




Matteo Lambertini, MDESMO Fellow
Institut Jules Bordet, Brussels (Belgium)
Physicians Attitudes and Knowledge about Fertility Preservation
Lugano, SwitzerlandOctober 7, 2018Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO

Disclosure InformationRelationship Relevant to this Session
Lambertini, Matteo:
• Consultant or advisor: Teva
• Honoraria: Theramex
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
Outline• Introduction
• Attitudes and knowledge about:
– Embryo/oocyte cryopreservation
– Cryopreservation of ovarian tissue
– Temporary ovarian suppression with GnRHa duringchemotherapy
• Attitudes and knowledge about fertility preservation in advanced breast cancer
• Conclusions
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO

Outline• Introduction
• Attitudes and knowledge about:
– Embryo/oocyte cryopreservation
– Cryopreservation of ovarian tissue
– Temporary ovarian suppression with GnRHa duringchemotherapy
• Attitudes and knowledge about fertility preservation in advanced breast cancer
• Conclusions
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
“Fertility and pregnancy-related issues are one of the five priority areas of concern for
young women with breast cancer”
Fertility and Pregnancy-related Issues: Young Women Advocates Statement
Paluch-Shimon S et al, Breast 2017;35:203-17
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO

Peccatori F et al, Ann Oncol 2013;24:vi160-70. Oktay K et al, J Clin Oncol 2018;36(19):1994-2001
ESMO GUIDELINES 2013
ASCO GUIDELINES 2018
Oncofertility Counseling is Mandatory As soon as Possible after Diagnosis
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
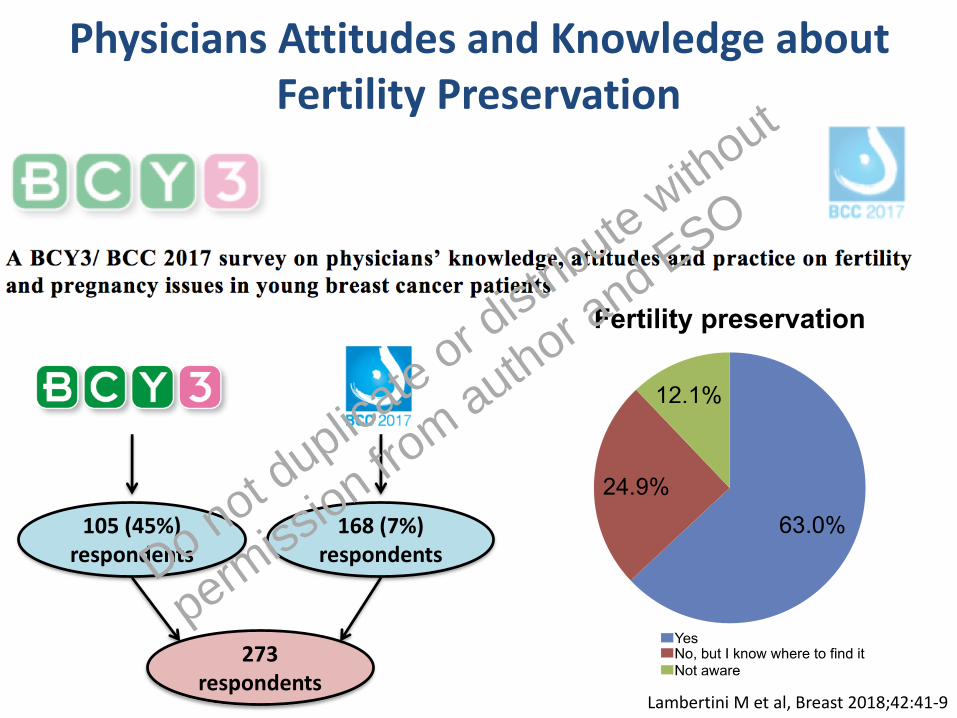
Lambertini M et al, Breast 2018;42:41-9
105 (45%) respondents
168 (7%) respondents
273 respondents
1
A BCY3/ BCC 2017 survey on physicians’ knowledge, attitudes and practice on fertility and pregnancy issues in young breast cancer patients
1) Demographic, medical training and background information (Q1-Q10)
Q1. Age
· _________ years
Q2. Gender
· Male
· Female
Q3. What is your country of practice?
· ____________________
Q4. What is your religion?
· Catholic
· Protestant (Anglican, Methodist etc)
· Muslim
· Hindu
· Jewish
· Atheist/none
· Other, please specify: ____________________
· I prefer to not answer
Q5. Do you have children or have currently parenthood project?
· Yes
· No
Q6. What is your speciality? (Please check all that apply)
· Medical oncology
· Radiation oncology
· Surgical oncology
· Other, please specify: ____________________
Q7. What is your clinical practice environment?
· Academic
· Private
· Both (academic and private)
· Other, please specify: ____________________
Q8. How many years of clinical practice (including your MD specialisation) do you have?
· _________ years
1
A BCY3/ BCC 2017 survey on physicians’ knowledge, attitudes and practice on fertility and pregnancy issues in young breast cancer patients
1) Demographic, medical training and background information (Q1-Q10)
Q1. Age
· _________ years
Q2. Gender
· Male
· Female
Q3. What is your country of practice?
· ____________________
Q4. What is your religion?
· Catholic
· Protestant (Anglican, Methodist etc)
· Muslim
· Hindu
· Jewish
· Atheist/none
· Other, please specify: ____________________
· I prefer to not answer
Q5. Do you have children or have currently parenthood project?
· Yes
· No
Q6. What is your speciality? (Please check all that apply)
· Medical oncology
· Radiation oncology
· Surgical oncology
· Other, please specify: ____________________
Q7. What is your clinical practice environment?
· Academic
· Private
· Both (academic and private)
· Other, please specify: ____________________
Q8. How many years of clinical practice (including your MD specialisation) do you have?
· _________ years
Physicians Attitudes and Knowledge about Fertility Preservation
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
Outline• Introduction
• Attitudes and knowledge about:
– Embryo/oocyte cryopreservation
– Cryopreservation of ovarian tissue
– Temporary ovarian suppression with GnRHa duringchemotherapy
• Attitudes and knowledge about fertility preservation in advanced breast cancer
• Conclusions
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO

Donnez J & Dolmans MM, N Engl J Med 2017;377(17):1657-65Peccatori F et al, Ann Oncol 2013;24:vi160-70. Oktay K et al, J Clin Oncol 2018;36(19):1994-2001
Embryo/Oocyte CryopreservationAvailable Guidelines
Guidelines Year Recommendations
ESMO 2013 Embryo or oocyte cryopreservation is the main method to preserve female fertility. Ovarian stimulation should be carried out before commencing chemotherapy.
ASCO 2018 Embryo cryopreservation is an established fertility preservation method, and it has routinely been used for storing surplus embryos after in vitro fertilization.Cryopreservation of unfertilized oocytes is an option, and may be especially well suited to women who do not have a male partner, do not wish to use donor sperm, or have religious or ethical objections to embryo freezing.Do not duplica
te or distr
ibute without
permiss
ion from author a
nd ESO
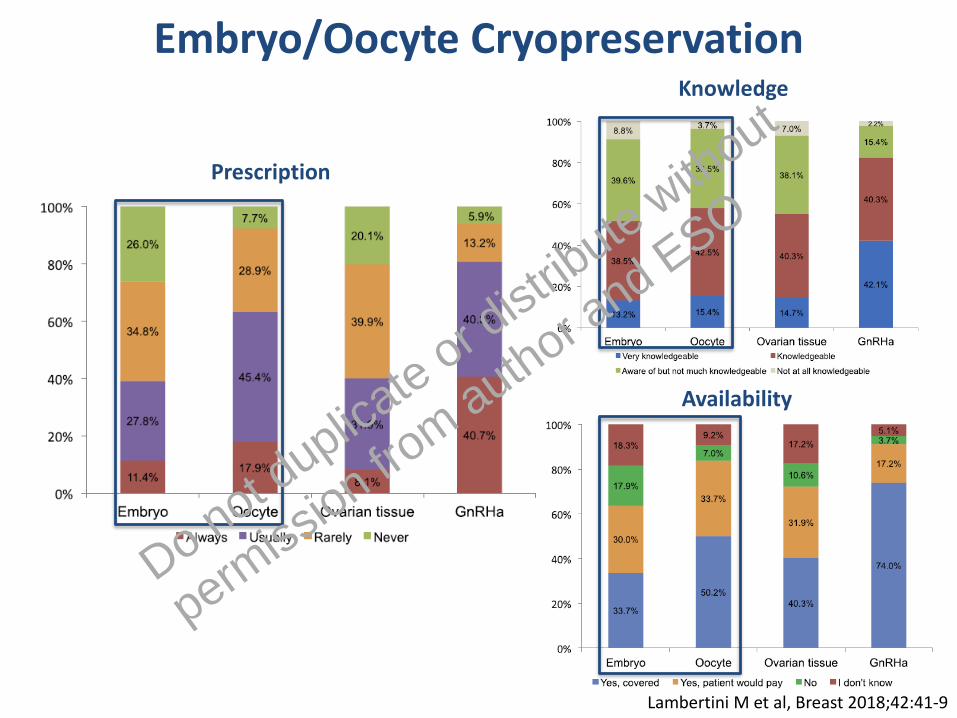
Embryo/Oocyte Cryopreservation
Prescription
Knowledge
Availability
Lambertini M et al, Breast 2018;42:41-9
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO

Embryo/Oocyte Cryopreservation: Efficacy Data
Oktay K et al, J Clin Oncol 2015;33(22):2424-9. Diaz-Garcia C et al, Fertil Steril 2018;109(3):478-85
Ooctye cryopreservationProspective multicenter cohort study
n=618 breast cancer patients
Embryo cryopreservation Prospective single-center cohort study
n=131 breast cancer patients
Pregnancy rate = 20/33 (61%) Pregnancy rate = 13/38 (34%)
33/131 (25%)
38/618 (6%)
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
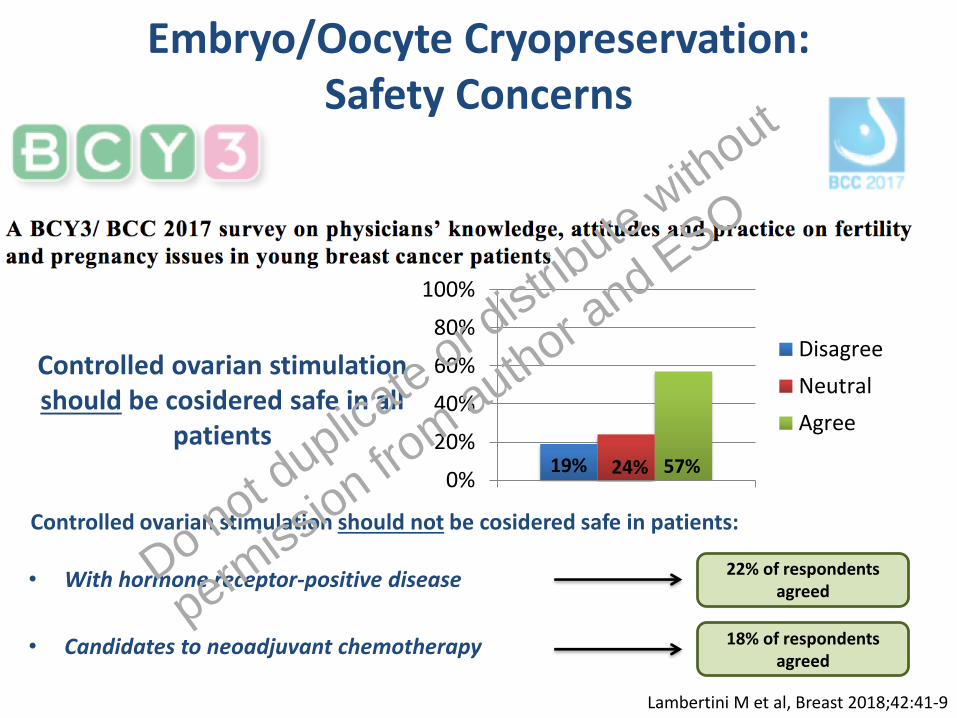
Controlled ovarian stimulation should be cosidered safe in all
patients
0%
20%
40%
60%
80%
100%
Disagree
Neutral
Agree
19% 24% 57%
Embryo/Oocyte Cryopreservation: Safety Concerns
Lambertini M et al, Breast 2018;42:41-9
Controlled ovarian stimulation should not be cosidered safe in patients:
• With hormone receptor-positive disease
• Candidates to neoadjuvant chemotherapy
22% of respondents agreed
18% of respondents agreed
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
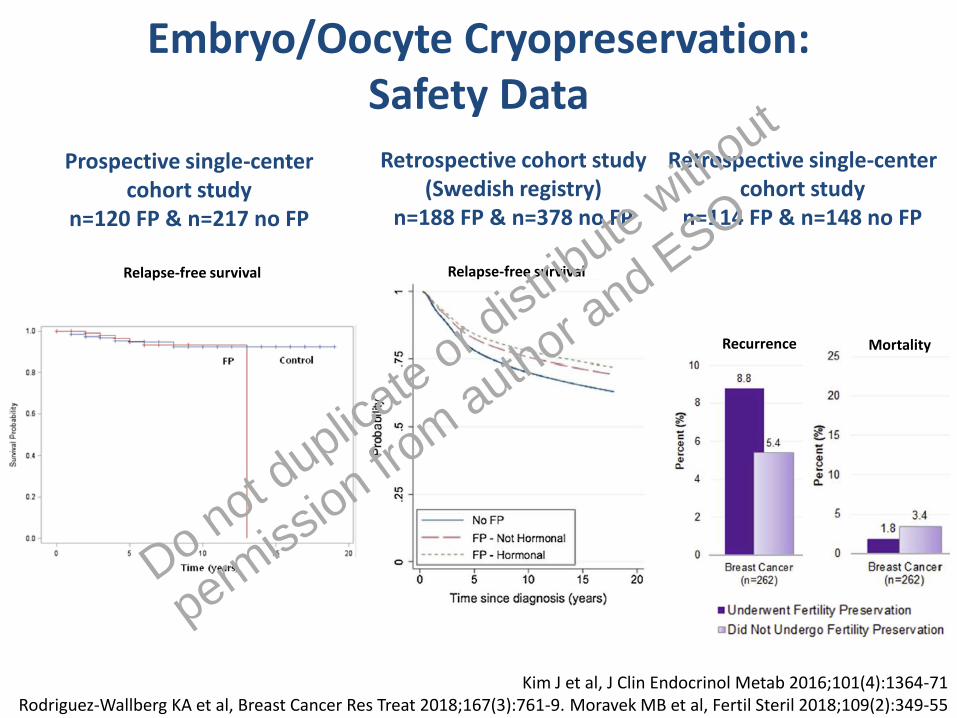
Embryo/Oocyte Cryopreservation: Safety Data
Kim J et al, J Clin Endocrinol Metab 2016;101(4):1364-71 Rodriguez-Wallberg KA et al, Breast Cancer Res Treat 2018;167(3):761-9. Moravek MB et al, Fertil Steril 2018;109(2):349-55
MortalityRecurrence
Retrospective single-center cohort study
n=114 FP & n=148 no FP
Retrospective cohort study (Swedish registry)
n=188 FP & n=378 no FP
Relapse-free survival
Prospective single-center cohort study
n=120 FP & n=217 no FP
Relapse-free survival
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO

Embryo/Oocyte Cryopreservation: Safety Data
Hormone-receptor status Timing of chemotherapy administration
Kim J et al, J Clin Endocrinol Metab 2016;101(4):1364-71. Meirow D et al, Fertil Steril 2014;102(2):488-95. Oktay K et al, J Clin Oncol 2015;33(22):2424-9. Letourneau JM et al, Hum Reprod 2017;32(10):2123-9. Chien AJ et al, BCRT 2017;165(1):151-9
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO

Outline• Introduction
• Attitudes and knowledge about:
– Embryo/oocyte cryopreservation
– Cryopreservation of ovarian tissue
– Temporary ovarian suppression with GnRHa duringchemotherapy
• Attitudes and knowledge about fertility preservation in advanced breast cancer
• Conclusions
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
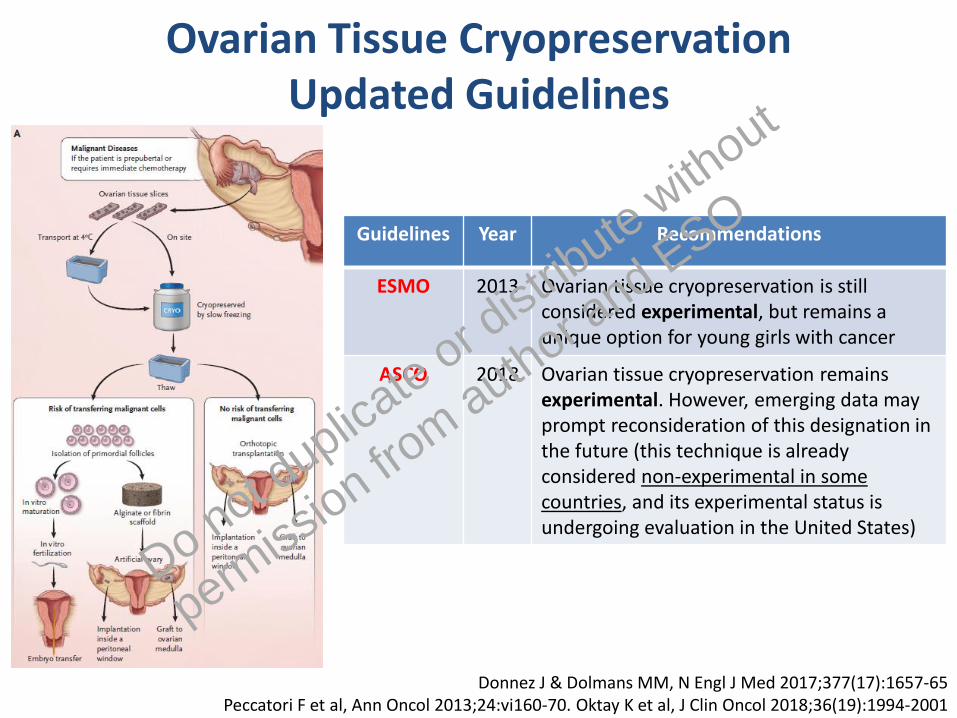
Ovarian Tissue CryopreservationUpdated Guidelines
Guidelines Year Recommendations
ESMO 2013 Ovarian tissue cryopreservation is still considered experimental, but remains a unique option for young girls with cancer
ASCO 2018 Ovarian tissue cryopreservation remains experimental. However, emerging data may prompt reconsideration of this designation in the future (this technique is already considered non-experimental in some countries, and its experimental status is undergoing evaluation in the United States)
Donnez J & Dolmans MM, N Engl J Med 2017;377(17):1657-65Peccatori F et al, Ann Oncol 2013;24:vi160-70. Oktay K et al, J Clin Oncol 2018;36(19):1994-2001
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO

Ovarian Tissue Cryopreservation
Prescription
Knowledge
Availability
Lambertini M et al, Breast 2018;42:41-9
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
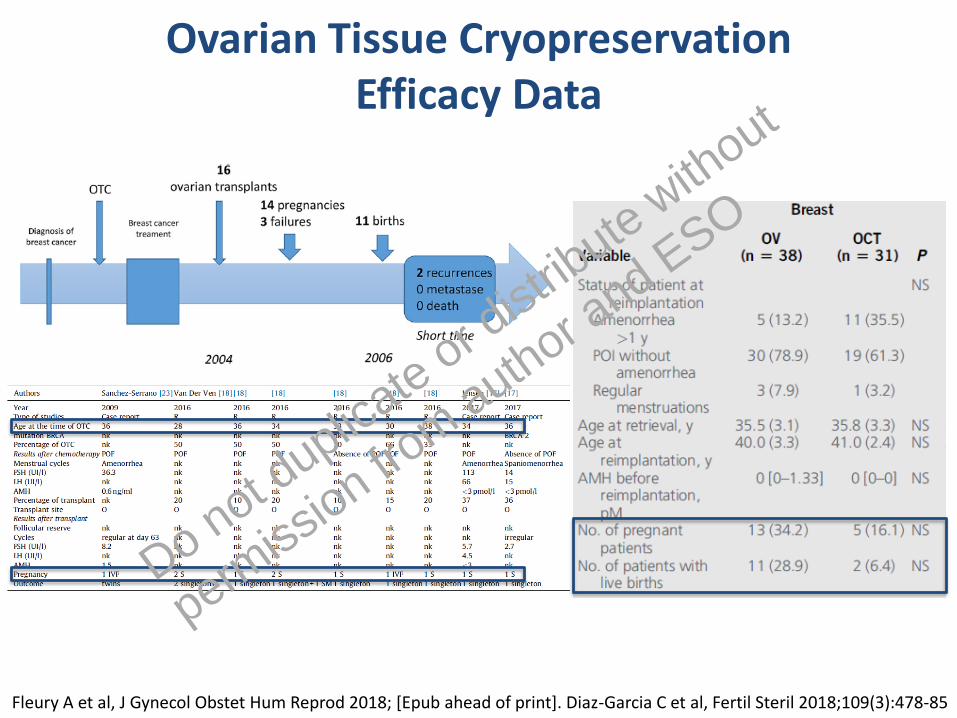
Ovarian Tissue CryopreservationEfficacy Data
Fleury A et al, J Gynecol Obstet Hum Reprod 2018; [Epub ahead of print]. Diaz-Garcia C et al, Fertil Steril 2018;109(3):478-85
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO

Ovarian Tissue CryopreservationSafety Data
Fleury A et al, J Gynecol Obstet Hum Reprod 2018; [Epub ahead of print]
Risk of malignant contamination appears to be low in breast cancer patients
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO

Outline• Introduction
• Attitudes and knowledge about:
– Embryo/oocyte cryopreservation
– Cryopreservation of ovarian tissue
– Temporary ovarian suppression with GnRHa duringchemotherapy
• Attitudes and knowledge about fertility preservation in advanced breast cancer
• Conclusions
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO

Ovarian Suppression with GnRHa during CTUpdated Guidelines
Paluch-Shimon S et al, Breast 2017;35:203-17. Lambertini M et al, Eur J Cancer 2017;71:25-33Oktay K et al, J Clin Oncol 2018;36(19):1994-2001
Guidelines Year Recommendations
ESO-ESMO BCY3 2017 GnRHa should be discussed as an option with all patients interested in potentially preserving fertility and/or ovarian function who are candidates for chemotherapy, irrespective of tumor subtype
AIOM 2017 GnRHa during chemotherapy should be recommended to all pre-menopausal breast cancer patients undergoing chemotherapy who are interested in ovarian function and/or fertility preservation
ASCO 2018 When proven fertility preservation methods are not feasible, and in the setting of young women with breast cancer, GnRHa may be offered to patients in the hope of reducing the likelihood of chemotherapy-induced ovarian insufficiency. GnRHa should not be used in place of proven fertility preservation methods.
Updated ESMO and ESHRE guidelines are upcoming
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO

Ovarian Suppression with GnRHa during CT
Prescription
Knowledge
Availability
Lambertini M et al, Breast 2018;42:41-9
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
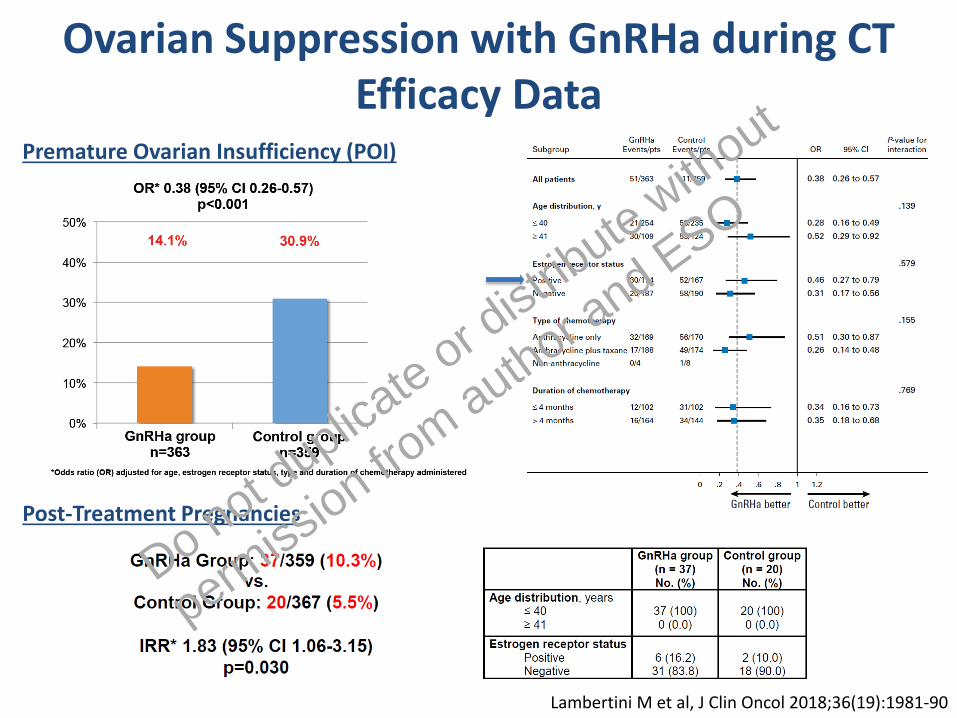
Ovarian Suppression with GnRHa during CTEfficacy Data
Lambertini M et al, J Clin Oncol 2018;36(19):1981-90
Premature Ovarian Insufficiency (POI)
Post-Treatment Pregnancies
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO

Ovarian Suppression with GnRHa during CTSafety Data
Lambertini M et al, J Clin Oncol 2018;36(19):1981-90
ER+
ER-
Disease-Free Survival Overall Survival
HR 1.17; 95% CI 0.62-2.20 HR 0.79; 95% CI 0.24-2.59
HR 0.95; 95% CI 0.64-1.42 HR 0.65; 95% CI 0.39-1.07
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO

Outline• Introduction
• Attitudes and knowledge about:
– Embryo/oocyte cryopreservation
– Cryopreservation of ovarian tissue
– Temporary ovarian suppression with GnRHa duringchemotherapy
• Attitudes and knowledge about fertility preservation in advanced breast cancer
• Conclusions
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
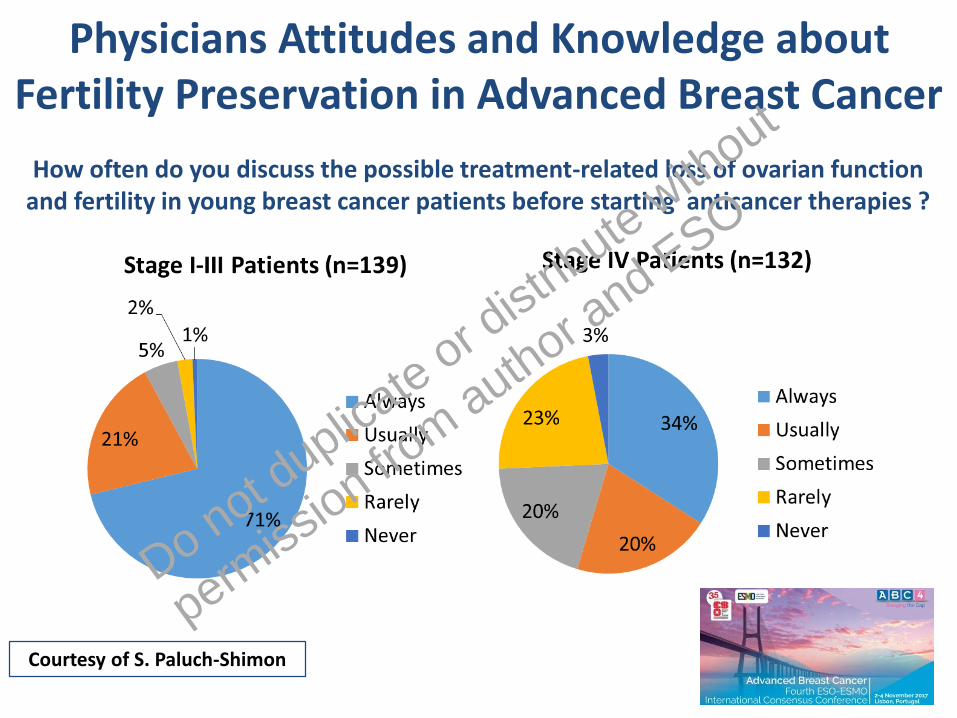
Physicians Attitudes and Knowledge about Fertility Preservation in Advanced Breast Cancer
How often do you discuss the possible treatment-related loss of ovarian function and fertility in young breast cancer patients before starting anticancer therapies ?
Courtesy of S. Paluch-Shimon
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
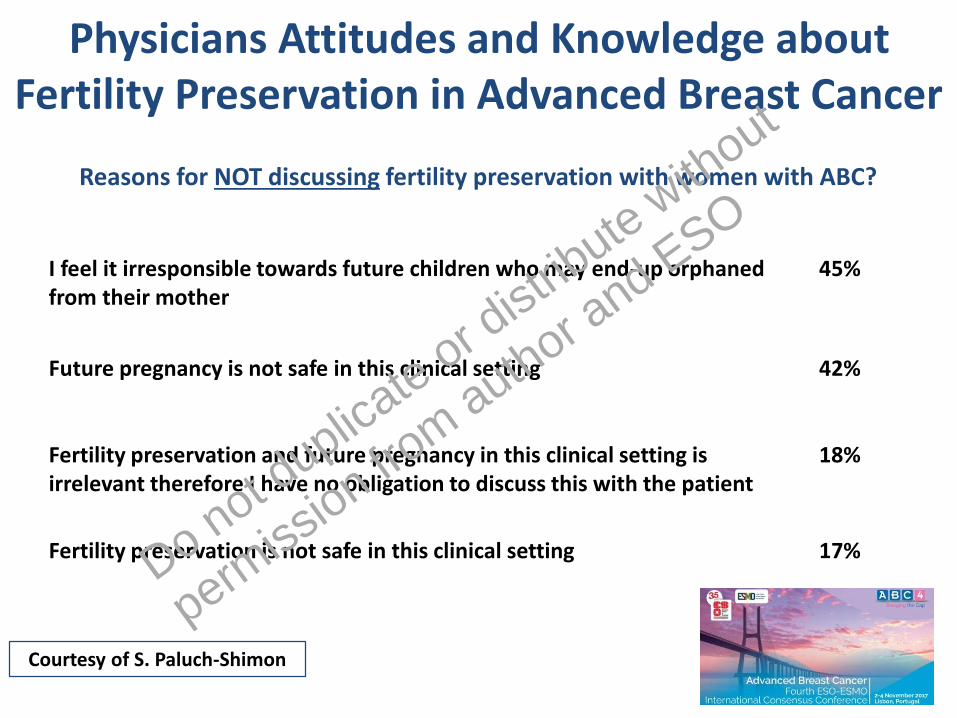
Physicians Attitudes and Knowledge about Fertility Preservation in Advanced Breast Cancer
Courtesy of S. Paluch-Shimon
I feel it irresponsible towards future children who may end-up orphaned from their mother
45%
Future pregnancy is not safe in this clinical setting 42%
Fertility preservation and future pregnancy in this clinical setting is irrelevant therefore I have no obligation to discuss this with the patient
18%
Fertility preservation is not safe in this clinical setting 17%
Reasons for NOT discussing fertility preservation with women with ABC?
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
Fertility Preservation in Advanced Breast CancerCurrent Recent Guidelines
Cardoso F et al, Ann Oncol 2018;29(8):1634-57
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO
Outline• Introduction
• Attitudes and knowledge about:
– Embryo/oocyte cryopreservation
– Cryopreservation of ovarian tissue
– Temporary ovarian suppression with GnRHa duringchemotherapy
• Attitudes and knowledge about fertility preservation in advanced breast cancer
• Conclusions
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO

• Fertility preservation and pregnancy-related issues are priority areas of concern for young breast cancer patients
• As early as possible after diagnosis, a proper oncofertility counseling is mandatory to inform all women irrespectively of the stage of their disease
• Embryo/oocyte cryopreservation are standard options for fertility preservation
• Ovarian tissue cryopreservation remains experimental in most of the countries but may be discussed in specific circumstances
• Temporary ovarian suppression with GnRHa during chemotherapy should now be considered an available option to preserve ovarian function and potential fertility in young breast cancer patients (but not an alternative to cryopreservation techniques)
• Improving physicians awareness and education in this field is crucial as well as strengthening the collaboration between oncologists and fertility specialists
Conclusions
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO

Institut Jules BordetAhmad AwadaMartine PiccartChristos SotiriouFrederic HenotBastien NguyenGiulia Viglietti
Evandro de AzambujaMichail IgnatiadisNoam F. PondeSamuel MartelChristian MaurerFrancois Richard
San Martino – IST HospitalLucia Del MastroFrancesca PoggioAlessia Levaggi
Paola AnseriniMaria Carolina PescioChiara Dellepiane
Istituto Europeo di OncologiaFedro A. Peccatori
American University of BeirutHatem A. Azim Jr.
Dana-Farber Cancer Institute
@matteolambe
Erasme HospitalIsabelle DemeestereFlorence Horicks
Oranite GoldratMargherita Condorelli
Breast International GroupDebora Fumagalli
Ann H. Partridge Philip Poorvu
Zambrano Hellion HospitalCynthia Villarreal-Garza
Shaare Zedek Medical CentreShani Paluch-Shimon
Do not duplicate or d
istribute without
permiss
ion from author a
nd ESO





























