


Clinical Medical & Case Reports
Open Journal of
ISSN2379-1039
Volume3(2017)Issue1
YadavS
OpenJClinMedCaseRep:Volume3(2017)
Pleomorphiclobularcarcinomaofbreast–cytologicalcharacteristicsanddifferentialsKavitaMunjal;SomaYadav*;DeepakAgarwal
*SomaYadav
MetropolisHealthcareLtd.India
Email:[email protected]
Abstract
Pleomorphic lobularcarcinomaofbreast(IPLC) isaveryrareanddistinctmorphologicalvariantof
invasivelobularcarcinoma(ILC),characterizedbynuclearatypiaandpleomorphismcontrastedwiththe
cytologicuniformityofILC.Alsoitisassociatedwithpoorprognosis.Thus,cytologicalrecognitionofthis
tumourisimportant.Wereportacasewiththisunusualtumourina�iftyeightyearoldfemalethat
presentedasadiagnosticdilemmaoncytology.
Introduction
Pleomorphiclobularcarcinoma(PLC)ofbreastisadistincthistologicalvariantofinvasivelobular
carcinoma(ILC)[1,2,3,4,5].Cytologicalrecognitionisimportantasthedegreeofpleomorphismexhibited
inthisspeci�icsubtypemayleadtomisinterpretationofthisparticularsubtypeoflobularcarcinomaas
in�iltratingductalcarcinoma.Also,itisassociatedwithaggressiveclinicalcourseinhavinglargersize,
markedcytologicatypia,morepronetodistantmetastasis,higherchanceoflymphovascularinvasionand
presentation at ahigher stage [6,7,8,9,10].The cytological literatureon this entity is very little.We
present a case of Pleomorphic Lobular Carcinoma diagnosed retrospectively, discuss the cytologic
featuresthatareusefulintherecognitionofthisentityandthediagnosticpitfalls.
CasePresentation
A �ifty eight year old female presented with a three month history of a self-discovered,
progressivelyincreasing,painlesspalpablelumpintheleftbreast.Shehadnosigni�icantmedicalhistory.
Therewasnofamilyhistoryofbreastdisease.Onphysicalexamination,arelativelyill-de�ined�irmmass
measuring7x6cmwaspalpableintheouterquadrant.Theoverlyingskinappearednormal.Therewas
evidenceofpalpablelymphadenopathyintheipsilateralaxilla.Mammographyreportedwell-de�ined
asymmetricdensityintheleftbreast(BIRADS-4).FineNeedleAspirationCytology(FNAC)wasdoneand
thesmearsshowedscantycellularitywithoccasionalcellsshowinglargenuclei.Asthenumberofthese
largecellswereveryfewandnoconclusioncouldbedrawnarepeataspirationwasperformedwhichwas
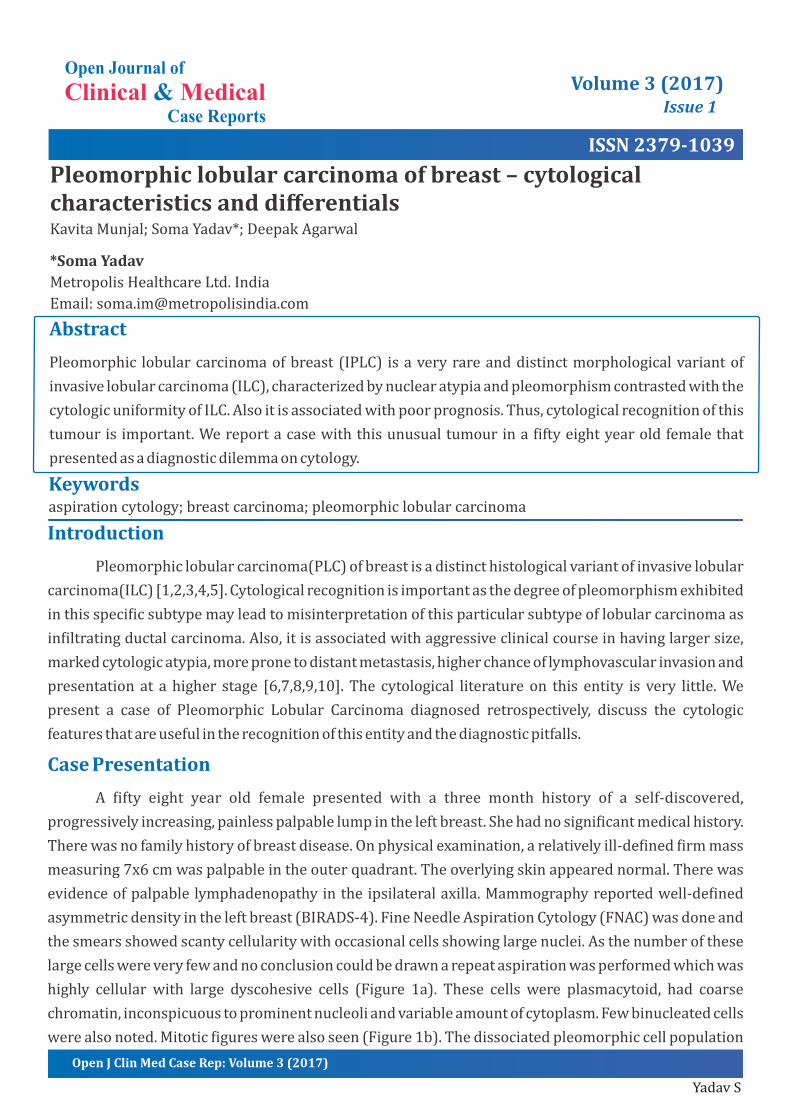
highly cellular with large dyscohesive cells (Figure 1a). These cells were plasmacytoid, had coarse
chromatin,inconspicuoustoprominentnucleoliandvariableamountofcytoplasm.Fewbinucleatedcells
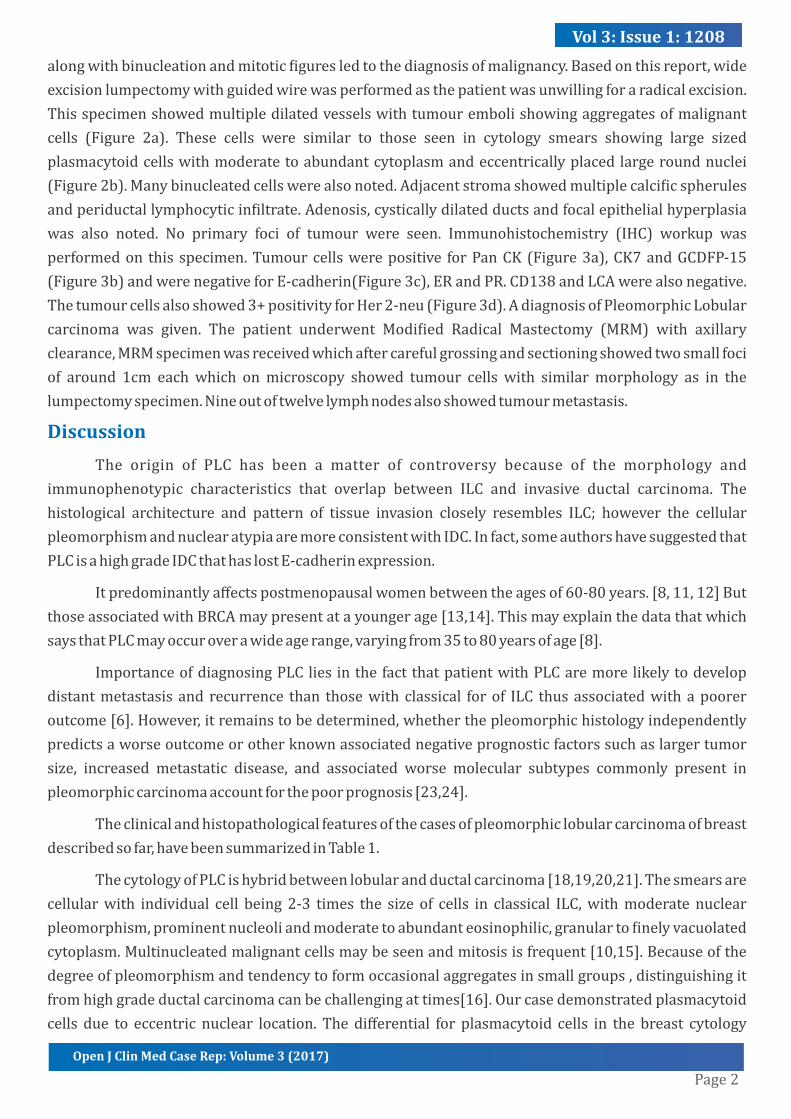
werealsonoted.Mitotic�igureswerealsoseen(Figure1b).Thedissociatedpleomorphiccellpopulation
Keywordsaspirationcytology;breastcarcinoma;pleomorphiclobularcarcinoma
Page2
Vol3:Issue1:1208
OpenJClinMedCaseRep:Volume3(2017)
alongwithbinucleationandmitotic�iguresledtothediagnosisofmalignancy.Basedonthisreport,wide
excisionlumpectomywithguidedwirewasperformedasthepatientwasunwillingforaradicalexcision.
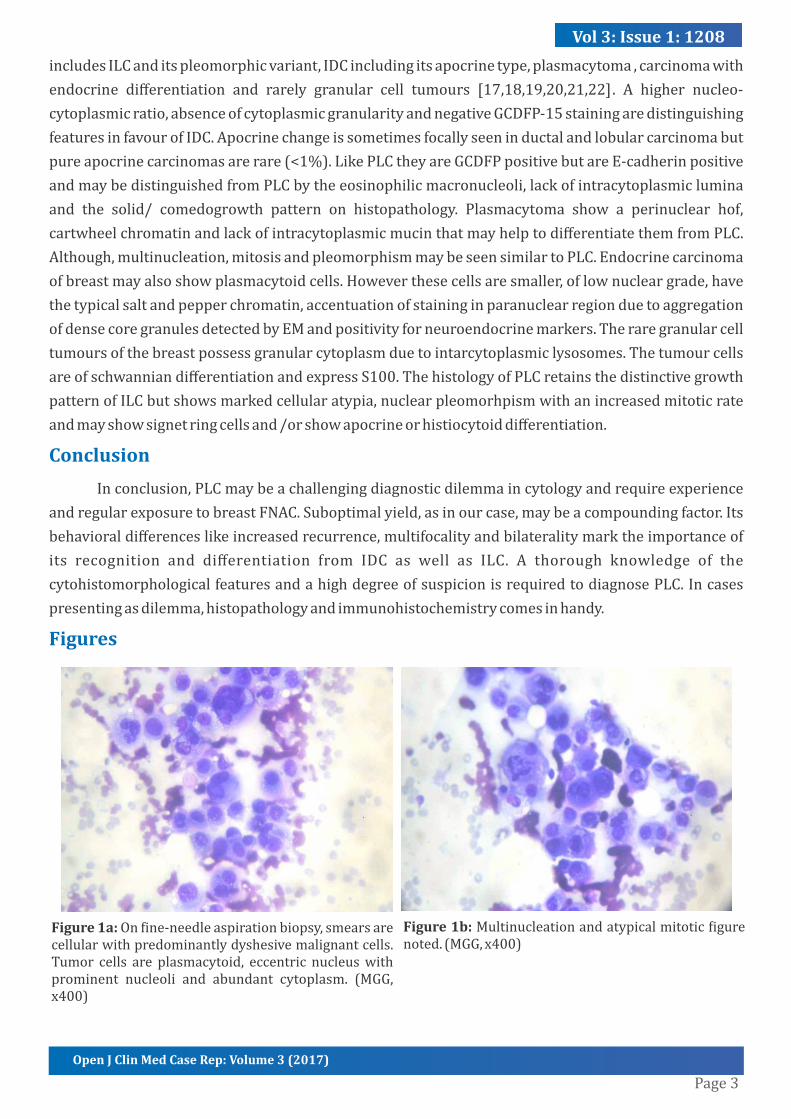
Thisspecimenshowedmultipledilatedvesselswithtumourembolishowingaggregatesofmalignant
cells (Figure 2a). These cells were similar to those seen in cytology smears showing large sized
plasmacytoidcellswithmoderatetoabundantcytoplasmandeccentricallyplacedlargeroundnuclei
(Figure2b).Manybinucleatedcellswerealsonoted.Adjacentstromashowedmultiplecalci�icspherules
andperiductallymphocyticin�iltrate.Adenosis,cysticallydilatedductsandfocalepithelialhyperplasia
was also noted. No primary foci of tumour were seen. Immunohistochemistry (IHC) workup was
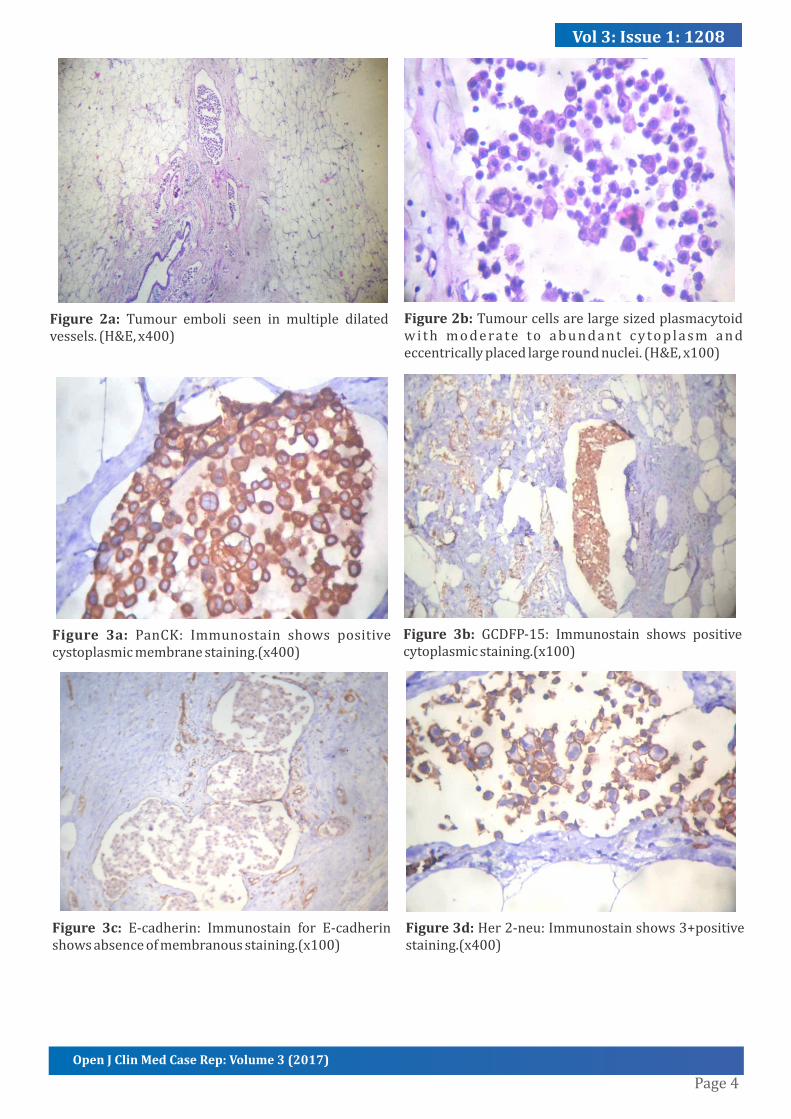
performedon this specimen.Tumourcellswerepositive forPanCK(Figure3a),CK7andGCDFP-15
(Figure3b)andwerenegativeforE-cadherin(Figure3c),ERandPR.CD138andLCAwerealsonegative.
Thetumourcellsalsoshowed3+positivityforHer2-neu(Figure3d).AdiagnosisofPleomorphicLobular
carcinoma was given. The patient underwent Modi�ied Radical Mastectomy (MRM) with axillary
clearance,MRMspecimenwasreceivedwhichaftercarefulgrossingandsectioningshowedtwosmallfoci
of around 1cm eachwhich onmicroscopy showed tumour cells with similarmorphology as in the
lumpectomyspecimen.Nineoutoftwelvelymphnodesalsoshowedtumourmetastasis.
Discussion
The origin of PLC has been a matter of controversy because of the morphology and
immunophenotypic characteristics that overlap between ILC and invasive ductal carcinoma. The
histological architecture and pattern of tissue invasion closely resembles ILC; however the cellular
pleomorphismandnuclearatypiaaremoreconsistentwithIDC.Infact,someauthorshavesuggestedthat
PLCisahighgradeIDCthathaslostE-cadherinexpression.
Itpredominantlyaffectspostmenopausalwomenbetweentheagesof60-80years.[8,11,12]But
thoseassociatedwithBRCAmaypresentatayoungerage[13,14].Thismayexplainthedatathatwhich
saysthatPLCmayoccuroverawideagerange,varyingfrom35to80yearsofage[8].
ImportanceofdiagnosingPLCliesinthefactthatpatientwithPLCaremorelikelytodevelop
distantmetastasis and recurrence than thosewith classical forof ILC thusassociatedwithapoorer
outcome[6].However,itremainstobedetermined,whetherthepleomorphichistologyindependently
predictsaworseoutcomeorotherknownassociatednegativeprognosticfactorssuchaslargertumor
size, increased metastatic disease, and associated worse molecular subtypes commonly present in
pleomorphiccarcinomaaccountforthepoorprognosis[23,24].
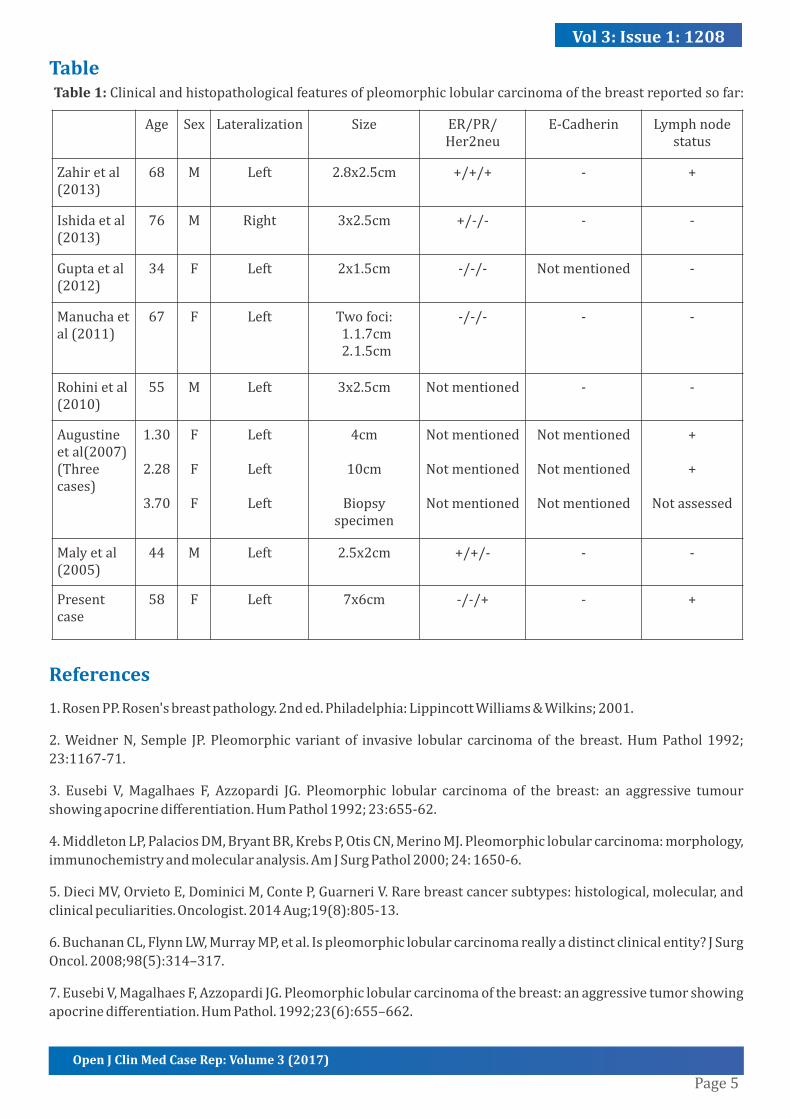
Theclinicalandhistopathologicalfeaturesofthecasesofpleomorphiclobularcarcinomaofbreast
describedsofar,havebeensummarizedinTable1.
ThecytologyofPLCishybridbetweenlobularandductalcarcinoma[18,19,20,21].Thesmearsare
cellularwith individual cell being 2-3 times the size of cells in classical ILC,withmoderate nuclear
pleomorphism,prominentnucleoliandmoderatetoabundanteosinophilic,granularto�inelyvacuolated
cytoplasm.Multinucleatedmalignantcellsmaybeseenandmitosisisfrequent[10,15].Becauseofthe
degreeofpleomorphismandtendencytoformoccasionalaggregatesinsmallgroups,distinguishingit
fromhighgradeductalcarcinomacanbechallengingattimes[16].Ourcasedemonstratedplasmacytoid
cells due to eccentric nuclear location. Thedifferential for plasmacytoid cells in the breast cytology
Page3
Vol3:Issue1:1208
OpenJClinMedCaseRep:Volume3(2017)
includesILCanditspleomorphicvariant,IDCincludingitsapocrinetype,plasmacytoma,carcinomawith
endocrine differentiation and rarely granular cell tumours [17,18,19,20,21,22]. A higher nucleo-
cytoplasmicratio,absenceofcytoplasmicgranularityandnegativeGCDFP-15stainingaredistinguishing
featuresinfavourofIDC.Apocrinechangeissometimesfocallyseeninductalandlobularcarcinomabut
pureapocrinecarcinomasarerare(<1%).LikePLCtheyareGCDFPpositivebutareE-cadherinpositive
andmaybedistinguishedfromPLCbytheeosinophilicmacronucleoli,lackofintracytoplasmiclumina
and the solid/ comedogrowth pattern on histopathology. Plasmacytoma show a perinuclear hof,
cartwheelchromatinandlackofintracytoplasmicmucinthatmayhelptodifferentiatethemfromPLC.
Although,multinucleation,mitosisandpleomorphismmaybeseensimilartoPLC.Endocrinecarcinoma
ofbreastmayalsoshowplasmacytoidcells.Howeverthesecellsaresmaller,oflownucleargrade,have
thetypicalsaltandpepperchromatin,accentuationofstaininginparanuclearregionduetoaggregation
ofdensecoregranulesdetectedbyEMandpositivityforneuroendocrinemarkers.Theraregranularcell
tumoursofthebreastpossessgranularcytoplasmduetointarcytoplasmiclysosomes.Thetumourcells
areofschwanniandifferentiationandexpressS100.ThehistologyofPLCretainsthedistinctivegrowth
patternofILCbutshowsmarkedcellularatypia,nuclearpleomorhpismwithanincreasedmitoticrate
andmayshowsignetringcellsand/orshowapocrineorhistiocytoiddifferentiation.
Conclusion
Inconclusion,PLCmaybeachallengingdiagnosticdilemmaincytologyandrequireexperience
andregularexposuretobreastFNAC.Suboptimalyield,asinourcase,maybeacompoundingfactor.Its
behavioraldifferenceslikeincreasedrecurrence,multifocalityandbilateralitymarktheimportanceof
its recognition and differentiation from IDC as well as ILC. A thorough knowledge of the
cytohistomorphologicalfeaturesandahighdegreeofsuspicionisrequiredtodiagnosePLC.Incases
presentingasdilemma,histopathologyandimmunohistochemistrycomesinhandy.
Figures
Figure1a:On�ine-needleaspirationbiopsy,smearsarecellularwithpredominantlydyshesivemalignantcells.Tumor cells are plasmacytoid, eccentric nucleuswithprominent nucleoli and abundant cytoplasm. (MGG,x400)
Figure1b:Multinucleationandatypicalmitotic�igurenoted.(MGG,x400)
Page4
Vol3:Issue1:1208
OpenJClinMedCaseRep:Volume3(2017)
Figure 2a: Tumour emboli seen in multiple dilatedvessels.(H&E,x400)
Figure2b:Tumourcellsarelargesizedplasmacytoidwi th moderate to abundant cytop lasm andeccentricallyplacedlargeroundnuclei.(H&E,x100)
Figure 3a: PanCK: Immunostain shows positivecystoplasmicmembranestaining.(x400)
Figure 3b: GCDFP-15: Immunostain shows positivecytoplasmicstaining.(x100)
Figure 3c: E-cadherin: Immunostain for E-cadherinshowsabsenceofmembranousstaining.(x100)
Figure3d:Her2-neu:Immunostainshows3+positivestaining.(x400)
Page5
Vol3:Issue1:1208
OpenJClinMedCaseRep:Volume3(2017)
Table
References
1.RosenPP.Rosen'sbreastpathology.2nded.Philadelphia:LippincottWilliams&Wilkins;2001.
2.WeidnerN,Semple JP.Pleomorphicvariantof invasive lobular carcinomaof thebreast.HumPathol1992;
23:1167-71.
3. Eusebi V,Magalhaes F, Azzopardi JG. Pleomorphic lobular carcinoma of the breast: an aggressive tumour
showingapocrinedifferentiation.HumPathol1992;23:655-62.
4.MiddletonLP,PalaciosDM,BryantBR,KrebsP,OtisCN,MerinoMJ.Pleomorphiclobularcarcinoma:morphology,
immunochemistryandmolecularanalysis.AmJSurgPathol2000;24:1650-6.
5.DieciMV,OrvietoE,DominiciM,ConteP,GuarneriV.Rarebreastcancersubtypes:histological,molecular,and
clinicalpeculiarities.Oncologist.2014Aug;19(8):805-13.
6.BuchananCL,FlynnLW,MurrayMP,etal.Ispleomorphiclobularcarcinomareallyadistinctclinicalentity?JSurg
Oncol.2008;98(5):314–317.
7.EusebiV,MagalhaesF,AzzopardiJG.Pleomorphiclobularcarcinomaofthebreast:anaggressivetumorshowing
apocrinedifferentiation.HumPathol.1992;23(6):655–662.
Table1:Clinicalandhistopathologicalfeaturesofpleomorphiclobularcarcinomaofthebreastreportedsofar:
Age Sex Lateralization Size ER/PR/Her2neu
E-Cadherin Lymphnodestatus
Zahiretal(2013)
68 M Left 2.8x2.5cm +/+/+ - +
Ishidaetal(2013)
76 M Right 3x2.5cm +/-/- - -
Guptaetal(2012)
34 F Left 2x1.5cm -/-/- Notmentioned -
Manuchaetal(2011)
67 F Left Twofoci:1.1.7cm2.1.5cm
-/-/- - -
Rohinietal(2010)
55 M Left 3x2.5cm Notmentioned - -
Augustineetal(2007)(Threecases)
1.30
2.28
3.70
F
F
F
Left
Left
Left
4cm
10cm
Biopsyspecimen
Notmentioned
Notmentioned
Notmentioned
Notmentioned
Notmentioned
Notmentioned
+
+
Notassessed
Malyetal(2005)
44 M Left 2.5x2cm +/+/- - -
Presentcase
58 F Left 7x6cm -/-/+ - +
Page6
Vol3:Issue1:1208
OpenJClinMedCaseRep:Volume3(2017)
8.JacobsM,FanF,Taw�ikO.Clinicopathologicandbiomarkeranalysisofinvasivepleomorphiclobularcarcinoma
ascomparedwithinvasiveclassiclobularcarcinoma:anexperienceinourinstitutionandreviewoftheliterature.
AnnDiagnPathol.2012;16(3):185–189.
9. Weidner N, Semple JP. Pleomorphic variant of invasive lobular carcinoma of the breast. Hum Pathol.
1992;23(10):1167–1171.
10.GanganeN,Anshu,ShivkumarVB,SharmaS.Pleomorphiclobularcarcinomaofthebreast:acasereport.Acta
Cytol.2002;46(5):909–911.
11.MonhollenL,MorrisonC,AdemuyiwaFO,ChandrasekharR,KhouryT.Pleomorphic lobular carcinoma: a
distinctiveclinicalandmolecularbreastcancertype.Histopathology.2012;61(3):365–377.
12.RadhiJM.Immunohistochemicalanalysisofpleomorphiclobularcarcinoma:higherexpressionofp53and
chromograninandlowerexpressionofERandPgR.Histopathology.2000;36(2):156–160.
13.SimpsonPT,Reis-FilhoJS,LambrosMB,JonesC,SteeleD,MackayA,etal.Molecularpro�ilingpleomorphic
lobular carcinomas of the breast: evidence for a common molecular genetic pathway with classic lobular
carcinomas.JPathol.2008;215(3):231–244.
14.MoeRE, AndersonBO.Distinctive biology of pleomorphic lobular carcinoma of the breast. J SurgOncol.
2005;90(2):47–50.
15.MonacoSE,DabbsDJ,Kanbour-ShakirA.Pleomorphiclobularcarcinomainpleural�luid:diagnosticpitfallfor
atypicalmesothelialcells.DiagnCytopathol.2008;36(9):657–661.
16.ButlerD,RosaM.Pleomorphiclobularcarcinomaofthebreast:amorphologicallyandclinicallydistinctvariant
oflobularcarcinoma.ArchPatholLabMed.2013Nov;137(11):1688-92.
17.JayaramG,SwainM,ChewMT,YipCH.Cytologicappearancesininvasivelobularcarcinomaofthebreast.Acta
Cytol2000;44:169-74.
18.JoshiA,KumarN,VermaK.Diagnosticchallengeoflobularcarcinomaonaspirationcytology.DiagnCytopathol
1998;18:179-83.
19.AbdullaM,HombalS,Al-JuwaiserA,NathM,StankovichD,KanbourA.Cytomorphologicfeaturesofclassicand
variantlobularcarcinoma:acomparativestudy.DiagnCytopathol2000;22:370-5.
20.AugerM,HuttnerI.Fineneedleaspirationcytologyofpleomorphiclobularcarcinomaofthebreast.Cancer
(CancerCytopathol)1997;81:29-32.
21.CangiarellaJ,WaismanJ,CohenJM,ChhiengD,SymmansWF,GoldenbergA.Plasmacytomaofthebreast.Acta
Cytol2000;44:91-4.
22.DeChiaraA,LositoS,TerraccianoL,DiGiacomoR,IaccarinoG,RubolottaMR.Primaryplasmacytomaofthe
breast.ArchPatholLabMed2001;125:1078-80.
23.Al-BaimaniK,BazzarelliA,ClemonsM,RobertsonSJ,AddisonC,etal.InvasivePleomorphicLobularCarcinoma
oftheBreast:Pathologic,Clinical,andTherapeuticConsiderations.ClinBreastCancer2015Dec;15(6):421-5.
24.NorendraS,JenkinsSM,KhoorA,NassarA(2015) Clinicaloutcomeinpleomorphiclobularcarcinoma:acase-
controlstudywithcomparisontoclassicinvasivelobularcarcinoma.AnnDiagnPathol.2015Apr;19(2):64-9.

Page7
Vol3:Issue1:1208
OpenJClinMedCaseRep:Volume3(2017)
ManuscriptInformation:Received:November02,2016;Accepted:January09,2017;Published:January11,2017
1 1 3AuthorsInformation:KavitaMunjal ;SomaYadav *;DeepakAgarwal
1MetropolisHealthcareLtd.India2SriAurobindoInstituteofMedicalSciences,India
Citation: Munjal K, Yadav S, Agarwal D. Pleomorphic lobular carcinoma of breast – cytological characteristics and
differentials.OpenJClinMedCaseRep.2017;1208
Copy right statement: Content published in the journal follows Creative Commons Attribution License
(http://creativecommons.org/licenses/by/4.0). ©YadavS2017
Journal:Open JournalofClinical andMedicalCaseReports is an international, openaccess,peer reviewed Journal
focusingexclusivelyoncasereportscoveringallareasofclinical&medicalsciences.
Visitthejournalwebsiteatwww.jclinmedcasereports.com
Forreprints&otherinformation,contacteditorialof�[email protected]


























![[PAPER] Pleomorphic Adenoma Print.docx](https://static.cupdf.com/doc/110x72/56d6bd9b1a28ab30168ea546/paper-pleomorphic-adenoma-printdocx.jpg)

