Growth in Body Fat and Adipose Tissue&
Adipose Tissue Metabolism

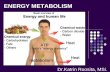
DENSITOMETRY
BODY DENSITY = MASS / VOLUME gm/ml
Underwater WeighingVolumetryHelium DilutionBODPOD (plethysmography)
Any method that determines body density

Predicting % Fat from Density
ASSUMPTIONS
Body can be divided into two components:
Fat & Non-Fat Masses
Each has different, known and constant densities

SIRI EQUATION
FAT MASS 0.9 gm/ml
Good Assumption
NON-FAT MASS 1.1 gm/ml
Poor Assumption
% Fat = (4.95/Density)-4.5) x 100

-40
-20
0
20
40
60
80
100
0.9 0.95 1 1.05 1.1 1.15 1.2
Density (gm/ml)
% F
AT
Siri Equation
95% confidence interval for prediction of percentage body fat
±7.5% Body Fat

TOTAL BODY WATER (isotope dilution)
Determined by introducing a marker fluid that moves freely in body water and is not metabolized.
Markers– Deuterium Oxide, tritiated water
Total Body water volume can be determined accurately To predict % Body Fat
– Assume constant fraction of Water in Fat Free Mass (72.3%, 73.2%, 73.8% or ……….) which is far from constant
– Introduces same error in prediction as seen for densitometry

Chemical Maturity
%H20 in FFM
FFM Density
Age Males Females Males Females
Birth 80.6 80.6 1.063 1.064
1 79 78.8 1.068 1.069
5 76.6 77.6 1.078 1.072
9 - 11 76.2 77 1.084 10.82
13 - 15 74.7 75.5 1.094 1.092
17 - 20 74 74.8 1.099 1.095

Adipose Tissue White adipocytes
– a scant ring of cytoplasm surrounding a single large lipid droplet. – nuclei are flattened and eccentric within the cell.– 25-150 micrometers– major role in glucose, fatty acid, lipoprotein & cholesterol metabolism– internal & subcutaneous deposition
Brown adipocytes – polygonal in shape, have a considerable volume of cytoplasm– contain multiple lipid droplets of varying size.– nuclei are round and almost centrally located. – 15 - 25 micrometers– thermogenesis
Brown White

Brown Adipose Tissue
Brown adipose tissue is most prominent in newborn animals. In human infants it comprises up to 5% of body weight, then diminishes with age to virtually disappear by adulthood.
In contrast to other cells, including white adipocytes, brown adipocytes express mitochondrial uncoupling protein, which gives the cell's mitochondria an ability to uncouple oxidative phosphorylation and utilize substrates to generate heat rather
than ATP.

Development of White Adipose Tissue
14th – 16th fetal week fat lobules form Gradient: head – trunk - limbs adipocyte lineage derives from an embryonic
stem cell precursor with the capacity to differentiate into the mesodermal cell types of adipocytes, chondrocytes, osteoblasts, and myocytes – (mesenchyme)

Growth and development of human adipose tissue during early gestation - Poissonnet, Burdi and Bookstein (1983)
Low-power photomicrograph of a frontal section of the face of a 28 week-old fetus Buccal fat pad in the left cheek region (arrow) .

Stages in the development of adipose tissue in the human buccal fat pad
Stage 1: At 14 weeks cheek is filled with loose connective tissue, composed chiefly of stellate cells and ground substance.
Stage 2: Vascular invasion or angiogenesis. By 14.5 weeks, blood vessels proliferate and signal areas where early fat cells will organize in groups.
Stage 3: By 19 weeks, development of mesenchymal lobules that contain stellate mesenchymal cells or pre-adipocytes without lipid droplets.
Stage 4: At 22 weeks appearance of primitive fat lobules. Fat storage is visible around the 16th week. The vascular stalk of each of these primitive fat lobules branches from one main vessel to enclose the densely packed fat cells
Stage 5: At 28 weeks the fat lobules are well separated from each other by connective tissue partitions or septa.

Adipose Tissue Development
Stage 1: Prior to the fourteenth prenatal week, future fat consists of loose connective tissue composed of an amorphous ground substance and fibres
Stage 1

Stage 2: The first indication of adipogenesis is the aggregation of a dense mass of mesenchymal cells.
Adipose Tissue Development
Condensation of mesenchyme, which marks the end of the undifferentiated stage is asssociated with the proliferation of primitive vessels and indicates the emergence ofcharacteristic fat tissue
Stage 2

Stage 3: a rich capillary network develops, around which mesenchymal cells differentiate into stellate preadipocytes.
Adipose Tissue Development
These mesenchymal lobules, which do not contain lipid droplets at this stage, are organized within a vascular structure or glomerulus, and will ultimately form a definitive fat lobule
Stage 3

Stage 4: Within the mesenchymal lobules, fine fat vacuoles form in the cytoplasm and increase in number.
At this time, the primitive fat lobule includes– the vascular network or glomerulus, and – densely-packed vacuolated fat cells adjacent to small vessels
Adipose Tissue Development
Stage 4

Stage 5: In the final stage, definitive fat lobules are surrounded by perilobular mesenchyme. This condenses rapidly, and progressively thickens to form interlobular septa
Adipose Tissue Development
Stage 5

Adipocyte Size
Regional variation in size

Adipocyte Number

Critical Periods
Periods when overfeeding can cause increase in fat cell number
1st year of life Early childhood growth spurt Prepubescent fattening

Skinfold to Fat Mass Ratio
Meaning of a skinfold




Secondary Sexual Adipose Tissue
Females– Upper arms & shoulders– Hips, thighs, medial calf– preferentially mobilized during
pregnancyMales similar intercorrelations


Adipose Tissue Volume
Females– Skinfold
curve similar to ATV

Adipose Tissue Volume
Males– Limb skinfold
curve responds to muscle growth spurt

Adipocyte Metabolism Triglycerides stored as
fat droplet Lipoproteinlipase acts
on Chylomicrons and Very Low Density Lipoproteins to form Free Fatty Acids which pass into cell
Lipogenesis from blood glucose is minor, although elevated in high carbohydrate diet or insulin
FFA also found bound to albumin in blood stream
In cell, triglyceride formed for storage

Leptin
1953, Kennedy proposed body energy stores were regulated by fat-derived, lipostatic, negative feedback signal acting centrally to inhibit feeding
1994, Leptin was identified– Although focused upon as a satiety signal it has more responsibility for
modulation and regulation of multiple systems.– Secreted by adipose tissue (also stomach, placenta, muscle).– Positive correlation between %body fat and circulating levels of Leptin.– However, manipulation of Leptin levels has only transient effects on food
intake.– Regulation of receptor expression may be important determinants of
Leptin sensitivity.– Primary functions maybe unrelated to satiety
Insulin Stress response Reproductive function Growth Factor

Leptin & Insulin
Majority of reports demonstrate inhibition of insulin secretion by Leptin, although this may be secondary to the metabolic state of the Islets of Langerhans (Pancreas).
Insulin does not have a direct effect on leptin expression and secretion. Hyperinsulinemia promotes fat deposition, which subsequently increases leptin expression.
Leptin – Insulin relationship is clouded by variability in sensitivities controlled by multiple other factors.

Leptin & Reproductive Function Leptin provides a link between fat and the
hypothalamic/pituitary/gonadal axis. Leptin stimulates hypothalamic gonadotrophic-releasing
hormone and pituitary gonadotrophins Plasma Leptin is higher in women than men for any % body fat In children and adults, Leptin is negatively associated with
testosterone in males and positively correlated with estrogen in females, after accounting for fat mass.
In women, Leptin fluctuations during the menstrual cycle correlate with estrogen, but not progesterone.
However, Leptin levels similar in pre- and postmenopausal women
Testosterone reported to inhibit or have no effect on leptin release.

Leptin & Sexual Maturation
Early puberty in obese children Leptin triples during puberty in normal girls In boys there is a prepubertal surge in Leptin,
which declines at the onset of puberty At the end of puberty, Leptin negatively correlated
with FSH and LH in girls, but no relationship in boys
Probable gender differences in hormone sensitivity Adequate Leptin levels probably necessary for
normal sexual maturation

Gonadal Steroids
Adipose tissue has estrogen, androgen and progesterone receptors– Androgen receptors more dense in visceral than
subcutaneous adipose tissue in both sexes– Estrogen binding capacity of visceral tissue lower than
subcutaneous in males but not females– Progesterone receptor concentrations higher in
subcutaneous (gluteal) than visceral adipose tissue Gonadal steroids largely account for the larger adipose
tissue mass in females

Gonadal Steroids
Androgen/Estrogen balance determines fat patterning– Genetic males with testicular feminization– Women given exogenous androgens or suffering
from virilizing tumours– Menopause– Smoking– Progesterone and Estrogen act synergistically– Fat patterning in pregnancy