Acute monoarthropathy Jaya Ravindran Rheumatologist

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Acute monoarthropathy
Jaya Ravindran
Rheumatologist

Aims
• an approach to the investigation and differential diagnosis of acute monoarticular pain
• focus on septic and crystal arthritis

Acute Monoarthritis - differential diagnosis
– Septic arthritis
– Crystal arthritis• Gout (uric acid)• Pseudogout/calcium pyrophosphate deposition
disease (CPPD)

What are other differentials for
acute monoarticular pain?

Monoarthritis - differential diagnosis
Psoriatic arthritis– Onycholysis– Subungual hyperkeratosis– Pitting– Extensor surfaces, scalp,
natal cleft, umbilicus– Other associated features
eg uveitis, inflammatory bowel disease, enthesitis, Ankylosing spondylitis

Monoarthritis - differential diagnosis
Reactive arthritis• Prodromal GI /GU
Infection eg
campylobacter,
salmonella, shigella,
Yersinia,chlamydia• Pustular psoriasis
and circinate balanitis

Monoarthritis - differential diagnosis
– Trauma - # and haemarthroses (warfarin, bleeding disorders)
– Palindromic rheumatism – 24-48 hours inflammatory monoarthritis, can evolve into polyarthritis eg RA

Others to think about• Osteonecrosis/AVN (steroids/alcohol)• Severe pain but good ROM
• Monoarticular RA
• Monoarticular OA
• Prosthetic joint - loosening, # or infection
• Periarticular pathology

Articular vs periarticular?

Is it an articular or extra-articular problem?
• ARTICULAR PERI-ARTICULAR
• pain all planes pain in plane of tendon• active = passive active > passive• capsular swelling/effusion linear swelling• joint line tenderness localised tenderness• diffuse erythema/heat localised
erythema/heat

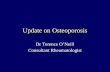
Olecranon bursitis

Septic arthritis
• 15-30 per 100,000 population
• Fatal in 11% of cases in UK
• Delayed or inadequate treatment leads to irreversible joint damage

How do you get septic arthritis?

Pathogenesis

Who gets septic arthritis?

Who gets septic arthritis?
• common organisms Staphylococci or Streptococcus
• young adults, significant incidence gonococcal arthritis
• Elderly & immunocompromised gram -ve organisms
• Anaerobes more common with penetrating trauma

Who gets septic arthritis?• pre-existing joint disease
• prosthetic joints
• low SE status, IV drug abuse, alcoholism
• diabetes, steroids, immunosuppression
• previous intra-articular steroid injection

Who gets septic arthritis?
• Skin lesions e.g. ulcers, particularly in context RA often source of infection
• poor prognostic features: older, pre-existing joint disease & presence of synthetic material within joint

What are the signs and
symptoms of septic
arthritis?

Symptoms & signs of septic arthritis
• Typically hot, swollen, red tender joint with reduced range of movement, difficulty weight bearing
• Systemic upset• Night and rest pain • Symptoms usually
present for < 2/52 • Large joints more
commonly affected than small
• majority of joint sepsis in hip or knee

Symptoms & signs of septic arthritis
• In pre-existing inflammatory joint disease symptoms in affected joint(s), out of proportion to disease activity in other joints.
• 10-15% of cases, > one joint - so polyarticular presentation does not exclude sepsis
• presence of fever not reliable indicator- if clinical suspicion high - treat

What investigations are useful
in septic arthritis?

Investigations
• Synovial fluid aspiration– volume/viscosity/
cellularity/appearance– gram stain/culture– Absence of organism does
not exclude septic arthritis– polarised light microscopy
(crystals)
– NB suspected prosthetic joint sepsis should ALWAYS be referred to orthopaedics

Investigations
• Always blood cultures
• significant proportion blood cultures + ve in absence of + ve synovial fluid cultures
• FBC ESR & CRP
• BUT absence of raised WBC, ESR or CRP not exclude diagnosis of sepsis - if clinical suspicion high always treat

Other investigations• CRP useful for monitoring response to
treatment
• Urate may be normal in acute gout and of no diagnostic value in acute gout or sepsis
• Measure urea, electrolytes & liver function for end organ damage (poor prognostic feature)
• Renal function may influence antibiotic choice

Other tests?
• If skin pustule is present, suggestive of gonococcal infection, then skin swab should be taken
• If history suggests possibility of genitourinary or respiratory tract infection then culture sputum (and CXR) & urine & take anogenital & throat swabs where appropriate
• If periarticular sepsis – appropriate swabs and cultures

Imaging
• Plain X rays no benefit in diagnosis but form baseline for any future joint damage. May show chondrocalcinosis.
• MRI useful in distinguishing sepsis from OA but less good between sepsis & inflammation
• MRI sensitive for osteomyelitis

Imaging
• Ultrasound useful in guiding needle aspiration eg hip
• White cell scanning helpful in diagnosing prosthetic sepsis

Antibiotic treatment of septic arthritis
• Local and national guidelines
• Liaise with micro. guided by gram stain
• Conventionally given iv for 2 weeks or until signs improve, then orally for around 4 weeks

Joint drainage & surgical options
• medical aspiration, surgical aspiration via arthroscopy or open arthrotomy
• Suspected hip sepsis – early orthopaedic referral – may need urgent open debridement

Recommendations specific to 1o care & emergency department
• commonest hot joint to present in 1o care is 1st MTP gout
• usually diagnosed on clinical grounds without needle aspiration or referral to hospital. (Make referral if inadequate recovery)
• Some GPs aspirate & inject joints for inflammatory arthritis or osteoarthritis. If withdraw pus/unexpected cloudy fluid should send sample with patient to local emergency department

Recommendations specific to 1o care & emergency department
• GPs & doctors in EAU should refer patients with suspected septic arthritis to specialist with expertise to aspirate joint. May be orthopaedic surgeon or rheumatologist
• Admit if sepsis is suspected or confirmed.

Summary
• with a short history of a hot, swollen, tender joint (or joints) plus restriction of movement; septic arthritis until proven otherwise
• If clinical suspicion high investigate & treat as septic arthritis even in absence of fever

THANK-YOU
Related Documents