Ultrasound confirmation of endotracheal tube placement Dr James Wheeler BSc MBBS FACEM DDU Emergency Physician, SCGH

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
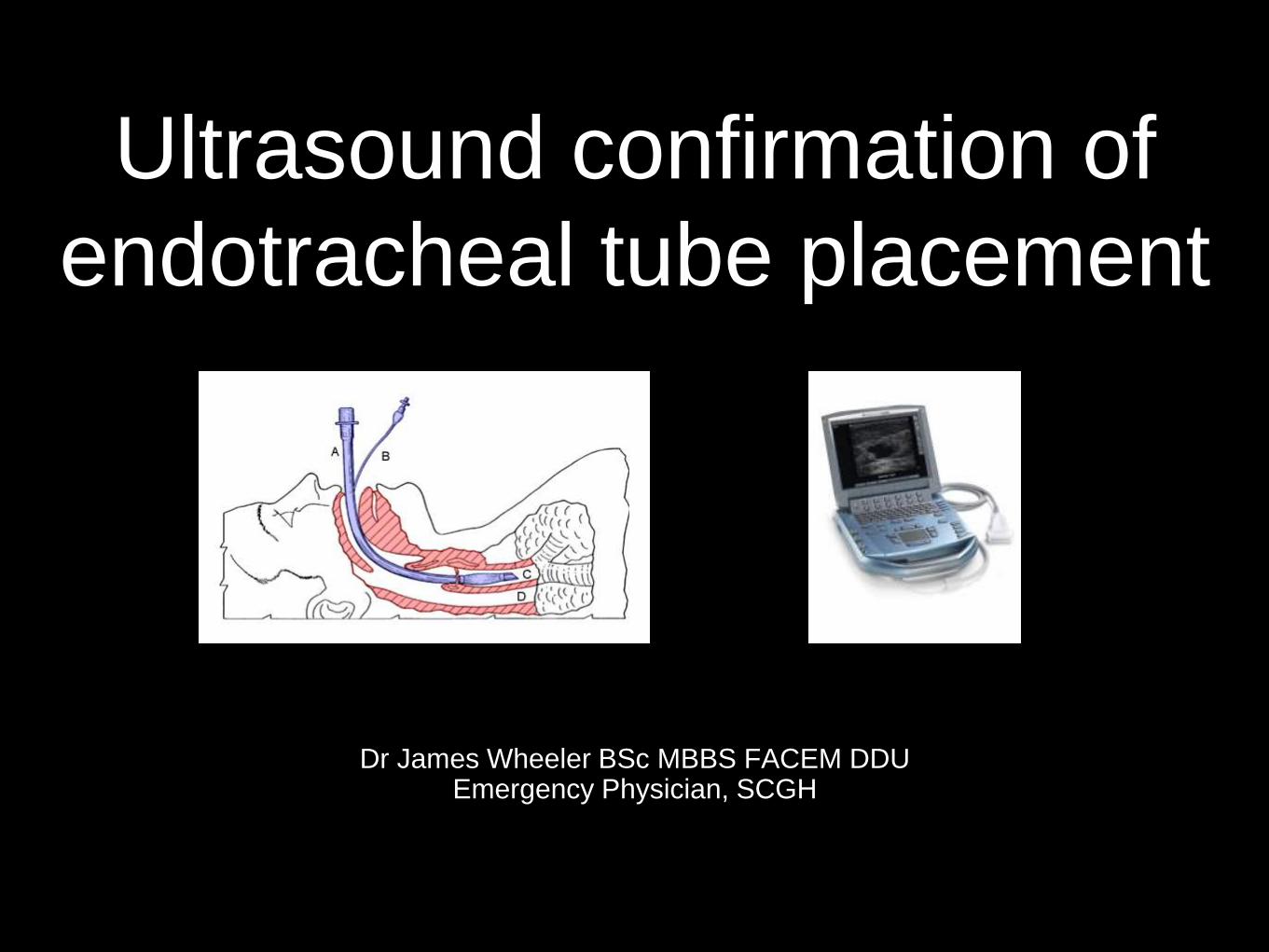
Ultrasound confirmation of
endotracheal tube placement
Dr James Wheeler BSc MBBS FACEM DDUEmergency Physician, SCGH
Will this replace traditional
methods of ETT confirmation?
• Specifically, does this replace capnography and
auscultation
• NO!
• But no single confirmatory method is entirely reliable in
emergency situations, and in certain circumstance US
confirmation can be a very helpful adjunct

Why would you do it?
• Transtracheal ultrasound is a relatively SIMPLE technique
• FAST (~8 sec vs 18 sec for capnography1)
• May be more reliable than capnography changes in certain patient groups?
• SENSITIVE and SPECIFIC 2,3,4
• The pooled sensitivity and specificity for the detection of proper ETT placement
with US were:
• Sensitivity: 98% (95% C.I. 97-99%); Specificity: 98% (95% C.I. 95-99%);
PPV: 99.5%, NPV: 93.8%
• Does not require ventilations to assess tube placement
• May prevent gastric insufflation and delay in diagnosis of misplacement

When would you use it?
• ETCO2 unreliable or not available
• Cardiac arrest / massive PE
• Emergency blind intubation
• Patient arrives intubated and requires rapid confirmation of
ETT placement
• Any patient not responding as expected after ETT
placement prior to attempting re-intubation
How do you do it?
Direct (Transtracheal)
• Looking for evidence of direct endotracheal intubation or oesophageal intubation (a “second trachea”)
• During intubation OR Post-intubation
Indirect (Transthoracic)
• Looking at the pleural space for evidence of lung ventilation (pleural movement)
• Post-intubation

Direct: Technique
Probe:
• high frequency (6-12MHz) linear probe (but
can use lower freq micro convex or
curvilinear in obese)
Preset:
• Superficial, depth sufficient to see posterior
to trachea, focal zone at trachea
Probe placement:
• in transverse plane just above the
suprasternal notch
• i.e. beneath cricoid

Direct: Technique
Endotracheal intubation:
• One air-mucosal interface
• Hyperechoic reverberation artifacts inside trachea
OR
Oesophageal intubation:
• Dynamic opening of the oesophagus by the ETT seen on US performed during laryngoscopy
• Two air-mucosal interfaces (“two tracheas” , “double track sign”)
• Hyperechoic reverberation artifacts inside oesophagus
May also interrogate cuff position by infiltrating saline
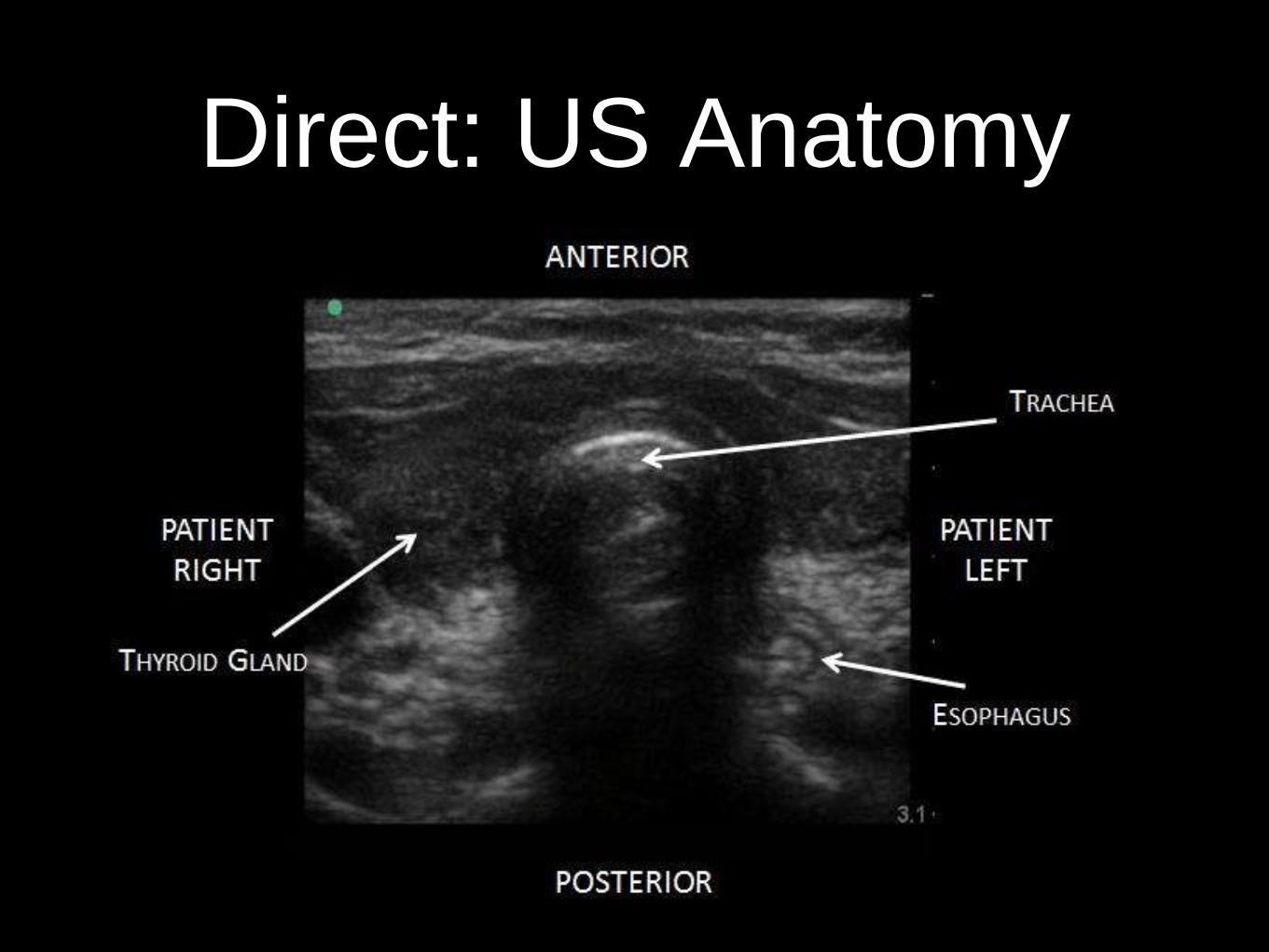
Direct: US Anatomy
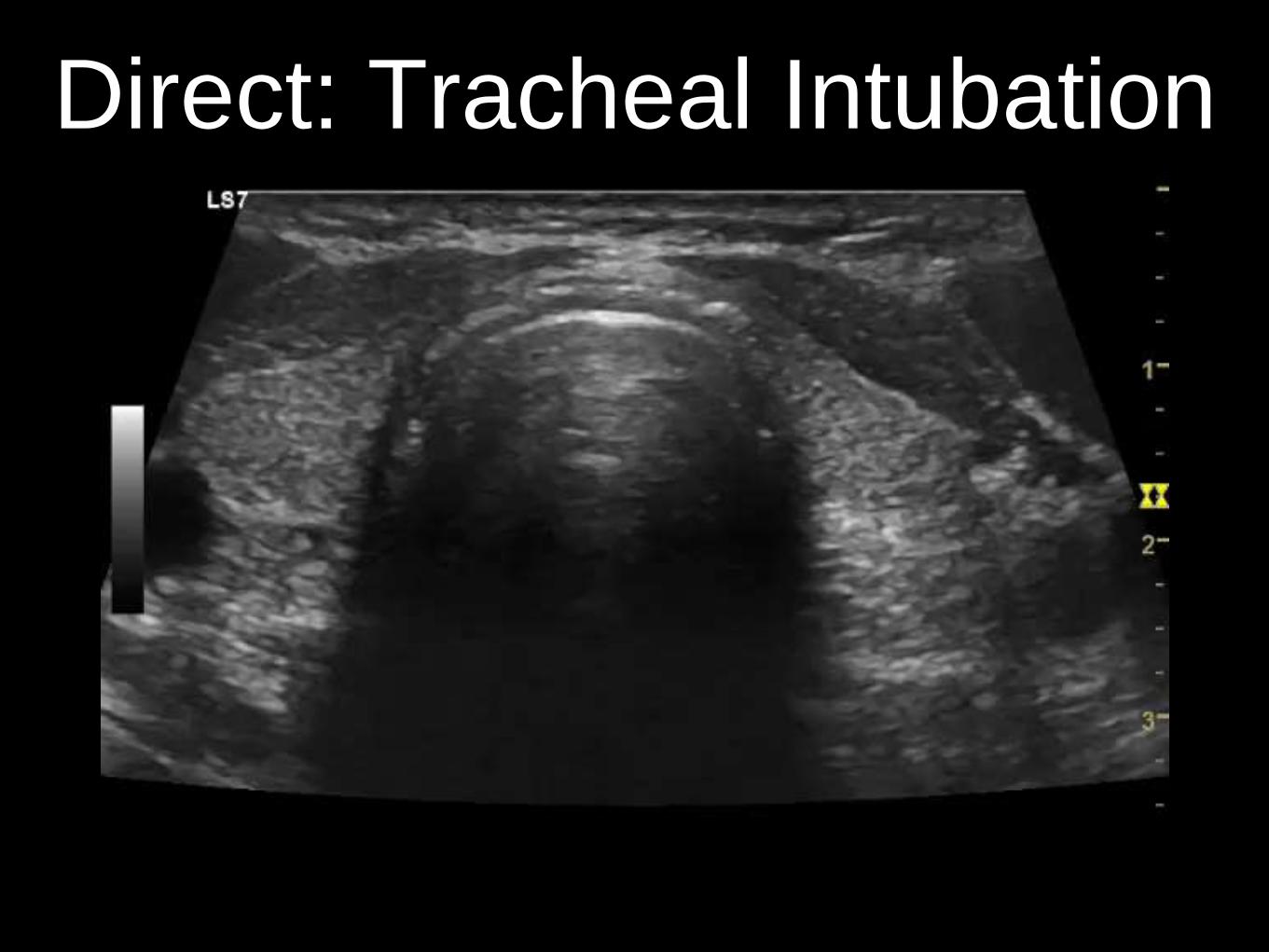
Direct: Tracheal Intubation



Direct - Oesophageal Intubation






Indirect
• Looking at the pleural space for evidence of lung
ventilation (pleural movement)
• Differential pleural movement may indicate RMS
intubation
• Requires ventilation

Indirect US Anatomy

Indirect: Ventilating Lung

Indirect: Non-Ventilating Lung

Indirect: Pneumothorax
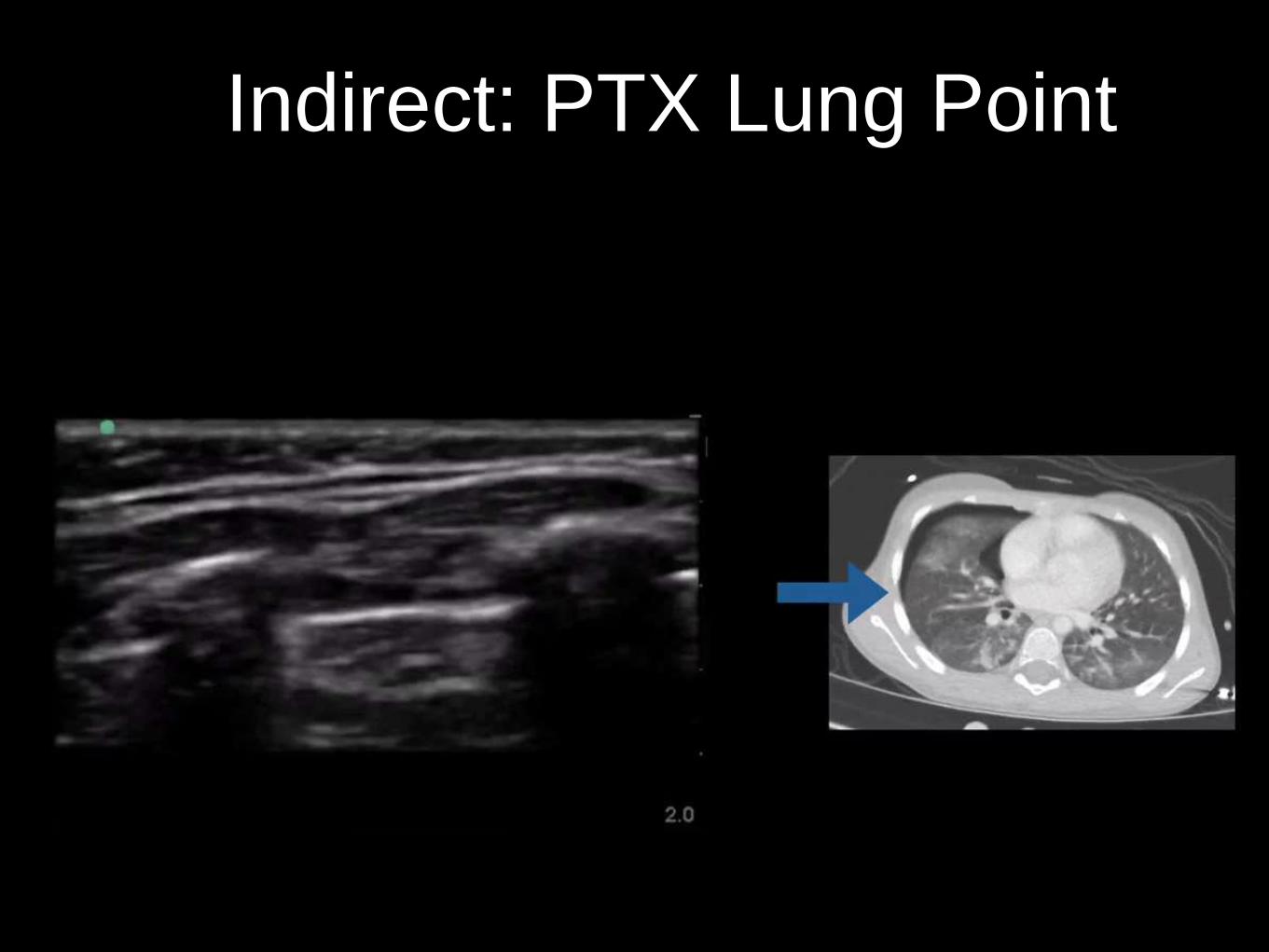
Indirect: PTX Lung Point

Pitfalls?
• Requires access to US machine
• No single confirmatory method is entirely reliable (esp. in
emergency situations)
• Operator dependent
• Surgical emphysema can obscure view
• Can’t identify supraglottic airway
• Pneumothorax (for indirect)

References
1. Reliability of Ultrasonography in Confirming Endotracheal Tube
Placement in an Emergency Setting. Vimal Koshy, Thomas et al.
Indian J Crit Care Med. 2017 May; 21(5): 257–261.
2. Transtracheal ultrasound for verification of endotracheal tube
placement: a systematic review and meta-analysis. Das SK1, Choupoo
NS, Haldar R, Lahkar A. Can J Anaesth. 2015 Apr;62(4):413-23
3. Ultrasonography for confirmation of endotracheal tube placement: A
systematic review and meta-analysis. Eric H.Chou et al. Resuscitation,
Volume 90, May 2015, 97-103
4. Can Transtracheal Ultrasonography Be Used to Verify Endotracheal
Tube Placement? Gottlieb M, Bailitz J .Ann Emerg Med. 2015 Oct;
66(4): 394-5
Related Documents