Host of the 2019 Congress of the World Federation of the Societies of Intensive and Critical Care Medicine
1
MELBOURNE

2



Mechanical ventilation strategies in acute hypoxic respiratory failure
Redefining ALI / ARDS in children Why we need the “P” in PARDS
Dr Simon Erickson Paediatric Intensive Care Princess Margaret Hospital

Clinical syndrome characterized by diffuse inflammation in the lung
Results in significant hypoxemia from endothelial injury to the pulmonary vasculature and alveolar epithelial injury
No definitive diagnostic test (i.e. biomarker) which is present in all cases (even histopathology inconsistent)

Hypoxemia (Shunt) Poor Respiratory System Compliance Decreased End Expiratory Lung Volumes
(FRC) Diffuse Process Endothelial Injury Edema Increased alveolar dead space

• Population estimates 1.4-9.5/100,000/yr • 1-4% of all PICU admissions have ALI • Mechanically Ventilated Children (>12-24h) ARDS: 2-7% ALI: 6-10%
• LRTI most common trigger • Indirect Lung Injury from Sepsis also common, with worse prognosis
Randolph 2009, 2003, Farias 2004, Dahlem 2003, Erickson 2007, Curley 2005, Willson 2005
•Mortality between 30-40% for adults and 8-30% for children with ALI or ARDS •RCTs: 8% (prone); 28% (Calfactant –with BMT); 14% (Calfactant-no BMT)

Is there any evidence to guide us?

How are we doing currently?
Courtesy S. Watson, PALICC
Zimmerman et al, Pediatrics 2009

AECC Definition AECC Limitations
Timing Acute onset No definition of acute
ALI category All patients with PaO2/FiO2<300 Misinterpreted as PaO2/FiO2 201-300
leading to the confusing ALI/ARDS term
Oxygenation PaO2/FiO2 ≤ 300 mmHg (regardless of PEEP)
Effect of PEEP and FiO2 on PaO2/FiO2 ; difficulty in estimating FiO2 in non-intubated patients
Chest Radiograph Bilateral infiltrates seen on frontal chest radiograph
Poor interobserver reliability of chest radiograph interpretation
PAWP PAWP ≤ 18 mmHg when measured or no clinical evidence of left atrial hypertension
High PAWP and ARDS may coexist
Poor interobserver reliability of PAWP and clinical assesments of left atrial hypertension
Risk Factor None Not formally included in definition
Phua: CCM 2008; Wheeler: NEJM; 2006; Villar: AJRCCM 2007;Meade: AJRCCM 2000; Rubenfeld Chest 1999; Komadina: Chest 1991;

Acute Respiratory Distress Syndrome
Timing Within 1 week of a known clinical insult or new/worsening respiratory symptoms
Origin of Edema Respiratory failure not fully explained by cardiac failure or fluid overload;
Need objective assessment (e.g., echocardiography) to exclude hydrostatic edema if no risk factor present
Mild Moderate Severe
Oxygenation b 200<PaO2/FiO2< 300
with PEEP or CPAP ≥ 5 cmH2O
100<PaO2/FiO2<200 with
PEEP ≥ 5 cmH2O
PaO2/FiO2<100 with
PEEP ≥ 10 cmH2O
Chest Imaging a Bilateral opacities - not fully explained by effusions, lobar
collapse, masses
Bilateral opacities - not fully explained by effusions, lobar
collapse, masses Opacities involving ≥3 quadrants
Ancillary Physiology N/A N/A VE, CORR ≥ 10 L/min d, f
or CRS ≤ 40 mL/cmH2O e, f
eSUPPLEMENT
1) Include radiographs of consensus interpretations for qualifying opacities vs not vs equivocal
2) Include case vignettes on how to assess “not fully explained by cardiac failure of fluid overload”






Pediatric Specific Definition Pathobiology and Ventilator Induced Lung
Injury Selected topics on ventilator/ancillary
management

Build off Berlin Definition- is Berlin alone Adequate? Pediatric Considerations
1. Timing (similar to adults?) 2. Age 3. Co-existence with cardiac failure/dysfunction (similar to
adults?) 4. What are best respiratory criteria for risk
stratification/disease severity 5. How do we handle patients on non-invasive ventilation
and/or those without arterial lines 6. How important/reliable are Radiographic Criteria for
Definition of ARDS 7. Defining it in patients with pre-existing cardiac or
pulmonary co-morbidities

OI = oxygenation index = (FiO2* mean airway pressure*100)/ PaO2
OSI = oxygen saturation index = (FiO2* mean airway pressure*100) /SpO2
Age Exclude patients with peri-natal related lung disease
Timing Within 7 days of known clinical insult
Origin of Edema Respiratory failure not fully explained by cardiac failure or fluid overload
Chest Imaging Chest imaging findings of new infiltrate(s) consistent with acute pulmonary parenchymal disease
Oxygenation
Non Invasive mechanical ventilation Invasive mechanical ventilation
PARDS (No severity stratification) Mild Moderate Severe
Full face-mask bi-level ventilation or CPAP ≥5 cm H20 2
PF ratio ≤ 300 SF ratio ≤ 264 1
4 ≤ OI < 8
5 ≤ OSI < 7.51
8 ≤ OI < 16
7.5 ≤ OSI < 12.31
OI ≥ 16
OSI ≥ 12.31
Special Populations
Cyanotic Heart Disease
Standard Criteria above for age, timing, origin of edema and chest imaging with an acute deterioration in oxygenation not explained by underlying cardiac disease. 3
Chronic Lung Disease
Standard Criteria above for age, timing, and origin of edema with chest imaging consistent with new infiltrate and acute deterioration in oxygenation from baseline which meet oxygenation criteria above.3
Left Ventricular dysfunction
Standard Criteria for age, timing and origin of edema with chest imaging changes consistent with new infiltrate and acute deterioration in oxygenation which meet criteria above not explained by left ventricular dysfunction.

Can we define paediatric? Perinatal causes?
Post-natal alveolar growth may continue until adult height achieved
Post-natal lung morphogenesis and immune development likely to affect responses
Exclusions IRDS
Perinatal lung injury
Congenital abnormalities

Epidemiology of Risk Factors Different
ANZ study 2007
Mortality or Length of Ventilation not different in most studies, not all
Upper limit?
Table 3. CDC age-adjusted mortality per 100,000
persons from sepsis and influenza and
pneumonia in the United States in 2009
Age (years) Sepsis Influenza and
Pneumonia
< 1 5.2 5.9
1 - 4 0.4 0.9
5 - 14 0.2 0.6
15 - 24 0.3 1
25 - 34 0.9 1.9
35 - 44 2.2 3.2
45 - 54 5.5 6.5
55 - 64 13.3 11.9
65 - 74 32 30.1
75 - 84 78.4 105.9
≥ 85 173.8 413.5
Zimmerman 2009, Flori 2005, Dahlem 2003, Erickson 2007, Ghuman 2012, Smith 2013

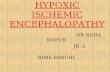
PF ratio versus OI
OI=(FiO2* mean airway pressure*100)/ PaO2
Variable ventilator management and in particular lower PEEP use in Pediatrics compared to Adults
Need to control for ventilator support
More Frequent use of HFOV

PEEP 5 cmH20
PaO2 = 60, FiO2=0.6, MAP = 8
PF Ratio 100
OI =8
PEEP 14 cmH20
PaO2 = 120, FiO2=0.5, MAP = 19
PF Ratio 240
OI = 8
OI versus PF ratio

* > 50% of patients with PEEP ≤5 cmH20
> 50% of adults in ARDSNet studies on PEEP
≥10cmH20 at study inclusion (Britos CCM)
Study PEEP
Flori 2005 5.3 +/- 2.6
Erikson 2007 8.5 (7,11)
Khemani 2009 6 (4,8)
Santishi 2010 (PALIVE)* 6.9 +/- 2.7
Lopez-Fernandez 2012 8.9 +/- 2.9

Variable PEEP use in Pediatrics
Santichi PALIVE 2011
Newth CPCCRN 2014
Oscillate NEJM 2013


OI >16 8-16 4-8 <4 Total
Category Severe Moderate Mild At Risk
Derivation Set
Khemani 2009
Number 98 (24.7%) 104 (26.2%) 147 (37.1%) 48 (12.1%) 397
Mortality 40 (40.8%) 21 (20.2%) 23 (11.6%) 2 (4.2%) 80 (20.2%)
Validation Set
Flori 2005
Number 28 (16.4%) 60 (35.1%) 67 (39.2%) 16 (9.4%) 171
Mortality 10 (35.5%) 16 (26.7%) 13 (19.4%) 1 (6.25%) 40 (23.4%)
Curley 2005
Number 34 (40%) 28 (33%) 20 (24%) 3 (3%) 85
Mortality 2 (5.9%) 4 (14.3%) 1 (5%) 0 (0%) 7 (8.2%)
Erickson 2007
Number 38 (33.3%) 31 (27.2%) 36 (31.6%) 9 (7.9%) 114
Mortality 20 (52.6%) 10 (32.3 %) 5 (13.9%) 0 (0%) 35 (30.7%)
Kneyber 2008
Number 8 (27.6%) 11 (37.9%) 10 (34.5%) 0 (0%) 29
Mortality 1 (12.5%) 3 (27.3%) 1 (10%) 0 (0%) 5 (17.3%)
Lopez-Fernandez 2012
Number 72 (55%) 47 (35.9%) 12 (9.1%) 0 (0%) 131
Mortality 24 (33.3%) 10 (21.3%) 3 (25%) 0(0%) 37 (28.2%)
Sapru 2013
Number 47 (28%) 68 (40.2%) 40 (23.7%) 14 (8.3%) 169
Mortality 9 (19.1%) 11 (16.2%) 0 (0%) 0 (0%) 20 (11.9%)
Validation Set Total
Number 225 (32.7%) 241 (34.8%) 184 (26.6%) 42 (6.1%) 692
Mortality 66 (29.3%) 54 (22.4%) 23 (12.5%) 1 (2.4%) 144 (20.8%)

1.5.1 Oxygenation Index [OI=(FiO2* mean airway pressure*100)/ PaO2], in preference to PaO2/FiO2 (PF) ratio, should be the primary metric of lung disease severity to define P-ARDS for all patients treated with invasive mechanical ventilation. Strong agreement
1.5.2 PaO2/FiO2 (PF) ratio should be used to diagnose ARDS for patients receiving non‐invasive full face mask ventilation (CPAP or BiPAP) with a minimum CPAP of 5 cm H2O. Strong agreement

Critical Care Medicine 2012

Requiring PF ratio selects for patients with hypoxemia and cardiovascular dysfunction
Not using pulse oximetry criteria underestimates the prevalence
of ARDS and over-estimates mortality, by selecting for a more ill
patient population

1.8.1 To apply SpO2 criteria to diagnose P-ARDS, oxygen therapy should be titrated to achieve an SpO2 between 88- 97%. Strong agreement

1.6.1 Oxygen Saturation Index [OSI =(FiO2* mean airway pressure*100)/SpO2]should be used when an OI is not available for stratification of risk for patients receiving invasive mechanical ventilation. Strong agreement
1.6.2 SF (SpO2/FiO2)ratio can be used when PF
ratio is not available to diagnose P-ARDS in patients receiving non‐invasive full face mask ventilation (CPAP or BiPAP) with a minimum CPAP of 5 cm H2O. Strong agreement

Left ventricular failure AECC vs. Berlin
Assessment of LV function
Common complication
Children with LV dysfunction that fulfill all other PARDS criteria where hypoxaemia and CXR changes cannot be explained by LV failure/fluid overload alone

OI 5.6 OI 18

Cyanotic congenital heart disease Very little data
Generally been considered an exclusion
CCHD at high risk
Role of echo to exclude cardiac changes
CCHD patients considered to have P-ARDS if acute deterioration in oxygenation, CXR changes, known insult not explained by underlying cardiac disease


Chronic lung disease At risk
Common underlying CLD (10-35%)
Includes dependence on supplemental O2, NIV, tracheostomy
P-ARDS requires known insult, acute CXR changes, acute worsening hypoxia



Increasing use in children with ARDS Immunocompromised and
chronic neurological disease
Reduced need for sedation
May reduce overall need for intubation
For non-invasive bi-level ventilation or CPAP ≥5 cm H20 If PaO2 available, then PF
ratio ≤ 300
If PaO2 not available, wean FiO2 to maintain SpO2 ≤ 97%, SF ratio ≤ 264


What is the sensitivity of CXR changes for Diffuse Alveolar Disease?
Sensitivity low (60-70%)
Correlation between CXR and CT poor
Timing lag
What is the inter-observer variability of CXR?
Significant (Angoulvant et al, Pediatr Pulmonol 2008)
Can ARDS exist with unilateral CXR changes? Does the presence of unilateral vs bilateral CXR
changes assist risk stratification?
Conflicting adult evidence
Paediatric data

Parvathaneni ATS 2016

Tidal volume and its effect on outcome Ventilatory strategies Ancillary treatments

Initial Vt and Mortalityn=398
0
20
40
60
80
100
120
<6 6 to 8 8 to 10 >10
Vt (ml/kg)
Co
un
t
0
0.05
0.1
0.15
0.2
0.25
0.3
0.35
Mo
rtali
ty
Survived Died Mortality
Day 1 Vt and Mortalityn=376
0
20
40
60
80
100
120
<6 6 to 8 8 to 10 >10
Vt (ml/kg)
Co
un
t
0
0.05
0.1
0.15
0.2
0.25
0.3
0.35
Mo
rtali
ty
Survived Died Mortality
Day 2 Vt and Mortalityn=343
0
20
40
60
80
100
120
<6 6 to 8 8 to 10 >10
Vt (ml/kg)
Co
un
t
0
0.05
0.1
0.15
0.2
0.25
0.3
0.35M
ort
ali
ty
Survived Died Mortality
Day 3 Vt and Mortality
n=290
0
20
40
60
80
100
120
<6 6 to 8 8 to 10 >10
Vt (ml/kg)
Co
un
t
0
0.05
0.1
0.15
0.2
0.25
0.3
0.35
Mo
rtali
ty
Survived Died Mortality
ICM 2009

Age < 1 year Age > 1 year
Higher VT associated with improved outcome,
particularly for children < 1 year

Multitude of subgroup analysis exploring various VT cut points
No clear relationship between VT and mortality in children regardless of ARDS severity

Baseline Lung Injury Score ICM 2009

Supra physiologic VT harmful in pediatric animal models, but younger animals less susceptible than older animals to VILI
Relatively more surfactant production in pediatric versus adult lung with high VT
Fewer inflammatory cytokines in pediatric versus adult lung with high VT
Difference in elastin and collagen in pediatric versus adult lung
Higher endothelial injury and coagulopathy in pediatric animal models of high VT

Mode of Ventilation (set versus controlled variables) ARDSNet – volume controlled Pediatric – Pressure control - PC or PRVC (volume targeted but
decelerating flow) Developmental Differences (changes in proportion of FRC, TLC, VT)
Body weight for calculating tidal volume
Adult: predicted BW (obesity, BW calculated from height) Pediatric: actual BW (obesity & FTT, contractures; now formulae for height
from ulnar length 0 < 18 years old)
Tidal Volume (VT exhaled) Adult: measured at ventilator – use SET volume Pediatrics: should be measured at ETT (tubing compliance)



More inotropres, more NMB, more sedatives in HFOV


Guerin NEJM June 2013

Curley et al. JAMA 2005
No improvement in clinically important outcomes, stopped early for futility Very low mortality, 8%.
PF =150 OI=14-18 VT=6-8 PEEP=7-9

Disease severity - Moderate ARDS (Peds) vs. Severe (Adults)
Chest Wall compliance issues- Age effects? Optimal use of Lung protective ventilation? Adults studies only have shown benefit when good LPV
being used
High Rate of HFOV use in both arms in pediatrics
Is VILI as big of a problem in PARDS as adults? Recruitability of lung disease Higher rates of sepsis in adults (? More recruitable
lung)



1. Timing √
2. Age √
3. Co-existence with cardiac failure/dysfunction √
4. What are best respiratory criteria for risk stratification/disease severity √
5. How do we handle patients on non-invasive ventilation and/or those without arterial lines √
6. How important/reliable are Radiographic Criteria for Definition of ARDS √
7. Defining it in patients with pre-existing cardiac or pulmonary co-morbidities √

OI = oxygenation index = (FiO2* mean airway pressure*100)/ PaO2
OSI = oxygen saturation index = (FiO2* mean airway pressure*100) /SpO2
Age Exclude patients with peri-natal related lung disease
Timing Within 7 days of known clinical insult
Origin of Edema Respiratory failure not fully explained by cardiac failure or fluid overload
Chest Imaging Chest imaging findings of new infiltrate(s) consistent with acute pulmonary parenchymal disease
Oxygenation
Non Invasive mechanical ventilation Invasive mechanical ventilation
PARDS (No severity stratification) Mild Moderate Severe
Full face-mask bi-level ventilation or CPAP ≥5 cm H20 2
PF ratio ≤ 300 SF ratio ≤ 264 1
4 ≤ OI < 8
5 ≤ OSI < 7.51
8 ≤ OI < 16
7.5 ≤ OSI < 12.31
OI ≥ 16
OSI ≥ 12.31
Special Populations
Cyanotic Heart Disease
Standard Criteria above for age, timing, origin of edema and chest imaging with an acute deterioration in oxygenation not explained by underlying cardiac disease. 3
Chronic Lung Disease
Standard Criteria above for age, timing, and origin of edema with chest imaging consistent with new infiltrate and acute deterioration in oxygenation from baseline which meet oxygenation criteria above.3
Left Ventricular dysfunction
Standard Criteria for age, timing and origin of edema with chest imaging changes consistent with new infiltrate and acute deterioration in oxygenation which meet criteria above not explained by left ventricular dysfunction.