PHARMACOTHERAPY OF HIV MANAGEMENT
Dr. Sourav ChakrabartyPost-graduate trainee
Department of Pharmacology

Overview• Introduction• HIV virus• Pathophysiology of AIDS• Anti-retroviral drugs• Principles of anti-HIV chemotherapy• WHO 2013 guideline• Conclusion

Introduction• HIV/ AIDS- a global threat to mankind
• 33 millions of HIV infected worldwide
• Cripples immune system, affects CNS, Kidney, vascular system, mucosa.
• Still no cure, • No vaccine

HIV virus

Life cycle of HIV virus

History of natural disease

Acquired Immune Deficiency Syndrome
• Two parameters:1. Clinical conditions 2. CD4+ T lymphocyte count at blood
• AIDS- if one or more specific opportunistic illness has been diagnosed OR CD4 T+ Lymphocyte <200/µl

Conditions defining AIDS

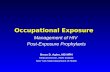
Anti-retroviral drugs- sites of action

History of anti-retroviral drugs
• Zidovudine – synthesized in 1964 Anti-HIV activity- 1985
• Saquinavir – 1995
• NNRTI- 1998
• Raltegravir- 2007

Anti-retroviral drugsNucleoside Reverse Transcriptase Inhibitors(NRTI)
Zidovudine (AZT)
Stavudine (d4T)
Tenofovir disoproxil (TDF)
Lamivudine(3TC)
Didanosine (ddl)
Zalcitabine(DDC)
Emtricitabine (FTC)
Abacavir (ABC)
Non-nucleosideReverse Transcriptase Inhibitors(NNRTI)
Nevirapine(NVP)
Delavirdine (DLV)
Efavirenz (EFV)
Etravirine (ETV)

Contd………Protease Inhibitors
Saquinavir (SQV)
Ritonavir (RTV)
Amprenavir (APV)
Atazanavir(ATV)
Indinavir (IDV)
Nelfinavir (NFV)
Lopinavir (LPV/r)
Fosamprenavir (FPV)
Tipranavir (TPV)
Darunavir (DRV)
Entry Inhibitors
Enfuvirtide (T-20)
Maraviroc (MVC)
Integrase Inhibitor
Raltegravir (RAL)

Nucleoside/ Nucleotide Reverse Transcriptase
Inhibitors(NRTI)

Intracellular activation of NRTIs


Zidovudine• Active against HIV 1 & 2, HTLV 1 & 2.• more active in lymphocytes than in
monocyte-macrophage cells• Dose- 300 mg twice a day• Crosses placenta & BBB.• Untoward Effects-1. fatigue, malaise, myalgia, nausea,
anorexia, headache and insomnia.2. Bone marrow suppression3. nail hyperpigmentation, myopathy4. Serious hepatic toxicity

Lamivudine• First line NRTI• manufactured as the pure
2Rcis(−)enantiomer• More active in resting cells• Dose- 300 mg once daily
• Untoward Effects- Neutropenia, headache, and nausea
• caution in using in co-infection with HBV

Tenofovir• only nucleotide analog• Available only as the disoproxil prodrug• Incomplete ribose ring• Dose- 300mg OD
• Untoward Effects-well tolerated, rarely acute renal failure and Fanconi’s syndrome
• Drug interaction with Didanosine

Emtricitabine• chemically related to lamivudine• one of the least toxic anti-retroviral drugs
Abacavir• Dose: 600 mg once daily• eliminated by metabolism by alcohol
dehydrogenase, and by glucuronidation• fatal hypersensitivity syndrome(HLA-
B*5701 genotype)

Didanosine• Dose-200 mg twice daily
• Acid labile, hence needs antacid buffer
• Not well tolerated
• peripheral neuropathy and pancreatitis

Non-Nucleoside Reverse Transcriptase
Inhibitors(NNRTI)• Active against HIV 1 only
• No activity against host cell DNA polymerases.
• 4 agents- Nevirapine/Efavirenz/ Delavirdine/ Etravirine.
• Susceptible to high-level drug resistance
• Cross-resistance

Mechanism of action

Pharmacokinetics

Efavirenz• First line NNRTI
• Once daily dosing
• Highly teratogenic
• Adverse effect- CNS toxicities
• Rash

Nevirapine• First line ART both for active treatment and for PPTCT
• Induces own metabolism
• Untoward Effects- Rash, increased liver enzymes
• Severe & fatal hepatitis in pregnancy.
• PPTCT- A single oral intrapartum dose of 200 mg nevirapine followed by a single dose given to the newborn

HIV Protease Inhibitors• Inhibit virus aspartyl protease
• Highly variable pharmacokinetics
• Metabolised by CYP 3A4
• Potential for metabolic drug interactions
• ADR-nausea, vomiting, and diarrhea

Mechanism of action
The viral maturation is
inhibited
The production of the viral particle is inhibited
Act as protease inhibitor in
which block the action of protease

Pharmacokinetics

Saquinavir• First approved Protease inhibitor• Poor oral bioavailability• Dose- 600 mg TDS
Lopinavir• Active against both HIV-1 and HIV-2• Extensive metabolism by CYP 3A4• lopinavir/ritonavir co-formulation in a fixed 4:1
ratio• ADRs- loose stools, diarrhea, nausea, and
vomiting

Ritonavir• Mostly used as a pharmacokinetic
enhancer (CYP 3A4 inhibitor)• Dose- antiretroviral treatment 600 mg
twice dailyBooster dose-100/ 200 mg once or
twice daily
• ADRs- GI upset, lipodystrophy

Entry Inhibitors• Two drugs- Enfuvirtide and Maraviroc
• gp 41 and CD4 interactions- enfuvirtide
• gp 120 and CCR5 interactions- maraviroc

Maraviroc

Contd……..• Active only against CCR5-tropic strains of
HIV
• Three different starting dose-1. with most CYP3A inhibitors- 150mg BD2. with most CYP3A inducers- 600mg BD3. With other- 300mg BD
• generally well tolerated

Enfuvirtide• only approved parenteral antiretroviral drug
• Evolved first as vaccine• High cost to manufacture
• ADRs- injection-site reactions, lymphadenopathy , pneumonia
• Indication- only in treatment-experienced adults

Mechanism of action

Integrase Inhibitors

GUIDELINES FOR HIGHLY ACTIVE ANTIRETROVIRAL THERAPY (HAART):HOW TO USE THE DRUGS?
Based on:Rapid Advice: antiretroviral therapy for HIV infection in adults and adolescentGuidelines For The Management Of Adult HIV Infection With Antiretroviral Therapyhttp://www.who.int/hiv/pub/arv/rapid_advice_art.pdf

HAART
Highly active antiretroviral therapy (ART) using 3 or more active anti HIV drugs from at least 2 different class with the
aim of achieving durable viral suppression to undetectable levels, the
therapeutic goal under most clinical circumstances.

BEFORE STARTING THE REGIMEN• Past treatment history Any resistance to medications Current CD4 and viral load counts Compliance to medication Pregnancy/lactation Concurrent illness (TB/HBV)• HIV tropism assay

GUIDELINES TO START ART
• Start ART in all individuals with a CD4 < 500/µl
• Priority to severe or advanced HIV disease and CD4 < 350/µl
• ART at any CD4 count in PLHIV Active TB disease HBV co-infection with severe chronic
liver disease HIV nephropathy HIV-positive partners in sero-
discordant couples Pregnant and breastfeeding women Children younger than five years of
age Stage 3 or later in WHO clinical
staging

First-line ARTPreferred first-line regimens
Alternative first-line
RegimensAdults(including pregnant andbreastfeeding women and adults with TB and HBV coinfection) TDF + 3TC (or FTC)
+ EFV
AZT + 3TC + EFVAZT + 3TC + NVPTDF + 3TC (or FTC) + NVP
Adolescents (10 to 19 years) ≥35 kg
AZT + 3TC + EFVAZT + 3TC + NVPTDF + 3TC (or FTC) + NVPABC + 3TC + EFV (or NVP)
Children 3 - 10 years and adolescents <35 kg
ABC + 3TC + EFV
ABC + 3TC + NVPAZT + 3TC + EFVAZT + 3TC + NVPTDF + 3TC (or FTC) + EFVTDF + 3TC (or FTC) + NVP
Children <3 yearsABC orAZT + 3TC + LPV/r
ABC + 3TC + NVPAZT + 3TC + NVP

• People receiving NVP discontinue because of adverse events
• With EFV no increased risk of birth defects compared with other ARV drugs during the first trimester of pregnancy
• TDF/FTC or TDF/3TC are the preferred NRTI backbone for
HIV + HBV HIV with TB and pregnant women. • EFV is the preferred NNRTI for HIV & TB (pharmacological
compatibility with TB drugs) HIV +HBV coinfection (less risk of
hepatic toxicity) and Pregnant women, including first
trimester.

ART for PMTCT

Simplified Infant Prophylaxis doses
Drug Infant age Daily dosing
NVP
Birth to 6 weeks• Birthweight 2000−2499 g• Birthweight ≥2500 g
10 mg once daily15 mg once daily
> 6 weeks to 6 months 20 mg once daily
> 6 months to 9 months 30 mg once daily
> 9 months until breastfeeding ends
40 mg once daily
AZTBirth to 6 weeks• Birthweight 2000−2499 g • Birthweight ≥2500 g
10 mg twice daily15 mg twice daily
If toxicity from NVP requires discontinuation or if NVP is not available,infant 3TC can be substituted.

Timing of ART with TB• ART should be started in all TB patients,
including drug-resistant TB, irrespective of the CD4 count
• ATD should be initiated first, followed by ART as soon as possible within the first 8 weeks of treatment.
• HIV-positive TB patients with profound
immunosuppression (CD4 <50) should receive ART immediately within the first 2 weeks of ATD .
.• Preferred NNRTI is EFV in patients starting
ART while on ATD .

ART FOR HIV/HBV CO-INFECTION
• Start ART in all HIV/HBV co-infected individuals who require treatment for their HBV infection, irrespective of CD4 cell count or WHO clinical stage
• Start tenofovir and lamivudine or emtricitabine (2 NRTIs = BACKBONE) containing antiretroviral regimens in all HIV/HbV co-infected individuals needing treatment

HIV-2 infection• HIV-2 is naturally resistant to NNRTIs
• Treatment-naive people coinfected with HIV-1 and HIV-2 should be treated with three NRTIs TDF + 3TC / FTC + AZT or AZT + 3TC + ABC or a ritonavir-boosted PI plus two NRTIs.
• In PI-based regimen, the preferred option is LPV/r
• SQV/r and DRV/r are alternative boosted-PI options, but they are not available as heat-stable fixed-dose combinations.

WHO definitions of Treatment failure
Failure Definition Comments
Clinical failure
Adults and adolescentsNew or recurrent clinical event indicating severe immunodeficiency (WHO clinical stage 4 condition) after 6 months of effective treatment--------------------------------------------------ChildrenNew or recurrent clinical event indicating advanced or severe immunodeficiency (WHO clinical stage 3 and 4 clinical condition with exception of TB) after 6 months of effective treatment
differentiate from IRIS
For adults, certain WHO clinical stage 3 conditions (PTB and severe bacterial infections) also indicate treatment failure

Immunologicalfailure
Adults and adolescentsCD4 count falls to baseline (orbelow) or Persistent CD4 <100 ------------------------------------------Children < 5 yearsPersistent CD4 <200 or <10% >5 yearsPersistent CD4 <100
Without concomitant or recent infection to cause a transient fall in CD4
Virologicalfailure
Plasma viral load >1000 based on two consecutive viral load measurements after 3 months, withadherence support
Must be on ARTfor at least 6 months before declaring failure

Preferred second-line ART regimens
for adults and adolescents Target population Preferred second-line regimen
Adults andadolescents(≥10 years)
If d4T or AZT was used in first-line ART TDF + 3TC (or FTC) + ATV/r or LPV/r
If TDF was used in first line ART AZT + 3TC + ATV/r or LPV/r
Pregnant women Same regimens recommended for adults and adolescents
HIV and TBCoinfection
If rifabutin is available Standard PI-containing regimens
If rifabutin is not availableSame NRTI plus double-dose LPV/r (ie, LPV/r 800 mg/200 mg ) or standard LPV dose with an adjusted dose of RTV(i.e, LPV/r 400 mg/400 mg )
HIV +HBVcoinfection AZT + TDF + 3TC (or FTC) + (ATV/r or LPV/r)

Third-line regimens• National programs should develop policies for
third-line therapy that consider funding, sustainability and the provision of equitable access to ART
• Third-line regimens should include new drugs likely to have anti HIV activity such as integrase inhibitors (eg. Raltegravir) and second generation NNRTIs (eg. Etravirine) and PIs (eg. Darunavir)
• Patients on a failing second-line regimen with no new antiretroviral options, should continue with a tolerated regimen

52
• All NRTIs**– Lactic acidosis/fatty
liver*– Lipoatrophy (loss of
subcutaneous fat)
• Anemia– Zidovudine (AZT,
ZDV)• Pancreatitis*
– didanosine (ddI)• Neuropathy
– didanosine (ddI)– stavudine (d4T)
*Potentially life-threatening**d4T > ddI, AZT > ABC, TDF, 3TC
Serious Adverse Effects of NRTIs

53
Serious Adverse Effects of NNRTIs
• All NNRTIs–Hepatitis*–Skin rash
• CNS symptoms– efavirenz
• Stevens-Johnson syndrome*– nevirapine
*Potentially life-threatening

54
Serious Adverse Effects of PIs
• All PIs– Insulin resistance hyperglycemia and
diabetes
– Elevated serum lipids
– Abnormal fat accumulation
– Liver toxicity**Potentially life-threatening

Conclusion• HIV replication is controllable
• ART is always lifelong
• Minimum 3 drugs
• Best combination- NRTI+ NRTI+ NNRTI
• NNRTI + PI- Should not be given
• But above all, Prevention from HIV is the best way

VACCINE???IS THERE ANY VACCINE AVAILABLE??
IS IT POSSIBLE TO MANUFACTURE ONE??

THANK YOU