Date of preparation: April 2015UK/G-NHS/1114/0058ac
Your ToolkitPolypharmacy Medicines Optimisation Review (PMOR)
The polypharmacy medicines review project, The Medicines Optimisation Academy and production of the supporting materials, including this leaflet, have been wholly supported with funding from RB Healthcare UK Ltd.
1

Having downloaded Your Toolkit, the next step is to implement a PMOR in your CCG for PPI patients. We have therefore provided all you will need to carry this out simply and efficiently. This toolkit includes information for you, your colleagues and your patients.
A step-by-step guide to your PMOR1. Raise awareness among GPs of rebound acid hypersecretion and how it can be managed with the use of
licensed alginate preparations
2. Identify those responsible to champion, train, educate and engage healthcare professionals and patients1,2
• Establish that PPIs are, in some instances, being prescribed unnecessarily3-5
• Understand the role of polypharmacy patient reviews in reducing drug use1,2
• Recognise that symptoms of rebound acid hypersecretion6 resulting from long-term PPI use make it difficult for patients to reduce PPI intake, and that this defines the role of alginates as short-term rescue medication
• Address team members’ objections to PPI-indicated PMOR
Prepare protocols to:
• aid in the understanding of indications for PPI
• aid in the understanding of the choice of NSAID
• give advice on those instances where SSRIs may be discontinued
3. Create a baseline audit of patients taking PPIs for more than eight weeks, who, having been filtered by robust exclusion criteria, are selected for review.
4. Conduct patient reviews, by invitation to the clinic. At consultation, ensure any change in medication is agreed with the patient. Education and support is provided in the form of patient information leaflets with advice on PPIs, NSAIDs and SSRIs, and support for making healthy lifestyle changes.
Ensure community pharmacies in the area are informed of PMOR project activity, so that they are prepared to advise patients who may present with questions as to why their medication has been changed. Patient satisfaction surveys are completed at 4 months in order to assess effectiveness of this strategy on prescribing costs. These surveys assess any changes that may have been made and look at patients’ opinions of the review process, together with feedback from healthcare professionals involved. Such surveys are in line with Patient Reported Outcomes Measures (PROMs) guidelines, which assess the quality of care delivered to NHS patients from the patients’ perspective.
Introduction
2

1 McGinn D, Roberts C. Outcomes of a medication optimisation review in patients taking proton pump inhibitors. Guidelines in Practice. January 2015.
2 Dr. Spencer. Medicines optimisation reviews in patients taking PPIs. Reprinted from Prescriber 5 May 2013.
3 Forgacs I. BMJ 2008;336(7634):2-3.
4 Walker NM, McDonald J. Pharmacy World and Science 2001; 23(3):p116-117.
5 Gupta R et al. Overuse of Acid Suppression Therapy in Hospitalized Patients.
6 Reimer C et al. Proton-Pump Inhibitor Therapy Induces Acid-Related Symptoms in Healthy Volunteers After Withdrawal of Therapy. Gastroenterology 2009;137:80-78.
References
3

Contents
Here is an overview of the contents of this toolkit and how each item has been designed to help you:
Protocols5 PPI protocol
• A comprehensive 14-page booklet. It provides a protocol for prescribing PPIs - initiation, review and how discontinuation of PPIs is part of the medications review process
19 NSAID protocol• A comprehensive 10-page booklet. It provides a protocol for prescribing NSAIDs - initiation, review and
how discontinuation of NSAIDs is part of the medications review process
PMOR implementation materials29 Objection Handler
• This will help you overcome any objections and answer questions your colleagues may have in order for you to put together a local PMOR team
30 Medication Review Process for PPI patients• Provides details of those patients who are not suitable for a PPI review, or who may be considered for a
PPI dose step-down, to help you select the most appropriate patients for the PMOR
33 Dyspepsia Clinic Patient Invitation• An example of how you could invite patients for a review appointment
34 Pharmacy Letter• A 2-page leaflet to inform community pharmacists of the planned PMOR and assist with patients’ questions
36 Patient Satisfaction Questionnaire• A short, post-review questionnaire to gain patient feedback in line with PROM guidelines
37 Audit spreadsheet• An example of a patient overview spreadsheet showing types of information to be captured at a review.
It will also assist you in measuring project outcomes
38 Discontinuation of SSRIs in Adults• A 4-page guide to discontinuing SSRIs in adults
Patient Leaflets42 SSRI Patient Leaflet
• Information about SSRIs and discontinuing them safely
44 PPI Patient Leaflet • A leaflet providing reassurance to patients stepping-down or off PPIs, with advice on managing rebound
symptoms
46 NSAID Patient Leaflet• Information about taking NSAIDs and the need for reviews
48 Healthy Living Patient Leaflet• Lifestyle advice and support
4

Protocol For PrescribingProton Pump InhibitorsInitiation, Review & Discontinuation
Date of preparation: April 2015UK/G-NHS/1114/0058p
This material was authored by Diane McGinn, Medicines Management Consultant, Preston, Lancashire, UK
The polypharmacy medicines review project, The Medicines Optimisation Academy and production of the supporting materials, including this leaflet, have been wholly supported with funding from RB Healthcare UK Ltd.
5
1 Indications for PPI
1.1 Treatment and Maintenance Therapy for GI Indication
• Lifestyle Advice
• Risks Associated with PPIs
• Licensed Indications, Doses, Length of Treatment
• Read Codes for GI Indications
• Patient Information and Review Timescales
1.2 Prophylaxis of GI Complications due to other Drugs
• Drugs Requiring use of Gastro-Protection
2 Medication Review Process2.1 Exclusion Criteria
2.2 Stepping down PPI dose
2.3 Stopping PPI and/or other meds
3 PPI Polypharmacy Medication Review Process3.1 Exclusion Criteria
3.2 Discontinuation of NSAIDs in Adults
Contents
6
1.1 Treatment and Maintenance Therapy for GI IndicationDiagnosis, referral and management should follow NICE CG184 2014 Management of dyspepsia in adults in primary care.
On first presentation with dyspepsia symptoms:
• Review medications for possible causes of dyspepsia, for example, calcium antagonists, nitrates, theophyllines, bisphosphonates, steroids and non-steroidal anti-inflammatory drugs (NSAIDs). Patients undergoing endoscopy should be free from medication with either a proton pump inhibitor (PPI) or an H2 receptor antagonist (H2RA) for a minimum of 2 weeks.
• If patient needs endoscopy stop NSAID and also where possible in uninvestigated dyspepsia patients.
• Consider trial of alginate or antacid if not already taking and review in one month if not needing referral.
Lifestyle Advice
• Offer simple lifestyle advice, including advice on healthy eating, weight reduction and smoking cessation.
• Advise patients to avoid known precipitants they associate with their dyspepsia where possible. These may include smoking, alcohol, coffee, chocolate, fatty foods and being overweight.
• Raising the head of the bed (using bricks or a plank of wood, not by using more pillows) and having a main meal well before going to bed may help some people.
Read codes for lifestyle advice should be recorded as follows:
• Lifestyle counselling 67H
• Smoking cessation advice 8CAL
• Patient advised re diet 8CA4
• Alcohol advice 8CAM
• Advice re exercise 8CA5
Provide patient information leaflets - www.patient.co.uk - for conditions as below plus local lifestyle and PPI step-down step-off leaflet.
• Dyspepsia (indigestion)
• Acid reflux and oesophagitis
Risks Associated with PPIs
PPIs may be associated with an increased risk of
• C. difficile
• Fractures of wrist, hip and spine
• Pneumonia
Consider if benefits of PPI outweigh risks for patients susceptible to these conditions e.g. elderly, care home residents, respiratory patients. Review continuing need for treatment regularly.
1 Indications for PPIs
7

Licensed Indications, Doses, Length of Treatment
PPIs may be used to treat uninvestigated dyspepsia, non-ulcer dyspepsia (NUD), gastro-oesophageal reflux disease (GORD) and peptic ulcer disease (PUD).
Generic omeprazole or lansoprazole capsules should be used first line. Dispersible formulations should be reserved for patients with dysphagia.
Refer to NICE algorithms for management pathway. Table 1 shows recommended dosages and treatment lengths from NICE.
Read Codes for GI Indications
Recording indication for PPI prescribing using Read code speeds up medication review and assists other HCPs who may see the patient.
Frequently used indications are as follows:
• Dyspepsia
• GORD
• Oesophagitis
• Hiatus hernia
• Reflux
• Gastritis
• Barrett’s oesophagus
• Non-ulcer dyspepsia
• Peptic ulcer disease
Patient Information and Review Timescales
• Ensure patients are aware of why they have been prescribed a PPI - supply patient leaflet from www.patient.co.uk
• Prescribe as acute for one month and ask patient to arrange a review appointment.
• Only put PPI on repeat if need for long-term therapy has been established.
• Explain to patients that over time their dose may be reduced and they may be asked to stop treatment once symptoms are well controlled - supply leaflet on step-down step-off.
8

Dosage information on proton pump inhibitors (NICE CG184 2014)1
Table 1. PPI doses relating to evidence synthesis and recommendations in the original
CG17; 2004 guideline
Table 2. PPI doses for severe oesophagitis in the NICE CG184 2014 update
Table 3. PPI doses for H pylori eradication therapy in the NICE CG184 2014 update
Esomeprazole 20mg1 once a day Not available 40 mg3 once a day
Lansoprazole 30mg once a day 15mg once a day 30mg2 twice a day
Omeprazole 20mg once a day 10mg2 once a day 40mg once a day
Pantoprazole 40mg once a day 20mg once a day 40mg2 twice a day
Rabeprazole 20mg once a day 10mg once a day 20mg2 twice a day
Esomeprazole 40mg1 once a day 20mg1 once a day 40mg1 twice a day
Lansoprazole 30mg once a day 15mg once a day 30 mg2 twice a day
Omeprazole 40mg1 once a day 20mg1 once a day 40mg1 twice a day
Pantoprazole 40mg once a day 20mg once a day 40mg2 twice a day
Rabeprazole 20mg once a day 10mg once a day 20mg2 twice a day
Esomeprazole 20mg
Lansoprazole 30mg
Omeprazole 20–40mg
Pantoprazole 40mg
Rabeprazole 20mg
PPI Full/standard doseLow dose
(on-demand dose)Double dose
PPI Full/standard doseLow dose
(on-demand dose)High/double dose
PPI Dose
1 Lower than the licensed starting dose for esomeprazole in GORD, which is 40mg, but considered to be dose-equivalent to other PPIs. When undertaking meta-analysis of dose-related effects, NICE classed esomeprazole 20mg as a full-dose equivalent to omeprazole 20mg.
2 Off-label dose for GORD.3 40mg is recommended as a double dose of esomeprazole because the 20mg dose is considered equivalent to omeprazole 20mg.
1 Change from the 2004 dose, specifically for severe oesophagitis, agreed by the GDG during the update of CG17.2 Off-label dose for GORD.
9
1.2 Prophylaxis of GI Complications due to other Drugs
Drugs Requiring use of Gastro-Protection
Certain patient groups may need gastro-protection with PPIs during treatment with the following drugs:
a. NSAIDs
Gastro-protection should be given to:
• Anyone with osteoarthritis or rheumatoid arthritis (NICE)
• Anyone 45 years of age and older with chronic low back pain (NICE)
• Patients aged 65 and over
• Past history of peptic ulcer disease (PUD) or serious GI complication
• Concomitant oral steroids or anticoagulants
• Presence of cardiovascular disease, diabetes, hypertension, renal or hepatic impairment
• Requirement for prolonged use of maximal doses of NSAIDs
Doses for NSAID Prophylaxis: Lansoprazole 15-30mg, Omeprazole 20mg
People younger than 45 years of age and at low risk of GI adverse events (e.g. no history of GI bleeding or Helicobacter pylori infection and not on aspirin, warfarin, or oral corticosteroids) may not need the concomitant use of a gastro-protective drug with an NSAID. Options for gastro-protective drugs to prescribe with standard NSAIDs also include misoprostol or a histamine2–receptor antagonist, but a PPI is the preferred choice (CKS Jan 2013).
b. Aspirin
Gastro-protect patients on low dose aspirin if also prescribed an NSAID, selective serotonin reuptake inhibitor (SSRI), a history of PUD or serious GI complication.
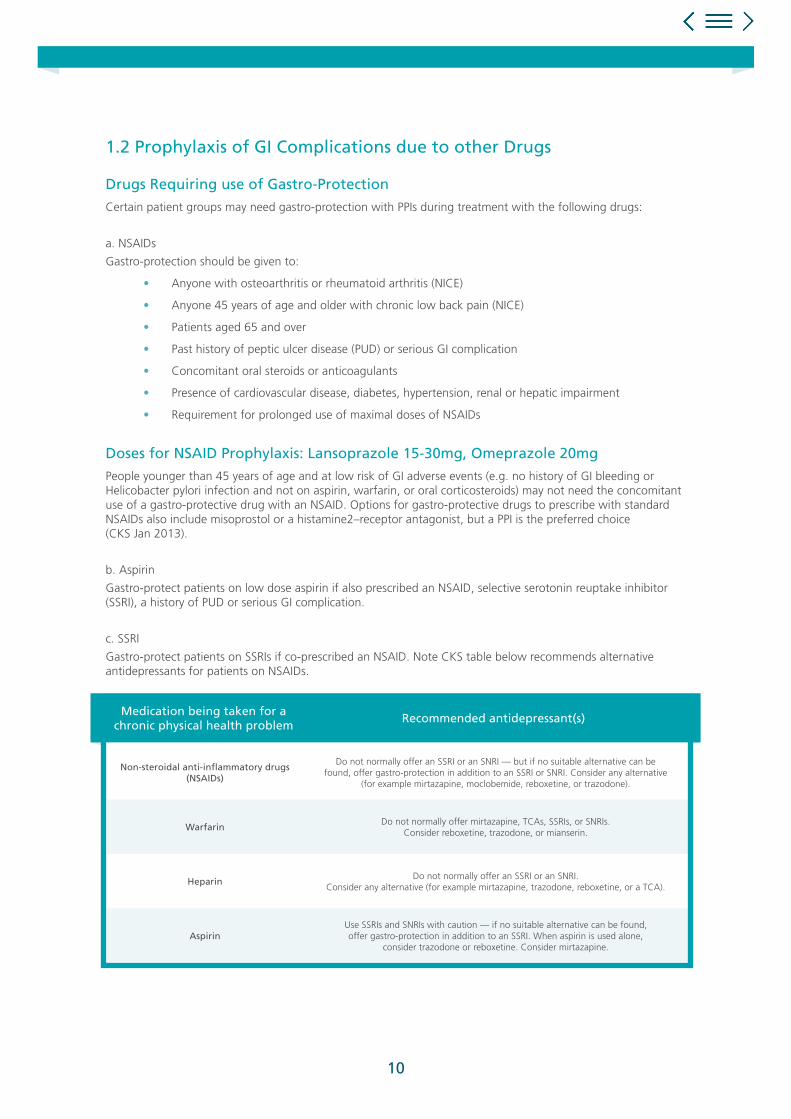
c. SSRI
Gastro-protect patients on SSRIs if co-prescribed an NSAID. Note CKS table below recommends alternative antidepressants for patients on NSAIDs.
Non-steroidal anti-inflammatory drugs (NSAIDs)
Do not normally offer an SSRI or an SNRI — but if no suitable alternative can be found, offer gastro-protection in addition to an SSRI or SNRI. Consider any alternative
(for example mirtazapine, moclobemide, reboxetine, or trazodone).
WarfarinDo not normally offer mirtazapine, TCAs, SSRIs, or SNRIs.
Consider reboxetine, trazodone, or mianserin.
HeparinDo not normally offer an SSRI or an SNRI.
Consider any alternative (for example mirtazapine, trazodone, reboxetine, or a TCA).
AspirinUse SSRIs and SNRIs with caution — if no suitable alternative can be found, offer gastro-protection in addition to an SSRI. When aspirin is used alone,
consider trazodone or reboxetine. Consider mirtazapine.
Medication being taken for a chronic physical health problem
Recommended antidepressant(s)
10

Major Drug Interactions & Cautions
PPIs undergo extensive hepatic metabolism. Recommended doses in hepatic impairment are as follows:
• In people with liver disease do not exceed 20mg daily for omeprazole, pantoprazole,and esomeprazole, and 30mg daily for lansoprazole. There are no data on the use of rabeprazole in people with severe hepatic impairment, and the manufacturer advises caution.
• Esomeprazole - 20mg in severe impairment; lansoprazole - half normal dose in moderate to severe impairment; omeprazole - 20mg in hepatic impairment; pantoprazole - max. 20mg daily in severe impairment and cirrhosis - monitor liver function (discontinue if deterioration); pantoprazole - caution in severe hepatic dysfunction.
• Occasional and unpredictable bleeding has been reported with warfarin and certain PPIs (esomeprazole, omeprazole, and lansoprazole). The interaction is not thought to occur with rabeprazole or pantoprazole. Advise INR clinic when starting or stopping PPIs with interaction potential.
• There are case reports of esomeprazole interacting with phenytoin (causing an increase in phenytoin level). No special precautions would normally seem necessary if lansoprazole or omeprazole is given with phenytoin, but prescribers should be aware of this possible interaction.
• Because of decreased intragastric acidity, the absorption of itraconazole may be reduced during PPI treatment as is that of voriconazole with esomeprazole and omeprazole.
• Esomeprazole and omeprazole can significantly reduce the efficacy of clopidogrel. Lansoprazole should be PPI of choice in patients prescribed clopidogrel.
• Omeprazole increases plasma concentration of cilostazol increasing risk of toxicity. Avoid concomitant use.
11

2.1 Exclusion criteria
The following patients are not suitable for PPI review:
• Patients under 18 (except for GP review)
• Patients on healing doses of PPIs <one month for uninvestigated dyspepsia
• Patients on maintenance dose PPIs <one month for non-ulcer dyspepsia
• Patients on healing doses of PPIs <two months for gastro-oesophageal reflux disease / peptic ulcer disease
• Patients currently on H. Pylori eradication therapy
• Patients under review at GI clinic or awaiting referral
• Patients awaiting gastroscopy or review
• Zollinger-Ellison Syndrome
• Patients in end stage GSF
• Patients with grade 3 or 4 oesophagitis
• Patients on high dose steroids with life threatening or chronic illness, e.g. patients awaiting transplant, post transplant patients
• Patients receiving immuno-suppression therapy
• Patients undergoing chemotherapy or radiotherapy
• Patients with oesophageal strictures or oesophageal dilation
• Patients with a history of oesophageal varices
• Alarm signs - refer to GP - If any of the following alarm features are present, the patient should be referred to the GP for immediate consultation
• Anaemia
• Vomiting
• Weight loss
• Dysphagia
• Epigastric mass
• Haematemesis
• Jaundice
• Progressively worsening symptoms
2 Medication Review Process
12
The following patients may be considered for step-down to the lowest maintenance dose of PPI (and change to generic, cost-effective PPI where applicable as per NICE), but should not proceed to self-management plans:
• Patients with a history of peptic ulceration associated with clo negative status.
• Patients diagnosed with Barrett’s oesophagus (20mg maintenance dose omeprazole).
• Patients who must unavoidably continue with NSAID therapy apart from those considered at high risk i.e. those with previous ulceration; those on other medication harmful to the gastric and duodenal lining; the elderly and those on long term high NSAID use. (20mg Omeprazole is defined as maintenance dose for NSAID coverage).
• Patients using aspirin or clopidogrel to prevent cardiovascular disease can be stepped-off concomitant PPI treatment, apart from those considered to be at high risk e.g. those with previous ulceration; those on other medication harmful to the gastric or duodenal lining and the elderly.
Review Process
If patient attends Long Term Condition (LTC) clinic - practice nurse to review at next clinic appointment.
If patients does not attend LTC clinic - practice pharmacist or GP to review.
1 Confirm drug indication - patient notes or by asking patient why they are taking the PPI.
2 Confirm if they are in the exclusion group or for step-down only as above.
3 Is the prescribing for treatment or prophylaxis? If for prophylaxis, is the other drug still being prescribed or still needed?
4 Check length of treatment and dosage - can healing dose be stepped down, maintenance dose stepped off? Check symptom control.
5 Discuss risk factors associated with long term use of PPIs i.e. increased risk of fractures, pneumonia and C. difficile.
6 Discuss lifestyle issues (see 1.1) and Read code for advice given.
7 Discuss rebound and rescue treatment.
8 Follow up after 2-3 months.
Refer to pharmacist if concerned about drug interactions, contra-indications or if concerned about stopping any other medications.
Patient Counselling/Lifestyle Advice
All patients will be counselled about effective non-pharmacological treatments to reduce the occurrence of heartburn.
Counselling will include advice on weight loss, head elevation in bed, avoidance of bending over, dietary advice (fatty foods), alcohol intake reduction etc.
13

2.2 Stepping Down PPI DosePatients who have been prescribed a PPI healing dose for more than four to eight weeks and are not excluded by the specified exclusion criteria in stage one of the protocol will be identified and counselled by the nurse/pharmacist. If appropriate, these patients should then be stepped down to a low dose treatment as required with an agreed limit on the number of repeat prescriptions.
To improve symptom control and the success of this dosage reduction, a suitable alginate/antacid symptomatic treatment may be recommended at a nurse/pharmacist clinic consultation, to prevent, and/or treat occasional breakthrough symptoms, due to rebound acid hypersecretion/acid breakthrough.
Patients stepped down from a PPI healing dose to a PPI maintenance dose, and who are not excluded by the step down only caution criteria, will be reviewed for step off (usually 2-3 months post step-down).
2.3 Stopping PPI & Other DrugsPatients who have been prescribed a PPI maintenance dose for more than eight weeks and are not excluded by the specified exclusion criteria in stage one of the protocol will be counselled and recommended by the nurse or pharmacist to be stepped off PPI treatment to a suitable alginate/antacid symptomatic treatment.
Consider stopping other medication that could be contributing to symptoms as follows:
a NSAIDs - See 1.2 for need for PPI. Follow NSAID discontinuation flow chart at end of this document. Give NSAID leaflet and try alternative analgesia. Review after one month. If successfully stopped NSAID, step off PPI.
b SSRIs - If patient has been taking for >2 years and not under regular review discuss possibility of withdrawal. Follow SSRI protocol for discontinuation. Once stopped discontinue PPI if appropriate. Follow SSRI discontinuation flowchart protocol.
c Aspirin/clopidogrel - No longer recommended for primary prevention patients. Stop and step off PPI if no other ongoing need.
d Nitrates and nicorandil - Was PPI started for chest pain prior to diagnosis of angina? If so try stepping off and monitor symptoms Is angina well controlled? Consider reducing dose of nitrate and/or nicorandil - refer to GP to confirm.
e Steroids - Only need PPI if also on NSAID or aspirin. If long term check prescribed bisphophonate for osteoporosis prophylaxis - if not refer to GP.
f Theophyllines - Are respiratory symptoms well controlled on maximum tolerated doses of inhaled meds? Try reducing theophylline dose and review symptom control.
Record step-down, step-off or any other amendments to medication. Where all medication has been reviewed, code as ‘medication review done’ and move diary date of next review on.
Review Period
Step-down patients - Review 2 - 3 months post step-down. If symptoms controlled, consider step-off where not covered in step-down only criteria.
Step-off patients - Follow up not necessary but encourage patients to report any further symptoms or issues.
14
3.1 Exclusion CriteriaExclusion Criteria as Follows:
• Patients under 18 (except for GP review)
• Patients on healing doses of PPIs <one month for uninvestigated dyspepsia
• Patients on maintenance dose PPIs <one month for Non-Ulcer dyspepsia
• Patients on healing doses of PPIs <two months for Gastro-oesophageal reflux disease / Peptic Ulcer disease
• Patients currently on H. pylori eradication therapy
• Patients under review at GI clinic or awaiting referral
• Patients awaiting gastroscopy or review
• Zollinger-Ellison Syndrome
• Patients in end stage GSF
• Patients with grade 3 or 4 oesophagitis
• Patients on high dose steroids with life threatening or chronic illness, e.g. patients awaiting transplant, post transplant patients
• Patients receiving immuno-suppression therapy
• Patients undergoing chemotherapy or radiotherapy
• Patients with oesophageal strictures or oesophageal dilation
• Patients with a history of oesophageal varices
• Alarm signs - refer to GP - If any of the following alarm features are present, the patient should be referred to the GP for immediate consultation.
• Anaemia
• Vomiting
• Weight loss
• Dysphagia
• Epigastric mass
• Haematemesis
• Jaundice
• Progressively worsening symptoms
3 PPI Polypharmacy Medication Review Process
15
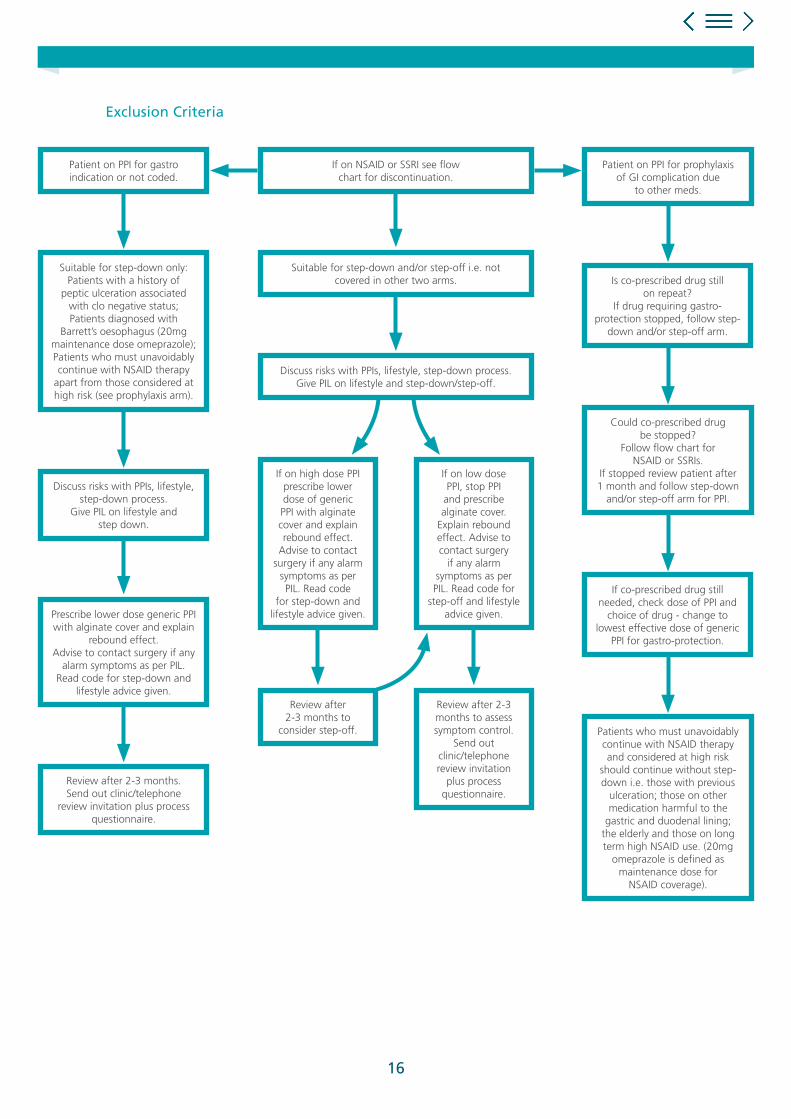
Patient on PPI for gastroindication or not coded.
Discuss risks with PPIs, lifestyle,step-down process.
Give PIL on lifestyle and step down.
Review after 2-3 months.Send out clinic/telephone
review invitation plus processquestionnaire.
Suitable for step-down only:Patients with a history of
peptic ulceration associatedwith clo negative status;Patients diagnosed with
Barrett’s oesophagus (20mg maintenance dose omeprazole);Patients who must unavoidablycontinue with NSAID therapy
apart from those considered athigh risk (see prophylaxis arm).
Prescribe lower dose generic PPIwith alginate cover and explain
rebound effect.Advise to contact surgery if any
alarm symptoms as per PIL. Read code for step-down and
lifestyle advice given.
Patient on PPI for prophylaxis of GI complication due
to other meds.
If on high dose PPIprescribe lowerdose of genericPPI with alginatecover and explainrebound effect.
Advise to contactsurgery if any alarm
symptoms as perPIL. Read code
for step-down andlifestyle advice given.
Review after2-3 months to
consider step-off.
Review after 2-3months to assesssymptom control.
Send out clinic/telephonereview invitation
plus processquestionnaire.
If on low dosePPI, stop PPI
and prescribe alginate cover.
Explain reboundeffect. Advise tocontact surgery
if any alarmsymptoms as perPIL. Read code for
step-off and lifestyleadvice given.
Is co-prescribed drug still on repeat?
If drug requiring gastro-protection stopped, follow step-
down and/or step-off arm.
Could co-prescribed drugbe stopped?
Follow flow chart for NSAID or SSRIs.
If stopped review patient after1 month and follow step-down
and/or step-off arm for PPI.
If co-prescribed drug still needed, check dose of PPI and
choice of drug - change to lowest effective dose of generic
PPI for gastro-protection.
Patients who must unavoidablycontinue with NSAID therapyand considered at high risk
should continue without step-down i.e. those with previous
ulceration; those on othermedication harmful to the
gastric and duodenal lining; the elderly and those on long term high NSAID use. (20mg
omeprazole is defined as maintenance dose for
NSAID coverage).
If on NSAID or SSRI see flowchart for discontinuation.
Suitable for step-down and/or step-off i.e. notcovered in other two arms.
Discuss risks with PPIs, lifestyle, step-down process.Give PIL on lifestyle and step-down/step-off.
Exclusion Criteria
16
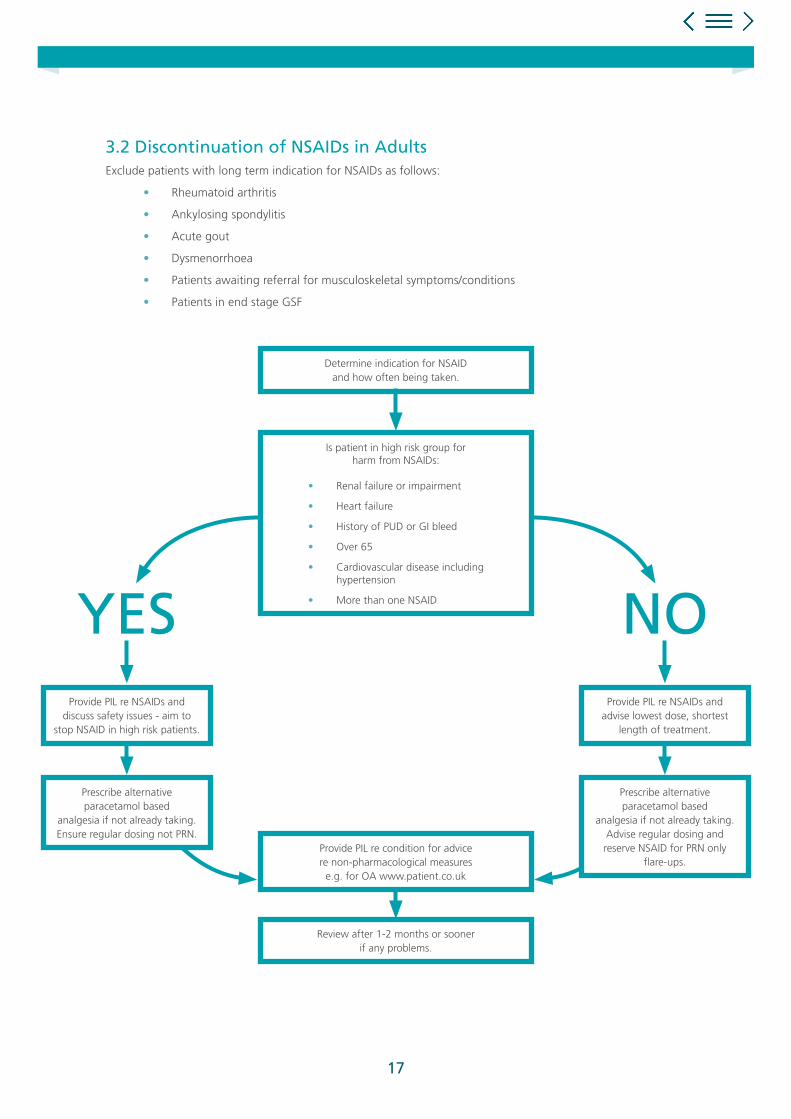
3.2 Discontinuation of NSAIDs in AdultsExclude patients with long term indication for NSAIDs as follows:
• Rheumatoid arthritis
• Ankylosing spondylitis
• Acute gout
• Dysmenorrhoea
• Patients awaiting referral for musculoskeletal symptoms/conditions
• Patients in end stage GSF
Determine indication for NSAIDand how often being taken.
Provide PIL re condition for advicere non-pharmacological measures
e.g. for OA www.patient.co.uk
Review after 1-2 months or soonerif any problems.
Is patient in high risk group forharm from NSAIDs:
• Renal failure or impairment
• Heart failure
• History of PUD or GI bleed
• Over 65
• Cardiovascular disease including hypertension
• More than one NSAID NOYESProvide PIL re NSAIDs and
discuss safety issues - aim to stop NSAID in high risk patients.
Prescribe alternative paracetamol based
analgesia if not already taking.Ensure regular dosing not PRN.
Provide PIL re NSAIDs and advise lowest dose, shortest
length of treatment.
Prescribe alternative paracetamol based
analgesia if not already taking.Advise regular dosing and reserve NSAID for PRN only
flare-ups.
17

• Dyspepsia: Managing dyspepsia in adults in primary care. NICE CG184 Sept 2014 www.nice.org.uk Date last accessed 02/4/2015
• NICE Key Therapeutic Topics- Medicines management options for local implementation: Non-steroidal anti-inflammatory drugs (NSAIDs) http://www.nice.org.uk/mpc/keytherapeutictopics/KTT13.jsp Date last accessed 02/4/2015
• MeReC Bulletin Vol 22 No3: Implementing key therapeutic topics:1 NSAIDs, antibiotics and inhaled corticosteroids in asthma. Jan 2012 http://www.npc.nhs.uk/merec/therap/other/merec_bulletin_vol22_no3.php Date last accessed 02/4/2015
• Clinical Knowledge Summaries (CKS) Dyspepsia- Unidentified cause Proton Pump Inhibitors http://cks.nice.org.uk/dyspepsia-unidentified-cause#!prescribinginfosub:4 Date last accessed 02/4/2015
• British National Formulary http://www.evidence.nhs.uk/formulary/bnf/current/search?q=PPIs Date last accessed 02/4/2015
References
This material is not approved for use for projects with RB (ie. MEGS/Joint working)
ARM and the Medicines Optimisation Academy are non-promotional education programmes designed by RB UK to improve patient care and support healthcare professional.
18

Protocol for Prescribing NSAIDs:Initiation, Review & Discontinuation
This material was authored by Diane McGinn, Medicines Management Consultant, Preston, Lancashire, UK
Date of preparation: April 2015UK/G-NHS/1114/0058q
The polypharmacy medicines review project, The Medicines Optimisation Academy and production of the supporting materials, including this leaflet, have been wholly supported with funding from RB Healthcare UK Ltd.
19

1 Choice of NSAID
1.1 Relative Efficacy and Side-Effects• Lifestyle Interventions
• Devices
• Walking Aids
• Alternatives to NSAIDs
• Cautions and Contra-Indications
1.2 Specific Safety Concerns• Cardiovascular events
• Gastro-intestinal toxicity and gastro-protection
• Major Drug Interactions
2 Discontinuation of NSAIDs in Adults
Contents
20
Non-steroidal anti-inflammatory drug (NSAIDs) are prescribed for their analgesic and anti-inflammatory effects.
All NSAIDs are associated with gastrointestinal, cardiovascular and renal side effects. If NSAIDs are required, they should be prescribed at the lowest effective dose for the shortest period of time necessary to control symptoms.
Wherever possible, and particularly for patients most at risk of side-effects, if NSAIDs are being considered for pain relief, alternative analgesia should be tried first line especially in conditions with minimal inflammation e.g. osteoarthritis.
Paracetamol (and/or topical NSAIDs) is recommended ahead of oral NSAIDs in the NICE osteoarthritis guideline.
1.1 Relative Efficacy & Side-EffectsDifferences in anti-inflammatory activity between NSAIDs are small but patients vary considerably in their response and ability to tolerate different drugs. 60% of patients will respond to any one NSAID - those who don’t respond to one may well respond to another.
Pain relief starts soon after first dose and full analgesic effect should normally be attained after one week.
Anti-inflammatory effect, if able to be assessed, may not be achieved for up to three weeks.
If effects are not seen after this time then another NSAID should be tried.
1 Choice of NSAID
21

Ibuprofen Weak anti-inflammatory Fewer side-effects than other NSAIDs
Naproxen Good anti-inflammatory Greater than ibuprofen but still low
Fenbufen Less GI bleeds, high risk of rash
Fenoprofen As effective as naproxen Slightly more GI side-effects than ibuprofen
Flurbiprofen Slightly more effective than naproxen Slightly more GI side-effects than ibuprofen
Ketoprofen Similar to ibuprofen Greater than ibuprofen
Tiaprofenic acid As effective as naproxenMore than ibuprofen including severe
cystitis
Diclofenac & aceclofenac Similar to naproxen Similar to naproxen
Etodolac Similar to naproxen
Indometacin Equal or better than naproxenHigh incidence of side-effects e.g.
headache, dizziness and GI disturbances
Mefenamic acid Minor anti-inflammatory propertiesDiarrhoea & haemolytic anaemia may
require stopping treatment
MeloxicamLicensed for short term pain relief in OA and long
term for RA & Ankylosing spondylitis
Nabumetone Comparable to naproxen
Piroxicam As effective as naproxen - long durationMore GI side-effects than most other
NSAIDs & frequent serious skin reactions
Sulindac Similar to naproxen
Tenoxicam Similar to naproxen. Long duration of action Similar to naproxen
Celecoxib and Etoricoxib As effective as naproxenGI events lower than non-selective (unless
on aspirin) but higher CV risk
Drug Frequently Prescribed NSAIDs
Relative Anti-Inflammatory Efficacy
Relative Side-Effects Compared
Lifestyle Interventions
For patients with osteoarthritis general lifestyle measures may help reduce the need for regular NSAIDs:
• Exercise - Regular exercise helps to strengthen the muscles around affected joints and maintain a good range of joint movement. Swimming is ideal for most joints, but any exercise is better than none. Many people can manage a regular walk.
• Weight Control - If overweight, even a modest weight loss can make quite a difference.
22

Devices
Some trials have shown that the following may help to ease symptoms from OA of the knee in some cases:
• Wearing a knee brace.
• Using shoe insoles.
• The use of tape to pull the kneecap inwards.
These measures slightly alter the distribution of weight and pressure on the knee joint. A podiatrist or physiotherapist can advise on use. Braces or supports may also be helpful for other joints affected by OA e.g. thumb.
Walking Aids
Use of a walking stick may help with OA of the hip or knee. It should be held in the hand on the opposite side of the body to the affected joint.
Alternatives to NSAIDs
For analgesia in conditions where an anti-inflammatory effect is not generally required the WHO pain ladder should be followed.
First line treatment should be paracetamol taken regularly i.e. 1g QDS. Patients should be reassured that this is safe to take on a regular basis with NSAIDs being reserved for PRN use rather than the other way round.
For patients at high risk of NSAID associated side-effects, addition of codeine to paracetamol is preferable to addition of an NSAID. Note that adjuvants such as TCAs for neuropathic pain can be added at any time.
e.g. morphine, oxycodone fentanyl
e.g. codeine
e.g. aspirin, paracetamol or a NSAID
23
Cautions & Contra-Indications
NSAIDs are contra-indicated in the following:
• Severe heart failure (although not contra-indicated it would be advisable to avoid use in any degree of heart failure due to risk of fluid retention).
• Non-selective (i.e. non-COX-II) NSAIDs C/I in previous or active peptic ulceration. If required in rheumatic disease in these patients COX-II inhibitors should be used with gastro-protection (see below).
• Celecoxib and etoricoxib are C/I in: - IHD - Cerebrovascular disease - Peripheral arterial disease - Moderate or severe heart failure
NSAIDs should be used with caution in:
• The elderly
• Allergic disorder including asthma
• Cardiac impairment due to risk of renal impairment
• Celecoxib and etoricoxib should be used with caution in: - Cardiac failure - Left ventricular dysfunction - Hypertension - Oedema for any reason - Patients with risk factor for heart disease
• Hepatic impairment - increased risk of GI bleeds and fluid retention. Avoid in severe liver disease.
• Renal impairment - avoid if possible
1.2 Specific Safety Concerns Cardiovascular Events
How can the CV risks of NSAIDs be reduced?
• If an NSAID is required, low-dose ibuprofen (1200mg/day or less) or naproxen 1000mg/day or less would appear more appropriate than other NSAIDs for patients in whom CV risk is a significant consideration in decision making.
• Coxibs (celecoxib and etoricoxib) are associated with an increased thrombotic risk.
• Diclofenac 150mg/day has a similar excess thrombotic risk to etoricoxib and possibly other coxibs.
• A meta-analysis of observational studies has confirmed an increased risk of CV events with diclofenac (even at comparatively low doses of 100mg/day or less).
• A high CV risk was also seen with etoricoxib and etodolac.
• With regard to ibuprofen, the meta-analysis underlined the need to use lower doses (1200mg/day or less) to avoid increasing the risk of CV events.
• The risk of CV events with naproxen was low or absent at higher as well as lower doses.
24
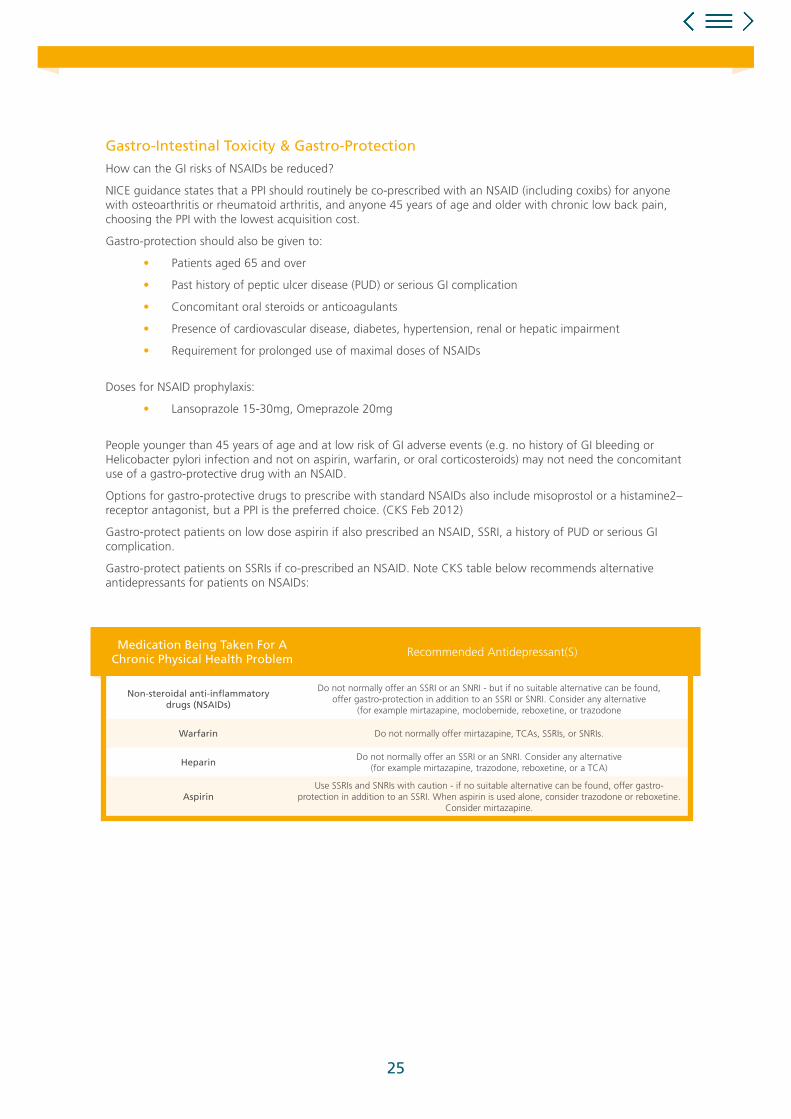
Gastro-Intestinal Toxicity & Gastro-Protection
How can the GI risks of NSAIDs be reduced?
NICE guidance states that a PPI should routinely be co-prescribed with an NSAID (including coxibs) for anyone with osteoarthritis or rheumatoid arthritis, and anyone 45 years of age and older with chronic low back pain, choosing the PPI with the lowest acquisition cost.
Gastro-protection should also be given to:
• Patients aged 65 and over
• Past history of peptic ulcer disease (PUD) or serious GI complication
• Concomitant oral steroids or anticoagulants
• Presence of cardiovascular disease, diabetes, hypertension, renal or hepatic impairment
• Requirement for prolonged use of maximal doses of NSAIDs
Doses for NSAID prophylaxis:
• Lansoprazole 15-30mg, Omeprazole 20mg
People younger than 45 years of age and at low risk of GI adverse events (e.g. no history of GI bleeding or Helicobacter pylori infection and not on aspirin, warfarin, or oral corticosteroids) may not need the concomitant use of a gastro-protective drug with an NSAID.
Options for gastro-protective drugs to prescribe with standard NSAIDs also include misoprostol or a histamine2–receptor antagonist, but a PPI is the preferred choice. (CKS Feb 2012)
Gastro-protect patients on low dose aspirin if also prescribed an NSAID, SSRI, a history of PUD or serious GI complication.
Gastro-protect patients on SSRIs if co-prescribed an NSAID. Note CKS table below recommends alternative antidepressants for patients on NSAIDs:
Non-steroidal anti-inflammatory drugs (NSAIDs)
Do not normally offer an SSRI or an SNRI - but if no suitable alternative can be found, offer gastro-protection in addition to an SSRI or SNRI. Consider any alternative
(for example mirtazapine, moclobemide, reboxetine, or trazodone
Warfarin Do not normally offer mirtazapine, TCAs, SSRIs, or SNRIs.
HeparinDo not normally offer an SSRI or an SNRI. Consider any alternative
(for example mirtazapine, trazodone, reboxetine, or a TCA)
AspirinUse SSRIs and SNRIs with caution - if no suitable alternative can be found, offer gastro-
protection in addition to an SSRI. When aspirin is used alone, consider trazodone or reboxetine. Consider mirtazapine.
Medication Being Taken For A Chronic Physical Health Problem
Recommended Antidepressant(S)
25

Major Drug Interactions - Refer To BNF For Full List
Wherever possible, combinations of drugs with additive side-effects should be avoided. Consider reviewing patients on NSAIDs and drugs which may increase the risk of bleeding, cardiovascular events and renal toxicity.
• Antiplatelets - increased risk of bleeding with aspirin, clopidogrel and prasugrel
• Quinolones - possible increased risk of convulsions when given with NSAIDs
• Anticoagulants - increased bleeding risk. Advise patients against purchasing oral and topical NSAIDs OTC.
• SSRIs and venlafaxine - increased bleeding risk. Gastro-protection may be advisable
• Sulphonylureas - NSAIDs possibly enhance effects - risk of hypos
• Phenytoin - NSAIDs possibly enhance effects
• Ciclosporin - increased risk of nephrotoxicity
• Methotrexate - increased risk of toxicity from methotrexate due to NSAIDs reducing excretion. Combination may be required in inflammatory disease but advise patients against self-medicating with OTC preparations
• Diuretics - increased risk of renal toxicity
• Lithium - NSAIDs reduce excretion - increased risk of toxicity. Avoid use of NSAIDs where possible
• Pentoxifylline - possible increased bleeding risk
• Tacrolimus - possible increased risk of toxicity
26

Exclude Patients With Long Term Indication for NSAIDs as Follows:
• Rheumatoid arthritis
• Ankylosing spondylitis
• Acute gout
• Dysmenorrhoea
• Patients awaiting referral for musculoskeletal symptoms/conditions
• Patients in end stage GSF
2 Discontinuation of NSAIDs in Adults
Determine indication for NSAIDand how often being taken.
Provide PIL re condition for advicere non-pharmacological measures
e.g. for OA www.patient.co.uk
Review after 1-2 months or soonerif any problems.
Is patient in high risk group forharm from NSAIDs:
• Renal failure or impairment
• Heart failure
• History of PUD or GI bleed
• Over 65
• Cardiovascular disease including hypertension
• More than one NSAID NOYESProvide PIL re NSAIDs and
discuss safety issues - aim to stop NSAID in high risk patients.
Prescribe alternative paracetamol based
analgesia if not already taking.Ensure regular dosing not PRN.
Provide PIL re NSAIDs and advise lowest dose, shortest
length of treatment.
Prescribe alternative paracetamol based
analgesia if not already taking.Advise regular dosing and reserve NSAID for PRN only
flare-ups.
27
1 British National Formulary http://www.evidence.nhs.uk/formulary/bnf/current/a1-interactions/list-of-drug-interactions/analgesics/nsaids Date last accessed 27/3/2015
2 NICE Key Therapeutic Topics- Medicines management options for local implementation: Non-steroidal anti-inflammatory drugs (NSAIDs) http://www.nice.org.uk/mpc/keytherapeutictopics/KTT13.jsp Date last accessed 27/3/2015
3 MeReC Bulletin Vol 22 No3: Implementing key therapeutic topics:1 NSAIDs, antibiotics and inhaled corticosteroids in asthma. Jan 2012 http://www.npc.nhs.uk/merec/therap/other/merec_bulletin_vol22_no3.php Date last accessed 27/3/2015
4 Clinical Knowledge Summaries (CKS) NSAIDs- Prescribing issues http://cks.nice.org.uk/nsaids-prescribing-issues#!scenarioclarification Date last accessed 27/3/2015
5 Osteoarthritis. Patient.co.uk http://www.patient.co.uk/health/Osteoarthritis.htm Date last accessed 27/3/2015
6 Dyspepsia: Managing dyspepsia in adults in primary care. NICE CG17 Aug 2004 www.nice.org.uk Date last accessed 27/3/2015
References
This material is not approved for use for projects with RB (ie. MEGS/Joint working)
ARM and the Medicines Optimisation Academy are non-promotional education programmes designed by RB UK to improve patient care and support healthcare professional.
28
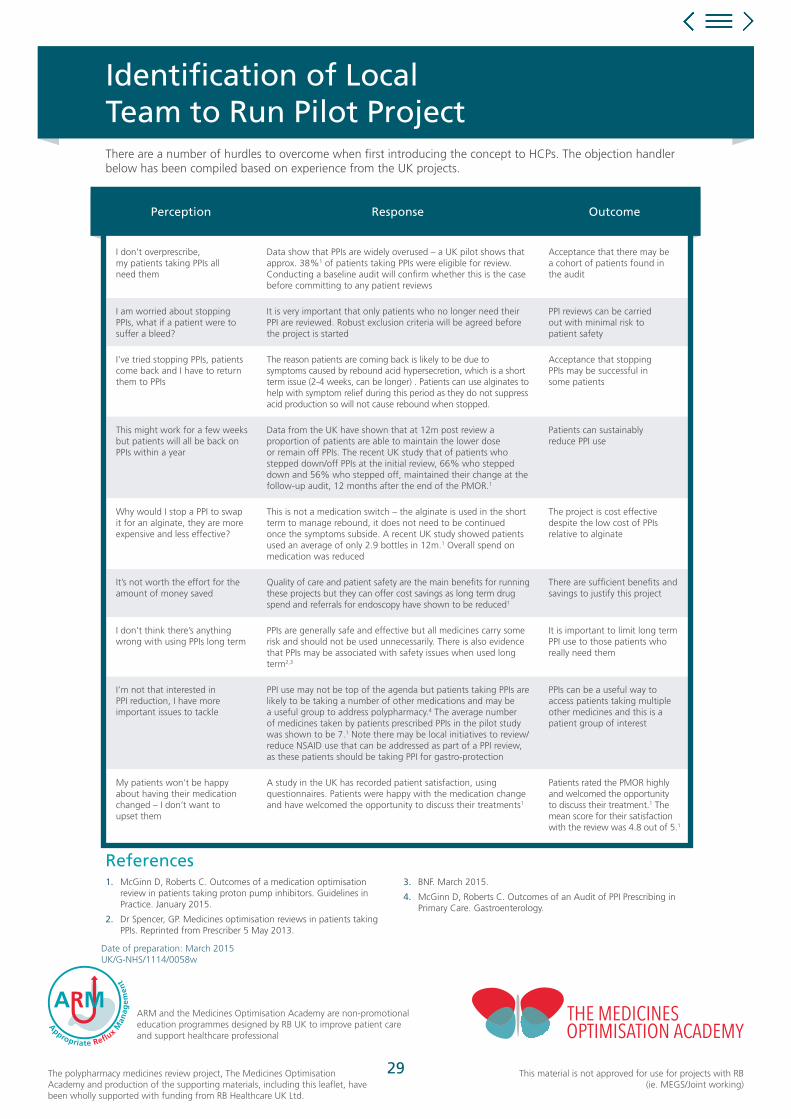
Identification of Local Team to Run Pilot Project
I don’t overprescribe, my patients taking PPIs all need them
Data show that PPIs are widely overused – a UK pilot shows that approx. 38%1 of patients taking PPIs were eligible for review. Conducting a baseline audit will confirm whether this is the case before committing to any patient reviews
Acceptance that there may be a cohort of patients found in the audit
I am worried about stopping PPIs, what if a patient were to suffer a bleed?
It is very important that only patients who no longer need their PPI are reviewed. Robust exclusion criteria will be agreed before the project is started
PPI reviews can be carried out with minimal risk to patient safety
I’ve tried stopping PPIs, patients come back and I have to return them to PPIs
The reason patients are coming back is likely to be due to symptoms caused by rebound acid hypersecretion, which is a short term issue (2-4 weeks, can be longer) . Patients can use alginates to help with symptom relief during this period as they do not suppress acid production so will not cause rebound when stopped.
Acceptance that stopping PPIs may be successful in some patients
This might work for a few weeks but patients will all be back on PPIs within a year
Data from the UK have shown that at 12m post review a proportion of patients are able to maintain the lower dose or remain off PPIs. The recent UK study that of patients who stepped down/off PPIs at the initial review, 66% who stepped down and 56% who stepped off, maintained their change at the follow-up audit, 12 months after the end of the PMOR.1
Patients can sustainably reduce PPI use
Why would I stop a PPI to swap it for an alginate, they are more expensive and less effective?
This is not a medication switch – the alginate is used in the short term to manage rebound, it does not need to be continued once the symptoms subside. A recent UK study showed patients used an average of only 2.9 bottles in 12m.1 Overall spend on medication was reduced
The project is cost effective despite the low cost of PPIs relative to alginate
It’s not worth the effort for the amount of money saved
Quality of care and patient safety are the main benefits for running these projects but they can offer cost savings as long term drug spend and referrals for endoscopy have shown to be reduced1
There are sufficient benefits and savings to justify this project
I don’t think there’s anything wrong with using PPIs long term
PPIs are generally safe and effective but all medicines carry some risk and should not be used unnecessarily. There is also evidence that PPIs may be associated with safety issues when used long term2,3
It is important to limit long term PPI use to those patients who really need them
I’m not that interested in PPI reduction, I have more important issues to tackle
PPI use may not be top of the agenda but patients taking PPIs are likely to be taking a number of other medications and may be a useful group to address polypharmacy.4 The average number of medicines taken by patients prescribed PPIs in the pilot study was shown to be 7.1 Note there may be local initiatives to review/reduce NSAID use that can be addressed as part of a PPI review, as these patients should be taking PPI for gastro-protection
PPIs can be a useful way to access patients taking multiple other medicines and this is a patient group of interest
My patients won’t be happy about having their medication changed – I don’t want to upset them
A study in the UK has recorded patient satisfaction, using questionnaires. Patients were happy with the medication change and have welcomed the opportunity to discuss their treatments1
Patients rated the PMOR highly and welcomed the opportunity to discuss their treatment.1 The mean score for their satisfaction with the review was 4.8 out of 5.1
Perception Response Outcome
References1. McGinn D, Roberts C. Outcomes of a medication optimisation
review in patients taking proton pump inhibitors. Guidelines in Practice. January 2015.
2. Dr Spencer, GP. Medicines optimisation reviews in patients taking PPIs. Reprinted from Prescriber 5 May 2013.
3. BNF. March 2015.
4. McGinn D, Roberts C. Outcomes of an Audit of PPI Prescribing in Primary Care. Gastroenterology.
There are a number of hurdles to overcome when first introducing the concept to HCPs. The objection handler below has been compiled based on experience from the UK projects.
Date of preparation: March 2015 UK/G-NHS/1114/0058w
ARM and the Medicines Optimisation Academy are non-promotional education programmes designed by RB UK to improve patient care and support healthcare professional
The polypharmacy medicines review project, The Medicines Optimisation Academy and production of the supporting materials, including this leaflet, have been wholly supported with funding from RB Healthcare UK Ltd.
This material is not approved for use for projects with RB (ie. MEGS/Joint working)
29
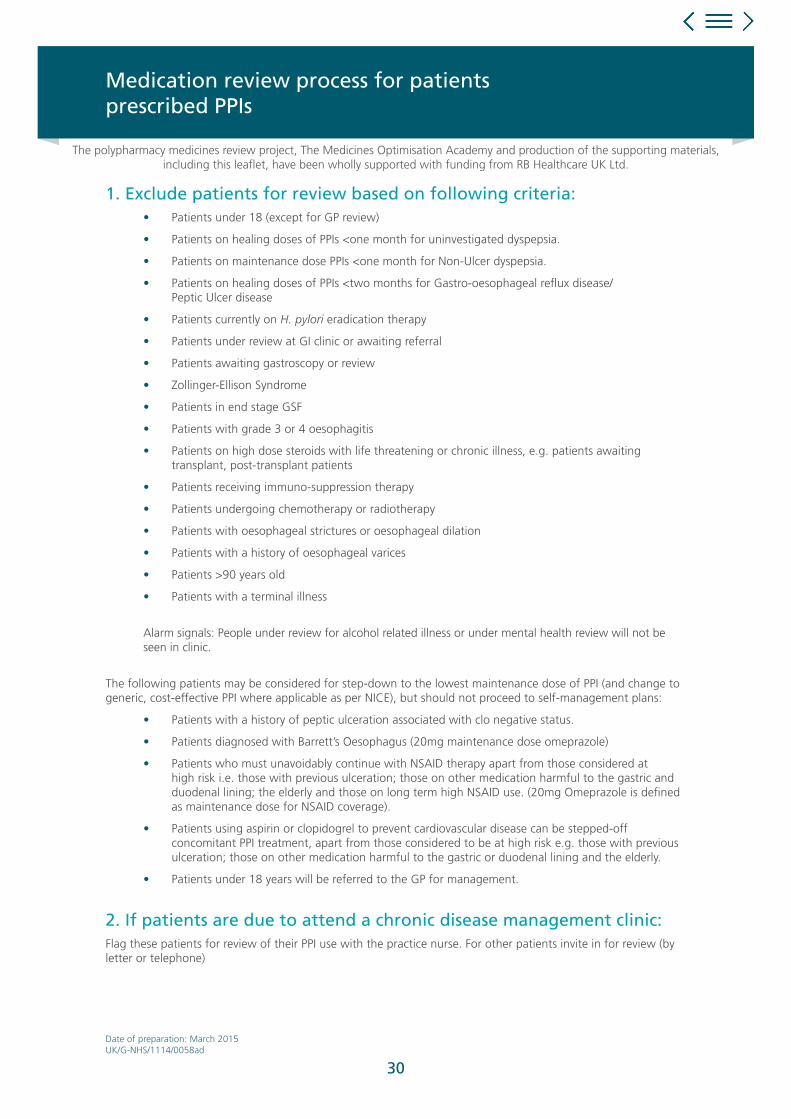
1. Exclude patients for review based on following criteria:• Patients under 18 (except for GP review)
• Patients on healing doses of PPIs <one month for uninvestigated dyspepsia.
• Patients on maintenance dose PPIs <one month for Non-Ulcer dyspepsia.
• Patients on healing doses of PPIs <two months for Gastro-oesophageal reflux disease/ Peptic Ulcer disease
• Patients currently on H. pylori eradication therapy
• Patients under review at GI clinic or awaiting referral
• Patients awaiting gastroscopy or review
• Zollinger-Ellison Syndrome
• Patients in end stage GSF
• Patients with grade 3 or 4 oesophagitis
• Patients on high dose steroids with life threatening or chronic illness, e.g. patients awaiting transplant, post-transplant patients
• Patients receiving immuno-suppression therapy
• Patients undergoing chemotherapy or radiotherapy
• Patients with oesophageal strictures or oesophageal dilation
• Patients with a history of oesophageal varices
• Patients >90 years old
• Patients with a terminal illness
Alarm signals: People under review for alcohol related illness or under mental health review will not be
seen in clinic.
The following patients may be considered for step-down to the lowest maintenance dose of PPI (and change to generic, cost-effective PPI where applicable as per NICE), but should not proceed to self-management plans:
• Patients with a history of peptic ulceration associated with clo negative status.
• Patients diagnosed with Barrett’s Oesophagus (20mg maintenance dose omeprazole)
• Patients who must unavoidably continue with NSAID therapy apart from those considered at high risk i.e. those with previous ulceration; those on other medication harmful to the gastric and duodenal lining; the elderly and those on long term high NSAID use. (20mg Omeprazole is defined as maintenance dose for NSAID coverage).
• Patients using aspirin or clopidogrel to prevent cardiovascular disease can be stepped-off concomitant PPI treatment, apart from those considered to be at high risk e.g. those with previous ulceration; those on other medication harmful to the gastric or duodenal lining and the elderly.
• Patients under 18 years will be referred to the GP for management.
2. If patients are due to attend a chronic disease management clinic:Flag these patients for review of their PPI use with the practice nurse. For other patients invite in for review (by letter or telephone)
The polypharmacy medicines review project, The Medicines Optimisation Academy and production of the supporting materials, including this leaflet, have been wholly supported with funding from RB Healthcare UK Ltd.
Medication review process for patientsprescribed PPIs
Date of preparation: March 2015 UK/G-NHS/1114/0058ad
30

3. At nurse review:Flag these patients for review of their PPI use with the practice nurse. For other patients invite in for review (by letter or telephone)
a Confirm drug indication - patient notes or by asking patient why they are taking the PPI
b Confirm if they are in the exclusion group or for step-down only as above. If any of the following alarm features are present, the patient should be referred to the GP for immediate consultation:
• Anaemia
• Vomiting
• Weight loss
• Dysphagia
• Epigastric mass
• Haematemesis
• Jaundice
• Progressively worsening symptoms
c Is the prescribing for treatment or prophylaxis? If for prophylaxis, is the other drug still being prescribed or still needed?
d Check length of treatment and dosage - can healing dose be stepped-down, maintenance dose stepped-off? Check symptom control.
e Discuss risk factors associated with long term use of PPIs i.e. increased risk of fractures, pneumonia and C. difficile.
f Discuss lifestyle issues and Read code for advice given. Provide patient information leaflets on PPIs and lifestyle advice.
g All patients will be counselled about effective non-pharmacological treatments for heartburn. Counselling will include advice on weight loss, head elevation in bed, avoidance of bending over, dietary advice (fatty foods), alcohol intake reduction etc.
h Discuss rebound and rescue treatment. If stepping-down/off arrange for prescription to be issued for alginate cover and lower dose PPI if applicable.
i Follow up after 2-3 months
Refer to pharmacist/GP if concerned about drug interactions, contra-indications or if concerned about stopping any other medications.
4. At pharmacist review:As above but conduct review of ALL medication prescribed in line with national and local guidance. Consider stopping medication no longer of benefit, or where risk outweighs benefit, after discussion with patient e.g. NSAIDs, aspirin for primary prevention of CHD.
Use patient information leaflets to discuss alternatives to NSAIDs and stepping-down/off SSRIs.
Rationalise any dosages where more cost-effective formulations exist.
Assess adherence to treatment for all medication and refer to GP where patient is experiencing new symptoms, poor control or side-effects from medication.
Date of preparation: March 2015 UK/G-NHS/1114/0058ad
31

5. Stepping-down PPI dose:Patients who have been prescribed a PPI healing dose for more than four to eight weeks and are not excluded by the specified exclusion criteria in stage one of the protocol, will be identified and counselled by the nurse/pharmacist. If appropriate these patients should then be stepped-down to a low dose treatment as required with an agreed limit on the number of repeat prescriptions.
To improve symptom control and the success of this dosage reduction, a suitable alginate/antacid symptomatic treatment may be recommended to prevent and/or treat occasional breakthrough symptoms due to rebound acid hypersecretion/acid breakthrough.
Patients stepped-down from a PPI healing dose to a PPI maintenance dose, and who are not excluded by the step-down only caution criteria, will be reviewed for step-off (usually 2-3 months post step-down).
6. Stopping PPI and other drugs:Patients who have been prescribed a PPI maintenance dose for more than eight weeks and are not excluded by the specified exclusion criteria in stage one of the protocol, will be counselled and recommended by the nurse or pharmacist to be stepped-off PPI treatment to a suitable alginate / antacid symptomatic treatment.
7. Consider stopping other medication which could be contributing to
symptoms as followsPatients who have been prescribed a PPI maintenance dose for more than eight weeks and are not excluded by the specified exclusion criteria in stage one of the protocol will be counselled and recommended by the nurse or pharmacist to be stepped-off PPI treatment to a suitable alginate/antacid symptomatic treatment.
a NSAIDs - Follow NSAID discontinuation flow chart. Give NSAID leaflet and try alternative analgesia. Review after one month. If successfully stopped NSAID, step-off PPI.
b SSRIs - If patient has been taking for >2 years and not under regular review discuss possibility of withdrawal. Follow SSRI protocol for discontinuation. Once stopped, discontinue PPI if appropriate.
c Aspirin/clopidogrel - No longer recommended for primary prevention patients. Stop and step-off PPI if no other on-going need.
d Nitrates and nicorandil - Was PPI started for chest pain prior to diagnosis of angina? If so try stepping-off and monitor symptoms. Is angina well controlled? Consider reducing dose of nitrate and/or nicorandil - refer to GP to confirm.
e Steroids - only need PPI if also on NSAID or aspirin. If long-term check prescribed bisphosphonate for osteoporosis prophylaxis - if not refer to GP.
f Theophyllines - Are respiratory symptoms well controlled on maximal tolerated doses of inhaled meds? Try reducing theophylline dose and review symptom control.
Record step-down or step-off or any other amendments to medication. Where all medication has been reviewed, code as ‘medication review done’ and move diary date of next review on.
The information above is advice only. When reviewing patients’ medicines always consider the current clinical guidance for the applicable therapy area.
Review Period• Step-down patients - Review 2 - 3 months post step-down. If symptoms controlled consider step
off where not covered in step down only criteria.
• Step-off patients - Follow up not necessary but encourage patients to report any further symptoms or issues.
Date of preparation: March 2015 UK/G-NHS/1114/0058ad
This material is not approved for use for projects with RB (ie. MEGS/Joint working)
ARM and the Medicines Optimisation Academy are non-promotional education programmes designed by RB UK to improve patient care and support healthcare professional.
32

Dear
Dyspepsia Clinic AppointmentWe are continually working to improve the healthcare offered to our patients, and to ensure that you receive the most appropriate medication for your condition. We are currently reviewing patients receiving repeat prescriptions for their acid-related disorders (heartburn, hiatus hernia etc.) and patients on medication after ulcer healing. Accordingly, I would like to invite you to attend the dyspepsia clinic where the nurse will review your condition and ensure that you continue to receive the most appropriate treatment.
This is a temporary clinic being run by the nurse specialist to ensure we are helping to achieve the curr nt guidelines and your records are kept up to date. Your individual appointment is for 15 mins during which you will be asked to help complete a simple questionnaire. It is also an ideal opportunity to ask any questions you may have.
We would be grateful if you could attend the surgery for your dyspepsia clinic appointment:
at:
on:
PLEASE INFORM THE SURGERY IF YOU ARE UNABLE TO ATTEND AS ANOTHER APPOINTMENT CAN BE ARRANGED.
It is to your benefit and therefore important that you attend. Thank you for your co-operation,
Yours faithfully,
Nurse Advisor (RGN)
On behalf of Medical Practice
Dyspepsia Clinic: Patient Invite
The polypharmacy medicines review project, The Medicines Optimisation Academy and production of the supporting materials, including this leaflet, have been wholly supported with funding from RB Healthcare UK Ltd.
Date of preparation: March 2015 UK/G-NHS/1114/0058t
This material is not approved for use for projects with RB (ie. MEGS/Joint working)
33

Dear Colleague,
A polypharmacy medicine review is being conducted in patients registered at the following practices: Mountview, Bellevue and Broadway. This leaflet will explain the purpose and scope of the project so that you are kept informed and prepared for questions your patients might have about their medication, as their prescription may change following clinical review.
BackgroundAs part of our work to achieve medicines optimisation we have conducted an audit of the prescribing of proton proton pump inhibitors (PPI) and found this patient group to be well suited to polypharmacy medicines review. On average, a patient taking a PPI was found to be taking six other medications.1
Polypharmacy Review: Project ScopeConsequently, we plan to review the prescribing of PPIs, NSAIDs and SSRIs, to reduce any inappropriate or obsolete use. Where possible this will take place at routine long term condition clinic appointments. Patients not attending these clinics will be invited to an appointment specifically for medicines review.
Information leaflets will be provided when medication is changed but some patients may require further help and advice from you as they change, reduce or stop medication they have been taking for some time.
Reviewing PPI PrescribingWhile PPIs are generally well tolerated we now know that long term PPI therapy may not be without its problems as seen in recent literature potentially linking long term PPI use with C. difficile infections and increased risk of infection.2 NICE guidance for dyspepsia recommends patients taking PPIs have their medication reviewed at least annually with a view to returning to self care using antacids or alginates.3 In practice this can be difficult as PPIs are now recognised to cause rebound acid hypersecretion symptoms on cessation, causing the symptoms they are often initiated to treat,4 as noted recently in the British National Formulary (BNF).2
Despite the short-lived nature of this rebound phenomenon, patients may still need help with symptom relief when reducing or stopping treatment and reassurance that this is to be expected and can be managed. It is advisable to check drug interactions when recommending a product for rebound as the patient may still be taking low dose PPIs and is likely to be on other medications.
Reviewing SSRI PrescribingPatients who take SSRIs along with NSAIDs have a higher risk of GI bleeds, hence why PPIs are often prescribed for gastro-protection.5
If patients have been taking a SSRI for longer than 2 years and are free from relapse in the last 6 months they will be considered for review.6,7 With patient agreement the SSRI will be stopped or reduced over a period of 4 weeks (depending on the individual SSRI). Patients will be made aware of the potential withdrawal effects including:
Please be aware patients may present in community pharmacy with these symptoms. If the symptoms are mild please reassure the patient that they will subside in a few days. However if the symptoms are more severe please refer back to the surgery where we can consider either reinstating the SSRI or consider a slower withdrawal.
• Anxiety
• Sleep Disturbances
• Dizziness & Vertigo
• Nausea, Vomiting & Diarrhoea
• Flu-like symptoms
• Headache
• Tremor
• Sweating
The polypharmacy medicines review project, The Medicines Optimisation Academy and production of the supporting materials, including this leaflet, have been wholly supported with funding from RB Healthcare UK Ltd.
Information for Community Pharmacy:Polypharmacy Medicines Review
Date of preparation: April 2015 UK/G-NHS/1114/0058u
34
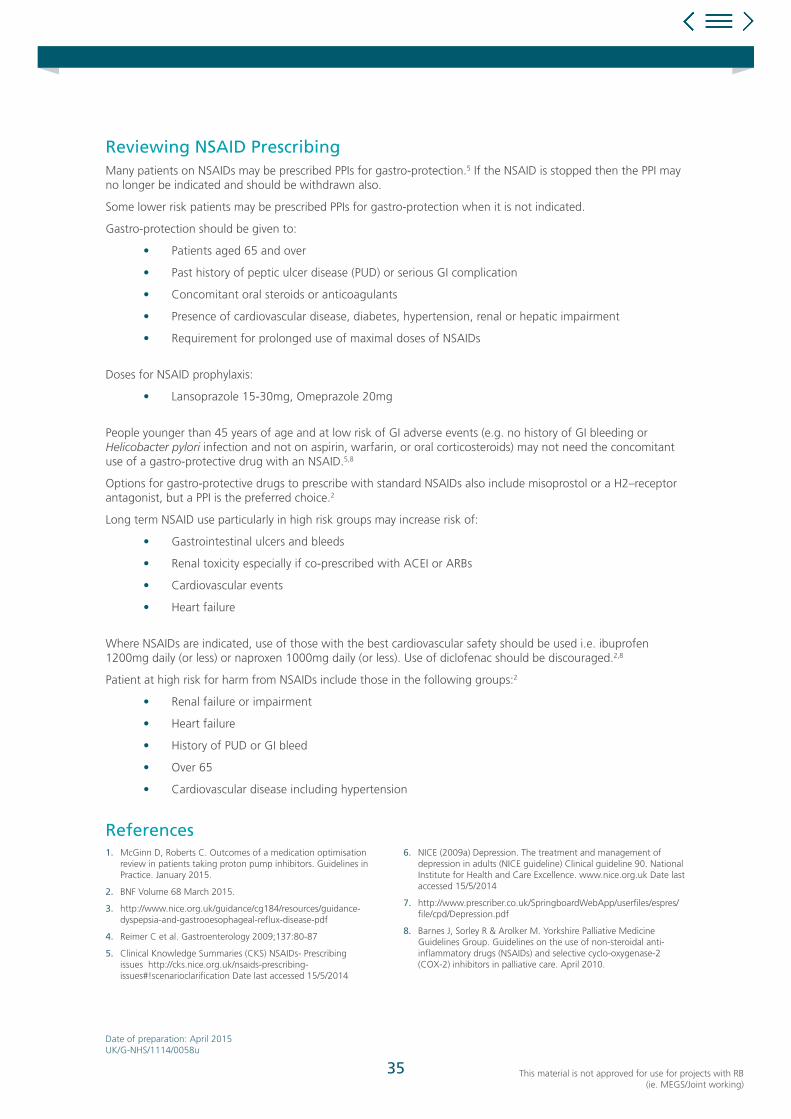
Reviewing NSAID PrescribingMany patients on NSAIDs may be prescribed PPIs for gastro-protection.5 If the NSAID is stopped then the PPI may no longer be indicated and should be withdrawn also.
Some lower risk patients may be prescribed PPIs for gastro-protection when it is not indicated.
Gastro-protection should be given to:
• Patients aged 65 and over
• Past history of peptic ulcer disease (PUD) or serious GI complication
• Concomitant oral steroids or anticoagulants
• Presence of cardiovascular disease, diabetes, hypertension, renal or hepatic impairment
• Requirement for prolonged use of maximal doses of NSAIDs
Doses for NSAID prophylaxis:
• Lansoprazole 15-30mg, Omeprazole 20mg
People younger than 45 years of age and at low risk of GI adverse events (e.g. no history of GI bleeding or Helicobacter pylori infection and not on aspirin, warfarin, or oral corticosteroids) may not need the concomitant use of a gastro-protective drug with an NSAID.5,8
Options for gastro-protective drugs to prescribe with standard NSAIDs also include misoprostol or a H2–receptor antagonist, but a PPI is the preferred choice.2
Long term NSAID use particularly in high risk groups may increase risk of:
• Gastrointestinal ulcers and bleeds
• Renal toxicity especially if co-prescribed with ACEI or ARBs
• Cardiovascular events
• Heart failure
Where NSAIDs are indicated, use of those with the best cardiovascular safety should be used i.e. ibuprofen 1200mg daily (or less) or naproxen 1000mg daily (or less). Use of diclofenac should be discouraged.2,8
Patient at high risk for harm from NSAIDs include those in the following groups:2
• Renal failure or impairment
• Heart failure
• History of PUD or GI bleed
• Over 65
• Cardiovascular disease including hypertension
References
Date of preparation: April 2015 UK/G-NHS/1114/0058u
This material is not approved for use for projects with RB (ie. MEGS/Joint working)
1. McGinn D, Roberts C. Outcomes of a medication optimisation review in patients taking proton pump inhibitors. Guidelines in Practice. January 2015.
2. BNF Volume 68 March 2015.
3. http://www.nice.org.uk/guidance/cg184/resources/guidance-dyspepsia-and-gastrooesophageal-reflux-disease-pdf
4. Reimer C et al. Gastroenterology 2009;137:80-87
5. Clinical Knowledge Summaries (CKS) NSAIDs- Prescribing issues http://cks.nice.org.uk/nsaids-prescribing-issues#!scenarioclarification Date last accessed 15/5/2014
6. NICE (2009a) Depression. The treatment and management of depression in adults (NICE guideline) Clinical guideline 90. National Institute for Health and Care Excellence. www.nice.org.uk Date last accessed 15/5/2014
7. http://www.prescriber.co.uk/SpringboardWebApp/userfiles/espres/file/cpd/Depression.pdf
8. Barnes J, Sorley R & Arolker M. Yorkshire Palliative Medicine Guidelines Group. Guidelines on the use of non-steroidal anti-inflammatory drugs (NSAIDs) and selective cyclo-oxygenase-2 (COX-2) inhibitors in palliative care. April 2010.
35

We recognise the importance of receiving feedback from our Service Users in order to help improve the quality of care and services we provide.
The polypharmacy medicines review project, The Medicines Optimisation Academy and production of the supporting materials, including this leaflet, have been wholly supported with funding from RB Healthcare UK Ltd.
Patient Satisfaction Questionnaire
Name (Optional)
Date
Please tell us what you appreciate most about our service
Please tell us how we can make our service better for you
1 = Lowest score, 5 = Highest score 1 2 3 4 5
1Did you feel that the review of your medicine was properly explained to you?
2 If your medication was changed, how happy were you about this?
3Did you feel that the nurse/pharmacist/doctor listened to what you had to say and took your concerns seriously?
4Did you feel that your questions were well answered and that you were given appropriate advice?
5What is your opinion of the patient information leaflets that you received for your service?
6Overall, how would you rate your satisfaction with the medicines review you received?
7 Was your privacy and dignity respected?
Date of preparation: March 2015 UK/G-NHS/1114/0058s
This material is not approved for use for projects with RB (ie. MEGS/Joint working)
36
Pt no Age Sex PPI DoseStart date
Indication GI medsTotal no of meds
Aspirin NSAIDs SSRI Steroids BisphosChronic disease clinic
4 week review?
Dose & time as per NICE?
Gastro-protection
as per NICE?
Example from PMOR pilot project not to be used without local clinical review and approval
The polypharmacy medicines review project, The Medicines Optimisation Academy and production of the supporting materials, including this leaflet, have been wholly supported with funding from RB Healthcare UK Ltd.
Date of preparation: March 2015 UK/G-NHS/1114/0058r 37

Discontinuation of SSRIs in Adults
Date of preparation: April 2015UK/G-NHS/1114/0058o
The polypharmacy medicines review project, The Medicines Optimisation Academy and production of the supporting materials, including this leaflet, have been wholly supported with funding from RB Healthcare UK Ltd.
This material was authored by Diane McGinn, Medicines Management Consultant, Preston, Lancashire, UK
38
39
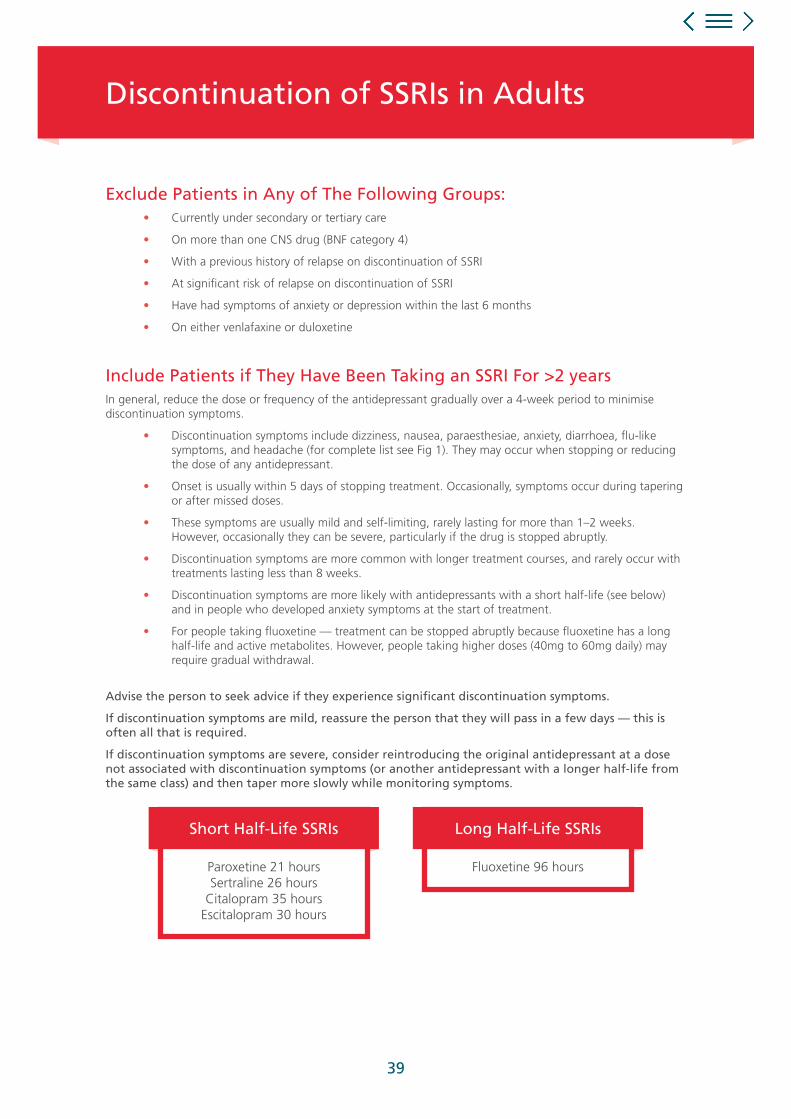
Exclude Patients in Any of The Following Groups: • Currently under secondary or tertiary care
• On more than one CNS drug (BNF category 4)
• With a previous history of relapse on discontinuation of SSRI
• At significant risk of relapse on discontinuation of SSRI
• Have had symptoms of anxiety or depression within the last 6 months
• On either venlafaxine or duloxetine
Include Patients if They Have Been Taking an SSRI For >2 yearsIn general, reduce the dose or frequency of the antidepressant gradually over a 4-week period to minimise discontinuation symptoms.
• Discontinuation symptoms include dizziness, nausea, paraesthesiae, anxiety, diarrhoea, flu-like symptoms, and headache (for complete list see Fig 1). They may occur when stopping or reducing the dose of any antidepressant.
• Onset is usually within 5 days of stopping treatment. Occasionally, symptoms occur during tapering or after missed doses.
• These symptoms are usually mild and self-limiting, rarely lasting for more than 1–2 weeks. However, occasionally they can be severe, particularly if the drug is stopped abruptly.
• Discontinuation symptoms are more common with longer treatment courses, and rarely occur with treatments lasting less than 8 weeks.
• Discontinuation symptoms are more likely with antidepressants with a short half-life (see below) and in people who developed anxiety symptoms at the start of treatment.
• For people taking fluoxetine — treatment can be stopped abruptly because fluoxetine has a long half-life and active metabolites. However, people taking higher doses (40mg to 60mg daily) may require gradual withdrawal.
Advise the person to seek advice if they experience significant discontinuation symptoms.
If discontinuation symptoms are mild, reassure the person that they will pass in a few days — this is often all that is required.
If discontinuation symptoms are severe, consider reintroducing the original antidepressant at a dose not associated with discontinuation symptoms (or another antidepressant with a longer half-life from the same class) and then taper more slowly while monitoring symptoms.
Discontinuation of SSRIs in Adults
Paroxetine 21 hoursSertraline 26 hours
Citalopram 35 hoursEscitalopram 30 hours
Short Half-Life SSRIs
Fluoxetine 96 hours
Long Half-Life SSRIs

40
Citalopram 40mg 30mg 20mg 10mg 10mg alt days
20mg 20mg/10mg alt days 10mg 10mg alt days 5mg alt days
10mg 10mg/5mg alt days 5mg 5mg alt days 5mg alt days
Escitalopram 20mg 20mg/10mg alt days 10mg 10mg alt days 5mg alt days
10mg 10mg/5mg alt days 5mg 5mg alt days 5mg alt days
Fluoxetine 20mg STOP
40mg 40mg/30mg alt days 30mg 30mg/20mg alt days 20mg
60mg* 60mg/40mg alt days 40mg As for 40mg above
Fluvoxamine** 150mg BD 150mg + 100mg 100mg + 50mg 50mg BD 50mg
100mg BD 100mg + 50mg 50mg BD 50mg 50mg alt days
100mg 50mg BD50mg BD + 50mg daily
alt days50mg 50mg alt days
50mg Miss every 3rd day’s dose 50mg alt days 50mg alt days 50mg every 4th day
Paroxetine 30mg 30mg/20mg alt days 20mg 20mg/10mg alt days 10mg
20mg 20mg/10mg alt days 10mg 10mg alt days 10mg alt days
Sertraline 200mg 200mg/150mg alt days 150mg 100mg 50mg
150mg 150mg/100mg alt days 100mg 100mg/50mg alt days 50mg
100mg 100mg/50mg alt days 50mg 50mg alt days 50mg half a tab alt days
50mg Miss every 3rd day’s dose 50mg alt days25mg
(half a tablet)25mg alt days
DrugStarting
Daily DoseWeek 1 Week 2 Week 3
Week 4 Then Stop
If patients experience withdrawal symptoms at any stage, move back to previous week’s dosage and reduce more slowly. For lowest doses patients may need to switch to liquid preparations where available — may also assist if need slower withdrawal.
Fluoxetine at doses of less than 40mg daily may be stopped without gradual reduction. For higher doses consider dosage reduction of 25% per week as for other drugs below.
* Check indication for fluoxetine 60mg not for eating disorders
** Where dose is split, choice of whether to reduce AM or PM dose first depends on patient preference

41
ParaesthesiaNumbness
Electric-shock-like sensationsRushing noise ‘in head’Palinopsia (visual trails)
General Symptoms
IrritabilityAnxiety/agitation
Low moodTearfulness
Affective Symptoms
Light-headednessDizzinessVertigo
Disequilibrium
NauseaVomitingDiarrhoea
Gastrointestinal Symptoms
LethargyHeadache
TremorSweatingAnorexia
General Somatis Symptoms
InsomniaNightmares
Excessive dreaming
Sleep Disturbance
Primary SSRIDiscontinuation
Syndrome
Fig 1: Key symptom groups of primary SSRI discontinuation syndrome. Common or characteristic symptoms are listed, but many others are reported. Patients vary in the number and combination of symptoms they manifest.
ARM and the Medicines Optimisation Academy are non-promotional education programmes designed by RB UK to improve patient care and support healthcare professional.
This material is not approved for use for projects with RB (ie. MEGS/Joint working)
42
Ad
vice
fo
r Pa
tien
ts t
akin
g
Sele
ctiv
e Se
roto
nin
Re-
up
take
In
hib
ito
rs (
SSR
Is)
A m
edic
ine
use
d t
o h
elp
wit
hd
epre
ssio
n a
nd
oth
er m
enta
lh
ealt
h d
iso
rder
s
This
mat
eria
l was
dev
elo
ped
by
Dia
ne
McG
inn
MPh
arm
Pro
du
ctio
n o
f th
is le
afl e
t h
as b
een
su
pp
ort
ed w
ith
fu
nd
ing
fro
m R
B H
ealt
hca
re U
K L
td.
UK
/G-N
SH/1
14/0
058x
Dat
e of
pre
para
tion:
Mar
ch 2
015.
Prac
tice
stam
p to
go
here
Ho
w D
o I
Sto
p S
afel
y?If
you
have
bee
n on
ant
idep
ress
ants
co
ntin
ually
for
6 w
eeks
or
mor
e yo
u sh
ould
no
t st
op t
reat
men
t ab
rupt
ly u
nles
s th
ere
are
spec
ial c
ircum
stan
ces.
The
exce
ptio
n to
thi
s is
fl uo
xetin
e at
a d
ose
of 2
0mg
a da
y. B
ecau
se it
rem
ains
in t
he
bloo
dstr
eam
for
suc
h a
long
tim
e an
yway
, it
can
be s
topp
ed s
trai
ght
away
with
out
redu
cing
th
e do
se s
low
ly. I
f yo
u pr
efer
, you
can
gra
dual
ly
spac
e ou
t th
e do
ses
from
onc
e da
ily t
o on
ce
ever
y tw
o da
ys a
nd s
o on
.
With
oth
er a
ntid
epre
ssan
ts t
hat
last
a s
hort
er
time
in y
our
bloo
dstr
eam
, the
bes
t th
ing
to d
o is
red
uce
the
daily
dos
e ev
ery
one
to t
wo
wee
ks.
Your
pra
ctic
e w
ill b
e ab
le t
o ad
vise
you
abo
ut
how
bes
t to
red
uce
your
dos
e.
With
draw
al s
ympt
oms
are
unlik
ely
to o
ccur
if
you
redu
ce t
he d
ose
grad
ually
. If
with
draw
al
sym
ptom
s do
occ
ur, t
hey
will
usu
ally
last
less
th
an t
wo
wee
ks. A
n op
tion
if th
ey d
o oc
cur
is
to r
esta
rt t
he d
rug
and
redu
ce t
he d
ose
even
m
ore
slow
ly.
Alw
ays
take
you
r m
edic
atio
n as
adv
ised
by
a he
alth
care
pro
fess
iona
l and
tal
k to
you
r do
ctor
be
fore
sto
ppin
g an
y tr
eatm
ents
you
rsel
f.
Rep
ort
ing
of
sid
e-ef
fect
s If
you
get
any
side
eff
ects
, tal
k to
you
r do
ctor
, ph
arm
acis
t or
nur
se. T
his
incl
udes
any
pos
sibl
e si
de-e
ffec
ts n
ot li
sted
in t
he p
acka
ge le
afl e
t. Y
ou
can
also
rep
ort
side
eff
ects
dire
ctly
via
the
Yel
low
C
ard
Sche
me
at w
ww
.mhr
a.go
v.uk
/yel
low
card
.
By r
epor
ting
side
eff
ects
you
can
hel
p pr
ovid
e m
ore
info
rmat
ion
on t
he s
afet
y of
thi
s m
edic
ine.
Follo
w U
pM
ost
peop
le c
ome
off
antid
epre
ssan
ts w
ith li
ttle
or
no
prob
lem
s an
d fo
llow
ing
the
advi
ce in
thi
s le
afl e
t sh
ould
hel
p yo
u do
tha
t. H
owev
er if
you
do
get
any
pro
blem
s th
en p
leas
e as
k fo
r he
lp.
You
can
cont
act
one
of t
he M
enta
l Hea
lth T
eam
or
dis
cuss
you
r w
orrie
s w
ith y
our
GP.
Hel
plin
esM
ind
Tel:
0300
123
339
3w
ww
.min
d.or
g.uk
NH
S ad
vice
Tel:
111
ww
w.n
hsdi
rect
.nhs
.uk
Dep
ress
ion
Alli
ance
ww
w.d
epre
ssio
nalli
ance
.org
Dep
ress
ion
UK
Tel:
0115
960
8855
ww
w.d
epre
ssio
n.uk
.org
Ret
hin
k M
enta
l Illn
ess
Tel:
0300
500
0927
(Mon
-Fri
10am
-2pm
)w
ww
.ret
hink
.org
San
elin
eTe
l: 08
45 6
7800
0 (6
pm-1
1pm
)

43
Wh
at A
re S
SRIs
?Se
lect
ive
sero
toni
n re
-upt
ake
inhi
bito
rs, k
now
n as
SSR
Is, a
re a
gro
up o
f m
edic
ines
pre
scrib
ed
to h
elp
with
the
sym
ptom
s of
dep
ress
ion
and
othe
r co
nditi
ons
such
as
pani
c di
sord
er,
obse
ssiv
e co
mpu
lsiv
e di
sord
er a
nd g
ener
alis
ed
anxi
ety
diso
rder
.
Ther
e ar
e a
num
ber
of S
SRIs
with
diff
eren
t na
mes
yo
u m
ay b
e ta
king
. The
se in
clud
e:
• C
italo
pram
• Es
citlo
pram
• Fl
uoxe
tine
• Fl
uvox
amin
e
• Pa
roxe
tine
• Se
rtra
line
Ho
w E
ffec
tive
Are
SSR
Is?
Abo
ut 5
-7 in
10
peop
le w
ith m
oder
ate
or s
ever
e de
pres
sion
hav
e an
impr
ovem
ent
in s
ympt
oms
with
in a
few
wee
ks o
f st
artin
g tr
eatm
ent
with
an
antid
epre
ssan
t.
It is
bes
t to
wai
t fo
r 3-
4 w
eeks
bef
ore
deci
ding
if
trea
tmen
t w
ith a
n SS
RI is
hel
ping
or
not.
Ho
w D
o S
SRIs
Wo
rk?
Ant
idep
ress
ants
alte
r th
e ba
lanc
e of
som
e of
the
ch
emic
als
in t
he b
rain
(neu
rotr
ansm
itter
s). S
SRI
antid
epre
ssan
ts m
ainl
y af
fect
a n
euro
tran
smitt
er
calle
d se
roto
nin.
An
alte
red
bala
nce
of s
erot
onin
an
d ot
her
neur
otra
nsm
itter
s is
tho
ught
to
play
a
part
in c
ausi
ng d
epre
ssio
n an
d ot
her
cond
ition
s.
Wh
en D
o I
Sto
p?
If yo
u st
op a
ntid
epre
ssan
ts b
efor
e 8
or 9
m
onth
s is
up,
the
sym
ptom
s of
dep
ress
ion
are
mor
e lik
ely
to c
ome
back
.
The
curr
ent
reco
mm
enda
tions
are
tha
t it
is b
est
for
mos
t pe
ople
to
cont
inue
tak
ing
antid
epre
ssan
ts f
or s
ix m
onth
s af
ter
thei
r sy
mpt
oms
have
red
uced
.
Will
I H
ave
An
y W
ith
dra
wal
Sym
pto
ms?
Stud
ies
have
sho
wn
that
up
to a
thi
rd o
f pe
ople
ha
ve d
isco
ntin
uatio
n sy
mpt
oms
for
a s
hort
tim
e w
hen
they
sto
p an
tidep
ress
ants
. You
may
get
sy
mpt
oms
if yo
u st
op to
o qu
ickl
y an
d th
is s
eem
s to
ha
ppen
mor
e of
ten
with
long
er tr
eatm
ent c
ours
es.
Sym
ptom
s in
clud
e:
• St
omac
h up
sets
• Fl
u-lik
e sy
mpt
oms
• A
nxie
ty
• D
izzi
ness
• V
ivid
dre
ams
at n
ight
• Se
nsat
ions
in t
he b
ody
like
little
sho
cks
They
are
mos
t lik
ely
to b
e ex
perie
nced
whe
n re
duci
ng f
rom
an
SSRI
ant
idep
ress
ant
calle
d Pa
roxe
tine
(Ser
oxat
)
(Ver
y ra
rely
som
e pe
ople
rep
orte
d su
icid
al
thou
ghts
eve
n in
tho
se w
ho h
ave
neve
r ex
perie
nced
thi
s be
fore
. If
this
occ
urs
plea
se
mak
e an
urg
ent
appo
intm
ent
to s
ee y
our
GP
and
rem
embe
r th
at t
hese
tho
ught
s do
not
re
mov
e yo
ur a
bilit
y to
con
trol
you
r ac
tions
.)
Wh
at A
re T
he
Poss
ible
Sid
e Ef
fect
s an
d R
isks
?M
ost
peop
le h
ave
eith
er li
ttle
, or
no s
ide-
effe
cts
and
thes
e m
ay v
ary
betw
een
diff
eren
t pr
epar
atio
ns. T
he le
afl e
t th
at c
omes
in t
he
med
icin
e pa
cket
giv
es a
ful
l lis
t of
pos
sibl
e si
de-e
ffec
ts.
The
mos
t co
mm
on s
ide-
effe
cts
incl
ude:
• D
iarr
hoea
, fee
ling
sick
, vom
iting
• H
eada
ches
• D
row
sine
ss
SSRI
s ar
e as
soci
ated
with
a s
mal
l inc
reas
ed r
isk
of b
leed
ing
into
the
gut
. Thi
s is
esp
ecia
lly in
ol
der
peop
le a
nd in
peo
ple
taki
ng o
ther
m
edic
ines
. The
refo
re, i
deal
ly, S
SRIs
sho
uld
be a
void
ed if
you
tak
e as
pirin
, war
farin
or
nons
tero
idal
ant
i-infl
am
mat
ory
drug
s (N
SAID
s)
such
as
ibup
rofe
n, n
apro
xen
or d
iclo
fena
c. If
no
sui
tabl
e al
tern
ativ
e to
an
SSRI
can
be
foun
d an
d yo
u ha
ve a
n in
crea
sed
risk
of b
leed
ing,
the
n yo
ur d
octo
r m
ay a
dvis
e th
at y
ou t
ake
anot
her
m
edic
ine
to p
rote
ct t
he li
ning
of
the
gut.
Ad
vice
fo
r Pa
tien
ts t
akin
g
Pro
ton
Pu
mp
Inh
ibit
ors
(PP
Is)
A m
edic
ine
use
d f
or
Hea
rtb
urn
an
d In
dig
esti
on
(als
o c
alle
d r
efl u
x)
Pro
du
ctio
n o
f th
is le
afl e
t h
as b
een
su
pp
ort
ed w
ith
fu
nd
ing
fro
m R
B H
ealt
hca
re U
K L
td.
UK
/G-N
HS/
1114
/005
8y D
ate
of p
repa
ratio
n: M
arch
201
5.
Prac
tice
stam
p to
go
here
Hel
p T
o M
anag
e R
ebo
un
d S
ymp
tom
sYo
ur h
ealth
care
pro
fess
iona
l will
adv
ise
on w
ays
to h
elp
with
hea
rtbu
rn a
nd in
dige
stio
n th
at
can
happ
en w
hen
you
try
to s
top
a PP
I. Th
ey
may
pre
scrib
e or
rec
omm
end
a di
ffer
ent
type
of
med
icin
e ca
lled
an a
lgin
ate.
Alg
inat
es w
ork
by f
orm
ing
a ph
ysic
al b
arrie
r at
the
top
of
the
stom
ach
that
can
sto
p th
e ac
id g
ettin
g ba
ck o
ut
into
the
oes
opha
gus
whe
re it
cau
ses
pain
.
Will
I N
eed
To
Tak
e a
PPI I
n T
he
Futu
re?
Hea
rtbu
rn a
nd in
dige
stio
n ar
e qu
ite c
omm
on
and
can
com
e an
d go
ove
r tim
e. Y
ou m
ight
fi nd
a
few
cha
nges
to
your
life
styl
e or
the
way
you
ea
t an
d dr
ink
will
hel
p ke
ep y
our
sym
ptom
s un
der
cont
rol.
If no
t, y
our
phar
mac
ist
can
advi
se o
n re
med
ies
you
can
buy
to h
elp.
If y
our
sym
ptom
s be
com
e co
mm
on o
r tr
oubl
esom
e ag
ain
you
shou
ld s
peak
to
your
doc
tor
who
may
th
ink
it ne
cess
ary
to p
resc
ribe
a PP
I aga
in.
Alw
ays
go s
trai
ght
to y
our
doct
or if
you
ex
perie
nce
any
of t
he f
ollo
win
g:
• W
eigh
t lo
ss t
hat
isn’
t in
tent
iona
l.
• D
iffi c
ulty
sw
allo
win
g.
• Vo
miti
ng r
outin
ely
or o
ften
.
• Si
gns
of b
lood
if y
ou v
omit
or w
hen
you
go
to t
he t
oile
t.
Way
s To
Try
& A
void
H
eart
bu
rn &
Ind
iges
tio
nLo
ts o
f pe
ople
get
hea
rtbu
rn a
nd in
dige
stio
n fr
om t
ime
and
time.
Get
ting
to k
now
whe
n yo
uge
t he
artb
urn
and
indi
gest
ion
can
allo
w y
ou t
o sp
ot t
he t
rigge
rs. I
f yo
u’re
not
sur
e w
hat
sets
off
yo
ur h
eart
burn
try
kee
ping
a f
ood
and
sym
ptom
di
ary
and
see
if yo
u ca
n sp
ot a
ny p
atte
rns.
So
met
imes
it’s
not
a pa
rtic
ular
foo
d bu
t a
time
of d
ay o
r ty
pe o
f ex
erci
se.
• Ea
t yo
ur m
eals
at
regu
lar
times
and
try
not
to
eat
too
qui
ckly.
Bet
ter
to e
at s
mal
ler
mea
ls
mor
e of
ten,
so yo
u do
n’t o
verfi
ll yo
ur st
omac
h.
• Tr
y no
t to
eat
too
clo
se t
o be
dtim
e if
you
tend
to
suff
er a
t ni
ght.
Lea
ving
3 h
ours
be
twee
n ea
ting
and
goin
g to
bed
can
hel
p.
• If
you’
re a
nig
ht t
ime
suff
erer
, lift
the
hea
d of
the
bed
. A g
ood
idea
is t
o pu
t br
icks
or
book
s un
der
the
bed.
• Tr
y no
t to
drin
k to
o m
any
fi zzy
drin
ks, e
ven
if it’
s sp
arkl
ing
wat
er. T
he g
as c
an c
ause
pr
essu
re in
you
r st
omac
h.
• If
you
drin
k al
coho
l, it
help
s to
cut
dow
n bu
t it
can
be t
he t
ype
of d
rink
that
’s a
prob
lem
as
wel
l, fo
r ex
ampl
e w
hite
win
e is
a
mor
e co
mm
on t
rigge
r th
an r
ed w
ine.
• If
you
smok
e tr
y to
cut
dow
n or
sto
p.
• A
void
foo
ds y
ou a
ssoc
iate
with
sym
ptom
s.
• M
any
peop
le k
now
the
ir tr
igge
rs -
tom
atoe
s ar
e a
com
mon
one
.
Alg
inat
eb
arrie
r
ACID
BILE
PEPSIN
44

Wh
at A
re P
roto
n P
um
p In
hib
ito
rs?
Prot
on p
ump
inhi
bito
rs, o
ften
cal
led
PPIs
are
a
type
of
med
icin
e, u
sual
ly p
resc
ribed
by
your
do
ctor
.
Ther
e ar
e a
num
ber
of P
PIs
with
diff
eren
t na
mes
, yo
u m
ay b
e ta
king
:
• O
mep
razo
le
• La
nsop
razo
le
• Pa
ntop
razo
le
• Ra
bepr
azol
e
• Es
omep
razo
le
Wh
y D
o P
eop
le T
ake
PPIs
?Yo
ur s
tom
ach
mak
es a
cid
to h
elp
dige
st f
ood
but
in s
ome
peop
le t
he a
cid
can
irrita
te t
he s
tom
ach
caus
ing
disc
omfo
rt. I
t ca
n al
so g
et b
ack
up in
to
the
oeso
phag
us (f
oodp
ipe
that
goe
s fr
om y
our
mou
th t
o yo
ur s
tom
ach)
and
cau
ses
pain
, kno
wn
as h
eart
burn
. Thi
s is
cal
led
refl u
x.
PPIs
are
use
d to
rel
ieve
sym
ptom
s of
hea
rtbu
rn
and
indi
gest
ion
and
rela
ted
stom
ach
prob
lem
s.
Som
e ot
her
med
icin
es c
an ir
ritat
e th
e st
omac
h so
som
etim
es p
eopl
e w
ho d
on’t
ha
ve t
hese
con
ditio
ns t
ake
PPIs
to
help
pr
even
t th
is h
appe
ning
.
Ho
w D
o P
PIs
Wo
rk?
PPIs
wor
k by
red
ucin
g th
e am
ount
of
acid
tha
t yo
ur s
tom
ach
mak
es. T
his
in t
urn
redu
ces
the
disc
omfo
rt o
r pa
in t
hat
you
feel
in y
our
stom
ach
or c
hest
whe
n th
e ac
id c
ause
s irr
itatio
n.
Wh
at H
app
ens
Wh
en Y
ou
Sto
pTa
kin
g P
PIs?
If yo
u ta
ke a
PPI
for
mor
e th
an a
few
wee
ks,
your
sto
mac
h ca
n in
crea
se it
s ab
ility
to
mak
e ac
id. T
his
mea
ns t
hat
whe
n th
e PP
I is
stop
ped,
ac
id le
vels
can
be
high
er t
han
befo
re y
ou s
tart
ed
taki
ng t
hem
.
For
this
rea
son
som
e pe
ople
fi nd
tha
t th
eir
hear
tbur
n or
indi
gest
ion
wor
sens
whe
n th
ey t
ry
to s
top
taki
ng a
PPI
. The
se a
re c
alle
d re
boun
d sy
mpt
oms
and
they
can
last
abo
ut 2
wee
ks.
Step
pin
g D
ow
n O
r O
ff P
PIs
Beca
use
of th
e re
boun
d sy
mpt
oms
it is
adv
isab
le
to s
top
taki
ng P
PIs
grad
ually
and
follo
w th
e ad
vice
of
you
r doc
tor o
r hea
lthca
re p
rofe
ssio
nal t
o he
lp
man
age
your
sym
ptom
s in
the
fi rst
few
wee
ks.
You
r H
ealt
hca
re P
rofe
ssio
nal
may
ad
vise
:
• Ju
st r
educ
ing
the
dose
of
the
PPI.
• St
oppi
ng t
he P
PI.
• Re
duci
ng t
he d
ose
for
a fe
w w
eeks
th
en s
topp
ing
alto
geth
er.
• C
hang
ing
the
way
you
tak
e th
e PP
I so
you
just
tak
e it
occa
sion
ally
whe
n yo
u fe
el s
ympt
oms.
• U
se o
f an
othe
r m
edic
ine
(cal
led
an
algi
nate
) for
a f
ew w
eeks
to
help
with
th
e re
boun
d sy
mpt
oms.
• Li
fest
yle
chan
ges
that
cou
ld h
elp
stop
sy
mpt
oms
com
ing
back
in t
he f
utur
e.
Ho
w L
on
g S
ho
uld
Yo
u T
ake
PPIs
Fo
r?A
lthou
gh P
PIs
are
wel
l tol
erat
ed in
mos
t pa
tient
s, n
o m
edic
ines
are
com
plet
ely
safe
or
with
out
side
eff
ects
. So
, as
with
all
med
icin
es, y
ou s
houl
d on
ly t
ake
a PP
I fo
r as
long
as
you
need
it.
Peop
le t
ake
PPIs
for
diff
eren
t le
ngth
s of
tim
e, y
our
doct
or w
ill a
dvis
e w
hat
is r
ight
for
you
.
On
aver
age,
if y
ou’r
e ta
king
PPI
s fo
r he
artb
urn
or
indi
gest
ion
you’
ll ta
ke t
hem
for
4-8
wee
ks t
o al
low
yo
ur b
ody
to h
eal a
ny in
fl am
mat
ion.
If yo
u’re
tak
ing
PPIs
bec
ause
you
’re
also
usi
ng
anot
her
med
icin
e th
at c
an ir
ritat
e th
e st
omac
h, y
ou
mig
ht n
eed
to t
ake
them
for
long
er.
Alw
ays
take
you
r m
edic
atio
n as
adv
ised
by
a he
alth
care
pr
ofes
sion
al a
nd t
alk
to y
our
doct
or b
efor
e st
oppi
ng
any
trea
tmen
ts y
ours
elf.
If y
ou g
et a
ny s
ide
effe
cts,
ta
lk t
o yo
ur d
octo
r, ph
arm
acis
t or
nur
se. T
his
incl
udes
an
y po
ssib
le s
ide
effe
cts
not
liste
d in
the
pac
kage
le
afl e
t. Y
ou c
an a
lso
repo
rt s
ide
effe
cts
dire
ctly
via
the
Ye
llow
Car
d Sc
hem
e at
ww
w.m
hra.
gov.
uk/y
ello
wca
rd.
By re
port
ing
side
eff
ects
you
can
hel
p pr
ovid
e m
ore
info
rmat
ion
on t
he s
afet
y of
you
r m
edic
ines
.
Aci
dre
�ux
Sto
mac
h
Low
er
oeso
pha
geal
sp
hinc
ter
45

Pra
ctic
e st
amp
to
go h
ere
Ad
vice
fo
r Pa
tien
ts t
akin
g
No
n-s
tero
idal
An
ti-i
nfl
amm
ato
ryD
rug
s (N
SAID
s)
A t
ype
of
med
icin
e u
sed
to
hel
p w
ith
pai
n a
nd
sw
ellin
gin
mu
scle
s an
d jo
ints
Pro
du
ctio
n o
f th
is le
afl e
t h
as b
een
su
pp
ort
ed w
ith
fu
nd
ing
fro
m R
B H
ealt
hca
re U
K L
td.
UK
/G-N
HS/
1114
/005
8z D
ate
of p
repa
ratio
n: M
arch
201
5.
Prac
tice
stam
p to
go
here
You
r Si
de-
effe
cts
Som
e pa
tient
s m
ay g
et s
ide-
effe
cts
with
NSA
IDs
whi
ch c
an in
clud
e th
e fo
llow
ing
- th
ese
shou
ld
stop
if y
ou s
top
taki
ng t
he N
SAID
:
Nau
sea
(fee
ling
sick
), di
arrh
oea,
ras
hes,
head
ache
, diz
zine
ss, n
ervo
usne
ss, d
epr e
ssio
n,
drow
sine
ss, i
nsom
nia
(poo
r sl
eep)
, ver
tigo
(diz
zine
ss),
and
tinni
tus
(noi
ses
in t
he e
ar).
Alw
ays
take
you
r m
edic
atio
n as
adv
ised
by
a he
alth
car e
pro
fess
iona
l and
tal
k to
you
r do
ctor
be
fore
sto
ppin
g an
y tr
eatm
ents
you
rsel
f.
If yo
u ge
t an
y si
de e
ffec
ts, t
alk
to y
our
doct
or,
phar
mac
ist
or n
urse
. Thi
s in
clud
es a
ny p
ossi
ble
side
eff
ects
not
list
ed in
the
pac
kage
leafl
et.
Yo
u ca
n al
so r
epor
t si
de e
ffec
ts d
irect
ly v
ia t
he
Yello
w C
ard
Sche
me
at w
ww
.mhr
a.go
v.uk
/ye
llow
card
. By
repo
rtin
g si
de e
ffec
ts y
ou c
an
help
pro
vide
mor
e in
form
atio
n on
the
saf
ety
of
your
med
icin
es
Oth
er M
edic
atio
nU
sing
mor
e th
an o
ne N
SAID
at
a tim
e ca
n in
crea
se t
he r
isk
of h
arm
. Alw
ays
tell
the
phar
mac
ist
wha
t m
edic
atio
n yo
u ar
e ta
king
w
hen
buyi
ng m
edic
ines
.
NSA
IDs
are
also
an
ingr
edie
nt in
man
y ru
bs
and
gels
tha
t ar
e us
ed f
or m
uscl
e an
d jo
int
pain
. Th
ese
shou
ld n
ot b
e us
ed if
you
are
als
o ta
king
N
SAID
tab
lets
or
caps
ules
.
Med
icat
ion
Rev
iew
If yo
u ha
ve b
een
taki
ng a
n N
SAID
reg
ular
ly a
s pa
rt o
f yo
ur r
epea
t m
edic
atio
n, y
our
GP,
pra
ctic
e nu
rse
or p
harm
acis
t m
ay n
eed
to r
evie
w t
his
from
tim
e to
tim
e to
ass
ess
if it
is s
afe
for
you
to c
ontin
ue o
r if
it w
ould
be
bett
er t
o pr
escr
ibe
an a
ltern
ativ
e m
edic
atio
n to
hel
p w
ith y
our
sym
ptom
s.
46
Wh
at A
re N
on
-ste
roid
al
An
ti-i
nfl
amm
ato
ry D
rug
s?N
on-s
tero
idal
ant
i-infl
am
mat
ory
drug
s, o
ften
ca
lled
NSA
IDs,
are
a t
ype
of m
edic
ine
that
is
pres
crib
ed b
y yo
ur G
P fo
r pa
in o
r in
fl am
mat
ion.
Th
ere
are
a nu
mbe
r of
NSA
IDs
with
diff
eren
t na
mes
tha
t yo
u m
ay b
e ta
king
. The
se in
clud
e:
Wh
y D
o p
eop
le T
ake
NSA
IDs?
NSA
IDs
are
used
for
tw
o m
ain
reas
ons:
• To
eff
ectiv
ely
help
with
pai
n -
NSA
IDs
are
used
in v
ario
us c
ondi
tions
suc
h as
os
teoa
rthr
itis,
mus
cula
r sp
rain
s an
d st
rain
s an
d he
adac
hes.
• To
red
uce
infl a
mm
atio
n -
NSA
IDs
take
n in
rep
eate
d do
ses
can
help
with
pai
n an
d st
iffne
ss in
con
ditio
ns s
uch
as
rheu
mat
oid
arth
ritis
.
Ho
w D
o N
SAID
s W
ork
?Th
ey w
ork
by s
topp
ing
the
body
mak
ing
chem
ical
s ca
lled
pros
tagl
andi
ns w
hich
cau
se
pain
and
infl a
mm
atio
n.
• C
elec
oxib
• D
iclo
fena
c
• Et
oric
oxib
• Ib
upro
fen
• In
dom
etac
in
• K
etop
rofe
n
• M
elox
icam
• N
apro
xen
• Pi
roxi
cam
Patie
nts
mos
t at
ris
k of
sto
mac
h bl
eeds
incl
ude:
• Th
ose
taki
ng a
n an
ti-in
fl am
mat
ory
plus
w
arfa
rin, s
tero
ids,
or
low
-dos
e as
pirin
. Th
ese
com
bina
tions
of
med
icin
es s
houl
d on
ly b
e us
ed if
abs
olut
ely
nece
ssar
y.
• Pe
ople
age
d ov
er 6
5
• Pe
ople
with
a p
ast
hist
ory
of a
sto
mac
h or
duo
dena
l ulc
er
Thes
e pa
tient
s m
ay n
eed
to t
ake
a m
edic
ine
to
prot
ect
thei
r st
omac
h fr
om t
he e
ffec
ts o
f th
e N
SAID
. You
r do
ctor
will
adv
ise
if th
is is
the
ca
se f
or y
ou.
Ad
vice
Ab
ou
t Ta
kin
g N
SAID
sN
SAID
s do
not
alte
r th
e co
urse
of
pain
ful
cond
ition
s su
ch a
s ar
thrit
is. T
hey
just
eas
e sy
mpt
oms
of p
ain
and
stiff
ness
.
If yo
u ta
ke a
n an
ti-in
fl am
mat
ory
pain
kille
r, as
a r
ule
you
shou
ld t
ake
the
low
est
dose
tha
t is
eff
ectiv
e, f
or t
he s
hort
est
leng
th o
f tim
e th
at is
pos
sibl
e to
red
uce
the
risk
of
deve
lopi
ng s
ide-
effe
cts.
Wh
at A
re T
he
Poss
ible
Ris
ks
of
Taki
ng
NSA
IDs?
The
chem
ical
s (p
rost
agla
ndin
s) t
hat
are
redu
ced
by a
nti-i
nfl a
mm
ator
ies
are
also
invo
lved
in h
elpi
ng
to p
rote
ct t
he li
ning
of
the
stom
ach
from
the
ef
fect
s of
the
aci
d w
ithin
the
sto
mac
h. U
sual
ly
NSA
IDs
are
effe
ctiv
e m
edic
ines
tha
t ar
e w
ell
tole
rate
d bu
t oc
casi
onal
ly a
sto
mac
h ul
cer
can
deve
lop.
Blee
ding
in t
he s
tom
ach
is a
pro
blem
tha
t ne
eds
urge
nt m
edic
al a
tten
tion.
Eld
erly
peo
ple
are
mor
e pr
one
to t
his
prob
lem
, but
it c
an o
ccur
in
any
body
.
Ther
efor
e, if
you
are
tak
ing
an a
nti-i
nfl a
mm
ator
y an
d yo
u de
velo
p up
per
abdo
min
al p
ains
, pas
s bl
ood
or b
lack
sto
ols,
or
vom
it bl
ood,
the
n st
op
taki
ng t
he t
able
ts a
nd s
ee a
doc
tor
urge
ntly
, or
go t
o a
casu
alty
dep
artm
ent.
47

Life
styl
eSe
rvic
es In
form
atio
n
Loca
l hel
p a
nd
su
pp
ort
fo
rw
hen
yo
u w
ant
to m
ake
po
siti
ve li
fest
yle
chan
ges
Pro
du
ctio
n o
f th
is le
afl e
t h
as b
een
su
pp
ort
ed w
ith
fu
nd
ing
fro
m R
B H
ealt
hca
re U
K L
td.
UK
/G-N
HS/
1114
/005
8aa
Dat
e of
pre
para
tion:
Mar
ch 2
015.
Prac
tice
stam
p to
go
here
Smo
kin
gIf
you
wan
t to
sto
p sm
okin
g an
d th
ink
you’
re
read
y to
giv
e it
a tr
y yo
u m
ight
sta
nd a
bet
ter
chan
ce o
f su
ccee
ding
if y
ou g
et s
ome
help
an
d su
ppor
t.
Your
loca
l pha
rmac
ist
can
advi
se o
r fo
r he
lp
incl
udin
g ni
cotin
e re
plac
emen
t an
d ot
her
prod
ucts
on
pres
crip
tion
you
can
cont
act
your
lo
cal S
top
Smok
ing
serv
ice.
Alc
oh
ol &
Ille
gal
Dru
g U
seTh
e re
com
men
ded
safe
leve
l of
alco
hol i
s no
m
ore
than
3-4
uni
ts (1
uni
t =
hal
f a
pint
of
lage
r or
a s
mal
l gla
ss o
f w
ine)
for
adu
lt m
ales
per
day
an
d no
mor
e th
an 2
-3 u
nits
for
adu
lt fe
mal
es p
er
day.
The
re a
re n
o sa
fe li
mits
for
you
ng p
eopl
e.
Exce
ssiv
e al
coho
l use
is li
nked
to
viol
ent
crim
es
and
dom
estic
vio
lenc
e, c
ar r
elat
ed d
eath
s an
d ta
king
ris
ks s
uch
as h
avin
g un
prot
ecte
d se
x.
You
can
fi nd
info
rmat
ion
abou
t se
xual
hea
lth,
cont
race
ptio
n an
d lo
cal c
linic
s at
you
r pr
actic
e.
Long
-ter
m a
lcoh
ol u
se c
an le
ad t
o liv
er d
amag
e,
stom
ach
canc
er a
nd h
eart
dis
ease
.
Usi
ng d
rugs
oth
er t
han
alco
hol a
lso
carr
ies
a w
hole
ran
ge o
f ris
ks d
epen
ding
on
wha
t dr
ug
you
take
.
Serv
ices
In Y
ou
r A
rea
Gen
eral
Hel
p &
Su
pp
ort
NH
S C
hoic
es -
Hea
lthy
Livi
ng A
dvic
ew
ww
.nhs
.uk/
livew
ell
Hel
p W
ith
Wei
gh
t Lo
ssW
eigh
t W
atch
ers®
ww
w.w
eigh
twat
cher
s.co
.uk
Tel:
0845
712
300
0
Slim
min
g W
orl
d®
ww
w.s
limm
ingw
orld
.com
Tel:
0844
897
800
0
Way
s To
Get
Act
ive
Cha
nge
4 Li
few
ww
.nhs
.uk/
chan
ge4l
ifeTe
l. 03
00 1
23 4
567
Sto
p S
mo
kin
g S
ervi
ces
ww
w.n
hs.u
k/sm
okef
ree
Alc
oh
olic
s A
no
nym
ou
sw
ww
.alc
ohol
ics-
anon
ymou
s.or
g.uk
Tel.
0845
769
755
5
FRA
NK
, fri
end
ly, c
on
fi d
enti
al d
rug
ad
vice
ww
w.t
alkt
ofra
nk.c
omTe
l: 08
00 7
7 66
00
Insp
ire
ww
w.c
ri.or
g.uk
/insp
ire_n
orth
lanc
s Te
l. 08
458
9417
45
NC
om
pas
s H
ealt
h T
rain
ers
ww
w.n
com
pass
nort
hwes
t.co
.uk
Tel.
0125
3 36
2140
Y-A
ctiv
ew
ww
.ym
caya
ctiv
e.or
g Te
l. 01
253
7715
05
48
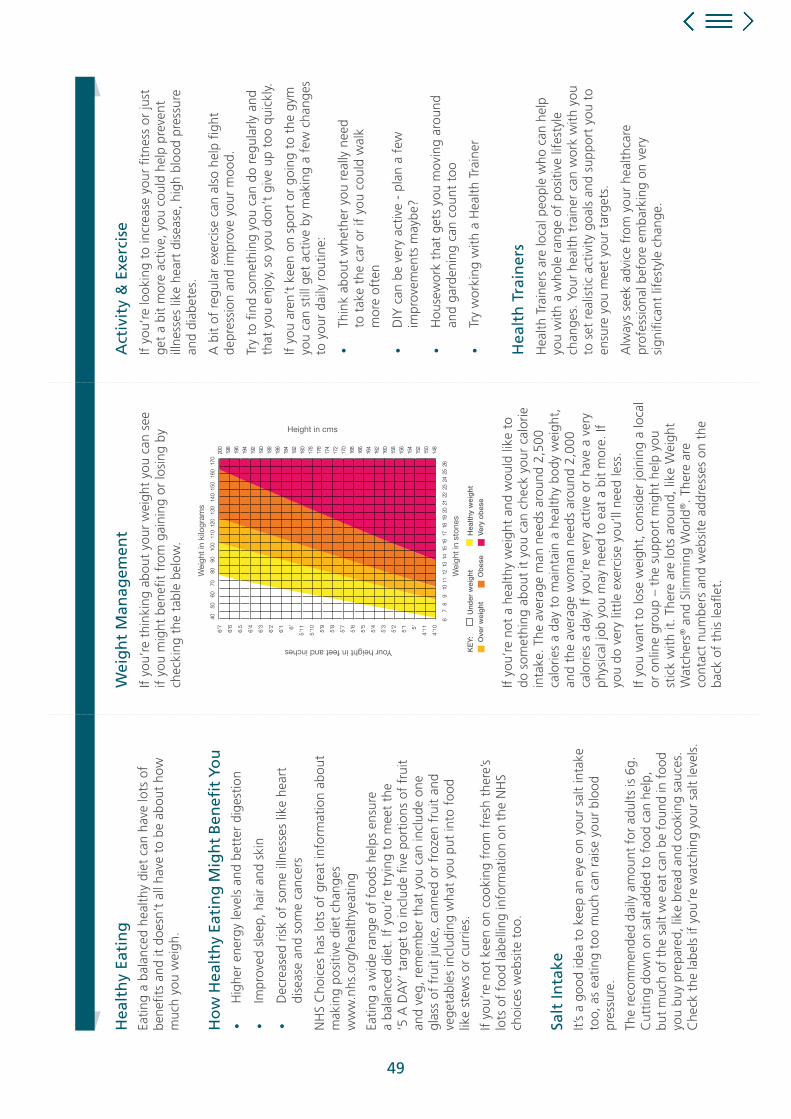
Hea
lth
y Ea
tin
gEa
ting
a ba
lanc
ed h
ealth
y di
et c
an h
ave
lots
of
bene
fi ts
and
it do
esn’
t al
l hav
e to
be
abou
t ho
w
muc
h yo
u w
eigh
.
Ho
w H
ealt
hy
Eati
ng
Mig
ht
Ben
efi t
Yo
u•
Hig
her
ener
gy le
vels
and
bet
ter
dige
stio
n
• Im
prov
ed s
leep
, hai
r an
d sk
in
• D
ecre
ased
ris
k of
som
e ill
ness
es li
ke h
eart
di
seas
e an
d so
me
canc
ers
NH
S C
hoic
es h
as lo
ts o
f gr
eat
info
rmat
ion
abou
t m
akin
g po
sitiv
e di
et c
hang
es
ww
w.n
hs.o
rg/h
ealth
yeat
ing
Eatin
g a
wid
e ra
nge
of f
oods
hel
ps e
nsur
e a
bala
nced
die
t. If
you
’re
tryi
ng t
o m
eet
the
‘5 A
DA
Y’ t
arge
t to
incl
ude
fi ve
port
ions
of
frui
t an
d ve
g, r
emem
ber
that
you
can
incl
ude
one
glas
s of
fru
it ju
ice,
can
ned
or f
roze
n fr
uit
and
vege
tabl
es in
clud
ing
wha
t yo
u pu
t in
to f
ood
like
stew
s or
cur
ries.
If yo
u’re
not
kee
n on
coo
king
fr o
m f
resh
the
re’s
lots
of
food
labe
lling
info
rmat
ion
on t
he N
HS
choi
ces
web
site
too
.
Salt
Inta
keIt’
s a
good
idea
to
keep
an
eye
on y
our
salt
inta
ke
too,
as
eatin
g to
o m
uch
can
rais
e yo
ur b
lood
pr
essu
re.
The
r eco
mm
ende
d da
ily a
mou
nt f
or a
dults
is 6
g.
Cut
ting
dow
n on
sal
t ad
ded
to f
ood
can
help
, bu
t m
uch
of t
he s
alt
we
eat
can
be f
ound
in f
ood
you
buy
prep
ared
, lik
e br
ead
and
cook
ing
sauc
es.
Che
ck t
he la
bels
if y
ou’r
e w
atch
ing
your
sal
t le
vels
.
Act
ivit
y &
Exe
rcis
eIf
you’
re lo
okin
g to
incr
ease
you
r fi t
ness
or
just
ge
t a
bit
mor
e ac
tive,
you
cou
ld h
elp
prev
ent
illne
sses
like
hea
rt d
isea
se, h
igh
bloo
d pr
essu
re
and
diab
etes
.
A b
it of
reg
ular
exe
rcis
e ca
n al
so h
elp
fi ght
de
pres
sion
and
impr
ove
your
moo
d.
Try
to fi
nd s
omet
hing
you
can
do
regu
larly
and
th
at y
ou e
njoy
, so
you
don’
t gi
ve u
p to
o qu
ickl
y.
If yo
u ar
en’t
kee
n on
spo
rt o
r go
ing
to t
he g
ym
you
can
still
get
act
ive
by m
akin
g a
few
cha
nges
to
you
r da
ily r
outin
e:
• Th
ink
abou
t w
heth
er y
ou r
eally
nee
d to
tak
e th
e ca
r or
if y
ou c
ould
wal
k m
ore
ofte
n
• D
IY c
an b
e ve
ry a
ctiv
e -
plan
a f
ew
impr
ovem
ents
may
be?
• H
ouse
wor
k th
at g
ets
you
mov
ing
arou
nd
and
gard
enin
g ca
n co
unt
too
• Tr
y w
orki
ng w
ith a
Hea
lth T
rain
er
Hea
lth
Tra
iner
sH
ealth
Tra
iner
s ar
e lo
cal p
eopl
e w
ho c
an h
elp
you
with
a w
hole
ran
ge o
f po
sitiv
e lif
esty
le
chan
ges.
You
r he
alth
tra
iner
can
wor
k w
ith y
ou
to s
et r
ealis
tic a
ctiv
ity g
oals
and
sup
port
you
to
ensu
re y
ou m
eet
your
tar
gets
.
Alw
ays
seek
adv
ice
from
you
r he
alth
care
pr
ofes
sion
al b
efor
e em
bark
ing
on v
ery
sign
ifi ca
nt li
fest
yle
chan
ge.
Wei
gh
t M
anag
emen
tIf
you’
re t
hink
ing
abou
t yo
ur w
eigh
t yo
u ca
n se
e if
you
mig
ht b
enefi
t f
rom
gai
ning
or
losi
ng b
y ch
ecki
ng t
he t
able
bel
ow.
If yo
u’re
not
a h
ealth
y w
eigh
t an
d w
ould
like
to
do s
omet
hing
abo
ut it
you
can
che
ck y
our
calo
rie
inta
ke. T
he a
vera
ge m
an n
eeds
aro
und
2,50
0 ca
lorie
s a
day
to m
aint
ain
a he
alth
y bo
dy w
eigh
t,
and
the
aver
age
wom
an n
eeds
aro
und
2,00
0 ca
lorie
s a
day.
If y
ou’r
e ve
ry a
ctiv
e or
hav
e a
very
ph
ysic
al jo
b yo
u m
ay n
eed
to e
at a
bit
mor
e. If
yo
u do
ver
y lit
tle e
xerc
ise
you’
ll ne
ed le
ss.
If yo
u w
ant
to lo
se w
eigh
t, c
onsi
der
join
ing
a lo
cal
or o
nlin
e gr
oup
– th
e su
ppor
t m
ight
hel
p yo
u st
ick
with
it. T
here
are
lots
aro
und,
like
Wei
ght
Wat
cher
s® a
nd S
limm
ing
Wor
ld®. T
here
are
co
ntac
t nu
mbe
rs a
nd w
ebsi
te a
ddre
sses
on
the
back
of
this
leafl
et.
Yo
ur w
eigh
t in
kilo
gram
s
Your
wei
ght
in s
tone
s
KE
Y:
Und
er w
eig
ht
Hea
lthy
wei
ght
O
ver
wei
ght
O
bes
e
Ver
y o
bes
e
Your height in centimetres
Your height in feet and inches
Wei
ght
in k
ilogr
ams
Wei
ght
in s
tone
s
Height in cms
6’7
6’6
6.5
6’4
6’3
6’2
6’1 6’
5’11
5’10 5’9
5’8
5’7
5’6
5’5
5’4
5’3
5’2
5’1 5’
4’11
4’10
49

50
Notes

51
Notes
52
Notes

Date of preparation: April 2015 UK/G-NHS/1114/0058ac
This material is not approved for use for projects with RB (ie. MEGS/Joint working)
ARM and the Medicines Optimisation Academy are non-promotional education programmes designed by RB UK to improve patient care and support healthcare professional.
53