Disaster and Field Triaging
Dr Selvendra

Disaster
• Incident that occurs in a sudden manner, complex in nature, resulting in the loss of lives, damages to the property or the environment as well as affecting the daily activities of the community
• Requires the handling of resources, equipment, and manpower from various agencies as well as effective coordination.
• Involves complex action, long period of duration
TYPES OF DISASTERS
• Natural disaster e.g. flood,landslide• Industrial disaster e.g. fire• Accidents of dangerous/hazardous material• Collapse of high rise buildings• Aviation accidents in public places• Railway accidents• Major fire incident• Collapse of hydroelectric dam• Nuclear and radiological accidents• Release of toxic gas in public places• Air and environmental disasters e.g. haze
Disaster management in Malaysia
• Majlis Keselamatan Negara Directive 20
• NSC formed Disaster Management and Relief Council
• Its aim is to coordinate disaster management at 3 levels – District, State, and Federal

Agencies Involved in Disaster
• PDRM• Tentera Diraja Malaysia• Special Malaysia Disaster Assistance and Rescue
Team (SMART)• Jabatan Kajicuaca• Jabatan Pengairan dan Saliran• Jabatan Kerja Raya• Jabatan Kebajikan• NGO e.g. PBSM, St. John Ambulance• JPAM• International cooperation
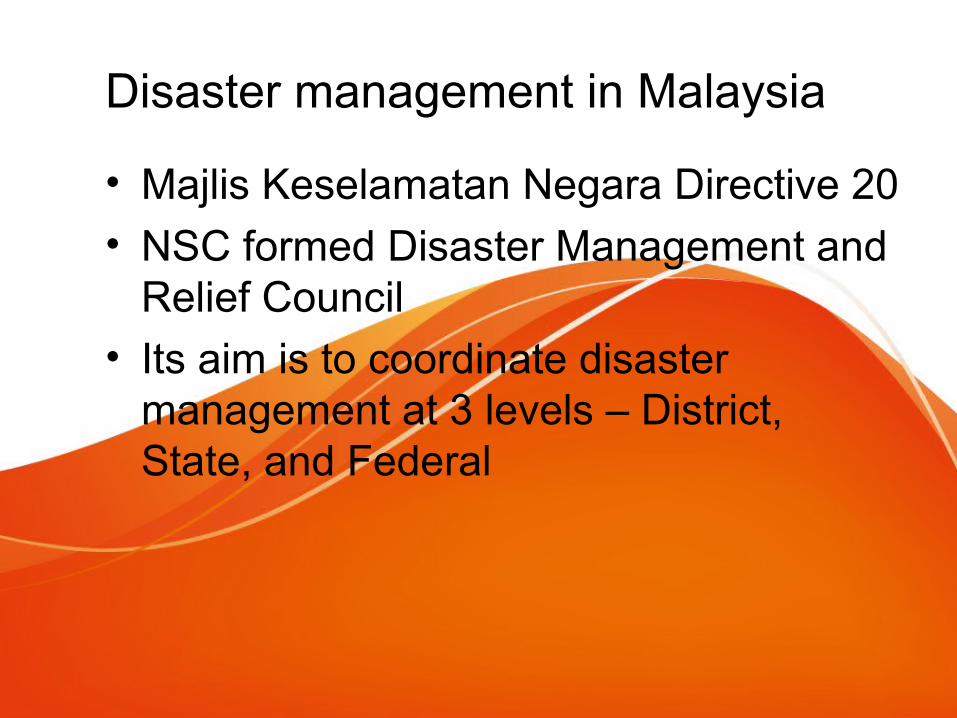
HIGHLAND TOWERS TRAGEDY 1993

TRIPLE TEN BUS ACCIDENT MAYHEM..
ON THE 10TH.10.10.. AT SIMPANG AMPAT, AYER KEROH, NORTH SOUTH HIGHWAY
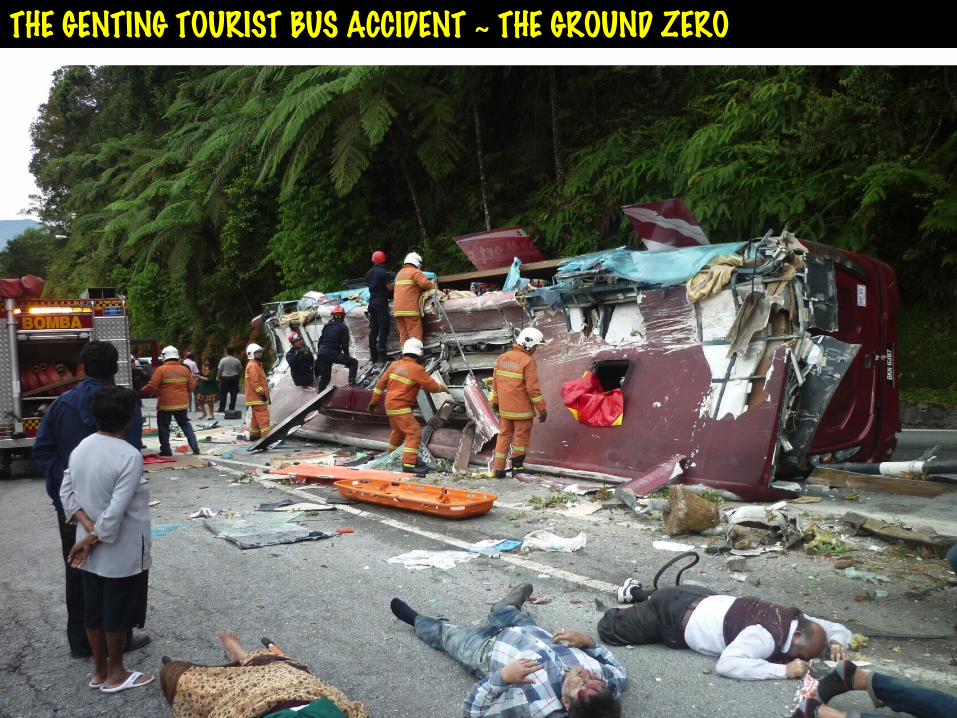
THE GENTING TOURIST BUS ACCIDENT ~ THE GROUND ZERO

Tsunami 2004





YET ANOTHER BUS ACCIDENT WITHIN ONE MONTH FOR GENTING BOUND PASSENGERS ~
sept 2013


Field Triage
Definition of Triage
• the process of deciding which patients should be treated first based on how sick or seriously injured they are.
Goal of Multicasualty Triage
“To do the best for the most
with the least.”

START(Simple Triage And Rapid Treatment)
Triaging < 15s
START• Triage categories:
– Green (ambulatory)– Red (immediate)– Yellow (delayed)– Black (dead or
nonsalvageable)
• Components of Assessment– Ambulation– Respirations– Perfusion– Mental status

START Triage
RESPIRATIONS
NO
YES
Non-salvageable
Immediate
Position Airway
NO YES
Over 30/min
Immediate
Under 30/min
PERFUSION
Radial PulseAbsent
ControlBleeding
Immediate
Radial Pulse Present
MENTALSTATUS
Failure to followsimple commands
Can followsimple commands
Immediate Delayed
JumpSTART
• For pediatric age group
• Reduce over and under triaging
• Achievable in 15s

The JumpSTART Field Pediatric Multicasualty Triage System ©(Patients aged 1- 8 years)
Black = Deceased/expectantRed = ImmediateYellow = DelayedGreen = Minor/Ambulatory
Identify and direct all ambulatory patients to designatedGreen area for secondary triage and treatment. Begin assessment of nonambulatory patients as you come to them.Proceed as below:
Spontaneous respirations?
NO
Open airway
Spontaneous respirations?
YES
IMMEDIATE
NO
DECEASED
YES
Peripheral pulse?
YES
Perform 15 sec.Mouth to MaskVentilations
Spontaneous respirations?
YES
IMMEDIATE
NO
DECEASED
NO
Check resp. rate
< 15/min or
> 40/minor irregular
IMMEDIATE
15 - 40/ min,regular
Peripheral pulse?
NO
IMMEDIATE
YES
Check mental status(AVPU)
AVP (appropriate)
DELAYED
P (inappropriate)U
IMMEDIATE
MINOR
© Lou Romig MD, FAAP, FACEP, 1995

JumpSTART: Breathing?
• If breathing spontaneously, go on to the next step, assessing respiratory rate.
• If apneic or with very irregular breathing, open the airway using standard positioning techniques.
• If positioning results in resumption of spontaneous respirations, tag the patient immediate and move on.
JumpSTART: Respiratory Rate• If respiratory rate is 15-40/min (roughly
one breath every 2-4 seconds), proceed to assess perfusion.
• If respiratory rate is <15 or >40/min (slower than one breath every four seconds or faster than one breath every 2 seconds) or irregular, tag patient as immediate and move on.
JumpSTART:Perfusion
• If peripheral pulse is palpable, proceed to assess mental status.
• If no peripheral pulse is present (in the least injured limb), tag patient immediate and move on.

JumpSTART: Mental Status• Use AVPU scale to assess mental status.
• If Alert, responsive to Verbal, or appropriately responsive to Pain, tag as delayed and move on.
• If inappropriately responsive to Pain or Unresponsive, tag as immediate and move on.

The “Jumpstart” Part If no breathing after airway opening, check
for peripheral pulse. If no pulse, tag patient deceased/nonsalvageable and move on.
If there is a peripheral pulse, give 15 sec of Mouth to Mask ventilations (about 5 breaths). If apnea persists, tag patient deceased/nonsalvageable and move on.
• If breathing resumes after the “jumpstart”, tag patient immediate and move on.

START/JumpSTART:Differences• Apneic children are rapidly assessed for
sustained circulation.
• Apneic children with circulation receive a brief ventilatory trial as an additional airway opening and stimulating maneuver.
• Respiratory rates are adjusted.
• Peripheral pulse is substituted for cap. refill. This is now done in START too.
• AVPU is used to assess mental status.




![Islam final ppw[1]](https://static.cupdf.com/doc/110x72/54c4917e4a795917618b4657/islam-final-ppw1.jpg)