




DISECCION AORTICA TIPO B
Arturo Evangelista

Variable All Type A Type B p-value
(n=1351) (n=846) (n=505)
Age (yrs) 62.4 61.3 64.1 <0.001
Male 67.5% 66.5% 69.1% NS
HTN 71.4% 68.5% 76.2% 0.003
Marfan 4.6% 5.4% 3.4% 0.10
Prior Heart 17.6% 16.3% 19.7% 0.13
Surgery
Iatrogenic 4.6% 5.5% 3.0% 0.04
Demographics and History
IRAD Investigators
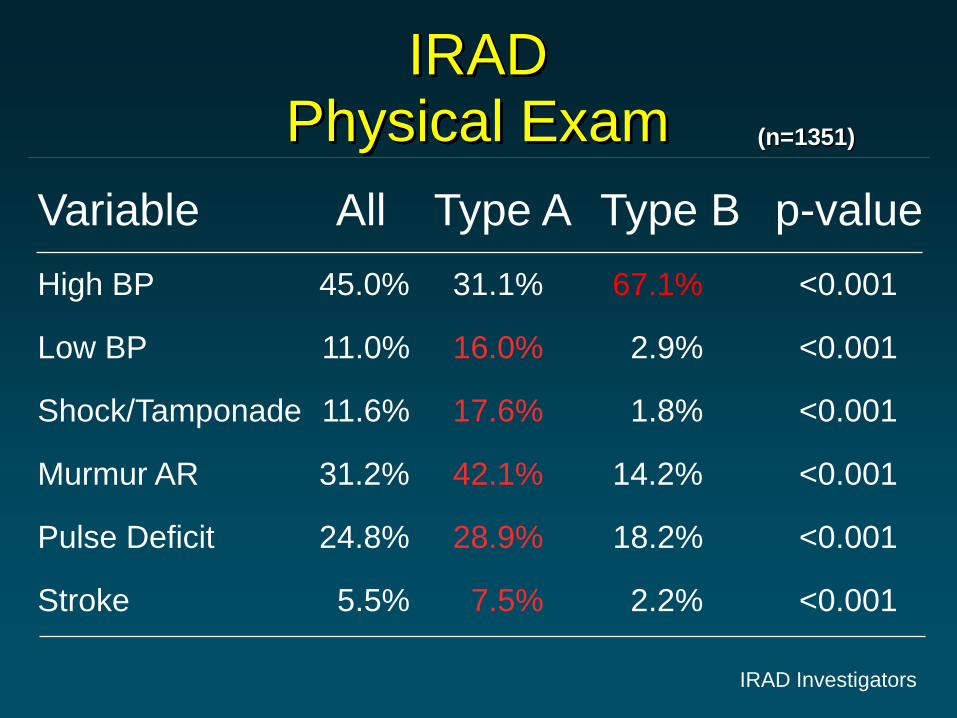
IRADPhysical Exam (n=1351)
Variable
High BP
Low BP
Shock/Tamponade
Murmur AR
Pulse Deficit
Stroke
All
45.0%
11.0%
11.6%
31.2%
24.8%
5.5%
Type A
31.1%
16.0%
17.6%
42.1%
28.9%
7.5%
Type B
67.1%
2.9%
1.8%
14.2%
18.2%
2.2%
p-value
<0.001
<0.001
<0.001
<0.001
<0.001
<0.001
IRAD Investigators

0
20
40
60
80
100
<=2.9 3.0-3.4 3.5-3.9 4.0-4.4 4.5-4.9 5.0-5.4 5.5-5.9 6.0-6.4 6.5-6.9 >=7.0
Descending Aortic Diameter ≥ 6.0cm:
A Poor Predictor of Type B Aortic Dissection
Co
un
t
Trimarchi S, et al. J Am Coll Cardiol 2009;53: A452.
Descending Diameter
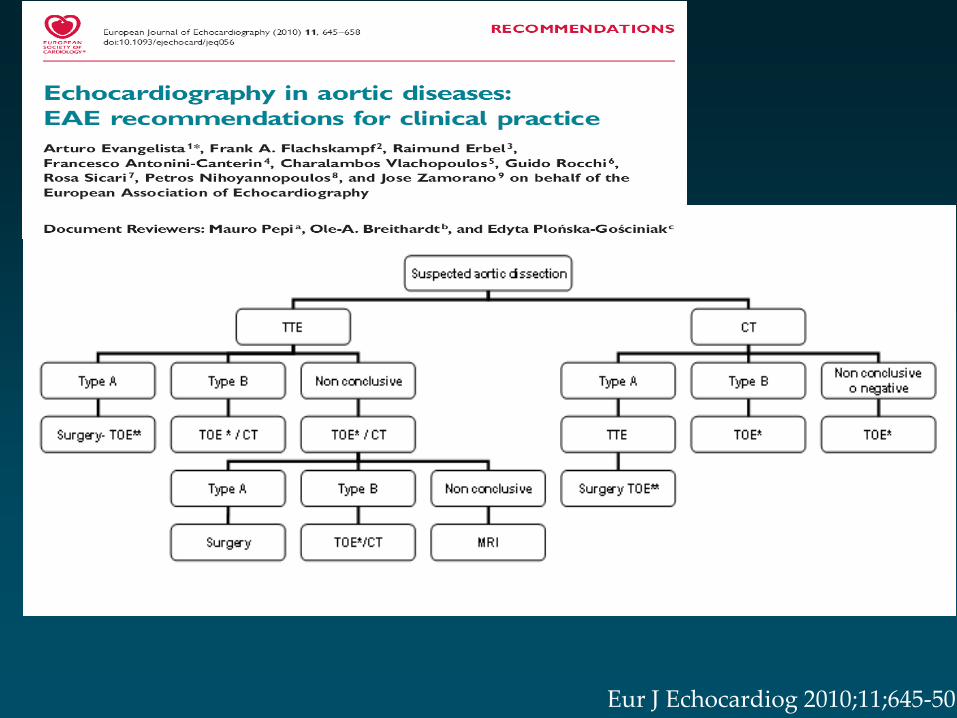
Eur J Echocardiog 2010;11;645-50

Three-year mortality of Type B AAS
Tsai TT, Evangelista A et al. Circulation 2006;114:2226-31
10,0%
22,4%
29,0%
17,2%
11,0%
23,8%
0,0%
10,0%
20,0%
30,0%
40,0%
Medical Surgical Endovasc.
In Hospital Follow-Up
p=ns

Registro Español del Síndrome Aórtico Agudo
Mortalidad Tipo BRegresión Logística Análisis Multivariado
Supervivientes
%
Exitus
%
OR ajustada Rango P
Shock 8,9 23,7 2,59 0,89-7,58 0,08
Déficit
neurológico
6,5 21,1 3,22 0,96-10,30 0,06
Isquemiamesenterica
0,8 23,7 41.74 4,89-356,37 0,001
Insuficiencia
renal
16,9 47,4 2,44 0,98-6,07 0,05
Modelado multivariado valor predictivo 81,2%
N:162 (31%

Compression Celiac Trunk and
Mesenteric Artery Ostia
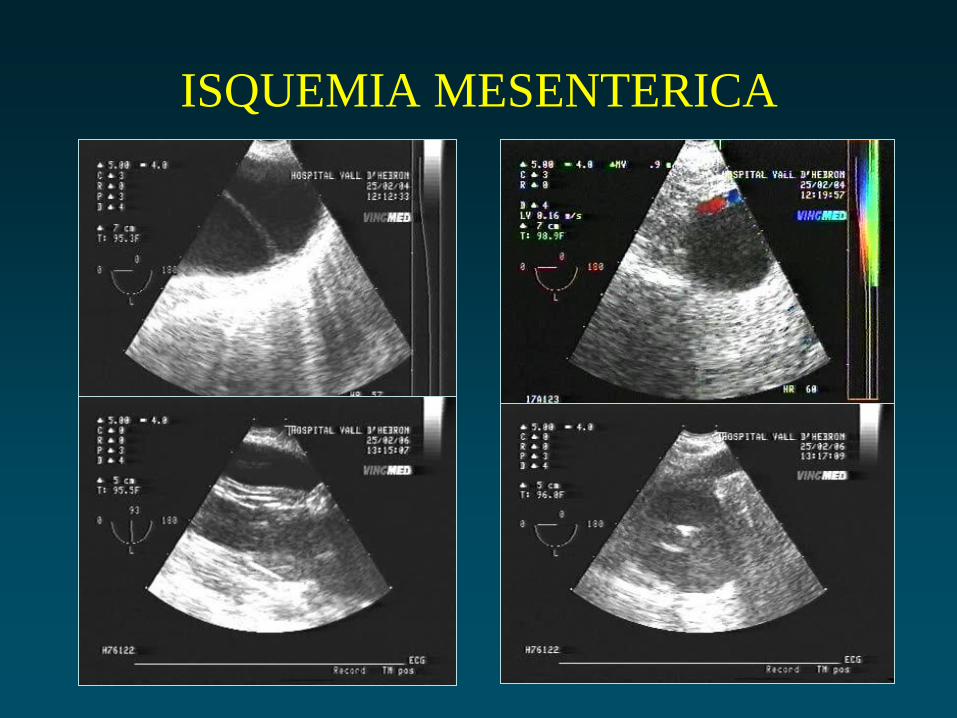
ISQUEMIA MESENTERICA

Type B Dissection
Use of Endovascular tx and Mortality
12%
10%
20%
12%
0%
4%
8%
12%
16%
20%
1996-2000 2000-2008
Endovascular
Mortality
p=.004
p=.72
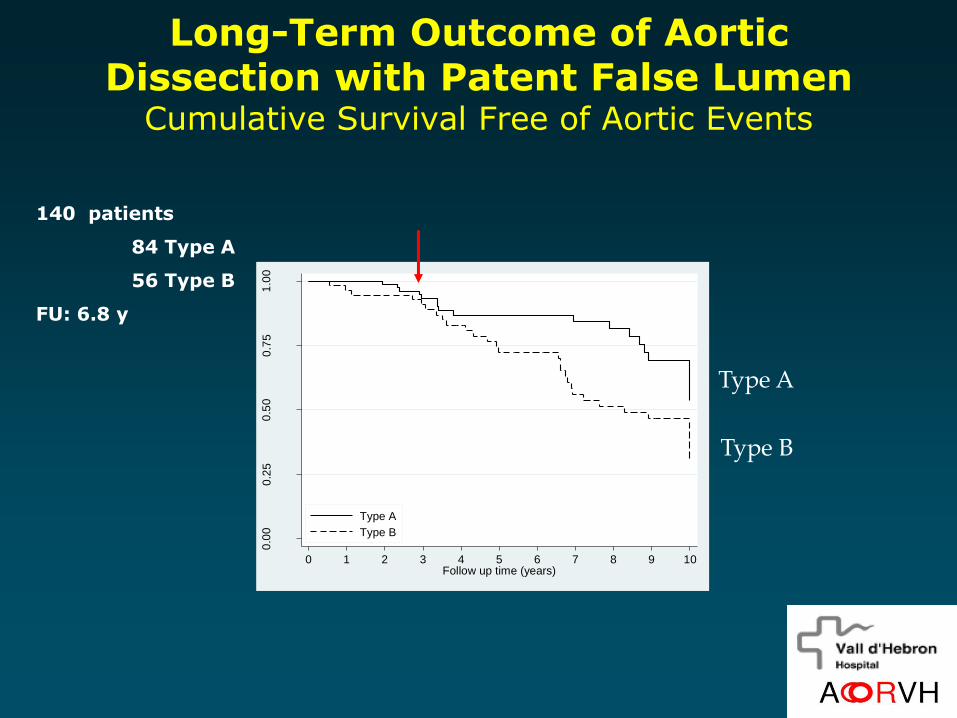
Long-Term Outcome of Aortic Dissection with Patent False Lumen
Cumulative Survival Free of Aortic Events
0.0
00
.25
0.5
00
.75
1.0
0
Su
rviv
al
0 1 2 3 4 5 6 7 8 9 10Follow up time (years)
Type A
Type B
Type A
Type B
140 patients
84 Type A
56 Type B
FU: 6.8 y
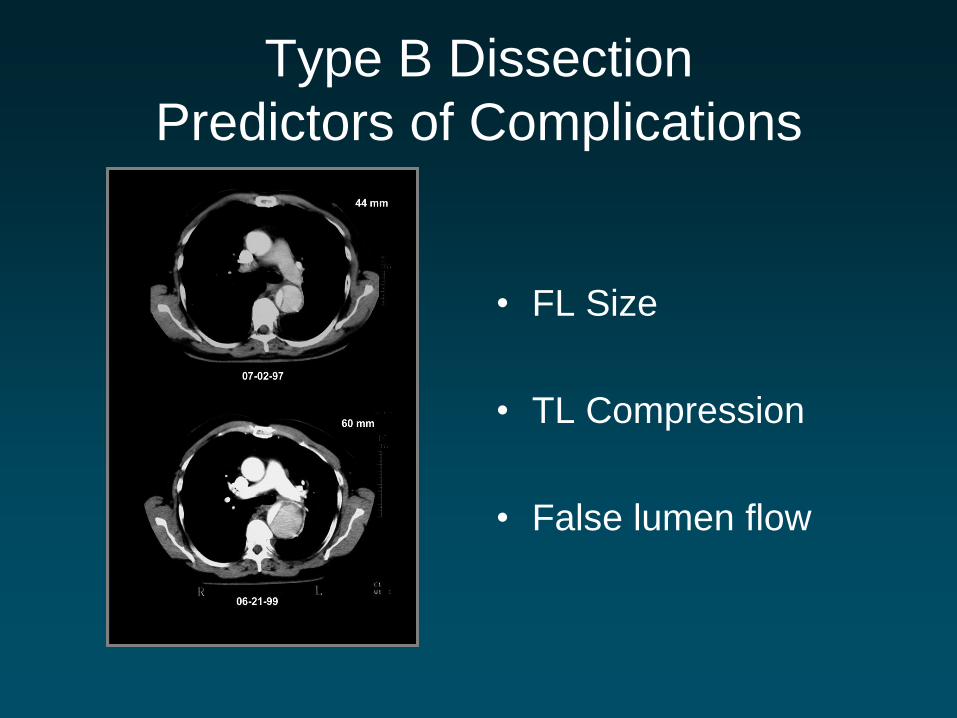
Type B Dissection
Predictors of Complications
• FL Size
• TL Compression
• False lumen flow

J AM Coll Cardiol 2007;50:799-804
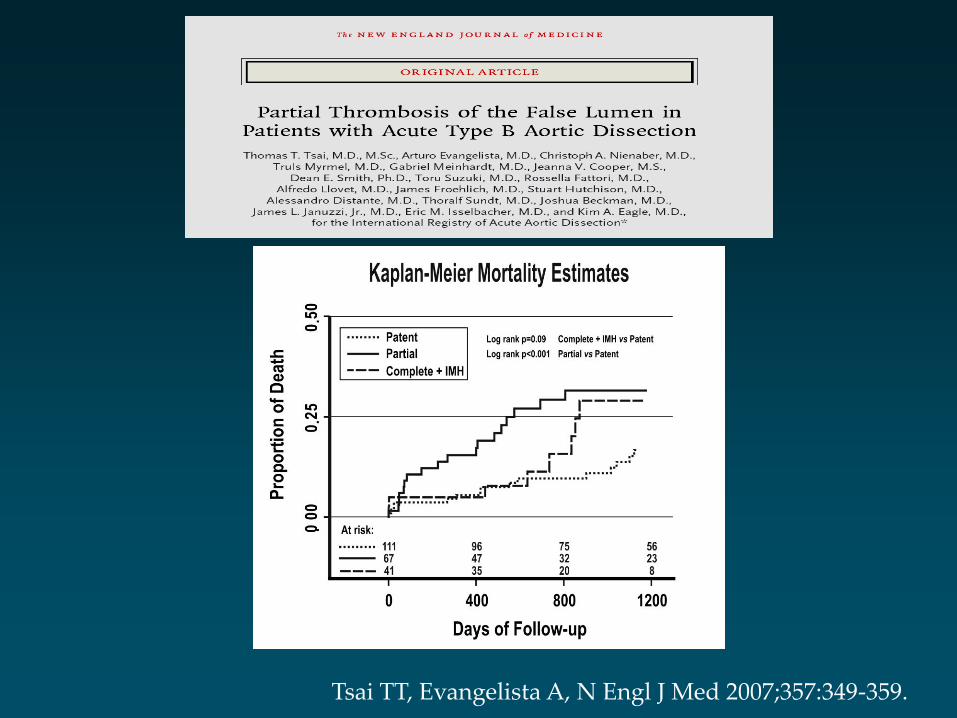
Tsai TT, Evangelista A, N Engl J Med 2007;357:349-359.

Tsai T, Evangelista A et al. NEJM 2007;357:349-359.

Entry tear location and size by TEE / CT
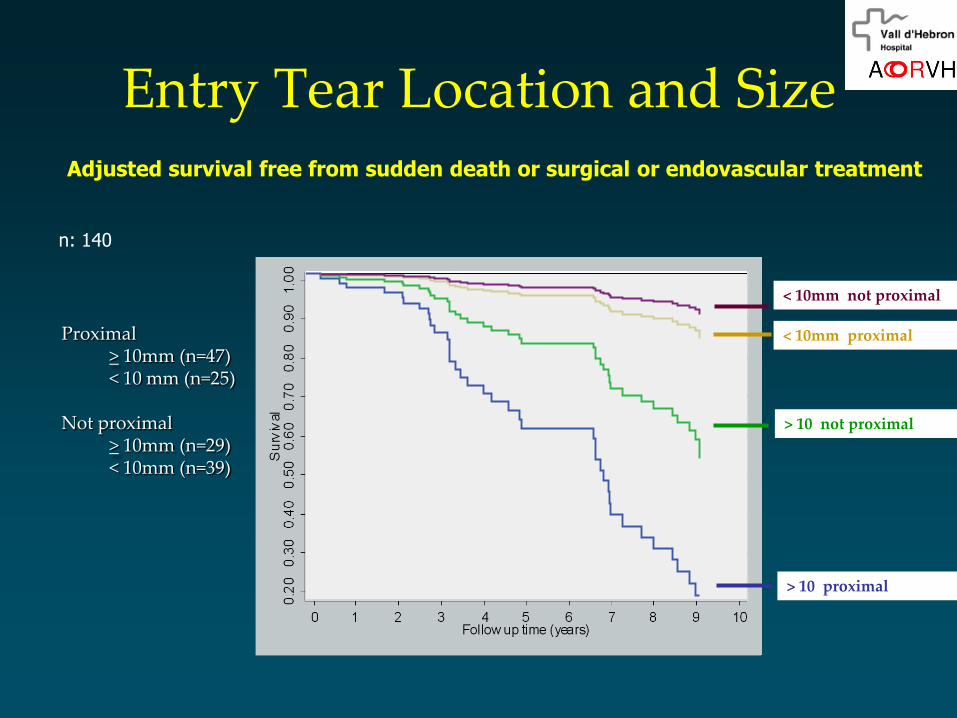
Entry Tear Location and Size
10,008,006,004,002,000,00
tiempo de seguimiento hasta el evento final(muerte, cirugía o stant de la AD)
1,0
0,9
0,8
0,7
0,6
0,5
0,4
Cu
m S
urv
ival
3,00
2,00
1,00
,00
0 '>9 y proximal' 1'>9 y NO Proximal'2 '<10 y proximal'
3 '<10 y NOproximal'
Survival Function for patterns 1 - 4
Adjusted survival free from sudden death or surgical or endovascular treatment
Proximal > 10mm (n=47)< 10 mm (n=25)
Not proximal> 10mm (n=29)< 10mm (n=39)
< 10mm not proximal
< 10mm proximal
> 10 not proximal
> 10 proximal
n: 140

Descending Aorta Enlargement
0
0,2
0,4
0,6
0,8
1
1,2
1,4
1,6
1,8
Type A Type B < 10 mm > 10 mm
P<0,001p: ns
0.68 1.67
1.07 1.80
0.41 0.73
1.62 2.72
mm/y
Follow-up: 6.8 y
Usefulness of real-time three-dimensional transoesophageal echocardiography in the assessment of
chronic aortic dissection.
Eur J Echocard in press
Artur Evangelista, Rio Aguilar , Hug Cuellar, Martin Thomas, Ana Laynez, Jose Rodríguez-Palomares, Patricia Mahia,
Teresa González-Alujas, David Garcia-Dorado.

Tratamiento Médico Endovascular+
Médico
p
Mortalidad 4,4% 11,1% 0,2
Mortalidad
aórtica
2,9% 5,6% 0,7
Cirugía 4,4% 4,2% 1
Paraplegia 1,4% 2,8% 0,9
AVC 0 2,8 0,5
Diámetro Ao
mm
48±13 44±13 0,3
Diámetro FL
mm
27 ±10 14±16 <0,001
597 pacientes (DA tipo B >14 dias) 293 rechazaron
164 exclusión
140 randomizados
Trat. Endovasc: 39 dias (18-252)

Endovascular TreatmentLarge and proximal entry tear






























