Drugs Pharmacology in Heart Disease
By
M.H.Farjoo M.D. , Ph.D.Shahid Beheshti University of Medical Science

M.H.FarjooM.H.Farjoo
Drugs Pharmacology in Heart Disease
Principles of Drug Therapy Variability in Drug Effect Dosage Optimization Drug Therapy in the Elderly Polypharmacy Adherence

M.H.FarjooM.H.Farjoo
Principles of Drug Therapy
The fundamental assumption for any drug is that the benefit exceeds the risk.
The goals of drug therapy in heart disease include: Acute correction of serious pathophysiology Symptom relief Changes in “surrogate” endpoints (blood pressure,
serum cholesterol, INR)

M.H.FarjooM.H.Farjoo
Principles of Drug Therapy Cont’d
A survey (CAST) tested the hypothesis that suppression of ventricular ectopic beats would reduce mortality.
CAST proved that some antiarrhythmics suppressed ventricular ectopic beats but increased mortality threefold.
In heart failure positive inotropic drugs are used but increase mortality (drug-induced arrhythmias).
Prescribers should be cautious about therapy in the absence of controlled clinical trials.

M.H.FarjooM.H.Farjoo
Principles of Drug Therapy Cont’d
The risks of drug therapy may be: Related to its pharmacological actions:
Excessive hypotension due to antihypertensives Bleeding due to anti platelet drugs (Abciximab,
Dipyridamol).
Unrelated to its action: Rhabdomyolysis with HMG-CoA reductase inhibitors Angioedema due to ACEI therapy Torsades de pointes by thioridazine or pentamidine.

M.H.FarjooM.H.Farjoo
Variability in Drug Effect
Variability in drug effect is due to: Pharmacokinetic parameters
Pharmacodynamic parameters
Pharmacogenomics parameters

M.H.FarjooM.H.Farjoo
Pharmacokinetic Parameters
Cardiovascular disorders that impair cardiac output may affect all the pharmacokinetic factors: Absorption of oral, SC, IM, and topical drugs is
erratic because of decreased blood flow to sites of drug administration.
Distribution is impaired because of decreased blood flow to sites of drug action.
Metabolism and excretion are impaired because of decreased blood flow to the liver and kidneys.

M.H.FarjooM.H.Farjoo
Pharmacokinetic Parameters Cont’d
Failure of one metabolizing pathway will not affect a drug using multiple elimination routes.
A drug eliminated by one pathway will accumulate if the pathway fails.
In this case there is a risk of toxicity, especially if therapeutic margin is narrow.

Therapeutic margin

M.H.FarjooM.H.Farjoo
Pharmacokinetic Parameters Cont’d
An example is terfenadine, which is eliminated exclusively by CYP3A.
Terfenadine is a highly potent QT-prolonging agent. Coadministration of terfenadine with CYP3A
inhibitors (ketoconazole, Erythromycin) leads to marked QT prolongation, and torsades de pointes.
CYP3A inhibition also increases the risk of rhabdomyolysis with some HMG-CoA reductase inhibitors and Fibrates.

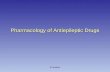
ECG

Torsade depointes
Polymorphic V.Tach. (torsades de pointes), which may degenerate into V. Fib.
There is a high risk of sudden death in this syndrome.

M.H.FarjooM.H.Farjoo
Pharmacokinetic Parameters Cont’d
Heart disease carries with it a number of disturbances of drug elimination and sensitivity.
Patients with LVH have baseline QT prolongation, and thus risks of QT-prolonging antiarrhythmics may increase.
In heart failure, hepatic congestion can lead to decreased clearance and an increased toxicity with usual doses of lidocaine and beta blockers.

M.H.FarjooM.H.Farjoo
Pharmacokinetic Parameters Cont’d
In heart failure renal perfusion is reduced and requires dose adjustments.
Heart failure causes redistribution of regional blood flow => volume of distribution ↓ => drug toxicity ↑ (lidocaine).

M.H.FarjooM.H.Farjoo
Pharmacokinetic Parameters Cont’d
β blockers in patients with defective metabolism produces exaggerated heart rate slowing.
Digoxin is eliminated by P-glycoprotein-mediated efflux into bile and urine.
Inhibition of P-glycoprotein increases digoxin concentrations.

M.H.FarjooM.H.Farjoo
Pharmacodynamic Parameters
The effect of lytic therapy in a patient with or without coronary thrombosis is different.
the arrhythmogenic effects of digitalis depend on K+.
The vasodilating effects of nitrates, beneficial in angina, can be catastrophic in aortic stenosis.

M.H.FarjooM.H.Farjoo
Pharmacogenomics Parameters
An example is resistance to antiplatelet actions of aspirin and Clopidogrel (an anti ADP receptor drug)
DNA variants are recognized as contributors to variability in drug action.
There is associations between disease severity and DNA polymorphisms.
This affects β blockers, ACEI, Fluvastatin, Diuretics, Antiplatelet drugs and Amiloride.

effect of a beta-receptor polymorphism on receptor function in vitro. Patients with the hypofunctional variant may display greater heart-rate slowing or blood pressure lowering on exposure to receptor blocking agents.
Beta blockers

M.H.FarjooM.H.Farjoo
Dosage Optimization
When the goal of drug therapy is to acutely correct a disturbance the drug should be administered IV.
Large IV boluses has the risk of enhancing drug-related toxicity.
Even with the most urgent of medical indications, this approach is rarely appropriate.
An exception is adenosine, which must be injected as a rapid bolus (1-2 Sec.) because rapid elimination from plasma.

Large IV bolus

M.H.FarjooM.H.Farjoo
Dosage Optimization Cont’d
When adverse effects are serious, the treatment should start at low doses.
For example the risk of torsades de pointes increases with sotalol dosage, the starting dose should be low.
Only when stable drug effects are achieved, increasing drug dosage may be considered.

low doses

M.H.FarjooM.H.Farjoo
Dosage Optimization Cont’d
Drug monitoring is best accomplished at the time of anticipated peak drug concentrations.
Assessing QT prolongation by sotalol or dofetilide is accomplished 1 to 2 hours after a dose of drug at steady state.

M.H.FarjooM.H.Farjoo
Drug Therapy in the Elderly
Age is a major factor in determining drug doses and sensitivity to drug effects.
Elderly persons have reduced creatinine clearance, even with a normal creatinine level
Dosages of renally excreted drugs should be adjusted.

M.H.FarjooM.H.Farjoo
Drug Therapy in the Elderly Cont’d
Systolic dysfunction with hepatic congestion is more common in the elderly.
Vascular disease and dementia are common in the elderly and can lead to increased postural hypotension.
Thus therapies such as sedatives, TCAs or anticoagulants should be initiated only when the benefits outweigh the risk.

M.H.FarjooM.H.Farjoo
Drug Therapy in the Elderly Cont’d
Weight adjustment for loading doses of digoxin, lidocaine and heparin are standard.
Fibrinolytic drugs without dosage adjustment increase the risk of intracranial hemorrhage in older age.
Dosage/weight adjustments should be made especially for drugs with low therapeutic index.

M.H.FarjooM.H.Farjoo
Drug Therapy in the Elderly Cont’d
Adverse drug events account for up to 5 percent of hospital admissions.
Digoxin, warfarin, diuretics, and Ca2+ channel blockers have “preventable” adverse effects in elderly.
The risk of side effects with cardiovascular drugs is 2.4 times that of other medications in hospitalized patients

M.H.FarjooM.H.Farjoo
Drug Therapy in the Elderly Cont’d
“Inappropriate” drugs in the elderly include: Amiodarone Clonidine Disopyramide Ethacrynic acid Guanethidine
Medications in patients with life expectancy too short to achieve long-term benefits merits discontinuation.

M.H.FarjooM.H.Farjoo
Polypharmacy
The most important principle in polypharmacy is to recognize the high potential for drug interactions.
A complete medication history should be obtained from each patient at regular intervals.
Patients omit topical medications, eye drops, “health food” supplements, and drugs prescribed by other practitioners.

M.H.FarjooM.H.Farjoo
Polypharmacy Cont’d
Even high dosages of grapefruit juice, which contains CYP3A and P-glycoprotein inhibitors, can affect drug responses.
Beta blocker eye drops (timolol) can produce systemic beta blockade in patients with defective metabolizing activity.

M.H.FarjooM.H.Farjoo
Adherence
Medication adherence is lower in older patients compared with younger patients.
Hospitalization for decompensated congestive heart failure was due to noncompliance in 42% of elderly patients.

M.H.FarjooM.H.Farjoo
Adherence Cont’d
Contributing factors for non-adherence include: The cost of medications Difficulty in reading small print of written directions Hearing impairment Impaired memory Inadequate instructions Complex dosing regimens Difficulties with packaging materials Insufficient education on medication use.


Thank youAny question?