



Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 1 ~

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 2 ~
Chief Editor
Mr. Sagar Aryal
(Founder)
Ambassador, iversity
M.Sc. Medical Microbiology
St. Xavier’s College, Nepal
Editors
Mr. Saumyadip Sarkar
ELSEVIER Student Ambassador South Asia 2013
Ph.D Scholar (Human Genetics), India
Mr. Avishekh Gautam
Ph.D Scholar
Hallym University, South Korea
Mr. Manish Thapaliya
Ph.D Scholar, China
Mr. Hasnain Nangyal
M.Phil.
Department of Botany, Hazara University, Pakistan
Mr. Sunil Pandey
ELSEVIER Student Ambassador South Asia 2014
B.Sc. Medical Microbiology
Nobel Medical College, Nepal

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 3 ~

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 4 ~
Table of Content
Page No.
Microbial Indicators: Role in monitoring
of drinking water quality and health prospects 5-8
Prevalence and prevention of thalassemia
in Khyber-Pakhtunkhwa, Pakistan 9-11
Do you have cold? Fomites may be responsible 12-13
Chinese Salt 14-19
Prions: The Killer Proteins 20-28
Hybridoma Technology: A Tool in immunotherapy 29-37
Lyophilisation: A Method of Preserving Biologicals 38-43
Rapid diagnosis of acute respiratory infections by
multiplex endpoint PCR technology 44-47
Bioweapons: A new trend in emerging Sciences 48-58

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 5 ~
Microbial Indicators: Role in monitoring of
drinking water quality and health prospects
Gaurav Saxena, Rohan Kanaujia and Ram Naresh Bharagava*
Department of Environmental Microbiology (DEM), School for Environmental Sciences
(SES), Babasaheb Bhimrao Ambedkar University (A Central University), Vidya Vihar,
Raebareli Road, Lucknow 226 025 (U.P.), India
Correspondence E-mail Address: [email protected]
Ensuring the safety of drinking water is an ongoing process. Water that looks perfectly
transparent and clean may be contaminated with pathogens, which may cause serious health
hazards. A clean and safe drinking water supply may be the norm in European and American
countries, but in developing countries, the assessment of clean water is not the rule and
therefore, the waterborne illness outbreaks are common. It is reported that around two and a
half billion people have no access of improved sanitation and more than 1.5 million children die
each year from diarrheal diseases (Fenwick 2006).
A number of disease occur due to contamination of drinking water with urban sewage, feces of
infected humans and animals having different kinds of microorganisms, which are termed as
enteric pathogens. However, the detail information on waterborne pathogens can be found in
Cabral (2010). These include enteric bacteria, viruses and protozoa’s and can be transmitted by
exposure to domestic waste either through swimming in contaminated water, ingesting
contaminated water or eating vegetables that has been irrigated with contaminated water or
grown in contaminated soil (WHO 2008). In general, any practice that involves the application of
domestic wastewater in soil has potential to cause microbial contamination of ground water
since treatment processes applied do not completely remove/inactivate microbial pathogens in
wastewater (Figueras & Borrego 2010).
The examination of drinking water for the presence of indicator microorganisms is a key to
determine the microbiological quality and public health safety because their presence indicate
the potential faecal contamination of water with pathogens and an index of quality deterioration.

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 6 ~
Indicator microorganisms are generally not themselves human pathogens (Verhille 2013). This
has been the foundation upon which the protection of public health from waterborne diseases
has been developed. The most widely used indicator microorganisms are coliforms (total
coliforms), faecal or thermo-tolerant coliforms, Escherichia coli, enterococci (Faecal streptococci
or Intestinal enterococci) and bacteriophages. Further, the detail information on microbial
indicators can be found in Cabral (2010) and Figueras & Borrego (2010) (Fig. 1).
Fig. 1: Microbial indicators in drinking water: Total coliform, faecal coliform and E. coli
Adapted from (Verhille 2013)
The criteria for a microorganism to act as an ideal indicator of pathogens in water environment
are as follows (Cabral 2010):
a. The organism should be present whenever enteric pathogens are present and absent
whenever pathogens are absent.
b. The organism present at a density that has some constant direct relationship to the
density of pathogens.
c. The organism should be useful for the analysis of all types of contaminated
environmental waters.
d. The organism should not grow in contaminated water.
e. The organism should be non-pathogenic to humans and easily identifiable.

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 7 ~
f. The organism should survive in environment as long as possible.
g. The organism should be the member of intestinal micro-flora of warm-blooded animals.
h. The organism should exist in high number in human intestine as well as in feces.
i. The organism should be detectable by easy, rapid and specific/sensitive, but
economically viable methods
In addition, the potential application of an indicator microorganism should be to indicate:
a. The fecal pollution.
b. The presence of domestic sewage.
c. The presence of microbial pathogens.
d. The efficiency of a particular water or wastewater treatment process.
e. The environmental fate of a target pathogen.
However, whether these indicator bacteria are the suitable indicator of human pathogens, it has
been questioned because of some serious limitations they include (Girones et al., 2010):
a. Sensitive to inactivation through wastewater treatment processes and sunlight exposure.
b. Short survival period as compared to microbial pathogens.
c. Not indicative of exclusive faecal source.
d. Ability to multiply in some natural environments.
e. Inability to recognize faecal contamination source (point or non-point).
f. Less correlation with pathogenic presence.
Further, it is also reported that the drinking water illness outbreaks have occurred both in
presence or absence of indicator microorganisms and involved pathogenic microorganisms that
have contaminated the drinking water and that either were not eliminated during the treatment
process or later failed at the time of outbreak (Figueras and Borrego 2010). These outbreaks
occurred despite the specific legislations that have been designed to prevent them (Figueras
and Borrego 2010).
The World Health Organization (WHO) is an active body in this field and has already published
many guidelines/documents in collaboration with International Water Association (IWA) and

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 8 ~
“Organization for Economic Co-operation and Development (OECD)” for improvement in
drinking water quality (WHO 2008). Water safety plan is the most recent that ensure the safety
of drinking water and can be found in the WHO technical guidance document and also available
in WHO directory.
Nevertheless, the presence of indicator microorganisms will likely continue to be used as a
criterion of drinking water quality. Although, there is no any perfect indicator microorganism and
research is ongoing to find a suitable microorganism that can act as a better indicator for the
presence of waterborne pathogens.
Acknowledgement
The authors are highly grateful to University Grants Commission (UGC), Government of India
(GOI) New Delhi for financial support as “Start-Up grant” for this work and UGC Fellowship
received by Mr. Gaurav Saxena is also duly acknowledged.
References
1. Cabral, J. P. S. (2010) Water Microbiology. Bacterial Pathogens and Water. Int. J.
Environ. Res. Public Health 7, 3657-3703.
2. Fenwick, A. (2006) Waterborne Diseases: could they be consigned to history. Science
313, 1077-1081.
3. Figueras, M. J., & Borrego J. J. (2010) New Perspectives in Monitoring Drinking Water
Microbial Quality. Int. J. Environ. Res. Public Health 7, 4179-4202.
4. Girones, R., Ferrus, M. A., Alonso, J. L., Manzano, J. R., Calgua, B., Correa, A. D. A.,
Hundesa, A., Carratala, A., & Bofill-Mas, S. (2010) Molecular detection of pathogens in
water- The pros and cons of molecular techniques. Water Res. 44, 4325-4339.
5. Verhille, S. (2013) Understanding microbial indicators for drinking water assessment:
interpretation of test results and public health significance. National collaborating centre
for environmental health. 1-12.
6. World Health Organization. (2008) Guidelines for drinking water quality. 3rd edn. (1)
Geneva, Switzerland.

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 9 ~
Prevalence and prevention of thalassemia in
Khyber-Pakhtunkhwa, Pakistan
1Maria Zubair, 2Tahir Hussain
1Peshawar Medical and Dental College, Warsak Road Peshawar, Khyber-
Pakhtunkhwa, Pakistan
2Atta-ur-Rahman School of Applied Biosciences, National University of Sciences and
Technology, Islamabad, Pakistan
Abstract:
Thalassemia is an inherited autosomal recessive blood disorder characterized by formation of
abnormal haemoglobin which in turn leads to destruction of RBCs. Since it is a recessive trait
and can be controlled, if planned properly, but because of lack of awareness and certain
traditional and cultural practices thalassemiac babies are still reported from rural population of
Khyber-Pakhtunkhwa province Pakistan. This report discusses the prevalence and various
treatment options available for thalassemia patients in a treatment center at Khyber-
Pakhtunkhwa, Pakistan.
Introduction:
Thalassemia is a form of inherited blood disorders, caused by weakening and destruction of
RBCs (Red Blood Cells). The genetic determinants for thalassemia are present on autosomes
and the condition arises when the genes are missing or variant of the genes are present. This
causes the malfunction of the body to make normal haemoglobin (Hb). Life span of Red Blood
cells (RBC) with normal haemoglobin (Hb) is 120 days while in thalassemia it becomes 10 to 15
days only.
Normally the majority of adult hemoglobin <Hb A> is composed of four protein chains i.e; two
alpha and two beta globin chains arranged in a hetrotetramer form. In thalassemia, patients
have defect either in alpha or beta globin chain causing production of abnormal RBC.

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 10 ~
Common treatment options available in Pakistan:
1. Blood transfusion: Blood transfusion is a common option available for extending life
expectancy of thalassemiacs. Since thalassemia patients need regular blood transfusions to
sustain their life and multiple transfusions can result in iron overload which then results in
severe physiological dysfunctions in the body.
2. Bone marrow transplantation: Bone marrow transplantation offers about 70% success rates in
pakistan1. However it is an expensive surgery and costs about Rs. 30 lac in Pakistan1.
3. Hydroxy urea: This drug is generally used in treatment of leukemia, breast cancer and
malignancy. However, recently, this drug was found to be effective against thalassemia as well1.
According to the research, about 60% of patients didn’t need further blood transfusion while in
remaining 40% there was decreased rate of blood transfusion noticed1.
As a case study in Hamza foundation Peshawar, a welfare organization providing healthcare
services to thalassemiac children, exercised the hydroxy urea treatment strategy on about 160
patients, out of them 31 patients are not receiving any further blood transfusion from past 9
months1. However certain side effects of this drug, such as, leukocytopenia and bone marrow
depression were noticed1.
Prevalence: About 823 thalassemiac patients from all over Khyber-Pakhtunkhwa, Pakistan,
registered at Hamza Foundation in seven years period1. These figures are available only on our
record. Of course there could be many more thalassemiac patients struggling for their life. 95%
of the thalassemiac patients belong to poor, deserving and uneducated class1. It is a
troublesome disease common in children and young patients with extremely high mortality rate.
Prevention: Prevention could be a better alternative as compared to expensive treatment.
Since thalassemia is a hereditary condition so controlling thalassemia in the population will only
be possible if thalassemia free babies are delivered. For this reason we need to take certain
measures in order to prevent thalassemia in the coming generations.
1. Family marriages: Cousin marriages are quite common in villages and poor set up. For
this purpose government should play its role in educating people about the hazards
resulting from cousin marriages.

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 11 ~
2. Pre marriage screening: All the first and second relatives of known thalassemia patients
should be screened. If they are diagnosed with diseased or carriers, their record should
be kept in view so that they must not marry member from other thalassemiac family.
3. Prenatal screening: If a thalassemiac couple gets expected they must undergo prenatal
screening i.e; CVS (Chorionic Villus Sampling) during first trimester. If the fetus is
diagnosed as thalassemiac major then it must be aborted. Healthcare authorities and
ethical bodies agree all over the world that aborting a fetus in certain conditions like for
saving life of mother or if fetus is diagnosed to b abnormal is not illegal.
4. Spreading the awareness: Generally uneducated people in our population do not know
the basic information regarding thalassemia. They should be properly educated about
the causes and ways to prevent thalassemia. Awareness campaign should be launched
through both electronic and print media. Radio, Tele vision, daily newspapers,
magazines, distributing pamphlets, conducting seminars, guiding imam masjids,
chodries and khans to educate people in their communities.
Acknowledgement:
We are grateful to Dr. Tariq khan, Hamza Foundation, for providing data about thalassemia
patients.
References:
Hamza Foundation, 2-A Park Avenue, University Town Peshawar, Khyber-Pakhtunkhwa
Pakistan.

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 12 ~
Do you have cold? Fomites may be responsible
Oyediji Kehinde Eyitayo
University of Abuja, Abuja, Nigeria
The common cold is a viral infectious disease of the upper respiratory tract which primarily
affects the nose. A cold usually begins with fatigue, a feeling of being chilled, sneezing and a
headache, followed in a couple of days by a runny nose and cough, nasal congestion and a
sore or scratchy throat, sometimes accompanied by loss of appetite, sneezing, hoarseness,
watery eyes, low-grade fever, headache, and body aches. Symptoms may begin within 16 hours
of exposure and typically peak two to four days after onset. The symptoms of the common cold
will typically last anywhere from 4-14 days, with most individuals improving in one week. The
common cold is the most common human disease and all peoples globally are affected. The
common cold is generally mild and self-limiting with most symptoms generally improving in a
week.
The common cold virus is typically transmitted via airborne droplets (aerosols), direct contact
with infected nasal secretions, or fomites. Diseases that spread by droplet transmission, fecal–
oral transmission, or contact transmission often do so by means of fomites. Germs commonly
live on fomites for minutes or hours or sometimes even longer.
Fomites are inanimate objects that can carry pathogenic agents from one susceptible source to
another. These objects can be anything, such as a handset, door knobs (handle), laboratory
benches, laptop keypads, ATM machines, money, clothes, dishes, books, pens, silverware, or
escalator hand rail. A cold virus can live on objects for several hours and can thus be acquired
from contact with these objects. Fomite transmission works best on hard, durable surfaces like
dishes, books, door knobs, telephones, and hand rails, all of which people come in contact with
on a daily basis.
Regular hand washing appears to be effective in reducing the transmission of cold viruses. Not
touching the nose or eyes is another. Individuals with colds should always sneeze or cough into

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 13 ~
a facial tissue, and promptly throw it away. If possible, one should avoid close, prolonged
exposure to persons who have colds.
In the laboratory and other healthcare environments, gowns and disposable gloves are also
used. Isolation, e.g. quarantine, is not possible as the disease is so widespread and symptoms
are non-specific. Vaccination has proved difficult as over 200 different viral types are associated
with colds and they mutate rapidly. Creation of a broadly effective vaccine is thus highly
improbable. Zinc supplements may help to reduce the prevalence of colds. Routine vitamin C
supplements do not reduce the risk or severity of the common cold, though they may reduce its
duration. Because common cold viruses can survive up to three hours outside the nasal
passages on inanimate objects and skin, cleaning environmental surfaces with a virus-killing
disinfectant might help prevent spread of infection.
No medications or herbal remedies have been conclusively demonstrated to shorten the
duration of infection. Treatment thus comprises symptomatic relief. Getting plenty of rest,
drinking fluids to maintain hydration, and gargling with warm salt water, are reasonable
conservative measures. One study has found chest vapor rub to provide some relief of
nocturnal cough, congestion, and sleep difficulty. Treatments that help alleviate symptoms
include simple analgesics and antipyretics such as ibuprofen and acetaminophen/paracetamol.
Other decongestants such as pseudoephedrine are also effective in adults. Ipratropium nasal
spray may reduce the symptoms of a runny nose but has little effect on stuffiness. Much of the
benefit from treatment is however attributed to the placebo effect.
Antibiotics have no effect against viral infections and thus have no effect against the viruses that
cause the common cold. Due to their side effects antibiotics cause overall harm, but are still
frequently prescribed. Some of the reasons that antibiotics are so commonly prescribed include
people's expectations for them, physicians' desire to help, and the difficulty in excluding
complications that may be amenable to antibiotics. There are no effective antiviral drugs for the
common cold even though some preliminary research has shown benefits.

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 14 ~
Chinese Salt 1Ammara Nawaz, 2Hasnain Nangyal, 3Sikander Khan Sherwani,
4Noor Nasir Khattak
1Department of Zoology Punjab University
2Department of Botany Hazara University Mansehra Khyber Pakhtoonkhwa
3Department of Microbiology Fedral Urdu University of Arts Science & Technology
Karachi
4Assistant Professor Gynecology and Obstetrics Kohat Medical College Khyber Medical
University
To say the history of salt is essentially the history of the world is not an overstatement. Some
call salt a "primordial condiment," and rightfully so. It has been part of this earth for as long as
there has been water and rock to create it. It has been a highly-valued commodity that served
many purposes, but perhaps the most useful and powerful purpose is preservation. Salt has an
uncanny ability to preserve just about anything, a vegetable or even a human cadaver. In the
history some riots for salt are also been observed.
Several types of salts are used by man in foods and for different applications also. Some of
them are Iodized table salt, table salt, sea salt, kosher salt, Chinese salt, pickling salt, black salt,
Himalayan pink salt, flake salt, smoked salt, seasoned salt, Hawaiian salt and many more.
Chinese salt is now a days a widely used salt in dishes. It is a white crystalline substance the
sodium salt of glutamic acid that has little flavour itself but enhancesthe flavour of proteins either
by increasing the amount of saliva produced in the mouth or by stimulating the taste buds used
as a food additive especially in Chinese Formula: NaC5H8O4. It is also called sodium glutamate
with abbreviation MSG.
History of Chinese salt
First stage of the story begins in 1908 with chemist Ikeda Kikunae’s isolated this ingredient in
sea kelp that gave flavor to konbu dashi, the standard Japanese broth. The product that

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 15 ~
emerged from Ikeda’s laboratory, Monosodium glutamate was quickly patented in Japan, the
United States, England, and France. In domestic announcements of his invention, Ikeda
proposed calling its distinctive taste umami a term derived from the word in Japanese meaning
“tasty.” Ikeda brought the powdered substance to iodine manufacturer Suzuki Saburo, whose
Suzuki Chemical Company began marketing it in 1909 under the brand name Ajinomoto,
meaning “essence of taste.”
Fig. 1: Varieties of salts used by man.
What are glutamates?
Glutamate is one of the most general amino acids found in nature. It is the main component of
many proteins and peptides, and is present in most tissues. Glutamate is also produced in the
body and plays an essential role in human metabolism. Virtually every food contains glutamate.
It is a major component of most natural protein foods such as meat, fish, milk and some
vegetables. This amino acid has a flavor enhancing property in both free and combined state. It

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 16 ~
is a major component of MSG, so when MSG is added into any food its flavor is enhanced due
to presence of glutamate in it giving food an Umami flavor which is a meaty taste.
MSG and our Metabolism
Our body is capable to digest MSG as it is capable to digest the naturally present amino acid
glutamate. Our body metabolizes glutamate easily. Once glutamate has entered into the body of
a human it metabolizes it and can’t distinguish between the origins of the amino acid. If it is a
part of a tomato or MSG added into the food.
MSG is low in sodium
It is a popular belief that MSG contains high percentage of sodium ions .Actually MSG contains
only one third the amount of sodium as compared to table salt. So it is safe to use by high blood
pressure patients, heart patients and many more that can’t afford much sodium in their diet and
also put a little effect on palatability even giving food a meaty more pleasant taste.
Contradictory views about Chinese salt
Many contradictory statements are there related to Chinese salt. Many people even scientists
think that Chinese salt be not good for human health and has some health risks associated to it.
Several aspects of Chinese salt in relation to human health are studied in detail. Some of these
are discussed as below:
Chinese salt and pregnant women
It was once thought that Chinese salt in not good for pregnant females, lactating mothers and
the fetus or placenta. Now various studies have proved that MSG intake has no adverse effect
in all above cases. It is known through deep investigations that the ratio of MSG in the blood
cannot be increased by the intake (Chinese salt). Pitkin a scientist to see the effect of MSG
increase on pregnant females and fetus conducted an experiment. He injected high amount of
MSG in the blood of the Monkey pregnant female and noticed no increase in level of MSG blood
level up to a dose of 220mg\kg of maternal weight. Thus no raise in level of blood MSG and no
effect of it on the female and the fetus were concluded.

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 17 ~
Chinese salt and lactating mothers
No bad effect of Chinese salt was seen in lactating mothers too. By certain experiments this
was proved. Lactating women were given MSG at about 100mg\kg of body weight and its effect
was noticed on the mother and the infant. No increase of level of glutamate in human milk was
seen and no effect was observed on the infant also. Naturally human milk has 10 times more
ratio of glutamate in it as compared to cow’s milk. Thus MSG intake in diet was declared not a
risk for the infants feeding on breast milk.
Chinese salt and its neurological effects
In the brain, glutamate serves as a neurotransmitter in addition to its general role in protein and
energy metabolism. Concerns were raised in the late 1960s by John Olney, M.D., of
Washington University, that high doses of MSG may adversely affect brain function. He
examined the possibility of MSG-induced brain lesions through injection or force-feeding
methods in rodents. But the dosage used in this experiment were very high not comparable to
the amount of glutamate taken up by a man by using Chinese salt in his diet in normal days.
Studies say that an amount of 40g\kg weight of the man of MSG is even safe which is actually
5000 times then normally taken amount by a man.
In another experiment by Bazzano it was also concluded that MSG has no bad effect on
humans. In this experiment 11 humans were given 147g\day of MSG for about 42 days and no
side effects were observed in them.
William Pardridge, M.D pointed up that dietary glutamate does not enter the brain because the
blood-brain barrier maintains a transport system for acidic amino acids, such as glutamate, to
effectively exclude circulating glutamate from the brain. Pardridge also showed that the levels of
brain glutamate do not rise or fall with changes in plasma glutamate levels. This point was
strengthened by many other investigations by many scientists.

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 18 ~
Thus it was concluded that ordinary daily intake level of MSG has no bad effect on human brain
and nervous system.
Chinese salt and hypersensitive reactions
Many people are observed by scientists having allergy to some food products or substance
such as cheese or peanuts etc due to many reasons. Some scientists questioned if Chinese salt
or MSG may be allergic to some people. Several investigations were made to study this
hypothesis.
In 1991, after reviewing the literature on MSG and food allergy and safety, a panel of the
American College of Allergy, Asthma and Immunology concluded that MSG is not an allergen
and reaffirmed its safety as a food ingredient.45. More recently, Ronald Simon, M.D.,
department of allergy and immunology, Scripps Clinic, La Jolla, California, conducted a well-
designed, double-blind, placebo-controlled study of 65 subjects with chronic urticaria. None of
the subjects exhibited positive reactions to doses of 2.5 g of MSG.
Chinese salt in relation to children health
It has been speculated that children would metabolize oral MSG more slowly than adults.
However, research conducted by Stegink and colleagues at the University of Iowa showed that
children as young as one year old metabolize glutamate as effectively as adults.
Chinese salt and Asthma
Early poor studies said that MSG might be a cause of asthma. However further controlled
investigations pointed out that it is not the case. MSG was not a cause of asthma. In an
experiment humans were given 25g\kg weight of MSG per day for a few days. No difference in
pulmonary reactions was noted in these humans.
In 1991 and 1993, researchers from the National Institutes of Health’s Institute of Allergy and
Infectious Diseases presented data analyzing the possible association of MSG to asthma. In
one study, they challenged 13 non-asthmatics and 30 asthmatics with a total dose of 7.6 g of

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 19 ~
MSG. Upon observation, none of the non-asthmatics experienced any change in pulmonary
reactions and only one asthmatic participant experienced some discomfort.
Chinese Restaurant Syndrome (CRS)
In 1968, Robert Ho Man Kwok, M.D., described a collection of symptoms he allegedly
experienced after eating Chinese food. He coined the phrase “Chinese Restaurant Syndrome”
(CRS) to describe these symptoms, which included numbness at the back of the neck and a
feeling of pressure in the face and upper chest muscles. As a consequence of Kwok’s account,
Kerr and colleagues developed a subjective questionnaire to assess the prevalence of CRS in
the population. The survey employed listed 18 adverse symptoms related to food, of which three
were related to CRS. Of the 3,222 general households that responded to the survey, 43 percent
reported food-related adverse reactions, but only 1.8 percent reported possible CRS symptoms.
Richard Kenney, M.D., of George Washington University did a lot of experiments to evaluate the
use of MSG and relation of CRS. He tested 60 people with He further tested 60 subjects with
orange juice, spiced tomato juice, black coffee, flavored milk and a two percent MSG solution.
Upon examining reactions, Kenney found that six subjects responded to coffee, six to spiced
tomato juice and only two to the MSG solution, indicating that MSG was not unique in producing
symptoms typical of CRS. However several people in many experimental studies have been
seen showing some indications of CRS by the uptake of MSG. These include tightness in the
chest, flushing and headache.
Conclusion
MSG is one of the most intensely used food ingredient on today’s culinary world. Numerous
researches have been conducted to see its adverse effects on human body and no concrete
evidence has been found to say that MSG is bad for health in the regular amounts used by the
common man. Chinese salt is safe to eat in a limit as it is mostly used. However excess of MSG
may cause bad results on human health.

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 20 ~
Prions: The Killer Proteins
Mr. Shaikh Rajesh Ali
Assitant Professor, Dept. Of Microbiology, Acharya Prafulla Chandra College,
New Barrackpore, Kolkata -700131
Introduction:
Prions is an acronym for ‘proteinaceous infectious particles’. The term was coined in 1982 by
Stanley B. Prusiner, a neurologist at the University of California at San Francisco, who proposed
that a new type of pathogen consisting solely of protein is responsible for deadly
neurodegenerative diseases called Transmissible Spongiform Encephalopathies (TSEs) and
received the Nobel Prize in medicine in 1997 for his work on them. These include scrapie in
sheep, bovine spongiform encephalopathy (BSE or ‘mad cow disease’) in cattle and Creutzfeldt-
Jakob Disease (CJD) in people.
Chemical Nature of prions:
The chemical nature of the prions, as stated earlier, is considered to be proteinaceous and they
have no nucleic acids of their own. This has been indicated by the various experimental
evidences gathered so far. This aspect of prion has been investigated by treating them with
nucleases (the enzymes that digest nucleic acids) and proteases (the enzymes that digest
proteins). It has been observed that the nucleases have no effect of prion infectivity, whereas
proteases can drastically reduce a prion infectivity. In addition, prions show high resistance to
ionizing and ultraviolet radiations, which act mainly on nucleic acids.
Structure of Prions:
Prion is 100 times smaller than a virus, contains only protein, are heterogenous in size and
density, and can exist in many molecular forms. The protein that prions are made of (PrP) is
found throughout the body, even in healthy people and animals. However, PrP found in
infectious material has a different structure and is resistant to proteases, the enzymes in the
body that can normally break down proteins.

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 21 ~
The normal form of the protein is called PrPC, while the infectious form is called PrPSc — the C
refers to 'cellular' or 'common' PrP, while the Sc refers to 'scrapie', a prion disease occurring in
sheep.
PrPC is a normal protein found on the membranes of cells. It has 209 amino acids (in
humans), one disulfide bond, a molecular weight of 35-36 kDa and a mainly alpha-
helical structure.
The infectious isoform of PrP, known as PrPSc, is able to convert normal PrPC proteins
into the infectious isoform by changing their conformation, or shape; this, in turn, alters
the way the proteins interconnect. Although the exact 3D structure of PrPSc is not known,
it has a higher proportion of β-sheet structure in place of the normal α-helix structure.
Aggregations of these abnormal isoforms form highly structured amyloid fibers, which
accumulate to form plaques.
Synthesis of prion:
The prion is a product of a human gene,
termed the PrP gene, found on
chromosome 20. This gene contains two
exons separated by a single intron.
Exon I and Exon II are transcribed and
the two RNAs ligated into a single
mRNA. This mRNA contains an open
reading frame (ORF) or protein coding region which is translated into the PrP protein. The PrP
protein is a precursor of the prion protein. It is termed PrP 33-35.
The PrP 33-35 undergoes several post-translational events to become the prion protein (PrP
27-30):
a) Glycosylation - at two sites.
b) Formation of a disulfide bond between two cysteine residues.
c) Removal of the N-terminal signal peptide.
d) Removal of the C-terminal hydrophobic segment.

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 22 ~
e) Addition of a phosphatidylinositol glycolipid at the C-terminal.
f) Removal of the N-terminal first 57 amino acids.
In normal cells only the PrP 33-35
protein is synthesized. It is found in
the neural cell membrane where it's
function is to sequester Cu++ ions.
In abnormal ("infected") cells, the
PrP 27-30 is produced from the
PrP 33-35 protein. The PrP 27-30
triggers a series of reactions that
produce more PrP 27-30 proteins,
i.e., PrP 27-30 induces its own
synthesis. In addition to the post
translational modifications, the PrP
27-30 protein differs from the PrP 33-35 protein in a single amino acid residue. Residue 178 in
the PrP 27-30 contains an asparagine residue whereas the PrP 33-35 protein has an aspartate
residue at this position. This causes a conformational change in the PrP 27-30 protein from an
a-helix to a b-sheet. This conformational change in the PrP 27-30 protein has three effects:
a) It imparts to the PrP 27-30 protein the ability to induce the same a-helix to b-sheet
conformation in the PrP 33-35 protein. This is a permanent conformational change. It
thus induces its own "replication."
b) The b-sheet-forming peptides aggregate to form amyloid fibrils.
c) The amyloid fibrils kill thalamus neurons through apoptosis, a programmed series of
events that leads to cell death.
Prion replication mechanism:
The hypothesis that tried to explain how prions replicate in a protein-only manner was the
heterodimer model. This model assumed that a single PrPSc molecule binds to a single PrPC

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 23 ~
molecule and catalyzes its conversion into PrPSc. The two PrPSc molecules then come apart and
can go on to convert more PrPC.
Transmission of prions:
Spread of the disease is via horizontal transmission, i.e., transmission from one person to
another, either directly or by fomites or by ingestion of contaminated meat. These diseases in
humans are now grouped together according to whether they are sporadic, inherited, or
acquired. Most cases of prion disease are sporadic; that is, they arise spontaneously for no
known reason. More rarely prion disease is inherited due to a faulty gene, or acquired by
medical procedures, transfusions, or contaminated food. Sporadic and inherited prion disease
occurs worldwide in all populations. The incidence of sporadic CJD is around 1 per million of
the population per annum; males and females are equally affected. The incidence of the
various acquired prion diseases, however, is more localized to specific groups and populations.
Prion pathway to brain:
The pathway to the brain is a subject of significant research, but currently, no comprehensive
answer exists. In TSE linked to consuming TSE-infected material, it is theorized that once prions
are ingested, they are taken up by the lymphoid tissue that drains the gastrointestinal tract
including Peyer's Patches and other nodes. Prions also have been found in tonsil, spleen and

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 24 ~
appendix. From the lymphatic system, research suggests that prions replicate, access and
move through the autonomic nervous system to the central nervous system. Once in the brain,
the higher concentration of cellular prion protein speeds up the replication process. Prions also
may enter lesions or wounds in the oral cavity and access the vagus nerve as a pathway to the
brain.
Recent laboratory research using fluorescent dye to "brand" scrapie proteins has tracked prions
as they invade nerve cells and then travel along wire-like circuits to points of contact with other
cells. This appears to be the way the prions that cause TSE invade nerve cells and are
transported along neural circuits throughout the nervous system.
Diseases caused by prions:
Affected animal(s) Disease
sheep, goat Scrapie
cattle Bovine spongiform encephalopathy (BSE), mad cow
disease
mink Transmissible mink encephalopathy (TME)

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 25 ~
white-tailed deer, elk, mule deer,
moose Chronic wasting disease (CWD)
cat Feline spongiform encephalopathy (FSE)
nyala, oryx, greater kudu Exotic ungulate encephalopathy (EUE)
ostrich Spongiform encephalopathy
(Not been shown to be transmissible.)
human
Creutzfeldt–Jakob disease (CJD)
iatrogenic Creutzfeldt-Jakob disease (iCJD)
variant Creutzfeldt-Jakob disease (vCJD)
familial Creutzfeldt-Jakob disease (fCJD)
sporadic Creutzfeldt-Jakob disease (sCJD)
Gerstmann–Sträussler–Scheinker syndrome (GSS)
Fatal familial insomnia (FFI)
Kuru
A survey of spongiform diseases:
Classic CJD or Creutzfeldt-Jakob disease (human)
The most prevalent of the spongiform diseases
Occurs spontaneously in 1 out of a million people
10% of cases are inherited mutations in the PRPN gene
Usually strikes people age 50 to 75
Symptoms: dementia, muscle twitching, vision problems
Fatal Familial Insomnia (human)
All cases are inherited mutations in the PrP gene
Usually strikes people age 36 to 61

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 26 ~
Disruption of sleep/wake cycle leads to coma, then death
Scrapie (goats, sheep)
Occurs as infection in genetically susceptible sheep
There is no evidence of spread to humans
BSE or Bovine Spongiform Encephalopathy (cattle)
Also known as "Mad Cow Disease" because infected animals act strangely and can be
aggressive
Spread rapidly through Britain by rendering
Chronic Wasting Disease (deer, elk)
Infectious disease in wild deer and elk primarily in the western United States
Drooling, difficulty swallowing, weight loss
Kuru (human)
Struck members of the Fore tribe in the 1950s and 1960s
Muscle weakness, loss of coordination, tremors, inappropriate episodes of laughter or
crying
Transmitted by ritual cannibalism as part of funeral ceremonies
Diseases caused by prions are known as
spongiform diseases, because the brain
tissue in infected individuals is filled with
holes, giving it a sponge-like appearance.
Although prions are found throughout the
brain, the symptoms of spongiform diseases
vary according to the regions they are most
concentrated in. There are currently no
effective treatments for spongiform diseases
and all are fatal.

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 27 ~
Treatments of prions:
The mechanism of prion replication has implications for designing drugs. Since the incubation
period of prion diseases is so long, an effective drug does not need to eliminate all prions, but
simply needs to slow down the rate of exponential growth. Models predict that the most effective
way to achieve this, using a drug with the lowest possible dose, is to find a drug that binds to
fibril ends and blocks them from growing any further.
Advancements in computer modeling have allowed for scientists to identify compounds which
can serve as a treatment for prion caused diseases, such as one compound found to bind a
cavity in the PrPC and stabilize the conformation, reducing the amount of harmful PrPSc.
Recently, anti-prion antibodies capable of crossing the blood-brain-barrier and targeting
cytosolic prion protein (an otherwise major obstacle in prion therapeutics) have been described.
Possible immunotherapeutic strategies for prion disease
a | Ablation of mature follicular dendritic
cells (FDCs) delays the development of
prion disease in mice. However, treatment
with multiple doses of CpG-containing
oligodeoxynucleotides (CpG ODNs)
produces severe unwanted side-effects,
including immunosuppression, liver
necrosis and thrombocytopaenia. b |
Treatment with the lymphotoxin- receptor
(LT- R)–Ig fusion protein seems to be
better tolerated, but the best protection is
achieved when the fusion protein is
administered immediately after exposure
to prions. c | Vaccination against a self-
protein is difficult because of immune
tolerance, and it has the potential to induce

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 28 ~
autoimmune disease. Mice devoid of the prion protein (PrP) develop high PrP-specific antibody
titres after immunization with PrP-derived peptides or full-length PrP; however, tolerance in wild-
type mice allows the induction of only low titres of PrP-specific antibodies. d | Treatment with
dimeric full-length PrP fused to the Fc portion of human IgG1 (PrP–Fc2) delays the development
of prion disease in transgenic mice, most probably owing to its interaction with the disease-
associated PrP (PrPSc). LT- 1 2, LT heterotrimer; TLR, Toll-like receptor.

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 29 ~
Hybridoma Technology: A Tool in
immunotherapy
Nwabufo Chukwunonso Kingsley
Department of Biochemistry, Faculty of life sciences, University of Benin, Benin city,
Edo state, Nigeria.
Corresponding Email: [email protected]
Abstract
Hybridoma technology involves forming hybrid cell lines (called hybridomas) by fusing an
antibody -producing B cell with a myeloma (B cell cancer) cell that is selected for its ability to
grow in tissue culture and for an absence of antibody chain synthesis. The antibodies produced
by the hybridoma are all of a single specificity and are therefore monoclonal antibodies. These
monoclonal antibody formed can be purified by antigen affinity chromatography. Considerable
advancements in the last 10-15 years have been made to improve the quality and yield of
monoclonal antibody by hybridoma technology such as the use of myelomas that do not secrete
their own antibodies and that therefore do not interfere with the production of the required
antibody. Immunotherapy is the "treatment of disease by inducing, enhancing or suppressing an
immune response". The quest to develop advanced and effective diagnosis and treatment to
certain disease conditions has led to advancement in immunotherapeutic procedures of which
the use of hybridoma technology has widely been credited to. In this so-called Monoclonal
antibody therapy, monoclonal antibody are targeted against specific antigen and thus enhances
the ability of the immune system to suppress the antigen. Some of the targeted disease
conditions in which monoclonal antibody therapy has widely been used include: cancer
(Tositumomab for non-Hodgkins lymphomas), autoimmune diseases (Infliximab and
Adalimumab which are effective in rheumatoid arthritis, crohn`s disease and uclerative Colitis.
Keywords: Hybridoma technology, Monoclonal antibody, Immunotherapy, Monoclonal Antibody
Therapy.

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 30 ~
Introduction
Hybridomas are cells that have been engineered to produce a desired antibody in large
amounts, to produce monoclonal antibodies [1,2]. Monoclonal antibody can be produced by a
technique called hybridoma technology. Hybridoma technology involves forming hybrid cell lines
(called hybridomas) by fusing a specific antibody-producing B- cells with a myeloma(B- cell
cancer) cell that is selected for its ability to grow in tissue culture and for an absence of antibody
chain synthesis. The antibodies produced by the hybridoma are all of single specificity and are
therefore monoclonal antibody [2].
In 1975, Ce`sar Milstein and Georges J. F kohler invented the production of monoclonal
antibodies and they shared the nobel prize of 1984 for medicine and physiology with Niels Kaj
Jerne, who made other contributions to immunology. The term hybridoma was coined by
Leonard Herzenberg during his sabbatical in César Milstein's laboratory in 1976/1977 [1].
Generally, the production of one MAb, using the hybridoma technology, costs between $8,000
and $12,000. The average reasonably SK can generate only 15 to 30 hybridoma fusions per
year, but in an environment where the focus is on diagnostic- or therapeutic-quality MAbs, there
are additional significant limitations than can further decrease throughput [3].
Passive immunity using monoclonal antibody is the largest category of biotechnology developed
chemotherapy. In passive immunity, instead of injecting a specific antigen and inducing the
body to produce an immune response (vaccination), a specific antibody targeted against an
antigen is introduced into the body which enhances the ability of the immune system to
suppress the antigen for example, administering multiple doses of HERCEPTIN, a monoclonal
antibody against breast cancer to a patient diagnosed of breast cancer helps the immune
system to suppress the growth of the cancer cell. This is the basis of the so-called "Monoclonal
Antibody Therapy" which has revolutionalised immunotherapy.
Methodology
Laboratory animals usually mice or rat are injected with an immunizing dose of a specific
antigen. Once the animal is making a good antibody response, the spleen is removed and a cell

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 31 ~
suspension is prepared, lymph node cells may also be used. These cells are fused with a
myeloma cell line by the addition of poly ethylene glycol which promotes membrane fusion. The
myeloma cell is a B cell cancer cell and consequently can grow indefinitely. In addition, the
myeloma cell is deficient in the enzyme HYPOXANTHINE GUANINE PHOSPHORIBOSYL
TRANSFERASE (HPGRT).This is a key enzyme in the biosynthesis of purines and pyrimidines
using the salvage pathway. This means that the myeloma cells can only use the De novo
pathway to synthesize purines and pyrimidines but cannot use the salvage pathway. However,
the spleen cells can use both the De novo and salvage pathway to synthesize purines and
pyrimidines. Only small proportion of the cells fuse successfully. The Fusion mixture is then
cultured in a medium containing HYPOXANTHINE, AMINOPTERIN AND THYMIDINE called a
HAT - MEDIUM.
Aminopterin blocks De novo pathway of purine and pyrimidine synthesis. However this pathway
can be bypassed in favour of the salvage pathway by the provision of hpoxanthine and
thymidine in the HAT medium. The spleen cells can grow in the HAT medium using the salvage
pathway but myeloma cells cannot grow in the HAT medium because they are incapable of
using the salvage pathway due to the deficiency of the enzyme HPGRT. They therefore die in
the HAT medium. When the culture was set up in the HAT-medium, it contains spleen cells,
myeloma cells and fused cells. The unfused spleen cells die in culture naturally after 1-2 weeks.
Unfused myeloma cells are killed by the HAT-medium but fused cells survive as they have the
immortality of the myeloma and the ability of spleen cells to use the salvage pathway for purine
and pyrimidine biosynthesis. Some of the fuse cells or hybridoma will also have the antibody
producing capacity of the spleen cells.
Any wells containing growing cells are tested for the production of the desired antibody and if
positive, the cultures are cloned, that is, plated out so that only one cell is in each well. This
produces a clone of cells derived from a single progenitor which is both immortal and produces
monoclonal antibody.

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 32 ~
Purification of Monoclonal
Antibodies
Monoclonal antibodies may need
to be purified before they are
used for a variety of purposes.
Before final purification, the
cultures may be subjected to cell
fractionation for enrichment of
the antibody protein. In E. coli,
the antibodies may be secreted
in the periplasm, which may be
used for enrichment of antibody,
so that further purification is
simplified. Alternatively the
antibodies may be purified from
cell homogenate or cell debris
obtained from the medium. (6, 7)
Antibodies can be purified by
anyone of the following techniques
(I) ion-exchange chromatography;
(II) antigen affinity chromatography
Advancements in Hybridoma Technology
Considerable efforts during the last 10-15 years have been made to improve the yield of
monoclonal antibodies using hybridoma technology [4, 5]. These efforts include the following:
(1) The substitution of a chemical fusion promoter (P.E.G.) for the Sendai virus initially used to
promote fusion, and
(2) The use of myelomas that do not secrete their own antibodies and that therefore do not
interfere with the production of the required antibody

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 33 ~
(3) A continuous cell line (Sp 2/0) was used as a fusion partner for the antibody producing B
cells.
(4) Feeder layers consisting of extra cells to feed newly formed hybridomas were used for
optimal growth and hybridoma production. Advancements OR Improvements in Hybridoma
Technology – Considerable efforts during the last 10-15 years have been made to improve the
yield of monoclonal antibodies using hybridoma technology. The most common feeder layers
consist of:
• murine peritoneal cells,
• marcrophages derived from mouse, rat or guinea pig
• extra non immunized spleen cells,
• human fibroblasts, human peripheral blood monocytes or thymus cells; these feeder cells had
some limitations like depletion of nutrients meant for hybridoma and contamination, so that other
sources of hybridoma growth factors (HGF) like interleukin-6 (II-6) derived from human cells
were used.
Application of Hybridoma Technology in Immunotherapy
The production of monoclonal antibody by hybridoma technology makes this technology an
indispensable tool in immunotherapy. The quest to develop advanced and effective diagnosis
and treatment to certain disease conditions has led to advancement in immunotherapeutic
procedures of which the use of hybridoma technology has widely been credited to.
Immunotherapy is the "treatment of disease by inducing, enhancing, or suppressing an immune
response" [8]. Immunotherapies designed to elicit or amplify an immune response are classified
as activation immunotherapies, while immunotherapy’s that reduce or suppress are classified as
suppression immunotherapy’s [9]. There are several types of immunotherapy’s including,
monoclonal antibody, and nonspecific immunotherapy and Cancer vaccines [9]. We shall look at
applications of monoclonal antibody in immunotherapy. Immunotherapy developed as a
technique with the discovery of the structure of antibodies and the development of hybridoma
technology, which provided the first reliable source of monoclonal antibodies, and allowed
therapeutic development since the 1970s [10, 11]. These advances allowed for the specific

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 34 ~
targeting of tumors both in vitro and in vivo. Initial research on malignant neoplasms found MAb
therapy of limited and generally short-lived success with malignancies of the blood [12, 13].
Furthermore treatment had to be specifically tailored to each individual patient, thus proving to
be impracticable for the routine clinical setting. Throughout the progression of monoclonal drug
development there have been four major antibody types developed: murine, chimeric,
humanized and human [9].
Initial therapeutic antibodies were simple murine analogues, which contributed to the early lack
of success. It has since been shown that these antibodies have: a short half-life in vivo (due to
immune complex formation), limited penetration into tumour sites, and that they inadequately
recruit host effectors functions [14]. To overcome these difficulties the technical issues initially
experienced had to be surpassed. Chimeric and humanized antibodies have generally replaced
murine antibodies in modern therapeutic antibody applications. Hybridoma technology has been
replaced by recombinant DNA technology, transgenic mice and phage display [15].
Understanding of proteomics has proven essential in identifying novel tumour targets. Some of
the targeted disease disease conditions in which monoclonal antibody therapy has widely been
used include:
Cancer
Anti-cancer monoclonal antibodies can be targeted against malignant cells by several
mechanisms:
Radioimmunotherapy (RIT) involves the use of radioactively conjugated murine antibodies
against cellular antigens. Most research currently involved their application to lymphomas, as
these are highly radio-sensitive malignancies. To limit radiation exposure, murine antibodies
were especially chosen, as their high immunogenicity promotes rapid clearance from the body.
Tositumomab is an example used for non-Hodgkins lymphoma.
Antibody-directed enzyme prodrug therapy (ADEPT) involves the application of cancer
associated monoclonal antibodies which are linked to a drug-activating enzyme. Subsequent
systemic administration of a non-toxic agent results in its conversion to a toxic drug, and
resulting in a cytotoxic effect which can be targeted at malignant cells. The clinical success of

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 35 ~
ADEPT treatments has been limited to date [16]. However it holds great promise, and recent
reports suggest that it will have a role in future oncological treatment.
Immunoliposomes are antibody-conjugated liposomes. Liposomes can carry drugs or
therapeutic nucleotides and when conjugated with monoclonal antibodies, may be directed
against malignant cells. Although this technique is still in its infancy, significant advances have
been made. Immunoliposomes have been successfully used in vivo to achieve targeted delivery
of tumour-suppressing genes into tumours, using an antibody fragment against the human
transferrin receptor. Tissue-specific gene delivery using immunoliposomes has also been
achieved in brain, and breast cancer tissue [17].
Fig. 2: Monoclonal antibodies for cancer. ADEPT, antibody directed enzyme prodrug
therapy; ADCC, antibody dependent cell-mediated cytotoxicity; CDC, complement
dependent cytotoxicity; MAb, monoclonal antibody; scFv, single-chain Fv fragment [18].

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 36 ~
Autoimmune diseases
Monoclonal antibodies used for autoimmune diseases include infliximab and adalimumab, which
are effective in rheumatoid arthritis, Crohn's disease and ulcerative Colitis by their ability to bind
to and inhibit TNF-α [19]. Basiliximab and daclizumab inhibit IL-2 on activated T cells and
thereby help preventing acute rejection of kidney transplants [19]. Omalizumab inhibits human
immunoglobulin E (IgE) and is useful in moderate-to-severe allergic asthma.
Conclusion
The limitation in the production of monoclonal antibody by hybridoma technology opened doors
for improvements. This advancement in hybridoma technology led to an appreciable increase in
the quality and quantity of monoclonal antibody produced hybridoma technology. These
monoclonal antibodies are essential tools in biochemical research, Diagnosis,
immunopurification and immunotherapy. With recent outbreak of Ebola virus infection, much
research should be carried out towards the efficacious treatment of this infection using
monoclonal antibody which will further highlight the so-called Monoclonal Antibody Therapy.
References
1. Bretton, PR, Melamed, MR, Fair, WR, Cote, RJ (1994). Detection of occult micrometastases
in the bone marrow of patients with prostate carcinoma. Prostate. 25(2), 108-14.
2. http://en.wikipedia.org/wiki/Hybridoma_technology #Method
3. Franklin, WA, Shpall, EJ, Archer, P, Johnston, CS, Garza-Williams, S, Hami, L, Bitter MA,
Bast RC, Jones, RB (1996). Immunocytochemical detection of breast cancer cells in marrow
and peripheral blood of patients undergoing high dose chemotherapy with autologous stem
cell support. Breast Cancer Res Treat. 41(1), 1-13.
4. Ghosh, AK, Spriggs, Al, Taylor-papadimitriou, J and Mason, DY (1983).
Immunocytochemical staining of cells in pleural and peritoneal effusions with a panel of
monoclonal antibodies. J Clin Pathol, 36, 11541164.
5. Kvalheim, G (1996). Detection of occult tumour cells in bone marrow and blood in breast
cancer patients—methods and clinical significance. Acta Oncol, 35, 13-8.

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 37 ~
6. http://www.molecular-plant-biotechnology.info/hybri doma-and-monoclonal-antibodies-mabs/
raising-theantibodies.htm
7. Elements of biotechnology, P.K. GUPTA (1st EDITION): 2006-2007, (203-211).
8. ^ "immunotherapies definition”. Dictionary.com. Retrieved 2009-06-02
9. http://en.m.wikipedia.org/wiki/Monoclonal_antibody_therapy
10. Prof FC Breedveld (2000). "Therapeutic monoclonal antibodies" Lancet. doi
:10.1016/S0140-6736(00)01034-5 .
11. Köhler G, Milstein C (August 1975). "Continuous cultures of fused cells secreting antibody of
predefined specificity". Nature 256 (5517): 495–7. Bibcode: 1975 Natur.256..495K. doi:
10.1038/256495a0. PMID 1172191.
12. Nadler LM, Stashenko P, Hardy R, et al. (September 1980). "Serotherapy of a patient with a
monoclonal antibody directed against a human lymphoma-associated antigen". Cancer Res.
40 (9): 3147–54. PMID 7427932.
13. Ritz J, Schlossman SF (January 1982). "Utilization of monoclonal antibodies in the treatment
of leukemia and lymphoma". Blood 59 (1): 1–11. PMID 7032624.
14. a b c Stern M, Herrmann R (April 2005). "Overview of monoclonal antibodies in cancer
therapy: present and promise". Crit. Rev. Oncol. Hematol. 54 (1): 11–29. doi
:10.1016/j.critrevonc.2004.10.011 . PMID 15780905.
15. a b Hudson PJ, Souriau C (January 2003). "Engineered antibodies". Nat. Med. 9 (1): 129–
34. doi: 10.1038/nm0103-129 .PMID 12514726.
16. Francis RJ, Sharma SK, Springer C, et al. (2002). "A phase I trialof antibody directed
enzyme prodrug therapy (ADEPT) in patientswith advanced colorectal carcinoma or other
CEA producingtumours. Br J Cancer 87 (6): 600–7. doi :10.1038/sj.bjc.6600517 .PMC
2364249 . PMID 12237768.
17. Krauss WC, Park JW, Kirpotin DB, Hong K, Benz CC (2000). "Emerging antibody-based
HER2 (ErbB-2/neu) therapeutics". BreastDis 11: 113–124. PMID 15687597.
18. Modified from Carter P (November 2001). "Improving the efficacy of antibody-based cancer
therapies". Nat. Rev. Cancer 1 (2): 118–29. doi : 10.1038/35101072 . PMID 11905803.
19. a b Rang, H. P. (2003). Pharmacology. Edinburgh: Churchill Livingstone. p. 241. ISBN 0-
443-07145-4.

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 38 ~
Lyophilisation: A Method of Preserving
Biologicals
Dr Sakshi Bhadouriya, M.V.Sc (Vet. Virology, IVRI, Bareilly)
Dr Sunil Singh Tomar, M.V.Sc (Vet. Clinical Medicine)
Introduction
Lyophilisation (also known as Freeze Drying or Cryodesiccation) is a dehydration process
typically used to preserve a perishable material or make the material more convenient for
transport. With proper packaging and storage, freeze-dried products can be stored for a very
long time without any appreciable loss of quality even at room temperature. Freeze-drying
works by freezing the material and then reducing the surrounding pressure and adding enough
heat to allow the frozen water in the material to sublime directly from the solid phase to the gas
phase. Lyophilisation technology is used to freeze-dry products such as biologicals, bacterial
cultures, analytical chemistry moieties, and therapeutic molecules (e.g., antibodies, vaccines,
drugs, and heat-sensitive proteins). Lyophilizing such products, particularly liquid formulations,
vastly increases their shelf-life and stability. Freeze-dried products have an optimal capacity to
take up water again (reconstitution, rehydration).
The Principles of Freeze-Drying
At atmospheric pressure (approx. 1,000 mbar) water can have three physical states:
1. Solid;
2. Liquid;
3. Gaseous.
Below the triple-point (for pure water at 0°C), only the solid and the gaseous states exists. The
principle of freeze/sublimation-drying is based on this physical fact. The ice in the product is
directly converted into water vapour without passing through the “fluid state”.

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 39 ~
Process of Freeze Drying
The process consists of three separate, unique, and interdependent processes:
Freezing
Primary drying (sublimation),
Secondary drying (desorption).
In a lab, this is often done by placing the material in a freeze-drying flask and rotating the flask
in a bath, called a shell freezer, which is cooled by mechanical refrigeration, dry ice and
methanol, or liquid nitrogen. On a larger scale, freezing is usually done using a freeze-drying
machine. In this step, it is important to cool the material below its triple point, the lowest
temperature at which the solid and liquid phases of the material can coexist. This ensures that
sublimation rather than melting will occur in the following steps. Larger crystals are easier to
freeze-dry. To produce larger crystals, the product should be frozen slowly or can be cycled up
and down in temperature. This cycling process is called annealing. However, in the case of

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 40 ~
food, or objects with formerly-living cells, large ice crystals will break the cell walls (a problem
discovered, and solved, by Clarence Birdseye), resulting in cell destruction, and, in the case of
rehydrated foods, a poor texture. In this case, the freezing is done rapidly, in order to lower the
material to below its eutectic point quickly, thus avoiding the formation of ice crystals. Usually,
the freezing temperatures are between −50 °C and −80 °C. The freezing phase is the most
critical in the whole freeze-drying process, because the product can be spoiled if badly done.
Amorphous materials do not have a eutectic point, but they do have a critical point, below which
the product must be maintained to prevent melt-back or collapse during primary and secondary
drying.
Primary Drying
During the primary drying phase, the pressure is lowered (to the range of a few millibars), and
enough heat is supplied to the material for the water to sublimate. The amount of heat
necessary can be calculated using the sublimating molecules’ latent heat of sublimation. In this
initial drying phase, about 95% of the water in the material is sublimated. This phase may be
slow (can be several days in the industry), because, if too much heat is added, the material’s
structure could be altered. In this phase, pressure is controlled through the application of partial
vacuum. The vacuum speeds sublimation, making it useful as a deliberate drying process.
Furthermore, a cold condenser chamber and/or condenser plates provide a surface(s) for the
water vapour to re-solidify on. This condenser plays no role in keeping the material frozen;
rather, it prevents water vapor from reaching the vacuum pump, which could degrade the
pump's performance. Condenser temperatures are typically below −50 °C (−60 °F). It is
important to note that, in this range of pressure, the heat is brought mainly by conduction or
radiation; the convection effect is considered to be inefficient.
Secondary drying
The secondary drying phase aims to remove unfrozen water molecules, since the ice was
removed in the primary drying phase. This part of the freeze-drying process is governed by the
material’s adsorption isotherms. In this phase, the temperature is raised higher than in the
primary drying phase, and can even be above 0 °C, to break any physico-chemical interactions

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 41 ~
that have formed between the water molecules and the frozen material. Usually the pressure is
also lowered in this stage to encourage desorption (typically in the range of microbars, or
fractions of a pascal). However, there are products that benefit from increased pressure as well.
After the freeze-drying process is complete, the vaccum is usually broken with an inert gas,
such as nitrogen, before the material is sealed. At the end of the operation, the final residual
water content in the product is extremely low, around 1-4%.
Flow Chart of Lyophilisation
Material in vial in shelves is pre-chilled the shelves to -45 c & initiate the drying when material
temp -40 c.
Vaccine harvest + stabiliser
Product in direct contact vd shelves (-40 c)
Condenser temp (-55 to -60 c)
Then primary drying starts (1% to 4%)
Remove crystalline ice by sublimation when water sublimes it takes energy so product is cooled
Energy of sublimated water is release to condenser so condenser tends to warm
Self heating & refrigeration & compressor works counteractly.
Product have residual 5-10 % moisture (not frozen so all ice is removed in this)
Key Component of Freeze Drying
Vaccum chamber
Lyophilisation shelves

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 42 ~
Heat transfer fluid
Product
Condenser
A mechanical or cryogenic refrigeration system
Heater
Vaccum pump
Control hardware and software
Freeze Drying Methods
Three methods of Freeze Drying are commonly used:
1. Manifold drying
2. Batch drying
3. Bulk Drying
Properties of freeze-dried products
If a freeze-dried substance is sealed to prevent the reabsorption of moisture, the substance may
be stored at room temperature without refrigeration, and be protected against spoilage for many
years. Preservation is possible because the greatly reduced water content inhibits the action of
microorganisms and enzymes that would normally spoil or degrade the substance. Freeze-
drying also causes less damage to the substance than other dehydration methods using higher
temperatures. Freeze-drying does not usually cause shrinkage or toughening of the material
being dried. Freeze-dried products can be rehydrated (reconstituted) much more quickly and
easily because the process leaves microscopic pores. The pores are created by the ice crystals
that sublimate, leaving gaps or pores in their place. This is especially important when it comes
to pharmaceutical uses. Freeze-drying can also be used to increase the shelf life of some
pharmaceuticals for many years
Disadvantages of Freeze Drying
Maintaining frozen storage is costly and takes up a lot of space
Transportation of frozen materials can be difficult and expensive

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 43 ~
Failure of freezing equipment would risk the total loss of the product
Conventional drying methods also have a major disadvantage as the high temperatures
used can cause chemical or physical changes to the product.
References
1. LYOPHILIZATION: Univ.Prof. Eng. Dumitru MNERIE, PhD “POLITEHNICA” University
of Timisoara ROMANIA
2. T. A. Jennings, “Lyophilization - Introduction and Basic Principles”, Interpharm Press,
Buffalo Grove, IL 1999.
3. A. I. Liapis and R. Bruttini, in A.S. Mujumdar ed., “Handbook of industrial Drying” vol.1,
2nd ed., Marcel Dekker, New York and Basel, 1995, 309 – 343.

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 44 ~
Rapid diagnosis of acute respiratory infections
by multiplex endpoint PCR technology 1Aurelian Udristioiu, 2Manole Cojocaru, 3Dana Alexandra Maria Panait, 4Nica
Badea Delia
1Clinical Laboratory, Department of Hematology, Emergency County Hospital Targu Jiu
& UCB University, Romania, E-mail: [email protected]
2Titu Maiorescu University, Faculty of Medicine, Physiology Department, Bucharest,
Romania; E-mail: [email protected]
3Titu Maiorescu University, Faculty of Medicine, Microbiology Department, Bucharest,
Romania, E-mail [email protected]
4Constantin Brancusi University, Faculty of Medical Science and Behavioral, Targu Jiu,
Romania, Email: [email protected]
Introduction
The multiplex endpoint PCR technology offers a number of potential advantages, results are
available in a matter of hours rather than days, the extreme sensibility facilitates detection of
even minutes the amounts of pathogen DNA in clinical samples and the test is not significantly
affected by prior administration of antibiotics.
Aim
The aim of this work was to rapidly identify the antibiotic resistance the monitoring of pathogen
growth at the patients admitted in Hospitalization Intensive Care Unit of Emergency County
Hospital Targu Jiu with the diagnosis of Community Acquired Pneumonia, (CAP), in months
December/2013-March/2014.
Method
The Analyzer Unyvero™ Pneumonia Application was used in detection of pneumonia
associated pathogens and their antibiotic resistance genes using the Pneumonia Unyvero™
System, following PCR pathogen species with sequencing of the amplified microbial DNA.

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 45 ~
Results
The main pathogens of community acquired pneumonia from the cohort study, 36 cases, (20
males in mean age 35-66 years and 16 females in mean age 40-55 mean years) were
Streptococcus pneumonia (16 cases), Staphilococcus aureus, (10 cases), Klebsiella
pneumonia (5 cases), and other important agents were “atypical”, such as Haemophilus
Influenzae, Chlamidophila pneumonie and Moraxela cataralis.
A case with Acinetobacter baumani and Proteus Sp. was also widely resistance to mefA gene /
ermB gene as all cases of analyzed. The more frequency of genes resistant (29 cases) are
ermA gene / ermC / ermB for Staphilococcus aureus and the gene tem+shv / gene / ctx-M with
the chromosomal mutation (7 cases), as gyrA83_87 Ecoli / Pseu for Klebsiella pneumonia
agents. Also most resistance antibiotics were Makrolides, (29 cases and Lincosamides (6
cases) and this cases have had the chromosomial integrates. The most resistance microbe,
Pseudomonas aeruginosa (1 case), has been registered as multi drugs resistance [MDR]*.
Fig. 1: Microorganism results in Pneumonia Panel

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 46 ~
No.
IDL
Microorganisms
detected
Antibiotic resistance Gene resistance
1310_1
Klebsiella pneumonia
Makrolides /],
[ermB],].Lincosamides
ermB gene
1310_2 Streptoccocus Sp.
Makrolides. ermB gene/tem gene
1310_3
Staphilococcus
aureus
Other/Fungi:
Chlamidophila
pneumonie
Penicilins (tem) ermB gene/tem gene
Chromosomal mutation;
Pseud. aeruginosa, (gyrA83-
Ecoli
1310_4 Klebsiella pneumonia
Makrolides / Lincosamides ermB gene
1310_5
Proteus Sp.
Other/Fungi:
Haemophilus
Influenzae,
Chlamidophila
pneumonie
Makrolides
Oxacilin
ermB gene/oxa51
Chromosomal mutation;
Escherichia Coli (gyrA83-
87_Ecoli ).
1311_1
Streptococcus
pneumonia Moraxela
cataralis
Makrolides,
Oxacillin Lincosamides,
ermB gene/tem gene/ mecA gene
1311_2
Streptococcus
pneumonia
Makrolides / [mefA],
[ermB],].Lincosamides
Penicilins (tem)
mefA gene / ermB gene / tem
1311_3
Streptococcus
pneumonia
Pseudomonas
aeruginosa
Makrolides / [mefA],
[ermB],].Lincosamides
[MDR]* [int1].
mefA gene / ermB gene
[int1gene].
1311_4 Klebsiella pneumonia Penicilins (shv) mefA gene / shv gene
[int1gene] /sul 1 gene
Chromosomal mutation;
(gyrA83_3Pseu).

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 47 ~
[MDR]*-Multi drugs resistance
Table 1. Resistance markers of the Pneumonia panel and the resulting antibiotic
resistances
Photo 1. Analyzer Unyvero™ Pneumonia
Conclusion
The Unyvero™ results have been available 2 days before the primary microbiology report and 3
days before the final confirmation results, obtained by microbiology culture. The Unyvero
Analyzer only provides rapid data to support the therapeutic decision of currant medic.
1311_5 Streptococcus
pneumonia
Acinetobacter
baumani
Makrolides / [mefA],
[ermB],].Lincosamides
mefA gene / ermB gene
1312_1
Staphilococcus
aureus
Klebsiella pneumonia
Makrolides / [mefA],
[ermB],].Lincosamides
3rd Gen Cephalosporins
[tem+shv], [ctx-M].
ermA gene / ermC / ermB
tem+shv / gene / ctx-M g
Chromosomal mutation;
gyrA83_87 Ecoli / Pseu

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 48 ~
Bioweapons: A new trend in emerging Sciences 1Hasnain Nangyal, 2Noor Nasir Khattak, 3Sikander Khan Sherwani
1Department of Botany, Hazara University, Khyber Pakhtoonkhwa, Pakistan
2Department of Gynocology and Obteristics, Kohat Medical College, Khyber
Pakhtoonkhwa, Pakistan
3Department of Microbiology, FUUAST, Karachi, Pakistan
Corresponding Author Email: [email protected]
Basically different biologists defined this term in different ways:
1. Bioweapons are the biological agents derived from the living organisms that are capable
of infecting and causing both sickness and death in people, animals and plants.
2. Bioweapons sometime called biowarfare which means that intentional use of
microorganisms or toxins derived from living organisms of as an act of war or political
violence with intent to cause death or disease in human, animal or in plants (1)
3. Biological warfare (BW)—also called germ warfare. It is the use of biological toxins or
infectious agents such as bacteria, viruses, and fungi with intent to kill or incapacitate
humans, animals or plants as an act of war.
4. Biological weapons (often termed "bio-weapons", "biological threat agents", or "bio-
agents") are living organisms or replicating entities (viruses, which are not universally
considered "alive") that reproduce or replicate within their host victims.
5. Biological warfare agents are likely to be selected for their ability to either incapitate or
kill human targets of attack.
Types of Bioweapons:
There are seven types of biological agents:
1: Parasites
2: Fungi and yeasts
3: Bacteria
4: Rickettsia and chlamydia

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 49 ~
5: viruses
6: Prions
7: Toxins
8: Insects
Among the biological agent only bacteria, viruses and toxins are considered when referring to
agents that can be used in a biological attack. While toxins are included in the list of biological
agents, they are not living organisms, but small proteins produced by bacteria that can poison to
a person, animal or plant. Bacteria, viruses and toxins can be spread through the contamination
of food, water or fomites; via vectors such as insects; or as aerosols suspended in wet or dry
formulations (2).
Entomological (insect) warfare is also considered a type of biological weapon. This type of
warfare is distinct from nuclear warfare and chemical warfare. None of these falls under the
term conventional weapons which are primarily effective due to their destructive potential.
Biological weapons (BWs) deliver toxins and microorganisms, such as viruses and bacteria, so
as to deliberately inflict disease among people, animals, and agriculture. Biological attacks can
result in destruction of crops, temporarily discomforting a small community, killing large numbers
of people, or other outcomes.
Possible Biological Warfare
Agents
Bacteria (examples)
Viruses (examples)
Toxins (examples)
Bacillus anthracis (anthrax)
Variola virus (smallpox)
Staphylococcal
enterotoxin B
Yersinia pestis (plague)
Equine encephalitis viruses (viral
equine
encephalitides)
Ricin

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 50 ~
Francisella tularensis
(tularemia)
Arenaviruses,bunyaviruses,
filoviruses
Botulinum toxins
Brucella species (brucellosis)
flaviviruses (hemorrhagic fevers)
Trichothecene mycotoxins
Coxiella burnetii (Q fever)
- Saxitoxin
Classification of Bioweapons:
There are four classifications for how biological agents can be used to harm or kill a person,
animal or plant.
1: Biological Warfare (BW): is the military use of biological agents, where targets of agents are
predominately soldiers, governments, or resources that might hinder a nation’s ability to attack
and/or defend it.
2: Bioterrorism (BT): is the threat or use of biological agents that, like most forms of terrorism,
is intended to make political, religious or personal statements to governments and populations
through attacks primarily aimed at civilians or resources that affect the civilian economy. With
few exceptions, bioterrorism is non-state sponsored.
3: Biocrime (BC): is the threat or use of biological agents for individual objectives such as
revenge or financial gain.
4: Bioaccident (BA): It is defined as the unintentional release of an agent from a laboratory or
other facility. Biocrimes and Bioaccidents comprise events that typically have small effects on
populations and do not require specific plans for large-scale preparedness and response (3).
Categories of Bioweapons:
The Critical Agent List classifies a relatively short list of possible biological weapons to be used
in either biological warfare or bioterrorism, and was created by the Centers for Disease Control
and Prevention (CDC) in conjunction with military, intelligence, medical and public health
agencies: (20)
Category A includes the highest priority agents because they are most likely to cause mass
casualties, create panic and require a specific public health response. According to intelligence

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 51 ~
sources, these are the agents that are most likely to be used in a future attack, and are being
researched and weaponized by biowarfare programs around the world.
Category B is the second highest priority agents, including those agents that could contaminate
food or water, are relatively easy to disseminate, and require enhanced disease surveillance
and diagnostic capacity. Many of these agents, such as brucellosis, glanders and ricin, were
either weaponized by state-sponsored programs in the past, or utilized successfully in biological
warfare or terrorist incidents
Category C includes emerging pathogens that could be weaponized in the future because of
the relative ease of accessing, producing and disseminating the agents, as well as the high
levels of morbidity and mortality these agents would cause.(4)
Although the CDC has been able to categorize a list of agents that are likely to be used as
bioweapons, there are additional diseases and variations of biological agents that are of great
concern. The Critical Agent List specifies only twenty-one diseases, but there are at least
seventy different types of biological agents that can be weaponized, not including agents that do
not already exist in nature. Of the disease caused by these seventy agents, only 20-30% is
currently treatable through reliable methods.(5)
Critical list of Biological agents
Category A Category B Category C
Small pox Q-fever nipah virus
Anthrax Brucellosis Hantavirus
Plague Glanders multidrug-resistant TB
Tularemia melioidosis
hemorrhagic fever viral encephalitis
Ebola Ricin
(21)
History
There is a long history of nations and peoples using biological agents as weapons. Many
examples of use have been cited from as long ago as 190 BC, where Hannibal used venomous
snakes to disrupt the enemy ships of Pergamus in Eurymedon. Biological weapons have a long

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 52 ~
history of use. In 1346, the invading Tartar army catapulted the bodies of plague victims into the
Crimean Peninsula city of Kaffa and infected its citizens. Another example of biological warfare
often referred to in the historical record is the use of smallpox during the French and Indian War
in 1763. Through the combined ingenuity of British Officers Sir Jeffrey Amherst and Colonel
Henry Bouquet, smallpox infested blankets were given to the Indians at Fort Pitt, setting off an
epidemic of smallpox that rendered the Indian tribes incapable of fighting off the British settlers
(6). In this instance, it is not clear if the blankets themselves caused the outbreak of smallpox or
whether it was due to previous exposure to the Europeans. Regardless, this method of
biological warfare was used again during the American Civil War, when Dr. Luke Blackburn of
Kentucky sold smallpox and yellow fever infected clothing to Union troops in an effort to support
the efforts of the Confederacy. There were also reports that the Germans used plague against
the Russians in 1915, and attempted to use cholera against Italy (7). Between 1933 and the
late 1940’s, Japan researched biological warfare at a compound known as Unit 731, where over
10,000 prisoners of war used for research purposes died of anthrax, meningitis, cholera and
plague. Japan followed its experiments with prisoners of war by using biological agents against
the people of China, causing outbreaks of typhus, cholera and plague, resulting in the deaths of
tens of thousands of Chinese civilians.(19) One method used by the Japanese in Manchuria
was dropping rice and plague infected fleas out of airplanes. The rice attracted rats, which then
became infected with the fleas, thus creating efficient epidemiologic conditions by which the
disease spread to humans over a large geographic area(8). The 2001 anthrax letter attacks in
the United States infected 22 people and killed five (Biological weapon technology, 1998).The
Genoese forces retreated back to Genoa, Venice and other Mediterranean ports, sparking the
second wave of the plague epidemic in Europe. (9)
Characterizing the Threat of Biological Weapons
On 11 September 2001, terrorists used hijacked passenger planes loaded with jet fuel as
explosion devices at the Pentagon and World Trade Center, killing approximately 3000. This
attack awakened the American public to the idea that terrorists have the will and the means of
inflicting harm on citizens of the United States within their national borders. Following the
September 11th attack, letters with anthrax were mailed to a targeted list of media and political

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 53 ~
personalities.(18) There are many reasons why biological agents are effective means of
spreading terror which include followings;
Availability
Biological agents are often simpler to acquire and produce than nuclear, chemical or some
conventional weapons. The material for biological agents can be easily grown or purchased.
Some agents, such as anthrax or brucellosis, occur naturally in animals in certain parts of the
world, and individuals can easily travel the globe to acquire biological agents from regions
where such diseases occur naturally. For example, the Aum Shinrikyo cult was reported to
have gone to Zaire to collect strains of Ebola for use in its bioweapons program. Until recently,
anyone could order agents from supply houses around the world (10).
Access to Technology
Technological advances over the last two decades in the field of biology have made it easier to
produce biological weapons. Techniques once considered beyond the capacity of scientists are
now commonplace, particularly in the field of genetic engineering. Bioengineers are now armed
with the knowledge needed to create antibiotic resistant strains of agents, combine aspects of
two agents, weaponize agents, and possibly target particular populations. The creation of
antibiotic resistant strains of anthrax was a key component of the Soviet biowarfare program28.
The Soviets were also successful in creating more virulent strains of the disease, capable of
bypassing the available anthrax vaccine currently given to United States active duty forces29.
Bioengineers are also now able to combine two agents to complicate the presentation of a
disease in humans. Again, it was the Soviets who first used this technology by using
recombinant DNA to combine features of smallpox and Ebola, and in 1995, Russian scientists
presenting at a scientific conference in England, reported that they had combined a food
poisoning organism with anthrax (11).
Access to Information
Information on how to create sophisticated biological weapons can be taken from articles
published in the scientific literature on a variety of topics, but it requires a trained scientist to

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 54 ~
understand the relevance of published findings to the creation of weapons. However,
information on how to weaponize simpler biological agents is widely available and
understandable to people with limited technological training.
Lethality
Biological agents can be extremely lethal, with some agents creating much more deadly affects
than others. According to the Department of Defense, ten kilograms of anthrax could cause
more casualties that a 10- kiloton nuclear weapon (12).
Lack of Collateral Damage
While biological agents may indiscriminately kill or injure humans, animals and plants, they do
not destroy structures. This aspect of biological agents may be of interest to groups who desire
to kill residents of an area, but protect surrounding assets, such as religious shrines, historical
buildings, or industrial plants (13).
Plague as a past bioweapon:
Plague is a zoonotic disease caused by the bacterium Yersinia pestis, typically harbored by wild
rodents (Fig). The plague epidemic that swept through Europe, the Near East, and North Africa
in the mid-14th century was probably the public health disaster in recorded history. An
estimated one-quarter to one-third of Europe’s population died from plague during the 14th
century pandemic, and North Africa, the Near East, and perhaps the Far East had similar high
levels of mortality.(14) However, the first recorded plague andemic began in 541 in Egypt when
the world population as considerably smaller and decimated an even greater ercentage of
the population.
Advantages and Disadvantages of Biological Weapons
Advantages
1: The potential deadly or incapacitating effects on a susceptible population
2: The self-replicating capacity of some biological agents to continue proliferating in the affected
individual and potentially in the local population and surroundings

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 55 ~
3: The relatively low cost of producing many biological weapons
4: The insidious symptoms that can mimic endemic diseases
5: The difficulty of immediately detecting the use of a biological agent, owing to the current
limitations in fielding a multi-agent sensor system on the battlefield, as well as to the prolonged
incubation period preceding onset of illness (or the slow onset of symptoms) with some
biological agents(15)
6: The sparing of property and physical surroundings (compared with conventional or nuclear
weapons)

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 56 ~
Disadvantages
1: The danger that biological agents can also affect the health of the aggressor forces
2: The dependence on prevailing winds and other weather conditions on effective dispersion
3: The effects of temperature, sunlight, and desiccation on the survivability of some infectious
organisms
4: The environmental persistence of some agents, such as spore-forming anthrax bacteria,
which can make an area uninhabitable for long periods
5: The possibility that secondary aerosols of the agent will be generated as the aggressor
moves through an area already attacked
6: The unpredictability of morbidity secondary to a biological attack, since casualties (including
civilians) will be related to the quantity and the manner of exposure
7: The relatively long incubation period for many agents, a factor that may limit their tactical
usefulness
8: The public’s aversion to the use of biological warfare agents (16)
Indications of Possible Biowarfare Attack
• A disease entity that is unusual or that does not occur naturally in a given geographic area, or
combinations of unusual disease entities in the same patient populations
• Multiple disease entities in the same patients, indicating that mixed agents have been used in
the attack
• Large numbers of both military and civilian casualties when such populations inhabit the same
area
• Data suggesting a massive point-source outbreak
• Apparent aerosol route of infection
• High morbidity and mortality relative to the number of personnel at risk
• Illness limited to fairly localized or circumscribed geographical areas
• Low attack rates in personnel who work in areas with filtered air supplies or closed ventilation
systems
• Sentinel dead animals of multiple species

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 57 ~
• Absence of a competent natural vector in the area of outbreak (for a b iological agent that is
vector-borne in nature) (17).
References:
1. Manchee R, Stewart W.1988. The decontamination of Gruinard Island. Chem Br.690–
691.
2. Nally R. E, Morrison MB, Stark M. 1993. Effectiveness of medical defense interventions
against predicted battle field levels of Bacillus anthracis. Science Applications
International.32-35
3. Patrick W.C.1992. Overview of biological warfare. Frederick, Unpublished
manuscript.11-14
4. North Atlantic Treaty Organization. NATO Handbook on the Medical Aspects of NBC
Defensive Operations. A-Med-P6, part 2, Biological. June 1992.
5. World Health Organization. Health Aspects of Chemical and Biological Weapons: Report
of a WHO Group of Consult- ants . Geneva, Switzerland: WHO; 1970.
6. Huxsoll D, Patrick W.C, Parrott C.1987. Veterinary services in biological disasters.
Journal of veterinary sciences. 714–722.
7. Department of the Army. Special Report to Congress. US Army Activities in the US
Biological Defense Programs,1942–1977. Vols 1 and 2. Washington, DC: DA. 24 Feb
1977. Unclassified.
8. Special Subcommittee on the National Science Foundation of the Committee on Labor
and Public Welfare, US.Senate. Chemical and Biological Weapons: Some Possible
Approaches for Lessening the Threat and Danger. Washing-ton, DC: US Government
Printing Office; May 1969.
9. Special Subcommittee on the National Science Foundation, Committee on Labor and
Public Welfare. Chemical and Biological Weapons. Washington, DC: US Government
Printing Office; May 1969.
10. Ursano R. Combat stress in the chemical and biological warfare environment. Aviation
Space & EnvironmentalMedicine. 1988;59(12):1123–1124.

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 58 ~
11. Mojecki, J.A.1994. Mission-essential training and weapons of mass destruction. Military
Review. 91–93.
12. Geissler E, ed.1986. Biological and Toxin Weapons Today. Stockholm International
Peace Research Institute. Oxford, England: Oxford University Press
13. Douglas, J.D. Livingstone, N.C.1987. America the Vulnerable: The Threat of Chemical
and Biological Warfare. Lexington,Mass: Lexington Books.
14. US Department of State. International Terrorism. Washington, DC: DOS; 1989. GIST.
15. Zilinskas, R.A.1990. Terrorism and biological weapons: Inevitable alliance? Perspect
Biol Med. 44–72.
16. Bates S.1992. Fairfax man accused of anthrax threat. Washington Post.
17. Kupperman, R.H, Smith, D. M.1991. Coping with biological terrorism. Washington, DC..
18. US Army Medical Research Institute of Infectious Diseases. Medical Management of
Biological Casualties Hand- book . Fort Detrick, Frederick, Md: USAMRIID; August 1993.
19. Wiener, S.L, Barrett, J.1986. Biological warfare defense. In trauma Management for
Civilian and Military Physicians. Philadelphia, Pa: WB Saunders.507–528.
20. Caudle L.1994. Major, Medical Corps, US Army. Officer in Charge, Problem Definition
and Assessment Team, Operation Vigilant Warrior. Personal communication.
21. Khan A, et al. Public health preparedness for biological terrorism in the USA. Lancet
2000; 356:1179

Microbiology World Issue 8 Nov – Dec 2014 ISSN 2350 - 8774
www.microbiologyworld.com www.facebook.com/MicrobiologyWorld ~ 59 ~
You can also send your articles to
or
Selected ones will be published in
our next issue of Jan-Feb 2015.
Thanks,
Sagar Aryal
Editor-In-Chief
Microbiology World









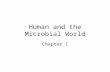



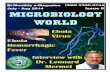




![World Journal of Microbiology and Biotechnology Volume 6 Issue 3 1990 [Doi 10.1007_bf01201297] L. Ban-Koffi; Y. W. Han -- Alcohol Production From Pineapple Waste](https://static.cupdf.com/doc/110x72/577cdbd91a28ab9e78a93d19/world-journal-of-microbiology-and-biotechnology-volume-6-issue-3-1990-doi.jpg)









