily function
• Emotional state
• Socioeconomic challenges
• Emphasize participation in patient
support groups and other resources1
• Provide patient education1
1. Beckerman NL, et al. J Multidiscip Healthc. 2011:63-72. 2. National Institute of Arthritis and Musculoskeletal and Skin Diseases, National Institutes of Health. Lupus:
A patient care guide for nurses and other health professionals. 3rd ed. 2006. ttp://www.niams.nih.gov/Health_Info/Lupus/Lupus_Guide/chapter_1.asp#chp1_tre.
Accessed May 8, 2013. 45
• Remind patients to schedule regular preventive care visits2
– Primary care, gynecologist, dentist, optometrist

Empower Patients to Take Charge of the Factors They Can Control
✔ Diet1
Eat a balanced diet to minimize cardiovascular risk and inflammation,
maintain bone health, and prevent anemia
✔ Exercise1
As tolerated, for physical/mental health and reduced fatigue
✔ Sunscreen1
Protect against both UVA and UVB rays, fluorescent lights
“Broad-spectrum protection” sunscreen with minimum SPF 15
✔ Sleep1
8-10 hours a night to combat fatigue; naps whenever needed
Reinforce that need for rest is not laziness
✔ Stress1-3
Practice stress management techniques
✔ Smoking1
Emphasize the importance of not smoking
✔ Immunizations1,4
Human papillomavirus; influenza and pneumococcal, with killed vaccines
1. National Institute of Arthritis and Musculoskeletal and Skin Diseases, National Institutes of Health. Lupus: A patient care guide for nurses and other health professionals. 3rd ed. 2006.
http://www.niams.nih.gov/Health_Info/Lupus/Lupus_Guide/chapter_1.asp#chp1_tre. Accessed May 8, 2013. 2. Greco CM, et al. Arthritis Rheum. 2004;51(4):625-634. 3. Da Costa D,
et al. Arthritis Care Res. 1999;12(2):112-119. 4. van Assen S, et al. Ann Rheum Dis. 2011;70:414-422. 46

Focus on the Positive
Results from the National Burden of Lupus Survey, conducted by Gfk Roper Public Affairs and Communications from July through September 2011. Survey was designed to evaluate the daily and long-term impact of lupus on health, family relationships, career, and quality of life, and to identify potential gaps in communication. Includes feedback from 957 people in the lupus community (502 people with SLE [75% female], 204 supporters, 251 rheumatologists who treat SLE). Funded and developed by GlaxoSmithKline.
More than half (56%) of people
with lupus reported feeling
hopeful or optimistic, regardless of lupus*
56%Feel
Hopeful
Living with lupus affects my life, but
does not define me as a person:
87%*
87%Don’t Let Lupus
Define Them
My healthcare professional is the best there
is when it comes to managing my lupus:
82%*
82%Trust HCPWith Care
Positive Outlook
47*To some extent.
Gfk Custom Research North America. National Burden of Disease Survey. 2011.

I was so achy today, but I pushed myself to put on sunblock and go for a 20-minute walk because I promised Nurse Samuels I would.
I am so glad I did! It gave me energy.
The fresh air really reminded me to
take things one day at a time and appreciate everything I have.
It’s strange, but in some ways, lupus has been a wake-up call.
It’s caused me to slow down and realize what is truly important in life.
Patient perspective is for educational purposes only
and represents hypothetical patient.
48
3/25/2012
Denise G.: Facing SLE With a Positive Outlook

Key Takeaways

Key Takeaways
• SLE is an autoimmune disease with a range of
manifestations and variable course, which make
diagnosis a challenge
50©2013 GlaxoSmithKline group of companies. All rights reserved.
Produced in USA. BN2280R0 May 2013

Key Takeaways
• SLE is an autoimmune disease with a range of
manifestations and variable course, which make
diagnosis a challenge
• The pathogenesis of SLE involves immune dysfunction
leading to autoantibody production, inflammation, and
organ/tissue damage
50©2013 GlaxoSmithKline group of companies. All rights reserved.
Produced in USA. BN2280R0 May 2013

Key Takeaways
• SLE is an autoimmune disease with a range of
manifestations and variable course, which make
diagnosis a challenge
• The pathogenesis of SLE involves immune dysfunction
leading to autoantibody production, inflammation, and
organ/tissue damage
• Immune dysfunction and subsequent organ/tissue
damage leave patients with SLE at risk for serious
chronic conditions and premature mortality
50©2013 GlaxoSmithKline group of companies. All rights reserved.
Produced in USA. BN2280R0 May 2013

Key Takeaways
• SLE is an autoimmune disease with a range of
manifestations and variable course, which make
diagnosis a challenge
• The pathogenesis of SLE involves immune dysfunction
leading to autoantibody production, inflammation, and
organ/tissue damage
• Immune dysfunction and subsequent organ/tissue
damage leave patients with SLE at risk for serious
chronic conditions and premature mortality
• SLE has a significant impact on daily function, work loss,
interpersonal relationships, and emotional health
50©2013 GlaxoSmithKline group of companies. All rights reserved.
Produced in USA. BN2280R0 May 2013

Key Takeaways
• SLE is an autoimmune disease with a range of
manifestations and variable course, which make
diagnosis a challenge
• The pathogenesis of SLE involves immune dysfunction
leading to autoantibody production, inflammation, and
organ/tissue damage
• Immune dysfunction and subsequent organ/tissue
damage leave patients with SLE at risk for serious
chronic conditions and premature mortality
• SLE has a significant impact on daily function, work loss,
interpersonal relationships, and emotional health
• Patient education and empowerment are valuable tools for improving quality of life
50©2013 GlaxoSmithKline group of companies. All rights reserved.
Produced in USA. BN2280R0 May 2013

Thank You!