Clinical Medical & Case Reports Open Journal of ISSN 2379-1039 Volume 3 (2017) Issue 1 Yadav S Open J Clin Med Case Rep: Volume 3 (2017) Pleomorphic lobular carcinoma of breast – cytological characteristics and differentials Kavita Munjal; Soma Yadav*; Deepak Agarwal *Soma Yadav Metropolis Healthcare Ltd. India Email: [email protected] Abstract Pleomorphic lobular carcinoma of breast (IPLC) is a very rare and distinct morphological variant of invasive lobular carcinoma (ILC), characterized by nuclear atypia and pleomorphism contrasted with the cytologic uniformity of ILC. Also it is associated with poor prognosis. Thus, cytological recognition of this tumour is important. We report a case with this unusual tumour in a ifty eight year old female that presented as a diagnostic dilemma on cytology. Introduction Pleomorphic lobular carcinoma(PLC) of breast is a distinct histological variant of invasive lobular carcinoma(ILC) [1,2,3,4,5]. Cytological recognition is important as the degree of pleomorphism exhibited in this speciic subtype may lead to misinterpretation of this particular subtype of lobular carcinoma as iniltrating ductal carcinoma. Also, it is associated with aggressive clinical course in having larger size, marked cytologic atypia, more prone to distant metastasis, higher chance of lymphovascular invasion and presentation at a higher stage [6,7,8,9,10]. The cytological literature on this entity is very little. We present a case of Pleomorphic Lobular Carcinoma diagnosed retrospectively, discuss the cytologic features that are useful in the recognition of this entity and the diagnostic pitfalls. Case Presentation A ifty eight year old female presented with a three month history of a self-discovered, progressively increasing, painless palpable lump in the left breast. She had no signiicant medical history. There was no family history of breast disease. On physical examination, a relatively ill-deined irm mass measuring 7x6 cm was palpable in the outer quadrant. The overlying skin appeared normal. There was evidence of palpable lymphadenopathy in the ipsilateral axilla. Mammography reported well-deined asymmetric density in the left breast (BIRADS-4). Fine Needle Aspiration Cytology (FNAC) was done and the smears showed scanty cellularity with occasional cells showing large nuclei. As the number of these large cells were very few and no conclusion could be drawn a repeat aspiration was performed which was highly cellular with large dyscohesive cells (Figure 1a). These cells were plasmacytoid, had coarse chromatin, inconspicuous to prominent nucleoli and variable amount of cytoplasm. Few binucleated cells were also noted. Mitotic igures were also seen (Figure 1b). The dissociated pleomorphic cell population Keywords aspiration cytology; breast carcinoma; pleomorphic lobular carcinoma

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Clinical Medical & Case Reports
Open Journal of
ISSN2379-1039
Volume3(2017)Issue1
YadavS
OpenJClinMedCaseRep:Volume3(2017)
Pleomorphiclobularcarcinomaofbreast–cytologicalcharacteristicsanddifferentialsKavitaMunjal;SomaYadav*;DeepakAgarwal
*SomaYadav
MetropolisHealthcareLtd.India
Email:[email protected]
Abstract
Pleomorphic lobularcarcinomaofbreast(IPLC) isaveryrareanddistinctmorphologicalvariantof
invasivelobularcarcinoma(ILC),characterizedbynuclearatypiaandpleomorphismcontrastedwiththe
cytologicuniformityofILC.Alsoitisassociatedwithpoorprognosis.Thus,cytologicalrecognitionofthis
tumourisimportant.Wereportacasewiththisunusualtumourina�iftyeightyearoldfemalethat
presentedasadiagnosticdilemmaoncytology.
Introduction
Pleomorphiclobularcarcinoma(PLC)ofbreastisadistincthistologicalvariantofinvasivelobular
carcinoma(ILC)[1,2,3,4,5].Cytologicalrecognitionisimportantasthedegreeofpleomorphismexhibited
inthisspeci�icsubtypemayleadtomisinterpretationofthisparticularsubtypeoflobularcarcinomaas
in�iltratingductalcarcinoma.Also,itisassociatedwithaggressiveclinicalcourseinhavinglargersize,
markedcytologicatypia,morepronetodistantmetastasis,higherchanceoflymphovascularinvasionand
presentation at ahigher stage [6,7,8,9,10].The cytological literatureon this entity is very little.We
present a case of Pleomorphic Lobular Carcinoma diagnosed retrospectively, discuss the cytologic
featuresthatareusefulintherecognitionofthisentityandthediagnosticpitfalls.
CasePresentation
A �ifty eight year old female presented with a three month history of a self-discovered,
progressivelyincreasing,painlesspalpablelumpintheleftbreast.Shehadnosigni�icantmedicalhistory.
Therewasnofamilyhistoryofbreastdisease.Onphysicalexamination,arelativelyill-de�ined�irmmass
measuring7x6cmwaspalpableintheouterquadrant.Theoverlyingskinappearednormal.Therewas
evidenceofpalpablelymphadenopathyintheipsilateralaxilla.Mammographyreportedwell-de�ined
asymmetricdensityintheleftbreast(BIRADS-4).FineNeedleAspirationCytology(FNAC)wasdoneand
thesmearsshowedscantycellularitywithoccasionalcellsshowinglargenuclei.Asthenumberofthese
largecellswereveryfewandnoconclusioncouldbedrawnarepeataspirationwasperformedwhichwas
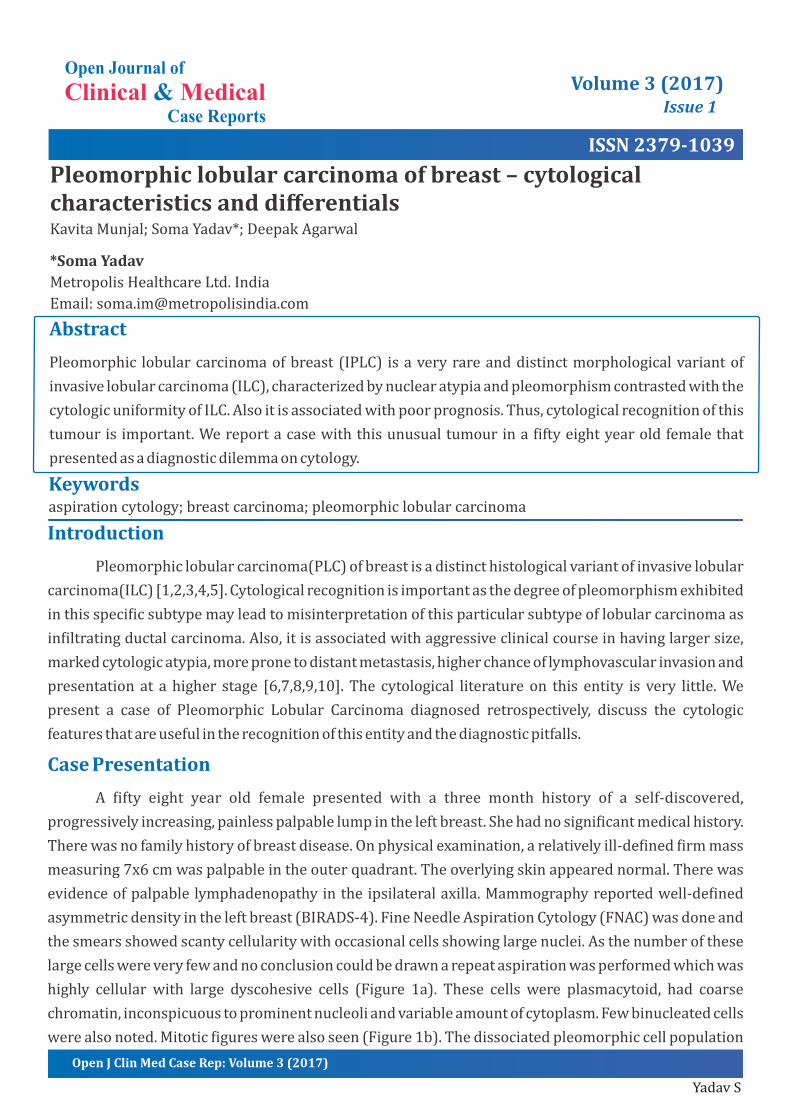
highly cellular with large dyscohesive cells (Figure 1a). These cells were plasmacytoid, had coarse
chromatin,inconspicuoustoprominentnucleoliandvariableamountofcytoplasm.Fewbinucleatedcells
werealsonoted.Mitotic�igureswerealsoseen(Figure1b).Thedissociatedpleomorphiccellpopulation
Keywordsaspirationcytology;breastcarcinoma;pleomorphiclobularcarcinoma
Page2
Vol3:Issue1:1208
OpenJClinMedCaseRep:Volume3(2017)
alongwithbinucleationandmitotic�iguresledtothediagnosisofmalignancy.Basedonthisreport,wide
excisionlumpectomywithguidedwirewasperformedasthepatientwasunwillingforaradicalexcision.
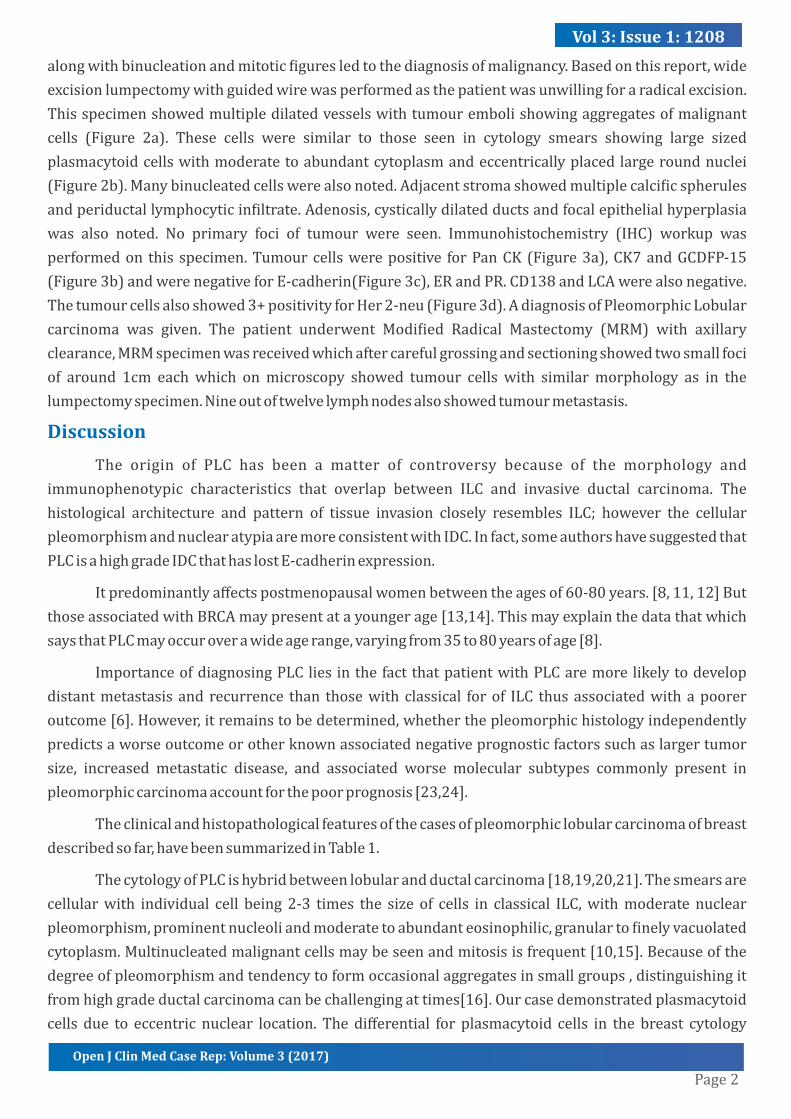
Thisspecimenshowedmultipledilatedvesselswithtumourembolishowingaggregatesofmalignant
cells (Figure 2a). These cells were similar to those seen in cytology smears showing large sized
plasmacytoidcellswithmoderatetoabundantcytoplasmandeccentricallyplacedlargeroundnuclei
(Figure2b).Manybinucleatedcellswerealsonoted.Adjacentstromashowedmultiplecalci�icspherules
andperiductallymphocyticin�iltrate.Adenosis,cysticallydilatedductsandfocalepithelialhyperplasia
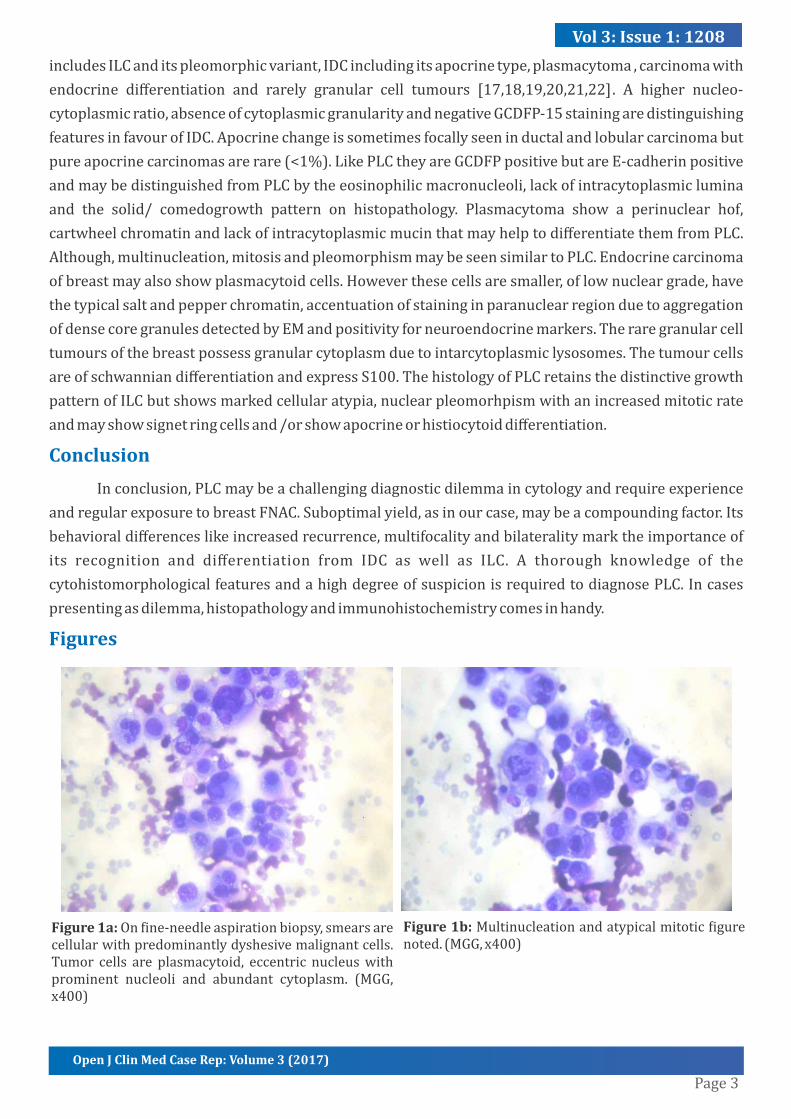
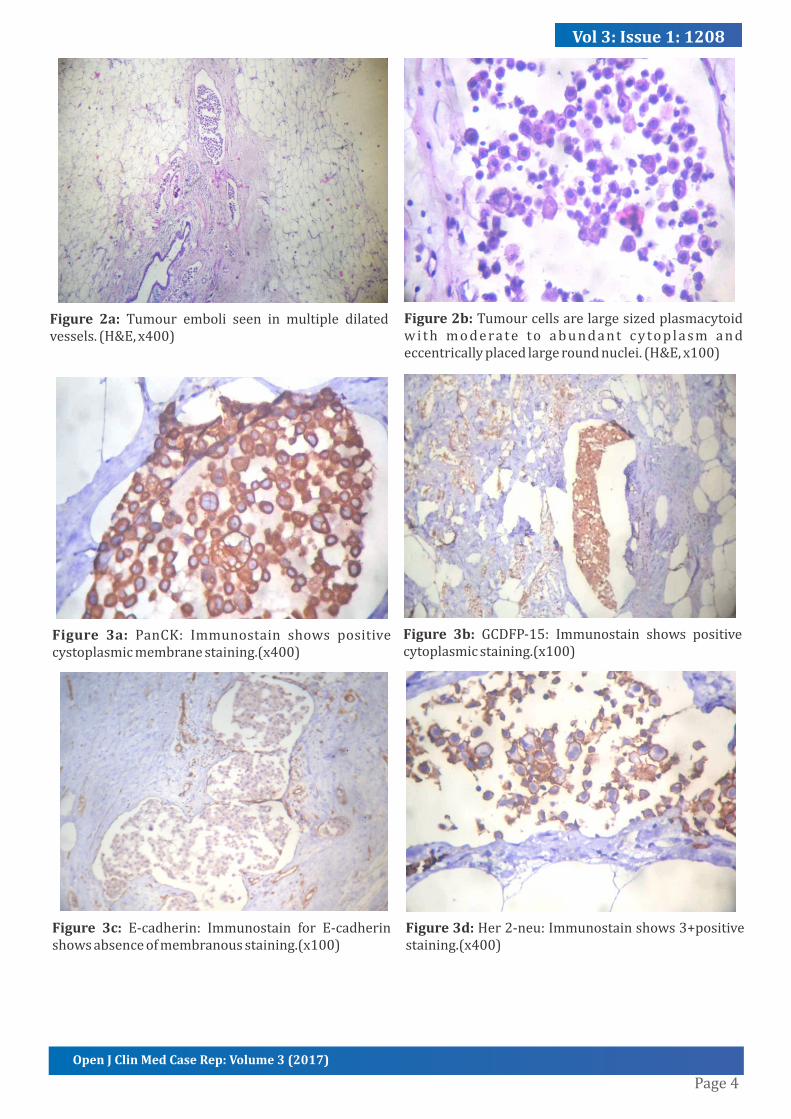
was also noted. No primary foci of tumour were seen. Immunohistochemistry (IHC) workup was
performedon this specimen.Tumourcellswerepositive forPanCK(Figure3a),CK7andGCDFP-15
(Figure3b)andwerenegativeforE-cadherin(Figure3c),ERandPR.CD138andLCAwerealsonegative.
Thetumourcellsalsoshowed3+positivityforHer2-neu(Figure3d).AdiagnosisofPleomorphicLobular
carcinoma was given. The patient underwent Modi�ied Radical Mastectomy (MRM) with axillary
clearance,MRMspecimenwasreceivedwhichaftercarefulgrossingandsectioningshowedtwosmallfoci
of around 1cm eachwhich onmicroscopy showed tumour cells with similarmorphology as in the
lumpectomyspecimen.Nineoutoftwelvelymphnodesalsoshowedtumourmetastasis.
Discussion
The origin of PLC has been a matter of controversy because of the morphology and
immunophenotypic characteristics that overlap between ILC and invasive ductal carcinoma. The
histological architecture and pattern of tissue invasion closely resembles ILC; however the cellular
pleomorphismandnuclearatypiaaremoreconsistentwithIDC.Infact,someauthorshavesuggestedthat
PLCisahighgradeIDCthathaslostE-cadherinexpression.
Itpredominantlyaffectspostmenopausalwomenbetweentheagesof60-80years.[8,11,12]But
thoseassociatedwithBRCAmaypresentatayoungerage[13,14].Thismayexplainthedatathatwhich
saysthatPLCmayoccuroverawideagerange,varyingfrom35to80yearsofage[8].
ImportanceofdiagnosingPLCliesinthefactthatpatientwithPLCaremorelikelytodevelop
distantmetastasis and recurrence than thosewith classical forof ILC thusassociatedwithapoorer
outcome[6].However,itremainstobedetermined,whetherthepleomorphichistologyindependently
predictsaworseoutcomeorotherknownassociatednegativeprognosticfactorssuchaslargertumor
size, increased metastatic disease, and associated worse molecular subtypes commonly present in
pleomorphiccarcinomaaccountforthepoorprognosis[23,24].
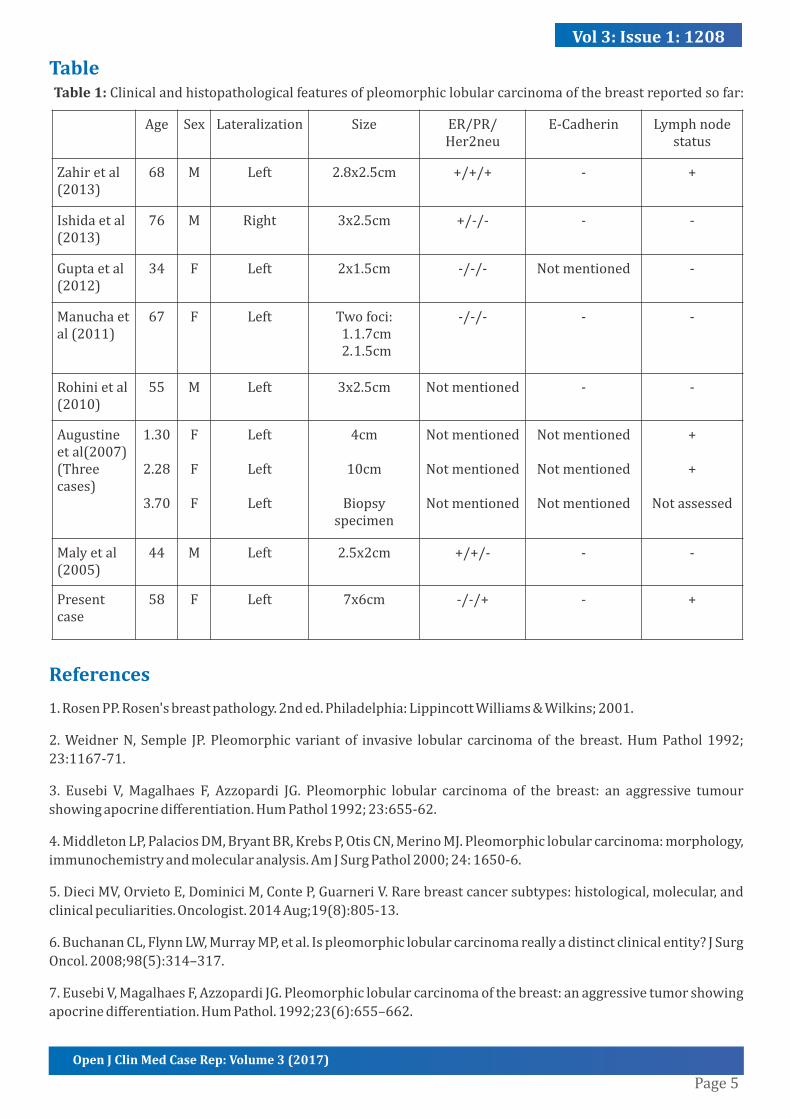
Theclinicalandhistopathologicalfeaturesofthecasesofpleomorphiclobularcarcinomaofbreast
describedsofar,havebeensummarizedinTable1.
ThecytologyofPLCishybridbetweenlobularandductalcarcinoma[18,19,20,21].Thesmearsare
cellularwith individual cell being 2-3 times the size of cells in classical ILC,withmoderate nuclear
pleomorphism,prominentnucleoliandmoderatetoabundanteosinophilic,granularto�inelyvacuolated
cytoplasm.Multinucleatedmalignantcellsmaybeseenandmitosisisfrequent[10,15].Becauseofthe
degreeofpleomorphismandtendencytoformoccasionalaggregatesinsmallgroups,distinguishingit
fromhighgradeductalcarcinomacanbechallengingattimes[16].Ourcasedemonstratedplasmacytoid
cells due to eccentric nuclear location. Thedifferential for plasmacytoid cells in the breast cytology
Page3
Vol3:Issue1:1208
OpenJClinMedCaseRep:Volume3(2017)
includesILCanditspleomorphicvariant,IDCincludingitsapocrinetype,plasmacytoma,carcinomawith
endocrine differentiation and rarely granular cell tumours [17,18,19,20,21,22]. A higher nucleo-
cytoplasmicratio,absenceofcytoplasmicgranularityandnegativeGCDFP-15stainingaredistinguishing
featuresinfavourofIDC.Apocrinechangeissometimesfocallyseeninductalandlobularcarcinomabut
pureapocrinecarcinomasarerare(<1%).LikePLCtheyareGCDFPpositivebutareE-cadherinpositive
andmaybedistinguishedfromPLCbytheeosinophilicmacronucleoli,lackofintracytoplasmiclumina
and the solid/ comedogrowth pattern on histopathology. Plasmacytoma show a perinuclear hof,
cartwheelchromatinandlackofintracytoplasmicmucinthatmayhelptodifferentiatethemfromPLC.
Although,multinucleation,mitosisandpleomorphismmaybeseensimilartoPLC.Endocrinecarcinoma
ofbreastmayalsoshowplasmacytoidcells.Howeverthesecellsaresmaller,oflownucleargrade,have
thetypicalsaltandpepperchromatin,accentuationofstaininginparanuclearregionduetoaggregation
ofdensecoregranulesdetectedbyEMandpositivityforneuroendocrinemarkers.Theraregranularcell
tumoursofthebreastpossessgranularcytoplasmduetointarcytoplasmiclysosomes.Thetumourcells
areofschwanniandifferentiationandexpressS100.ThehistologyofPLCretainsthedistinctivegrowth
patternofILCbutshowsmarkedcellularatypia,nuclearpleomorhpismwithanincreasedmitoticrate
andmayshowsignetringcellsand/orshowapocrineorhistiocytoiddifferentiation.
Conclusion
Inconclusion,PLCmaybeachallengingdiagnosticdilemmaincytologyandrequireexperience
andregularexposuretobreastFNAC.Suboptimalyield,asinourcase,maybeacompoundingfactor.Its
behavioraldifferenceslikeincreasedrecurrence,multifocalityandbilateralitymarktheimportanceof
its recognition and differentiation from IDC as well as ILC. A thorough knowledge of the
cytohistomorphologicalfeaturesandahighdegreeofsuspicionisrequiredtodiagnosePLC.Incases
presentingasdilemma,histopathologyandimmunohistochemistrycomesinhandy.
Figures
Figure1a:On�ine-needleaspirationbiopsy,smearsarecellularwithpredominantlydyshesivemalignantcells.Tumor cells are plasmacytoid, eccentric nucleuswithprominent nucleoli and abundant cytoplasm. (MGG,x400)
Figure1b:Multinucleationandatypicalmitotic�igurenoted.(MGG,x400)
Page4
Vol3:Issue1:1208
OpenJClinMedCaseRep:Volume3(2017)
Figure 2a: Tumour emboli seen in multiple dilatedvessels.(H&E,x400)
Figure2b:Tumourcellsarelargesizedplasmacytoidwi th moderate to abundant cytop lasm andeccentricallyplacedlargeroundnuclei.(H&E,x100)
Figure 3a: PanCK: Immunostain shows positivecystoplasmicmembranestaining.(x400)
Figure 3b: GCDFP-15: Immunostain shows positivecytoplasmicstaining.(x100)
Figure 3c: E-cadherin: Immunostain for E-cadherinshowsabsenceofmembranousstaining.(x100)
Figure3d:Her2-neu:Immunostainshows3+positivestaining.(x400)
Page5
Vol3:Issue1:1208
OpenJClinMedCaseRep:Volume3(2017)
Table
References
1.RosenPP.Rosen'sbreastpathology.2nded.Philadelphia:LippincottWilliams&Wilkins;2001.
2.WeidnerN,Semple JP.Pleomorphicvariantof invasive lobular carcinomaof thebreast.HumPathol1992;
23:1167-71.
3. Eusebi V,Magalhaes F, Azzopardi JG. Pleomorphic lobular carcinoma of the breast: an aggressive tumour
showingapocrinedifferentiation.HumPathol1992;23:655-62.
4.MiddletonLP,PalaciosDM,BryantBR,KrebsP,OtisCN,MerinoMJ.Pleomorphiclobularcarcinoma:morphology,
immunochemistryandmolecularanalysis.AmJSurgPathol2000;24:1650-6.
5.DieciMV,OrvietoE,DominiciM,ConteP,GuarneriV.Rarebreastcancersubtypes:histological,molecular,and
clinicalpeculiarities.Oncologist.2014Aug;19(8):805-13.
6.BuchananCL,FlynnLW,MurrayMP,etal.Ispleomorphiclobularcarcinomareallyadistinctclinicalentity?JSurg
Oncol.2008;98(5):314–317.
7.EusebiV,MagalhaesF,AzzopardiJG.Pleomorphiclobularcarcinomaofthebreast:anaggressivetumorshowing
apocrinedifferentiation.HumPathol.1992;23(6):655–662.
Table1:Clinicalandhistopathologicalfeaturesofpleomorphiclobularcarcinomaofthebreastreportedsofar:
Age Sex Lateralization Size ER/PR/Her2neu
E-Cadherin Lymphnodestatus
Zahiretal(2013)
68 M Left 2.8x2.5cm +/+/+ - +
Ishidaetal(2013)
76 M Right 3x2.5cm +/-/- - -
Guptaetal(2012)
34 F Left 2x1.5cm -/-/- Notmentioned -
Manuchaetal(2011)
67 F Left Twofoci:1.1.7cm2.1.5cm
-/-/- - -
Rohinietal(2010)
55 M Left 3x2.5cm Notmentioned - -
Augustineetal(2007)(Threecases)
1.30
2.28
3.70
F
F
F
Left
Left
Left
4cm
10cm
Biopsyspecimen
Notmentioned
Notmentioned
Notmentioned
Notmentioned
Notmentioned
Notmentioned
+
+
Notassessed
Malyetal(2005)
44 M Left 2.5x2cm +/+/- - -
Presentcase
58 F Left 7x6cm -/-/+ - +
Page6
Vol3:Issue1:1208
OpenJClinMedCaseRep:Volume3(2017)
8.JacobsM,FanF,Taw�ikO.Clinicopathologicandbiomarkeranalysisofinvasivepleomorphiclobularcarcinoma
ascomparedwithinvasiveclassiclobularcarcinoma:anexperienceinourinstitutionandreviewoftheliterature.
AnnDiagnPathol.2012;16(3):185–189.
9. Weidner N, Semple JP. Pleomorphic variant of invasive lobular carcinoma of the breast. Hum Pathol.
1992;23(10):1167–1171.
10.GanganeN,Anshu,ShivkumarVB,SharmaS.Pleomorphiclobularcarcinomaofthebreast:acasereport.Acta
Cytol.2002;46(5):909–911.
11.MonhollenL,MorrisonC,AdemuyiwaFO,ChandrasekharR,KhouryT.Pleomorphic lobular carcinoma: a
distinctiveclinicalandmolecularbreastcancertype.Histopathology.2012;61(3):365–377.
12.RadhiJM.Immunohistochemicalanalysisofpleomorphiclobularcarcinoma:higherexpressionofp53and
chromograninandlowerexpressionofERandPgR.Histopathology.2000;36(2):156–160.
13.SimpsonPT,Reis-FilhoJS,LambrosMB,JonesC,SteeleD,MackayA,etal.Molecularpro�ilingpleomorphic
lobular carcinomas of the breast: evidence for a common molecular genetic pathway with classic lobular
carcinomas.JPathol.2008;215(3):231–244.
14.MoeRE, AndersonBO.Distinctive biology of pleomorphic lobular carcinoma of the breast. J SurgOncol.
2005;90(2):47–50.
15.MonacoSE,DabbsDJ,Kanbour-ShakirA.Pleomorphiclobularcarcinomainpleural�luid:diagnosticpitfallfor
atypicalmesothelialcells.DiagnCytopathol.2008;36(9):657–661.
16.ButlerD,RosaM.Pleomorphiclobularcarcinomaofthebreast:amorphologicallyandclinicallydistinctvariant
oflobularcarcinoma.ArchPatholLabMed.2013Nov;137(11):1688-92.
17.JayaramG,SwainM,ChewMT,YipCH.Cytologicappearancesininvasivelobularcarcinomaofthebreast.Acta
Cytol2000;44:169-74.
18.JoshiA,KumarN,VermaK.Diagnosticchallengeoflobularcarcinomaonaspirationcytology.DiagnCytopathol
1998;18:179-83.
19.AbdullaM,HombalS,Al-JuwaiserA,NathM,StankovichD,KanbourA.Cytomorphologicfeaturesofclassicand
variantlobularcarcinoma:acomparativestudy.DiagnCytopathol2000;22:370-5.
20.AugerM,HuttnerI.Fineneedleaspirationcytologyofpleomorphiclobularcarcinomaofthebreast.Cancer
(CancerCytopathol)1997;81:29-32.
21.CangiarellaJ,WaismanJ,CohenJM,ChhiengD,SymmansWF,GoldenbergA.Plasmacytomaofthebreast.Acta
Cytol2000;44:91-4.
22.DeChiaraA,LositoS,TerraccianoL,DiGiacomoR,IaccarinoG,RubolottaMR.Primaryplasmacytomaofthe
breast.ArchPatholLabMed2001;125:1078-80.
23.Al-BaimaniK,BazzarelliA,ClemonsM,RobertsonSJ,AddisonC,etal.InvasivePleomorphicLobularCarcinoma
oftheBreast:Pathologic,Clinical,andTherapeuticConsiderations.ClinBreastCancer2015Dec;15(6):421-5.
24.NorendraS,JenkinsSM,KhoorA,NassarA(2015) Clinicaloutcomeinpleomorphiclobularcarcinoma:acase-
controlstudywithcomparisontoclassicinvasivelobularcarcinoma.AnnDiagnPathol.2015Apr;19(2):64-9.

Page7
Vol3:Issue1:1208
OpenJClinMedCaseRep:Volume3(2017)
ManuscriptInformation:Received:November02,2016;Accepted:January09,2017;Published:January11,2017
1 1 3AuthorsInformation:KavitaMunjal ;SomaYadav *;DeepakAgarwal
1MetropolisHealthcareLtd.India2SriAurobindoInstituteofMedicalSciences,India
Citation: Munjal K, Yadav S, Agarwal D. Pleomorphic lobular carcinoma of breast – cytological characteristics and
differentials.OpenJClinMedCaseRep.2017;1208
Copy right statement: Content published in the journal follows Creative Commons Attribution License
(http://creativecommons.org/licenses/by/4.0). ©YadavS2017
Journal:Open JournalofClinical andMedicalCaseReports is an international, openaccess,peer reviewed Journal
focusingexclusivelyoncasereportscoveringallareasofclinical&medicalsciences.
Visitthejournalwebsiteatwww.jclinmedcasereports.com
Forreprints&otherinformation,contacteditorialof�[email protected]
Related Documents











