Hypertensive crisis management in hypoxemic situations in ICU. Impact of hypoxic pulmonary vasoconstriction.

Hypoxic pulmonary vasoconstriction & hypertensive crisis
Aug 15, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Hypertensive crisis management in hypoxemic situations in ICU.
Impact of hypoxic pulmonary vasoconstriction.

Hypoxic pulmonary vasoconstriction inhibition & hypertensive crisis management
1. Case report: vasodilator-induced worsening of hypoxia. Inhibition of hypoxic pulmonary vasoconstriction (HPV).
2. Underlying compensatory mechanisms in hypoxia: HPV1. Physiological role2. Efficiency3. Ablation4. Mechanism
3. Hypertensive crisis in hypoxia1. Understanding2. Management

1. Vasodilator-induced worsening of hypoxia: Role of inhibition of hypoxic pulmonary vasoconstriction (HPV).
• 55-year old man with hypoxemic pneumonia– initial traumatic cervical & thoracic vertebral fracture– nosocomial Pseudomonas aeruginosa & Haemophilus influenzae infection (day 10)– rapidly progressing ARDS– ceftazidime/ciprofloxacine, mechanical ventilation, inhaled NO, tracheotomy (day 18)– favorable evolution– FiO2 45%; SpO2: 98%; PaO2=111 mmHg; PaCO2=41mmHg; pH=7.48 (day 20)
• hypertension > 180mmHg (day 20)– probably associated with sympathetic hyperactivity (concomitant with awakening)– treated with i.v. vasodilator: nicardipine i.v. 4mg/h
• worsening of hypoxia– FiO2 45%; SpO2: 92%; PaO2=60 mmHg; PaCO2=41mmHg; pH=7.5– withdrawal of nicardipine– favorable evolution with FiO2 80%: SpO2=100%
Cotte J, et al. Rev Pneumol Clin (2012)
Inhaled Nitric Oxide in refractory hypoxemia in ARDS
Inhaled Nitric Oxide: • potent vasodilator• delivered directly to ventilated areas to improve ventilation-perfusion
mismatch• results in improved oxygenation• relieving pulmonary hypertension resulting from regional hypoxia. The current evidence:• suggests that inhaled nitric oxide should not be routinely used in patients
with ARDS• may be considered as adjunctive therapy in selected patients (eg, those
with coexisting pulmonary hypertension) to transiently improve oxygenation in patients with severe ARDS while other therapies are considered.
Pipeling M, et al. JAMA. 2010;304(22):2521-2527

Effects of systemic vasodilation (from intravenous, subcutaneous, or oral administration) versus selective pulmonary vasodilation (from inhalation).
Siobal M, et al. Respir Care 2010;55(2):144 –157.

In contrast to iNO and inhaled prostacyclin (PGE1), intravenous prostacyclin caused systemic vasodilation, which worsened arterial oxygenation in ARDS.
Siobal M, et al. Respir Care 2010;55(2):144 –157.
PaO2 with inhaled or infused prostacyclin or inhaled nitric oxide (INO) in 10 adult patients with acute respiratory distress syndrome.
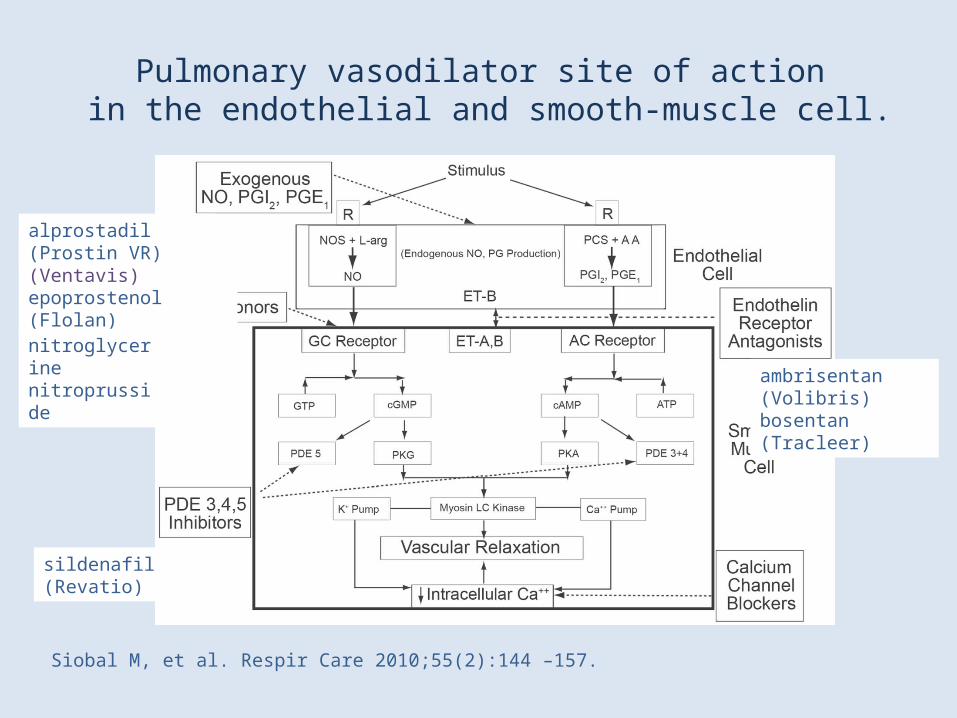
Pulmonary vasodilator site of action in the endothelial and smooth-muscle cell.
Siobal M, et al. Respir Care 2010;55(2):144 –157.
iloprost (Ventavis)epoprostenol (Flolan)
ambrisentan (Volibris)bosentan (Tracleer)
alprostadil (Prostin VR)
sildenafil (Revatio)
nitroglycerinenitroprusside
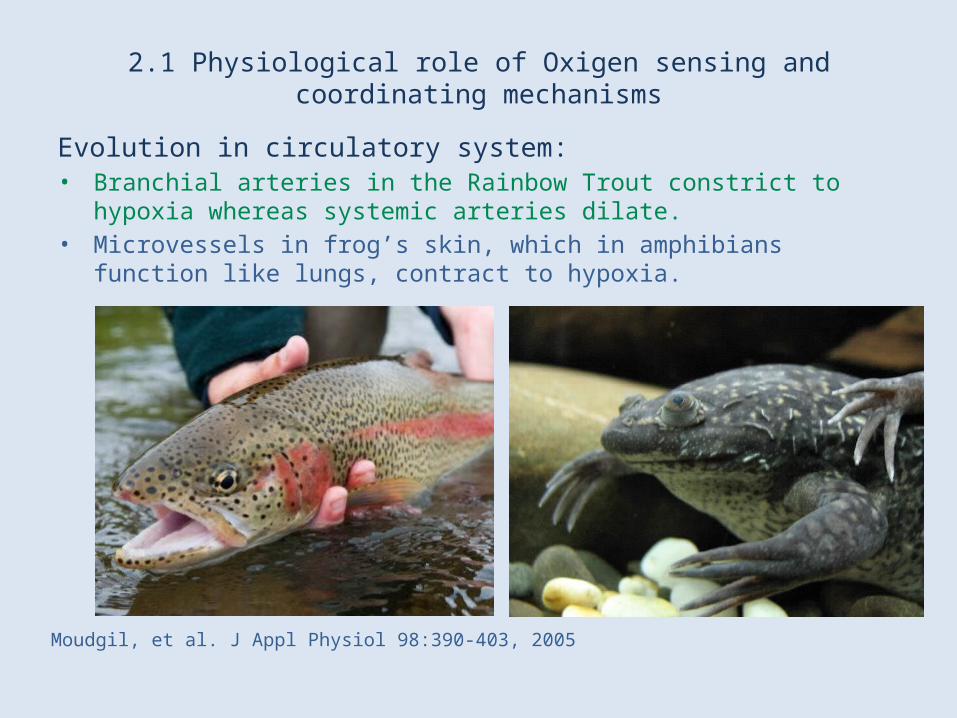
2.1 Physiological role of Oxigen sensing and coordinating mechanisms
Evolution in circulatory system: • Branchial arteries in the Rainbow Trout constrict to hypoxia whereas systemic
arteries dilate.• Microvessels in frog’s skin, which in amphibians function like lungs, contract to
hypoxia.
Moudgil, et al. J Appl Physiol 98:390-403, 2005
2.1a Physiological role of Hypoxic Pulmonary Vasoconstriction
HPV: • adaptive vasomotor response to alveolar hypoxia• redistributes blood to optimally ventilated lung segments • active process of vasoconstriction involving the small muscular
“resistance” pulmonary arteries (PA)
Simultaneous systemic opposing response:• hypoxia dilates most arteries• decrease of systemic vascular resistance (e.g. renal vasodilation)
Moudgil, et al. J Appl Physiol 98:390-403, 2005
2.1b Physiological role of Hypoxic Pulmonary Vasoconstriction
Elicited by: • moderate physiologically relevant hypoxia (e.g. summit of Mount Everest)
Kinetics in response to hypoxia:• onsets in minutes• reaching a maximum within 15 min• can be sustained for hours• exposure for 3 h can elicit selective suppression of HPV (down-regulation)
Moudgil, et al. J Appl Physiol 98:390-403, 2005

2.1c Physiological role of Hypoxic Pulmonary Vasoconstriction
Genetical adaptation to life in high altitude: • The Yak and the native Tibetan have weak or absent HPV
Moudgil, et al. J Appl Physiol 98:390-403, 2005
Picture: http://www.mantra-tibet.com
2.1d Physiological regulation of HPV
HPV is inhibited by: • substance P• calcitonine gene-related peptide• atrial natriuretic peptides• endothelium-derived vasodilators
– prostacylin– nitric oxide (NO)
• alpha-adrenergic blockade• beta-adrenergic stimulation• increased left atrial pressure• increased alveolar pressure• alkalosis• peripheral chemoreceptor stimulation
Naeije R, et al. Critical Care 2001, 5:67–71
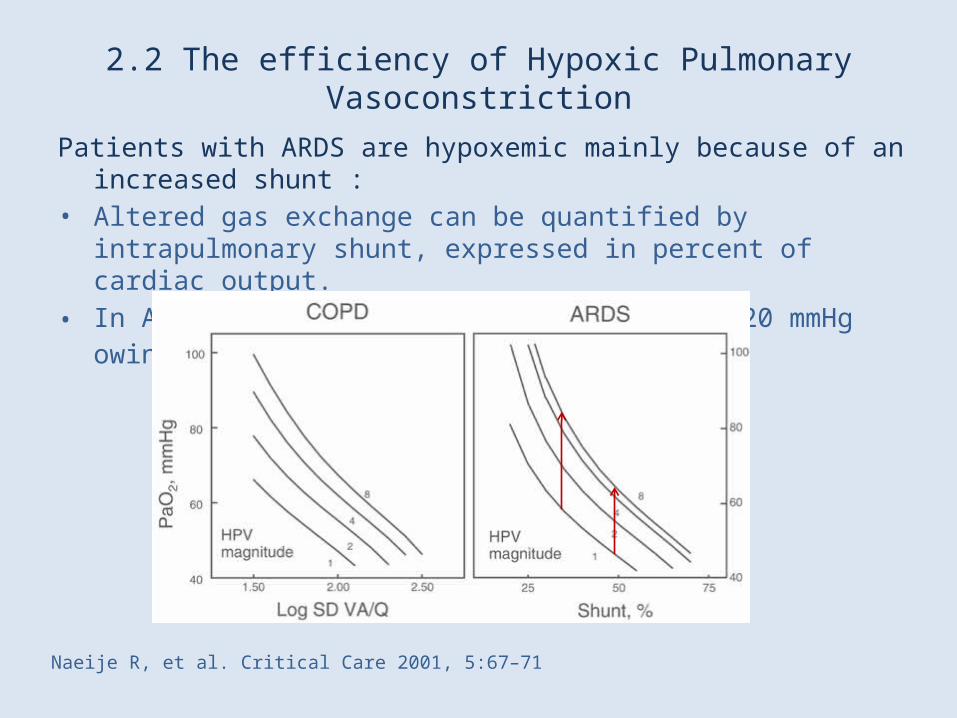
2.2 The efficiency of Hypoxic Pulmonary Vasoconstriction
Patients with ARDS are hypoxemic mainly because of an increased shunt : • Altered gas exchange can be quantified by intrapulmonary shunt, expressed
in percent of cardiac output. • In ARDS, PaO2 may increase by as much as 20 mmHg owing to vigorous HPV.
Naeije R, et al. Critical Care 2001, 5:67–71
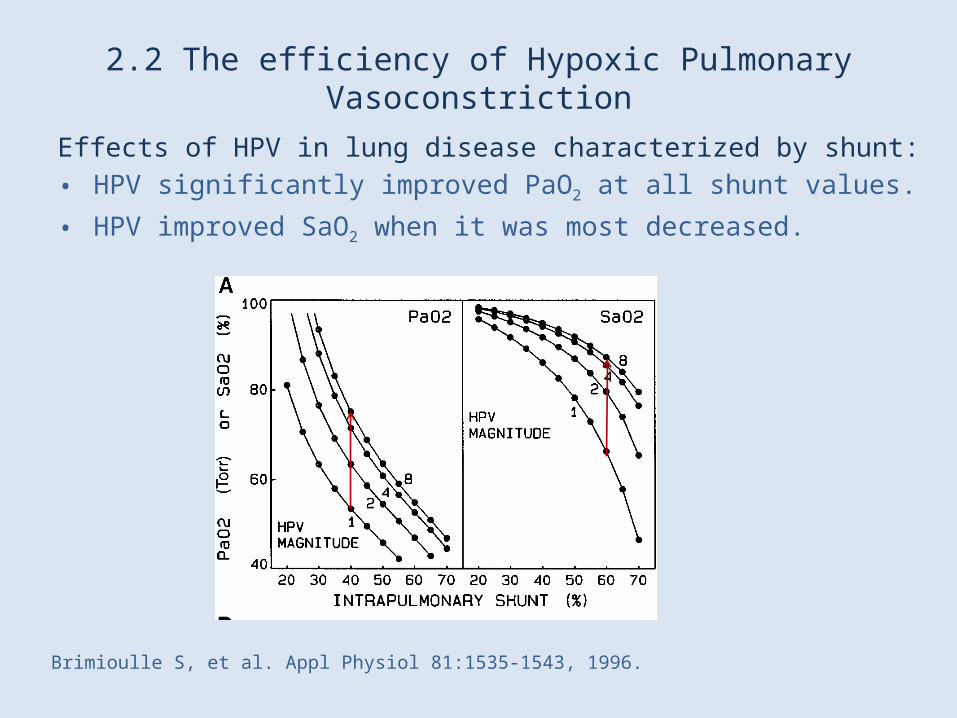
2.2 The efficiency of Hypoxic Pulmonary Vasoconstriction
Effects of HPV in lung disease characterized by shunt: • HPV significantly improved PaO2 at all shunt values.
• HPV improved SaO2 when it was most decreased.
Brimioulle S, et al. Appl Physiol 81:1535-1543, 1996.
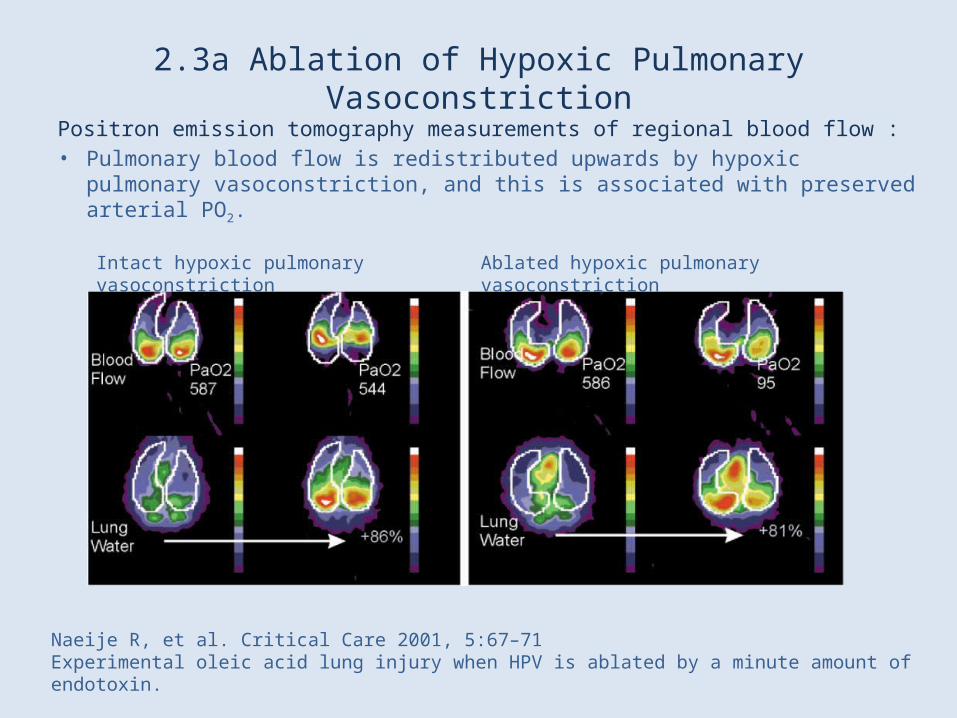
2.3a Ablation of Hypoxic Pulmonary Vasoconstriction
Positron emission tomography measurements of regional blood flow : • Pulmonary blood flow is redistributed upwards by hypoxic pulmonary
vasoconstriction, and this is associated with preserved arterial PO2.
Naeije R, et al. Critical Care 2001, 5:67–71Experimental oleic acid lung injury when HPV is ablated by a minute amount of endotoxin.
Intact hypoxic pulmonary vasoconstriction Ablated hypoxic pulmonary vasoconstriction
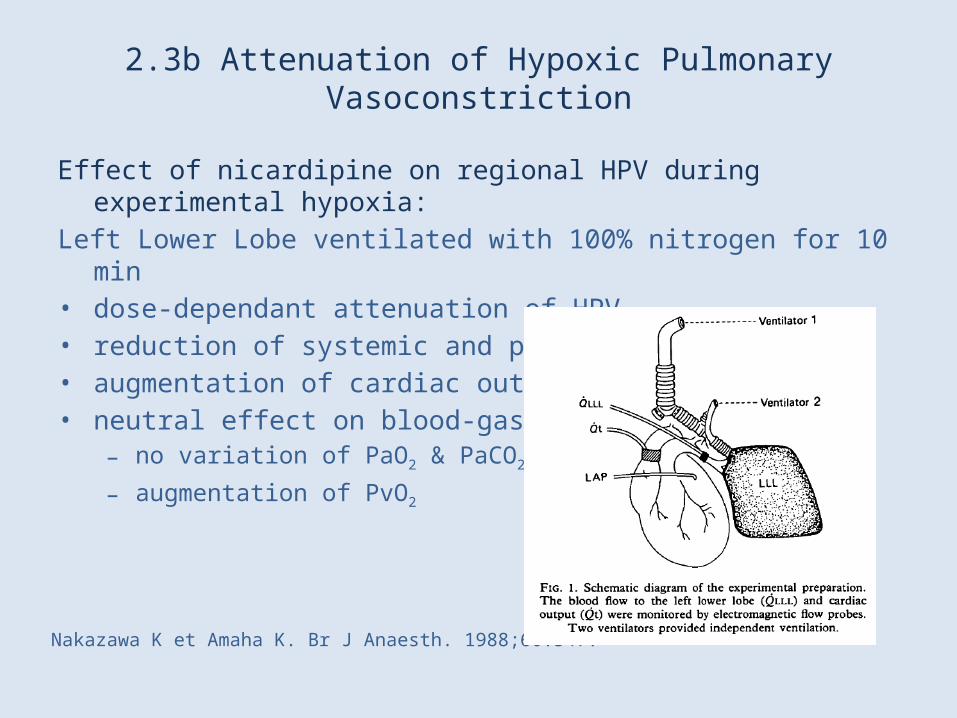
2.3b Attenuation of Hypoxic Pulmonary Vasoconstriction
Effect of nicardipine on regional HPV during experimental hypoxia:Left Lower Lobe ventilated with 100% nitrogen for 10 min• dose-dependant attenuation of HPV• reduction of systemic and pulmonary resistances• augmentation of cardiac output• neutral effect on blood-gas variables:
– no variation of PaO2 & PaCO2
– augmentation of PvO2
Nakazawa K et Amaha K. Br J Anaesth. 1988;60:547.
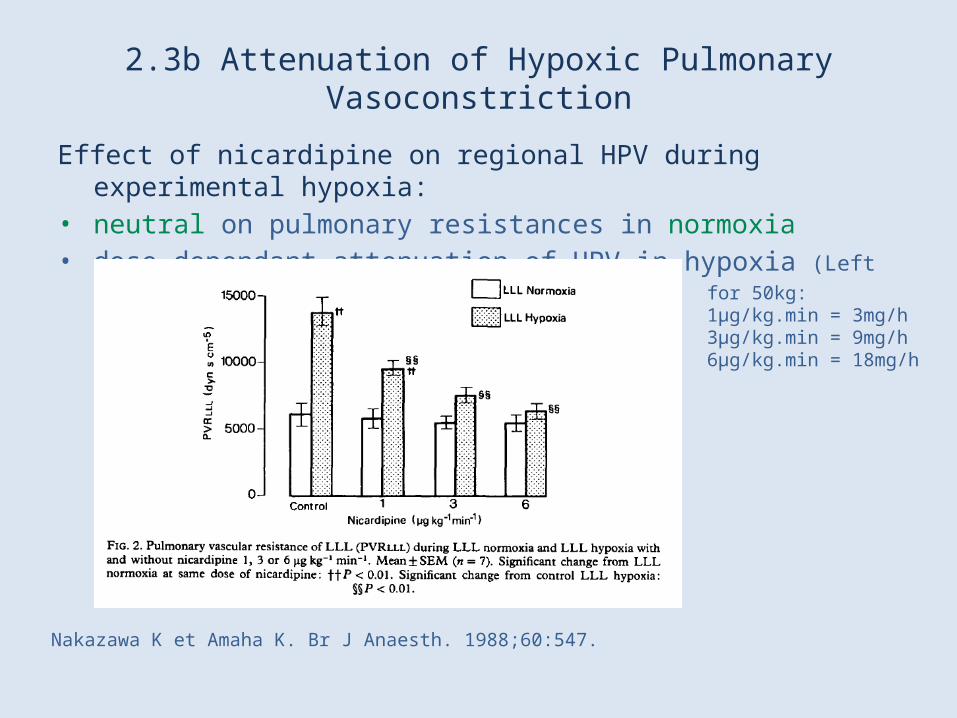
2.3b Attenuation of Hypoxic Pulmonary Vasoconstriction
Effect of nicardipine on regional HPV during experimental hypoxia:• neutral on pulmonary resistances in normoxia• dose-dependant attenuation of HPV in hypoxia (Left Lower Lobe: 100% nitrogen)
Nakazawa K et Amaha K. Br J Anaesth. 1988;60:547.
for 50kg:1µg/kg.min = 3mg/h3µg/kg.min = 9mg/h6µg/kg.min = 18mg/h
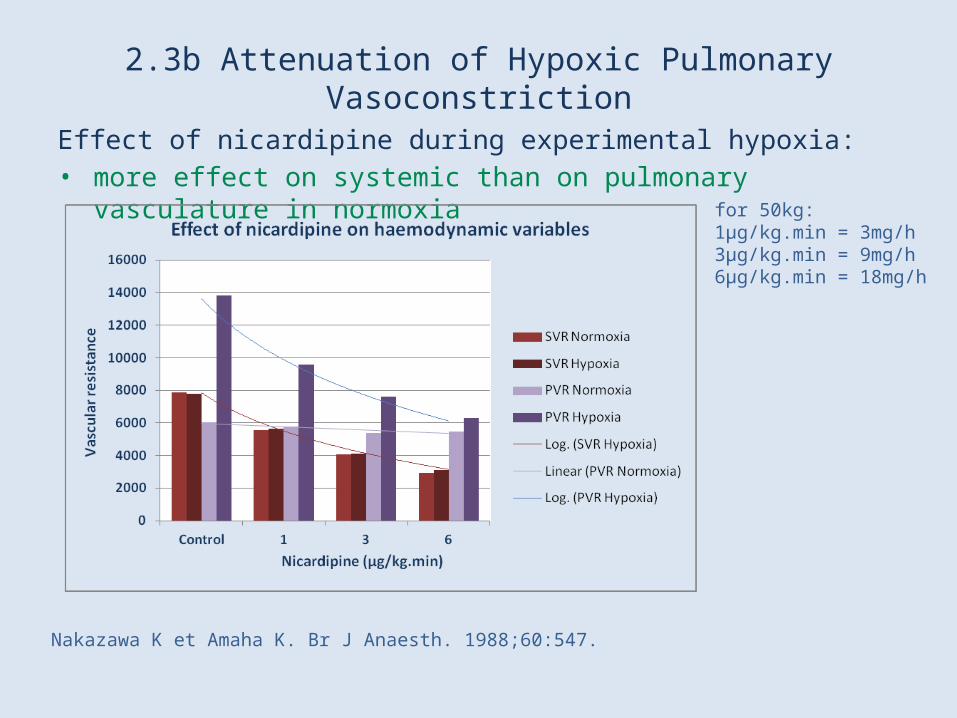
2.3b Attenuation of Hypoxic Pulmonary Vasoconstriction
Effect of nicardipine during experimental hypoxia:• more effect on systemic than on pulmonary vasculature in normoxia
Nakazawa K et Amaha K. Br J Anaesth. 1988;60:547.
for 50kg:1µg/kg.min = 3mg/h3µg/kg.min = 9mg/h6µg/kg.min = 18mg/h
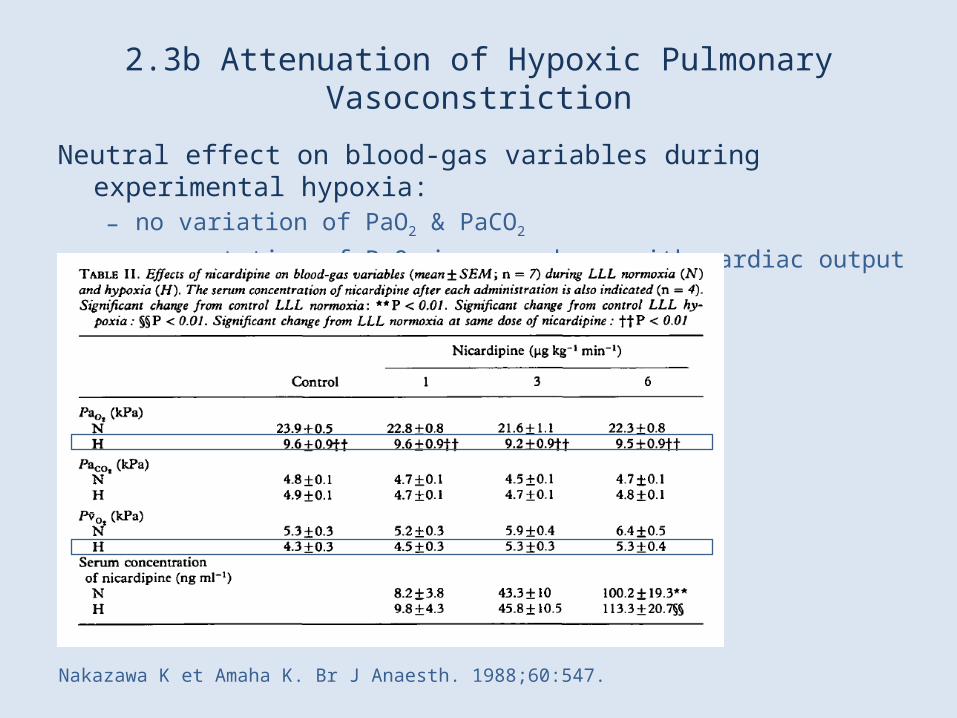
2.3b Attenuation of Hypoxic Pulmonary Vasoconstriction
Neutral effect on blood-gas variables during experimental hypoxia:– no variation of PaO2 & PaCO2
– augmentation of PvO2 in accordance with cardiac output
Nakazawa K et Amaha K. Br J Anaesth. 1988;60:547.
2.4 Mechanism of Hypoxic Pulmonary Vasoconstriction
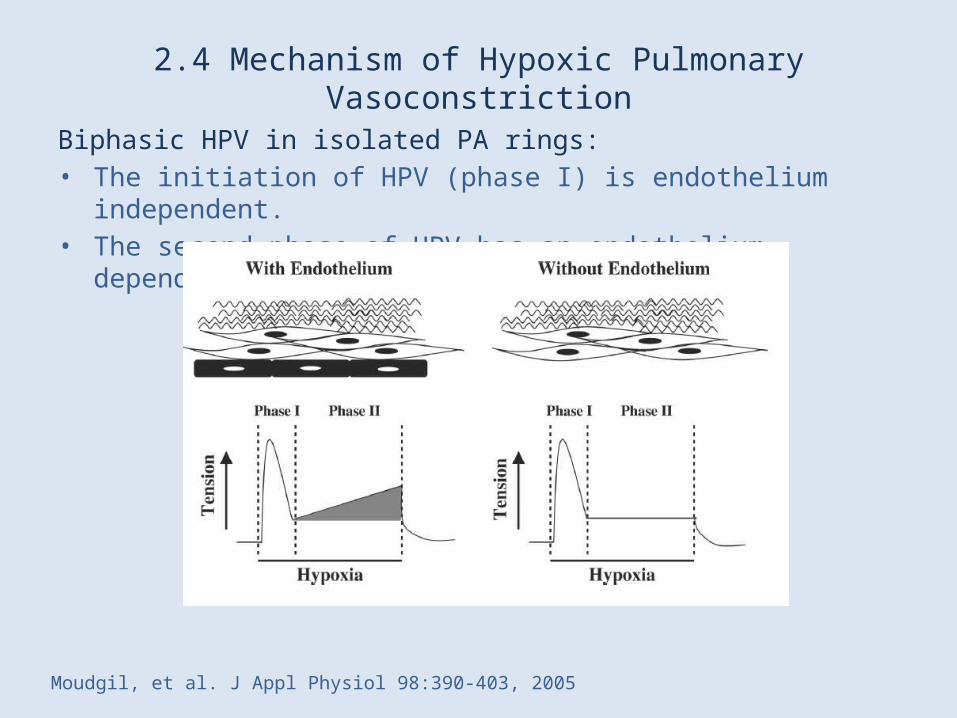
Biphasic HPV in isolated PA rings: • The initiation of HPV (phase I) is endothelium independent.• The second phase of HPV has an endothelium-dependent component to it.
Moudgil, et al. J Appl Physiol 98:390-403, 2005
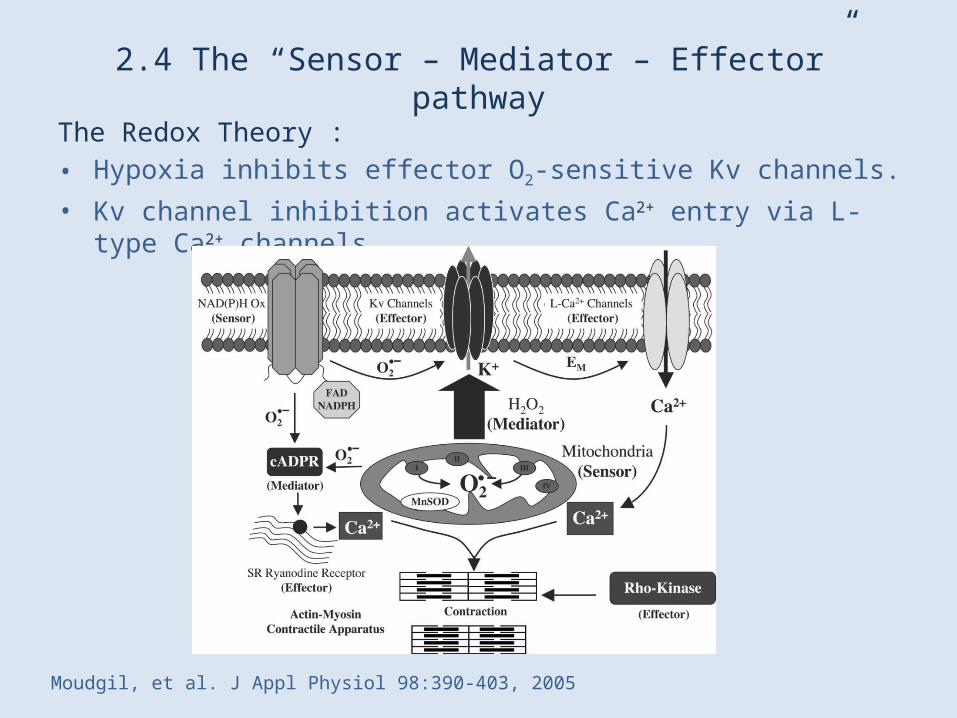
2.4 The “Sensor – Mediator – Effector” pathway
The Redox Theory : • Hypoxia inhibits effector O2-sensitive Kv channels. • Kv channel inhibition activates Ca2+ entry via L-type Ca2+ channels.
Moudgil, et al. J Appl Physiol 98:390-403, 2005

2.4 Minor influence of CCB on HPV
Calcium channel blockers (nifedipine, isoptine, diltiazem): • partially blunted phase I, but did not affect phase II of HPV.
Hypoxia under control & following preincubation with verapamil
Hypoxia under control & following preincubation with nifedine
Robertson et al. Journal of Physiology (2000), 525.3, pp. 669—680

Origins of Ca2+ in hypoxic pulmonary vasoconstriction
• Depolarization-mediated Ca2+ influx plays at best a minor role in the transient phase I constriction of HPV, and is not involved in the sustained phase II constriction.
• Phase I appears to be mainly dependent on capacitative Ca2+ entry (CCE) related to release of Ca2+ stores.
• Phase II is supported by Ca2+ entry via a separate voltage-independent pathway.
Robertson et al. Journal of Physiology (2000), 525.3, pp. 669—680

2.4 Role of multiple ion channels in HPV
The multiple ion channels Theory : • inhibition of voltage-gated K (Kv)• membrane potential (Em)
depolarization• activation of voltage-dependent Ca2+
channels (VDCC)• activation of inositol-1,4,5-
triphosphate receptor (IP3-R) and ryanodine receptors (RyR) in the sarcoplasmic reticulum (SR)
• Ca2+ release indirectly activating store-operated Ca2+ channels (SOC)
• induction of capacitative Ca2+ entry (CCE) by depleting Ca2+ from the SR
• indirectly opening of Ca2+-activated Cl (ClCa) channels (due to released Ca2+)
• inducing Em depolarization.
Mauban J, et al. J Appl Physiol 98:415-420, 2005.
Mechanisms of hypoxic pulmonary vasoconstriction• HPV
– is mediated via K+ channel inhibition and Ca2+ entry in arteriolar smooth muscle cells.
Sommer et al. Eur Respir J 2008; 32: 1639–1651

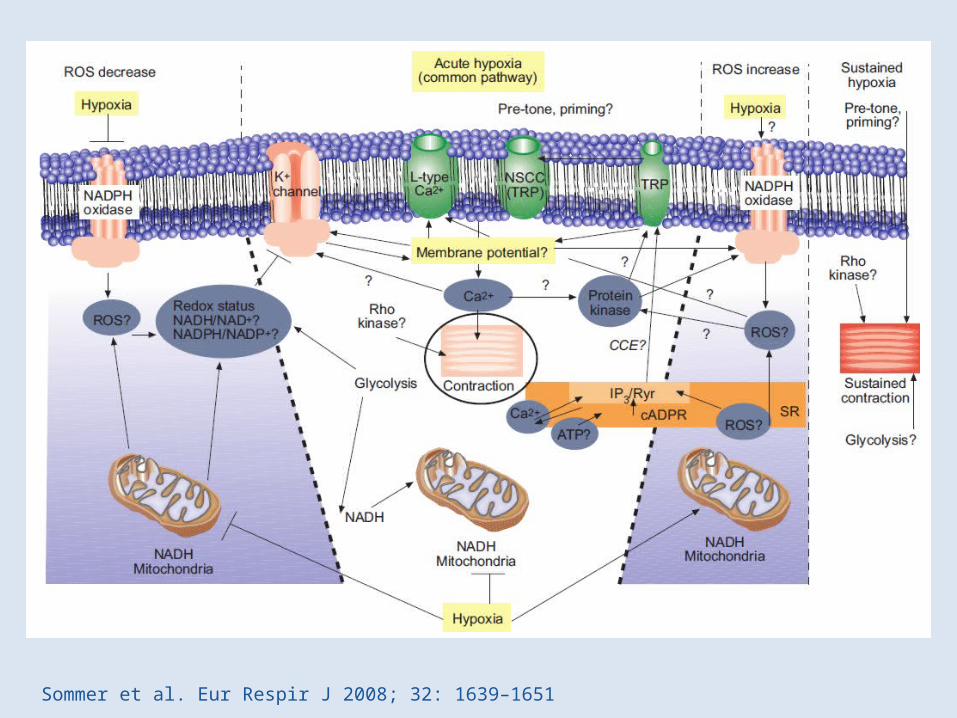
2.4 Mechanisms of hypoxic pulmonary vasoconstriction
The effector pathway is suggested to include:• voltage-dependent K+ channels• L-type calcium channels• nonspecific cation channels
Mitochondria and NADPH oxidases are discussed as oxygen sensors.
Sommer et al. Eur Respir J 2008; 32: 1639–1651

3.1 Hypertensive crisis in hypoxia: understanding
Paradoxal augmentation of peripheral resistance ?• probably associated with sympathetic hyperactivity
– (e.g. concomitant with awakening)
Classical etiological management of hypertensive crisis:• insufficient analgesia• awakening• hypervolemia• urethral obstruction• rebound (clonidine)• hypothermia / malignant hyperthermia• intracranial hypertension
Cotte J, et al. Rev Pneumol Clin (2012)Albrecht et al. In “Manuel pratique d’anesthésie”. Ed Masson. 2009

3.2 Hypertensive crisis in hypoxia: management ?
Acute respiratory Distress Syndrome treatment guidelines: • No mention of hypertensive crisis management• Negative fluid balance was associated with better outcome• Vasoconstrictors can improve oxygenation in ARDS patients by decreasing
intrapulmonary shunt.
Hypertensive crisis treatments guidelines: • No mention of respiratory distress• Role of excessive circulating catecholamines ??
Pierrakos C, et al. J Clin Med Res • 2011;4(1):7-16Grossman E, et al. Drug Safety 1998;19(2):99-122

3.2 Sympathetic crisis in hypoxia: management ?
Dutch guidelines – 2010 revision:Recommended treatment of autonomic hyperreactivity: • Phentolamine• Nitroprusside, urapidil
American recommendations – 2007 update:Recommended antihypertensive agents for sympathetic crisis: • Nicardipine, verapamil, diltiazem in combination with a benzodiazepine• “experimental studies do not support the use of labetalol in this setting”
! All of these vasodilators could potentially depress the hypoxic pulmonary vasoconstrictor response !
Marik PE et Varon J. CHEST 2007; 131:1949–1962Van den Born, et al. The Netherlands J of Medicine May 2011;vol69(5):248
Conclusion: Traditional “British empiricism” as a guideline
“It is concluded that since NG and SNP appear to produce arterial hypoxaemia by depressing the hypoxic pulmonary vasoconstrictor response, their administration should be accompanied by oxygen enrichment of the inspired gases and careful monitoring on PaO2.”D’Oliveira M, et al.Br J Anesthesia 1981;53:11
The experimental and clinical evidences call for a careful approach with all vasodilators without exception.The risk-benefit ratio of vasodilators should always be carefully evaluated in case of hypertensive crisis management in patient with potential pulmonary vasoconstriction .
D’Oliveira M, et al. Br J Anesthesia 1981;53:11
Related Documents











