RESEARCH ARTICLE
New Clinico-Genetic Classification ofTrichothiodystrophyFanny Morice-Picard,1,2* Muriel Cario-Andr�e,3 Hamid Rezvani,3 Didier Lacombe,2 Alain Sarasin,4
and Alain Ta€ıeb1,3
1Department of Pediatric Dermatology, National Reference Center for Rare Skin Disorders, Pellegrin University Hospitals, Bordeaux, France2Department of Medical Genetics (National Reference Center for Developmental Defects), Pellegrin University Hospitals, Bordeaux, France3INSERM U876, Victor Segalen Bordeaux 2 University, Bordeaux, France4CNRS FRE 2939, University Paris-Sud, Gustave Roussy Institute, Villejuif, France
Received 11 February 2009; Accepted 4 April 2009
Trichothiodystrophy (TTD) is a congenital hair dysplasia with
autosomal recessive transmission. Cross banding pattern under
polarized light plus trichoschisis and a low sulfur content of hair
shafts define the disorder, which is associated with variable and
neuroectodermal symptoms. So-called photosensitive forms of
TTD (with low level of in vitro UV-induced DNA repair, not
constantly associated with marked clinical photosensitivity) are
caused by mutations in genes encoding subunits of the
transcription/repair factor IIH (TFIIH). Ten percentage of non-
photosensitive patients are known to have TTDN1 mutations,
the specific role of which is unknown. We studied nine patients
recruited at our institution and reviewed 79 with molecular
analysis out of 122 TTD patients reported in literature with the
aim to collect systematically the clinical findings in TTD patients
and establish genotype–phenotype correlations. The frequency
of congenital ichthyosis, collodion-baby type, was significantly
higher in the TFIIH mutated group. Hypogonadism was signifi-
cantly more frequent in the non-photosensitive group. There was
no statistical difference regarding osseous anomalies. Mutations
in TFIIH sub-units leading to abnormal expression in genes
involved in epidermal differentiation could explain the particu-
lar dermatological changes seen in photosensitive cases of TTD.
We suggest a new clinico-genetic classification of TTD, which
may help clinicians confused by the current acronyms used
(IBIDS, PIBIDS. . .). Understanding the TTD ichthyotic pheno-
type could lead to therapeutic advances in the management of
TTD and other types of ichthyoses. � 2009 Wiley-Liss, Inc.
Key words: TTD; photosensitivity; DNA repair; transcription
factor THFIIH; ichthyosis
INTRODUCTION
Trichothiodystrophy (TTD) is a rare ectodermal disorder first
described by Pollitt et al. [1968] and named by Price et al.
[1980]. The patients usually present with dry and sparse hair. Hair
shafts break easily with trauma. The name trichothiodystrophy was
proposed to group several phenotypes on the basis of a common
deficiency in sulfur proteins of the hair shaft [Price et al., 1980].
Several neuroectodermal manifestations are variably seen in this
phenotype including mental retardation, ichthyotic skin, reduced
stature, osseous anomalies and hypogonadism but none is a con-
stant trait [Itin and Pittelkow, 1990; Itin et al., 2001].
TTD is inherited as an autosomal recessive trait [Jackson et al.,
1974; Price et al., 1980; Howell et al., 1981]. DNA repair defect is
present in around 50% of patients, which have been referred to as
‘‘photosensitive’’ even without clear-cut evidence of associated
clinical photosensitivity [Nishiwaki et al., 2004]. Mutations in
XPD, XPB, p8 have been subsequently found in ‘‘photosensitive’’
TTD patients [Stefanini et al., 1986; Weeda et al., 1997; Giglia-Mari
et al., 2004]. Mutations in C7Orf11, encoding TTDN1 of unknown
function was found in the group of patients without DNA repair
anomalies [Nakabayashi et al., 2005]. However mutations in this
gene were excluded in some non-photosensitive patients including
those described by Howell et al. [1981] (Sabinas syndrome) and
Pollitt et al. [1968] suggesting further genetic heterogeneity in the
group without DNA repair anomaly [Nakabayashi et al., 2005]. A
genetic classification into three groups can thus be proposed
distinguishing a group with DNA repair anomalies (I), a group
*Correspondence to:
Fanny Morice-Picard, National Reference, Center for Rare Skin Disorders,
Unit�e de Dermatologie P�ediatrique, Hopital Pellegrin-Enfants, 33076
Bordeaux, France. E-mail: [email protected]
Published online 13 August 2009 in Wiley InterScience
(www.interscience.wiley.com)
DOI 10.1002/ajmg.a.32902
How to Cite this Article:Morice-Picard F, Cario-Andr�e M, Rezvani H,
Lacombe D, Sarasin A, Ta€ıeb A. 2009. New
clinico-genetic classification of
trichothiodystrophy.
Am J Med Genet Part A 149A:2020–2030.
� 2009 Wiley-Liss, Inc. 2020

without DNA repair defect and with TTDN1 mutations (II), and a
group without DNA repair defect and without identified genetic
basis (III).
XPD, XPB, and p8 are subunits of the transcription/DNA repair
factor IIH (TFIIH). TFIIH is a complex consisting of 10 proteins
essential for both nucleotide excision-repair (NER) and transcrip-
tion [Schultz et al., 2000; Coin et al., 2006; Laine and Egly, 2006].
Mutations in subunits associated with TTD destabilize the TFIIH
structure and lead to decreased cellular concentrations [Coin et al.,
1998; Vermeulen et al., 2000]. The lower amount of TFIIH found in
individuals with TTD contributes to a limiting level of transcription
of targeted genes and could explain the TTD phenotype including
cutaneous and neurological features [Compe et al., 2007].
TTDN1 is a nuclear protein not involved in DNA repair. It has
been shown that TTDN1 interacts with polo-like kinase 1 (PLK1), a
highly conserved serine-threonine kinase regulating cellular cycle
and mitosis [Zhang et al., 2007]. TTDN1 has several phosphoryla-
tion sites and is a regulator of mitosis. Interactions between cell
cycle regulation and transcription efficiency could explain the TTD
phenotype observed in patients with TTDN1 mutations.
In this article, we review patients seen in our Clinical Department
and those published to compare the phenotypes in photosensitive
and non-photosensitive groups, especially for cutaneous, neuro-
logical, osseous and gonadal aspects with the aim to establish
genotype–phenotype correlations in TTD.
PATIENTS AND METHODS
We analyzed the clinical condition of TTD patients and their genetic
characterization when available, through a literature review. Pa-
tients were included if the characteristic hair anomalies were
present, including a sulfur deficiency of hair and an abnormal
microscopic aspect (trichoschisis and hair-banding under polar-
ized light) allowing a definite diagnosis of TTD. Following a
comprehensive literature review, we selected a series of informative
features of the TTD phenotype to establish a clinical database,
including mental retardation, growth failure, osteosclerosis, go-
nadal dysfunction, cutaneous changes, and clinical photosensitivi-
ty. We looked at the associated genetic status of each patient
published in the literature, generally in consecutive reports. For
the analysis, two groups where distinguished, namely group A with
DNA repair anomalies and group B without DNA repair anomalies
and irrespective of the classification in three genetic groups. We
compared the frequencies of the selected clinical findings in both
groups using the c2 test (a¼ 5%).
RESULTS
Literature ReviewWe reviewed 122 patients with criteria for TTD [Pollitt et al., 1968;
Brown et al., 1970; Tay, 1971; Jackson et al., 1974; Arbisser et al.,
1976; Jorizzo et al., 1980; Price et al., 1980; Howell et al., 1981;
Crovato and Rebora, 1983; Diaz-perez and Vasquez, 1983; Van
Neste and Bore, 1983; Happle and Traupe, 1984; King et al., 1984;
Lucky et al., 1984; De Prost et al., 1986; Rebora et al., 1986; Stefanini
et al., 1986, 1992; Meynadier et al., 1987; Baden and Katz, 1988; Fois
et al., 1988; Lehmann et al., 1988; Motley and Finlay, 1989; Van
Neste et al., 1989; Broughton et al., 1990; Przedborski et al., 1990;
Kousseff, 1991; Savary et al., 1991; Peserico et al., 1992; Rizzo et al.,
1992; Sarasin et al., 1992; Alfandari et al., 1993; Calvieri et al., 1993;
Hersh et al., 1993; McCuaig et al., 1993; Chen et al., 1994; Feier and
Solovan, 1994; Tolmie et al., 1994; Eveno et al., 1995; Lynch et al.,
1995; Bracun et al., 1997; Brusasco and Restano, 1997; Malvehy
et al., 1997; Schepis et al., 1997; Takayama et al., 1997; Botta et al.,
1998, 2002, 2009; Petrin et al., 1998; Foulc et al., 1999; Itin et al.,
2001; Toelle et al., 2001; Vermeulen et al., 2001; Viprakasit et al.,
2001; Mazereeuw-Hautier et al., 2002; Dollfus et al., 2003; Giglia-
Mari et al., 2004; Wakeling et al., 2004; Faghri et al., 2008].
DNA repair analysis data and genetic status was available on 79
patients.
UV-induced DNA repair deficiency was found in 42 (group A).
The genetic status was available on 36 patients in group A, including
30 patients with XPD mutations [Crovato and Rebora, 1983; King
et al., 1984; Stefanini et al., 1986, 1992; Broughton et al., 1990;
Peserico et al., 1992; Chen et al., 1994; Tolmie et al., 1994; Eveno
et al., 1995; Takayama et al., 1997; Botta et al., 1998, 2009; Foulc
et al., 1999; Vermeulen et al., 2000; Boyle et al., 2008], 4 with p8
mutations [Jorizzo et al., 1980; Giglia-Mari et al., 2004] and 2 with
XPB mutations [Sarasin et al., 1992; Weeda et al., 1997]. Six patients
were presenting with abnormal DNA repair without molecular
characterization.
Thirty-seven patients presented with normal DNA repair
(group B). Twenty-eight patients had TTDN1 mutations
[Nakabayashi et al., 2005; Botta et al., 2007]. We obtained clinical
data on 26 of them [Jackson et al., 1974; Diaz-perez and Vasquez,
1983; Fois et al., 1988; Lehmann et al., 1988; Przedborski et al., 1990;
Rizzo et al., 1992; Nakabayashi et al., 2005; Botta et al., 2007].
Normal DNA repair was found in 11 patients, two of them had no
TTDN1 mutations [Nakabayashi et al., 2005]. Molecular analysis
was not performed in the nine remaining patients.
All observations are summarized in Table I.
Summary of the Observations of Our PatientsNine TTD cases were diagnosed at our institution between 1982 and
2007. Only the seven patients on whom DNA repair analysis data are
available are described here.
Patient 1 (TTD1VI). This boy was the first child born at term to
nonconsanguineous healthy parents. Family history was not rele-
vant. Intrauterine growth retardation was noted. Birth weight (BW)
was: 2,740 g (�1.5 SD), length (BL) 44 cm (�2 SD). Ichthyosiform
lesions of lower legs were noted on the 8th day of life. He was first
seen at 8 years for severe psychomotor delay. Neurologic exam
showed axial hypotonia with peripherical hypertonia and general-
ized convulsions. He had large protruding ears and unilateral single
palmar crease. Sparse brittle hair was noted. Magnetic resonance
imaging (MRI) showed pachygyria and ventricular dilatation.
Metabolic investigations including very long chain fatty acid level,
lysosomal enzymatic activities, mucopolysaccharides dosage were
normal. Hair microscopy showed a tiger-tail banding and bio-
chemical exam displayed a low-sulfur-hair content thus confirming
the diagnosis of TTD. UV-induced DNA repair deficiency was
found in vitro at about 30–40% of control. Full complementation
was observed following transfection with wild-type XPD gene. XPD
MORICE-PICARD ET AL. 2021

TAB
LEI.
Sum
mar
yof
Clin
ical
and
Mol
ecul
arFi
ndi
ngs
of7
9TT
DPa
tien
ts
Pati
ent
Ref
eren
ces
Der
mat
olog
ical
aspe
cts
Gon
adal
anom
alie
s
Oss
eou
s
anom
alie
s
DN
A
UD
SM
olec
ula
ran
alys
isCl
inic
alre
port
Mut
atio
nre
port
edCo
llodi
onIc
hthy
osis
Phot
osen
siti
vity
TTD
2B
RTo
lmie
etal
.[1
99
4]
Tolm
ieet
al.
[19
94
]�
þþ
��
þXP
Dp
.fs7
30
hm
z
TTD
1B
ILe
hman
net
al.
[19
88
]B
roug
hton
etal
.[1
99
0]
þþ
�Pu
bert
ald
elay
�þ
XPD
p.fs
73
0h
mz
TTD
2G
LK
ing
etal
.[1
98
4]
Bro
ught
onet
al.
[19
90
]�
Mod
erat
eic
hthy
osis
��
�þ
XPD
p.R
11
2H
hm
z
TTD
1PV
Crov
ato
etal
.[1
98
3]
Stef
anin
iet
al.
[19
86
]�
þM
oder
ate
Hyp
ogon
adis
m�
þXP
Dp
.R1
12
Hh
mz
TTD
2PV
Tr� ev
isan
etal
.[1
98
3]
Stef
anin
iet
al.
[19
86
]�
þYe
s,er
ythe
ma
��
þXP
Dp
.R1
12
Hh
mz
TTD
3PV
Tr� ev
isan
etal
.[1
98
3]
Stef
anin
iet
al.
[19
86
]�
þYe
s,er
ythe
ma
��
þXP
Dp
.R1
12
Hh
mz
TTD
4PV
Stef
anin
iet
al.
[19
86
]St
efan
ini
etal
.[1
98
6]
�þ
Yes,
butt
erfl
y
eryt
hem
a
��
þXP
Dp
.G4
13
Ah
mz
TTD
6PV
Mar
inon
iet
al.
[19
90
]St
efan
ini
etal
.[1
99
2]
þþ
þ�
�þ
XpD
p.D
67
3G
,n
e
TTD
7PV
Mar
inon
iet
al.
[19
90
]St
efan
ini
etal
.[1
99
2]
�þ
þ�
�þ
XPD
p.L
46
1V,
p.R
72
2W
TTD
8PV
Mar
inon
iet
al.
[19
90
]St
efan
ini
etal
.[1
99
2]
�þ
þ�
�þ
XPD
p.R
11
2H
hm
z
TTD
10
PVPe
seri
coet
al.
[19
92
]B
otta
etal
.[1
99
8]
�þ
þ�
Bon
em
atur
atio
n
del
ay
þXP
D
TTD
11
PVB
otta
etal
.[1
99
8]
Bot
taet
al.
[19
98
]þ
þþ
��
þXP
Dp
.R1
12
H,
del
12
1-1
59
TTD
12
PVB
otta
etal
.[1
99
8]
Bot
taet
al.
[19
98
]�
þ�
��
þXP
Dp
.R7
22
W,
p.C
25
2Y
TTD
15
PVB
otta
etal
.[1
99
8]
Bot
taet
al.
[19
98
]�
þ�
��
þXP
Dp
.R7
22
W,
p.C
25
2Y
TTD
9VI
Even
oet
al.
[19
95
]Ev
eno
etal
.[1
99
5]
��
þ�
�þ
XPD
p.R
11
2H
hm
z
TTD
1D
OD
Verm
eule
net
al.
[20
00
]Ve
rmeu
len
etal
.[2
00
0]
�Ye
sth
erm
osen
siti
ve�
��
þXP
Dp
.R6
58
Ch
mz
TTD
1R
OSt
efan
ini
etal
.[1
99
3]
Stef
anin
iet
al.
[19
93
]�
Yes
ther
mos
ensi
tive
þ�
�þ
XPD
p.R
65
8C
hm
z
TTD
3VI
/p2
Stef
anin
iet
al.
[19
93
]St
efan
ini
etal
.[1
99
3]
��
þH
ypog
onad
ism
�þ
XPD
p.R
65
8H
,p
.L4
61
V
TTD
2VI
Even
oet
al.
[19
95
]Ev
eno
etal
.[1
99
5]
þþ
ne
��
þXP
Dp
.R5
92
Ph
mz
TTD
18
3M
ETa
kaya
ma
etal
.[1
99
7]
Taka
yam
aet
al.
[19
97
]þ
Mod
erat
e,
impr
ovem
ent
þ�
�þ
XPD
p.7
25
Ph
mz
TTD
1B
ELSt
efan
ini
etal
.[1
99
3]
Stef
anin
iet
al.
[19
93
]�
þ�
��
þXP
Dp
.R7
22
Wh
mz
TTD
1VI
/p1
Bro
ught
onet
al.
[19
90
]B
roug
hton
etal
.[1
99
0]
�M
oder
ate
þ�
�þ
XPD
p.R
72
2W
,p
.L4
61
V
TTD
35
1B
EB
oyle
etal
.[2
00
8]
Boy
leet
al.
[20
08
]�
þþ
��
þXP
Dp
.R7
22
W,
p.R
37
8H
TTD
35
5B
EB
oyle
etal
.[2
00
8]
Boy
leet
al.
[20
08
]�
�þ
��
þXP
Dp
.E7
31
R,
ne
TTD
22
PVB
otta
etal
.[2
00
9]
Bot
taet
al.
[20
09
]þ
þ�
�O
steo
scle
rosi
sþ
XPD
,p.
Q6
62
X,pE
73
1Vf
sX1
00
/Gfs
X50
TTD
24
PVB
otta
etal
.[2
00
9]
Bot
taet
al.
[20
09
]�
Icht
hyos
iform
eryt
hrod
erm
a,AD
þ�
�þ
XPD
,p.
R7
22
W,
pE3
17
Dfs
X11
0
Foul
cet
al.
[19
99
]Fo
ulc
etal
.[1
99
9]
þIc
htyo
seal
opec
iaþ
Hyp
ofer
tilit
yO
steo
scle
rosi
s
oste
open
ia
þXP
D
Foul
cet
al.
[19
99
]Fo
ulc
etal
.[1
99
9]
þþ
þ�
Ost
eosc
lero
sis
oste
open
ia
þXP
D
Chen
etal
.[1
99
4]
Chen
etal
.[1
99
4]
�Ic
htyo
se,
ther
mos
ensi
tive
þ�
�þ
XPD
Chen
etal
.[1
99
4]
Chen
etal
.[1
99
4]
�Ic
htyo
sis
trun
k,PP
Kþ
��
þXP
D
TTD
1B
RJo
rizz
oet
al.
[19
82
]G
iglia
-Mar
iet
al.
[20
04
]þ
Xero
sis,
ADM
oder
ate
Cryp
torc
hid
iaN
orm
alX-
ray
þTT
Da
p.A
56
X/p
.L2
1P
TDD
99
RO
Gig
lia-M
ari
etal
.[2
00
4]
Gig
lia-M
ari
etal
.[2
00
4]
�Ic
hthy
osis
mod
erat
eM
oder
ate
��
þTT
Da
pA5
6X/
p.L2
1P
TTD
13
PVG
iglia
-Mar
iet
al.
[20
04
]G
iglia
-Mar
iet
al.
[20
04
]�
�M
oder
ate
��
þTT
Da
p.M
1T
hm
z
2022 AMERICAN JOURNAL OF MEDICAL GENETICS PART A

TAB
LEI.
(Con
tin
ued)
Pati
ent
Ref
eren
ces
Der
mat
olog
ical
aspe
cts
Gon
adal
anom
alie
s
Oss
eou
s
anom
alie
s
DN
A
UD
SM
olec
ula
ran
alys
isCl
inic
alre
port
Mut
atio
nre
port
edCo
llodi
onIc
hthy
osis
Phot
osen
siti
vity
TTD
14
PVG
iglia
-Mar
iet
al.
[20
04
]G
iglia
-Mar
iet
al.
[20
04
]�
�M
oder
ate
��
þTT
Da
p.M
1T
hm
z
TTD
6VI
p3Sa
rasi
net
al.
[19
92
]W
eeda
etal
.[1
99
7]
þM
oder
ate
icht
hyos
is
trun
k
Mod
erat
e�
Nor
mal
X-ra
yþ
XPB
p.Y
11
9P
hm
z
TTD
4VI
/p4
Sara
sin
etal
.[1
99
2]
Wee
daet
al.
[19
97
]þ
Mod
erat
eic
hthy
osis
trun
k
Mod
erat
e�
Nor
mal
X-ra
yþ
XPB
p.Y
11
9P
hm
z
Luck
yet
al.
[19
84
]�
þþ
Test
ishy
pop
last
icO
steo
pen
iaþ
nd
Van
Nes
tean
dB
ore
[19
83
]�
þþ
�B
one
mat
urat
ion
del
ay
þn
d
Mey
nad
ier
etal
.[1
98
7]
þþ
þCr
ypto
rchi
dia
,
hypo
f
�þ
nd
Fort
ina
etal
.[2
00
1]
�Ic
htyo
se,
derm
atit
e
atop
ique
þCr
ypto
rchi
dia
Ost
eosc
lero
sis
þn
d
McC
uaig
etal
.[1
99
3]
�Ic
htyo
sis
trun
k,
PPK
�Te
stis
hypo
pla
stic
Ost
eosc
lero
sis
þn
d
McC
uaig
etal
.[1
99
3]
þIc
htyo
seAD
þCr
ypto
rchi
dia
Axia
l
oste
oscl
eros
is
þn
d
TTD
5PV
Fois
etal
.[1
98
8]
Nak
abay
ashi
etal
.[2
00
5]
�Fo
llicu
lar
kera
tosi
s�
Hyp
ogon
adis
mLo
caliz
ed
oste
oscl
eros
is
�TT
DN
1n
e
TTD
9PV
Riz
zoet
al.
[19
92
]N
akab
ayas
hiet
al.
[20
05
]�
��
�N
orm
alX-
ray
�TT
DN
1d
elex
on1
,2h
mz
TTD
1M
ALe
hman
net
al.
[19
88
]N
akab
ayas
hiet
al.
[20
05
]�
Icht
hyos
istr
unk
��
��
TTD
N1
p.R
77
Gfs
X76
hm
z
Prze
dbor
ski
etal
.[1
99
0]
Nak
abay
ashi
etal
.[2
00
5]
��
�H
ypof
erti
lity
Ost
eop
enia
�TT
DN
1p
.R7
7G
fsX7
6h
mz
Prze
dbor
ski
etal
.[1
99
0]
Nak
abay
ashi
etal
.[2
00
5]
��
��
Ost
eop
enia
�TT
DN
1p
.R7
7G
fsX7
6h
mz
Prze
dbor
ski
etal
.[1
99
0]
Nak
abay
ashi
etal
.[2
00
5]
��
��
��
TTD
N1
p.R
77
Gfs
X76
hm
z
Jack
son
etal
.[1
97
4]
Nak
abay
ashi
etal
.[2
00
5]
��
�H
ypof
erti
lity
��
TTD
N1
p.M
14
4V
hm
z
Jack
son
etal
.[1
97
4]
Nak
abay
ashi
etal
.[2
00
5]
��
�H
ypof
erti
lity
��
TTD
N1
p.M
14
4V
hm
z
18
amis
hpa
tien
tsN
akab
ayas
hiet
al.
[20
05
]�
��
hypo
fert
ility
��
TTD
N1
p.M
14
4V
hrn
z
Maz
eree
uw-H
auti
eret
al.
[20
02
]þ
þ�
��
�n
d
Maz
eree
uw-H
auti
eret
al.
[20
02
]þ
þ�
Hyp
ofer
tilit
y�
�n
d
Tolm
ieet
al.
[19
94
]�
þ�
��
�n
d
Tolm
ieet
al.
[19
94
]�
��
��
�n
d
TTD
4B
RTo
lmie
etal
.[1
99
4]
��
��
��
nd
Lyn
chet
al.
[19
95
]�
��
�N
orm
alX-
ray
s�
nd
Polli
ttet
al.
[19
68
]�
��
��
�n
d
Polli
ttet
al.
[19
68
]�
��
��
�n
d
p5�
��
Hyp
ofer
tilit
yN
orm
alX-
ray
s�
nd
p6þ
��
�N
orm
alX-
ray
s�
nd
p7þ
��
�N
orm
alX-
ray
s�
nd
þ,
pres
ent;�
,ab
sen
t;AD
,at
opic
derm
atit
is;
PPK
,pa
lmop
lan
tar
kera
tosi
s;n
d,n
otde
term
ined
;n
e,n
otex
pres
sed;
hmz,
hom
ozyg
ous.
Phot
osen
siti
vepa
tien
tsar
ein
whi
te;
TTD
N1
mut
ated
pati
ents
are
ingr
ay;
non
-pho
tose
nsi
tive
not
TTD
N1
mut
ated
pati
ents
are
inbl
ue;
Yello
win
dica
tes
our
pat
ien
ts.
MORICE-PICARD ET AL. 2023

gene analysis found two deleterious mutations (First allele:
p.R722W and second allele p.L461V/716-730del) [Takayama
et al., 1997].
Patient 2 (TTD3VI). This boy was born at term after a normal
pregnancy. Family history was uninformative. He was first seen for
chronic alopecia. Clinical examination showed ichthyosis most
prominent on trunk, dry sparse hair with alopecia. Photosensitivity
was noted since age 7 years. A major psychomotor delay was
present. Hair analysis showed a tiger-tail pattern under polarized
light (Fig. 1). Amino-acid dosage shown diminished sulfur hair
content confirming the diagnosis of TTD. Skin histological exami-
nation showed a thin granular layer (Fig. 2). Zonular cataract was
present. UV-induced DNA repair deficiency was confirmed in
vitro. XPD gene analysis found two deleterious mutations (First
allele: p.R658H, and second allele p.L461V and Del p.716-730)
[Takayama et al., 1997].
Patients 3 and 4. The first child of a first-cousin healthy couple
was a boy. He was born at term after an uneventful pregnancy. He
was seen at birth, when he presented with congenital ichthyosis
(collodion baby) progressing to mild ichthyosis on the trunk
(Fig. 3a). Diagnosis of TTD was suspected at age 3 years on the
basis of mild ichthyosis of trunk, scalp, palms and soles (Fig. 3b),
mild photosensitivity noted after sun exposure and hair macro-
scopically normal but coarse and with a tiger-tail pattern under
polarized light. The diagnosis of TTD was confirmed by the analysis
of hair aminoacid content. Minor facial anomalies included broad
nasal bridge, apparently low-set abnormaly modelate ears. Growth
and psychomotor development were normal. Osseous radiogra-
phies were normal. A full blood count was normal. Hemoglobin
electrophoresis was normal. IgE were elevated. A UV-induced DNA
repair anomaly was detected. Complementation analysis showed
for the first time that the DNA repair defect was associated with the
XPB gene [Weeda et al., 1997]. Homozygous deleterious mutations
in the XPB gene were found. He was seen again at age 22. Photo-
sensitivity had disappeared. Ichthyosis of the flanks was more
marked and associated with a palmar hyperkeratosis (Fig. 3c–e).
A sensorineural deafness was recently diagnosed.
The second child was a girl. She was born at term with the same
presentation of congenital ichthyosis with a favorable outcome
(Fig. 4a). The diagnosis of TTD was confirmed by hair microscopy
and biochemical analysis. There was no mental or growth delay. She
was reevaluated at age 18. Ichthyosis was noted on the trunk with
desquamation following sun exposure (Fig. 4b). She had also mild
deafness. The two patients have two homozygous mutations in the
XPB gene (p.Y119P) [Weeda et al., 1997].
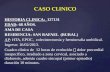
FIG. 1. Hair anomalies observed in Patient 2. a: Hypotrichosis with
brittle short hair. b: Trichoschisis with irregular aspect of cuticle. c:
Tiger-tail banding under polarized light (courtesy of Dr. D. Van
Neste).FIG. 2. Histologic examination of skin showing a thin granular layer,
compatible with ichthyosis vulgaris.
2024 AMERICAN JOURNAL OF MEDICAL GENETICS PART A

Patient 5. The patient is the first child of a nonconsanguineous
healthy couple. He was examined at 15 years for short, sparse hair
with alopecia associated with a generalized xerosis and keratosis
pilaris. Hair microscopical exam shown trichoschisis associated to a
tiger-tail banding under polarized light. Hypogonadism was asso-
ciated with micropenis and cryptorchidia. He also had leucopenia,
microcytosis, myopia, moderate developmental delay but normal
growth. Bone X-rays were normal. The diagnosis of TTD was
confirmed by hair aminoacid analysis showing a low sulfur hair
content. UV-induced DNA repair analyses were normal.
Patient 6 and 7. The boy (No. 6) was the first child of a non-
consanguineous healthy couple. Toxaemia was noted during preg-
nancy. He was born at 37 weeks (birth weight 2,700 g) and was
found to have a congenital ichthyosis (collodion baby). He was first
seen at age 7 years with his sister who had presented with the same
history of toxemia and collodion baby. Both had sparse, brittle,
hypopigmented hair. Microscopical and biochemical analysis of
hair confirmed a diagnosis of TTD. Hair loss following fever
episodes was noted. The girl (No. 7) had early onset insulin-
dependent diabetes. Other findings included moderate leuconeu-
tropenia, normal growth and developmental delay. DNA repair
studies were normal in both sibs. Both of them had a marked
pigmentary dilution (skin and hair) as compared with their parents.
Phenotype Analysis of 79 TTD PatientsNon-Cutaneous Aspects. The non-cutaneous aspects are sum-
marized in Table II.
Neurological involvement consists mainly in mental retardation,
and more uncommonly in ataxia, spastic paralysis or cerebellar
atrophy. Convulsions have rarely been described. MRI may show
abnormal white matter aspects. The two groups were similar. For
example, mental retardation was observed in 87% of in vitro
photosensitive patients (group A) and in 84% of the non-in vitro
photosensitive patients (group B).
Growth failure was observed in both groups, usually moderate
and rarely severe.
Typical osseous manifestations manifested as axial osteosclerosis
with peripherical osteopenia. Osseous manifestations were more
frequent in group A, but the difference was not significant
(c2 ¼ 2.62). Osseous anomalies can be asymptomatic and are not
often specified in the reports.
Hypoplastic testis, cryptorchidia are observed in males. Hypo-
gonadism has been sometimes substantiated by hormonal dosages
(diminished testosterone, elevated FSH, LH levels). A low fecundity
rate has been observed in the TTDN1-mutated Amish families
suggesting a defect in fertility. This may be the consequence of
gonadal dysfunction. Gonadal anomalies were significantly more
frequent in group B than in group A (65% in group B vs. 24% in
group A; c2¼ 13.69). However the lack of detailed clinical descrip-
tion including gonadal function constitutes a bias in this analysis.
Cutaneous Aspects. The results are summarized in Table III.
Skin anomalies mainly consisting of ichthyosis. An aspect of
collodion baby with a favorable course may precede the develop-
ment of ichthyosis. The descriptions of ichthyosis are often consis-
tent with the vulgaris type with small, white scales of the legs. Other
FIG. 3. Skin aspects of Patient 3. a: Collodion aspect at birth, (b) Moderate ichthyosis aspect of trunk at age 5, (c,d) Ichthyosiform skin changes more
pronounced at 22 years, (e) Moderate palmar keratoderma.
MORICE-PICARD ET AL. 2025

findings include xerosis, palmoplantar keratoderma, atopic der-
matitis, follicular keratosis. Pooled data shows a significantly
elevated frequency of ichthyosis in group A than in group B
(c2¼ 47), and a higher prevalence of neonatal forms (collodion
baby) (c2 ¼ 5.34). Moreover no description of collodion baby
was found in patients with TTDN1 mutations [Nakabayashi
et al., 2005; Botta et al., 2007]. However, two of our patients were
described as mild collodion babies and were subsequently found to
have normal DNA repair. Skin changes in group B are most often
non-specific, consisting of xerosis, follicular keratosis, and atopic
dermatitis.
The frequency of ichthyosis in patients with clinical photosensi-
tivity is higher than the frequency of ichthyosis in the global TTD
population (Table IV) These results highlight the association
between congenital ichthyosis and group A TTD with abnormal
DNA repair.
DISCUSSION
Our main finding is a significantly higher frequency of neonatal
ichthyosis in TFIIH-related TTD (group A) patients, as compared
to the non-TFIIH related group (group B). Ichthyosis in group A
has a mild course and looks like ichthyosis vulgaris. An aspect of
collodion baby can be observed at birth in nearly a third of the
patients. Among the environmental modifications, which could
lead to the more severe cutaneous phenotype in the neonatal period,
temperature might be considered. Cyclic hair loss has been de-
scribed in association with fever in four patients belonging to group
A [Kleijer et al., 1994]. This feature has been associated with the
XPD p.Arg658Cys mutation which gives rise to a thermosensitive
XPD protein. Elevation of temperature would be responsible for a
worsening of DNA repair and transcription anomalies leading
clinically to hair loss and increase of severity of ichthyosis
[Vermeulen et al., 2001].
In TTD cells, abnormal TFIIH needs to be produced quickly
enough to compensate its instability [Botta et al., 2002]. In differ-
entiating TTD cells, de novo synthesis is insufficient and leads
to accumulation of inactive factors and depression of basal
transcription particularly for genes involved in terminal
epidermal differentiation or neuronal myelination and pseudo-
thalassemia. Mutations in epidermal differentiation genes (TGM1
(MIM190195), ALOXE3 (MIM607206), ALOX12B (MIM603741),
ABCA12 (MIM607800), ichthyin (MIM609383), loricrin
(MIM152445)) involved in the congenital ichthyoses manifest also
commonly by a collodion baby phenotype. It could thus be specu-
lated that the clinical and histological aspects of ichthyosis vulgaris
observed in TTD patients could result of the defective expression of
epidermal differentiation complex proteins, most of which are
FIG. 4. Skin aspects of Patient 4. a: Short brittle hair with collodion
changes of the skin at birth. b,c: Ichthyotic skin with palmar
hyperlinearity at age 18.
TABLE II. Frequency of the Main Non-Cutaneous Features in TTD Groups A and B
Group A Group B
n ¼ 42 % n ¼ 37 %Failure to thrive 38 90 27 73Psychomotor delay 37 88 31 84Osseous anomalies 9 21.5 5 13.5Genital/reproductive anomalies 10 24 24 65
2026 AMERICAN JOURNAL OF MEDICAL GENETICS PART A

located in 1q21 including filaggrin and SPRR2. Skin biopsies of
ichthyosis performed in group A patients had similarities with
ichthyosis vulgaris, with diminished keratohyalin expression, a
marker of profilaggrin (Fig. 2). Furthermore, a diminution of
SPRR2 expression has been found in the TTD mouse model
homozygous for the XpdR722W allele [De Boer et al., 1998]. In vitro
reconstruction of TTD human epidermis could allow to study the
modification of the expression of proteins involved in keratinocyte
differentiation and their dependence on temperature.
Instability and dysfunction of TFIIH with mutated sub-units
could account for TTD findings [Schultz et al., 2000; Dubaele et al.,
2003]. It has been shown that TFIIH activates transcription by
phosphorylation of nuclear receptors such as RARa or thyroid
hormone receptor through its CDK subunit [Htun et al., 1996; Liu
et al., 2005]. Mutations in C terminal domain of XPD are directly
responsible for a decrease of phosphorylation of nuclear receptors
and expression of targeted genes [Keriel et al., 2002]. In particular, it
has been shown that the phosphorylation of the N-terminal domain
of the g subunit of the RAR by the CDK7 component of TFIIH leads
to receptor activation through modulation of its interaction with a
coregulator (vinexin b) [Bour et al., 2007].
Hypogonadism, which was initially described in Amish and
Moroccan patients who belong to group B, is also found in group
A. The difference of frequency between the two groups was signifi-
cant but more patients with TTDN1 mutations have to be studied to
make definitive conclusions. TTDN1 mutants responsible for
group II TTD could be involved in the maturation of spermatozoid
sulfur-rich proteins. In the drosophila, spermatogenesis is sensitive
to b2-tubulin level, a protein of the tubula. XPD mutations in
drosophila affect b2-tubulin leading to sterility in males. This
mechanism could explain gonadal immaturity in TTD group A
patients [Raff et al., 1982].
Osseous anomalies were found at a similar frequency in groups I
and II, suggesting that abnormal function of both TFIIH or of
TTDN1 could affect bone formation. The TTD-Xpd mouse model
provides a good clinical reproduction of the disease for bony
anomalies, which indicates a potent modulation of bone minerali-
zation by abnormal TFIIH [De Boer et al., 1998, 2002].
Unlike xeroderma pigmentosum, TTD is not a cancer prone-
disease. The group I cells are unable to repair the major cyclobutane
pyrimidine dimers (CPD) induced by solar UV. However, the TTD
cells mutated on the 50 part of the XPD gene are also defective in the
repair of the second type of UV-induced DNA lesions (pyrimidine
6-4 pyrimidone), while the cells mutated on the 30 part of the same
gene are proficient in this repair [Chigancas et al., 2008]. Never-
theless, none of these TTD patients are cancer-prone and therefore
the cancer-free phenotype in TTD should not be directly related to a
DNA repair defect [Nishiwaki et al., 2004]. On the other hand,
differences in cellular catalase activity between TTD and XP indi-
cate that UV light, directly or indirectly, together with defective
oxidative metabolism may increase the initiation and/or the pro-
gression steps in the XP environment compared to TTD [Vuillaume
et al., 1992]. It has been shown on normal and XP human recon-
structed epidermis that catalase overexpression had a protective
effect against deleterious effects of UV irradiation [Rezvani et al.,
2007, 2008]. This may partly explain the differences in skin tumor
proneness between group A TTD and XP.
In conclusion, TTD regroups recessively inherited affections,
which have in common a specific hair dysplasia. Molecular studies
suggest to classify TTD in three genetic groups. Mutations in the
three genes encoding TFIIH subunits (XPD, XPB, p8) are respon-
sible for the in vitro photosensitive form (group I). The non-
photosensitive group is genetically heterogeneous including
TTDN1 mutated patients (group II) and a third group without
known molecular basis. Our phenotype/genotype correlation study
showed a highly significant association between ichthyosis and
group I, and the collodion baby phenotype gives an early diagnostic
orientation for this group, without being completely specific. This
classification is presented with its genetic and clinical correlations in
Table V.
TABLE III. Frequency of Cutaneous Anomalies in TTD Groups A and B
Group A Group B
n ¼ 42 % n ¼ 37 %Ichthyosis 38 90 5 13.5Collodion baby 14 33.5 4 11
TABLE IV. Frequency of Ichthyosis in Patients With Clinical Photosensitivity and in Global TTD Population
Clinical photosensitivity Total TTD population
N¼ 39 % N¼ 122 %Ichthyosis 31 79 55 44
MORICE-PICARD ET AL. 2027

ACKNOWLEDGMENTS
Dr. Peter Itin and Dr. Mark Pittelkow for their help with literature
review. This study was supported by the GENESKIN 6th PCRD
programme 512117.
REFERENCES
Alfandari S, Delaporte E, Van Neste D, Lucidarme-Delespierre E, PietteF, Bergoend H. 1993. A new case of isolated trichothiodystrophy.Dermatology 186:197–200.
Arbisser AI, Scott CI Jr, Howell RR, Ong PS, Cox HL Jr. 1976. A syndromemanifested by brittle hair with morphologic and biochemical abnormal-ities, developmental delay and normal stature. Birth Defects 12:219–228.
Baden HP, Katz A. 1988. Trichothiodystrophy without retardation: Onepatient exhibiting transient combined immunodeficiency syndrome.Pediatr Dermatol 5:257–259.
Botta E, Nardo T, Broughton BC, Marinoni S, Lehmann AR, Stefanini M.1998. Analysis of mutations in the XPD gene in Italian patients withtrichothiodystrophy: Site of mutation correlates with repair deficiency,but gene dosage appears to determine clinical severity. Am J Hum Genet63:1036–1048.
Botta E, Nardo T, Lehmann AR, Egly JM, Pedrini AM, Stefanini M. 2002.Reduced level of the repair/transcription factor TFIIH in trichothiodys-trophy. Hum Mol Genet 11:2919–2928.
Botta E, Offman J, Nardo T, Ricotti R, Zambruno G, Sansone D, Balestri P,Raams A, Kleijer WJ, Jaspers NG, Sarasin A, Lehmann AR, Stefanini M.2007. Mutations in the C7orf11 (TTDN1) gene in six nonphotosensitivetrichothiodystrophy patients: No obvious genotype-phenotype relation-ships. Hum Mutat 28:92–96.
Botta E, Nardo T, Orioli D, Guglielmino R, Ricotti R, Bondanza S,Benedicenti F, Zambruno G, Stefanini M. 2009. Genotype-phenotyperelationships in trichothiodystrophy patients with novel splicing muta-tions in the XPD gene. Hum Mutat 30:438–445.
Bour G, Lalevee S, Rochette-Egly C. 2007. Protein kinases and the pro-teasome join in the combinatorial control of transcription by nuclearretinoic acid receptors. Trends Cell Biol 17:302–309.
Boyle J, Ueda T, Oh KS, Imoto K, Tamura D, Jagdeo J, Khan SG, Nadem C,Digiovanna JJ, Kraemer KH. 2008. Persistence of repair proteins atunrepaired DNA damage distinguishes diseases with ERCC2 (XPD)
mutations: Cancer-prone xeroderma pigmentosum vs. non-cancer-prone trichothiodystrophy. Hum Mutat 29:1194–1208.
Bracun R, Hemmer W, Wolf-Abdolvahab S, Focke M, Botzi C, Killian W,Gotz M, Jarisch R. 1997. Diagnosis of trichothiodystrophy in 2 siblings.Dermatology 194:74–76.
Broughton BC, Lehmann AR, Harcourt SA, Arlett CF, Sarasin A, Kleijer WJ,Beemer FA, Nairn R, Mitchell DL. 1990. Relationship between pyrimi-dine dimers, 6-4 photoproducts, repair synthesis and cell survival:Studies cells from patients with trichothiodystrophy. Mut Res 235:33–40.
Brown AC, Belser RB, Crounse RG, Wehr RF. 1970. A congenital hairdefect: Trichoschisis with alternating birefringence and low sulfur con-tent. J Invest Dermatol 54:496–509.
Brusasco A, Restano L. 1997. The typical ‘‘tiger tail’’ pattern of the hair shaftmay not be evident at birth. Arch Dermatol 133:249.
Calvieri S, Rossi A, Amorosi B, Giustini S, Innocenzi D, Micale G, Rizzo R.1993. Trichothiodystrophy: Ultrastructural studies of two patients.Pediatr Dermatol 102:111–116.
Chen E, Cleaver JE, Weber CA, Packman S, Barkovich AJ, Koch TK,Williams ML, Golabi M, Price VH. 1994. Trichothiodystrophy: Clinicalspectrum, central nervous system imaging, and biochemical characteri-zation of two siblings. J Invest Dermatol 103:154S–158S.
Chigancas V, Lima-Bessa KM, Stary A, Menck CF, Sarasin A. 2008.Defective transcription/repair factor IIH recruitment to specific UVlesions in trichothiodystrophy syndrome. Cancer Res 68:6074–6083.
Coin F, Marinoni JC, Rodolfo C, Fribourg S, Pedrini AM, Egly JM. 1998.Mutations in the XPD helicase gene result in XP and TTD phenotypes,preventing interaction between XPD and the p44 subunit of TFIIH. NatGenet 20:184–188.
Coin F, Proietti De Santis L, Nardo T, Zlobinskaya O, Stefanini M, Egly JM.2006. p8/TTD-A as a repair-specific TFIIH subunit. Mol Cell 21:215–226.
Compe E, Malerba M, Soler L, Marescaux J, Borrelli E, Egly JM. 2007.Neurological defects in trichothiodystrophy reveal a coactivator functionof TFIIH. Nat Neurosci 10:1414–1422.
Crovato F, Rebora A. 1983. PIBI(D)S syndrome: A new entity with defect ofthe deoxyribonucleic acid excision repair system. J Am Acad Dermatol11:340–346.
Crovato F, Borrone C, Rebora A. 1983. Trichothiodystrophy - BIDS, IBIDSand PIBIDS? Br J Dermatol 108:247.
De Boer J, de Wit J, van Steeg H, Berg RJ, Morreau H, Visser P, LehmannAR, Duran M, Hoeijmakers JH, Weeda G. 1998. A mouse model for the
TABLE V. Classification of TTD
Group A(in vitro photosensitivity)
Group B(no in vitro photosensitivity)
TTD-TFIIH/TTDP Group I TTD-non-TFIIH/TTDN-1 Group II Not classified Group IIIOMIM 601675 234050 275550, 211390Locus 19q 13.2–q 13.3 (XP-D)
6p25.3 (TTD-a/p8) 2q21(XP-B)
7p14 (C7Orf11) Unknown
Function DNA repair-transcription Unknown UnknownClinical subtype
of TTDTay; IBIDS (TTD-A) ABHS; BIDS Pollitt; Sabinas; other
TTD subtypes
IBIDS: ichthyosis, brittle hair, intellectual impairment, decrease fertility, short stature; BIDS: brittle hair, intellectual impairment, decrease fertility, short stature; ABHS: Amish brittle hair syndrome.
2028 AMERICAN JOURNAL OF MEDICAL GENETICS PART A

basal transcription/DNA repair syndrome trichothiodystrophy. Mol Cell1:981–990.
De Boer J, Andressoo JO, de Wit J, Huijmans J, Beems RB, van Steeg H,Weeda G, van der Horst GT, van Leeuwen W, Themmen AP, Meradji M,Hoeijmakers JH. 2002. Premature aging in mice deficient in DNA repairand transcription. Science 296:1276–1279.
De Prost Y, Lemaistre R, Dupr�e A. 1986. Trichothiodystrophie associ�ee�a unretard statural et psychomoteur (syndrome de Tay). Ann DermatolVenereol 113:1016–1017.
Diaz-perez JL, Vasquez JA. 1983. Flattened hair syndrome: A new disease.Arch Dermatol 119:854–855.
Dollfus H, Porto F, Caussade P, Speeg-Schatz C, Sahel J, Grosshans E,Flament J, Sarasin A. 2003. Ocular manifestations in the inherited DNArepair disorders. Surv Ophthalmol 48(1):107–122.
Dubaele S, Proietti De Santis L, Bienstock RJ, Keriel A, Stefanini M, VanHouten B, Egly JM. 2003. Basal transcription defect discriminatesbetween xeroderma pigmentosum and trichothiodystrophy in XPDpatients. Mol Cell 11:1635–1646.
Eveno E, Quilliet X, Chevallier-Lagente O, Daya-Grosjean L, Stary A, ZengL, Benoit A, Savini E, Ciarrocchi G, Kannouche P. 1995. Stable SV40-transformation and characterisation of some DNA repair propertiesof fibroblasts from a trichothiodystrophy patient. Biochimie 77:906–912.
Faghri S, Tamura D, Kraemer KH, Digiovanna JJ. 2008. Trichothiodys-trophy: A systematic review of 112 published cases characterises a widespectrum of clinical manifestations. J Med Genet 45:609–621.
Feier V, Solovan C. 1994. Trichothiodystrophie et syndrome d’hyper�eosinophilie, une association insolite. Ann Dermatol Venereol 121:151–155.
Fois A, balestri P, Calvieri S, Zampetti M, Giustini S, Stefanini M,Lagomarsini P. 1988. Trichothiodystrophy without photosensitivity:Biochemical, ultrastructural and DNA repair studies. Eur J Pediatr147:439–441.
Fortina AB, Alaibac M, Piaserico S, Peserico A. 2001. PIBI(D)S: clinical andmolecular characterization of a new case. 15:65–69.
Foulc P, Jumbou O, David A, Sarasin A, Stalder JF. 1999. Trichothio-dystrophies: Manifestations �evolutives. Ann Dermatol Venereol 126:703–707.
Giglia-Mari G, Coin F, Ranish JA, Hoogstraten D, Theil A, Wijgers N,Jaspers NG, Raams A, Argentini M, van der Spek PJ, Botta E, Stefanini M,Egly JM, Aebersold R, Hoeijmakers JH, Vermeulen W. 2004. A new, tenthsubunit of TFIIH is responsible for the DNA repair syndrome tricho-thiodystrophy group A. Nat Genet 36:714–719.
Happle R, Traupe H. 1984. The Tay syndrome (congenital ichthyosis withtrichothiodystrophy). Eur J Pediatr 141:147–152.
Hersh JH, Klein LR, Joyce MR. 1993. Trichothiodystrophy and associatedanomalies: A variant of SIBIDS or new symptom complex? PediatrDermatol 10:117–122.
Howell RR, Arbisser AI, Parsons DS, Scott CI, Fraustadt U, Collie WR,Marshall RN, Ibarra OC. 1981. The Sabinas syndrome. Am J Hum Genet33:957–967.
Htun H, Barsony J, Renyi I, Gould DL, Hager GL. 1996. Visualization ofglucocorticoid receptor translocation and intranuclear organization inliving cells with a green fluorescent protein chimera. Proc Natl Acad SciUSA 93:4845–4850.
Itin PH, Pittelkow MR. 1990. Trichothiodystrophy: Review of sulfur-deficient brittle hair syndromes and association with the ectodermaldysplasias. J Am Acad Dermatol 22:705–717.
Itin PH, Sarasin A, Pittelkow MR. 2001. Trichothiodystrophy: Update onthe sulfur-deficient brittle hair syndromes. J Am Acad Dermatol44:891–920.
Jackson CE, Weiss L, Watson JH. 1974. Brittle hair with short stature,intellectual impairment and decreased fertility: An autosomal recessivesyndrome in an Amish kindred. Pediatrics 54:201–207.
Jorizzo JL, Crounse RG, Wheeler CE. 1980. Lamellar ichthyosis, dwarfism,mental retardation and hair shaft abnormalities. A link between theichthyosis-associated and BIDS syndromes. J Am Acad Dermatol2:309–317.
Jorizzo JL, Atherton DJ, Crounse RG, Wells RS. 1982. Ichthyosis, brittlehair, impaired intelligence, decreased fertility and short stature (IBIDSsyndrome). Br J Dermatol 106:705–710.
Keriel A, Stary A, Sarasin A, Rochette-Egly C, Egly JM. 2002. XPDmutations prevent TFIIH-dependent transactivation by nuclear recep-tors and phosphorylation of RAR alpha. Cell 109:125–135.
King MD, Gummer CL, Stephenson JBP. 1984. Trichothiodystrophy-neurotrichocutaneous syndrome of Pollitt: A report of two unrelatedcases. J Med Genet 28:514–520.
Kleijer WJ, Beemer FA, Boom BW. 1994. Intermittent hair loss in a childwith PIBI(D)S syndrome and trichothiodystrophy with defective DNArepair-xeroderma pigmentosum group D. Am J Med Genet 52:227–230.
Kousseff BG. 1991. Collodion baby, sign of Tay syndrome. Pediatrics87:571–574.
Laine JP, Egly JM. 2006. When transcription and repair meet: A complexsystem. Trends Genet 22:430–436.
Lehmann AR, Arlett CF, Broughton BC, Harcourt SA, Steingrimsdottir H,Stefanini M, Malcolm A, Taylor R, Natarajan AT, Green S, King MD,MacKie RM, Stephenson JBP, Tolmie JL. 1988. Trichothiodystrophy, ahuman DNA repair disorder with heterogeneity in the cellular responseto ultraviolet light. Cancer Res 48:6090–6096.
Liu Y, Ando S, Xia X, Yao R, Kim M, Fondell J, Yen PM. 2005. p62, A TFIIHsubunit, directly interacts with thyroid hormone receptor and enhancesT3-mediated transcription. Mol Endocrinol 19:879–884.
Lucky PA, Kirsch N, Lucky AW, Carter DM. 1984. Low-sulfur hairsyndrome associated with UVB-sensitivity and testicular failure. J AmAcad Dermatol 11:340–346.
Lynch SA, De Berker D, Lehmann AR, Pollitt RJ, Reid MM, Lamb WH.1995. Trichothiodystrophy with sideroblastic anemia and developmentaldelay. Arch Dis Child 73:249–251.
Malvehy J, Ferrando J, Soler J, Tuneu A, Ballesta F, Estrach T. 1997.Trichothiodystrophy associated with urologic malformation and prima-ry hypercalciuria. Pediatr Dermatol 14:441–445.
Marinoni S, Tr�evisan G, Gaeta G, Not T, Lagomarsini P, Stefanini M,Nazarro V, Ermacora E. 1990. Trichothiodystrophy associated withgroup D xeroderma pigmentosum in seven Italian patients. Bordeaux:Third Congress of the European Society for Paediatric Dermatology.
Mazereeuw-Hautier J, Pech JH, Heitz F, Bonafe JL. 2002. Trichothiody-strophie et cardiopathie cong�enitale chez deux s?urs. Ann DermatolVenereol 129:1168–1171.
McCuaig C, Marcoux D, Rasmussen JE, Werner MM, Gentner NE. 1993.Trichothiodystrophy associated with photosensitivity, gonadal failure,and striking osteosclerosis. J Am Acad Dermatol 28:820–826.
Meynadier J, Guillot B, Barneon G, Djian B, Levy A. 1987. Trichothio-dystrophie. Ann Dermatol Venereol 114:1529–1536.
Motley RJ, Finlay AY. 1989. A patient with Tay’s syndrome. PediatrDermatol 6:202–205.
MORICE-PICARD ET AL. 2029

Nakabayashi K, Amann D, Ren Y, Saarialho-Kere U, Avidan N, GentlesS, MacDonald JR, Puffenberger EG, Christiano AM, Martinez-Mir A,Salas-Alanis JC, Rizzo R, Vamos E, Raams A, Les C, Seboun E, Jaspers NG,Beckmann JS, Jackson CE, Scherer SW. 2005. Identification of C7orf11(TTDN1) gene mutations and genetic heterogeneity in nonphotosensi-tive trichothiodystrophy. Am J Hum Genet 76:510–516.
Nishiwaki Y, Kobayashi N, Imoto K, Iwamoto TA, Yamamoto A, KatsumiS, Shirai T, Sugiura S, Nakamura Y, Sarasin A, Miyagawa S, Mori T. 2004.Trichothiodystrophy fibroblasts are deficient in the repair of ultraviolet-induced cyclobutane pyrimidine dimers and (6–4) photoproducts. JInvest Dermatol 122:526–532.
Peserico A, Battistella PA, Bertoli P. 1992. MRI of a very rare hereditaryectodermal dysplasia: PIBI(D)S. Neuroradiology 34:316–317.
Petrin JH, Meckler KA, Sybert VP. 1998. A new variant of trichothiodys-trophy with recurrent infections, failure to thrive, and death. PediatrDermatol 15:31–34.
Pollitt RJ, Jenner FA, Davies M. 1968. Sibs with mental end physicretardation and trichorrhexis nodosa with abnorma amino acid compo-sition of the hair. Arch Dis Child 43:211–216.
Price VH, Odom RB, Ward WH, Jones FT. 1980. Trichothiodystrophy:Sulfur-deficient brittle hair as a marker for a neuroectodermal. ArchDermatol 116:1375–1384.
Przedborski S, Ferster A, Goldman S. 1990. Trichothiodystrophy, mentalretardation, short stature ataxia and gonadal failure in 3 Moroccansiblings. Am J Med Genet 35:566–573.
Raff EC, Fuller MT, Kaufman TC, Kemphues KJ, Rudolph JE, Raff RA.1982. The testis-specific beta-tubulin subunit in Drosophila melanogast-er has multiple functions in spermatogenesis. Cell 28:33–40.
Rebora A, Guarrera M, Crovato F. 1986. Amino acid analysis in hair fromPIBID(S) syndrome. J Am Acad Dermatol 15:109–111.
Rezvani HM, Cario-Andr�e M, Pain C, Ged C, deVerneuil H, Taieb A. 2007.Protection of human reconstructed epidermis from UV by catalaseoverexpression. Cancer Gene Ther 14:174–186.
Rezvani HR, Ged C, Bouadjar B, de Verneuil H, Ta€ıeb A. 2008. Catalaseoverexpression reduces UVB-induced apoptosis in a human xerodermapigmentosum reconstructed epidermis. Cancer Gene Ther 15:241–251.
Rizzo R, Pavone L, Micali G, Calvieri S, Di Gregorio L. 1992. Trichothiodys-trophy: Report of a new case with severe nervous system impairment. JChild Neurol 7:300–303.
Sarasin A, Blanchet-Bardon C, Renault G, Lehmann A, Arlett C, Dumez Y.1992. Prenatal diagnosis in a subset of trichothiodystrophy patientsdefective in DNA repair. Br J Dermatol 127:485–491.
Savary JB, Vasseur F, Vinatier D, Manouvrier S, Thomas P, Deminatti MM.1991. Prenatal diagnosis of PIBIDS. Prenat Diagn 11:859–866.
Schepis C, Elia M, Siragusa M, Barbareschi M. 1997. A new case oftrichothiodystrophy associated with autism seizures and mental retar-dation. Pediatr Dermatol 14:125–128.
Schultz P, Fribourg S, Poterszman A, Mallouh V, Moras D, Egly JM. 2000.Molecular structure of human TFIIH. Cell 102:599–607.
Stefanini M, Lagomarsini P, Arlett CF, Marinoni S, Borrone C, Crovato F,Tr�evisan G, Cordone G, Nuzzo F. 1986. Xeroderma pigmentosum(complementation group D) mutation is present in patients affectedby trichothiodystrophy with photosensitivity. Hum Genet 74:107–112.
Stefanini M, Giliani S, Nardo T, Marinoni S, Nazzaro V, Rizzo R, Tr�evisanG. 1992. DNA repair investigations in nine Italian patients affected bytrichothiodystrophy. Mutat Res 273:119–125.
Stefanini M, Lagomarsini P, Giliani S, Nardo T, Botta E, Peserico A, KleijerWJ, Lehmann AR, Sarasin A. 1993. Genetic heterogeneity of the excisionrepair defect associated with trichothiodystrophy. Carcinogenesis 14:1101–1105.
Takayama K, Danks DM, Salazar EP, Cleaver JE, Weber CA. 1997. DNArepair characteristics and mutations in the ERCC2 DNA repair andtranscription gene in a trichothiodystrophy patient. Hum Mutat9:519–525.
Tay CH. 1971. Ichthyosiform erythroderma, hair shaft abnormalities andmental and growth retardation: A new recessive disorder. Arch Dermatol104:201–207.
Toelle SP, Valsangiacomo E, Boltshauser E. 2001. Trichothiodystrophywith severe cardiac and neurological involvement in two sisters. Eur JPediatr 160:728–731.
Tolmie JL, de Berker D, Dawber R, Galloway C, Gregory DW, Lehmann AR,McClure J, Pollitt RJ, Stephenson JB. 1994. Syndromes associated withtrichothiodystrophy. Clin Dysmorphol 3:1–14.
Tr�evisan G, Marinoni S, Capelli E, Gandini A, Levi N. 1983. Fotosensibilita,alterazioni immunologiche e anomalie dei capelli in due sorelle. BollDermatol Podiatr 2:153.
Van Neste D, Bore P. 1983. Trichothiodystrophy: A morphological andbiochemical study. Ann Dermatol Venereol 110:409–417.
Van Neste D, Miller X, Bohnert E. 1989. Clinical symptoms associated withtrichothiodystrophy: A review of the litterature with special emphasis onlight sensitivity and the association with xeroderma pigmentosum(complementation group D). Trends Hum Hair Growth Alopecia Res19:183–193.
Vermeulen W, Bergmann E, Auriol J, Rademakers S, Frit P, Appeldoorn E,Hoeijmakers JH, Egly JM. 2000. Sublimiting concentration of TFIIHtranscription/DNA repair factor causes TTD-A trichothiodystrophydisorder. Nat Genet 3:307–313.
Vermeulen W, Rademakers S, Jaspers NG, Appeldoorn E, Raams A, Klein B,Kleijer WJ, Hansen LK, Hoeijmakers JH. 2001. A temperature-sensitivedisorder in basal transcription and DNA repair in humans. Nat Genet27:299–303.
Viprakasit V, Gibbons RJ, Broughton BC, Tolmie JL, brown D, Lunt P,Winter RM, Marinoni S, Stafanini M, Brueton L, Lehmann AR, HiggsDR. 2001. Mutations in the general transcripttion factor TFIIH result inbeta-thalassemia in individuals with trichothiodystrophy. Hum MolGenet 10:2797–2802.
Vuillaume M, Daya¼Grosjean L, Vincens P, Pennetier JL, Tarroux P, BaretA, Calvayrac R, Taieb A, Sarasin A. 1992. Striking differences in cellularcatalase activity between two DNA repair-deficient diseases: Xerodermapigmentosum and trichothiodystrophy. Carcinogenesis 13:321–328.
Wakeling EL, Cruwys M, Suri M, Brady AF, Aylett SE, Hall C. 2004. Centralosteosclerosis with trichothiodystrophy. Pediatr Radiol 34:541–546.
Weeda G, Eveno E, Donker I, Vermeulen W, Chevallier-Lagente O, Taieb A,Stary A, Hoeijmakers JH, Mezzina M, Sarasin A. 1997. A mutation in theXPB/ERCC3 DNA repair transcription gene, associated with trichothio-dystrophy. Am J Hum Genet 60:320–329.
Zhang Y, Tian Y, Chen Q, Chen D, Zhai Z, Shu HB. 2007. TTDN1 is Plk1-interacting protein involved in maintenance of cell cycle integrity. CellMol Life Sci 64:632–640.
2030 AMERICAN JOURNAL OF MEDICAL GENETICS PART A