ENDOTRACHEAL INTUBATION
PRESENTED BY : R.PRASANTH MSC(N) 2ND YEAR

DEFINITION
It is a procedure of passing of an endotracheal tube into trachea through the nose or mouth.

PURPOSE
It is performed to establish and maintain a patent airway, facilitate oxygenation and ventilation, reduce the risk of aspiration, and assist with the clearance of secretions.

INDICATIONSAND
CONTRAINDICATIONS

ADVANTAGES

DISADVANTAGES
Need advanced training to properly perform procedure
Bypasses the nares function of warming and filtering the air
Increased incidence of trauma due to neck manipulation when spinal cord injury is suspected
May increase respiratory resistance
Improper placement

EQUIPMENTS

LARYNGOSCOPE : handle & blade

Macintosh (curved) and Miller (straight) blade
Adult : Macintosh blade
small children : Miller blade
LARYNGOSCOPIC BLADE:
Mc coy blade Miller blade
Macintosh blade

ENDOTRACHEAL TUBE

TYPES OF ETTs:1) Portex tubes:
Semirigid, with little tendency to kink. Most commonly used.
2) Rubber tubes:
Soft, easily kinked.
3) Reinforced tubes:
- Cuffed or non cuffed. Reinforced with wire to prevent kinking.
4) Special tubes:
Double lumen (Robertshaw

ENDOTRACHEAL TUBE: (ETT)
Male : ID 8.0 mms
Female : ID 7.5 mms
New born - 3 mths : ID 3.0 mms
3-9 months : ID 3.5 mms
9-18 months : ID 4.0 mms
2- 6 yrs : ID = (Age/3) + 3.5
> 6 yrs : ID = (Age/4) + 4.5
1) Size of ETT : internal diameter (ID)

2) MATERIAL : Red rubber or PVC
3) ETT CUFF
High volume Low pressure cuff
Low volume High pressure cuff

ETT CUFF• cuff inflating system consisting of:
• valve, balloon, inflating tube & cuff.
• Uncuffed tubes used in children to minimise pressure injury
• Purpose of cuff is:
• seal between tube & trachea
• Protect from aspiration of blood, mucus or vomitus.

4) BEVEL5) MURPHY’S EYE

6) Depth of insertion:
Midtrachea or below vocal cord~2 cm
Adult Male ~23 cmFemale ~21 cm
ChildrenOral ETT = (Age/2) + 12 (cm)Nasal ETT = (Age/2) + 15 (cm)

OTHER EQUIPMENTS:
STYLET(malleabl
e)

FACE MASK & SELF INFLATING BAG
MAGILL FORCEPS

LOCAL ANAESTHETIC SPRAY

Syringe
Lubricating jelly
Dynaplast/ tape to strap endotracheal tube
Monitoring success of intubation:
Stethoscope
Endtidal - CO2
Pulse oximeter

PREOXYGENATION
PROCEDURE
• ventilate with 100 % oxygen for approximately 3 min
• Position bed / table height:bring the patient's head to naval height

SNIFFING POSITIONExtension at atlanto-occipital joint
Flexion at lower cervical spine
Neck flexion is maintained by placing a few
inches of padding behind the head

Sniffing position

STEPS OF OROENDOTRACHEAL
INTUBATION

BAG MASK VENTILATION
•Thumb and index finger of left hand in the shape of a “C” press down
•The other 3 fingers at the inferior ramus of the mandible and lift the mandible up (jaw thrust) “E”
C
E

HOLDING A LARYNGOSCOPE
Hold the handle ofthe laryngoscope with your left hand

OPEN MOUTH TECHNIQUES
Hyper-extension technique (no touch technique) Cross fingers techniques

INTUBATION TECHNIQUE
introduce the blade into the right side of the patient's mouth
move the blade posteriorly and toward the midline, sweeping the tongue to the left and keeping it away from the visual path with the flange of the blade
ensure the lower lip is not being pinched by the lower incisors and laryngoscope blade
advance the laryngoscope until the epiglottis is in view

INSERTING THE BLADE

INTUBATION TECHNIQUE
lift the laryngoscope upward and forward
insert the ETT from the right angle of mouth with its concave curve facing downward and to the right side of the patient
maneuver the endotracheal tube into the larynx, midway between the cricoid cartilage and the sternal angle

LIFTING UP A LARYNGOSCOPE:
• Pull the blade forward and upward using firm but Steady pressure without rotating the wrist
• Avoid leaning on the upper teeth with the blade

EXPOSURE OF THE LARYNX:
•In most situations vocal cords should become visible • If not, exert gentle pressure over the cricoid area to help bring them into view

BURP Maneuver:
ON THYROID CARTILAGE
•Backward:• against the cervical Vertebrae
•Upward
•Right: lateral pressure to the right

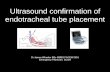
HOW TO CONFIRM THE CORRECT PLACEMENT OF ETT?
Primary Confirmation
Secondary Confirmation

PRIMARY CONFIRMATION :By Physical Exam
Confirm tube placement immediately
Listen over the epigastrium and observe the chest wall for movement
If stomach gurgling and no chest wall expansion –
esophagus intubated: deflate the cuff and remove ET tube
Reattempt intubation after re -oxygenation

PRIMARY CONFIRMATION: CONTD.
If chest wall rises and stomach not gurgling,
perform 5-point auscultation
If still doubt, use laryngoscope to see the tube passing through the vocal cords (best)
Secure the tube
Look for moisture condensation on the inside of the tracheal tube
(not 100%: false +ve with esophageal intubations)

SECONDARY CONFIRMATION
End-Tidal CO2 Detectors
Commercial device that reacts with a color change to CO2 exhaled from the lungs:
Qualitative detection device indicates exhaled CO2 indicates proper tracheal tube placement
Absence of CO2 (unless prolonged CPR), indicates esophageal intubation
False +ve: Distended stomach, carbonated beverages
False - ve: Low or no blood flow states

Endotracheal tube(ET) trachea, endotracheal tube (arrows) and
location of carina (^).

AFTER CARE OF THE PATIENT

PROCEDURE FOR REMOVAL

THANK YOU