An Update On HIV An Update On HIV Pharmacotherapy Pharmacotherapy Gonzalo M.L. Bearman MD,MPH Gonzalo M.L. Bearman MD,MPH Assistant Professor of Medicine Assistant Professor of Medicine Associate Hospital Epidemiologist Associate Hospital Epidemiologist

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

An Update On HIV An Update On HIV PharmacotherapyPharmacotherapy
Gonzalo M.L. Bearman MD,MPHGonzalo M.L. Bearman MD,MPHAssistant Professor of MedicineAssistant Professor of Medicine
Associate Hospital EpidemiologistAssociate Hospital Epidemiologist

OutlineOutline•• ReviewReview
–– HIV epidemiologyHIV epidemiology–– HIV natural historyHIV natural history–– Viral Dynamic and three compartment model of HIV infectionViral Dynamic and three compartment model of HIV infection
•• Current Current AntiretroviralsAntiretrovirals–– Nucleoside/Nucleotide AnalogsNucleoside/Nucleotide Analogs–– NNRTINNRTI–– PIPI–– Fusion InhibitorsFusion Inhibitors–– Once daily dosingOnce daily dosing
•• Highlight important toxicities and drug interactionsHighlight important toxicities and drug interactions•• DHHS guidelines for the use of DHHS guidelines for the use of antiretroviralsantiretrovirals•• Treatment failureTreatment failure
–– Compliance and barriers to adherenceCompliance and barriers to adherence


Natural History of HIV Infection INatural History of HIV Infection I
PantaleoPantaleo NEJM 1993;328:327NEJM 1993;328:327
Viral Dynamics Viral Dynamics ---- SummarySummary
•• 10 billion new 10 billion new virionsvirions created and created and cleared dailycleared daily
•• 200 million CD4 cells destroyed daily 200 million CD4 cells destroyed daily (twice the rate of replacement by the (twice the rate of replacement by the hematopoietichematopoietic system)system)
Ho et al, Nature 1995;373:123Ho et al, Nature 1995;373:123

MACS cohort, MACS cohort, MellorsMellors,et al. Ann Intern Med 1997;126:946,et al. Ann Intern Med 1997;126:946

Antiretroviral Therapy: 2004Antiretroviral Therapy: 2004
Antiretroviral Drugs: 2004Antiretroviral Drugs: 2004nucleoside nucleoside RTIsRTIs•• zidovudinezidovudine (ZDV)(ZDV)•• didanosinedidanosine ((ddIddI))•• zalcitabinezalcitabine ((ddCddC))•• stavudinestavudine (d4T)(d4T)•• lamivudinelamivudine (3TC)(3TC)•• abacavirabacavir (ABC)(ABC)•• emtricitabineemtricitabine (FTC)(FTC)
NNRTIsNNRTIs•• nevirapinenevirapine (NVP)(NVP)•• delavirdinedelavirdine (DLV)(DLV)•• efavirenzefavirenz (EFV)
nucleotide nucleotide RTIsRTIs•• tenofovirtenofovir (TFV)(TFV)
protease inhibitorsprotease inhibitors•• saquinavirsaquinavir (SQV)(SQV)•• ritonavirritonavir (RTV)(RTV)•• indinavirindinavir (IDV)(IDV)•• nelfinavirnelfinavir (NFV)(NFV)•• amprenaviramprenavir (APV)(APV)•• lopinavirlopinavir/r (LPV/r)/r (LPV/r)•• atazanaviratazanavir (ATV)(ATV)
fusion inhibitorsfusion inhibitors•• enfuvirtideenfuvirtide (T(T--20)
(EFV)20)

Life Cycle of HIVLife Cycle of HIV
DS dna COMPLEX

Life Cycle of HIVLife Cycle of HIV
DS dna COMPLEX
entry inhibitors
reversetranscriptase
inhibitors
proteaseinhibitors

N
N N
NH
NH2
O
HON
N
NNH
O
N
N N
N
NH2
OP
OO
O
OO
O CH3
CH3O
O
OH3C
CH3
N
HN N
NH
O
H2N
HON
N
NN
NH2
HN
N
NH
O
NH2
S
O
HON
NO
NH2
S
O
HON
NO
NH2
F
O
HON
NO
NH2
HN
NH
O
O
CH3
O
HON
HN
OO
H3NCH3
O
HON
HN
OO
CH3CH3
O
O
HON
N
N N
NH2
NH2
adenosine
didanosine (ddI)
tenofovir (TDF)
cytosine
zalcitabine (ddC)
lamivudine (3TC)
emtricitabine (FTC)
guanine
abacavir (ABC)
amdoxovir (DAPD)
thymine
zidovudine (ZDV)
stavudine (d4T)

Nucleoside/tide Analogs: ToxicityNucleoside/tide Analogs: Toxicity•• zidovudinezidovudine –– GI, anemia, GI, anemia, leukopenialeukopenia, , myositismyositis•• didanosinedidanosine –– PN, PN, pancreatitispancreatitis, diarrhea, diarrhea•• zalcitabinezalcitabine –– PN, PN, aphthousaphthous ulcersulcers•• stavudinestavudine –– PNPN•• lamivudinelamivudine, , emtricitabineemtricitabine –– (uncommon)(uncommon)•• abacavirabacavir –– GI, hypersensitivity reaction, rashGI, hypersensitivity reaction, rash•• tenofovirtenofovir –– (uncommon)(uncommon)•• nucleosides as a class nucleosides as a class –– lactic acidosis with lactic acidosis with
hepatic hepatic steatosissteatosisDHHS Guidelines 11/10/03 <www.DHHS Guidelines 11/10/03 <www.aidsinfoaidsinfo..nihnih..govgov>>
Nucleoside/tide Analogs: ToxicityNucleoside/tide Analogs: Toxicity
•• Lactic Acidosis/hepatic Lactic Acidosis/hepatic steatosissteatosis–– Chronic compensated Chronic compensated hyperlactatemiahyperlactatemia–– Incidence of severe, Incidence of severe, decompensated decompensated lactic acidosis lactic acidosis
with with hepatomegaly hepatomegaly and and steatosis steatosis is rareis rare•• 1.3 cases/1,000 person years of NRTI exposure1.3 cases/1,000 person years of NRTI exposure
–– Must correlate blood lactate level with clinical presentationMust correlate blood lactate level with clinical presentation
•• Treatment Treatment –– Cessation of HAARTCessation of HAART–– Supportive managementSupportive management
Newer formulations and once daily Newer formulations and once daily dosing.dosing.•• Didanosine Didanosine ECEC-- once daily dosingonce daily dosing•• Stavudine Stavudine XRXR--once daily dosingonce daily dosing•• LamivudineLamivudine--300 mg 300 mg po qdpo qd•• NevirapineNevirapine--400 mg 400 mg po qdpo qd•• AtazanavirAtazanavir--400mg 400mg po qdpo qd•• TenofovirTenofovir--300 mg 300 mg po qdpo qd•• EmtricitabineEmtricitabine-- 200mg 200mg po qdpo qd
New nucleoside RTINew nucleoside RTI
•• EmtricitabineEmtricitabine ((EmtrivaEmtriva))–– One Capsule, Once daily One Capsule, Once daily
•• 200mg 200mg po qdpo qd–– Chemically structure similar to Chemically structure similar to Epivir Epivir (3TC)(3TC)
•• Clinical trials suggest that efficacy is similar to Clinical trials suggest that efficacy is similar to Epivir Epivir in in treatment naive patientstreatment naive patients
–– Likely not effective on Likely not effective on lamivudine lamivudine resistant virusresistant virus
•• Clinical activity against hepatitis B virus.Clinical activity against hepatitis B virus.–– Common side effects include headache, diarrhea, Common side effects include headache, diarrhea,
nausea and rashnausea and rash

Nucleoside/tide Analogs: Nucleoside/tide Analogs: Selected Drug InteractionsSelected Drug Interactions•• ZDV and ZDV and ganciclovirganciclovir: : leukopenialeukopenia•• ZDV and ZDV and ribavirinribavirin: antagonism : antagonism in vitroin vitro•• ZDV and d4T: antagonism, decreased CDZDV and d4T: antagonism, decreased CD44
•• ddIddI, , ddCddC, d4T: PN, d4T: PN--causing agentscausing agents•• ddIddI and other and other pancreatitispancreatitis--causing agentscausing agents•• ddIddI and d4T: methadone decreases levelsand d4T: methadone decreases levels•• ddIddI and and tenofovirtenofovir: increased : increased ddIddI levelslevels•• tenofovirtenofovir and and atazanaviratazanavir: decreased : decreased atazanaviratazanavir levels levels
must ‘boost’ 300mg ofmust ‘boost’ 300mg of atazanaviratazanavir with 100mg of with 100mg of ritonavirritonavir
DHHS Guidelines 11/10/03 <www.DHHS Guidelines 11/10/03 <www.aidsinfoaidsinfo..nihnih..govgov>>

Structures of NNRTI Structures of NNRTI -- NVP, DLV, EFVNVP, DLV, EFV
efavirenz (EFV)nevirapine (NVP)
delavirdine (DLV)

NNRTI: ToxicityNNRTI: Toxicity•• RashRash
–– Majority are mild to moderate in severity, Majority are mild to moderate in severity, occuring occuring within within the first several weeks of therapythe first several weeks of therapy
–– Most are confined to Most are confined to cutaneous cutaneous reactions onlyreactions only-- do not do not involve mucous membranes.involve mucous membranes.
–– NVP 7%, DLV 4%, EFV 2% require discontinuationNVP 7%, DLV 4%, EFV 2% require discontinuation–– StevensStevens--Johnson syndrome reportedJohnson syndrome reported
•• Hepatic Hepatic transaminasetransaminase elevations elevations –– NVP (EFV, DLV)NVP (EFV, DLV)–– Nevirapine Nevirapine 400mg 400mg po qdpo qd
•• Greater incidence of Greater incidence of hepatoxicity hepatoxicity than 200 mg than 200 mg po po bid dosingbid dosing
•• CNS symptoms (~50%) CNS symptoms (~50%) ---- EFVEFV•• TeratogenicityTeratogenicity in monkeys in monkeys ---- EFVEFV
DHHS Guidelines 11/10/03 <www.DHHS Guidelines 11/10/03 <www.aidsinfoaidsinfo..nihnih..govgov>>

NNRTI: NNRTI: Selected Drug InteractionsSelected Drug Interactions•• CYP 3A4 effects (NVP + EFV inducers; DLV CYP 3A4 effects (NVP + EFV inducers; DLV
inhibitor): inhibitor): rifampinrifampin/(/(rifabutinrifabutin), ), ketoconazoleketoconazole, , anticonvulsants, anticonvulsants, simvastatinsimvastatin//lovastatinlovastatin, , astemizoleastemizole//tefenadinetefenadine, , midazolammidazolam//triazolamtriazolam, , ergotaminesergotamines
•• NVP, EFV decrease methadone levelsNVP, EFV decrease methadone levels•• NNRTINNRTI--PI interactionsPI interactions
–– NVP decreases SQV, IDV, LPV NVP decreases SQV, IDV, LPV –– DLV increases SQV, IDVDLV increases SQV, IDV–– EFV decreases SQV, IDV, APV, LPVEFV decreases SQV, IDV, APV, LPV–– Efavirenz Efavirenz decreases decreases atazanaviratazanavir: must ‘boost’ 300mg of : must ‘boost’ 300mg of
atazanavir atazanavir with 100mg of with 100mg of ritonavirritonavir
DHHS Guidelines 11/10/03 <www.DHHS Guidelines 11/10/03 <www.aidsinfoaidsinfo..nihnih..govgov>>



HIV Protease Inhibitors (2)HIV Protease Inhibitors (2)
amprenavir (APV) lopinavir (LPV)
atazanavir (ATV)

PI: ToxicityPI: Toxicity
•• SQV: GISQV: GI•• RTV: GI, RTV: GI, circumoralcircumoral paresthesiasparesthesias•• IDV: IDV: nephrolithiasisnephrolithiasis, incr. indirect , incr. indirect bilirubinbilirubin•• NFV: diarrheaNFV: diarrhea•• APV: GI, rashAPV: GI, rash•• LPV: GI, diarrheaLPV: GI, diarrhea•• ATV: increased indirect ATV: increased indirect bilirubinbilirubin•• PIs as a class: increased hepatic PIs as a class: increased hepatic transaminasestransaminases, ,
hyperglycemia, hyperglycemia, lipodystrophylipodystrophy and and lipidemialipidemia, , increased bleeding in hemophiliacsincreased bleeding in hemophiliacs
DHHS Guidelines 11/10/03 <www.DHHS Guidelines 11/10/03 <www.aidsinfoaidsinfo..nihnih..govgov>>

New PI formulation: New PI formulation: fosamprenavirfosamprenavir
•• LexivaLexiva: : fosamprenavirfosamprenavir–– ‘‘prodrug’ prodrug’ of of ageneraseagenerase ((amprenaviramprenavir))–– Likely will not be effective in patients who are Likely will not be effective in patients who are
resistant to resistant to ageneraseagenerase–– For PI experienced patientFor PI experienced patient
•• 700 mg 700 mg fosamprenavirfosamprenavir and 100mg and 100mg ritonavirritonavir bidbid–– Advantage over Advantage over amprenaviramprenavir
•• Easier dosingEasier dosing•• Decreased incidence of nausea, diarrhea, abdominal Decreased incidence of nausea, diarrhea, abdominal
pain and pain and rashrash

New PI: New PI: AtazanavirAtazanavir•• Indicated both for PI naïve and PI experienced Indicated both for PI naïve and PI experienced
patientspatients•• Once daily dosing; preferably taken with food to Once daily dosing; preferably taken with food to
increase absorptionincrease absorption•• DosingDosing
–– PI naive: 400mg PI naive: 400mg po qdpo qd–– PI experienced:300mg PI experienced:300mg atazanaviratazanavir/100mg /100mg norvirnorvir–– Boosted 300mg Boosted 300mg atazanaviratazanavir/100mg /100mg norvir norvir when when
administered with either administered with either efavirenzefavirenz or or tenofovirtenofovir•• Side effectsSide effects
–– Increased indirect Increased indirect bilirubinbilirubin–– May not increase triglycerides and LDL as do other May not increase triglycerides and LDL as do other
protease inhibitorsprotease inhibitors•• Impact on Impact on lipodystrophy lipodystrophy and CAD not well known yetand CAD not well known yet

PI: Selected Drug InteractionsPI: Selected Drug Interactions
•• CYP 3A4 effects (RTV>>other PIs): CYP 3A4 effects (RTV>>other PIs): rifampinrifampin/(/(rifabutinrifabutin), ), ketoconazoleketoconazole, anticonvulsants, , anticonvulsants, simvastatinsimvastatin//lovastatinlovastatin, , astemizoleastemizole//tefenadinetefenadine, , midazolammidazolam//triazolamtriazolam, , ergotaminesergotamines, St. John’s , St. John’s WortWort
•• RTV increases levels of other PIs (1.5RTV increases levels of other PIs (1.5--40X)40X)•• RTV, NFV, APV lower oral contraceptive levelsRTV, NFV, APV lower oral contraceptive levels•• APV lowers methadone levelsAPV lowers methadone levels
DHHS Guidelines 11/10/03 <www.DHHS Guidelines 11/10/03 <www.aidsinfoaidsinfo..nihnih..govgov>>

FuzeonFuzeon::enfuvirtide enfuvirtide (T(T--20)20)•• Enfuvirtide Enfuvirtide (T(T--20)20)
–– New CategoryNew Category•• Fusion Inhibitors/entry inhibitorsFusion Inhibitors/entry inhibitors
–– Fuzeon Fuzeon binds to gp41 protein thus preventing viral binding and binds to gp41 protein thus preventing viral binding and entry into Tentry into T--cellscells
–– IndicationIndication•• For HAART experienced patient with resistant virusFor HAART experienced patient with resistant virus•• InjectableInjectable formulation with bid dosingformulation with bid dosing
–– Side effects:Side effects:•• Skin irritation at injection site is most commonSkin irritation at injection site is most common•• Fatigue, insomnia and peripheral neuropathyFatigue, insomnia and peripheral neuropathy


Combination Therapy: 3 vs. 2Combination Therapy: 3 vs. 2
33--drugs: ~75% drugs: ~75% HIV RNA <400 cps/ml HIV RNA <400 cps/ml (compared to 37%)(compared to 37%)
ZDV/3TC vs. ZDV/3TC vs. ZDV/3TC/NFVZDV/3TC/NFV
AgouronAgouron 511511(N=297)(N=297)SaagSaag, AIDS 2001, AIDS 2001
33--drugs: ~80% drugs: ~80% HIV RNA <500 cps/ml HIV RNA <500 cps/ml (compared to 30(compared to 30--45%)45%)
ZDV/3TC vs. IDV vs. ZDV/3TC vs. IDV vs. ZDV/3TC/IDVZDV/3TC/IDV
Merck 035Merck 035(N=97)(N=97)Gulick, NEJM 1997Gulick, NEJM 1997
33--drugs reduced drugs reduced AIDS/death by ~50%AIDS/death by ~50%
ZDV/3TC vs. ZDV/3TC vs. ZDV/3TC/IDVZDV/3TC/IDV
ACTG 320ACTG 320(N=1156)(N=1156)Hammer, NEJM 1997Hammer, NEJM 1997
Results (1 yr f/u)Results (1 yr f/u)RegimensRegimensStudyStudy
Combination three drug management (HAART) is the standard of careCombination three drug management (HAART) is the standard of care

Population based data correlates HAART -PI use with decreased HIV mortality
Population based data correlates HAART -PI use with decreased HIV mortality
PalellaPalella et al NEJM 1998;338:853et al NEJM 1998;338:853

When To Start Treatment? When To Start Treatment? ––Summary of Current GuidelinesSummary of Current Guidelines
consider if VL consider if VL >50>50--100K100K
considerconsidertreatmenttreatment
treattreatIASIAS--USA:USA:JAMA 2002JAMA 2002
defer if VL defer if VL <55K; treat or <55K; treat or defer if VL defer if VL >55K>55K
offer offer treatmenttreatment
treattreatDHHS:DHHS:7/14/03 update 7/14/03 update <<www.www.aidsinfoaidsinfo..nihnih..govgov>>
CD4 >350CD4 >350CD4 200CD4 200--350350
symptoms symptoms ororCD4 <200CD4 <200
GuidelinesGuidelines

Early Early vsvs Late TreatmentLate Treatment
EARLY RX:EARLY RX:•• HIV disease is progressiveHIV disease is progressive•• Rx decreases HIV RNA Rx decreases HIV RNA
(and resistance) and (and resistance) and increases CDincreases CD44(and immune function)(and immune function)
•• 6+ years of 6+ years of virologicvirologicsuppression demonstratedsuppression demonstrated
•• ? Decrease transmission
DELAYED RX:DELAYED RX:•• Risk of clinical progression Risk of clinical progression
low in early diseaselow in early disease•• Practical factors Practical factors
(adherence, toxicity, quality (adherence, toxicity, quality of life outweigh benefits in of life outweigh benefits in earlyearly--disease)disease)
•• Long term effects unknownLong term effects unknown•• Preserve rx options? Decrease transmission Preserve rx options
Based on Based on DHHS Guidelines 11/10/03 <www.DHHS Guidelines 11/10/03 <www.aidsinfoaidsinfo..nihnih..govgov>>

Goal of Antiretroviral TherapyGoal of Antiretroviral Therapy
•• To suppress HIV RNA (viral load level) To suppress HIV RNA (viral load level) as low as possible, for as long as possibleas low as possible, for as long as possible
•• To preserve or enhance immune functionTo preserve or enhance immune function
•• To delay clinical progression of HIV diseaseTo delay clinical progression of HIV disease
DHHS Treatment Guidelines:DHHS Treatment Guidelines:Recommended Initial ARTRecommended Initial ART•• NNRTINNRTI--based regimensbased regimens
–– Preferred: ZDV (or TDF or d4T) + 3TC + EFV Preferred: ZDV (or TDF or d4T) + 3TC + EFV (except for pregnant women)(except for pregnant women)
–– Alternatives:Alternatives:•• ddIddI + 3TC + EFV (except for pregnant women)+ 3TC + EFV (except for pregnant women)•• ZDV or d4T or ZDV or d4T or ddIddI + 3TC + NVP+ 3TC + NVP
•• PIPI--based regimensbased regimens–– Preferred: ZDV (or d4T) + 3TC + LPV/rPreferred: ZDV (or d4T) + 3TC + LPV/r–– Alternatives: Alternatives:
•• ZDV (or d4T) + 3TC +APV/r, IDV, IDV/r, NFV, or SQV/rZDV (or d4T) + 3TC +APV/r, IDV, IDV/r, NFV, or SQV/rDHHS Guidelines 11/10/03 <www.DHHS Guidelines 11/10/03 <www.aidsinfoaidsinfo..nihnih..govgov>>
DHHS Treatment Guidelines:DHHS Treatment Guidelines:Triple NRTI RegimenTriple NRTI Regimen•• A 3 NRTI regimenA 3 NRTI regimen
–– AbacavirAbacavir+ + ZidovudineZidovudine+ (or + (or StavudineStavudine) + ) + LamivudineLamivudine•• Should only be used when an NNRTIShould only be used when an NNRTI--based or PIbased or PI--based regimen based regimen
cannot or should not be used as initial Rxcannot or should not be used as initial Rx–– egeg..-- drugdrug--drug interactions; regimen complexitydrug interactions; regimen complexity
•• Randomized clinical trial comparing triple NRTI Randomized clinical trial comparing triple NRTI vs vs PIPI--based based regimens:regimens:
–– Substantially higher rate of early Substantially higher rate of early virologic virologic nonnon--response was seen in response was seen in the 3the 3--NRTI arm.NRTI arm.
•• TenofovirTenofovir//abacavirabacavir//lamivudine lamivudine or or tenofovirtenofovir//didanosinedidanosine//lamivudinelamivudineshould not be used as a sole antiretroviral agent for naïve or should not be used as a sole antiretroviral agent for naïve or treatment experienced patientstreatment experienced patients
–– earlyearly virologicvirologic nonnon--responseresponse
DHHS Guidelines 11/10/03 <www.aidsinfo.nih.gov>DHHS Guidelines 11/10/03 <www.DHHS Guidelines 11/10/03 <www.aidsinfoaidsinfo..nihnih..govgov>>

DHHS Treatment Guidelines:DHHS Treatment Guidelines:Not RecommendedNot Recommended•• SingleSingle--drug therapy (drug therapy (monotherapymonotherapy): not potent, rapid resistance): not potent, rapid resistance•• TwoTwo--drug therapy: rapid development of resistancedrug therapy: rapid development of resistance•• Certain nucleoside pairs and antiretroviral components:Certain nucleoside pairs and antiretroviral components:
–– d4T + ZDV: antagonisticd4T + ZDV: antagonistic–– d4T + d4T + ddCddC: additive peripheral neuropathy: additive peripheral neuropathy–– d4T + d4T + ddIddI: additive peripheral neuropathy: additive peripheral neuropathy–– EmtricitabineEmtricitabine++lamivudinelamivudine: similar resistance profile; no potential benefit: similar resistance profile; no potential benefit
•• Protease inhibitorsProtease inhibitors–– AtazanavirAtazanavir++indinavirindinavir: potential additive: potential additive hyperbilirubinemiahyperbilirubinemia–– Saquinavir Saquinavir hard gel capsule; poor bioavailability (4%)hard gel capsule; poor bioavailability (4%)
•• 3 3 ––NRTI regimens containingNRTI regimens containing–– abacavirabacavir++tenofovirtenofovir++lamivudine lamivudine or or didanosinedidanosine++tenofovortenofovor++lamivudinelamivudine
•• HydroxyureaHydroxyurea: promotes toxicity of : promotes toxicity of didanosinedidanosine, increased peripheral neuropathy and , increased peripheral neuropathy and pancreatitispancreatitis
•• In pregnancy: d4T + In pregnancy: d4T + ddIddI (lactic acidosis) ; EFV ((lactic acidosis) ; EFV (teratogenicteratogenic); APV solution); APV solution
DHHS Guidelines 11/10/03 <www.DHHS Guidelines 11/10/03 <www.aidsinfoaidsinfo..nihnih..govgov>>

What about Once Daily Dosing?What about Once Daily Dosing?Nucleoside/Nucleotide Analogues Nonnucleoside Reverse Transcriptase Inhibitors Protease Inhibitors
Didanosine (enteric-coated) Efavirenz Amprenavir/ritonavir
Emtricitabine Nevirapine Atazanavir
Lamivudine Saquinavir/ritonavir
Stavudine (extended-release)
Tenofovir
M o s t o f th e s e m e d ic a t io n s h a v e b e e n s tu d ie d in c o m b in a t io n w ith tw ic e -d a i ly d ru g s , b u t h a v e n o t b e e n s tu d ie d a s c o m p o n e n ts o f a n e n t i r e ly o n c e -d a i ly r e g im e n .
O n e tr ip le n u c le o s id e re g im e n , a b a c a v ir + la m iv u d in e + te n o fo v ir h a s re c e n tly b e e n fo u n d to h a v e a h ig h ra te o f v iro lo g ic f a i lu re a n d s h o u ld b e a v o id e d .

What about Once Daily Dosing?What about Once Daily Dosing?•• few efficacy studies of oncefew efficacy studies of once--daily antiretroviral combinations daily antiretroviral combinations
have been conductedhave been conducted•• most are small and nonrandomized and must therefore be most are small and nonrandomized and must therefore be
interpreted with cautioninterpreted with caution•• regimens most thoroughly studied containregimens most thoroughly studied contain didanosinedidanosine,,
efavirenzefavirenz, and, and lamivudinelamivudine oror emtricitabineemtricitabinedidanosine + emtricitabine** + efavirenz
ddI 400 mg (wt >= 60 kg), FTC 200 mg, EFV 600 mg QD
RCT (compared with ddI/EFV + d4T [immediate-release, BID]); blinded to FTC and d4T
571 (286 on this regimen)
Treatment naive
Viral load 4.9 log10 copies/mL; CD4 = 288 cells/mm
3
60 weeks
At 24 weeks, viral load <50 in 81%, compared to 70% in d4T arm. At 60 weeks, virologic failure in 7% versus 15% of d4T arm (by KM probability).
163 Better virologic and CD4 response and fewer adverse events in FTC-containing regimen
Largest RCT of a once-daily regimen
[12, 14]
Once Daily Dosing has not been extensively studied and these are not regimens of choice by DHHS guidelines.
Once Daily Dosing has not been extensively studied and these are not regimens of choice by DHHS guidelines.

Once Daily Dosing Caveats:Once Daily Dosing Caveats:
•• Paucity of longPaucity of long--term clinical trials with term clinical trials with comparison to potent twice daily regimenscomparison to potent twice daily regimens
•• CaveatCaveat--consequences of a missed dose:consequences of a missed dose:–– May result in inadequate drug exposure over a May result in inadequate drug exposure over a
defined time perioddefined time period–– Consequent higher probability for development of Consequent higher probability for development of
drug resistance drug resistance

DHHS Monitoring GuidelinesDHHS Monitoring Guidelines
Monitoring CDMonitoring CD44 cell countscell counts•• When to measureWhen to measure
–– baseline (at time of diagnosis, 2 specimens)baseline (at time of diagnosis, 2 specimens)–– ongoing evaluations every 3ongoing evaluations every 3--6 months6 months
•• Treatment decisionsTreatment decisions–– based on trend over time (at least 2 values)based on trend over time (at least 2 values)
•• Significant change is >30% of absolute CDSignificant change is >30% of absolute CD44value (or >3% of CDvalue (or >3% of CD44 percentage)percentage)
DHHS Guidelines 11/10/03 <www.DHHS Guidelines 11/10/03 <www.aidsinfoaidsinfo..nihnih..govgov>>

DHHS Monitoring GuidelinesDHHS Monitoring Guidelines
Monitoring viral loadMonitoring viral load•• When to measureWhen to measure
–– at baseline (2 specimens, 1at baseline (2 specimens, 1--2 weeks apart)2 weeks apart)–– prior to initiation of antiretroviral rxprior to initiation of antiretroviral rx–– 22--8 weeks after initiation of rx8 weeks after initiation of rx–– ongoing evaluations every 3ongoing evaluations every 3--4 months4 months
•• Do not measure within 2Do not measure within 2--4 weeks of acute 4 weeks of acute illness or immunizationillness or immunization
•• Minimum sign. change is 3Minimum sign. change is 3--fold or 0.5 logfold or 0.5 logDHHS Guidelines 11/10/03 <www.DHHS Guidelines 11/10/03 <www.aidsinfoaidsinfo..nihnih..govgov>>
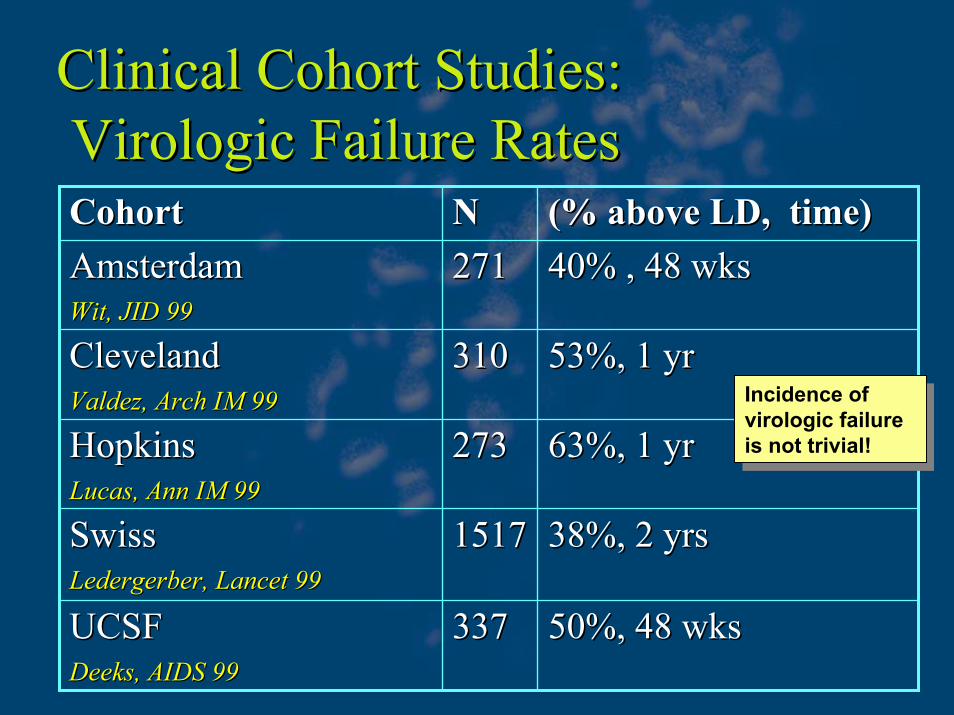
Clinical Cohort Studies: Clinical Cohort Studies: VirologicVirologic Failure RatesFailure Rates
50%, 48 wks50%, 48 wks337337UCSF UCSF DeeksDeeks, AIDS 99, AIDS 99
38%, 2 yrs38%, 2 yrs1517 1517 SwissSwissLedergerberLedergerber, Lancet 99, Lancet 99
63%, 1 yr63%, 1 yr273273HopkinsHopkinsLucas, Ann IM 99Lucas, Ann IM 99
53%, 1 yr53%, 1 yr310310ClevelandClevelandValdez, Arch IM 99Valdez, Arch IM 99
40% , 48 wks40% , 48 wks271271AmsterdamAmsterdamWit, JID 99Wit, JID 99
(% above LD, time)(% above LD, time)NNCohortCohort
Incidence of virologic failure is not trivial!
Incidence of virologic failure is not trivial!

Clinical Cohort Studies: Clinical Cohort Studies: VirologicVirologic Failure Rates 2002Failure Rates 2002ART Cohort collaborationART Cohort collaboration
13 HIV clinical cohort studies13 HIV clinical cohort studies10 Europe, 2 Canada, 1 US10 Europe, 2 Canada, 1 US12574 individuals starting 12574 individuals starting >>3 drug ART3 drug ART73% had HIV RNA <400 73% had HIV RNA <400 cpmcpm at 6 monthsat 6 months
Chene, et al., TuOrB1140, XIV AIDS Conf. 2002

Treatment Regimen FailureTreatment Regimen Failure•• VirologicVirologic failurefailure
–– Not achieving HIV RNA <400 Not achieving HIV RNA <400 cpmcpm by wk 24 or by wk 24 or <50 <50 cpmcpm by wk 48by wk 48
–– After After virologicvirologic response, repeated detection of response, repeated detection of viremiaviremia
•• Immunologic failureImmunologic failure–– Failure to increase CD4 count by 25Failure to increase CD4 count by 25--50 cells over 50 cells over
the first year of therapy or decrease to below the first year of therapy or decrease to below baselinebaseline
•• Clinical failureClinical failure–– Occurrence or recurrence of HIVOccurrence or recurrence of HIV--related eventsrelated events
DHHS Guidelines 11/10/03 <www.DHHS Guidelines 11/10/03 <www.aidsinfoaidsinfo..nihnih..govgov>>

Why Does Treatment Fail Patients?Why Does Treatment Fail Patients?
•• AdherenceAdherence–– Complicated regimens, heavy pill burden, toxicityComplicated regimens, heavy pill burden, toxicity
•• Baseline resistance or crossBaseline resistance or cross--resistanceresistance•• Use of less potent antiretroviral regimensUse of less potent antiretroviral regimens•• Sequential Sequential monotherapymonotherapy•• Drug levels and drug interactionsDrug levels and drug interactions•• Tissue reservoir penetrationTissue reservoir penetration•• Patient ‘not ready’ to take Patient ‘not ready’ to take antiretroviralsantiretrovirals

HIV Drug Resistance PreHIV Drug Resistance Pre--existsexists
•• HIV genome contains 10,000 nucleotidesHIV genome contains 10,000 nucleotides•• Mutation rate of HIV is ~3 X 10Mutation rate of HIV is ~3 X 10--55
•• 10 billion 10 billion virionsvirions produced dailyproduced daily•• Therefore all single (and many double) Therefore all single (and many double)
mutations are produced dailymutations are produced daily•• Leads to extensive viral diversityLeads to extensive viral diversity

HIV Drug ResistanceHIV Drug Resistance
•• Clinical resistanceClinical resistance–– Follow HIV RNA on antiretroviral therapyFollow HIV RNA on antiretroviral therapy
•• Genotypic resistanceGenotypic resistance–– Perform Perform in vitroin vitro assay to assess substitutions in assay to assess substitutions in
viral genetic sequence; correlate with drug viral genetic sequence; correlate with drug resistanceresistance
•• Phenotypic resistancePhenotypic resistance–– Perform Perform in vitroin vitro assay to assess growth of viral assay to assess growth of viral
strain in the presence of antiretroviral drugsstrain in the presence of antiretroviral drugs
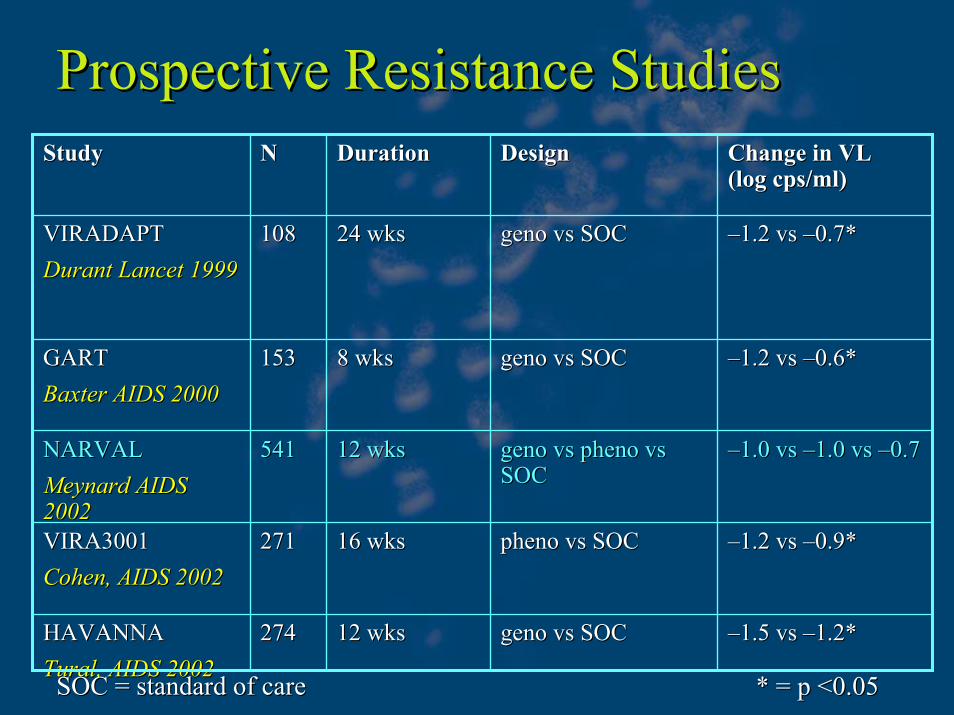
Prospective Resistance StudiesProspective Resistance Studies
––1.5 1.5 vsvs ––1.2*1.2*genogeno vsvs SOCSOC12 wks12 wks274274HAVANNAHAVANNATuralTural, AIDS 2002, AIDS 2002
––1.2 1.2 vsvs ––0.9*0.9*phenopheno vsvs SOCSOC16 wks16 wks271271VIRA3001VIRA3001Cohen, AIDS 2002Cohen, AIDS 2002
––1.0 1.0 vsvs ––1.0 1.0 vsvs ––0.70.7genogeno vsvs phenopheno vsvsSOCSOC
12 wks12 wks541541NARVALNARVALMeynardMeynard AIDS AIDS 20022002
––1.2 1.2 vsvs ––0.6*0.6*genogeno vsvs SOCSOC8 wks8 wks153153GARTGARTBaxter AIDS 2000Baxter AIDS 2000
––1.2 1.2 vsvs ––0.7*0.7*genogeno vsvs SOCSOC24 wks24 wks108108VIRADAPTVIRADAPTDurant Lancet 1999Durant Lancet 1999
Change in VL Change in VL (log cps/ml)(log cps/ml)
DesignDesignDurationDurationNNStudyStudy
* = p <0.05* = p <0.05SOC = standard of careSOC = standard of care

Reduced Susceptibility (>10 Fold)Reduced Susceptibility (>10 Fold)
0
5
10
15
20
1996 1997 1998 1999 2000
Per
cent
NRTINNRTIPI
N = 32 106 88 71 15Year
Little, et al. NEJM 2002;347:385.
Primary HIV infection / 10 U.S. cities
The proportion of non-susceptible HIV isolates is increasing.
The proportion of non-susceptible HIV isolates is increasing.

DHHS Monitoring GuidelinesDHHS Monitoring Guidelines
Use of drug resistance assaysUse of drug resistance assays•• RecommendedRecommended
–– virologicvirologic failure on rxfailure on rx–– suboptimal HIV RNA suppression after starting rxsuboptimal HIV RNA suppression after starting rx–– acute HIV infectionacute HIV infection
•• ConsiderConsider–– chronic HIV infection prior to starting rxchronic HIV infection prior to starting rx
•• Not usually recommendedNot usually recommended–– after discontinuation of drugsafter discontinuation of drugs–– HIV RNA <1000 copies/mlHIV RNA <1000 copies/ml
DHHS Guidelines 11/10/03 <www.DHHS Guidelines 11/10/03 <www.aidsinfoaidsinfo..nihnih..govgov>>

Current Approach to Salvage RxCurrent Approach to Salvage Rx
•• Review antiretroviral history; assess adherence, Review antiretroviral history; assess adherence, tolerability, and PK issuestolerability, and PK issues
•• Distinguish first/second from multiple failuresDistinguish first/second from multiple failures•• Perform resistance testing while on drugsPerform resistance testing while on drugs•• Identify susceptible drugs/drug classesIdentify susceptible drugs/drug classes•• Consider novel strategies Consider novel strategies
(PK enhancement with RTV; (PK enhancement with RTV; multidrugmultidrug regimens)regimens)•• Consider newer agents through expanded access or Consider newer agents through expanded access or
clinical trialsclinical trials•• Design a regimen with Design a regimen with >>3 active drugs (if possible)3 active drugs (if possible)
DHHS Guidelines 11/10/03 <www.DHHS Guidelines 11/10/03 <www.aidsinfoaidsinfo..nihnih..govgov>>
Antiretroviral Rx: ConclusionsAntiretroviral Rx: Conclusions•• Antiretroviral rx suppresses HIV RNA, improves Antiretroviral rx suppresses HIV RNA, improves
immune immune fxfx, decreases disease progression and , decreases disease progression and prolongs survival.prolongs survival.
•• The optimal time to begin therapy is not clear.The optimal time to begin therapy is not clear.•• The optimal initial rx is not clear, but there are The optimal initial rx is not clear, but there are
effective combination regimens available.effective combination regimens available.•• FirstFirst--line rx fails in 10line rx fails in 10--60% of patients.60% of patients.•• Resistance testing demonstrates benefits in selecting Resistance testing demonstrates benefits in selecting
antiretroviral therapy.antiretroviral therapy.•• There are a number of new drugs in development.There are a number of new drugs in development.•• Further research is needed.Further research is needed.


Question 1Question 1
•• EmtricitabineEmtricitabine (FTC) is similar in both structure (FTC) is similar in both structure and efficacy to which antiretroviral?and efficacy to which antiretroviral?–– A. A. StavudineStavudine–– B. B. NelfinavirNelfinavir–– C. C. TenofovorTenofovor–– D. D. LamivudineLamivudine

Question 2Question 2
•• Which would be a DEFINITE indication for Which would be a DEFINITE indication for initiating initiating antitretroviral antitretroviral therapy as per DHHS therapy as per DHHS guidelines?guidelines?–– A. Asymptomatic, CD4>250 but <350, VL > A. Asymptomatic, CD4>250 but <350, VL >
55,00055,000–– B. Asymptomatic, CD4<200, VL=30,000B. Asymptomatic, CD4<200, VL=30,000–– C. Asymptomatic, CD4>350, VL>55,000C. Asymptomatic, CD4>350, VL>55,000–– D. Asymptomatic, CD4>350, VL<55,000D. Asymptomatic, CD4>350, VL<55,000

Question 3Question 3
•• The most common side effect of the fusion The most common side effect of the fusion inhibitor Tinhibitor T--20 (20 (enfuvirtideenfuvirtide) is:) is:–– A. DiarrheaA. Diarrhea–– B. CNS side effectsB. CNS side effects-- vivid dreamsvivid dreams–– C. Skin irritation at injection site C. Skin irritation at injection site –– D. Hepatic D. Hepatic steatosis steatosis and lactic acidosisand lactic acidosis
Question 4Question 4
•• As per the DHHS guidelines, when is HIV As per the DHHS guidelines, when is HIV resistance testing not recommended?resistance testing not recommended?–– A. A. virologicvirologic failure while on treatmentfailure while on treatment–– B. suboptimal HIV RNA suppression after starting B. suboptimal HIV RNA suppression after starting
rxrx–– C. acute HIV infectionC. acute HIV infection–– D. HIV RNA <1000 copies/mlD. HIV RNA <1000 copies/ml

Question 5Question 5
•• Which most accurately describes the class Which most accurately describes the class level TOXICITY of protease inhibitors?level TOXICITY of protease inhibitors?–– A. Bone marrow suppression, anemiaA. Bone marrow suppression, anemia–– B. Increased hepaticB. Increased hepatic transaminasestransaminases, ,
hyperglycemia,hyperglycemia, lipodystrophylipodystrophy andand lipidemialipidemia, , increased bleeding in hemophiliacs.increased bleeding in hemophiliacs.
–– C. Lactic acidosis and hepatic C. Lactic acidosis and hepatic steatosissteatosis–– D. Rash and CNS side effects (vivid dreams)D. Rash and CNS side effects (vivid dreams)

AnswersAnswers
•• Question 1: DQuestion 1: D•• Question 2: BQuestion 2: B•• Question 3: CQuestion 3: C•• Question 4: DQuestion 4: D•• Question 5: BQuestion 5: B
Related Documents











