




DISCUSSION
ST ELEVATION MYOCARDIAL INFARCTION (STEMI)
DEFINITION
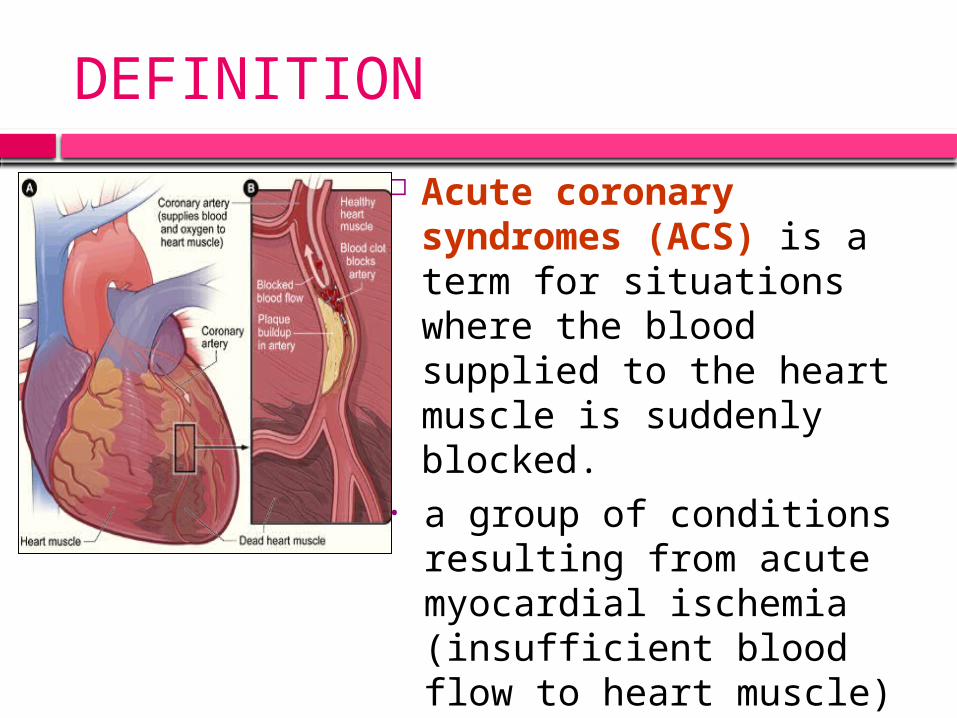
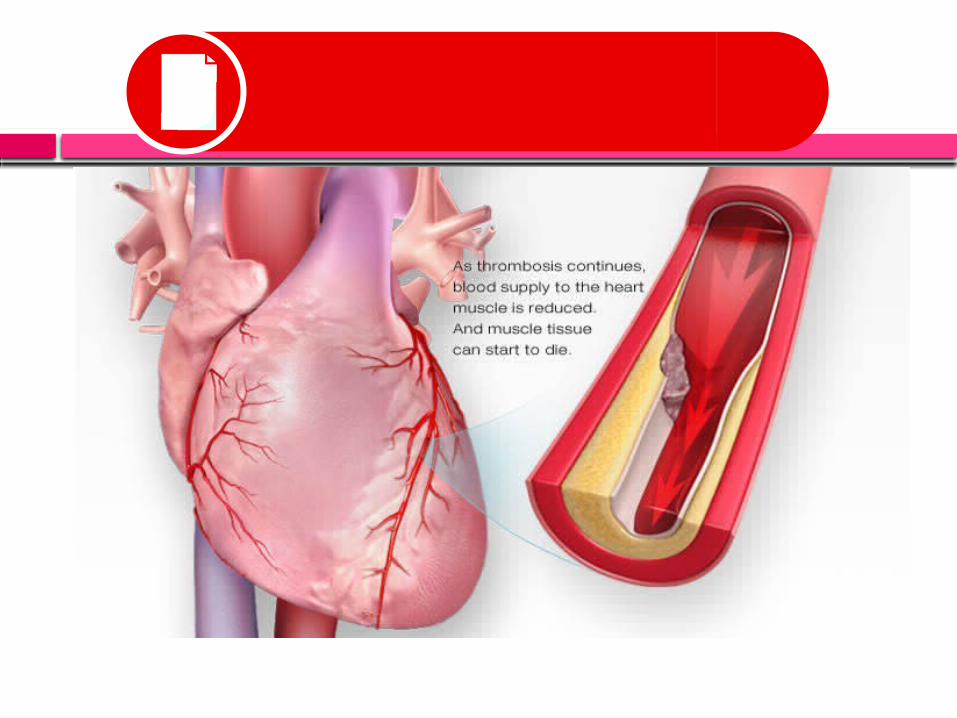
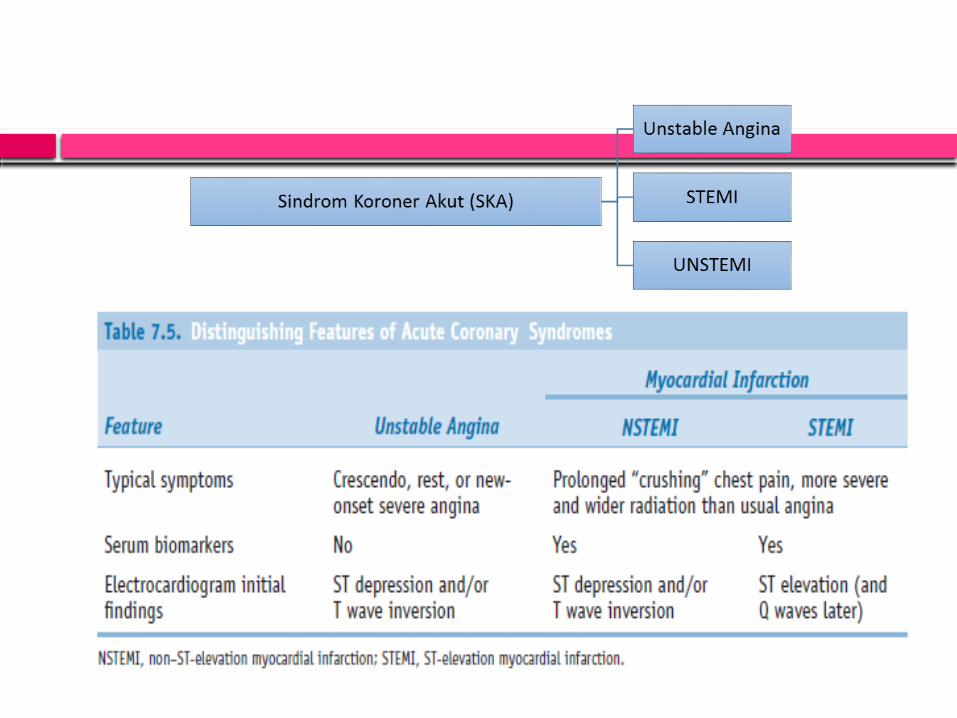
Acute coronary syndromes (ACS) is a term for situations where the blood supplied to the heart muscle is suddenly blocked.
• a group of conditions resulting from acute myocardial ischemia (insufficient blood flow to heart muscle)
• ranging from unstable angina (increasing, unpredictable chest pain) to myocardial infarction (heart attack).
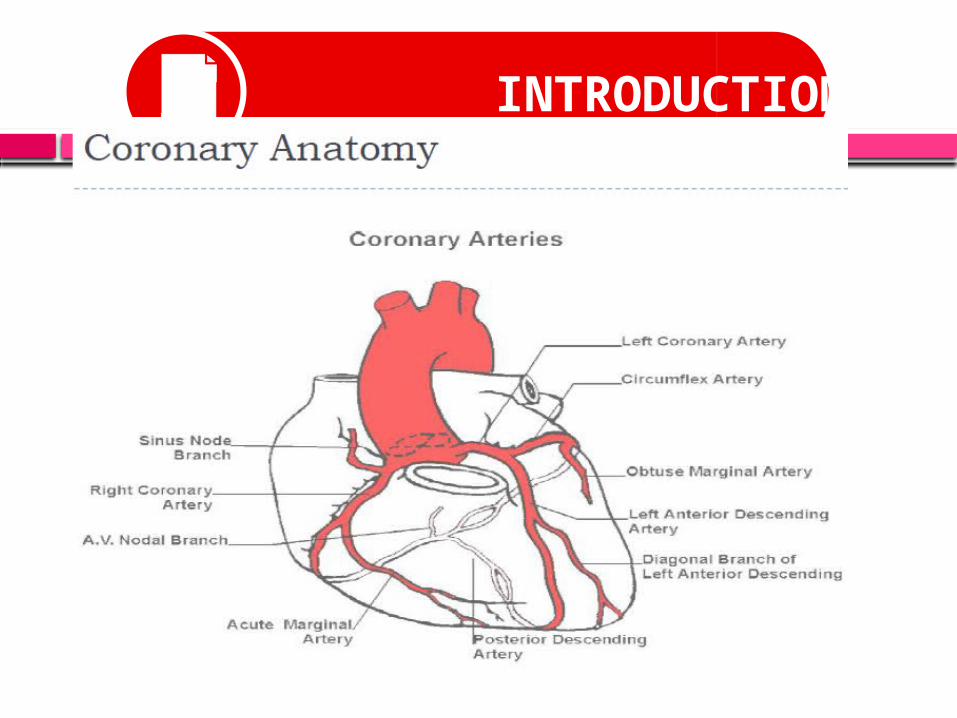
INTRODUCTION
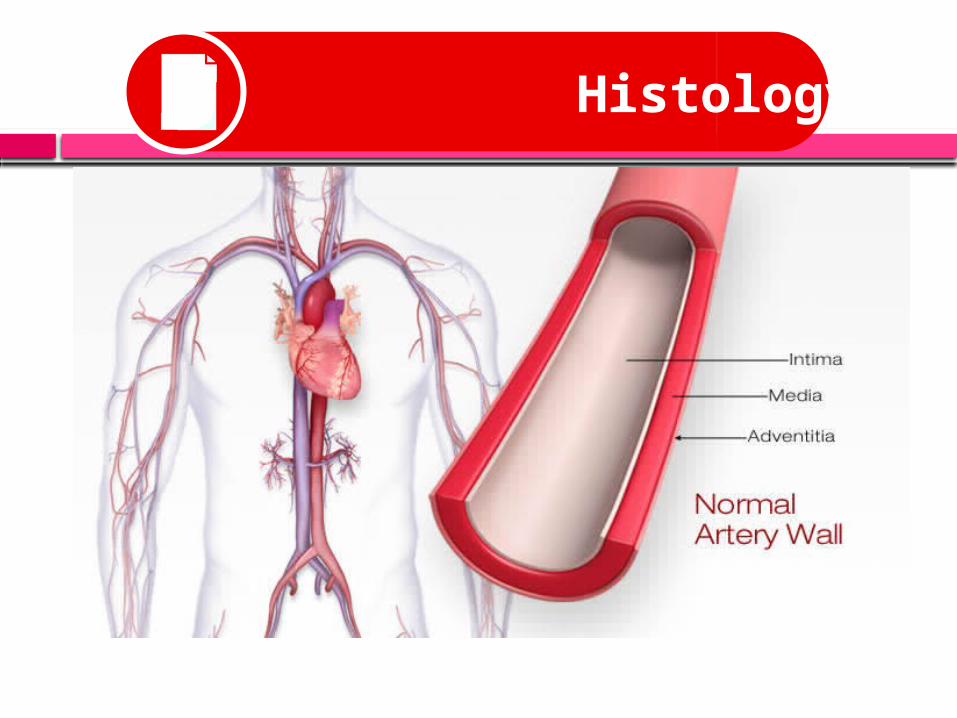
Histology

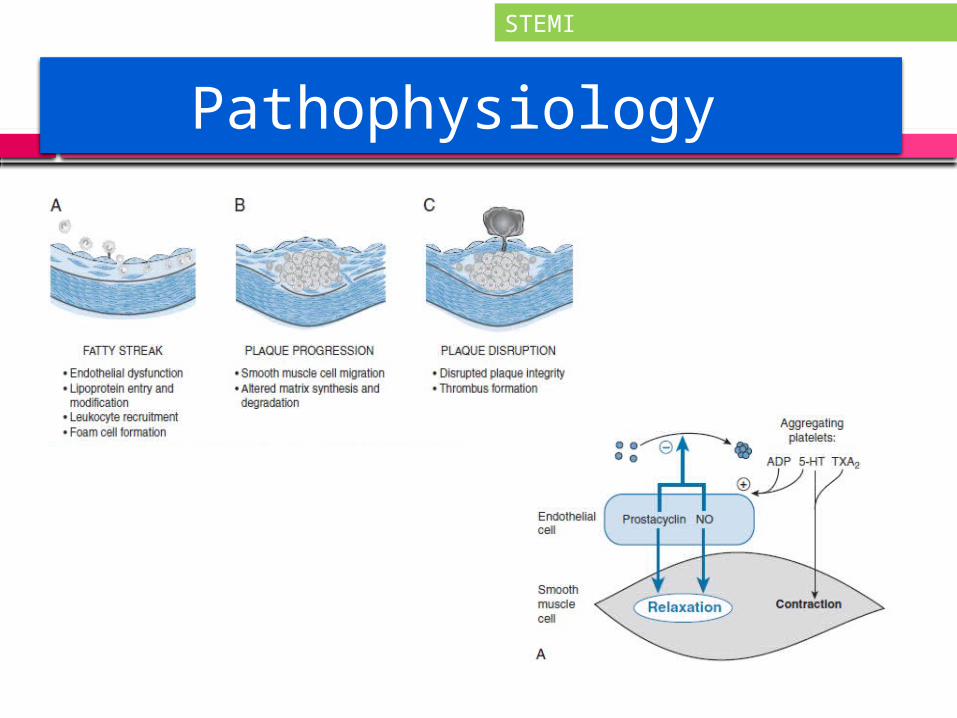
Pathophysiology
STEMI


PATHOPHYSIOLOGY

PATHOPHYSIOLOGY

PATHOPHYSIOLOGY
PATHOPHYSIOLOGY

PATHOPHYSIOLOGY

ACUTE CORONARY SYNDROME
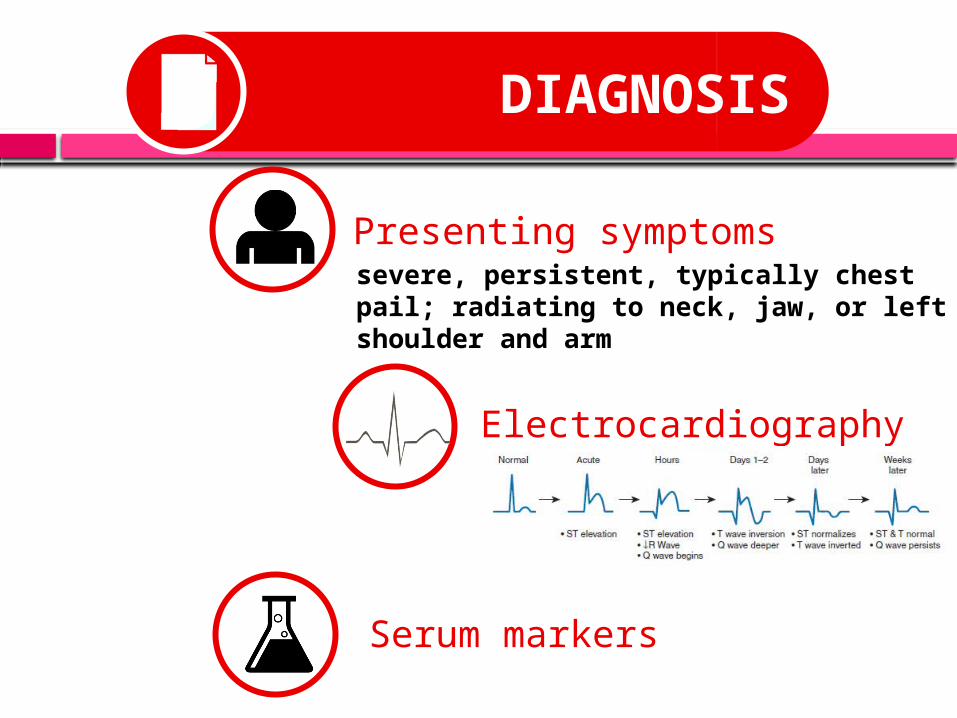
DIAGNOSIS
Presenting symptoms
Electrocardiography
Serum markers
severe, persistent, typically chest pail; radiating to neck, jaw, or left shoulder and arm
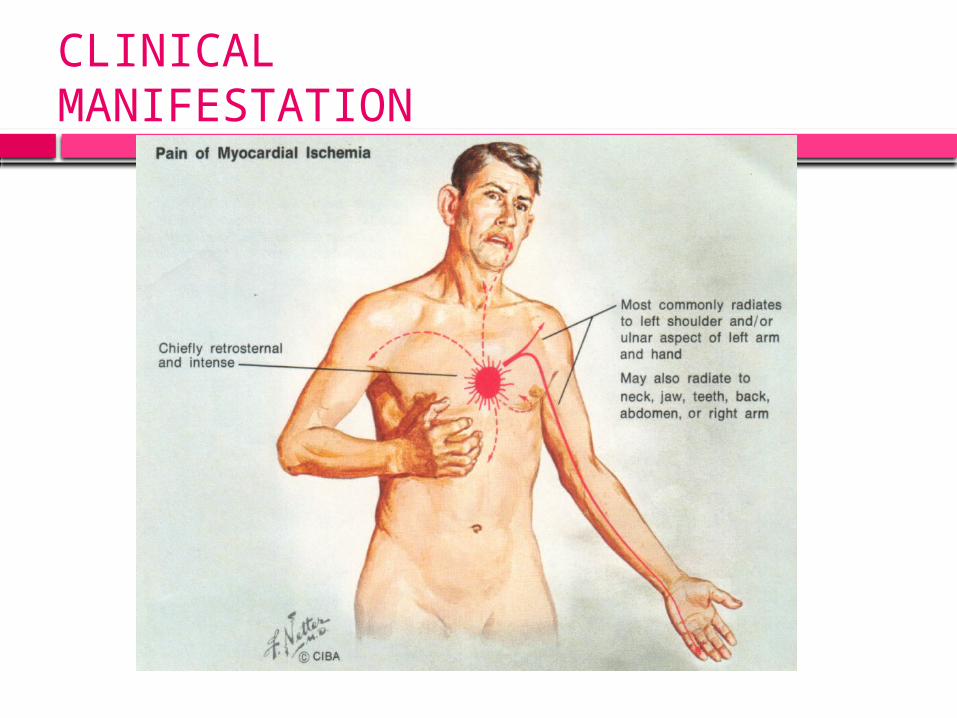
CLINICALMANIFESTATION
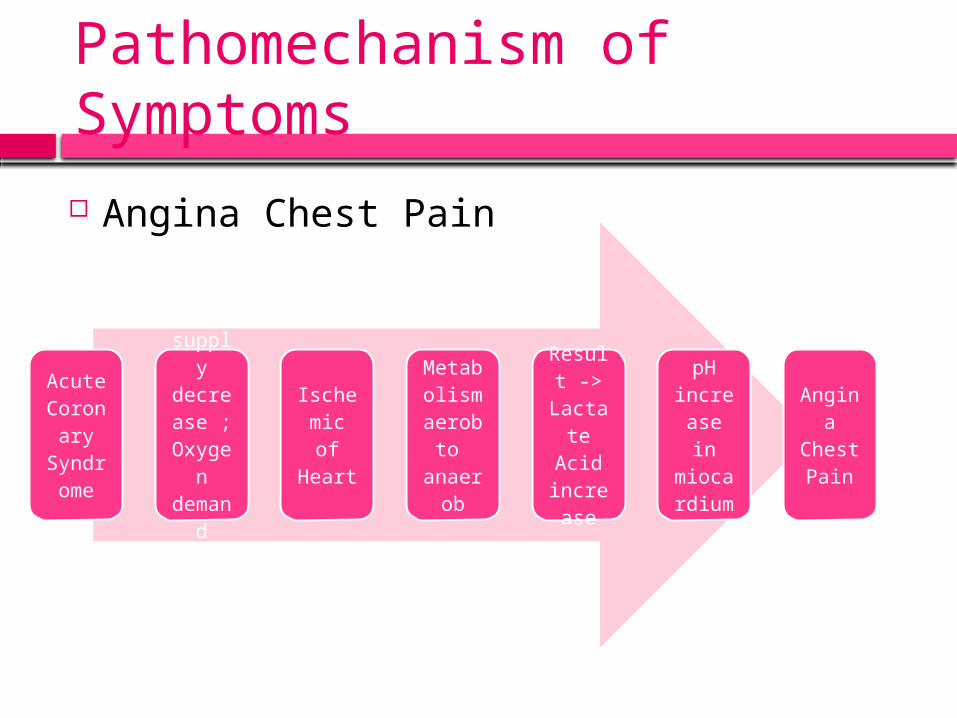
Pathomechanism of Symptoms Angina Chest Pain
Acute Coron
ary Syndrome
Oxygen
supply
decrease ; Oxyg
en dema
nd increa
se
Ischemic of Heart
Metabolism aerob
to anaer
ob
Result ->
Lactate Acid increa
se
pH increase in
miocardium
Angina
Chest Pain


Electrocardiography
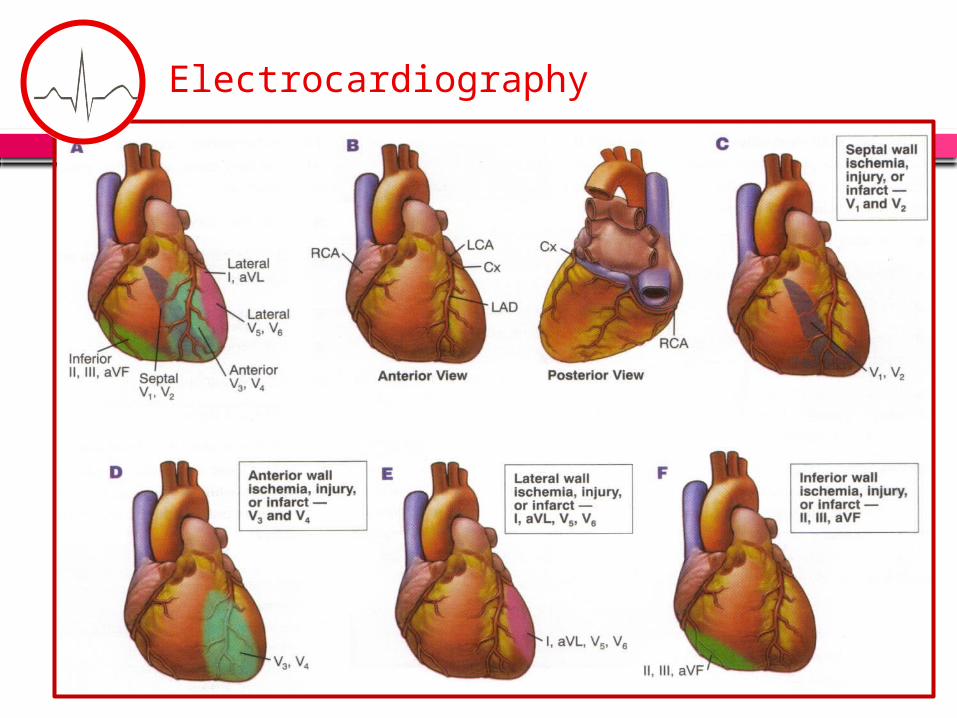
Electrocardiography
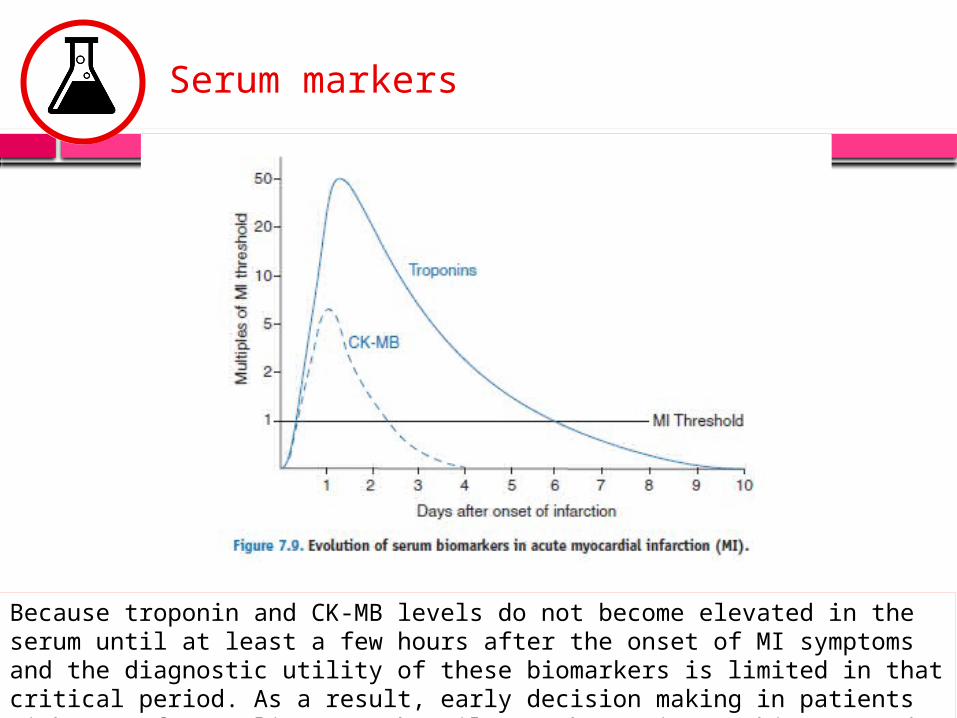
Because troponin and CK-MB levels do not become elevated in the serum until at least a few hours after the onset of MI symptoms and the diagnostic utility of these biomarkers is limited in that critical period. As a result, early decision making in patients with ACS often relies most heavily on the patient’s history and ECG findings.
Serum markers
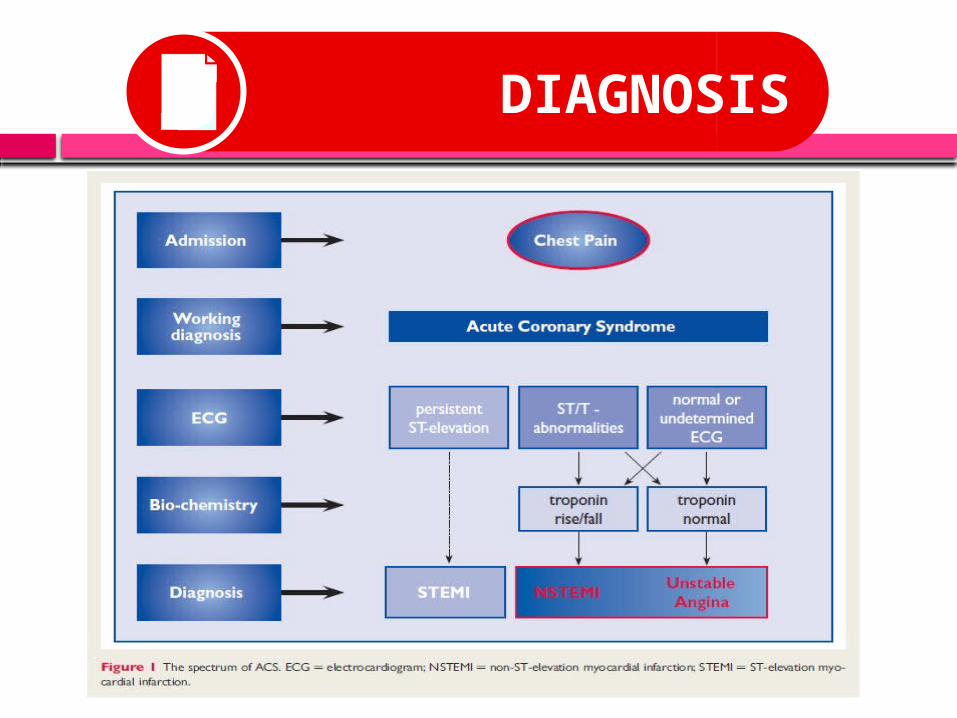
DIAGNOSIS

GOAL OF TREATMENT
Relieve pain
Hemodynamic stabilization
Myocardial reperfusion
Prevent the complication
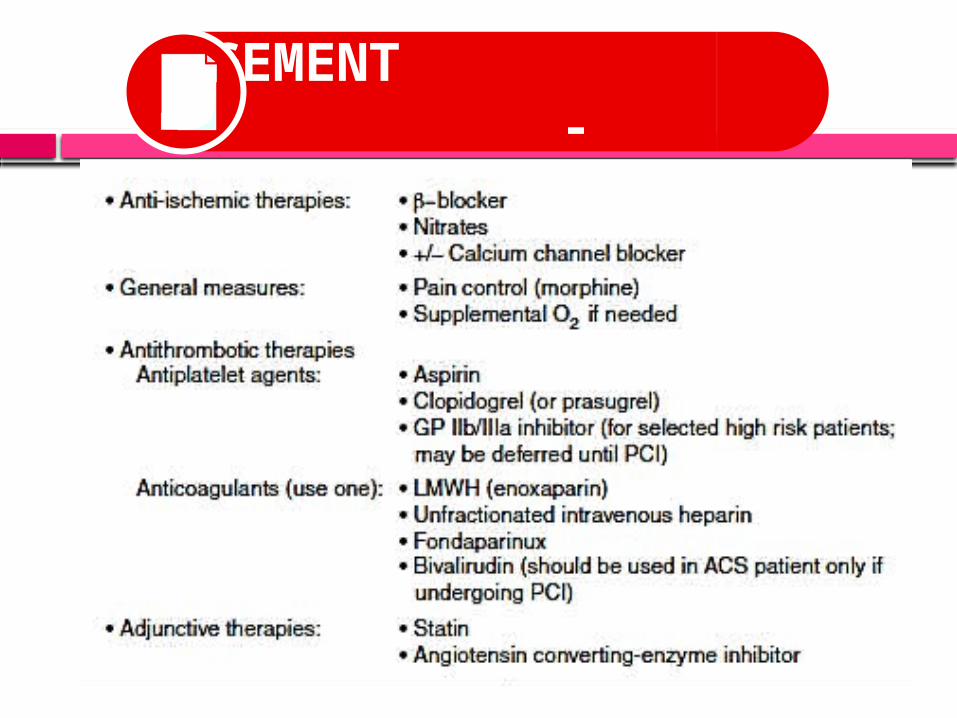
MANAGEMENT - Medications -


MANAGEMENT - Reperfusion Therapy -
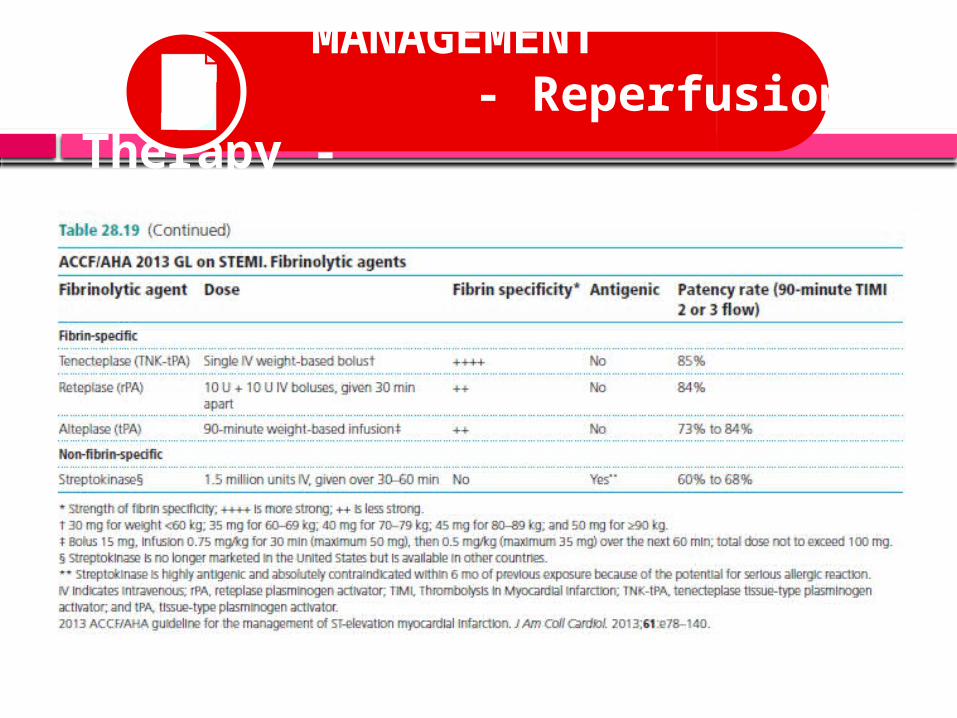
MANAGEMENT - Reperfusion Therapy -
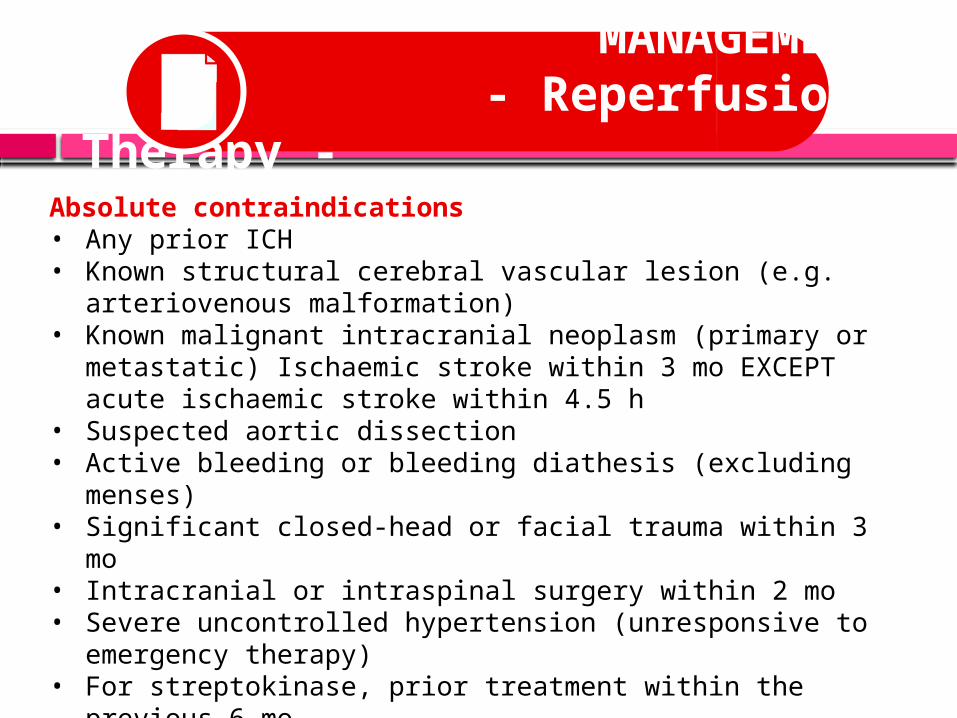
MANAGEMENT - Reperfusion Therapy -
Absolute contraindications• Any prior ICH• Known structural cerebral vascular lesion (e.g. arteriovenous
malformation)• Known malignant intracranial neoplasm (primary or metastatic)
Ischaemic stroke within 3 mo EXCEPT acute ischaemic stroke within 4.5 h
• Suspected aortic dissection• Active bleeding or bleeding diathesis (excluding menses)• Significant closed-head or facial trauma within 3 mo• Intracranial or intraspinal surgery within 2 mo• Severe uncontrolled hypertension (unresponsive to emergency
therapy)• For streptokinase, prior treatment within the previous 6 mo

MANAGEMENT - Reperfusion Therapy -
Relative contraindications• History of chronic, severe, poorly controlled hypertension• Significant hypertension on presentation (SBP >180 mmHg or DBP
>110 mmHg)• History of prior ischaemic stroke >3 mo• Dementia• Known intracranial pathology not covered in absolute
contraindications• Traumatic or prolonged (>10 min) CPR• Major surgery (<3 wk)• Recent (within 2 to 4 wk) internal bleeding• Non-compressible vascular punctures• Pregnancy• Active peptic ulcer• Oral anticoagulant therapy
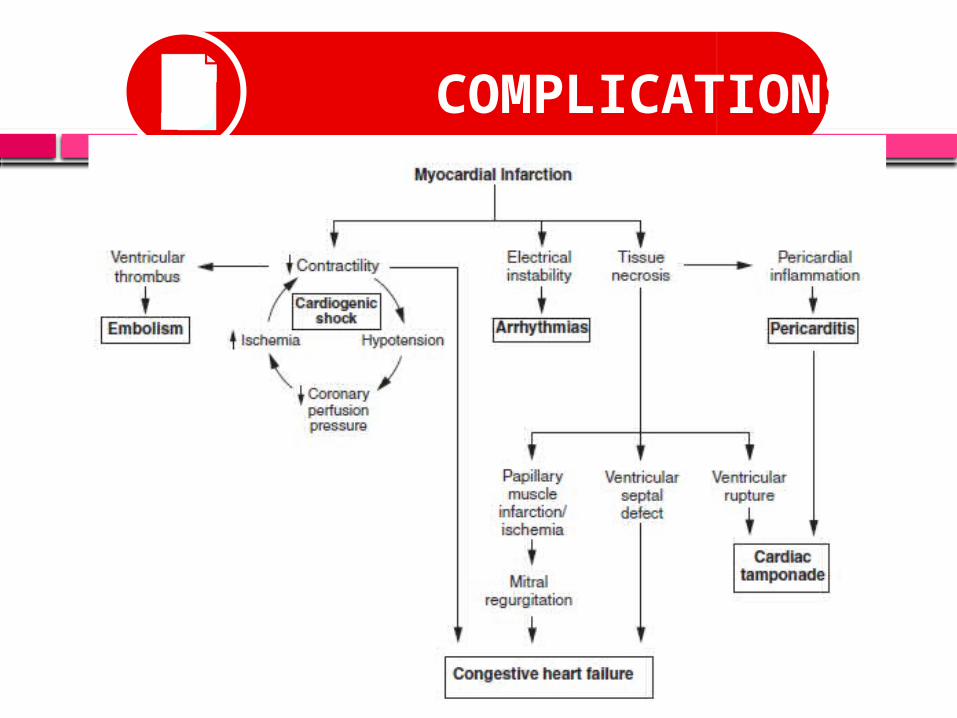
COMPLICATIONS

PROGNOSIS






























